Medea Gegia, Iagor Kalandadze, Mikheil Madzgharashvili, and Jennifer Furin
Health and Human Rights 13/2
Published December 2011
Abstract
Tuberculosis (TB) is one of the leading infectious killers of adults globally. Incarcerated individuals represent a vulnerable population when it comes to TB exposure, development of disease, and poor treatment outcomes. The TB pandemic in prisons is a serious human rights issue, and multiple global organizations have called for human rights-based strategies to address it. There are, however, few countries implementing such programs on the ground. Georgia, a former Soviet republic located in the Caucasus Mountains, has high rates of TB and a large prison population. This paper describes a needs assessment carried out in one prison in Georgia and the human rights-based strategy being implemented by the Georgian National TB Program to address TB control in the prison setting. It is hoped that the proposed program can serve as a model for other countries with high rates of TB among incarcerated individuals.
Background
Tuberculosis (TB) is a public health problem with major human rights implications.1 An estimated 2 billion people are infected with the highly infectious disease. In 2010, 9 million people became sick with the disease—this is the highest number of cases ever reported. Despite the fact that there is effective treatment, almost 2 million people die from TB each year, largely due to lack of access to care.2
Tuberculosis disproportionately affects vulnerable populations around the globe, and the group with the highest risk for TB is the prison population.3 An estimated nine million people in the world are incarcerated and it is estimated that prisoners account for 8.5% of all TB infections.4,5 Prisoners are not only more likely to become infected with the TB bacteria, but they are also less likely to be diagnosed with the disease, receive treatment once diagnosed, and have successful treatment outcomes even if they begin therapy. Several factors may account for high rates of TB in prisons, chief among them, crowding, malnutrition, and the movement of prisoners from site to site.6,7,8,9 However, the lack of access to even basic health care in prisons remains the major problem.10
In the late 1990s, there were a number of articles written about TB in prisons and human rights, with much attention given to the prisons of the former Soviet Union.11,12,13 In 1997, the World Health Organization, the International Committee of the Red Cross, and the governments of Russia, Georgia, and Azerbaijan issued what has become known as the Baku Declaration, which officially recognized TB as the prison system’s major health problem and called for improved care of prisoners with the disease.14 In 2001, the World Health Organization published “A Human Rights Approach to Tuberculosis” and more recently, the Stop TB Partnership issued a document on tuberculosis and human rights.15 These comprehensive documents address human rights issues in TB control for a range of populations, including prisoners. The broad approach focuses on: 1) equal partnerships with affected communities; 2) identifying and empowering the most vulnerable populations to access services; 3) assuring dignity; 4) addressing social and economic determinants of diseases; 5) addressing human rights implications of policy and programs; 6) addressing institutional constraints and capacity gaps; 7) providing a multisectoral response; 8) providing accountability tools; 9) developing a platform for sharing best practices, advocacy efforts, and social mobilization.16
Many countries have focused on an “infection control”-based approach to TB control in prisons. While this approach can limit the spread of TB, it can compromise the rights of individuals infected and sick with TB in prisons. Under international law, countries have an obligation to provide adequate health care to individuals in prisons, and the International Covenant on Civil and Political Rights states that danger to a prisoner’s health and life as a result of an infectious disease constitutes a violation of international human rights law.17 Human rights law also states that countries have an obligation to ensure that TB services in prisons are at least equivalent to those provided to the general population.18 Given that people are at increased risk of contracting TB and of having a poor outcome if they become sick with the disease in prison, the government of Georgia has elected instead to promote a standard of TB care in their prisons that is better than the level of health care in the community. This article will discuss an ethnographic assessment carried out in the prison system in Georgia and describe the human rights-based approach proposed by the National TB Program to address weaknesses in the system.
Setting
Georgia is a country in the South Caucasus that regained its independence from the Soviet Union in 1991. Since that time, the country has undergone multiple political, social, and health reforms, and the current government has made great strides in addressing some of the most pressing health and social concerns. However, the country is still facing significant health problems, and none of these is more significant than the problem of TB.
Georgia currently has the fifth-highest rate of TB in the European region, with an estimated 100 incident cases per 100,000 persons in 2010.19 Rates of drug-resistant TB are also extremely high, estimated to be 10% among newly diagnosed patients and 30% among those who have been previously treated for the disease.20 The prison population is disproportionately affected by TB, accounting for over one-third of the cases reported annually.21 Furthermore, individuals diagnosed with TB while incarcerated are far less likely to be cured than are patients in the civilian sector; only 40% of patients diagnosed in prison actually complete their treatment if they are released from prison while still on therapy.22
Georgia has long suffered from high rates of TB within its prison system. A study done in the Georgian prison system in 1997 and 1998 found that prevalence of smear- or culture-positive tuberculosis was 5995 per 100,000 prisoners (n=448 cases among 7473 inmates). Of additional concern were the high rates of drug resistance found among the prisoners. Of all the strains on which drug susceptibility testing (DST) was done, 215 (77.9%) were resistant to at least one drug and 37 (13.0%) were multidrug resistant.23
As part of a response to these extraordinarily high rates of tuberculosis and multidrug resistant tuberculosis (MDRTB) in the Georgian prisons, the ICRC launched a major effort to improve diagnosis and treatment. The initiative included improved access to diagnostic and therapeutic services, administrative infection control measures, infrastructure and lab improvement, training for prisoners and providers, and the provision of incentives to health care staff working in prisons.24 In 2010, the ICRC handed the prison program over to the Georgian Ministry of Health, describing the situation as “a success story.”25
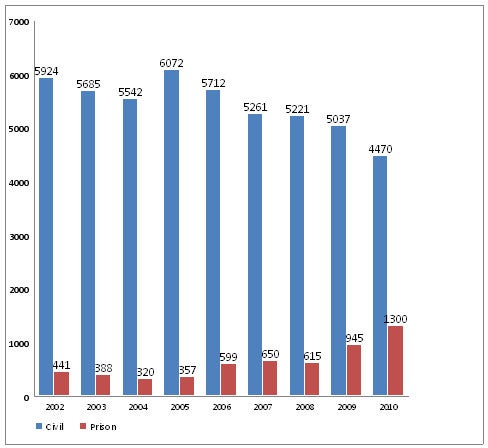
This declaration of success may have been premature. Country-level data show a steady rise in both the incidence and prevalence of TB in the prison population, and a rise in the percentage of cases the prison population is contributing to the overall TB pandemic in Georgia. These numbers are illustrated in Figures 1 and 2.
Figure 1: Notification of TB cases in the prison, Georgia, 1998-2010 (per 100 prisoners)
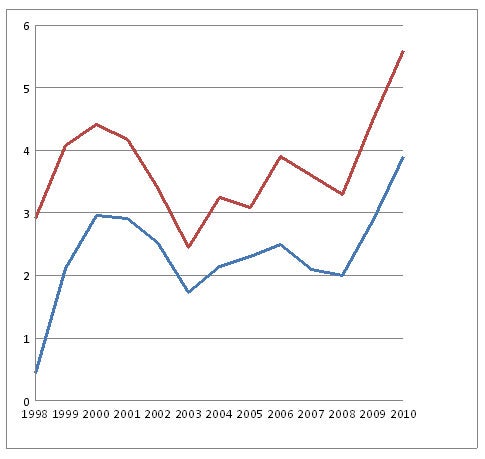
Figure 2: All TB cases in civil and prison sectors, Georgia, 2002-2010 (absolute numbers)
The dramatic increase in the number of prisoners over the last seven years is a significant problem. Fewer than 4,000 prisoners were documented in 2004; in 2010, that number had increased to more than 25,000. This increase is largely attributable to the influx of political prisoners who were jailed after the 2003 Rose Revolution and the 2008 war with Russia.26,27 Staffing issues in the prisons—particularly with regard to health services—have not kept pace with the increase in the incarcerated population. Currently, Georgia has 19 prisons and overcrowding is the norm with most prisons functioning at 125% capacity. Overall, Georgia has an estimated 415 prisoners per 100,000 people.28 There is one prison facility in Ksani specifically focused on treating prisoners with TB. This facility is overwhelmed: The number of prisoners is almost eight times what it was five years ago. TB screening is done upon entry into the prison system, but health and lab facilities limit these ongoing screening efforts.29 Thus, the disease continues to spread unabated, and although incidence is declining among the civilian population, it is rising among the prison population. The government of Georgia has declared the situation a health and human rights emergency requiring urgent attention and resources.30
Methods
The researchers used a combination of qualitative methods to describe the problem of TB control in the Georgian prisons and to present the human rights-based strategy developed to address these problems. Qualitative methods have a long history of use in TB research, and are useful in providing valid data on health care problems.31 The methods used in this study included participant observation, ethnographic interviewing, and key informant interviewing. Participant observation was done in one prison facility in Ksani, in the National TB Program, at two health centers, and in the National TB Reference Hospital. Key informant interviews were done with a convenience sample of national TB program officers (13 participants), health officials at the prisons (four participants), physicians (two participants) and nurses (three participants) at the prisons, and with prisoners (four participants). Observations and interviews focused on the current situation of TB control and services in the prisons, actions needed to improve TB control and services in the prisons, and human rights issues in prison TB control. The ethnographic assessments were carried out over a five-month period between July 2010 and January 2011 by a trained anthropologist (JF). Data were recorded using detailed field notes and analyzed for theme, pattern, and content, according to standard ethnographic methods.32
Results
The results of the ethnographic study and analysis are presented in the following section. First, a review of the current situation in the prisons is presented. Second, a description of proposed reforms is discussed. Finally, a discussion of the limitations of the proposed program is presented.
Current TB control conditions in the Georgian prison system
The study revealed a number of concerns with the current TB control situation in Georgia, including:
1) Lack of coordinated screening efforts
Although all incarcerated individuals are screened for TB on admission to the prison system, there is no ongoing active systematic screening. This is largely due to a lack of medical and laboratory staff to perform screening on a regular basis. In terms of passive screening, prisoners who have signs and symptoms of TB must wait weeks to see a medical provider who may or may not screen them for TB. Furthermore, many prisoners are not aware of the signs and symptoms that should prompt them to request a screening.
2) Delays in initiation of appropriate therapy
Once a prisoner has presented to a health care provider for TB screening, he or she must often wait weeks to months before appropriate treatment is initiated. Laboratory results are not routinely available to health providers in the prisons, and even when there is a positive smear or culture, it can take weeks for these results to reach the proper providers. In some regions of the country (western Georgia, for example), it can take two to four weeks for patients diagnosed with TB to be transferred to the treatment colony at Ksani. These delays lead to increased periods of exposure for other incarcerated individuals.
3) Lack of human resources for managing TB in the prisons
Although there are enough physicians and nurses in the country of Georgia to manage the problem of TB, the prison system is suffering from a lack of human resources. The prison rules have capped the number of physicians and nurses that can be hired. Recruitment of staff to work in the prisons is problematic, and health care personnel are demoralized. Turnover of most key personnel is reported every three to six months. In addition to their overwhelming clinical loads, the physicians and nurses are burdened by paperwork. For security reasons, they do not have Internet access and are isolated in the work they are doing. For example, none of them were able to attend World TB Day activities in 2011. If screening is to increase and more patients are diagnosed, action must be taken to strengthen the prison health system to accommodate the increasing work load.
In addition to managing TB, some prisoners also have co-morbid conditions that decrease the likelihood of their TB being cured. Chief among these is diabetes mellitus, which has been shown not only to increase the likelihood of developing active TB but also to reduce the chances of TB cure. There are no medicines in the prisons for managing co-morbid conditions such as diabetes.
4) Lack of laboratory resources
The prison has an excellent laboratory system, but it is unable to handle the increased work load of mass screening, even at a single prison facility. Physicians reported being unable to screen prison suspects because they were limited in their ability to send sputum samples. If screening efforts are to improve, then laboratory facilities must also be strengthened.
5) Poor infrastructure
Certain prisons have upgraded facilities and improved not only living conditions but also reduced the risk of becoming infected with TB. However, many prison facilities in Georgia have sub-standard living conditions that facilitate the spread of TB. For example, one prison which reports a large proportion of TB cases has a facility in which 100 to 150 incarcerated individuals are kept in one large room with no ventilation and no windows. In order to decrease the spread of TB, major infrastructure improvements are needed.
6) Poor follow-up of patients with TB who are released from the prisons
For those prisoners who do become sick with TB while in the prison system, successful treatment outcomes are less likely, especially among those released from prison while on treatment. It is estimated that fewer than 40% of incarcerated individuals who are released from prison while on treatment actually report to health centers to complete therapy. This means they are more likely to develop drug-resistant forms of TB and to spread TB in the larger community. There is no system for following up with prisoners who have been released, nor for tracing their household and community contacts.
Proposed reforms
There are several potential strategies for addressing these problems. The Georgian National TB Program NTP has chosen to address them using a human rights-based approach. This was done to promote prisoners’ rights, access to health information, development of useful skills among the prison population, and facilitation of return into the general community.
1) Incarcerated health workers
The backbone of the rights-based program in Georgia will be the development of a group of lay health workers from among the prisoners known as “Incarcerated Health Workers” or “IHWs.” The IHW group will be developed using community health worker (CHW) models of care as a guide. CHW programs have been used in a wide variety of settings to treat myriad health problems.33 While there are many instances of community-based organizations working on the problem of TB in prisons, there are to date no documented programs where prisoners themselves are trained as health workers. There is a history in the Georgian prisons of using highly motivated incarcerated individuals to perform certain administrative and security-related jobs in the prisons, and a similar method will be used for selecting and employing the IHWs.34
The IHWs will focus on TB education, facilitation of sputum collection and diagnostic referral, advocacy efforts, and working with the National TB program to improve TB care. Selected IHWs will be trained in these activities using standard TB training materials for health care providers. As part of their training, they will receive certification as TB educators and care providers, and this certification will be valid when they are released. IHWs could lead to many improvements in diagnosis and care of TB. First, the workers will be educating their peers and doing so on an ongoing basis. Second, they will provide routine, ongoing screening for all persons within their respective prisons. Third, they will be able to request sputum testing for TB, so that suspected patients do not have to wait to see physicians. Fourth, they will be able to ensure that patients in need of medical attention do not have to rely solely on prison staff or medical staff to address their medical needs. It has been hypothesized that when prisoners have an increased sense of control over their health, they are able to enact healthy behaviors.35 The proposed program is expected to give prisoners control over their own health, increase their access to health knowledge, and allow them to undergo sputum testing without having to see a physician or nurse.
A second important role of the IHWs could be in the arena of advocacy. Prisoners often have few advocates and are rarely in a position to advocate for themselves and their fellow inmates. By training the IHWs and integrating them into the prison health network, these individuals should be able to speak directly with health care providers about their needs and the needs of other prisoners. This information could then be conveyed directly to those in positions of power who can make changes. This open line of communication is expected to decrease frustrations among both the prisoners and those caring for them, an additional benefit to this program.
A third important role for the IHWs will be in their transition and the transition of other prisoners back into general society upon release from prison. IHWs will have certification of their skills and can be employed by the Ministry of Health, Ministry of Corrections and Legal Assistance, and nongovernmental organizations to continue providing TB care and advocacy in a new capacity. Released IHWs can also help manage unacceptably high default rates among persons released from prison while still being treated for TB. The current system requires the physicians or nurses to make a referral to the TB clinic in the community to which the prisoner is being released. The onus is then on the recently released individual to report to the clinic. By employing the IHWs to follow up directly with all prisoners released while on TB treatment, default will likely be reduced. It has been shown in other prison settings that when there is a concrete plan for release, and active tracing efforts are in place to contact those who do not make their appointments, health outcomes among recently released prisoners are improved.36
The very real problem of human resource shortages in the prisons in Georgia must be addressed. While the country itself has sufficient numbers of physicians and nurses, the situation in the prisons is dire, and there are simply not enough health care professionals to meet the needs of the ever-growing prison population. Thus, Georgia’s prisons could be considered an area of scarce human resources and plans for dealing with human resource shortages in other settings will be adopted in the proposed program. These strategies include incentives for health professionals in the prisons, improved integration into overall TB care, ongoing training, participation in conferences, and salary incentives.37 These also include task shifting work to other lay personnel, and the IHWs will be key in these task shifting activities.38
2) Molecular testing
Improved TB diagnosis in prisons is central to improving Georgia’s overall TB care. This is the area where prisoners will actually have better access to health care because of their increased exposure to TB. The main component of this plan is to implement molecular diagnostic testing for persons in the prisons, prior to introducing it universally throughout the country. New molecular methods are revolutionizing the way TB is diagnosed throughout the world.39 These methods remain somewhat costly and have not yet been recommended for universal implementation. Georgia has access to two of these molecular diagnostic methods but not enough funding and supplies to roll them out nationally. Thus, they will be used preferentially for prisoners, not only to improve infection control, but also, as noted earlier, on the human rights principle of better care for vulnerable populations at highest risk.
3) Infrastructure improvement
Infrastructure improvements throughout the prison system are also crucial in the new plan. Prisoners have “faked” having TB in order to be transferred to the TB prison in Ksani, where conditions are far superior to other institutions. It is telling of the extreme conditions that prisoners find it preferable to fake having a deadly, contagious disease, and to place themselves in the risky situation of being surrounded by TB patients. Rather than punishing individuals caught doing this, or worrying about how many might try, Georgia is committed to improving all the prisons. This will also lead to improved infection control and decreased transmission of TB as windows are put in, air ventilation increased, and large cells holding hundreds of individuals are transformed into more humane housing where TB is less likely to be transmitted.
4) Tanadgoma
Finally, the NTP will work closely with the community-based organization Tanadgoma. Tanadgoma (Georgian for “support”) has worked in the prison system for many years.40 Their work has largely focused on access to HIV testing and care, and they have established HIV testing centers in all prisons. Their work will be used as a model and support for the proposed TB plan.
Limitations of proposed plan
As a proposed plan of reform has not yet been put into place, the potential benefits described above are theoretical. Once implemented, the proposed plan must be closely monitored, and will have several important limitations:
1) Funding
Securing an adequate and sustainable source of funding is of major concern. The Georgian National TB Program has applied to two major international funding organizations to support this project. Furthermore, the country is seeking internal public-private partnerships to fund the proposed reforms. These internal funding sources could potentially provide ongoing support for TB control in the prisons. To date, however, there is no available funding for the proposed project.
2) Implementation
Until funding is obtained, there can be no project implementation. The Georgian NTP has a proposed timeline for the project implementation, which will occur over a six-month period. The time will largely be spent recruiting and training IHWs. Other logistical issues still need to be addressed; chief among these is compensation for the IHWs. While there is general agreement that they should be compensated for their work, it is unclear how this will be done. In addition, prison staff incentives and training are being planned, and the Ministry of Health and Ministry of Corrections and Legal Assistance must approve these. This process can be time consuming and may delay project implementation. Efforts are being made to obtain approvals now so that the project can move forward once funding is obtained.
3) Monitoring
Monitoring of the proposed reforms and the prison health system in general plays a significant role in ensuring that the human rights of the prison population are met. The rights-based approach to TB put forth by the Stop TB Initiative stresses the importance of monitoring and accountability in prison TB control. Currently, the only proposed monitoring of the program is by government-sponsored institutions in Georgia, including the Ministry of Health and the Ministry of Corrections and Legal Assistance. The lack of independent monitoring poses potential problems for the program.
4) Human rights concerns
The proposed reforms begin to address some of the human rights issues the prison population faces with regard to TB. Specifically, the reforms focus on issues of partnership, prisoner empowerment, social and economic factors, dignity, and institutional capacity gaps. However, there are some concerns that the proposed reforms may not offer equivalent care to prisoners with and at risk for TB. IHWs, although an innovative way of addressing capacity gaps, are not substitutes for trained physicians and nurses, and the current reforms do not address this. And although IHWs can provide some advocacy, the proposed reforms do not adequately address the need for advocacy among other populations, in addition to prisoners and former prisoners. Finally, there are other human rights issues raised by politically driven arrests and incarcerations, and overall prison conditions that are not considered in the proposed reforms focused on TB control and care.
Conclusions
The problem of TB in the Georgian prisons has existed for decades, and although some progress has been made, the growing rate of incarcerated individuals has led to a situation that is currently out of control. The government of Georgia has decided to introduce a number of reforms, and it has chosen to do so in a way that addresses some of the human rights issues facing the prison population. Although there have been multiple policy pieces written about human rights and TB care in the prison system, this is one of the first reports to document the planned activities of a national strategy.
However, narrative data collected support the statistical data and point to a very serious problem for TB control in the prisons and the human rights issues inherent therein. The steps taken by Georgia are important and timely, and it is hoped that their example can serve as a model for other countries developing TB programs in their prison systems.
Medea Gegia, MD, MSc, is Head of Epidemiologic Surveillance and Strategic Planning Department, National Center for Tuberculosis and Lung Diseases, Tbilisi, Georgia.
Iagor Kalandadze, PhD, Dr Sc, is Executive Director of the National Center for Tuberculosis and Lung Diseases, Tbilisi, Georgia.
Mikheil Madzgharashvili, MD, is Head of Control Service of TB Project of Penitentiary Department, National Center for Tuberculosis and Lung Diseases, Tbilisi, Georgia.
Jennifer Furin is an assistant professor of medicine and infectious diseases at Case Western Reserve University School of Medicine, TB Research Unit, Cleveland, Ohio, USA.
Please address correspondence to Jennifer Furin, CWRU School of Medicine, TBRU, 2010 Circle Dr., Room E-202, Cleveland, OH, USA 44106; email jjf38@case.edu.
References
1. N. Awofeso, “Prisons as social determinants of hepatitis C virus and tuberculosis infections,” Public Health Reports 125 (2010), Supp 4:25-33.
2. World Health Organization, Global tuberculosis control: WHO report 2010 (Geneva: WHO, 2010).
3. International Journal of Tuberculosis and Lung Disease 13/12 (2009), pp. 1557-1559.
4. International Centre for Prison Studies, World prison brief. Available at http://www.prisonstudies.org/info/worldbrief.
5. I. Baussano, B. Williams, P. Nunn, M. Beggiato, U. Fedeli, and F. Scano, “Tuberculosis incidence in prisons: A systematic review,” PLoS Medicine 7/12 (2010), e1000381.
6. T.P. Flanigan, N. Zaller, L. Taylor et al, “HIV and infectious disease care in jails and prisons: Breaking down the walls with the help of academic medicine.” Transactions of the American Clinical & Climatological Association 120 (2009), pp.73-83.
7. L. Moller, A. Gatherer, and M. Dara,“ Barriers to implementation of effective tuberculosis control in prisons,” Public Health 123/6 (2009), pp. 419-421.
8. H.J. Rutz, S. Bur, M.N. Lobato, S. Baucom, et al “ Tuberculosis control in a large urban jail: discordance between policy and reality. Journal of Public Health Management & Practice 14/5 (2008), pp. 442-447.
9. S. Basu, D. Stuckler, and M. McKee, “Addressing institutional amplifiers in the dynamics and control of tuberculosis epidemics,” American Journal of Tropical Medicine & Hygiene 84/1 (2011), pp. 30-37.
10. A. Sanchez, B. Larouze, A.B. Espinola, J. Pires et al, “Screening for tuberculosis on admission to highly endemic prisons? The case of Rio de Janeiro State prisons,” International Journal of Tuberculosis & Lung Disease 13/10 (2009), pp. 1247-1252.
11. F. Drobniewski, “Tuberculosis in prisons: A forgotten plague,” Lancet 346 (1995), pp. 948–949.
12. R. Coninx, B. Eshaya-Chauvin, and H. Reyes, “Tuberculosis in prisons.” Lancet 346 (1995), p. 1238.
13. F. Portaels, L. Rigouts, and I. Bastian, “Addressing multidrug-resistant tuberculosis in penitentiary hospitals and in the general population of the former Soviet Union,” International Journal of Tuberculosis and Lung Disease 3/7 (1999), pp. 582-588.
14. H. Reyesa and R. Coninx, “Pitfalls of tuberculosis programmes in prisons,” British Medical Journal 315 (1997), p. 1447.
15. World Health Organization. A human rights approach to TB: Stop TB guidelines for social mobilization. (Geneva: WHO, 2001).
16. Stop TB Partnership, Tuberculosis and human rights. Available at http://www.stoptb.org/assets/documents/global/hrtf/Briefing%20note%20on%20TB%20and%20Human%20Rights.pdf.
17. United Nations, First United Nations Congress on the Prevention of Crime and the Treatment of Offenders, Geneva, Switzerland, 1955, U.N. Doc. A/CONF/611, annex I, E.S.C. res. 663C, 24 U.N. ESCOR Supp. (No. 1) at 11, U.N. Doc. E/3048 (1957), amended E.S.C. res. 2076, 62 U.N. ESCOR Supp. (No. 1) at 35, U.N. Doc. E/5988 (1977). Available at http://www2.ohchr.org/english/law/treatmentprisoners.htm.
18. M. Levy, “Prison health services should be as good as those for the general community,” British Medical Journal 315 (1997), pp. 1394-1385.
19. World Health Organization, Global tuberculosis control: WHO report 2011 (Geneva: WHO, 2011). Available at http://www.who.int/tb/publications/global_report/en.
20. The Global Fund Against AIDS, Tuberculosis, and Malaria. Country Reports, Georgia. Available at http://www.theglobalfund.org/en/application/materials/reports.
21. L. Jugheli, L. Rigouts, I.C. Shamputa, W. Bram de Rijk, and F. Portaels, “High levels of resistance to second-line anti-tuberculosis drugs among prisoners with pulmonary tuberculosis in Georgia,” International Journal of Tuberculosis and Lung Disease 12/5 (2008), pp. 561-566.
22. National Tuberculosis Program, Annual report 2010. (Tbilisi, Georgia: National Tuberculosis Program, 2011).
23. A. Aerts, M. Habouzit, L. Mschiladze, N. Malakmadze et al, “Pulmonary tuberculosis in prisons of the ex-USSR state Georgia: Results of a nation-wide prevalence survey among sentenced inmates,” International Journal of Tuberculosis and Lung Disease 4/12 (2000), pp. 1104-1110.
24. International Committee of the Red Cross, ICRC Annual Report. Geneva, 2010. Available at http://www.icrc.org/eng/resources/annual-report/index.jsp.
25. A. Blua, “Azerbaijan, Georgia ‘show the way’ to fight TB in prisons,” Radio Free Europe Radio Liberty (March 23, 2010). Available at http://www.rferl.org/content/Azerbaijan_Georgia_Show_The_Way_For_Fighting_TB_In_Prisons/1991715.html.
26. V.J. Bunce and S. L.Wolchik, “International diffusion and postcommunist electoral revolutions” Communist and Post-Communist Studies 39/3(2006), pp. 283-304.
27. Amnesty International, Georgia/Russia: Civilians in the line of fire: The Georgia-Russia conflict (London: Amnesty International, 2008). Available at http://amnesty.org/en/library/info/EUR04/005/2008/en.
28. International Center for Prison Studies, World prison population list, 8th edition (2008). Available at http://www.kcl.ac.uk/depsta/law/research/icps/downloads/wppl-8th_41.pdf.
29. Ministry of Corrections and Legal Assistance of Georgia, Annual report 2010 (Tbilisi, Georgia: Ministry of Corrections and Legal Assistance of Georgia, 2011. Available at http://www.mcla.gov.ge/cms/site_images/pdf1.pdf.
30. Ministry of Corrections and Legal Assistance Emergency Meeting, Tbilisi, Georgia. April 5, 2011.
31. R.G. Jones, A.N. Trivedi, and J.Z. Ayanian, “Factors influencing the effectiveness of interventions to reduce racial and ethnic disparities in health care.” Social Science & Medicine 70/3 (2010), pp. 337-341.
32. K.C. Maes, C. Hadley, F. Tesfaye, and S. Shifferaw, “Food insecurity and mental health: Surprising trends among community health volunteers in Addis Ababa, Ethiopia during the 2008 food crisis,” Social Science & Medicine 70/9 (2010), pp. 1450-1457.
33. H.L. Behforouz, P.E. Farmer, and J.S. Mukherjee, “From directly observed therapy to accompagnateurs: Enhancing AIDS treatment outcomes in Haiti and in Boston,” Clinical Infectious Diseases 38 Supp 5 (2004), pp. S429-436.
34. J.P. May, P. Joseph , J.W. Pape., and I.A. Binswange, “Health care for prisoners in Haiti,” Annals of Internal Medicine 153/6 (2010), pp. 407-410.
35 Z. Achmat, “Science and social justice: The lessons of HIV/AIDS activism in the struggle to eradicate tuberculosis,” International Journal of Tuberculosis and Lung Disease 10/12 (2006), pp. 1312-1317.
36. T. Conklin,T. Lincoln, and T. Flanigan, “A public health model to connect correctional health care with communities,” American Journal of Public Health 88/8 (1998), pp. 1249-1250.
37. K. Dorman, L. Satterthwaite, A.Howard, S. Woodrow et al, “Addressing the severe shortage of health care providers in Ethiopia: Bench model teaching of technical skills,” Medical Education 43/7 (2009), pp. 621-627.
38. F. Shumbusho, J. van Griensven, D. Lowrance, I. Turate et al, “Task shifting for scale-up of HIV care: Evaluation of nurse-centered antiretroviral treatment at rural health centers in Rwanda.” PLoS Medicine / Public Library of Science 6/10 (2009), p. e1000163.
39. J.C. Palomino, “Molecular detection, identification and drug resistance detection in Mycobacterium tuberculosis,” FEMS Immunology & Medical Microbiology 56/2 (2009), pp. 103-111.
40. The Global Fund for AIDS, Tuberculosis and Malaria. Available at http://portfolio.theglobalfund.org/en/Grant/List/GEO.