Truth and Reconciliation Commissions and Health Care System Responses for Indigenous Peoples: A Scoping Review
Vol 26/1, 2024, pp. 57-70 PDF
Sarah Larson, Cortez Standing Bear, Devon Olson, and Nicole Redvers
Abstract
Grounded in human rights approaches, truth and reconciliation commissions (TRCs) explore an event or process that did widespread and systematic intentional harm to a group of people. Health as a fundamental right is an important component addressed by TRCs. Yet despite TRCs often having recommendations for health care systems, it is unknown how well these recommendations are being translated within health care settings. Therefore, the overarching purpose of our scoping review was to identify academic articles that discussed health care system discourse or responses to TRCs in the context of Indigenous Peoples. Our thematic analysis of the included articles identified three main themes for health care system responses to TRCs: (1) the acknowledgment of multiple ways of knowing, being, and doing in health systems; (2) current interventions as responses within health systems; and (3) suggestions for change within health systems. Although a TRC may create a specific road map and mandate for health care systems, we found considerable variability in the uptake of these actions across institutions. Concerted efforts within and around health care systems and across sectors are therefore necessary to achieve large-scale, meaningful change for Indigenous Peoples post-TRCs and to maintain accountability as a foundational human rights principle.
Introduction
Grounded in human rights approaches, truth and reconciliation commissions (TRCs) create platforms and space to explore an event or process that did widespread and systematic intentional harm to a group of people from human rights violations. Typically established at the national level by a governing body, TRCs are an opportunity to uncover, explore, and acknowledge wrongdoings in a specific context. TRCs have been established for various reasons and have become increasingly common in certain regions around the globe that have faced political strife.[1]
TRCs are very relevant to Indigenous Peoples due to many nationwide policies and practices having systematically worked against Indigenous Peoples’ health and well-being in countries such as the United States and Canada. The “truth” portion of TRCs explores history and seeks to uncover previous wrongdoings, and the “reconciliation” part of TRCs focuses on healing and moving forward. For example, in 2015, born out of the Indian Residential Schools Settlement Agreement, the Truth and Reconciliation Commission of Canada reported its findings on the injustices done to Indigenous Peoples within Canada, particularly within the residential school system.[2] The commission detailed a way forward, with seven “calls to action” specific to health.[3] Other TRCs specific to Indigenous Peoples include the recent commissions established within the Nordic countries of Sweden, Finland, and Norway seeking a path forward for reconciliation with Sámi Peoples.[4] The state of Victoria in Australia has also been active in TRC efforts since 2020, and the state of Maine in the United States established a TRC in 2012.[5] While some TRCs, such as in Canada, are born out of legal settlements at the national or international level, others, such as those in the Nordic region, have been more inspired by social and political movements.[6] Although these commissions may not be focused solely on health, the need for healing has been deeply embedded in many of their processes.
Nations must recognize the human rights violations that have occurred due to colonization and the harm it has caused to Indigenous Peoples and their health.[7] The TRC process may be one pathway to accountability and may act as an impetus for health care systems to uphold human rights. The World Health Organization recognizes the right to health for all peoples, without discrimination, via services that are culturally acceptable, yet it is currently unclear how TRCs may help fulfill this right. That said, TRCs may be an effective mechanism for beginning the process of healing within communities and reversing the complex health disparities that are present within Indigenous communities globally by creating guidance around how to fulfill the human right to health within health care systems.[8]
Despite TRCs (both established and in progress) often having provisions for health care systems, it is unknown the extent to which TRCs’ recommendations are applied to health care settings.[9] There has been no widespread examination of TRCs’ involvement in health care, particularly in the context of Indigenous health. Therefore, the overarching purpose of our scoping review was to identify academic articles that discuss health care system discourse or responses to TRCs internationally in the context of Indigenous Peoples. The specific objectives of our review were to identify specific health system responses to TRCs in the context of Indigenous health, as well as any current recommendations, gaps, and ongoing discussions.
Positionality
“Nothing about us, without us” is an increasingly applied concept in academic writing.[10] Given this, it is best practice to ensure that authors, when writing by or about Indigenous Peoples, position themselves in relation to the work.[11] The first author of this paper (SL) is of settler descent participating as an ally in this work and is currently based in the United States. The second author (CSB) is a member of the Oglala Sioux Tribe and is currently based in the United States. The third author (DO) is of settler descent participating in this work as a medical research librarian and ally and is currently based in the United States. The senior author (NR) is an Indigenous health scholar and a member the Deninu K’ue First Nation and is currently based in Canada.
Methods
Overall design
This scoping review follows the framework developed by Hilary Arksey and Lisa O’Malley, further refined by Micah Peters et al.[12] The search process was co-created with a medical research librarian (DO) and conducted systematically. A protocol was published within the Open Science Framework on September 30, 2022.[13] The PRISMA-ScR extension was used for ensuring appropriate reporting standards for scoping reviews.[14] Our specific research question for this review was, What health care system discourse or responses exist as a result of truth and reconciliation commissions in the context of Indigenous Peoples?
Eligibility criteria, procedures, and search terms
We searched the following electronic databases using Boolean phrases and key terms to identify relevant studies: PubMed, Embase (Elsevier), CINAHL (EBSCO), Web of Science (Clarivate), and Academic Search Ultimate (EBSCO). Our specific search terms varied by database and represented combinations of the terms “truth commission,” “truth and reconciliation,” “health,” “medicine,” “wellness,” “primary care,” “emergency care,” “tertiary care,” “hospital,” and “clinic” (see Table 1 for an example search strategy and Appendix A—available from the authors—for the full search strategy). We then searched Google Scholar by reviewing the first two pages, and then subsequently screened the next set of two pages until no article titles within our inclusion criteria were found. We then completed manual searches for relevant articles in the iPortal Indigenous Studies Portal, Native Health Database, International Journal of Indigenous Health, International Indigenous Policy Journal, Turtle Island Journal of Indigenous Health, and Journal of Indigenous Wellbeing-Te Mauri Pimatisiwin. We also searched the reference lists of key articles to further identify relevant articles. All articles identified as part of the search strategy were transferred into Covidence review software (v2721 a9510157) to facilitate the selection process.

Article screening
For the purposes of article selection, we defined a health care system as any system, program, or field that influences the delivery of health care. In this light, we included academic articles that discussed health system discourse or responses to TRCs that related specifically to Indigenous Peoples. Articles had to therefore mention both TRCs and an aspect of health care systems, as well as to have a focus on Indigenous Peoples. We included articles if they were published after the establishment of a TRC process or as a direct result. For the purposes of this review, we utilized the United Nations system’s understanding of Indigenous Peoples, which is based on the following characteristics:
self-identification as [I]ndigenous [P]eoples at the individual level and accepted by the community as their member; historical continuity with pre-colonial and/or pre-settler societies; strong link to territories and surrounding natural resources; distinct social, economic or political systems; distinct language, culture and beliefs; form non-dominant groups of society; resolve to maintain and reproduce their ancestral environments and systems as distinctive peoples and communities.[15]
We included only those articles written in English, with no limits on the date of publication. There were no restrictions on article type as long as it was published in an academic journal.
For our scoping review, we engaged a two-stage article review process. The title and abstract screening stage included 100% double screening by two independent reviewers (SL and CSB). A third reviewer (NR) was brought in whenever there were cases of discrepancies, which were subsequently resolved by discussion. The full-text screening stage was completed 100% by one reviewer (SL), with a 25% double screening process (CSB) to ensure consistency, and a third reviewer (NR) brought in for any discrepancies, which were resolved by discussion.
Data characterization, summary, and synthesis
We extracted data from the relevant articles and charted them in Excel 365. These data included general article information, type of article, level or sector of health care, rural or urban setting (if known), geographic location, specific Indigenous population (if specified), and name of the TRC or truth commission involved. We uploaded included articles to NVivo software for the coding process. Articles were coded for commission responses and contexts via an inductive process to identify themes through thematic analysis as described by Virginia Braun and Victoria Clarke.[16] We tracked the stages of coding through analytic folders while refining, defining, and naming the themes. We had one author (SL) carry out the preliminary coding, and we brought in a second author (NR) for discussion and coding audit that led to ongoing refining of the codes and themes.
Results
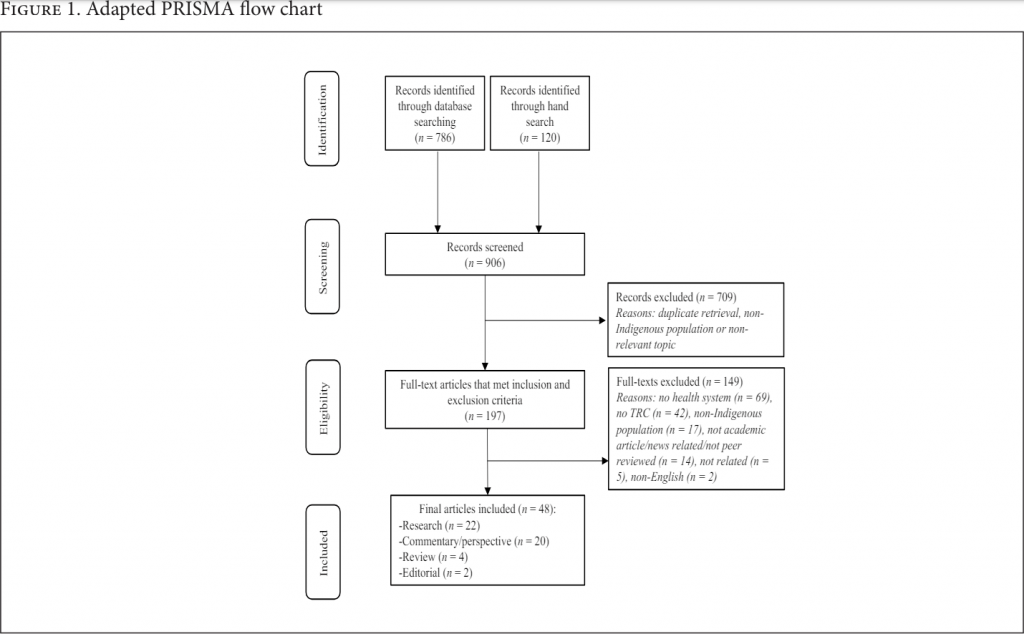
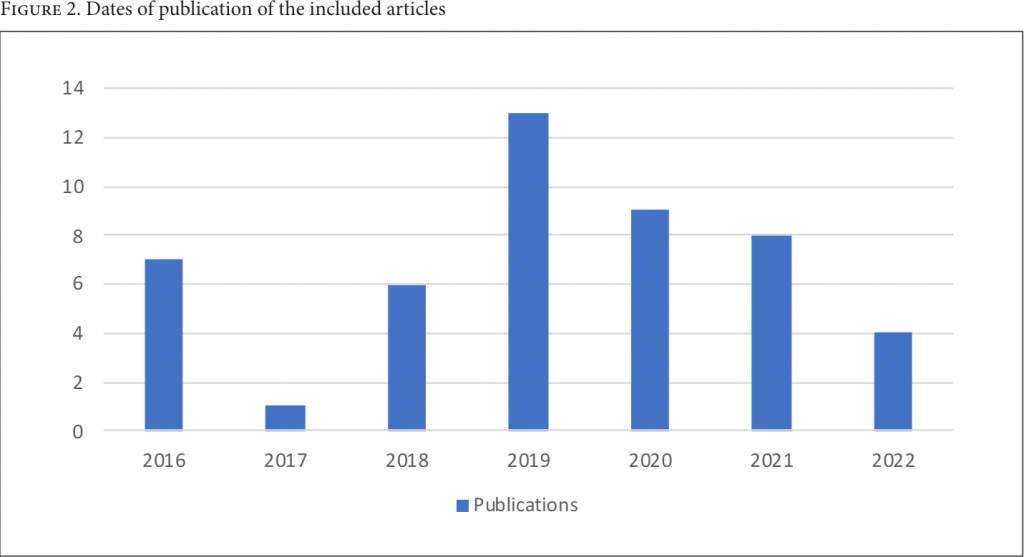
Of the 906 articles imported for screening, 48 met the inclusion criteria (see Figure 1). Despite our search strategy being globally inclusive (i.e., no limitations on region), all 48 articles were in response to the Truth and Reconciliation Commission of Canada. The included articles represented many different health system professional fields, including occupational therapy, nursing, and physiotherapy, as well as varied sub-specialties. Some of the included articles focused on health care delivery more broadly, such as in the primary care setting. Additional articles addressed the larger health care systems in place that include hospital systems, policies, and interdisciplinary collaboration. The majority of the included articles were published relatively recently, with the oldest article dating back to 2016 (see Figure 2). (Appendix B, available from the authors, provides the full data extraction for all included articles.)
TRC responses
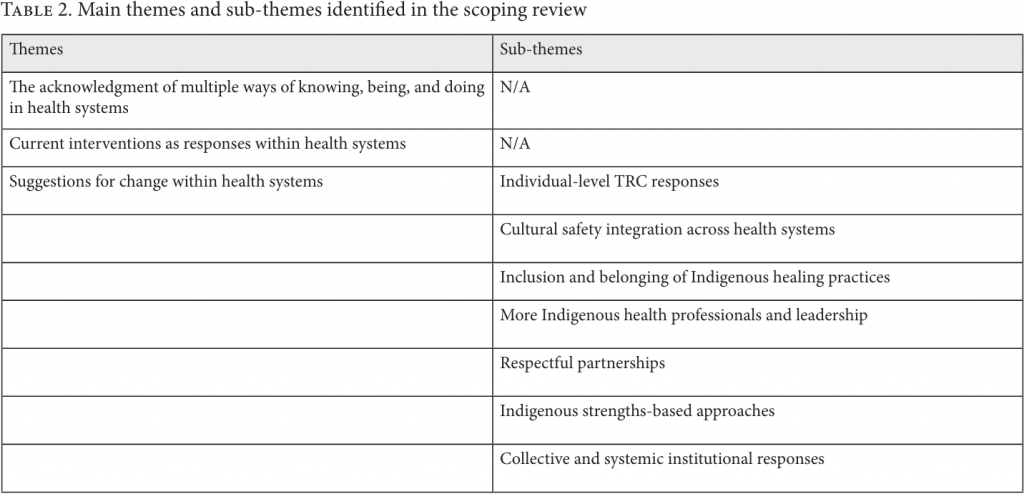
Our thematic analysis identified three main themes for health care system responses to TRCs in the reviewed literature: (1) the acknowledgment of multiple ways of knowing, being, and doing in health systems; (2) current interventions as responses within health systems; and (3) suggestions for change within health systems, which itself had seven sub-themes (see Table 2).
The acknowledgment of multiple ways of knowing, being, and doing in health systems
Health care services in Canada are currently created and maintained by a Euro-Western system that many articles challenged as not adequately serving Indigenous Peoples. To move forward in enacting truth and reconciliation in health care, seven articles stated that fundamental assumptions and understandings about health care must be evaluated from, and more integrated with, an Indigenous perspective (i.e., one that acknowledges explicitly multiple ways of knowing, being, and doing).[17] Some articles discussed epistemic racism within the system, which is “the privileging of one knowledge system over another.”[18] Authors from one article highlighted the Euro-Western-dominated worldview in health care, where colonialism and structural racism remain ingrained: “entrenched structural racism persists and, we believe, impedes meaningful application of cultural safety and humility across the human service sector … chaotic emergency rooms are built upon colonial administrative systems.”[19]
Additionally, an evaluation of the client-centered enablement model was found to not be appropriate in Indigenous contexts because “the model itself is developed within a colonial, Eurocentric context.”[20] Better acknowledgment of multiple ways of being (i.e., moving away from colonial systems) lies in what they call “micro reconciliation,” which builds on cultural safety to shape everyday interactions to better reflect overall reconciliation efforts.[21] Micro reconciliation is to be implemented at a systems level with “administrative and practitioner levels of engagement.”[22] Another article argued that quality health care delivery for Indigenous Peoples in Canada is dependent on both individual and institutional reflection and change.[23]
Dominique Fijal and Brenda Beagan created a new theory based on the established “Two-Eyed Seeing” approach (“the gift of multiple perspectives”) that incorporates balance, spirituality, community, and meaning in order to address the need for a better health system response to the TRC.[24] Another form of health system response proposed was to platform “epistemic pluralism” (i.e., acknowledging multiple ways of knowing) where dialogue and mutual understanding exist between Western evidence-based practice and Indigenous healing practices to better provide appropriate care.[25] One example of epistemic pluralism in practice was embodied in a qualitative study in which the First Nations individuals interviewed called for the increased integration of traditional healing practices in the health care system, including destigmatization, collaboration, the application of practices, and funding.[26] An article in the field of occupational therapy further identified the need for incorporating epistemic pluralism into their practice, stating that “Canadian occupational therapists working with Indigenous Peoples are armed with models of practice that do not reflect Indigenous perspectives.”[27] Article authors generally found that epistemic pluralism, through micro reconciliation and the adoption of theoretical approaches in operations, such as Two-Eyed Seeing, is needed as part of the reconciliation process.
Current interventions as responses within health systems
Fourteen of the included articles discussed current interventions or strategies that exist in response to the TRC, some seeking to respond directly to the TRC’s calls to action.[28] For example, one identified program hired Elders as allied health professionals, while another incorporated Elders in primary care teams and direct patient care.[29] Another project used a “Two Row Wampum” approach to further tuberculosis programming as part of a broader human rights effort to promote health outcomes for Indigenous communities within the Canadian prairies.[30] The “Wellness Wheel” clinics additionally used a unique hub-and-spoke model to serve remote communities in a culturally safe way.[31]
Many programs featured traditional healing options within the clinical setting, such as creating space in a hospital to hold ceremonies, for smudging, or to meet with healers, as well as ensuring that other forms of cultural supports are available.[32] The Nîsohkamâtowak program specifically integrates Indigenous practices and perspectives to serve those seeking kidney care in northern Saskatchewan via a partnership with First Nations and Metis Health Services.[33] Other approaches for diabetes trauma-informed care have emerged via guidance from Elders and Indigenous Peoples.[34] To better understand and plan how to integrate traditional practices within health care, a video and discussion guide was created by the intercultural Online Health Network at the University of British Columbia.[35]
Aside from programmatic-level activities and efforts, systems-level interventions have been identified as a response to the TRC within health systems. For example, the First Nations Health Authority was established in 2013 and was a significant transformation of the health governance structure toward self-determination that emulated the TRC recommendations that were concurrently in process at the time.[36]
Suggestions for change within health systems
Forty-seven articles presented various suggestions for change within health systems. More specifically, many of the included articles in this section outlined suggestions or recommendations for how to implement the TRC calls to action in the health care system. Notably, the need for cultural safety training was referenced in 27 out of the 48 articles. In addition, 15 of the 47 articles called for some recognition or incorporation of Indigenous knowledges or healing practices in the health care setting. There were seven associated sub-themes identified under this theme of “suggestions for change,” as discussed below.
Individual-level TRC responses. Responses to the TRC in the health care setting can occur at several levels. At the individual level, many articles recognized that individual health care providers have a responsibility to engage with reconciliation.[37] There were calls for health professionals, especially those in leadership positions, to personally read, understand, and engage with the TRC report directly.[38] Caroline Tait, William Mussel, and Robert Henry wrote, “recognizing what aspects of the TRC’s Calls to Action are in one’s own personal power to put into practice begins a process of challenging systems that underlie settler colonialism.”[39] Some articles suggested that once professionals are familiar with the TRC and its calls to action, they in turn can bring about discussion in their respective organizations and sectors.[40] These actions were stated to be imperative because “a renewed commitment and concrete steps are needed by non-Indigenous leaders and allies to support this decolonizing work so that it does not fall solely upon First Nations, Inuit, and Metis Peoples.”[41] Overall, many of the articles called on Indigenous and non-Indigenous health professionals to be personally engaged in the reconciliation processes.
Cultural safety integration across health systems. One of the most frequently cited elements for change was through culturally safe practices and training within health systems.[42] The TRC calls to action specifically refer to the provision of “cultural competency” training; however, most of the articles within this section advocated for “cultural safety training” instead, with a focus on “power imbalances that characterize encounters in clinical settings.”[43] In this regard, many articles called for cultural safety training that contextualizes Indigenous health within the understanding of past and ongoing colonization.[44] Colonization must be understood as one of the “upstream causes of poor health,” and “the need for health care providers to understand how colonization affects the health and wellbeing of Indigenous [P]eople is compulsory.”[45]
Cultural safety modules that have been established may differ across organizations. For example, one study evaluated the “Indigenous relationship and cultural safety” courses in nursing as an effective way to gain knowledge and skills.[46] Not only did the online course increase users’ knowledge, but users also reported the ability to apply that knowledge in practice. Another article, however, emphasized that cultural safety as a model was an important step, yet it may not be enough without considering how to fully revise mainstream Western models while “honouring our past and reconciling with history.”[47]
Inclusion and belonging of Indigenous healing practices. Colonization has enabled the suppression and stigmatization of Indigenous knowledge systems, structures, and healing practices. The TRC calls to action specifically reference the need to return to Indigenous healing traditions as part of the reconciliation process.[48] Bringing Indigenous cultural practices and wellness concepts into care delivery has been shown to improve mental health, and there were calls in some of the articles to expand these offerings within health care settings.[49] For example, Indigenous patients have vocalized the desire for increased culturally appropriate services that may include Elders and healers.[50] With this, the integration of Elders in health care settings has been shown to be a successful approach as a response to the TRC calls to action.[51]
A survey of rheumatologists across Canada found that they generally support the integration of Indigenous healing practices.[52] However, Logan emphasized that while physicians generally seemed open to a differing worldview, “it is important for physicians not to judge, nor to simply learn about Indigenous healing practices, but rather to create space for these practices as an act of reconciliation.”[53] To consider the bridging of Western health systems with Indigenous healing practices, it is important that Indigenous healing practices be truly respected.[54] Definitions of health and wellness should also be adapted to Indigenous perspectives, while addressing misconceptions about traditional healing.[55] The recognition of the importance of Indigenous healing methods must occur because “in reality, many … [First Nations P]eople are already making these choices to apply traditional healing for their wellbeing,” and there are consistent calls for ensuring a collaborative approach to care.[56]
More Indigenous health professionals and leadership. The TRC calls to action advocate for an increase in Indigenous health professionals and health system leaders. Many articles noted that Indigenous health professionals and leaders can help provide culturally safe and appropriate care as well as assist organizations in creating systems to do the same.[57] The recruitment and retention of Indigenous health care workers are also stated to be important, in addition to actually listening to their guidance.[58] These elements (i.e., increasing, retaining, and listening to Indigenous health professionals) must occur in tandem. While increasing the recruitment and retention of Indigenous health professionals is important, systems must also work to ensure safe spaces, inclusion, belonging, and therefore effective care for Indigenous and all patients.[59]
In general, Indigenous leadership was noted to be an important factor in instigating changes in health care systems. This change was not only in the case of Indigenous health professionals serving clients directly, but also in cases where Indigenous leaders were active decision-makers and policy makers within the health system.[60] Indigenous health system leaders can help integrate Indigenous perspectives in decision-making, “rather than preserving norms of colonial control.”[61]
Respectful partnerships. Directed by Indigenous leadership, partnerships were emphasized in many of the included articles as fundamental to health systems change.[62] Partnerships should be conducted with special attention to ground them “in Indigenous collaborative approaches such as Two-Eyed Seeing and Ethical Space … mutual trust, respect, equality, and collaboration for respectful interactions of differing ways of knowing.”[63] As an example, Alberta Health Services established an Indigenous Health Core Committee, which was a 55-member network that supported the creation of guiding principles and strategic directions.[64] Other partnerships were for tuberculosis care based in the spirit of the Two Row Wampum belt, and the Wellness Wheel Mobile Outreach clinic.[65] Collaborating systems are particularly important in remote areas of service, which is reflected in the Wellness Wheel model.[66]
An article by John O’Neil et al. discussed the development of partnerships as key to systems and governance changes. The authors noted that partnerships need “to be enabled by administrative and structural changes within and between partners to align with commitments” and that “reciprocal accountability requires each partner to effectively position themselves and build their capacity to support shared commitments.”[67] They found the formation of individual and personal relationships to be important in facilitating and building institutional relationships and noted that those delivering health services must be part of the partnership process and implementation.[68]
Indigenous strengths-based approaches. As health systems consider adopting changes to better meet the needs of Indigenous communities in response to the TRC, there were consistent calls within the included articles for strengths-based approaches that not only recognize the importance of traditional and Indigenous knowledges and practice but also acknowledge the strengths of the communities and individuals they serve.[69] Health system changes should acknowledge and bolster the strengths within Indigenous communities instead of perpetuating a deficit-based lens. As noted by one article, “We are recommending a shift away from deficit, disease, and disparity approaches to investigation which locate the problem in the individual and instead, move towards locating areas of improvement at a larger, systems level, with a strengths-based lens to achieve health equity.”[70] Such initiatives must be guided by self-determination given that Indigenous communities already host resilience and innovative leadership within them.[71]
Collective and systemic institutional responses. Institutional and system-level responses were suggested as fundamental to the TRC process for health system change. Any institutional change process was noted, however, to require “dedicated human, material, and financial resources.”[72] One suggestion was that “accountability processes such as accreditation and quality reviews for hospitals and institutions must include metrics for Indigenous health equity and reconciliation” at the systems level.[73]
One article noted specific actions that leaders in the health care system should take to shift institutional response.[74] The article suggested incorporating TRC discussions into regular meetings and strategic planning; partnering with other organizations interested in the same work; and importantly, being mindful not to overburden “First Nations, Metis, and Inuit employees with the responsibility to move Truth and Reconciliation forward” in their organizations.[75] Overall, the included articles made it clear that system-level changes would require in-depth reflection and engagement, with respect for and deep involvement of Indigenous perspectives. It was suggested that models of care be broadened to include health promotion and disease prevention, with attention on the social determinants of health and the impacts of colonization at the community level.[76] One additional suggestion for a TRC-inspired health system change was a movement toward increased infrastructure at the national level to create a “centre of excellence committed to Indigenous PHC [primary health care] to strategically frame clinical services within a population health approach” as an exemplar for other health system stakeholders.[77]
Discussion
This scoping review sought to identify health system responses to TRCs in the context of Indigenous health, as well as any current recommendations and discussions. We identified three main themes: (1) the acknowledgment of multiple ways of knowing, being, and doing in health systems; (2) current interventions as responses within health systems; and (3) suggestions for change within health systems. Notably, Canada was the only TRC represented in the health care systems literature in this review. Though several other national and subnational governments are working on their unique TRC processes, there is little formal scholarship examining these processes. This gap in the literature highlights the need for increasing discussion and transparency around TRC dialogue and implementation effects for Indigenous Peoples globally.
Overall, we identified a broad range of health care system responses to the TRC in Canada. Many of the suggested responses highlighted a need for balance between individual, relational, and institutional responsibility and action for overall change. Many of the articles noted the importance of individual health care professionals and leaders personally investing in reconciliation efforts. Challenging personal assumptions and beliefs was a central tenet to transformation through processes such as mandated cultural safety training. Leaders and those engaged in providing direct care must be active participants in this work to propel policies and changes. The incorporation of Indigenous knowledges and healing traditions must be central to the TRC process for health care institutions. The spirit of reconciliation is not just one of apology and subsequent maintenance of the status quo. Instead, it is an inspiration and mandate to instigate great change to promote human rights, equity, and justice for the health of all peoples.
The articles presented many current and ongoing challenges of responding to the TRC in the Canadian health care system. At an individual level, there may continue to be a lack of recognition of the need for changes. For example, “as physicians, we may perpetuate health inequities through ignorance about colonial determinants of health, ignoring our role in perpetuating power imbalances, complicity in institutional racism, and failing to question paternalistic models of care.”[78] Physicians, while often open to change, may still be hesitant to incorporate Indigenous healing practices in their care plans in cooperation with Indigenous healers. One article noted that “they would only do so if the practices were tested and shown to fulfill their western paradigm of understanding.”[79] This perspective is consistent with findings from other scholarship in this area.[80] The concepts of healing and wellness often remain different for Western practitioners and their Indigenous patients, with sometimes very different goals.[81] These differing conceptualizations of care echo a similar concern found in an article investigating nurses’ cultural competency, where many respondents were overly confident in their knowledge, signifying a knowledge gap.[82] Regarding individuals being agents for change in responding to the TRC, personal perceptions are a potential barrier overall. Some health professionals and leaders may not know where to begin or how to approach implementing the TRC recommendations due to the lack of discourse and understanding within their respective fields.[83] Additionally, the length and depth of attention and investment needed from individual professionals and leaders can be a challenge to accomplish the suggested action of understanding colonial histories and their implications for health inequities.[84]
The health care system serving Indigenous communities is being called to decolonize, yet there are little to no real indicators (policy or otherwise) that this is in process or is being taken seriously by high-level operational mechanisms. In this regard, there were noted gaps in accountability mechanisms for the uptake of the calls to action across the included articles. Accountability is a foundational principle of human rights and must be included in TRC efforts. For example, very few articles noted health system indicators to assess for measured changes in meeting the TRC calls to action. There is thus a need for better discussion, research, and action to further develop, in collaboration with Indigenous communities, quality indicators that can track how health systems are meeting their TRC objectives. Without specific and detailed accountability measures in place, it is difficult to ensure that health systems are meeting their TRC commitments. Health systems attempting to meet TRC commitments are further strained by concerns about whose interests—those of the health system or those of Indigenous Peoples—reconciliation is really serving. Overall accountability is important to measure actionable change, as apologies are often currently framed as being the beginning of reconciliation, yet they are “often where actions stop.”[85] Given this, partnerships for change are often “more challenging in light of the negative legacy of relationships between First Nations and federal and provincial governments, as well as the broader scope required to acknowledge the needs of many partners, which further impacts the capacity to deliver in a timely manner and endangers legitimacy.”[86]
Although the need for systemic change was highlighted in some of the articles, the articles pointed to a general gap in specific policy actions at a systems level. One article noted how current changes lack “a sustained approach that allows resourcing to implement, evaluate, and eventually innovate models.”[87] While solutions such as cultural safety trainings are important, “more is needed to achieve a system-level course correction.”[88] The health care system generally does not seem to have a strong, cohesive, and active approach for systemic change; however, this could be due to a complete lack of investigation into related TRC system-level approaches. Some articles did recognize that it is difficult to “examine, identify, and modify policy and standards of practice that either obviously or inadvertently foster inequitable health care and health outcomes for Indigenous People.”[89]
Lastly, articles emphasized the importance of addressing histories and contexts that shape health statuses. Current movements toward health equity for Indigenous Peoples may remain entrenched in Western and colonial paradigms that will not change the actual status of health. For example, one article stated that “reconciliation as a state approach that claims to take up structural violence in fact entrenches settler-colonial biogovernance through its technologies of chronic disease management.”[90] The current focus on individuals “rather than societal, economic, and political contexts, further exacerbates health impacts.”[91] Acknowledgment of and action on the wider Indigenous determinants of health—with a clear understanding of historical and contemporary colonial contexts—are necessary to implement effective practice and accountability, while creating health system change in the context of the TRC calls to action.[92] It must be additionally noted, however, that while TRCs provide an authoritative process and vehicle by which health care systems can engage with reconciliation, they may not be a necessary precondition.
Given the dominance of articles from Canada, the country may provide a unique TRC model for other nations to reflect on in terms of how to move forward in creating a health care system that considers culturally appropriate care as a human right. Caution is still advised, however, given the lack of accountability metrics associated within the included articles, which makes it difficult to assume overall effectiveness within the Canadian context. Indigenous Peoples in Canada still face substantial health inequities and human rights violations.[93] Even if improvements have been made since the TRC was created in Canada, these have not been adequately qualified within health systems at the national level to make any firm statements of efficacy. Regardless, the literature out of Canada may imply the importance of a formal TRC in bringing about discourse and change toward health equity and reconciliation.
Limitations
Since this review sought to understand the academic discourse on the topic, we did not include government or health system documents that may further explore the implementation of TRC recommendations in public and private arenas. Future work on this topic should therefore seek to review the gray literature to assess any additional elements focusing specifically on TRC accountability measures that may be in place outside of the academic literature. Additionally, while this review intended to gather international data, all the articles that we found were within the Canadian context. This could have been due to our being able to review only English-language articles. Therefore, generalizing to other countries and contexts may be difficult. Additional work should be done to further this review to other languages to increase the potential breadth of information on how varied health systems may be responding to TRCs or truth commissions in their respective contexts. Future research is also needed to better understand the connection between the role of TRCs, health care system changes, and social movements.
Conclusion
While the calls to action of the TRC in Canada created a specific road map and mandate for the health care system in Canada, “there is considerable variability in the uptake of these actions across institutions.”[94] Concerted efforts within and around the health care system and across sectors must take place to have large-scale, meaningful change for Indigenous Peoples. Such system-level efforts, however, may be undermined by the frameworks in which they are conceived. Therefore, there is a strong need for fundamental decolonization and the centering of Indigenous Peoples and their perspectives, with both elements being imperative to all continued health care responses to the TRC.
Sarah Larson is an MPH graduate with a focus on Indigenous health in the School of Medicine and Health Science at the University of North Dakota, Grand Forks, United States.
Cortez Standing Bear is an MPH student specializing in population health research and analytics in the School of Medicine and Health Science at the University of North Dakota, Grand Forks, United States.
Devon Olson, MLIS, AHIP, is a research and education librarian in the School of Medicine and Health Science at the University of North Dakota, Grand Forks, United States.
Nicole Redvers, ND, MPH, is an associate professor in the Schulich School of Medicine and Dentistry at the University of Western Ontario, London, Canada, and an adjunct professor in the Department of Indigenous Health at the University of North Dakota, Grand Forks, United States.
Please address correspondence to Sarah Larson. Email: sarahjlars@outlook.com.
Competing interests: None declared.
Copyright © 2024 Larson, Standing Bear, Olson, Redvers. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] M. B. Hirsch, M. Mackenzie, and M. Sesay, “Measuring the Impacts of Truth and Reconciliation Commissions: Placing the Global ‘Success’ of TRCs in Local Perspective,” Cooperation and Conflict 47/3 (2012).
[2] Truth and Reconciliation Commission of Canada, Honouring the Truth, Reconciling for the Future: Summary of the Final Report of the Truth and Reconciliation Commission of Canada (Winnipeg: Truth and Reconciliation Commission of Canada, 2015).
[3] Truth and Reconciliation Commission of Canada, Truth and Reconciliation Commission of Canada: Calls to Action (Winnipeg: Truth and Reconciliation Commission of Canada, 2015).
[4] A. Szpak and D. Bunikowski, “Saami Truth and Reconciliation Commissions,” International Journal of Human Rights 26/2 (2022).
[5] A. Mashford-Pringle, “How’d We Get Here from There? American Indians and Aboriginal Peoples of Canada Health Policy,” Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health 9/1 (2011); B. Collins and A. Watson, “Refusing Reconciliation with Settler Colonialism: Wider Lessons from the Maine Wabanaki-State Child Welfare Truth and Reconciliation Commission,” International Journal of Human Rights 27/2 (2023).
[6] Szpak and Bunkiowski (see note 4).
[7] Mashford-Pringle (see note 5).
[8] L. J. Kirmayer and G. Brass, “Addressing Global Health Disparities among Indigenous Peoples,” Lancet 388/ 10040 (2016).
[9] Truth and Reconciliation Commission of Canada, Calls to Action (see note 3).
[10] P. Roach and F. McMillan, “Reconciliation and Indigenous Self-Determination in Health Research: A Call to Action,” PLOS Global Public Health 2/9 (2022); M. Lock, F. McMillan, B. Bennet, et al., “Position Statement: Research and Reconciliation with Indigenous Peoples in Rural Health Journals,” Australian Journal of Rural Health 30/1 (2022).
[11] Roach and McMillan (see note 10); Lock et al. (see note 10).
[12] H. Arksey and L. O’Malley, “Scoping Studies: Towards a Methodological Framework,” International Journal of Social Research Methodology 8/1 (2005); M. D. J. Peters, C. Marnie, H. Colquhoun, et al., “Scoping Reviews: Reinforcing and Advancing the Methodology and Application,” Systematic Reviews 10/1 (2021).
[13] S. Larson, “Truth and Reconciliation Commissions and Healthcare System Responses for Indigenous Peoples: A Scoping Review Methodology,” OSF, https://osf.io/5zxck/.
[14] M. J. Page, J. E. McKenzie, P. M. Bossuyt, et al., “The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews,” BMJ 372 (2021).
[15] United Nations Permanent Forum on Indigenous Issues, Fact Sheet: Who Are Indigenous Peoples? (2006).
[16] V. Braun and V. Clarke, “Using Thematic Analysis in Psychology,” Qualitative Research in Psychology 3/2 (2006); V. Braun and V. Clarke, “Reflecting on Reflexive Thematic Analysis,” Qualitative Research in Sport, Exercise and Health 11/4 (2019).
[17] M. Anderson, “An Indigenous Physician’s Response to the Settler Physician Perspective on Indigenous Health, Truth, and Reconciliation,” Canadian Medical Education Journal 9/4 (2018); S. M. Cohen-Fournier, G. Brass, and L. J. Kirmayer, “Decolonizing Health Care: Challenges of Cultural and Epistemic Pluralism in Medical Decision-Making with Indigenous Communities,” Bioethics 35/8 (2021); D. Fijal and B. L. Beagan, “Indigenous Perspectives on Health: Integration with a Canadian Model of Practice,” Canadian Journal of Occupational Therapy 86/3 (2019); G. Kyoon Achan, R. Eni, K. A. Kinew, et al., “The Two Great Healing Traditions: Issues, Opportunities, and Recommendations for an Integrated First Nations Health care System in Canada,” Health Systems and Reform Journal 7/1 (2021); N. Lachance and T. Rose, “From Colonization to Reconciliation: Increasing the Collaborative Capacity of Public Servants,” Canadian Public Administration 63/4 (2020); C. Hunter and T. Pride, “Critiquing the Canadian Model of Client-Centered Enablement (CMCE) for Indigenous Contexts,” Canadian Journal of Occupational Therapy 88/4 (2021); C. L. Tait, W. Mussell, and R. Henry, “Micro-Reconciliation as a Pathway for Transformative Change,” International Journal of Indigenous Health 14/2 (2019).
[18] Anderson (see note 17); M. Djkowich, C. Ceci, and O. Petrovskaya, “Bearing Witness in Nursing Practice: More Than a Moral Obligation?,” Nursing Philosophy 20/1 (2019); Cohen-Fournier et al. (see note 17); R. Long, C. Heffernan, M. Cardinal-Grant, et al., “Two Row Wampum, Human Rights, and the Elimination of Tuberculosis from High-Incidence Indigenous Communities,” Health and Human Rights Journal 21/1 (2019).
[19] Tait et al. (see note 17).
[20] Hunter and Pride (see note 17).
[21] Tait et al. (see note 17).
[22] Ibid.
[23] Ibid.
[24] Fijal and Beagan (see note 17); C. Bartlett, M. Marshall, and A. Marshall, “Two-Eyed Seeing and Other Lessons Learned within a Co-learning Journey of Bringing Together Indigenous and Mainstream Knowledges and Ways of Knowing,” Journal of Environmental Studies and Sciences 2/4 (2012).
[25] Cohen-Fournier et al. (see note 17).
[26] Kyoon Achan et al. (see note 17).
[27] Fijal and Beagan (see note 17).
[28] R. Henderson, S. Montesanti, L. Crowshoe, and C. Leduc, “Advancing Indigenous Primary Health Care Policy in Alberta, Canada,” Health Policy 122/6 (2018); G. Hadjipavlou, C. Varcoe, D. Tu et al., “‘All My Relations’: Experiences and Perceptions of Indigenous Patients Connecting with Indigenous Elders in an Inner City Primary Care Partnership for Mental Health and Well-Being,” CMAJ 190/20 (2018).
[29] Ibid.
[30] Long et al. (see note 18).
[31] M. Pandey, S. Nicolay, M. Clark, et al., “Wellness Wheel Mobile Outreach Clinic: A Community-Led Care Model Improving Access to Care in Indigenous Communities,” Annals of Family Medicine 18, no. 5 (2020).
[32] Cohen-Fournier et al. (see note 17); J. L. Drost, “Developing the Alliances to Expand Traditional Indigenous Healing Practices within Alberta Health Services,” Journal of Alternative and Complementary Medicine 25/S1 (2019); L. I. A. Sanzone, E. Doucette, N. Fansia, et al., “Indigenous Approaches to Healing in Critical Care Settings: Addressing the Truth and Reconciliation Report’s Calls to Action,” Canadian Journal of Critical Care Nursing 30/3 (2019).
[33] T. Blair, P. Babyn, G. Kewistep, et al., “Program Report: Nîsohkamâtowak-Helping Patients and Families Living with Kidney Disease in Northern Saskatchewan,” Canadian Journal of Kidney Health and Disease 9 (2022).
[34] R. Sovdi and B. Macdonald, “Honouring the Stories and Experiences of Indigenous Peoples with Diabetes Through Trauma-Informed Care,” Canadian Journal of Diabetes 45/7 (2021).
[35] A. Hyman, E. Stacy, K. Atkinson, et al., “Digital Storytelling and Dialogue to Support Culturally Safe Health Care for Indigenous Patients in British Columbia,” British Columbia Medical Journal 62/3 (2020).
[36] J. O’Neil, J. Gallagher, L. Wylie, et al., “Transforming First Nations’ Health Governance in British Columbia,” International Journal of Health Governance 21/4 (2016).
[37] D. Jaworsky, “A Settler Physician Perspective on Indigenous Health, Truth, and Reconciliation,” Canadian Medical Education Journal 9/3 (2018); M. E. Pearce, K. Jongbloed, L. Demerais, et al., “‘Another Thing to Live for’: Supporting HCV Treatment and Cure among Indigenous People Impacted by Substance Use in Canadian Cities,” International Journal of Drug Policy 74 (2019); P. Smith, “Commentary: A Settler Physician Perspective on Indigenous Health, Truth, and Reconciliation,” Canadian Medical Education Journal 9/3 (2018); A. Phenix and K. Valavaara, “Occupational Therapy Responses to the Truth and Reconciliation Commission,” Occupational Therapy Now 21/4 (2019); Lachance and Rose (see note 17).
[38] K. Gasparelli, H. Crowley, M. Fricke, et al., “Mobilizing Reconciliation: Implications of the Truth and Reconciliation Commission Report for Physiotherapy in Canada,” Physiotherapy Canada 68/3 (2016); K. D. Fellner, J. Ansloos, N. L. Oullette, and G. D. Villebrund, “Reconciling Relations: Shifting Counselling Psychology to Address Truth and Reconciliation,” Canadian Journal of Counselling and Psychotherapy 54/4 (2020); Drost (see note 32).
[39] Tait et al. (see note 17).
[40] G. Restall, A. Gerlach, K. Valavaara, and A. Phenix, “The Truth and Reconciliation Commission’s Calls to Action: How Will Occupational Therapists Respond?,” Canadian Journal of Occupational Therapy 83/5 (2016); A. Phenix and K. Valavaara, “Reflections on the Truth and Reconciliation Commission: Calls to Action in Occupational Therapy,” Occupational Therapy Now 18/6 (2016).
[41] L. Richardson and A. Boozary, “Truth and Reconciliation in Canada’s Health System,” Lancet 398/10303 (2021).
[42] M. McNally and D. Martin, “First Nations, Inuit and Métis Health: Considerations for Canadian Health Leaders in the Wake of the Truth and Reconciliation Commission of Canada Report,” Healthcare Management Forum 30/2 (2017); C. C. Jacek, K. M. Fritz, M. E. Lizon, and T. L Packham, “Knowledge Gaps Regarding Indigenous Health in Occupational Therapy: A Delphi Process,” Canadian Journal of Occupational Therapy (2022); Tait et al. (see note 17); E. McGibbon, “Truth and Reconciliation: Health Care Organizational Leadership,” Healthcare Management Forum 32/1 (2019).
[43] McNally and Martin (see note 42).
[44] J. Morgan, K. Jameson, S. Joolaee, and A. Ho, “Calls to Action: Truth, Reconciliation, and Indigenous Rights for Supportive Decision-Making in Health Care,” International Journal of Indigenous Health 16/1 (2021); McNally and Martin (see note 42); T. Nguyen, V. W. L Tsang, P. A. Randhawa, et al., “Highlighting Current Needs in Addressing Youth Mental Health in British Columbia,” UBC Medical Journal 10/2 (2019); Jaworsky (see note 37); J. Reading, C. Loppie, and J. O’Neil, “Indigenous Health Systems Governance: From the Royal Commission on Aboriginal Peoples (RCAP) to Truth and Reconciliation Commission (TRC),” International Journal of Health Governance 21/4 (2016).
[45] L. L. Crowshoe, A. Sehgal, S. Montesanti, et al., “The Indigenous Primary Health Care and Policy Research Network: Guiding Innovation within Primary Health Care with Indigenous Peoples in Alberta,” Health Policy 125/6 (2021); Pearce et al. (see note 37).
[46] M. Rand, “Evaluation of the Indigenous Relationship and Cultural Safety Courses among a Sample of Indigenous Services Canada Nurses,” International Journal of Indigenous Health 14/1 (2019).
[47] Fijal and Beagan (see note 17).
[48] Truth and Reconciliation Commission of Canada, Calls to Action (see note 3).
[49] M. E. Morton Ninomiya, B. Tanner, L. J. Peach, et al., “Anishinabek Sources of Strength: Learning from First Nations People Who Have Experienced Mental Health and Substance Use Challenges,” Social Science and Medicine 309 (2022).
[50] Morgan et al. (see note 44).
[51] Hadjipavlou et al. (see note 28).
[52] L. Logan, J. McNairn, S. Wiart et al., “Creating Space for Indigenous Healing Practices in Patient Care Plans,” Canadian Medical Education Journal 11/1 (2020).
[53] Ibid.
[54] Hyman et al. (see note 35).
[55] Ibid.
[56] Kyoon Achan et al. (see note 17).
[57] R. N. Asiniwasis, E. Heck, A. Amir Ali, et al., “Atopic Dermatitis and Skin Infections Are a Poorly Documented Crisis in Canada’s Indigenous Pediatric Population: It’s Time to Start the Conversation,” Pediatric Dermatology 38/Suppl 2 (2021); Morgan et al. (see note 44); Sanzone et al. (see note 32).
[58] Rand (see note 46); Nguyen et al. (see note 44); Gasparelli et al. (see note 38).
[59] Hunter and Pride (see note 17).
[60] Henderson et al. (see note 28); Hadjipavlou et al. (see note 28).
[61] Jaworsky (see note 37).
[62] Drost (see note 32); McGibbon (see note 42); Richardson and Boozary (see note 41); Jacek et al. (see note 42).
[63] Hunter and Pride (see note 17).
[64] K. Williams, M. L. Potestio, and V. Austen-Wiebe, “Indigenous Health: Applying Truth and Reconciliation in Alberta Health Services,” CMAJ 191/Suppl (2019).
[65] Long et al. (see note 18); Pandey et al. (see note 31).
[66] T. Holt, G. Hansen, V. McKinney, and I. Mendez, “Contemplating Remote Presence Technology for Culturally Safe Health Care for Rural Indigenous Children,” AlterNative: An International Journal of Indigenous Peoples 15/1 (2019).
[67] O’Neil et al. (see note 36).
[68] Ibid.
[69] Morton Ninomiya et al. (see note 49); Z. Yu, A. Steenbeek, M. Biderman, et al., “Characteristics of Indigenous Healing Strategies in Canada: A Scoping Review,” JBI Evidence Synthesis 18/12 (2020); Hunter and Pride (see note 17); Williams et al. (see note 64).
[70] Crowshoe et al. (see note 45).
[71] Holt et al. (see note 66); McGibbon (see note 42); Williams et al. (see note 64).
[72] McGibbon (see note 42)
[73] Richardson and Boozary (see note 41).
[74] McGibbon (see note 42).
[75] Ibid.
[76] Ibid.
[77] Henderson et al. (see note 28).
[78] Jaworsky (see note 37).
[79] Logan et al. (see note 52).
[80] N. Redvers and B. Blondin, “Traditional Indigenous Medicine in North America: A Scoping Review,” PLOS ONE 15 (2020).
[81] Logan et al. (see note 52).
[82] Sanzone et al. (see note 32).
[83] K. Gasparelli, B. McKenzie, H. Crowley, et al., “Exploring the Implications of the Truth and Reconciliation Commission: What Is Our Role? Canadian Physiotherapy Association National Congress 2016 May 26-28 Victoria BC,” Physiotherapy Canada 68 (2016); Sovdi and Macdonald (see note 34).
[84] Williams et al. (see note 64).
[85] Fellner et al. (see note 38).
[86] Lachance and Rose (see note 17).
[87] Henderson et al. (see note 28).
[88] Ibid.
[89] McNally and Martin (see note 42).
[90] H. A. Howard, “History, Truth, and Reconciliation in Settler Health Care,” American Anthropologist 122/3 (2020).
[91] McGibbon (see note 42).
[92] N. Redvers, P. Reid, D. Carroll, et al., “Indigenous Determinants of Health: A Unified Call for Progress,” Lancet 402/10395 (2023).
[93] Public Health Agency of Canada, Key Health Inequalities in Canada: A National Portrait (Ottawa: Public Health Agency of Canada, 2018).
[94] Richardson and Boozary (see note 41).