International Human Rights and the Mistreatment of Women during Childbirth
Rajat Khosla*, Christina Zampas*, Joshua P. Vogel, Meghan A. Bohren, Mindy Roseman, and Joanna N. Erdman
Abstract
International human rights bodies have played a critical role in codifying, setting standards, and monitoring human rights violations in the context of sexual and reproductive health and rights. In recent years, these institutions have developed and applied human rights standards in the more particular context of maternal mortality and morbidity, and have increasingly recognized a critical human rights issue in the provision and experience of care during and after pregnancy, including during childbirth. However, the international human rights standards on mistreatment during facility-based childbirth remain, in an early stage of development, focused largely on a discrete subset of experiences, such as forced sterilization and lack of access to emergency obstetric care. As a consequence, the range of mistreatment that women may experience has not been adequately addressed or analyzed under international human rights law. Identifying human rights norms and standards related to the full range of documented mistreatment is thus a first step towards addressing violations of human rights during facility-based childbirth, ensuring respectful and humane treatment, and developing a program of work to improve the overall quality of maternal care. This article reviews international human rights standards related to the mistreatment of women during childbirth in facility settings under regional and international human rights law and lays out an agenda for further research and action.
Introduction
International human rights bodies have played a critical role in codifying, setting standards, and monitoring human rights violations in the context of sexual and reproductive health and rights.1 In recent years, these institutions have developed and applied human rights standards in the more particular context of maternal mortality and morbidity, and have increasingly recognized a critical human rights issue in the provision and experience of care during and after pregnancy, including during the time of childbirth.2, 3 However, the international human rights standards on mistreatment during facility-based childbirth remain in an early stage of development, focused largely on a discrete subset of issues such as forced or coerced sterilization and denied or neglected access to emergency obstetric care. A recent systematic review of the scientific literature documented an extensive range of mistreatment to which women are subjected during childbirth, including forms of physical, verbal, and sexual abuse; experiences of discrimination and neglect; and denials of privacy, confidentiality, and high-quality care.4 However, many forms of mistreatment remain unaddressed or inadequately analyzed under international human rights law.
The World Health Organization (WHO) addressed this gap in a 2014 statement on mistreatment during childbirth and its associated human rights violations, calling for greater action, dialogue, research, and advocacy on this global problem.5 The statement, endorsed by more than 90 international, civil society, and health professional organizations, affirms that “every woman has the right to the highest attainable standard of health, which includes the right to dignified, respectful health care throughout pregnancy and childbirth.”6 This right was further highlighted in 2015, as UN and regional human rights experts, the rapporteur on the rights of women of the Inter-American Commission on Human Rights, and the special rapporteurs on the rights of women and human rights defenders of the African Commission on Human and Peoples’ Rights issued a joint statement explicitly calling on states to address “acts of obstetric and institutional violence.”7
Identifying human rights norms and standards related to the full range of documented mistreatment is thus a first step towards addressing violations of human rights during facility-based childbirth, ensuring respectful and humane treatment, and developing a program of work to improve the overall quality of maternal care. A qualitative evidence synthesis found that mistreatment during childbirth is a potent disincentive for women to attend facilities in low- and middle-income countries.8 Hence, efforts to improve maternity care could also encourage more women to use facilities during pregnancy and childbirth.
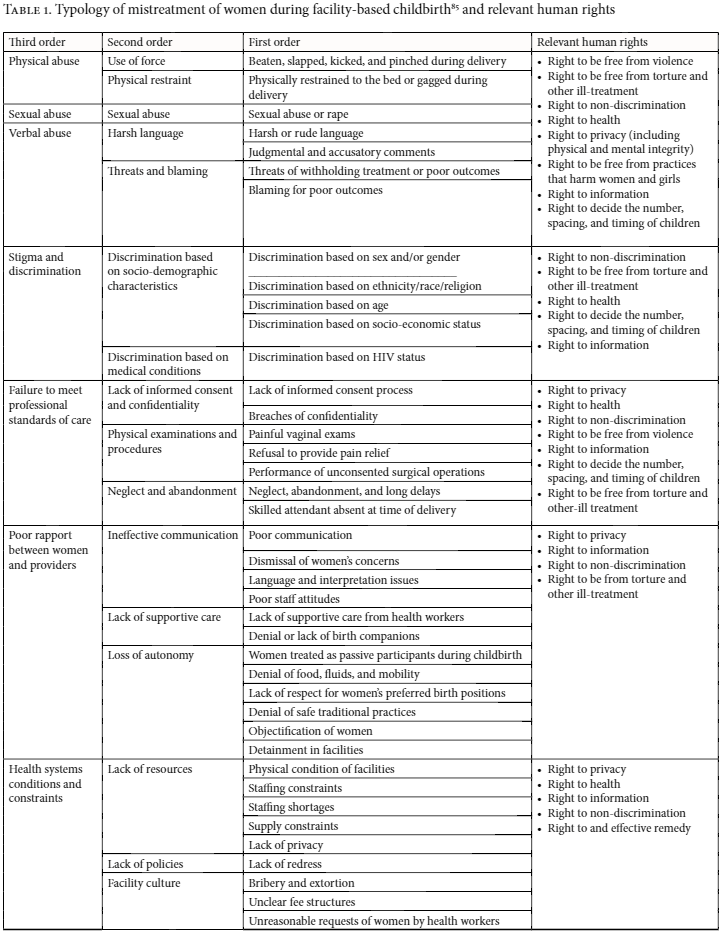
Based in international and regional treaty law, human rights standards are developed through authoritative interpretations by a diverse set of institutions, including treaty-monitoring bodies, the Human Rights Council and special rapporteurs, and regional courts and commissions, all of which have been addressing different aspects of treatment of pregnant women in health care settings in their different reports over the years. Any one form of mistreatment may implicate multiple human rights and result in their violations, reflected in Table 1.
This article reviews existing international human rights standards related to the mistreatment of women during childbirth in facility settings under regional and international human rights law. While this article acknowledges the critical role of national legal systems in developing human rights standards, its objective is to identify and articulate human rights standards in international law.
Methods
The starting point of this review of human rights standards was a mixed-methods systematic review published by Bohren and colleagues which identified several forms of mistreatment women experience during childbirth in health facilities: physical, sexual, and verbal abuse; stigma and discrimination; care that falls short of professional standards; and poor rapport with providers. The review also identified health system factors contributing to these occurrences and proposed a typology of the identified forms of mistreatment.9 This typology, presented in Table 1, is organized by common attributes of specific events or instances of mistreatment during childbirth in facilities.
The review of human rights standards was conducted in two stages. First, a review was undertaken of reports, concluding observations, and general comments of the UN Human Rights Council, treaty monitoring bodies, and special rapporteur reports. Four databases were searched: the OHCHR Universal Human Rights Index; Bayefsky.com; the University of Minnesota Human Rights Library; and the Universal Periodic Review (UPR). Findings included results from documents of the Committee against Torture (CAT); Committee on the Elimination of Discrimination against Women (CEDAW); Committee on the Rights of the Child (CRC); Committee on Economic, Social and Cultural Rights (CESCR); Human Rights Committee (HRC); the special rapporteur on the right to health; and the special rapporteur on torture. Relevant findings of the UN Human Rights Council, other treaty monitoring bodies, and special rapporteurs (including reports, concluding observations, and general comments) were also reviewed. Second, a regional review was undertaken. This included a review of resolutions and decisions of regional human rights bodies: Inter-American Commission of Human Rights (IACHR/CIDH) (including the Organization of American States (OAS)); the African Commission of Human and Peoples’ Rights (including the African Union); and the European Court of Human Rights (ECHR) (including the Council of Europe). All recovered documents were critically reviewed in relation to normative developments regarding mistreatment of women during childbirth.
For both stages of review, search terms were variations on the following concepts: childbirth, informed consent, discrimination, accountability, abuse in childbirth, mistreatment during childbirth, sterilization, stigma, harmful practices during childbirth, sexual and reproductive health and rights, respect and disrespect, and reproductive choice. The review included findings covering 2000 to 2015 (general comments issued in 2016 were also reviewed). Searches were done for documents written in English, and also in Spanish for IACHR/CIDH, including the OAS and national judgments. We elected to begin the search with findings from 2000, when the UN Committee on Economic, Social and Cultural Rights issued General Comment No. 14, which set down a common framework for the development of human rights standards in health.10
The search covered all findings (including concluding observations, general comments, and recommendations) where international or regional human rights bodies had made explicit observations on mistreatment during childbirth, as well as those that dealt with the issue implicitly. Based on this initial search, data was extracted and organized according to human rights norms and standards that explicitly address events of mistreatment during childbirth (as referenced in the typology). Human rights standards that address more generally the treatment of women in the provision of reproductive health care were also included, on the assumption that such care includes childbirth. Findings without a specific focus on issues related to childbirth, or on mistreatment occurring during childbirth, were excluded.
Results
This section provides an overview of the international and regional human rights standards related to the mistreatment of women during childbirth in facility settings organized by the third-order themes presented in the Bohren et al. typology (Table 1). Acknowledging the indivisibility and interconnectedness of human rights, any one form of mistreatment may implicate multiple human rights, as reflected in the overlap of rights shown in Table 1.
Violence (physical, sexual, and verbal abuse)
Manifestations of violence against women during childbirth in facility settings are varied. Women have reported physical and verbal abuse, such as beatings, hitting, slapping, kicking, and pinching.11 The use of mouth gags and bed restraints, such as shackles and ropes, during labor is also documented.12 Health care professionals (including obstetricians) have been reported for sexually assaulting their patients.13 There is extensive documentation of demeaning and degrading verbal abuse by maternity care providers.14 These include the use of abusive, harsh, or rude language, threats to withhold treatment or of poor outcomes, as well as judgmental, accusatory remarks.15 Women from marginalized communities, such as racial and ethnic minorities, refugees, unmarried women, and adolescents, may be more vulnerable to this abuse.16
International and regional human rights experts have also noted the severity of obstetric violence faced by women giving birth while in detention facilities. In a joint statement, a group of special rapporteurs noted: “We are deeply disturbed by reports of women being shackled to their hospital beds whilst giving birth in prison.”17 Other human rights bodies have reiterated this concern. The UN Committee Against Torture has also expressed concern over “the treatment of detained women,” including “incidents of shackling of women detainees during childbirth.”18 The committee recommended that state parties “should adopt all appropriate measures to ensure that women in detention are treated in conformity with international standards.”19
Such abuse impinges on women’s human right to be free from gender-based violence, defined as “acts that inflict physical, mental or sexual harm of suffering, threats of such acts, coercion, and other deprivations of liberty.” These acts impair or nullify women’s fundamental rights, including the rights to health and privacy.20 The right to live free from violence is based in norms of physical, sexual, and psychological integrity, and extends to both the public and private spheres.21
Acts of violence during childbirth may also constitute violations of the right to be free from torture, or cruel, inhuman, or degrading treatment, which is protected by numerous international and regional treaties.22 Cruel, inhuman, and degrading treatment is not restricted to acts that cause physical pain, but also encompasses acts that result in mental suffering.23 Treatment withheld during pregnancy that causes the patient emotional distress, for example, has been interpreted as inhuman and degrading treatment.24 The special rapporteur on torture recently called attention to the ways health care professionals may inflict physical and psychological suffering, amounting to cruel, inhuman, and degrading treatment and torture, on women before, during, and after childbirth.25
Stigma and discrimination
International human rights law guarantees the right to be free from discrimination on the basis of sex, race, health status, sexual orientation, economic or social status, gender, disability, age, and other statuses.26
The mistreatment of women during facility-based childbirth raises concerns of sex and gender discrimination because it exclusively impinges upon the health and rights of women and limits their enjoyment of equality in access to health care.27 International human rights law recognizes, too, the particular vulnerability of pregnant women, including during childbirth and for a reasonable period before and after, which may render them at greater risk of mistreatment in health care settings.28
Such mistreatment can result from negative gender stereotyping, for example, about women’s lack of decision-making capacity, or their deservedness of suffering or punishment.29 The African Commission on Human and People’s Rights has addressed the need to eliminate gender stereotyping in reproductive health care settings, emphasizing that efforts should “be especially made to address patriarchal attitudes, as well as the prejudices of health care providers.”30
Women who belong to marginalized groups may also be vulnerable to mistreatment during childbirth due to their age, race/ethnicity, socio-economic, migration, and/or health status, sexual orientation/gender expression, and/or location.31 The enhanced risk of human rights abuses in the context of reproductive health care, based on sex and/or gender and such intersecting factors is well documented, and is often referred to as intersectional or multiple discrimination.32 The HRC and CRC, for example, have both recognized the vulnerability of girls to denials of reproductive health services and information on the basis of age.33 The CEDAW Committee attributed poor quality of care in a case on maternal mortality to the intersecting vulnerabilities of gender, race, and socio-economic status.34 Other forms of mistreatment that violate the right to be free from discrimination include segregation within maternity hospitals on the basis of race and/or ethnic origin, as experienced by Roma women in Europe, and the detention of women in maternity hospitals following childbirth because of their inability to pay (economic status).35, 36
Refusal of care is another form of economic discrimination. The CEDAW Committee, for example, raised concern under the right to non-discrimination in access to health care services for the “many women [who] are at risk of death or disability from pregnancy-related causes because they lack the funds to obtain or access the necessary services, which include antenatal, maternity and post-natal services.”37
Committees have also drawn attention to stigma and discrimination against poor women, manifested in the form of post-delivery detention of women within health facilities for non-payment of fees. The UN Committee against Torture (CAT) has recognized such detention as a deprivation of liberty and called for an end to the practice. Such practices are condemned in other human rights treaties. CEDAW obligates States Parties to ensure women receive appropriate services in connection with pregnancy, confinement, and the post-natal period, including free services where necessary.38 In interpreting this provision, the CEDAW Committee addressed the economic vulnerability of women in the context of childbirth.39 Part of the state obligation to ensure women’s right to safe motherhood thus includes state provision of services to the maximum extent of available resources.40
International human rights institutions have developed strong standards on coercive sterilization, including during labor and delivery, against HIV-positive women, Roma and indigenous women, and women with disabilities, which address, in particular, claimed medical justification for the practice.41 The UN special rapporteur on torture, for example, acknowledged that “the administration of non-consensual medication or involuntary sterilization is often claimed as being a necessary treatment for the so-called best interest of the person concerned.”42 In setting a human rights standard against this practice, he referenced the ethical guidelines of the International Federation of Gynecology and Obstetrics, which state: “sterilization for the prevention of future pregnancy cannot be ethically justified on grounds of medical emergency.”43
In the context of individual cases, the CEDAW Committee and the ECHR have each developed human rights standards on coercive sterilization where professional standards of care, including informed consent standards, were not met.44 The ECHR, in a case against Slovakia in 2012, highlighted that in failing to secure a woman’s informed consent, they had acted with “gross disregard for her right to autonomy and choice as a patient” —regardless of the fact that the medical staff involved did not intend to mistreat the patient. The Court described the actions of the hospital staff as “paternalistic, since, in practice, the applicant [patient] was not offered any option but to agree to the procedure which the doctors considered appropriate.”45 Such treatment caused the patient “feelings of fear, anguish and inferiority and to entail lasting suffering.”46 Imposing medical treatment without informed consent, the Court concluded, is “incompatible with the requirement of respect for human freedom and dignity, one of the fundamental principles on which the [European] Convention [on Human Rights] is based.”47 The African Commission on Human and People’s Rights’ resolution on sterilization places particular emphasis on the involuntary sterilization of HIV-positive women.48
Failure to meet professional standards of care
Mistreatment of women in the reproductive health context, including mistreatment during childbirth, often occurs in the context of overall failures to meet professional standards of care. Painful and unnecessary exams, refusals to provide pain relief, neglect, abandonment and long delays, breaches of confidentiality, and the lack of informed consent including in the context of sterilization, as discussed above, are documented examples of such failures.49
The CEDAW Committee, in the context of women’s health generally, has called on governments to monitor the quality of health services, and to ensure that professional standards of care are met and health services are “delivered in a way that ensures that a woman gives her fully informed consent, respects her dignity, guarantees her confidentiality and is sensitive to her needs and perspectives.”50
Sexual and reproductive health, including during childbirth, involves many sensitive and personal matters that patients may wish to keep private within families or communities, but that they entrust to health care workers. Confidentiality includes the duty of providers to protect an individual’s privacy, and thus not to share patient information with third parties, including the woman’s spouse, parents, or other family members or friends, without the patient’s full and informed consent.51
This duty of medical confidentiality is important in the provision of health care during childbirth because many women are vulnerable to personal harm or discrimination when it is breached.52 Fear of disclosure of private information, such as HIV status, has also deterred women from attending facilities for childbirth.53
The ECHR has recognized the necessity of ensuring confidentiality and informed consent during facility-based childbirth. In a case involving a group of medical students observing a woman during childbirth without her consent, the Court noted that the patient only learned of the presence of the medical students while in a state of extreme stress and fatigue, between two sessions of drug-induced sleep, and during prolonged contractions. Given these circumstances, the Court questioned whether the patient actually had a choice regarding the students’ participation, and whether she was capable of making an intelligible, informed decision. In finding a violation of the right to respect for private life, the Court emphasized the lack of adequate notice, the patient’s vulnerable condition during childbirth, and the lack of alternative arrangements to ensure the patient has a meaningful opportunity to refuse observation.54
Failure to meet professional standards of care is sometimes attributed to power dynamics in health care settings, especially between health care providers, who hold medical knowledge, and patients, who are dependent upon the health system to obtain information and care. The UN special rapporteur on the right to health has recognized this power dynamic, describing the right to autonomy over medical decision-making as a counterweight to “the imbalance of power, experience and trust inherently present in the doctor-patient relationship.”55 This imbalance is reflected in the abuse of the doctrine of medical necessity to justify mistreatment. The UN special rapporteur on torture has recognized that “the doctrine of medical necessity continues to be an obstacle to protection from arbitrary abuses in health-care settings” and has acknowledged reports of “health providers withholding care or performing treatments that intentionally or negligently inflict severe pain or suffering for no legitimate medical purpose.”56 Medical care that causes severe suffering for no justifiable reason can be considered “cruel, inhuman or degrading treatment or punishment.”57
The CEDAW Committee has noted, for example, unnecessary and non-medically indicated interventions during childbirth, and has called for adequate safeguards to ensure that medical procedures during childbirth are subject to objective assessments of need, and are conducted with respect for women’s autonomy and informed consent.58 In addressing the historical practice of symphysiotomies conducted during childbirth, the Human Rights Committee called for the investigation, prosecution, and punishment of perpetrators, and for reparations to victims.59
Poor rapport between women and providers
Autonomy, often captured by the concept of informed decision-making, is a critical human rights component of reproductive health. Yet women commonly describe communication failures with health workers during facility-based childbirth, which leave them “feeling in the dark” about the state of their health (for example, with labor complications) and the nature of proposed care (benefits, risks, and alternatives).60 These failures sometimes stem from language or other interpretation barriers, but women also report that health workers withhold or rush through information in an effort to secure patient compliance.
Under the European Convention of Human Rights, the right of a pregnant woman to obtain available information about her health is protected under the right to respect for private life.61 The ECHR affirms: “In the context of pregnancy, effective access to relevant information on the mother’s and foetus’ health … is directly relevant for the exercise of personal autonomy.”62 To ensure equality in access to health care services, CEDAW likewise guarantees women the right “to be fully informed, by properly trained personnel, of their options in agreeing to treatment … including likely benefits and potential adverse effects of proposed procedures and available alternatives.”63 Critical to the full scope of this right is the timing and manner of information provision. For example, in a case involving the coercive sterilization of a Roma woman during an emergency Caesarean section, the CEDAW Committee emphasized that the patient “did not understand the Latin term for sterilization that was used on the barely legible consent note that had been handwritten by the doctor … [She was not given] information in a way in which she was able to understand it.”64 In finding the State Party in violation of its human rights obligations, the Committee referred to the medical records that revealed the patient was in a very poor state of health, even shock, when she was informed about the procedure and her consent obtained.
Human rights standards routinely link informed decision-making to values of both autonomy and dignity.65 Under the right to health, acceptable services are defined as those “delivered in a way that ensures that a woman gives her fully informed consent, respects her dignity, guarantees her confidentiality and is sensitive to her needs and perspectives.”66 Women commonly report not being respected, supported, or cared for by health workers during facility-based childbirth.67 Though technically sound, care that is lacking in compassion, attentiveness, and concern for women’s needs and perspectives leaves the patients feeling disempowered, frightened, and alone.68 In the aforementioned case involving non-consensual medical student observation of childbirth, the ECHR reaffirmed its longstanding position that the intimate nature of any medical intervention on the human body, however minor, implicates the right to respect for private life.69 In another case, a woman was denied access to prenatal diagnostic care, and the Court found a State Party in violation of the right to be free from inhuman and degrading treatment.70 The Court again recognized the vulnerability of pregnant women seeking information and care, especially those concerned with the healthy development of their pregnancies. The woman had endured weeks of painful uncertainty about her own and her family’s future because health workers failed to acknowledge and address her concerns.71 Moreover, the Court found that health workers had deliberately withheld treatment in an effort to frustrate the patient’s exercise of autonomy in the management of her pregnancy.72
UN treaty monitoring bodies and regional mechanisms have also drawn attention to the serious harms of removing newborns from the care of their mothers, against the mothers’ will, and without a compelling health-related justification.73 Such practices exploit the vulnerability of women in childbirth, reducing them to dependent and passive patients.
Health system conditions and constraints
Broader health system constraints and limitations can contribute, directly or indirectly, to women’s negative experiences during childbirth. Overworked or undertrained providers, overcrowded or unsanitary facilities, or a lack of medical supplies make it challenging for health care providers to provide respectful, woman-centered care.74 Under CESCR, the availability and quality of health facilities, goods, and services is an essential component of the right to health, as is the adequate training of obstetric care professionals.75
The Protocol on the Rights of Women in Africa (Maputo Protocol) more specifically obligates State Parties to “establish and strengthen existing pre-natal, delivery and post-natal health and nutritional services for women during pregnancy and while they are breast-feeding,” and requires that provider training include not only technical aspects of care, but quality of care issues such as “non-discrimination, confidentiality, respect for autonomy and free and informed consent.”76 In a case involving a poor woman who died as a result of obstetric complications while seeking care in multiple health facilities, the CEDAW Committee found the State Party in violation of the rights to life, health, and non-discrimination.77 These violations, as well as the CEDAW Committee’s recommendations for redress, reached system-level factors of neglect, including the inadequate resources and ineffective implementation of existing state policies.78 The Committee also affirmed that “the State is directly responsible for the action of private institutions when it outsources its medical services, and that furthermore, the State always maintains the duty to regulate and monitor private health-care institutions.”79
Human rights standards, including the right to health, the right to privacy, the right to be free from torture and other ill-treatment, and the right to an effective remedy, among other rights, require the adoption of clear legal and procedural frameworks to ensure the effective delivery of and access to health services. While health system constraints, including lack of resources or services, may create conditions for mistreatment in facility-based childbirth, they cannot be used to justify these actions.80 Rather, the UN special rapporteur on torture identifies states obligation to redress abuse within health systems by establishing adequate redress and accountability mechanisms, reforming regulation of the system, and promoting a culture of respect for human integrity and dignity within health settings.81 CESCR requires states to “ensure that all individuals have access to justice and to a meaningful and effective remedy in instances where the right to sexual and reproductive health is violated.”82 As interpreted in the maternal health context, the United Nations Human Rights Council obligates states to ensure accountability at the professional and institutional levels of the health system.83
Conclusion
Human rights standards are an important accountability tool for recognizing and protecting the human rights of women during childbirth in facilities, and for supporting health system reform to prevent mistreatment in the future. Human rights standards assist health care practitioners and policy makers to define what constitutes mistreatment during childbirth and to develop effective interventions and policies to address this mistreatment in all its forms. This review of existing human rights standards thus suggests two areas for action. First, there is a call for continued human rights monitoring and documentation to deepen our understandings of the nature of violations, their causes and effects, and the development of more comprehensive human rights standards to guide remedy and redress measures.84 Meaningful human rights accountability is not possible without systematic monitoring and other initiatives to gather information about the conditions of service access and delivery, to identify where and why patient-provider relations break down, and to thereby identify concrete actions the state can take to fulfill women’s human rights. Second, there is a need to develop innovative human rights accountability measures to enforce standards both for individual remedy and redress for victims of mistreatment, but also for constructive accountability within health systems to prevent future violations. These are measures that can effectively and sustainably transform health systems to shape and change the experience of service provision and access. This includes measures taken to ensure that hospital environments and staff are sufficiently trained and empowered to meet women’s emotional, physical, and medical needs and guarantee that human rights are respected. Supporting institutional arrangements for the active and informed participation of women as intended beneficiaries of maternal care in all aspects of its design and implementation is critical for constructive accountability.85 Engaging women and accounting for their experiences in health system reform is the first order of respect in a human rights approach to maternal care.86 Lastly, further research is needed to develop effective human rights-based interventions to promote and protect women’s sexual and reproductive health and rights and ensure respectful and dignified care for women during childbirth.
Acknowledgments
We would like to thank Ronita Bhattacharya for help with references.
Rajat Khosla is human rights advisor in the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland.
Christina Zampas is Reproductive and Sexual Health Fellow, International Reproductive and Sexual Health Law Program, Faculty of Law, University of Toronto, Ontario, Canada.
Joshua P. Vogel is a technical officer in maternal and perinatal health and preventing unsafe abortion, at the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland.
Meghan A. Bohren is a researcher in maternal and perinatal health and preventing unsafe abortion, at the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland.
Mindy Roseman is the Director of International Programs and Director of the Gruber Program for Global Justice and Women’s Rights, Yale Law School, New Haven, Connecticut, USA.
Joanna N. Erdman is the MacBain Chair in Health Law and Policy, Schulich School of Law, Dalhousie University, Halifax, Nova Scotia, Canada.
Please address correspondence to the authors c/o Rajat Khosla, Department of Reproductive Health and Research, World Health Organization, 20 Avenue Appia, CH-1211 Geneva 27, Switzerland. Email: khoslar@who.int.
Competing interests: None declared.
Copyright © 2016 Khosla, Zampas, Vogel, Bohren, Roseman, Erdman. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
*Rajat Khosla and Christina Zampas are joint first authors.
This article represents the views of the named authors only and not the views of their institutions or organizations.
References
- See, for example, Declaration of Commitment on HIV/AIDS, G.A Res. S-26/2. Available at http://www.un.org/ga/aids/docs/aress262.pdf.
- Office of the United Nations High Commissioner for Human Rights, Information series on sexual and reproductive health and rights: Maternal Mortality and Morbidity (2015). Available at http://www.ohchr.org/Documents/Issues/Women/WRGS/SexualHealth/INFO_MMM_WEB.pdf); United Nations Population Fund and Center for Reproductive Rights, ICPD and Human Rights: 20 years of advancing sexual and reproductive rights through UN treaty bodies and legal reform (2013). Available at https://www.unfpa.org/sites/default/files/pub-pdf/icpd_and_human_rights_20_years.pdf.
- Ibid.
- M.A. Bohren, J.P. Vogel, E.C. Hunter, et al., “The mistreatment of women during childbirth in health facilities globally: A mixed-methods systematic review,” PLoS Medicine 12(6) (2015), p. e1001847.
- World Health Organization, WHO Statement: The prevention and elimination of disrespect and abuse during facility-based childbirth (Geneva: WHO, 2014).
- Ibid.
- African Commission on Human and People’s Rights, Joint Statement by UN human rights experts, the Rapporteur on the rights of women of the Inter-American Commission on human rights and the Special Rapporteurs on the rights of women and human rights defenders of the African Commission on human and peoples’ rights (September 2015). Available at http://www.achpr.org/news/2015/09/d192/.
- M.A. Bohren, E.C. Hunter, H.M. Munthe-Kaas, et al., “Facilitators and barriers to facility-based delivery in low- and middle-income countries: A qualitative evidence synthesis,” BioMed Central Reproductive Health 11, no. 1 (2014), p. 71.
- Bohren et al. (2015, see note 4).
- United Nations Committee on Economic, Social and Cultural Rights, The Right to the Highest Attainable Standard of Health, E/C.12/200/4 (2000). (New York: United Nations, 2000); UN Committee on Economic Social, and Cultural Rights, Right to Sexual and Reproductive Health, E/C.12/GC/22. General Comment No. 14, (New York: United Nations, 2016), para. 8.
- Bohren et al. (2015, see note 4).
- Ibid.; Teixeira, N.Z. Fanaia, and W.R. Pereira, “Hospital delivery: women’s experience from the suburbs of Cuibá-MT.” Revista brasileira de enfermagem 59(6) (2006), pp. 740-744; L.T. Mselle, T.W. Kohi, A. Mvungi, et al., “Waiting for attention and care: birthing accounts of women in rural Tanzania who developed obstetric fistula as an outcome of labour,” BioMed Central Pregnancy and Childbirth 11(1) (2011), p. 1.
- I.I. Okafor, O.U. Emmanuel, and N.O. Samuel, “Disrespect and abuse during facility-based childbirth in a low-income country,” International Journal of Gynecology & Obstetrics 128 (2) (2015), pp. 110-113.
- C.E. Dehlendorf and S.M. Wolfe, “Physicians disciplined for sex-related offenses,” Journal of the American Medical Association 279(23) (1998), pp. 1883-1888.
- R.J. Chadwick, D. Cooper, and J. Harries, “Narratives of distress about birth in South African public maternity settings: A qualitative study,” Midwifery 30(7) (2014), pp. 862-868; L. d’Ambruoso, M. Abbey, and J. Hussein, “Please understand when I cry out in pain: women’s accounts of maternity services during labour and delivery in Ghana,” BioMed Central Public Health 5, no. 1 (2005), p. 1; S.A McMahon, S.G Asha, J.C Joy et al., “Experiences of and responses to disrespectful maternity care and abuse during childbirth : A qualitative study with women and men in Morogoro Region, Tanzania,” BioMed Central Pregnancy and Childbirth 14(1) (2014), p. 1.
- Ibid.; See also T. Janevic, P. Sripad, E. Bradley, and V. Dimitrievska, “There’s no kind of respect here: A qualitative study of racism and access to maternal health care among Romani women in the Balkans,” International Journal for Equity in Health 10, no. 1 (2011), p. 1; J.M. Turan, S. Miller, E.A. Bukusi et al., “HIV/AIDS and maternity care in Kenya: How fears of stigma and discrimination affect uptake and provision of labor and delivery services,” AIDS care 20(8) (2008), pp. 938-945.
- The UN Special Rapporteurs on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, on the situation of human rights defenders, on violence against women, its causes and consequences, and the Working Group on discrimination against women in law and in practice. (24 September 2015) Available at: http://www.achpr.org/news/2015/09/d192/
- UN Comm. against Torture, Conclusions and Recommendations, United States of America, 33, U.N. Doc. CAT/C/USA/CO/2 (July 2006).
- Ibid.
- United Nations Committee on the Elimination of Discrimination Against Women, Violence against Women, A/47/38. General Recommendation No. 19, (New York: United Nations, 1992), para. 6.7
- United Nations Committee on the Elimination of Discrimination Against Women, Women and Health, CEDAW/C/1999/I/WG.II/WP.2/Rev.1. General Recommendation No. 24, (New York: United Nations, 1999); Organization of American States, Inter-American Convention on the Prevention, Punishment and Eradication of Violence against Women, 33 ILM 1534 (Washington: OAS, 1994); Council of Europe, Convention on Preventing and Combating Violence against Women and Domestic Violence, CETS No.210 (Strasburg: COE, 2011).
- Ibid.; Committee on Economic, Social and Cultural Rights, General Comment No. 14 (see note 10) para.8.
- United Nations Committee on Economic Social and Cultural Rights, Non-Discrimination in Economic, Social And Cultural Rights (Article 2, para. 2), E/C.12/GC/20(2009). General Comment No. 20, (New York: United Nations, 2009), para. 5.
- UN Human Rights Committee, Communication No. 1153/2003, K.L. v. Peru, U.N. Doc CCPR/C/85/D/1153/2003 (2005).
- Juan E. Mendez, UN Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment U.N Doc. No.A/HRC/31/57 (2016), para. 47. Available at https://documents-dds-ny.un.org/doc/UNDOC/GEN/G16/000/97/PDF/G1600097.pdf?OpenElement.
- United Nations Committee on Economic, Social and Cultural Rights, General Comment No 20 (see note 23); General Comment No 14 (see note 10).
- Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 21); UN Human Rights Committee, Equality of Rights Between Men and Women (Article 3), CCPR/C/21/Rev.1/Add.10 (2000). General Comment No. 28 (New York: United Nations, 2000); Committee on Economic Social, and Cultural Rights, General Comment No. 22, paras. 25-29; Anand Grover, UN Special Rapporteur on the right to the highest attainable standard of health, UN Doc. No. A/66/254 (2011), para.17.
- International Covenant on Economic, Social and Cultural Rights (ICESR), G.A Res. 2200A (XXI) Article 10(2)(1966). Available at http://www.ohchr.org/EN/ProfessionalInterest/Pages/CESCR.aspx; Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 21).
- R. Cook, and S. Cusack, Gender stereotyping: transnational legal perspectives (Philadelphia: University of Pennsylvania Press, 2010).
- African Commission on Human and Peoples’ Rights, General Comment No. 2, Rights of Women in Africa, (Article 14.1 (a), (b), (c) and (f) and Article 14. 2 (a) and (c)) para. 60. Available at http://www.achpr.org/files/instruments/general-comments-rights-women/achpr_instr_general_comment2_rights_of_women_in_africa_eng.pdf.
- T. Janevic et al., (see note 28); J.M. Turan et al., (see note 28); Committee on Economic Social, and Cultural Rights, General Comment No. 22 (see note 27), paras. 30-32.
- United Nations Committee on Economic Social, and Cultural Rights, General Comment No. 22 (see note 27), paras. 30-32; UN Committee Against Torture, Implementation of Article 2 by States Parties, CAT/C/GC/2 (2008). General Comment No. 2, (New York: United Nations), para. 22; African Commission on Human and Peoples’ Rights, General Comment No. 2 (see note 30) para. 1.
- UN Human Rights Committee, K.L. v. Peru, (see note 24) para. 6.5; Committee on the Rights of the Child, General Comment No. 15, Right of the Child to the Highest Attainable Standard of Health, (Article 24), U.N Doc. No. CRC/C/GC/15(2013), paras. 31-34, 56, and 61.
- Committee on the Elimination of Discrimination against Women, Alyne da Silva Pimentel v. Brazil.
- Committee for the Elimination of Discrimination against Women, Concluding observations on the combined fifth and sixth periodic reports of Slovakia, UN Doc. No. CEDAW/C/SVK/CO/5-6 (2015), paras. 30-31; UN Human Rights Council, Compilation prepared by the Office of the High Commissioner for Human Rights: Hungary, UN Doc. No. A/HRC/WG.6/11/HUN/2(2011), para. 55.
- Committee on Economic Social, and Cultural Rights, General Comment No. 22 (see note 27), para. 17.
- Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 21).
- UN Committee on the Elimination of Discrimination against Women, Concluding observations of the Committee on the Elimination of Discrimination against Women: Chile, UN Doc. No. CEDAW/C/CHL/CO/5-6 (2012), para. 34; Committee against Torture, Concluding observations of the Committee against Torture, Czech Republic, UN Doc. No. CAT/C/CZE/CO/4-5 (2012), para. 12.
- UN Committee on the Elimination Of Discrimination Against Women, A.S. v Hungary; UN Human Rights Committee, Concluding observations of the Human Rights Committee: Czech Republic, UN Doc. No. CCPR/C/CZE/CO/2 (2007), para. 10; Committee Against Torture, Concluding observations on the second periodic report of Kenya, UN Doc No. CAT/C/KEN/CO/2 (2013), para. 27; Committee on the Elimination of Racial Discrimination, Concluding observations of the Committee on the Elimination of Racial Discrimination: Mexico, UN Doc. No. CERD/C/MEX/CO/15(2006), para.17; UN Human Rights Committee, Concluding observations of the Human Rights Committee: Slovakia, UN Doc. No. CCPR/CO/78/SVK, para. 12; UN Human Rights Council, Report of the Working Group on the Universal Periodic Review: Namibia, UN Doc. No. A/HRC/17/14(2011), para. 27.
- CEDAW, G.R. Res. 24 (see note 21)
- Ibid. para. 27.
- Juan E. Mendez, United Nations Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, UN Doc. No. A/HRC/22/53 (2013), para. 32.
- Ibid, para. 33.
- Committee on the Elimination of Discrimination against Women, A.S. v Hungary (see note 39); V.C. v. Slovakia, No. 18968/07, European Court of Human Rights, (2012); N.B. v. Slovakia, No. 29518/10, European Court of Human Rights (2012); I.G. and Others v Slovakia, Application no. 15966/04, European Court of Human Rights (2012).
- Ibid.
- Ibid.
- A.S. v Hungary (see note 39); I.G. and Others v Slovakia, (see note 41); Csoma v Romania, No. 8759/0, European Court of Human Rights (2013); V.C. v. Slovakia (see note 44); N.B. v. Slovakia(see note 41); See also case of F.S v Chile pending before the Inter-American Commission on Human Rights, regarding an HIV-positive pregnant women sterilized during childbirth, Centre for Reproductive Rights, Litigation Briefing Series, F.S. v Chile: Forced Sterilization of HIV positive women. Available at http://www.reproductiverights.org/lbs-fs-vs-chile
- see also African Commission on Human and Peoples’ Rights, Resolution on Involuntary Sterilisation (2013). Available at http://www.achpr.org/sessions/54th/resolutions/260.
- Bohren et al. (2015, see note 4).
- UN Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 21), para. 22; UN Committee on Economic Social and Cultural Rights, General Comment No. 14 (see note 10) para. 12.
- UN Committee on Economic Social and Cultural Rights, General Comment No. 14 (see note 10) paras. 12 and 23.
- World Health Organization and United Nations Population Fund, Ensuring human rights within contraceptive service delivery: implementation guide (2015). Available at http://apps.who.int/iris/bitstream/10665/158866/1/9789241549103_eng.pdf.
- Bohren et al. (2013, see note 8).
- Konovalova v Russia, No. 37873/04, European Court of Human Rights (2014).
- Anand Grover, United Nations Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, UN Doc. No, A/64/272 (2009), para. 45.
- Juan E. Mendez, United Nations Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment (2013, see note 25), para. 39.
- Ibid.; African Commission on Human and Peoples’ Rights, General Comment No. 2 (see note 30).
- UN Committee on the Elimination of Discrimination against Women, Concluding observations of the Committee on the Elimination of Discrimination against Women: Czech Republic, UN Doc. No. CEDAW/C/CZE/CO/5 (2010), para. 36.
- UN Human Rights Council, Concluding observations on the fourth periodic report of Ireland, UN Doc. No. CCPR/C/IRL/CO/4(2014). Available at http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CCPR/C/IRL/CO/4&Lang=En.
- Bohren et al. (2015, see note 4).
- European Convention for the Protection of Human Rights and Fundamental Freedoms, European Treaty Series 5 (1950), Article 8. Available at http://www.echr.coe.int/Documents/Convention_ENG.pdf.
- R.R v. Poland, No. 27617/04, European Court of Human Rights, (2011), para. 197.
- Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 21), para. 24; See also Committee on Economic Social and Cultural Rights, General Comment No. 14 (see note 10) para. 12.
- Committee on The Elimination Of Discrimination Against Women, A.S. v Hungary (see note 47).
- Juan E. Mendez, United Nations Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment (2013, see note 25), para. 89(e).
- Committee on the Elimination of Discrimination Against Women, General Recommendation No. 24 (see note 18), para. 24.
- R.J Chadwick (see note 15); L D’Ambruoso (see note 15); S.A McMahon (See note 15); A. El-Nemer, S. Downe, and N. Small, “She would help me from the heart: an ethnography of Egyptian women in labour,” Social Science and Medicine 62, no. 1 (2006), pp. 81-92.
- Ibid.
- Konovalova v. Russia (see note 54).
- R.R v. Poland (see note 62).
- Ibid.
- Ibid.
- UN Committee on the Elimination of Discrimination against Women, Concluding observations of the Committee on the Elimination of Discrimination against Women: Czech Republic (see note 39), para. 36; Hanzelkovi v Czech Republic, No. 43643/10, European Court of Human Rights, 2015.
- Bohren et al. (2015, see note 4).
- UN Committee on Economic Social and Cultural Rights, General Comment No. 14 (see note 10) paras. 12 and 46-52.
- Protocol To The African Charter On Human And Peoples’ Rights On The Rights Of Women In Africa (Maputo Protocol), Article 14 (2)(b) (2003). Available at http://www.achpr.org/files/instruments/women-protocol/achpr_instr_proto_women_eng.pdf; African Commission on Human and Peoples’ Rights, General Comment No. 2 (see note 30), para. 58.
- Committee on the Elimination of Discrimination against Women, Alyne da Silva Pimentel (see note 34).
- Ibid.
- Ibid.
- Committee on Economic Social and Cultural Rights, General Comment No. 14 (see note 10).
- Maputo Protocol (see note 76); African Commission on Human and Peoples’ Rights, General Comment No. 2 (see note 27), para.60.
- Committee on Economic Social, and Cultural Rights, General Comment No. 22 (see note 27), para. 64.
- United Nations, Human Rights Council, Annual Report of the UN High Commissioner for Human Rights and Reports of the Office of the High Commissioner and the Secretary General, Technical Guidance on the Application of a Human Rights-Based Approach to the Implementation of Policies and Programmes to Reduce Preventable Maternal Morbidity and Mortality A/HRC/21/22 (2012), para 75.
- Center for Reproductive Rights and Federation of Women Lawyers–Kenya, Failure to deliver: Violations of women’s rights in Kenyan health facilities (New York: Center for Reproductive Rights, 2007); Human Rights Watch, Stop Making Excuses: Accountability for Maternal Health Care in South Africa (New York: Human Rights Watch, 2011).
- H. Potts and P.H. Hunt, Participation and the right to the highest attainable standard of health (Colchester, UK: Human Rights Centre, 2008.)
- ibid