Extending the Right to Health to the Moment of Death: End of Life Care and the Right to Palliation in Rwanda
Authors
Agnes Binagwaho, Sardis H. Harward, Theophile Dushime, Jean de Dieu Ngirabega, Parfait Uwaliraye, Cathy Mugeni, Kirstin W. Scott, Marie Aimee Muhimpundu, Jean Pierre Nyemazi
Introduction
The right to the highest attainable state of health is a key cornerstone in international and regional human rights legal frameworks.1 In the terminal stages of life-limiting illness, however, the highest attainable state of health may involve measures focused on preserving dignity and mitigating pain. Efforts made toward curative treatment may be more harmful than helpful at this difficult stage of life.2 Palliative care, although insufficient to return a patient to ideal health status, aims to relieve the suffering associated with chronic, non-communicable or terminal disease, thereby achieving an optimal quality of life for patients and their families in spite of the challenging circumstances before them.
Concern has been raised about the quality and availability of palliative care globally, and these concerns are particularly acute in resource-limited settings.3 Despite absorbing over 60% of global cancer deaths and approximately 95% of deaths associated with HIV/AIDS worldwide, the developing world consumes only 6% of the global market of opioids for medical use.4 Deficits in palliative care service delivery are further exacerbated in countries that have experienced rapid gains in life expectancy while also witnessing a corresponding epidemiologic transition from communicable to non-communicable diseases. As chronic diseases overcome acute illness and injury as the leading cause of death, protracted and painful illness courses constitute a greater share of the human experience worldwide. This will not only increase demand for palliative services but also the obligation on States to provide such services. Rwanda is currently experiencing such an epidemiologic transition and the attendant demand for palliative services: since 2000, the country’s average life expectancy has increased by a third and under-5 mortality has decreased by 70%; at the same time, deaths due to non-communicable diseases have increased dramatically.5 In the past 25 years, deaths in Rwanda due to cancer alone have increased by 25%.6
This essay discusses the right to palliative care as a corollary of the right to health, using Rwanda as a case study of a resource-limited setting in the process of palliative care scale up. Rwanda was chosen for critical examination due to the depth of the authors’ personal and professional experience in Rwanda and the nation’s commitment to expanding access to palliative care, formalized in the 2011 Rwanda National Palliative Care Policy (NPCP).7 The essay relates the 2011 policy to the current international palliative care and human rights discourses, and discusses the role of expanding access to palliative care in realizing human rights in Rwanda and other resource-limited settings.
Methods
The authors undertook an in-depth analysis of the international human rights legal framework as it relates to palliative care and closely reviewed Rwandan policies impacting palliative care service delivery. Together with contributions from the authors’ extensive experience working in the Rwandan health sector, these policy reviews were synthesized to elucidate factors impacting the need for palliative care, the international rights-based imperative to make palliative care available, and the implications each of these has for palliative care policy and program development in Rwanda and elsewhere.
The Palliative Care Landscape in Rwanda
In 2010, approximately 3,670 Rwandans were reported to have died of cancer and 8,670 reported deaths were attributed to HIV/AIDS and tuberculosis; these numbers corresponded to approximately 5% and 11.5% of all cause mortality that year in Rwanda, respectively.8 According to estimation methods described elsewhere, these national cancer and HIV/AIDS disease burdens translate to 7,271 Rwandans in need of palliation every year due to cancer and HIV/AIDS alone.9 While Rwanda’s opioid consumption during the corresponding time frame was not reported to the International Narcotic Control Board, only 0.6% of estimated need was procured during 2006 to 2008.10 A survey conducted by the Rwanda Ministry of Health (MoH) in 2009 revealed that even in areas where palliative medications were available, patients were often unable to access adequate care due to poorly integrated service delivery.11 Recognizing the unmet need for readily accessible palliative care services and bidirectional patient referral systems, the MoH adopted the NPCP in 2011.12
The objectives of the NPCP—to provide accessible and integrated services, ensure the availability of essential palliative care medications, strengthen palliative care education, and develop an appropriate monitoring and evaluation framework—reveal the ambitious scope of the interventions to be implemented in accordance with the policy.13 By formally codifying patients’ rights to palliative services and outlining policies that aim to uphold the dignity of those nearing the end of life, Rwanda has made a commitment to provide optimal care despite limited financial and human resources. It is also stating its clear intention to realize the human right to health, even when preventive and curative services can no longer assist a person.
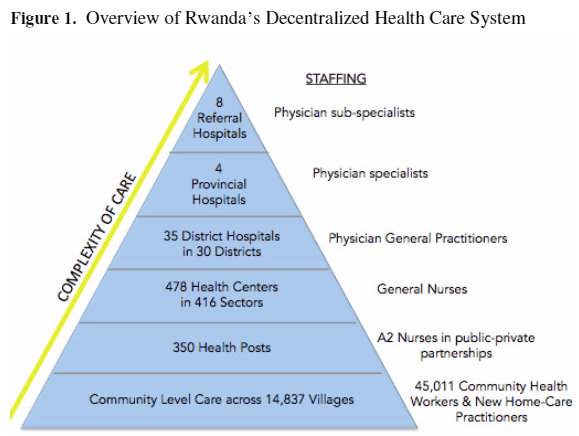
Specific activities to be undertaken in support of palliative care provision are also included in Rwanda’s Third Health Sector Strategic Plan (HSSP III) and Health Sector Policy 2015.14 Palliative services are currently offered at referral, provincial and district hospitals—the top three levels of Rwanda’s decentralized health care delivery system (Figure 1). Some development partners, including Partners in Health, the Roros Foundation, and the Tropical Health and Education Trust, are supporting the MoH in its efforts to provide locally available palliative services to limited catchment areas. The palliative care scale up described in HSSP III plans to make care universally available at the community level. This will be achieved through a home-based practitioner program integrated with pre-existing infrastructure for care delivery at the village level.15
Additional activities, including the development of palliative care training curricula at all levels of the health care system, creation of monitoring and evaluation systems, and community outreach and education are currently in progress.16 Together, the NPCP, HSSP III, and the programs they have given rise to, aim to promote the highest attainable state of health for those nearing the end of life, allowing people to die with dignity in the vicinity of loved ones, either at home or in a community setting that provides spiritual and emotional comfort as well as alleviation of physical symptoms.
Given the dramatic increase in life expectancy coupled with the changing drivers of morbidity and mortality, Rwanda’s attention and commitment to palliative care provision comes at a fortuitous time. Expanding acute and curative care services is expensive, but palliation provided at the community level offers a financial reprieve. Cost effectiveness evaluations conducted in developed countries, where, relatively, health and financial resources abound, indicate that home-based palliative services reduce utilization of high level health services such as intensive care unit admission, and emergency room and specialist visits.17 While similar conclusions have yet to be drawn in resource-limited settings—primarily due to the dearth of palliative services in these areas—the decentralized delivery of palliation could reasonably be expected to be associated with reduced care seeking at the hospital level. Moreover, investment in palliative care has the potential to provide access to a universal human right frequently cited in the international human rights legal framework, but only rarely realized.
Access to Palliative Care is a Fundamental Human Right
Complementary to the broadly applicable statements regarding the right to the highest attainable standard of health made in various human rights legal instruments, a universal right to palliative care is expressed explicitly in several recent additions to the international human rights documents. Although neither the 2002 Palliative Care Trainers Declaration of Cape Town nor the Declaration on Hospice and Palliative Care of 2005 is legally binding, each represents the perspective of deeply involved stakeholders. The Cape Town Declaration unambiguously states that “Palliative care is a right of every adult and child with a life-limiting disease,” and further, that palliative care service provision should be a component of all national health care strategies—both of these sentiments are echoed in the 2005 Declaration.18 One year after the adoption of the Cape Town Declaration, the European Committee of Ministers issued a recommendation recognizing palliative care as “an inalienable element of a citizen’s right to health care,” and urging governments of Member States to adopt policy frameworks enabling and supporting palliative care provision.19
Discussions of palliative care as a human right also extend beyond the right to health. Due to the severity of pain associated with the majority of terminal illnesses, certain policymakers, researchers and advocates have argued that withholding palliation qualifies as cruel, inhuman and degrading treatment, and is tantamount to torture.20 Multiple UN covenants and regional human rights agreements describe cruel, inhuman and/or degrading treatment as a human rights violation, and oblige State governments to protect their citizens accordingly.21 If, as many authors argue, withholding palliation is understood to be cruel, inhuman and/or degrading, then governments are required to protect their citizens from unnecessary pain associated with disease or injury at all stages of life.22 Arguments made for palliation as a human right are further fortified by the terms of several international narcotic control conventions that recognize the medical use of narcotic drugs as indispensable, and state that provisions must be made to ensure their availability.23
The human right to palliation thus resides at the interstices of distinct human rights elements, which are too often interpreted in isolation. Health systems and policies that deny or constrain access to palliative care when adequate service delivery is possible, thereby violate patients’ right to health, allow cruel, inhuman and degrading treatment to occur, and disregard international narcotic control laws. As an effort to expand access to, and quality of, palliative care services, Rwanda’s NPCP reflects both the terms and the sentiment of the international human rights framework surrounding palliative care provision. Scale up of decentralized palliative services in Rwanda will help to uphold this right to palliation by improving the health status of patients nearing the end of life, guaranteeing access to necessary medications, and allowing patients to die in the settings, and near the people, they choose.
Conclusion
Every person is entitled to palliation of unnecessary pain by virtue of his or her right to the highest attainable standard of health. Rwanda’s approach to palliative care delivery is occurring at a time when health care resources in developing and developed nations alike are predominantly allocated to curative and maintenance care rather than palliative measures. However, Rwanda’s holistic decentralized health care system has complemented the growth of acute care capacity with proportional gains in preventive—and soon, palliative—care administered at the community level. Incorporating palliative services by expanding pre-existing community health care delivery structures will increase access to palliation and reduce unnecessary transfer of people to referral centers. These measures will further realize Rwandans’ rights to health, decrease the direct and opportunity costs associated with high-level care at specialty centers, protect Rwandan citizens from inhumane treatment at the end of life, and align the Rwandan palliative care policy framework with international human rights standards.
Agnes Binagwaho, MD, MPed, PhD, is Minister of Health of the Republic of Rwanda (Kigali, Rwanda), Senior Lecturer in the Department of Global Health and Social Medicine at Harvard Medical School (Boston, MA, USA), and Adjunct Clinical Professor of Pediatrics at Geisel School of Medicine at Dartmouth (Hanover, NH, USA). *
Sardis H. Harward, MPH is a research fellow at The Dartmouth Institute for Health Policy and Clinical Practice (Lebanon, NH, USA).
Theophile Dushime, MD is Director General of Clinical Services of the Ministry of Health of the Republic of Rwanda (Kigali, Rwanda).
Jean de Dieu Ngirabega, MD, PhD, MSc, MPH is Head of Department of the Institute of HIV/AIDS Disease Prevention and Control of Rwanda Biomedical Center (Kigali, Rwanda).
Parfait Uwaliraye, MPH is Director General of Planning, Health Financing and Information Systems of the Ministry of Health of the Republic of Rwanda (Kigali, Rwanda).
Cathy Mugeni, MPH is Community Health Division Manager at Rwanda Biomedical Center (Kigali, Rwanda).
Kirstin W. Scott, MPhil, PhD is a student at Harvard Medical School (Boston, MA, USA).
Marie Aimee Muhimpundu, MD, MSc is the Non-Communicable Diseases Division Manager at Rwanda Biomedical Center (Kigali, Rwanda).
Jean Pierre Nyemazi, MD, MS, MHCDS is the Planning, Monitoring, Evaluation and Business Strategy Division Manager at Rwanda Biomedical Center (Kigali, Rwanda).
Corresponding author – please send all communications to agnes_binagwaho@hms.harvard.edu
References
- Universal Declaration of Human Rights (UDHR), G.A. Res. 217A (III) (1948). Available at http://www.un.org/Overview/rights.html; International Covenant on Economic, Social and Cultural Rights (ICESCR), G.A. Res. 2200A (XXI) (1966). Available at http://www.ohchr.org/EN/ProfessionalInterest/Pages/CESCR.aspx; Convention on the Rights of the Child (CRC), G.A. Res. 44/25 (1989). Available at http://www.ohchr.org/en/professionalinterest/pages/crc.aspx; African Charter on Human and Peoples Rights, OAU Doc. No. CAB/LEG/67/3 rev. 5 (1981), reprinted in International Legal Materials 21 (1982), p. 58. Available at http://www.achpr.org/files/instruments/achpr/banjul_charter.pdf; World Health Organization, Conference on Primary Health Care: Declaration of Alma-Ata, Alma-Ata, September 6-12, 1978. Available at http://www.who.int/publications/almaata_declaration_en.pdf.
- M.A. Ashby, “The futility of futility: death causation is the ‘elephant in the room’ in discussions about limitation of medical treatment,” Bioethical Inquiry 8 (2011), pp. 151-154; R.W. Griffiths, Y.K. Zee, S. Evans et al, “Outcomes after multiple lines of chemotherapy for platinum-resistant epithelial cancers of the ovary, peritoneum, and fallopian tube,” International Journal of Gynecological Cancer 21/1 (2011), pp. 58-65; T.H. Lippert, H.J. Ruoff, M. Volm, “Could a revision of the current guidelines for cancer drug use improve the quality of cancer treatment?” Journal of Therapeutics and Clinical Risk Management 10 (2014), pp. 69-72.
- R. Harding, L. Selman, R.A. Powell, “Research into palliative care in sub-Saharan Africa,” Lancet Oncology 14 (2013), pp. e183-188; M. O’Brien, F. Mwangi-Powell, I.F. Adewole et al, “Improving access to analgesic drugs for patients with cancer in sub-Saharan Africa,” Lancet Oncology 14 (2013), pp. e176-182; D. Spence, A. Merriman, A. Binagwaho, “Palliative care in Africa and the Caribbean,” PLoS Medicine 1/1 (2004), pp. e5; R. Webster, J. Lacey, S. Quine, “Palliative care: a public health priority in developing countries,” Journal of Public Health Policy 28 (2007), pp. 28-39.
- D. Manjiani, D.B. Paul, S. Kunnumpurath et al, “Availability and utilization of opioids for pain management: global issues,” The Oschner Journal 14 (2014); pp. 208-215; Economic and Social Council Res. 2005/25, Treatment of pain using opioid analgesics. Available at http://www.un.org/en/ecosoc/docs/2005/resolution%202005-25.pdf.
- World DataBank. Health Nutrition and Population Statistics. Accessed September 25, 2014; World DataBank. World Development Indicators. Accessed September 25, 2014.
- Institute for Health Metrics and Evaluation, Global Burden of Disease Cause Patterns. Available at http://vizhub.healthdata.org/gbd-cause-patterns. Accessed November 15, 2014.
- Republic of Rwanda Ministry of Health, National Palliative Care Policy. Available at http://pdf.usaid.gov/pdf_docs/pnaed053.pdf.
- Institute for Health Metrics and Evaluation, Global Burden of Disease Cause Patterns. Available at http://vizhub.healthdata.org/gbd-cause-patterns. Accessed November 15, 2014.
- M. O’Brien, F. Mwangi-Powell, I.F. Adewole et al, “Improving access to analgesic drugs for patients with cancer in sub-Saharan Africa,” Lancet Oncology 14 (2013), pp. e176-182.
- Human Rights Watch, “Please, do not make us suffer any more…” Access to pain treatment as a human right (March 2009). Available at http://www.hrw.org/sites/default/files/reports/health0309webwcover_1.pdf.
- Republic of Rwanda Ministry of Health, National Palliative Care Policy. Available at http://pdf.usaid.gov/pdf_docs/pnaed053.pdf.
- Ibid.
- Ibid.
- Republic of Rwanda Ministry of Health, Third Health Sector Strategic Plan. Available at http://www.moh.gov.rw/fileadmin/templates/Docs/HSSP_III_FINAL_VERSION.pdf; Republic of Rwanda Ministry of Health, Health Sector Policy, 2015. Available at http://www.moh.gov.rw/fileadmin/templates/policies/Health_Sector_Policy___19th_January_2015.pdf.
- Republic of Rwanda Ministry of Health, National Palliative Care Policy. Available at http://pdf.usaid.gov/pdf_docs/pnaed053.pdf; Republic of Rwanda Ministry of Health, Third Health Sector Strategic Plan. Available at http://www.moh.gov.rw/fileadmin/templates/Docs/HSSP_III_FINAL_VERSION.pdf.
- Ibid.
- D.E. Meier, “Increased access to palliative care and hospice services: opportunities to improve value in health care,” The Milbank Quarterly 89/3 (2011), pp. 343-380; R.S Morrison, J. Dietrich, S. Ladwig et al, “Palliative care consultation teams cut hospital costs for Medicaid beneficiaries,” Health Affairs 30/3 (2011), pp. 454-463; D. Gans, G.F Kominski, D.H. Roby et al, “Better outcomes, lower costs: palliative care program reduces stress, costs of care for children with life-threatening conditions,” UCLA Center for Health Policy Research, 29 Aug, 2012. Available at https://escholarship.org/uc/item/7244h6wq.
- The Palliative Care Trainers Declaration of Cape Town (November 2002), reprinted in Journal of Palliative Medicine 6/3 (2003), p. 339. Available at http://online.liebertpub.com/doi/abs/10.1089/109662103322144637; Global Summit of National Hospice and Palliative Care Associations, Declaration on Hospice and Palliative Care, Seoul, March 2005. Available at http://www.coe.int/t/dg3/health/Source/KoreaDeclaration2005_en.pdf
- Council of Europe Committee of Ministers Rec. 2003/24 of the Committee of Ministers to member states on the organisation of palliative care. Available at http://www.eapcnet.eu/LinkClick.aspx?fileticket=3KJ5U3BQLVY%3d&tabid=1709.
- Human Rights Watch, “Please, do not make us suffer any more…” Access to pain treatment as a human right (March 2009). Available at http://www.hrw.org/sites/default/files/reports/health0309webwcover_1.pdf; F. Brennan, D.B. Carr, M. Cousins, “Pain management: a fundamental human right,” Pain Medicine 105/1 (2007), pp. 205-221; L. Gwyther, F. Brennan, D. Obs et al, “Advancing palliative care as a human right,” Journal of Pain and Symptom Management 38/5 (2009), pp. 767-774; D. Lohman, R. Schleifer, JJ. Amon, “Access to pain treatment as a human right,” BMC Medicine 8 (2010), p. 8.
- African Charter on Human and Peoples Rights, OAU Doc. No. CAB/LEG/67/3 rev. 5 (1981), reprinted in International Legal Materials 21 (1982), p. 58. Available at http://www.achpr.org/files/instruments/achpr/banjul_charter.pdf; International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966). Available at http://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx; Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, G.A. Res. 39/45 (1984). Available at http://www.ohchr.org/EN/ProfessionalInterest/Pages/CAT.aspx.
- African Charter on Human and Peoples Rights, OAU Doc. No. CAB/LEG/67/3 rev. 5 (1981), reprinted in International Legal Materials 21 (1982), p. 58. Available at http://www.achpr.org/files/instruments/achpr/banjul_charter.pdf; Human Rights Watch, “Please, do not make us suffer any more…” Access to pain treatment as a human right (March 2009). Available at http://www.hrw.org/sites/default/files/reports/health0309webwcover_1.pdf; International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966). Available at http://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx; Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, G.A. Res. 39/45 (1984). Available at http://www.ohchr.org/EN/ProfessionalInterest/Pages/CAT.aspx.
- United Nations Conference for the Adoption of a Single Convention on Narcotic Drugs, Geneva, January 24-March 25, 1961. Available at http://www.unodc.org/pdf/convention_1961_en.pdf; Commission on Narcotic Drugs Res. 53/4, Promoting adequate availability of internationally controlled licit drugs for medical and scientific purposes while preventing their diversion and abuse. Available at http://www.unodc.org/documents/commissions/CND/Drug_Resolutions/2010-2019/2010/CND_Res-53-4.pdf; Commission on Narcotic Drugs Res. 54/6, Promoting adequate availability of internationally controlled narcotic drugs and psychotropic substances for medical and scientific purposes while preventing their diversion and abuse. Available at http://www.unodc.org/documents/commissions/CND/Drug_Resolutions/2010-2019/2011/CND_Res-54-6.pdf; United Nations Conference for the Adoption of a Protocol on Psychotropic Substances, Vienna, January 11-February 21, 1971. Available at http://www.unodc.org/pdf/convention_1971_en.pdf.