“It’s Not Whatever, Because This Is Where the Problem Starts”: Racialized Strategies of Elimination as Determinants of Health in Palestine
Volume 24/2, December 2022, pp. 237-254 | PDF
Benjamin Bouquet,* Rania Muhareb,* and Rhona Smith
Abstract
In this paper, we examine the social construction of race as a determinant of health inequities in Palestine. Race myths about Palestinians conform to the “logic of elimination” integral to settler colonialism, predicated on the dispossession and removal of the Indigenous people from the land. Racialized legal categorizations of Palestinians are deployed in strategies of elimination that include policies and practices of extrajudicial killing, maiming, and excessive use of force; displacement, dispossession, isolation, and containment; and arbitrary detention and movement restrictions. Differential freedoms and entitlements derive from the deployment of racialized legal categorizations, regulating the material conditions of life and exposure to deliberate bodily harm that make up intermediary determinants of health. Our iterative model outlining the symbolic and systemic constitution of racialized health inequities in Palestine aims to support analysis of the root causes of human rights violations, essential to a human rights-based approach to health. Root-cause analysis confers appropriate recommendations for action. The radical dismantling of systematic racial oppression and domination in Palestine, tantamount to apartheid, is a precondition for realizing the right to health for all.
Introduction
Enjoyment of the right to the highest attainable standard of physical and mental health depends on successfully addressing all conditions of life that determine health and well-being.[1] Systemic racism and apartheid have been declared antithetical to the Constitution of the World Health Organization (WHO) and its commitment to health as a “fundamental right … of every human being without distinction of race, religion, political belief, economic or social condition.”[2]
WHO’s 2010 Conceptual Framework for Action on the Social Determinants of Health identifies racism as a structural determinant of health through its role in constituting socioeconomic position, affecting the material conditions of life as intermediary determinants of health.[3] Legal freedoms and entitlements represent a critical pathway for understanding this process of determination and differentiation. We argue that freedoms and entitlements themselves represent intermediary determinants, centering the obligations of states to realize the right to health for all, in conformance with a human rights-based approach. Similarly, aligning with the duties of states for respect and protection, we emphasize the exposure to deliberate bodily harm as further representing an intermediary determinant of health. This builds on wider efforts to move beyond the context of European welfare states in formulating models for the social determination of health.
We examine the ideological production of race myths within the “logic of elimination” integral to settler colonialism, predicated on the dispossession and removal of the Indigenous Palestinian people from the land.[4] Such race myths inform racialized legal categorizations that are deployed in “strategies of elimination,” including policies and practices of extrajudicial killing, maiming, and excessive use of force; displacement, dispossession, isolation, and containment; and arbitrary detention and restriction of movement.[5] We examine how these categories and strategies affect intermediary determinants of health, outlining an iterative model for understanding race as a determinant of health inequities in Palestine.
For over seven decades, Israel has denied millions of Palestinian refugees and exiles their right to return to their homes, lands, and properties, and prevented exercise of the right to self-determination by the Palestinian people. Through discriminatory laws, policies, and practices, the Israeli state apparatus has instituted a regime of systematic racial oppression and domination over Indigenous Palestinians, which amounts to the crime of apartheid.[6] Accurate assessment of root causes of human rights violations confers appropriate recommendations for action. In 1977, WHO reported to the United Nations (UN) Special Committee against Apartheid that the policies of “apartheid in the health field … are inimical to the letter and spirit of the WHO Constitution.”[7] This assessment remains valid today; it is only through the radical dismantling of systems of racial oppression and domination that we can achieve the right to health for all.
Health inequities and race as a structural determinant of health
Health inequities are “differences in health status or in the distribution of health resources between different population groups, arising from the social conditions in which people are born, grow, live, work and age.”[8] In 2020, the life expectancy for Israeli Jewish women (85.1 years) was 3.2 years higher than for Palestinian women with Israeli citizenship (81.9), 9.5 years higher than for Palestinian women in the West Bank (75.6), and 10.3 years higher than for Palestinian women in the Gaza Strip (74.8).[9] There are similar observable differences for men, for other health outcome measures (such as infant, child, and maternal mortality), and for indicators of health system capacities.[10] At their root, health inequities are fundamentally unjust; tackling them requires analyzing the mechanisms of their social production.
In a report published in 2010, the WHO Commission on Social Determinants of Health (CSDH) identifies racism as a determinant of health inequities, or a structural determinant of health.[11] According to Orielle Solar and Alec Irwin, who authored the report, structural determinants are those that produce social stratification within a “socioeconomic and political context” (encompassing governance, macroeconomic policies, social policies, public policies, and culture and societal values). These are manifested in social hierarchies by “structural stratifiers” that include “Income, Education, Occupation, Social Class, Gender, Race/ethnicity.”[12] The authors posit that intermediary determinants “constitute … the primary mechanism through which socioeconomic position generates health inequities.”[13] They propose that intermediary determinants include “material circumstances, such as neighborhood, working and housing conditions; [sic] psychosocial circumstances, and also behavioral and biological factors,” as well as access to health care.[14]
Pointing to the intrinsic link between the production of race and inequitable health outcomes, Ruth Wilson Gilmore defines racism itself as “the state-sanctioned and/or extra-legal production and exploitation of group-differentiated vulnerability to premature death.”[15] Frantz Fanon further emphasizes the primacy of race for understanding social stratification in colonial contexts: “It is neither the act of owning factories, nor estates, nor a bank balance which distinguishes the governing classes. The governing race is first and foremost those who come from elsewhere, those who are unlike the original inhabitants, ‘the others’.”[16] Zachary Lockman, meanwhile, challenges the distinction of colonialism and capitalism—where the latter is “as much about slavery as it is about wage labor, as much about plantations and shipyards as it is about factories, and as much about the Caribbean and Brazil as it is about England.”[17] The categories of class and race outlined in the CSDH model, therefore, must be understood as intersecting. These categories not only determine the material circumstances of life, principally through group-defined “interests with regard to indigenous people’s land and labor,” but are determined by those material circumstances, which are the product of “the formative historical processes of class, identity and state.”[18]
Chandra Ford and Collins Airhihenbuwa have argued for the application of critical race theory within public health, which includes antiracism praxis “that builds on community-based participatory approaches linking research, practice, and communities.”[19] Anticolonial and subaltern approaches align with the focus in critical race theory of “centering in the margins,” where the social determination of the health-disease-care process, for example, “recognize[s] the dialectics of dominance/subalternity and visibility/invisibility in the global agenda for health equity … [and] the need to intertwine processes of transformation on ontological, epistemological and praxiological level[s].”[20]
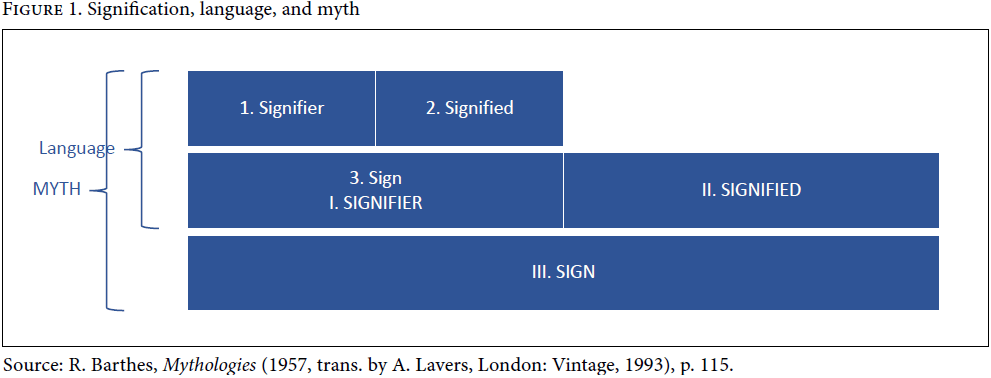
Critical race theory further emphasizes the contingent nature of race categories as they are socially constituted in historical and political context.[21] Stuart Hall, in his explanations of decoding cultural representation based on the work of French structuralists and semiologists Ferdinand de Saussure and Roland Barthes, outlines how race labels operate at the levels of language (denotation) and myth (connotation).[22] While denotation “is the simple, basic, descriptive level,” connotation connects race labels “to broader themes and meanings, linking them with what we may call the wider semantic fields of our culture” (Figure 1).[23] In short, race myths are the broader social value(s) attached to race labels. Hence, Edward Said describes the production of a myth of the “Orient” in the context of European colonialism, where “the Oriental is irrational, depraved (fallen), childlike, ‘different’; thus the European is rational, virtuous, mature, ‘normal’.”[24] Such race myths are simultaneously structured by utterance in language and structuring of language, determining the “always-already” framework through which we view and construct the world symbolically.[25]
Conceptualizing how race determines health inequities requires elaboration beyond the CSDH model to examine the construction of race categories in context and their deployment in laws, policies, and practices. This distinction of construction and deployment aligns with Slavoj Žižek’s subcategorization of objective violence as comprising symbolic and systemic forms.[26] The symbolic production of race labels and myths toward an end of domination through exploitation or elimination is necessarily a form of violence. Meanwhile, the observable deployment of race labels—or their manifestation within—laws, policies, and practices constitutes systemic violence. The following sections examine these processes, before outlining an iterative model for conceptualizing race as a structural determinant of health in Palestine.
Symbolic violence: Constructing race myths in Palestine within a logic of elimination
Settler colonialism has been described as a “structure rather than an event,” where “a settler society is always, in Derridean terms, a society “to come,” characterized by the promise rather than the practice of a truly “settled” lifestyle.”[27] Through its “logic of elimination,” settler colonialism primarily seeks the removal and replacement of the Indigenous people living on the land.[28] The settler colonial process employs racialization as an instrument of dispossession and domination.[29] The connotations attached to race signifiers within settler colonial discourse thus conform to this logic.
Pierre Bourdieu, in describing “division of the labour of domination,” distinguishes ideology that deploys symbols as instruments of domination and ideological power that derives from the “specific contribution of symbolic violence (orthodoxy) to political violence (domination).”[30] Similarly, Said argues that the production of a discourse on the Orient, and the ideological power invested in this, is based on its relationship with political (“as with a colonial or imperial establishment”), intellectual, cultural (“as with orthodoxies and canons of tastes, texts, values”), and moral forms of power.[31]
When Golda Meir (born Golda Mabovitch in Kyiv, Ukraine) claimed in an interview in 1970 to be Palestinian¾at the time she was prime minister of Israel¾she provided a demonstration of this eliminatory logic as manifested in the ideological production of race myths. She elaborated on the statement in an op-ed in 1974: “‘There is no Palestinian people. There are Palestinian refugees.’ … When in 1921 I came to Palestine¾until the end of World War I a barren, sparsely inhabited Turkish province¾we, the Jewish pioneers, were the avowed Palestinians.”[32] Meir ties the label of Palestinian directly to the settler colonial myth of a “barren” land or terra nullius (the myth of “a land without people for a people without land”).[33] In her 1970 interview, she simultaneously emphasized the label of Arab to discredit claims to self-determination and land rights by non-Jewish Palestinians who had lived in Palestine before 1948:
Without Israel in this area there won’t be peace. The Arabs are not so friendly with each other … Well this is a solution. It just so happens that there are 14 Arab countries and immense territories … We’ve come back. We’ve been here before … What did we take away from the Arabs when we came back? We didn’t want to live with them in peace. We asked them to leave … What difference is there between Arabs who are on this side of the Jordan and the other side of the Jordan?[34]
The race myths attached here to the label of Arab justify the attempts to eliminate Indigenous Palestinians. According to Meir, Arabs are violent (“not so friendly”) and the Indigenous belonging of Arabs is not applicable within, or at least confined to, the borders of Palestine (“there are 14 Arab countries and immense territories”). Meanwhile, she depicts the Zionist militias that forcibly removed (non-Jewish) Palestinians from their homes as civilized and reasonable in opposition to Oriental irrationality (“We asked them to leave”) and as rightful custodians of the land (“We’ve been here before”). Lorenzo Veracini, in examining settler colonial transferrist approaches, refers to the latter as “Narrative Transfer (IV): when ‘settlers are also indigenous peoples’ claims are made.”[35] Meanwhile, Meir’s portrayal of Palestinians as non-Indigenous is based on the previous existence of a spatial reality for Palestinians that transcended the borders put in place under British colonial rule. This myth of Indigenous non-indigeneity Veracini calls “transfer by conceptual displacement.”[36] Hence, race as a structural determinant of health depends not only on the systems that employ race categories in the exploitation or attempted elimination of one racial group by another, but also on the race myths that ideologically justify domination.
Systemic violence: Race categories in Israeli law
In 2018, the Israeli parliament (the Knesset) adopted the so-called Basic Law: Israel as the Nation-State of the Jewish People. Besides rejecting the right of the Palestinian people to self-determination, the basic law declared in article 7 “the development of Jewish settlement as a national value” to be encouraged, promoted, and consolidated by the state.[37] That the construction of Jewish settlements, on either side of the Green Line (1949 Armistice Agreements line), is premised on racial exclusiveness and racial supremacy was clear to Palestinian scholars already prior to the start of the Israeli military occupation in 1967.[38] Additionally, it was understood that the Jewish nation-state basic law only crystallized Palestinian oppression since at least 1948.
Indeed, Israeli law and Zionist policy institutionalized in 1948 and thereafter systematically privilege persons categorized as “Jewish,” while excluding and subordinating the Indigenous Palestinian people as “non-Jewish.” Zionist ideology and doctrine is particularly visible in the 1950 so-called Law of Return and the 1952 Citizenship Law, which allow “every Jew … to settle in Israel” and to automatically receive Israeli citizenship.[39] In contrast to the privileges accorded to Jewish settlers under Israeli law, Palestinians, including citizens of the settler colony, face systematic oppression, from the state’s denial of Palestinians’ right of return to the appropriation of their land and property under the 1950 Absentee Property Law. The Absentee Property Law is applied not only to Palestinian refugees and exiles abroad but also to those Palestinians remaining inside the Green Line. For the latter, Israeli authorities created the Orwellian category of Palestinian “present absentees,” whose predicament reflects the overarching race myth of Palestinian transience according to Zionist ideology.
Areej Sabbagh-Khoury highlights Indigenous citizenship in settler colonial states as “premised on the process of dispossession.”[40] She describes the Absentee Property Law as among the “primary mechanisms of legalized dispossession” for Palestinians within Israeli settler colonialism.[41] Palestinians who became internally displaced and receive Israeli citizenship, like Palestinian refugees in exile, have been prevented from returning to their homes and lands since 1948. As Sabbagh-Khoury writes, “Despite having remained in their homeland, Israeli law considered [internally displaced Palestinians] ‘present-absentees’—that is, present for political purposes and absent for property purposes”—in order to dispossess them.[42]
Following the occupation and annexation of East Jerusalem in 1967, Palestinian refugees in the city became effectively “present” and able to access the properties they had lost, but they were still denied the right to return to their homes. The Baramki home, situated at the frontier between West and East Jerusalem, is a case in point; Thomas Abowd exposed the absurdity of Israeli legal categorizations of Palestinians in his recollection of his father’s attempt to regain his home in 1967:
Imagine, my father at the time, a 70-year-old person going to the Israelis and telling them “here I am now and I want my property” and them telling him that, no, you are an “absentee”. And he said, “How am I absent? I am present!” He could not understand how he was absent and present at the same time![43]
Deriving from the fundamental distinction of “Jewish” versus “non-Jewish” under Israeli law are racialized categories of Palestinians according to the legal status imposed on them by the Israeli regime, whether as citizens, residents of the occupied Palestinian territory since 1967, or refugees and exiles. According to a 2017 report authored by Richard Falk and Virginia Tilley for the UN Economic and Social Commission for Western Asia, Israel’s policy of “strategic fragmentation” of the Palestinian people is a main tool of apartheid.[44] The report identifies four domains of Israeli control, reflecting Israel’s racialized legal categorizations of Palestinians: (1) Israeli civil law applicable to Palestinians with Israeli citizenship; (2) Israel’s permanent residency regime imposed on Palestinians in occupied East Jerusalem; (3) Israeli military law applied in the occupied West Bank and Gaza Strip, and associated identity cards entailing varying degrees of freedoms and entitlements; and (4) Israel’s policy since 1948 to deny Palestinian refugees and exiles their right of return, thus prolonging their unlawful displacement and dispossession.[45]
Implemented according to an openly racist logic that describes Palestinians as a demographic “threat,” the legal, political, social, and geographical fragmentation of the Palestinian people operates as an overarching strategy of elimination within Zionist settler colonial discourse and logic.[46] Resisting fragmentation, the Manifesto of Dignity and Hope of the May 2021 Unity Intifada (uprising) reaffirmed the unity of the Palestinian people in the face of the Zionist attempt at “isolating us and separating us in small strips of our land,” stressing that this “is how they worked to fragment our political will, and to prevent a united struggle in the face of racist settler colonialism in all of Palestine.”[47]
Strategies of elimination as pathways for determining health inequities in Palestine
Israel’s logic of “absenting” Palestinians is implemented through strategies of elimination that deploy racialized legal categorizations. In this section, we outline some of the pathways by which these strategies affect recognized intermediary determinants of health in the production of health inequities. Intermediary determinants comprise material conditions, such as access to housing, employment, and health care, as well as exposure to deliberate bodily harm. These determinants are closely regulated by legal freedoms and entitlements. Explicit mention of legal freedoms and entitlements has been mostly absent in models of social determinants of health derived from the context of European welfare states, where the principle of equality before the law—with the exception of migrants and refugees—is largely taken for granted.[48] Incorporation of freedoms and entitlements as intermediary determinants also centers the responsibilities of states, in line with a human rights-based approach to health. The purpose of this section is to explore the link between racialized legal categorizations and established intermediary determinants of health, rather than to reiterate the empirical foundation of intermediary determinants, as the basis for understanding the mechanisms by which race operates as a structural determinant of health in Palestine.
Extrajudicial killing, maiming, and excessive use of force
One of the clearest strategies of elimination with direct consequences for health is Israel’s systematic use of lethal force against Palestinians, a constant since the founding violence of the Nakba. In 2021 alone, 337 Palestinians were killed and 19,171 were injured by the Israeli occupying forces and settlers, including 1,229 non-fatal injuries from live ammunition and 1,630 from air-launched explosive weapons.[49] The trend of extrajudicial killing and maiming has continued in 2022, with 120 occupation-related fatalities of Palestinians and 7,621 injuries as of September 11.[50]
Between March 30, 2018, and the end of 2019, the Israeli occupying forces systematically shot to kill, injure, and maim Palestinian civilians protesting as part of the Great March of Return demonstrations against the illegal closure and blockade of the Gaza Strip and calling for the realization of their right of return.[51] Over 36,100 Palestinians, including nearly 8,800 children and 842 health workers, were injured, including one in five injured by live ammunition; a significant proportion of these injuries have led to permanent disabilities.[52]
International human rights law enshrines the right to security of person and freedom from arbitrary deprivation of life.[53] The use of force, particularly lethal force, in law enforcement situations, including the policing of peaceful assemblies by Israeli occupying authorities, is permissible only in order to protect life.[54] In 2019, the UN Commission of Inquiry on the Great March of Return demonstrations “found reasonable grounds to believe that Israeli snipers shot at journalists, health workers, children and persons with disabilities, knowing they were clearly recognizable as such.”[55] The commission called on Israel, the occupying power, to revise its rules of engagement for the use of live fire and to bring these in line with its international human rights law obligations.[56] Yet, as found by the latest UN investigatory body on Palestine, this call and all recommendations for accountability remain unimplemented to date.[57]
According to the ongoing UN Commission of Inquiry, this repeated failure to implement international recommendations lies “at the heart of the systematic recurrence of violations in both the Occupied Palestinian Territory, including East Jerusalem, and Israel.”[58] Within the Israeli legal system, there is impunity for the use of excessive force against Palestinians.[59] In May 2022, the extrajudicial execution of Palestinian journalist Shireen Abu Akleh by Israeli occupying forces in Jenin drew international outrage and condemnation. Yet, even for such a high-profile case involving a renowned Palestinian journalist, who was also a US citizen, over five months since her deliberate killing, no Israeli soldier has been held accountable.[60] As observed by Saleh Hijazi, formerly of Amnesty International, Abu Akleh’s killing “unfortunately … is not unique … It fits a pattern, a pattern of unlawful killing, and also a pattern of targeting journalists and human rights defenders.”[61]
Displacement, dispossession, isolation, and containment
The mass displacement and dispossession of Palestinians, of whom 67% worldwide are refugees, including 812,000 Palestinians internally displaced, has profound implications for intermediary determinants of health—including access to livelihoods, housing, a healthy environment, clean water, sanitation, and nutritious food.[62] Refugees have greater health needs and vulnerabilities, face additional barriers to accessing health care (depending on the degree of social protection afforded to them by host countries), and are disproportionately affected by population-level health risks or emergencies, such as the COVID-19 pandemic.[63] Within Palestine, infant mortality for children born in refugee camps in the West Bank and Gaza Strip was nearly 50% higher in 2019 to 2020 compared to Palestinian non-refugees in the same area (17 versus 12 per 1,000 live births).[64] Meanwhile, Palestinian refugees in Lebanon were three times more likely than the general Lebanese population to die from COVID-19.[65]
Centering the role of states in the protection of refugee rights, including property rights, under international law and domestic law of host countries and countries of origin, is essential to upholding a human rights-based approach in understanding the relationship between structural and intermediary determinants of health for refugees. The UN Conciliation Commission for Palestine was established in 1948 “to facilitate the repatriation, resettlement and economic and social rehabilitation of the refugees and the payment of compensation.”[66] In its early years, the commission “attempted to protect and promote the restitution of [Palestinian] refugee properties,” including calling for “the abrogation of Israel’s 1950 Absentees’ Property Law … [and] the suspension of all measures of requisition and occupation of Arab houses.”[67] Today, however, the commission’s role is “no more than functionary¾a symbol of international responsibility to the refugees, and a sad reminder of unfulfilled commitments.”[68] The UN Relief and Works Agency for Palestine Refugees in the Near East assumes the dominant role in support to Palestinian refugees, though it is a temporary agency whose mandate is “to provide assistance and protection to Palestine refugees pending a just and lasting solution to their plight.”[69] Even at the level of social protection, Palestinian refugees face constant precarity, demonstrated from January 2018, when the agency—heavily dependent on voluntary contributions—encountered “the greatest financial predicament in its history” following a US funding cut of US$300 million. The cut jeopardized the provision of essential primary health care for 3 million patients, as well as food assistance to 1.7 million and education services for 525,000 students.[70]
Forced displacement and dispossession of Palestinians remains ongoing on either side of the Green Line. From 2009 to June 2022, Israel demolished over 8,475 Palestinian structures in the West Bank, resulting in the displacement of over 12,500 Palestinians.[71] Four-fifths (78%) of demolitions were in Area C, the 60% of the West Bank largely slated for illegal Israeli settlement construction and expansion. Israel’s discriminatory zoning and planning policies prevent development for Palestinians living in Area C, while hundreds of illegal Israeli settlements are built each year, ranging from 350 in 1973 to 7,750 in 1991.[72] Palestinian communities, such as Masafer Yatta in the south Hebron hills, currently face mass expulsion orders by the Israeli occupying authorities.[73] A decision by the Israeli Supreme Court on May 4, 2022, to reject a community petition affects over 1,000 Palestinians in 12 villages who face imminent forcible transfer.[74] In addition to the psychological effects of impending displacement and dispossession, discriminatory planning policies and a lack of social protection prevent the establishment of quality housing. Palestinian families in Masafer Yatta mostly live in ramshackle structures and caves covered with corrugated iron and tarpaulin. The communities do not have piped water, mains electricity, or a fixed health facility, relying on expensive tanked water, generators, and mobile health clinics that confront funding shortages and inadequate supplies.
Israel’s ongoing project to displace and dispossess Palestinians has also been accompanied by policies of containment in densely populated areas. These areas encompass the 27 refugee camps run by the UN Relief and Works Agency in the occupied Palestinian territory, while the Gaza Strip and Palestinian urban centers designated Areas A and B in the West Bank have become Bantustans according to the demographic logic of excluding Palestinians from most of the land of historic Palestine. In October 2022, approximately 130,000 Palestinians in the Shu’fat refugee camp and Anata neighborhood of Jerusalem were placed under siege by the Israeli occupying authorities for over four days, prevented from accessing their places of employment, schools, and health care as a form of collective punishment, in violation of article 33 of the Fourth Geneva Convention.[75] Residents were denied exit to access health care, including to reach chemotherapy, to receive regular dialysis treatment, to give birth in hospital, and to receive emergency care for acute chest pain, acute abdominal pain, and following injury.[76]
Palestinian citizens of Israel experience similar policies of confinement as Palestinians in East Jerusalem, with the vast majority living in municipalities with a jurisdiction of less than 3% of the land, while making up one-fifth of the Israeli population.[77] In East Jerusalem, Israel has permitted intense, deregulated Palestinian development within the areas of Kufr Aqab and Shu’fat refugee camp behind the Wall. These neighborhoods are characterized by overcrowding, absence of coordinated planning, under-provision of services, poor housing, slack building regulations, and lawlessness.[78] The extent of population containment has been multiplied by the requirement of Palestinians with East Jerusalem residency to demonstrate a continued “center of life” in Jerusalem. Palestinian neighborhoods behind the Wall but within the Israeli municipality of Jerusalem currently provide an affordable way to maintain residency rights in the city, where 75% of Palestinian families live below the poverty line, compared to 22% of Jewish Israeli families.[79]
The entitlements attached to East Jerusalem residency, including movement into the city and across the Green Line without Israeli-issued permits, access to Israeli health insurance, and other forms of social security, create a perverse incentive to seek lower-quality accommodation in overcrowded areas, despite the negative health consequences associated with limited access to green space, playgrounds, municipal facilities, and essential health care services.[80] In addition to the requirement for Palestinians to maintain their “center of life” in Jerusalem, Israel has adopted growing criteria for the revocation of Jerusalem residency status under Israeli law, including as a punitive measure to target the work of Palestinian human rights defenders.[81] The overall objective is to remove Palestinians from Jerusalem in line with the municipality’s target of a Jewish demographic majority in the city.[82]
Additionally, the “silent violence” of Israel’s denial of Palestinian family unification across its domains of control has been fundamental to an overall policy of fragmenting the Indigenous people.[83] The policy was reenacted by the Israeli parliament on March 10, 2022, with the renewal of the racist Citizenship and Entry into Israel Law (Temporary Order).[84] Fragmentation of the Palestinian people operates as an overarching strategy of elimination and denial of self-determination.
Movement restrictions and incarceration
Racist policies of population containment have further been accompanied by a regime controlling Palestinian movement in the West Bank and Gaza Strip since 1967 and in continuity with the military rule imposed on Palestinian citizens inside the Green Line between 1948 and 1966. Alina Korn notes the applicability of Loïc Wacquant’s analysis of the “deadly symbiosis” of the “hyperghetto and prison” to existing strategies of domination over the Palestinian people.[85] Wacquant argues that currently in the United States, race is fundamentally constituted through policies of mass incarceration and hyper-ghettoization that have served the dominant labor and economic model there since the 1960s, productive of social types combining welfare recipient and criminal.[86] Palestinian citizens of Israel and Palestinian residents of Jerusalem fulfill a parallel role of fixed surplus labor within an overall subordinate position in the Israeli labor market, though without requiring Israeli-issued permits. According to annual incarceration rates, between 1949 and 2001, Palestinian citizens inside the Green Line were also between 2.0 and 8.2 times more likely to be incarcerated than Jewish Israelis.[87]
For Palestinians in the West Bank (excluding those with East Jerusalem residency) and the Gaza Strip, access to the Israeli labor market is controlled by Israel’s permit regime. In the years following 1967, up to the 1980s, Israel pursued a policy of economic integration that included relatively open Palestinian access to the Israeli labor market from the West Bank and Gaza Strip.[88] From 1980 to 1987, 45% of working Palestinians from the Gaza Strip and 32% from the West Bank were employed in Israel.[89] After the first Intifada and associated closures, the percentage of Palestinians employed in Israel dropped substantially.[90] At the same time, Israel enabled the entry of workers from overseas¾particularly Southeast Asia and Eastern Europe¾to replace dependence on the Palestinian workforce.[91]
After the start of the second Intifada, between 2001 and 2005, just 2% of working Palestinians in the Gaza Strip and 14% in the West Bank were employed in Israel.[92] Since the blockade of the Gaza Strip in 2007, according to data reported by the UN Office for the Coordination of Humanitarian Affairs, the number of crossings for “Palestinian traders”-largely Palestinians seeking informal employment in Israel-to access the Israeli labor market ranged from 31 in 2009 to 125,683 in 2019.[93] Exclusion from the Israeli labor market combined with severe constraint on the Gaza economy under blockade can be seen as a transition from the model of fixed surplus labor of the hyperghetto to one of fixed surplus population in the “mega-prison.”[94] By 2020, in the context of the ongoing COVID-19 pandemic, 46.6% of Gaza’s population was unemployed, with higher rates among young people and women.[95] In the West Bank in the same year, one in eight Palestinians was employed in Israel or Israeli settlements, while 43% were employed in informal sectors.[96] In addition to landlessness and unemployment, employment precariousness produces “fear, uncertainty and disruption” that contribute to and are associated with negative physical and mental health.[97]
Meanwhile, Israel’s permit regime systematically restricts Palestinian access to health care as an intermediary determinant of health. Movement limitations fundamentally hinder the Palestinian economy, affecting revenues for public health care and exacerbating barriers to ensuring adequate health care provision and financial protections for the population.[98] Wide variation in the approval rate for patient permits and inconsistent outcomes for individual successive applications demonstrate the arbitrariness of restrictions on health access. For the Gaza Strip, the approval rate for patient permits has ranged from 94% in 2012 to 54% in 2017.[99] Unpredictability of the process creates uncertainty and stress, while Palestinian children are frequently separated from their parents when traveling to reach health care. From 2018 to 2021, 43% of patient permits for children were approved without the accompaniment of a parent companion.[100] The permit regime impacts patient mortality: cancer patients referred for chemotherapy or radiotherapy from 2015 to 2017 were 1.45 times less likely to survive in the coming months and years if they were initially delayed or denied a permit to exit the Gaza Strip.[101] The death of individual patients can also be attributed to the non-approval of permits. In March 2022, 19-month-old Fatma Al-Misri from Khan Younis in the Gaza Strip died from complications of an atrial septal defect (ASD) after being issued repeated appointments for surgery at Makassed Hospital in East Jerusalem since December 2021.[102] The surgery she needed has very high rates of success. As the Norton Children’s Heart Institute explains to parents of children undergoing the procedure, “In more than 99[%] of cases, patients have no complications after an ASD repair … Most children have no difficulty with physical activity or restrictions after ASD repair.”[103] For cases such as Fatma, the denial of access to health care not only violates Palestinians’ right to health but amounts to the arbitrary deprivation of life.[104]
Iterative model for race as a structural determinant of health in Palestine
In Figure 2, we propose an iterative model for race as a structural determinant of health in Palestine. The ideological production of race myths associated with constructed race labels constitutes symbolic violence and forms the basis of racialized legal categories deployed in discriminatory laws, policies, and practices that represent systemic violence.
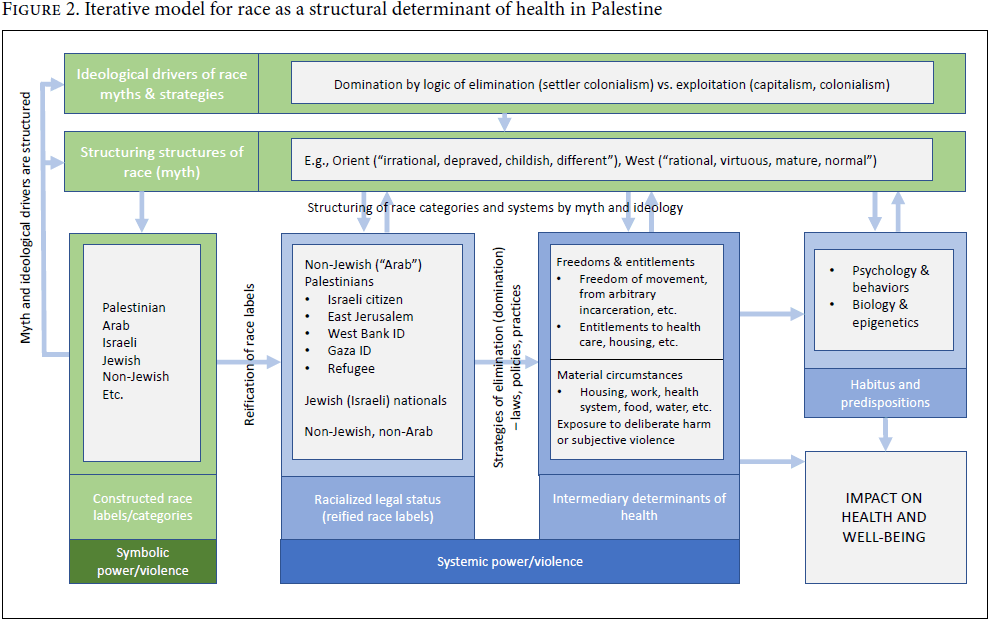
Intermediary determinants of health—that are also the “downstream” focus of social policies—encompass material living conditions that are demonstrably associated with better or poorer health outcomes.[105] We extend the category to include exposure to harm or violence, while also incorporating freedoms and entitlements in law as measurable or deducible intermediary health determinants, in line with a human rights-based approach. For conceptual clarity, we have separated individual-level measures such as psychology, behaviors, biology, and epigenetics. These are themselves affected by social conditions, where habitus is the “set of dispositions which incline agents to act and react in certain ways” or the “pre-reflexive” embodiment of our social conditioning—the way that we have been ourselves structured by the “structuring structures” of our social surroundings.[106]
The crime of apartheid and the Palestinian right to health
In 1970, two years before his assassination by Mossad in Beirut, Ghassan Kanafani gave an interview to Australian journalist Richard Carleton, which has since been widely shared.[107] Discussing the Palestinian struggle, Kanafani said to Carleton, “It’s not a conflict. It’s a liberation movement fighting for justice.” “Well, whatever it might be best called,” Carleton responded. Pointing to the importance of language not only as a tool of domination but as instrument for “knowing and constructing” the world and resisting oppression, Kanafani said:
It’s not whatever, because this is where the problem starts … This is a people who is discriminated [against] … fighting for [their] rights. If you will say it’s a civil war, then your questions will be as justified. If you will say it’s a conflict, then of course it’s a surprise to know what’s happening.[108]
Our accurate “knowing and constructing” of systems of domination depends on “the production and validation of knowledges anchored in the experiences of resistance of all social groups that have been systematically victims of injustice, oppression and destruction caused by capitalism, colonialism and patriarchy.”[109]
For decades, Palestinian scholars have characterized Israel’s settler colonial project as inherently racial.[110] Already in 1965, Fayez Sayegh theorized Zionist colonialism as amounting to apartheid.[111] Sayegh showed that “Zionist racial discrimination is written into the fundamental laws of Israel [whereby] the Jew has privileges which the non-Jew, the indigenous Palestinian Arab, does not have.”[112] During the following decade, Sayegh’s advocacy would lead to the adoption of Resolution 3379 by the UN General Assembly in 1975, recognizing Zionism as a form of racism and racial discrimination. While this resolution was revoked over a decade later as a condition for Israel’s participation in the 1991 Madrid Peace Conference, it was never challenged on the merits and reflects decades of Palestinian intellectual contributions to understanding the nature of Zionist settler colonialism.[113]
In 2009, a detailed study applying the crime of apartheid to the experience of the Palestinian people under occupation was published by the Human Sciences Research Council of South Africa, with contributions from Palestinian human rights organizations Al-Haq and Adalah.[114] Additionally, in 2007, 2012, and 2019, following Palestinian-led civil society engagement, the UN Committee on the Elimination of Racial Discrimination issued concluding observations finding that Israeli policies and practices are inconsistent with article 3 of the International Convention on the Elimination of All Forms of Racial Discrimination, in which states “particularly condemn racial segregation and apartheid and undertake to prevent, prohibit and eradicate all practices of this nature in territories under their jurisdiction.”[115] This work has been linked in praxis with antiracist mobilizing, including grassroots engagement with the 2001 Durban World Conference against Racism, during which the nongovernmental organization forum recognized Israel’s “brand of apartheid”; the launch of the Stop the Wall Campaign in 2002; and the issuance in 2005 by a broad Palestinian civil society coalition of a call to boycott, divest from, and issue sanctions against Israel, in an effort to end Israel’s regime of occupation, colonialism, and apartheid.[116]
Building on the analysis and mobilization by Palestinian civil society on the root causes of Palestinian oppression, recent years have seen Israeli and international human rights organizations, including Human Rights Watch and Amnesty International, publish reports concluding that Israeli policies and practices targeting the Palestinian people constitute the crime of apartheid.[117] As a specific form of colonial race domination, the crime of apartheid is prohibited as an egregious form of racial discrimination and a crime against humanity under international law.[118] Article II of the 1973 International Convention on the Suppression and Punishment of the Crime of Apartheid lists a range of inhuman acts that, if “committed for the purpose of establishing and maintaining domination by one racial group of persons over any other racial group of persons and systematically oppressing them,” constitute the crime of apartheid. These include, among others, denial of the right to life; arbitrary detention; denial of the rights to work and education; denying the right to return to one’s country; restricting freedom of movement and residence; violating the right to freedom of opinion and expression; the “expropriation of landed property”; and the persecution of individuals and organizations “because they oppose apartheid.”[119] In 2020, in the context of the ongoing COVID-19 pandemic, the health implications of Israeli apartheid became more starkly evident.[120] Israel’s discriminatory response to the outbreak resulted in vast inequities in the distribution of vaccines to some five million Palestinians under Israeli occupation, which led commentators to describe the situation as one of “medical apartheid.”[121]
That apartheid is incompatible with the realization of the right to health has long been emphasized by the global health community, including in the 1981 Brazzaville Declaration. Adopted at the International Conference on Apartheid and Health hosted by WHO, the declaration asserts that apartheid and health are mutually exclusive and that “policies of apartheid are inimical to, and irreconcilable with, the social target of governments and of WHO of health for all.”[122] From the 1960s until the formal dismantling of the South African apartheid regime in the 1990s, the World Health Assembly consistently condemned the impacts of apartheid on health, asserting the assembly’s “clear and uncompromising stand on the elimination of apartheid.”[123] Apartheid was also deemed a total barrier to radical improvements in mental health provision.[124] In 1977, WHO noted that apartheid was inconsistent with the WHO Constitution, as it involved “almost total control over the lives of men and women through legislation based on racial distinctions. For the individual, the simple fact of his or her racial categorization as defined on an official identity card determines every aspect of life from cradle to grave.”[125]
Similarly, WHO identified key apartheid policies as sources of psychosocial stress for black South Africans at the time.[126] These included policies of “forced mass uprooting” and Bantustanization; the “forced splitting of families,” declaring black South Africans “aliens in their own country”; economic deprivation, poverty, and an inferior legal status; harassment and insecurity (“The literally hundreds of laws to which the African is subjected … result[ing] in a society in which law infringement is the inevitable rule and police harassment or repression a constant feature of everyday life”); and outlawing political and social activity, including “indeterminate detention without trial.”[127] All of these practices are starkly mirrored in the racial oppression imposed on Palestinians today by the Israeli regime.
Drawing on Palestinian scholars’, civil society’s, and activists’ engagement with the apartheid framework for several decades, this paper considers anti-apartheid from a decolonial perspective that seeks to center Palestinian indigeneity.[128] In recognizing the context of Israeli apartheid as one of settler colonialism, this approach rejects “liberal equality” approaches to Israeli apartheid, which have notably been critiqued by Palestinian scholar Lana Tatour.[129] These misleadingly suggest that legal and other “reforms” are sufficient to dismantle Israeli apartheid.[130] In addressing not only Israeli apartheid but also its broader context of Zionist settler colonialism, our approach subscribes to the practice of WHO during the anti-apartheid era in South Africa and occupied Namibia, with its insistence that only the complete dismantling of apartheid and the system of domination can secure health for all.
Conclusion
In this paper, we have proposed an iterative model for race as a structural determinant of health in Palestine, to support root-cause analysis of racialized health inequities in line with a human rights-based approach to health. Race myths of Palestinians produced within Zionist discourse represent symbolic violence, conforming to a “logic of elimination” and the ideological objectives of settler colonialism toward the removal of the Indigenous people. The translation of race myths and labels into racialized legal categories further constitutes systemic violence, where the differentiation of legal freedoms and entitlements along race lines is a principal pathway for understanding the regulation of intermediary determinants of health and the constitution (and reconstitution) of differential health outcomes across different domains of Israeli control.
Enjoyment of the right to the highest attainable standard of health requires the improvement of all conditions of life that determine health, “without distinction of race, religion, political belief, economic or social condition.”[131] In Palestine, the “right to a system of health protection which provides equality of opportunity for people to enjoy the highest attainable level of health” demands the complete eradication of the logics and structures of systematic racial oppression and domination, manifested in racialized strategies of elimination.[132] As this paper has advanced, these strategies include policies and practices of extrajudicial killing, maiming, and excessive use of force; displacement, dispossession, isolation, and containment; and arbitrary detention and restriction of movement.
Throughout this discussion, we have been reminded of WHO’s critical work during the 1970s and 1980s in exposing the detrimental health impacts of apartheid.[133] The 1981 Brazzaville Declaration on apartheid and health was clear that to redress health inequities in South Africa at the time, the total elimination of apartheid was an essential precondition, insisting that “it is impossible to speak of health in the absence of political rights, self-determination and acceptance of the principles of social justice as imperative for society as a whole.”[134] These words remain instructive and remind us that we cannot speak of Palestinian health in the absence of discussion on political rights and self-determination for the Palestinian people as a whole.
Closing his address to the Brazzaville conference, the then WHO director-general Halfdan Mahler insisted that “change … is inevitable, if not imminent … By change, I mean the radical dismantling of the system based on apartheid and racial discrimination.”[135] For Palestinians, any positive improvement toward the fulfillment of the right to health is predicated on the radical dismantling of Zionist settler colonialism, its effort to remove the Indigenous Palestinian people from the land, and the systematic manifestation of this objective in the deployment of racialized legal categories that amounts to apartheid. Toward this end, third states must adopt effective, coercive measures, and address the root causes of racialized strategies of elimination as determinants of health in Palestine.
Disclaimer
The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Benjamin Bouquet, MA Cantab, MBBS, MPH, MFPH, is a PhD candidate in health and human rights at the Population Health Sciences Institute and School of Law at Newcastle University, Newcastle, United Kingdom.
Rania Muhareb, BA, LLM, is an Irish Research Council and Hardiman PhD scholar at the Irish Centre for Human Rights in the School of Law, University of Galway, Ireland.
Rhona Smith, LLB(Hons), PhD, LLM, MA, is a professor of international human rights at the School of Law at Newcastle University, Newcastle, United Kingdom.
*Both authors contributed equally to this manuscript as first authors.
Please address correspondence to Benjamin Bouquet. Email: benbouquet@gmail.com.
Competing interests: None declared.
Copyright © 2022 Bouquet, Muhareb, and Smith. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction.
References
[1] Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000), paras. 3–4.
[2] Constitution of the World Health Organization (1946).
[3] O. Solar and A. Irwin, “A Conceptual Framework for Action on the Social Determinants of Health,” Discussion Paper 2 (Geneva: World Health Organization, 2010).
[4] M. Foucault, Archaeology of Knowledge and the Discourse on Language (1972, trans. A. M. Sheridan Smith), p. 49; P. Wolfe, “Settler Colonialism and the Elimination of the Native,” Journal of Genocide Research 8/4 (2006).
[5] Wolfe (see note 4).
[6] F. Sayegh, “Zionism: A Form of Racism and Racial Discrimination,” in A. W. Al Kayyali (ed), Zionism, Imperialism and Racism (London: Croom Helm, 1979); R. Lentin, Traces of Racial Exception: Racializing Israeli Settler Colonialism (London: Bloomsbury Academic, 2018), pp. 62, 78; A. Sabbagh-Khoury, “Tracing Settler Colonialism: A Genealogy of a Paradigm in the Sociology of Knowledge Production in Israel,” Politics and Society 50/1 (2021); N. Erakat, “Beyond Discrimination: Apartheid Is a Colonial Project and Zionism Is a Form of Racism,” EJIL: Talk! (July 5, 2021), https://www.ejiltalk.org/beyond-discrimination-apartheid-is-a-colonial-project-and-zionism-is-a-form-of-racism.
[7] World Health Organization, Apartheid and Mental Health Care (Geneva: World Health Organization, 1977).
[8] World Health Organization, “Health Inequities and Their Causes” (February 22, 2018), https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes.
[9] State of Israel Central Bureau of Statistics, “Life Expectancy by Sex, Religion and Population Group” (September 15, 2009), https://www.cbs.gov.il/he/publications/doclib/2020/3.shnatonhealth/st03_05.pdf; State of Palestine, Palestinian Central Bureau of Statistics, “H.E. Dr. Awad, Highlights the Situation of the Palestinian Women on the Eve of the International Women’s Day” (March 8, 2021), https://www.pcbs.gov.ps/post.aspx?lang=en&ItemID=3934.
[10] World Health Organization, Health Conditions in the Occupied Palestinian Territory, including East Jerusalem, and in the Occupied Syrian Golan, WHA Doc. A74/22 (2021).
[11] Solar and Irwin (see note 3), p. 6.
[12] Ibid.
[13] Ibid., p. 41.
[14] Ibid., p. 40.
[15] R. Gilmore, Golden Gulag: Prisons, Surplus, Crisis, and Opposition in Globalizing California (Berkeley: University of California Press, 2007), p. 247.
[16] F. Fanon, The Wretched of the Earth (New York: Grove Press, 1963), p. 40.
[17] Z. Lockman, Contending Visions of the Middle East: The History and Politics of Orientalism (Cambridge University Press, 2004), p. 61.
[18] R. Greenstein, Genealogies of Conflict: Class, Identity and State in Palestine/Israel and South Africa (Middletown: Wesleyan University Press, 1995), pp. 3, 21.
[19] C. Ford and C. Airhihenbuwa, “Critical Race Theory, Race Equity, and Public Health: Toward Antiracism Praxis,” American Journal of Public Health 100/Suppl 1 (2010).
[20] Ibid.; E. Borde and M. Hernández, “Revisiting the Social Determinants of Health Agenda from the Global South,” Global Public Health 14/6–7 (2019), pp. 849, 855.
[21] Ford and Airhihenbuwa (see note 19).
[22] S. Hall, J. Evans, and S. Nixon, Representation: Cultural Representation and Signifying Practices Second Edition (London: Sage, 2013), pp. 1–47.
[23] Ibid., p. 23.
[24] E. Said, Orientalism (New York: Vintage Books, 1979), p. 40.
[25] P. Bourdieu, Language and Symbolic Power (1991, trans. G. Raymond and M. Adamson), p. 165; D. Pavón-Cuéllar, “Lacan and Social Psychology,” Social and Personality Psychology Compass 7/5 (2013).
[26] S. Zizek, Violence: Six Sideways Reflections (New York, Picador, 2008).
[27] Wolfe (see note 4), pp. 388, 390; L. Veracini, Settler Colonialism: A Theoretical Overview (Houndmills: Palgrave Macmillan, 2010), p. 23.
[28] Wolfe (see note 4).
[29] R. Muhareb and P. Clancy, “Palestine and the Meaning of Domination in Settler Colonialism and Apartheid,” República y Derecho 4/6 (2021).
[30] Bourdieu (see note 25), p. 165.
[31] Said (see note 24).
[32] G. Meir, op-ed in the New York Times (January 14, 1976, reprinted in AISH, January 11, 2018), https://aish.com/golda-meir-on-the-palestinians/.
[33] O. Solombrino, “Where Is Palestine? Notes on Palestine and the (Post)colonial,” in G. Proglio (ed), Decolonising the Mediterranean: European Colonial Heritages in North Africa and the Middle East (Newcastle: Cambridge Scholars, 2016), p. 7.
[34] G. Meir, “I Am Palestinian,” https://www.youtube.com/watch?v=GZPyyAWGK0w.
[35] Veracini (see note 27), p. 31.
[36] Ibid., p. 35.
[37] Basic Law: Israel¾The Nation State of the Jewish People (unofficial translation, July 25, 2018), https://www.adalah.org/en/content/view/9569; Adalah, “The Illegality of Article 7 of the Jewish Nation-State Law: Promoting Jewish Settlement as a National Value,” Adalah Position Paper (March 2019), https://www.adalah.org/uploads/uploads/Position_Paper_on_Article_7_JNSL_28.03.19.pdf.
[38] Office of the United Nations High Commissioner for Human Rights, “Israel: UN Experts Urge Authorities to Cease Eviction and Demolition of Bedouin Village” (June 3, 2022), https://www.ohchr.org/en/press-releases/2022/06/israel-un-experts-urge-authorities-cease-eviction-and-demolition-bedouin; Sayegh (see note 6), p. 22.
[39] Law of Return 5710 (1950); Citizenship Law 5712 (1952).
[40] A. Sabbagh-Khoury, “Citizenship as Accumulation by Dispossession: The Paradox of Settler Colonial Citizenship,” Sociological Theory 40/2 (2022), p. 152.
[41] Ibid., p. 156.
[42] Ibid.
[43] T. Abowd, “The Politics and Poetics of Place: The Baramki House,” Jerusalem Quarterly 21 (2004).
[44] R. Falk and V. Tilley, Israeli Practices towards the Palestinian People and the Question of Apartheid (Beirut: United Nations Economic and Social Commission for Western Asia, 2017), p. 37.
[45] Ibid., pp. 37–38.
[46] Al-Haq, BADIL Resource Center for Palestinian Residency and Refugee Rights, Palestinian Center for Human Rights, et al., Joint Parallel Report to the United Nations Committee on the Elimination of Racial Discrimination on Israel’s Seventeenth to Nineteenth Periodic Reports (November 10, 2019), https://www.alhaq.org/advocacy/16183.html.
[47] “The Manifesto of Dignity and Hope,” Mondoweiss (May 18, 2021), https://mondoweiss.net/2021/05/the-manifesto-of-dignity-and-hope/.
[48] Borde and Hernández (see note 20).
[49] United Nations Office for the Coordination of Humanitarian Affairs, “Data on Casualties,” https://www.ochaopt.org/data/casualties.
[50] Ibid.
[51] Al-Haq, “Israel Deliberately Injures and Maims Palestinian Civilians, Prevents Evacuation of Wounded, and Denies Access to Vital Healthcare Facilities Outside the Gaza Strip” (April 18, 2018), https://www.alhaq.org/monitoring-documentation/6243.html.
[52] United Nations Office for the Coordination of Humanitarian Affairs, “Two Years On: People Injured and Traumatized during the ‘Great March of Return’ Are Still Struggling,” Humanitarian Bulletin (April 6, 2020), https://www.ochaopt.org/content/two-years-people-injured-and-traumatized-during-great-march-return-are-still-struggling; World Health Organization, Emergency Trauma Response to the Gaza Mass Demonstrations 2018–2019 (occupied Palestinian territory: World Health Organization, 2019), pp. 14, 39; World Health Organization, “Attacks on Health Care during the Gaza Great March of Return (March 2018 to November 2019)” (November 30, 2019), https://www.un.org/unispal/document/attacks-on-health-care-during-the-gaza-great-march-of-return-march-2018-to-nov-2019-who-infographic.
[53] International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966), arts. 6(1), 9.
[54] See, for example, legal analysis in Al-Haq, “‘Bloody Monday’: Documentation of the Shoot-to-Kill, Egregious Killings Committed by the Israel Occupying Force (IOF) on 14 May 2018” (May 26, 2018), https://www.alhaq.org/advocacy/6196.html.
[55] Human Rights Council, Report of the Independent International Commission of Inquiry on the 2018 Protests in the Occupied Palestinian Territory, UN Doc. A/HRC/40/74 (2019).
[56] Office of the United Nations High Commissioner for Human Rights, “UN Commission Urges Israel to Review Rules of Engagement before Gaza Protest Anniversary” (March 18, 2019), https://www.ohchr.org/en/news/2019/03/un-commission-urges-israel-review-rules-engagement-gaza-protest-anniversary?LangID=E&NewsID=24348; Human Rights Council (2019, note 55), para.119(b).
[57] See discussion in R. Muhareb, “Addressing the ‘Full Context’: The First Report of the Commission of Inquiry on Root Causes in Palestine,” Irish Centre for Human Rights Blog (June 14, 2022), https://ichrgalway.wordpress.com/2022/06/14/addressing-the-full-contextthe-first-report-of-the-commission-of-inquiry-on-root-causes-in-palestine/.
[58] Human Rights Council, Report of the Independent International Commission of Inquiry on the Occupied Palestinian Territory, including East Jerusalem, and Israel, UN Doc. A/HRC/50/21 (2022), p. 1.
[59] See, for example, Al-Haq, “Sham Investigation by Israel’s Military Advocate General into IOF Killing of Razan Al-Najjar” (June 13, 2018), https://www.alhaq.org/advocacy/6187.html.
[60] See, recently, “Joint Investigation Finds Abu Akleh’s Killing ‘Deliberate’,” Al-Jazeera (September 20, 2022), https://www.aljazeera.com/news/2022/9/20/joint-investigation-reveals-abu-aklehs-killing-premeditated.
[61] B. Browne, “Killing of Shireen Abu Akleh a Fatal Sign of Israel’s Control: Pattern of Palestinian Media Bodies Being Attacked by Israeli Policy Is All Too Evident,” Irish Times (May 16, 2022), https://www.irishtimes.com/opinion/killing-of-shireen-abu-akleh-a-fatal-sign-of-israel-s-control-1.4878879.
[62] BADIL, Biennial Survey on Palestinian Refugees and Internally Displaced Persons 2016-2018 (Bethlehem: BADIL, 2019).
[63] World Health Organization, “Refugee and Migrant Health” (May 2022), https://www.who.int/news-room/fact-sheets/detail/refugee-and-migrant-health.
[64] World Health Organization, Health Conditions in the Occupied Palestinian Territory, including East Jerusalem, and in the Occupied Syrian Golan, WHA Doc. A75/26 (2022).
[65] UNRWA, Palestine Refugees in Lebanon: Struggling to Survive (Beirut: UNRWA, 2022).
[66] Human Rights Watch, “Human Rights Watch Policy on the Right to Return” (2021), https://www.hrw.org/legacy/campaigns/israel/return/un194-rtr.htm.
[67] T. Rempel, “The United Nations Conciliation Commission for Palestine, Protection, and a Durable Solution for Palestinian Refugees,” BADIL Information and Discussion Brief 5 (2000).
[68] Ibid.
[69] UNRWA, “What Is the Mandate of UNRWA?,” https://www.unrwa.org/what-mandate-unrwa-0; Charter of the United Nations (1945), arts. 7.2, 22; L. Bartholomeusz, “The Mandate of UNWRA at Sixty,” Refugee Studies Quarterly 28/2–3 (2009).
[70] United Nations, “UNRWA Faces Greatest Financial Crisis in its History following 2018 Funding Cuts, Commissioner‑General Tells Fourth Committee,” https://www.un.org/unispal/document/unrwa-faces-greatest-financial-crisis-in-its-history-following-2018-funding-cuts-commissioner‑general-tells-fourth-committee-press-release/.
[71] United Nations Office for the Coordination of Humanitarian Affairs, “Data on Demolitions and Displacement in the West Bank,” https://www.ochaopt.org/data/demolition; United Nations Office for the Coordination of Humanitarian Affairs, “Data on Casualties” (see note 49).
[72] M. Farah, “Planning in Area C: Discrimination in Law and Practice,” Palestine-Israel Journal of Politics, Economics and Culture 21/3 (2016); Peace Now, “Construction Starts in Settlements by Year,” https://peacenow.org.il/en/settlements-watch/settlements-data/construction.
[73] United Nations Office for the Coordination of Humanitarian Affairs, “Court Ruling on Masafer Yatta: Statement by United Nations Resident and Humanitarian Coordinator in the Occupied Palestinian Territory, Lynn Hastings” (May 6, 2022), https://www.ochaopt.org/content/statement-united-nations-resident-and-humanitarian-coordinator-occupied-palestinian-territory-lynn-hastings.
[74] Ibid.
[75] Geneva Convention Relative to the Protection of Civilian Persons in Time of War, 75 UNTS 287 (1949), art. 33.
[76] Information provided by World Health Organization (2022); see also L. Masarwa, “Palestine: Jerusalem Refugee Camp under Siege as Israel Hunts Shooter,” Middle East Eye (October 10, 2022), https://www.middleeasteye.net/news/israel-palestine-jerusalem-shuafat-refugee-camp-under-siege.
[77] Human Rights Watch (2021, see note 66).
[78] A. Asmar, Kufr Aqab: The Arab Neighborhoods in East Jerusalem Infrastructure Research and Evaluation (Jerusalem: Jerusalem Institute for Policy Research, 2018).
[79] Association for Civil Rights in Israel, East Jerusalem: Facts and Figures 2021 (Tel Aviv: Association for Civil Rights in Israel, 2021).
[80] A. Rigolon, M. Browning, O. McAnirlin, and H. Yoon. “Green Space and Health Equity: A Systematic Review on the Potential of Green Space to Reduce Health Disparities,” International Journal of Environmental Research and Public Health 18 (2021).
[81] Al-Haq, “Punitive Residency Revocation: The Most Recent Tool of Forcible Transfer” (March 17, 2018), https://www.alhaq.org/advocacy/6257.html; Al-Haq, “Al-Haq Condemns the Revocation of Lawyer and Human Rights Defender Salah Hammouri’s Jerusalem Residency” (October 19, 2021), https://www.alhaq.org/advocacy/18995.html; Addameer, “Israeli Minister of Interior to Officially Revoke Permanent Residency of Lawyer Salah Hammouri” (October 18, 2021), https://www.addameer.org/news/4531.
[82] Al-Haq, Annexing A City: Israel’s Illegal Measures to Annex Jerusalem Since 1948 (Ramallah: Al-Haq, 2020).
[83] B. Hassan, “Silent Violence: This Is How Israeli Colonialism Breaks into Our Family Lexicon,” 7iber (April 19, 2022), https://www.7iber.com/politics-economics/%d8%a7%d9%84%d8%a7%d8%ad%d8%aa%d9%84%d8%a7%d9%84-%d8%a7%d9%84%d8%a5%d8%b3%d8%b1%d8%a7%d8%a6%d9%8a%d9%84%d9%8a-%d9%8a%d9%82%d8%aa%d8%ad%d9%85-%d9%85%d8%b9%d8%ac%d9%85%d9%86%d8%a7/.
[84] Jerusalem Legal and Human Rights Centre, “Families Divided: Israel Passes New Citizenship Law, Fortifies Apartheid Regime,” https://www.jlac.ps/details.php?id=j5odbba2295y2r34zkmv5.
[85] A. Korn, “The Ghettoization of the Palestinians,” in R. Lentin (ed), Thinking Palestinian (London: Zed Books, 2008); L. Wacquant, “Deadly Symbiosis: When Ghetto and Prison Meet and Mesh,” Punishment and Society 3/1 (2001).
[86] Wacquant (see note 85).
[87] A. Korn, “Rates of Incarceration and Main Trends in Israeli Prisons,” Criminology and Criminal Justice 3/1 (2003).
[88] A. Arnon, “Israeli Policy towards the Occupied Palestinian Territories: The Economic Dimension, 1967–2007,” Middle East Journal 61/4 (2007).
[89] Ibid.
[90] Ibid.
[91] M. Niezna, “Under Control: Palestinian Workers in Israel during COVID-19,” University of Oxford, Faculty of Law Blog (July 7, 2020), https://www.law.ox.ac.uk/research-subject-groups/centre-criminology/centreborder-criminologies/blog/2020/07/under-control.
[92] Arnon (see note 88).
[93] United Nations Office for the Coordination of Humanitarian Affairs, “Gaza Crossings: Movement of People and Goods,” https://www.ochaopt.org/data/crossings.
[94] I. Pappe, The Biggest Prison on Earth: A History of the Occupied Territories (London: Oneworld Publications, 2017).
[95] International Labour Organization, The Situation of Workers in the Occupied Arab Territories: Report of the Director-General – Appendix (Geneva: International Labour Organization, 2021), p. 11.
[96] Ibid., p. 20.
[97] J.-C. Barbier, “‘Employment Precariousness’ in a European Cross-National Perspective: A Sociological Review of Thirty Years of Research,” Documents de travail du Centre d’Economie de la Sorbonne, https://ideas.repec.org/p/mse/cesdoc/11078.html; A. Clair, A. Reeves, M. McKee, and D. Stuckler, “Constructing a Housing Precariousness Measure for Europe,” Journal of European Social Policy 29/1 (2019).
[98] United Nations Conference on Trade and Development, Report on UNCTAD Assistance to the Palestinian People: Developments in the Economy of the Occupied Palestinian Territory, UN Doc. TD/B/EX(72)/2 (2022).
[99] World Health Organization, Right to Health 2018 (Cairo: WHO Regional Office for the Eastern Mediterranean, 2019), p. 1.
[100] World Health Organization, 15 Years of Gaza Blockade and Barriers to Health Access, http://www.emro.who.int/images/stories/palestine/15_Years_Gaza_Blockade_Factsheet.jpg?ua=1.
[101] B. Bouquet, F. Barone-Adesi, M. Lafi, et al., “Comparative Survival of Cancer Patients Requiring Israeli Permits to Exit the Gaza Strip for Health Care: A Retrospective Cohort Study from 2008 to 2017,” PLoS ONE 16/6 (2021).
[102] World Health Organization, Health Access: Barriers for Patients in the Occupied Palestinian Territory (March 2022), http://www.emro.who.int/images/stories/palestine/March_2022_Monthly.pdf?ua=1.
[103] Norton Children’s, “Atrial Septal Defect (ASD) Repair” (2022), https://nortonchildrens.com/services/cardiology/conditions/treatments/surgical/atrial-septal-defect-asd-repair/#:~:text=In%20more%20than%2099%25%20of,or%20restrictions%20after%20ASD%20repair.
[104] International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966), art. 6(1).
[105] Solar and Irwin (see note 3), p. 28.
[106] Bourdieu (see note 25), pp. 12, 129, 165.
[107] “PFLP Ghassan Kanafani, Richard Carleton Interview Complete,” YouTube, https://youtu.be/Veoy32G7trY.
[108] Bourdieu (see note 25), p. 165.
[109] B. de Sousa Santos, The End of the Cognitive Empire: The Coming of Age of Epistemologies of the South (Durham: Duke University Press, 2018), pp. 1–18.
[110] Sayegh (see note 6); Erakat (see note 6).
[111] F. Sayegh, Zionist Colonialism in Palestine (Beirut: PLO Research Centre 1965); F. Sayegh, “Zionism: A Form of Racism and Racial Discrimination,” in A. W. Al Kayyali (ed), Zionism, Imperialism and Racism (London: Croom Helm, 1979), p. 51.
[112] Sayegh (1979, see note 111), p. 54; see also A. W. Kayyali, “Zionism and Imperialism: The Historical Origins,” Journal of Palestine Studies 6/3 (1977), p. 105.
[113] A. Abofoul, “Sound but Insufficient: The Mainstream Discussion on the Question of the Applicability of Apartheid in the Occupied Palestinian Territory,” Opinio Juris (March 21, 2022), http://opiniojuris.org/2022/03/21/sound-but-insufficient-the-mainstream-discussion-on-the-question-of-the-applicability-of-apartheid-in-the-occupied-palestinian-territory/; Erakat (see note 6).
[114] V. Tilley (ed), Occupation, Colonialism, Apartheid?: A Re-assessment of Israel’s Practices in the Occupied Palestinian Territories under International Law (Cape Town: Human Sciences Research Council, 2009); see also Al-Haq, “South African Study Finds That Israel Is Practicing Colonialism and Apartheid in the Occupied Palestinian Territory” (June 4, 2009), https://www.alhaq.org/advocacy/7207.html.
[115] Committee on the Elimination of Racial Discrimination, Concluding Observations: Israel, UN Doc. CERD/C/ISR/CO/13 (2007), paras. 22–23; Committee on the Elimination of Racial Discrimination, Concluding Observations: Israel, UN Doc. CERD/C/ISR/CO/14-16 (2012), paras. 11, 24; Committee on the Elimination of Racial Discrimination, Concluding Observations: Israel, UN Doc. CERD/C/ISR/CO/17-19 (2019), para. 23; Al-Haq et al. (2019, note 46); BADIL Staff, “The UN Anti-Racism Committee Questions Israel’s Policy of Apartheid in Israel and the OPT and Calls for Equality in the implementation of the Right of Return,” Al-Majdal 33 (2007); International Convention on the Elimination of All Forms of Racial Discrimination, G.A. Res. 2106A (XX), art. 3.
[116] World Conference Against Racism, “NGO Forum Declaration” (September 3, 2021), https://www.hurights.or.jp/wcar/E/ngofinaldc.htm, para. 98; Adalah, “International Advocacy (2001) UN World Conference Against Racism, Racial Discrimination, Xenophobia and Related Intolerance – Durban, South Africa, August-September 2001,” https://www.adalah.org/en/content/view/7467; see generally Stop the Wall: Palestinian Grassroots Anti-Apartheid Wall Campaign, “About Us,” https://www.stopthewall.org/about-us/; BDS, “Palestinian Civil Society Calls for Boycott, Divestment and Sanctions against Israel Until It Complies with International Law and Universal Principles of Human Rights” (July 9, 2005), https://bdsmovement.net/call.
[117] N. Alazza and M. Yvonne (eds), “Forced Population Transfer: The Case of Palestine¾Segregation, Fragmentation and Isolation,” BADIL Working Paper No. 23 (February 2020), https://www.badil.org/cached_uploads/view/2021/04/19/wp23-sfi-1618823935.pdf; Al-Haq et al. (2019, see note 46); Israel and the Crime of Apartheid: The Vision of the Anti-apartheid Struggle, themed edition, Al-Majdal 48 (2012), https://www.badil.org/phocadownload/Badil_docs/publications/al-majdal48.pdf; Racism, Refugees, and Apartheid, themed edition, Al-Majdal 15 (2002), https://www.badil.org/cached_uploads/view/2021/05/06/al-majdal-15-1620308690.pdf; M. Sfard, The Israeli Occupation of the West Bank and the Crime of Apartheid: Legal Opinion (Tel Aviv: Yesh Din, July 2020); B’Tselem, “A Regime of Jewish Supremacy from the Jordan River to the Mediterranean Sea: This Is Apartheid” (January 12, 2021), https://www.btselem.org/publications/fulltext/202101_this_is_apartheid; Human Rights Watch, A Threshold Crossed: Israeli Authorities and the Crimes of Apartheid and Persecution (New York: Human Rights Watch, 2021); Amnesty International, Israel’s Apartheid against Palestinians: Cruel System of Domination and Crime against Humanity (London: Amnesty International, 2022).
[118] International Convention on the Elimination of All Forms of Racial Discrimination, G.A. Res. 2106A (XX) (1965), art. 3; Rome Statute of the International Criminal Court, 2187 UNTS 3 (1998), art. 7(1)(j); International Convention on the Suppression and Punishment of the Crime of Apartheid, 1015 UNTS 243 (1973), art. I.1.
[119] International Convention on the Suppression and Punishment of the Crime of Apartheid, 1015 UNTS 243 (1973), arts. II.c, II.d, II.f.
[120] See Al-Haq, “Israeli Apartheid Undermines Palestinian Right to Health Amidst COVID-19 Pandemic,” (April 7, 2020), https://www.alhaq.org/advocacy/16692.html.
[121] Y. Asi, “The Fight against Vaccine Apartheid Goes Global: Israel’s Refusal to Vaccinate Palestinians under Occupation Has Stirred Widespread Outrage—and Linked the Struggle for Justice in Palestine to Struggles around the World,” Nation (April 27, 2021), https://www.thenation.com/article/world/vaccine-palestine-israel/; M. Kearney, A. Khdair, and R. Muhareb, COVID-19 and the Right to Health of Palestinians under Israeli Occupation, Colonisation, and Apartheid (Ramallah: Al-Haq, 2020); Amnesty International, “Israel/OPT: Denying COVID-19 Vaccines to Palestinians Exposes Israel’s Institutionalised Discrimination’ (January 6, 2021), https://www.amnesty.ie/israel-opt-denying-covid-19-vaccines-to-palestinians-exposes-israels-institutionalised-discrimination/.
[122] World Health Organization, Apartheid and Health (Geneva: World Health Organization, 1983), p. 47.
[123] Ibid., p. 21.
[124] World Health Organization (1977, note 7), p. 1.
[125] Ibid., p. 5.
[126] Ibid., pp. 5–8.
[127] Ibid.
[128] R. Muhareb, “International Law and the Palestinian Anti-Apartheid Movement,” Al-Shabaka (March 23, 2022), https://al-shabaka.org/memos/international-law-and-the-palestinian-anti-apartheid-movement/; A. Amara and Y. Hawari, “Using Indigeneity in the Struggle for Palestinian Liberation,” Al-Shabaka (August 8, 2019), https://al-shabaka.org/commentaries/using-indigeneity-in-the-struggle-for-palestinian-liberation/; M. Rifkin, “Indigeneity, Apartheid, Palestine: On the Transit of Political Metaphors,” Cultural Critique 95 (2017).
[129] L. Tatour, “Why Calling Israel an Apartheid State Is Not Enough,” Middle East Eye (January 18, 2021), https://www.middleeasteye.net/opinion/why-calling-israel-apartheid-state-not-enough.
[130] S. Asaad and R. Muhareb, “Dismantle What? Amnesty’s Conflicted Messaging on Israeli Apartheid,” Institute for Palestine Studies (February 15, 2022), https://www.palestine-studies.org/en/node/1652565.
[131] Constitution of the World Health Organization (1946).
[132] Committee on Economic, Social and Cultural Rights (see note 1), para. 8.
[133] See, e.g., Human Rights Council, Report of the Special Rapporteur on the Situation of Human Rights in the Palestinian Territories Occupied Since 1967, UN Doc. A/HRC/49/87 (2022), para. 55.
[134] World Health Organization (1983, see note 122), p. 48.
[135] Ibid., p. 26.