Toward Human Rights-Consistent Responses to Health Emergencies: What Is the Overlap between Core Right to Health Obligations and Core International Health Regulation Capacities?
Volume 22/2, December 2020, pp 99 -112
Brigit Toebes, Lisa Forman, and Giulio Bartolini
Abstract
COVID-19 has highlighted the responsibilities of states under the International Health Regulations (IHR), as well as state accountability in case of a breach. These approaches and dimensions are valuable, as many COVID responses have breached human rights. We should also look beyond this crisis and address country preparedness for effective and equitable responses to future infectious disease outbreaks. This paper assesses countries’ international legal obligations to be prepared to respond to this and future public health emergencies. It does so from the perspective of the right to health, in interaction with the IHR. We analyze the functional relationship between the right to health and the IHR, focusing in particular on “core obligations” under the right to health and “core capacities” under the IHR. We find considerable parallels between the two regimes and argue in favor of more cross-fertilization between them. This regime interaction may enrich both frameworks from a normative perspective while also enhancing accountability and public health and human rights outcomes.
Introduction
COVID-19 has put a spotlight on the responsibilities of states under the International Health Regulations (IHR) and on state accountability in case of a breach.1 In addition, there has been much debate about how measures to protect against COVID-19 infringe on the enjoyment of civil and political rights, in particular the rights to privacy and freedom of movement.2 It is important to evaluate these matters carefully given the current crisis. While these approaches and dimensions are valuable, we should also look beyond this crisis and address country preparedness to respond to future infectious disease outbreaks.
To this end, this paper assesses countries’ international legal obligation to be prepared to respond to this and future public health emergencies. It does so from the perspective of the right to health as a fundamental economic and social right, in interaction with the IHR. This contribution is grounded in the understanding that COVID-19 reflects, in essence, a crisis of the right to health: because countries do not deliver the right to health in its own right or as reflected by the IHR, many other problems, including violations of international law, arise. We contend that better integration of human rights into the IHR will not simply boost social justice and health equity in IHR-related pandemic responses but could also boost the public health efficacy of such measures.3 We analyze the functional relationship between the right to health and the IHR, focusing in particular on core obligations under the right to health and core capacities under the IHR. We consider the overlaps between these two international law regimes insofar as they prescribe prioritized state duties within both regimes, and the extent to which their respective duties may assist in defining or implementing each other. We argue that this kind of systemic integration is supported within international law’s accepted rules for treaty interpretation in the Vienna Convention on the Law of Treaties, which provides that “international standards may be interpreted in the light of any relevant rules of international law applicable in the relations between the parties.”4 We argue further that doing so helps resolve the problem of fragmentation within international law, as demonstrated by interpretations of the IHR that are not compliant with human rights. It also helps advance a more human rights-consistent implementation of the IHR. Legal analysis of this nature offers important guidance to states implementing the IHR during the COVID-19 pandemic, as well as for future disease outbreaks. It is also relevant to potential reforms of the IHR that seek to boost adherence to human rights during pandemic outbreaks.5
Historical emergence of the right to health and the IHR
The right to health
To understand the interaction between the right to health and the IHR, one must go back to the period right after World War II. It was a period of optimism and belief in a better and healthier world, a time where the idea was voiced that “medicine is one of the pillars of peace.”6 In 1946, states adopted the Constitution of the World Health Organization (WHO), the founding document that led to WHO’s establishment in 1948. It is a remarkable and groundbreaking document in many ways. The preamble to the WHO Constitution defines health as a “state of complete physical, mental and social well-being, and not merely the absence of disease.” This definition has often been criticized for being too absolute, yet it should be seen in the light of postwar idealism and can be appreciated for its reference to mental and social well-being as important dimensions of health.7
The preamble was also pioneering for its recognition of health as a right: “the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.” This wording informed the right to health provisions in the United Nations (UN) human rights treaties that were adopted in the decades thereafter. The most authoritative provision is arguably article 12 of the International Covenant on Economic, Social and Cultural Rights (ICESCR), which stipulates the “right to the highest attainable standard of health.” Other key provisions include article 12 of the Convention on the Elimination of All Forms of Discrimination against Women; article 24 of the Convention on the Rights of the Child; and article 25 of the Convention on the Rights of Persons with Disabilities. Since the beginning of this century, article 12 of the ICESCR and article 24 of the Convention on the Rights of the Child have begun to be complemented with “general comments,” explanatory documents that carry the status of soft law but are nonetheless seen as authoritative.8
These treaties are widely ratified—171 countries have ratified the ICESCR, 182 countries have ratified the Convention on the Rights of Persons with Disabilities, 189 countries have ratified the Convention on the Elimination of All Forms of Discrimination against Women, and 196 countries have ratified the Convention on the Rights of the Child.9 Thus, in contrast to the universality of ratifications of the Convention on the Rights of the Child, approximately 25 of 196 states globally have not ratified the ICESCR and are not legally bound by this treaty’s right to health. On the one hand, this shortfall underscores that our analysis is relevant for the majority of states. On the other, the fact that nonratifying states include the United States points to the larger political challenge of advancing a right to health lens for the IHR given the United States’ long-standing objections to the legal status of economic, social, and cultural rights in general and the right to health in particular.
As indicated above, WHO was the first international organization to recognize health as a human right. However, over the past 73 years of its existence, WHO has not manifested itself as a human rights organization. Yet the organization has gradually embraced the human rights framework owing to the way that it has been developed by UN human rights mechanisms.
The International Health Regulations
The WHO Constitution grants considerable legislative powers to the World Health Assembly. Based on articles 19–23 of the Constitution, the assembly may adopt conventions, (binding) regulations, and (nonbinding) recommendations. The results have been very disappointing so far: since its establishment in 1948, WHO has adopted only one treaty (the Framework Convention on Tobacco Control) and two regulations (the Nomenclature Regulations and the IHR). While the results are scant, the Framework Convention on Tobacco Control and the IHR are highly authoritative instruments. Central to this paper is the IHR.
International collaboration in the field of infectious disease control started in the second half of the 19th century. In 1851, the first international sanitary conference took place. Many similar meetings followed, and subsequent sets of international sanitary regulations were gradually adopted. The IHR, adopted in 2005 and entered into force 2007, is the most recent set of regulations. Given its status as regulations, the IHR is binding on all 194 WHO member states without their consent (although members may notify the director-general of rejection or reservations).
The new IHR is innovative because of its “all hazards” approach: it covers risks arising from numerous sources, not just a limited list of diseases.10 Thus, even a terrorist attack with anthrax or a chemical spill could fall within the remit of this instrument if it is established that the threat constitutes a “public health emergency of international concern.”11 Such emergencies have been declared six times since the IHR’s adoption: influenza in Mexico (2009); Ebola in West Africa (2014); polio in Pakistan, Afghanistan, and Nigeria (2014); Zika in South America (2016); Ebola in Congo (2018); and COVID-19 in China (2020).
The IHR refers to human rights in various provisions (articles 3, 23, 32, and 45). Article 3, which outlines general principles of the regulations, states that the IHR shall be implemented with “full respect for the dignity, human rights and fundamental freedoms of persons” and “guided by the Charter of the United Nations and the Constitution of the WHO.”12 Despite this reference to the WHO Constitution, these references are, in essence, linked to respect for civil and political rights, including the rights to privacy, physical integrity, and freedom of movement (for example, medical consent in article 23 and respect for travelers in article 32). Contrary to the WHO Constitution and the Framework Convention on Tobacco Control, the IHR does not mention the right to health.11 This is an important omission, given that—as we will demonstrate below—states’ obligation to prepare and respond to infectious disease outbreaks is an essential component of the right to health. This overlap is apparent in the stated goal of the IHR—“universal application for the protection of all people of the world from the international spread of disease”—which is functionally similar to the ICESCR’s duty to prevent, treat, and control epidemic, endemic, and other diseases, even though the former has a more explicitly universal focus than the largely domestically oriented duties of the ICESCR.13
Another important shortcoming of the IHR is its lack of sanctions: states refusing to collaborate with WHO in case of an outbreak can go without any warning or punishment. As we argue below, the UN human rights monitoring system and domestic courts may offer complementary mechanisms for holding states accountable under the IHR.
Comparing and contrasting core obligations and core capacities: Connecting the dots
Our main point is that the core obligations under the right to health are closely intertwined with the core capacities under the IHR. Starting with the UN human rights framework, we will now briefly discuss both regimes and discuss their interaction with each other.
The right to health’s prioritized obligations: Essential elements and core and comparable priority obligations
Article 12 of the ICESCR stipulates that states should take steps necessary for “the prevention, treatment and control of epidemic, endemic, occupational and other diseases.” Hence, there is a clear human rights obligation on the part of states to take measures to combat epidemic diseases. An explanation of the meaning and scope of the right to health is provided in General Comment 14, issued by the Committee on Economic, Social and Cultural Rights. Although this instrument is not legally binding, it is seen as highly authoritative. Three components of this general comment are important for infectious disease control because they identify and define essential, core, and otherwise prioritized aspects of this right:
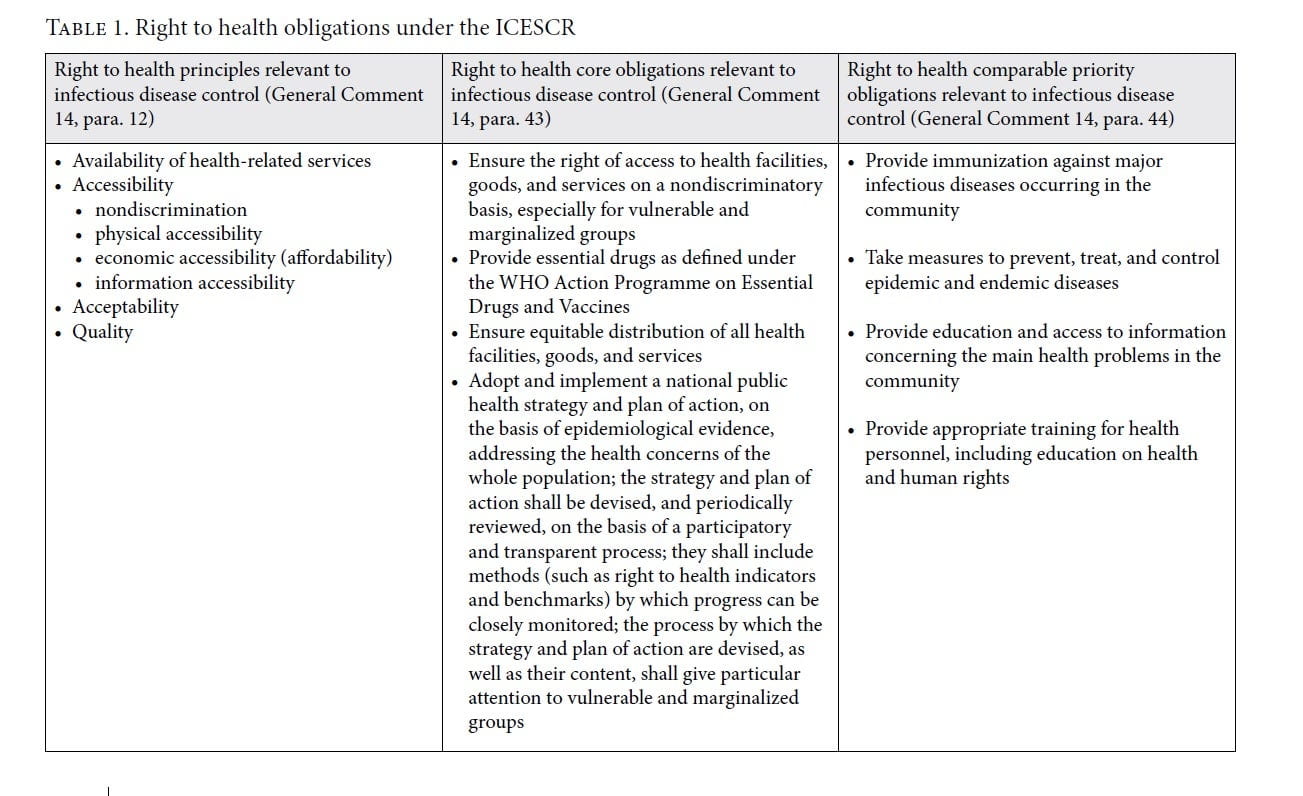
AAAQ. According to General Comment 14, the right to health contains a set of interrelated and essential elements, which are considered to provide guidance to the actions by states: availability, accessibility, acceptability, and quality. This so-called AAAQ is an authoritative set of standards that is increasingly applied across international and domestic health settings. While it certainly lacks precision, it helps identify weak spots in health decision-making. Given that these (and similar) principles are applied frequently in health settings and because their importance is underscored by governments and health authorities, we suggest that this framework is emerging as a norm of customary international (health) law.
The AAAQ is also very informative in the context of COVID-19, as it pinpoints the weak spots in states’ responses to this crisis. First, key problems stem from a lack of availability of health personnel, intensive care beds, drugs, masks, and gloves. Second, many problems occur in the context of accessibility—for example, inequalities in access to health care by vulnerable persons (such as older persons, persons with low socioeconomic status, and persons with underlying health conditions) and a lack of geographically accessible, affordable, and good-quality health care. Third, in terms of acceptability, COVID-19 creates many health care settings where medical ethics are under threat, such as care homes where older and disabled persons are denied contact with the outside world. Lastly, in terms of quality, due to a scarcity of properly trained personnel and suitable medical equipment, many people are deprived from accessing good-quality health care. Again, while this framework lacks precision and may not be used to identify concrete human rights violations, it helps frame the analysis and debate about how the right to health is guaranteed in the context of COVID-19, and it shows the extent to which countries are prepared to address future crises.
Core obligations. The second concept in the right to health framework that is of key importance to infectious disease control is the recognition of “core obligations” under the right to health. General Comment 14 refers to General Comment 3, which notes that states have “a core obligation to ensure the satisfaction of, at the very least, minimum essential levels of each of the rights enunciated in the Covenant, including essential primary health care.” For the identification of the specific core obligations under the right to health, General Comment 14 makes reference to the Programme of Action of the International Conference on Population and Development (1994) and WHO’s Alma-Ata Declaration (1978), stating that these programs provide “compelling guidance” on the core obligations arising from article 12.14 The committee identifies a set of core obligations, four of which are particularly relevant to the COVID-19 crisis: (1) ensure nondiscriminatory access to health facilities, goods, and services on a nondiscriminatory basis, especially for vulnerable or marginalized groups; (2) provide essential drugs as defined by WHO; (3) ensure equitable distribution of all health facilities, goods, and services; and (4) adopt and implement a national public health strategy and plan of action addressing population health concerns. General Comment 14 reinforces the importance of core obligations, indicating that they are non-derogable and that states cannot justify noncompliance under any circumstances.
The meaning of the concept of core obligations has been discussed extensively in human rights discourse, and interpretations regarding its scope and force differ.15 For example, there are debates about the omission of essential health care as a core obligation, and confusion as to whether the core obligations of the right to health are non-derogable or whether resource scarcity may be an excuse for governments not to fulfill these obligations.16 In addition, there has been controversy over the legitimacy of this concept in toto, as well as discussion about whether the Committee on Economic, Social and Cultural Rights was justified in importing into the ICESCR a set of obligations without obvious textual basis in the covenant itself.17 In its subsequent general comments, the committee has moved away from its controversial articulation of core obligations as non-derogable, focusing instead on whether implementation is reasonable or proportionate.18 This shift is potentially reflective of the committee’s response to wide-standing criticisms of the unfeasibility of a non-derogable standard for core obligations, particularly for low- and middle-income countries.19 It also reflects the committee’s broader adoption of a contextual “reasonableness” analysis as a standard for adjudicating violations of economic, social, and cultural rights under the Optional Protocol to the ICESCR, adopted in 2013.20 The committee’s defined criteria for assessing reasonableness include whether states have taken deliberate, concrete, and targeted steps to fulfill rights; have acted in a nondiscriminatory manner; and have taken into account the precarious situation of disadvantaged and marginalized individuals and groups and prioritized grave situations or situations of risk.21 Core obligations are cited explicitly insofar as they are affected by retrogressive resource constraints.22 This interpretation implies that the committee sees the minimum core acting as a bar to regression, and an important consideration in assessing the legitimacy of resource constraints.23 The suggestion is that states hold core obligations under the right to health as specified in General Comment 14, with a duty to take reasonable steps toward fulfilling them.
Thus, the idea of a core content—and the notion that there is a basic subsistence line below which no government should fall—is informative in a crisis setting, where resources are limited and there are surging needs for urgent health care.
Comparable priority obligations. Core obligations are buttressed by obligations of comparable priority, which also hold validity in relation to COVID-19. These duties include providing immunization against major infectious diseases occurring in the community; taking measures to prevent, treat, and control epidemic and endemic diseases; providing education and access to information concerning the main health problems in the community; and providing appropriate training for health personnel, including education on health and human rights.24
In essence, all the principles and obligations set out in Table 1 are related to states’ duty to build resilient health systems.
Core capacities under the IHR
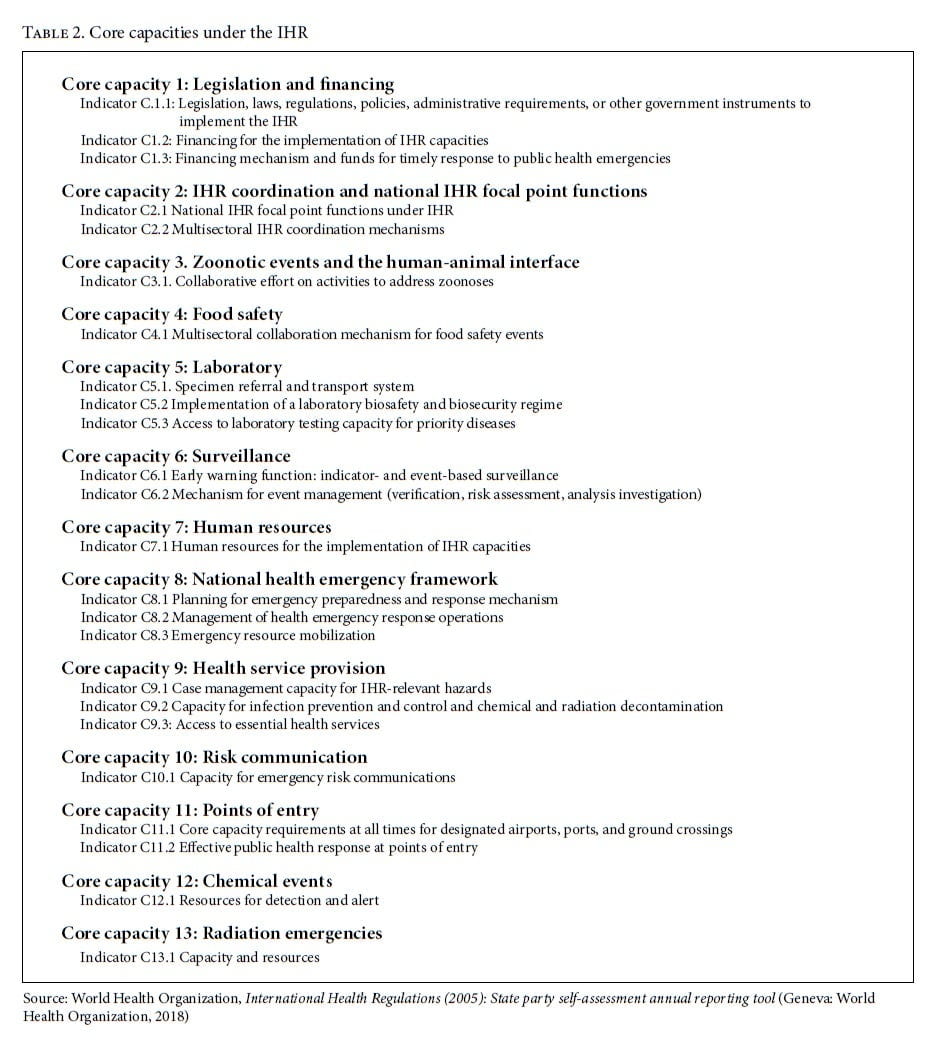
Alongside the core content of the right to health outlined above, the IHR include a series of obligations related to structural and capacity-building measures that are expected to contribute to the overall goal “to prevent, protect against, control and provide a public health response to the international spread of disease.”25 Articles 5 and 13 require states to develop within fixed deadlines the capacities to detect, assess, notify, and report public health risks and public health emergencies and respond promptly and effectively to such events. Core capacities to be implemented at the local, intermediate, and national level are detailed in annex 1 of the IHR and further specified in subsequent technical documents.26 Currently, according to the IHR monitoring process, states are requested to self-assess the implementation of 13 core capacities spelled out in 24 indicators related to different issues, including health infrastructure, legal and financial frameworks, staff, decision-making, and information capacities (Table 2).27
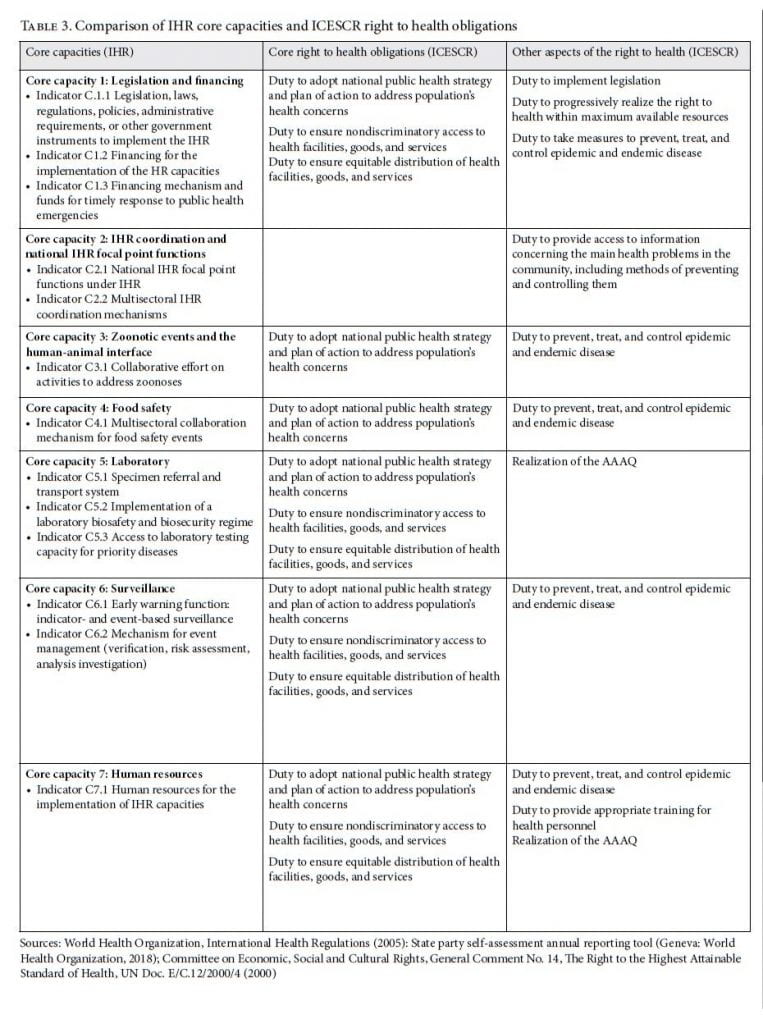
The parallels and overlaps between the core right to health obligations under the ICESCR and the core capacities under the IHR are striking. For instance, as set out in Table 1, the right to health framework requires states to “adopt a national public health strategy and plan of action, on the basis of epidemiological evidence.” This element has several commonalities in the IHR, where, for example, core capacity 1 addresses the need to have “an adequate legal framework in all relevant sectors to support and facilitate the effective and efficient implementation of all of their obligations and rights under the IHR”; core capacity 8 “focuses on the overall national health emergency framework and system for enabling countries to be prepared and operationally ready for response to any public health event, including emergencies, as per the requirement of IHR”; and indicator C9.3 refers to “access to essential health services” aimed to guarantee “resilient national health systems.”28 Core capacities provided by the IHR, as further detailed in WHO practice, might thus give more substance to the less detailed wording under the right to health through the identification of minimum requirements provided by the IHR, regardless of the structural and economic differences among states.
However, while core capacities are a cornerstone of the IHR system, evidence suggests that their implementation and monitoring remain a challenge. Even if states were required to comply with them by 2016, based on self-assessments provided by states in 2018, about two-thirds of states have poor or modest levels of preparedness, with overall scores ranging from 1 to 3 out of 5. 29 According to Lawrence Gostin and Rebecca Katz, many countries lack the financial resources to meet the core capacities, while high-income countries have offered little financial support; further, Amitabh Suthar et al. suggest that there is limited knowledge on how countries should achieve the core capacities domestically.30
In addition, the IHR is not accompanied by an effective monitoring system able to push states toward the implementation of core capacities: mandatory annual reports to be provided by states on their implementation are not subjected to any review mechanism or follow-up, as is common in other areas of international law. Only in 2016, based on the recommendation “to move from exclusive self-evaluation to approaches that combine self-evaluation, peer review and voluntary external evaluations,” did WHO’s director-general launch some new technical tools aimed at supporting states in the implementation of core capacities.31 These instruments, reflected in the current IHR Monitoring and Evaluation Framework, include guidance on simulation exercises and after-action reviews, as well as a joint external evaluation tool aimed at independently assessing states’ capacities to prevent, detect, and respond to public health risks. This latter tool has resulted in the preparation of detailed reports reviewing the strengths and weaknesses of countries under scrutiny. Thus far, around 110 countries have been evaluated through this process: however, no follow-up on reports is expected, and the above-mentioned tools are voluntary ones.32 While these processes are worthwhile and may strengthen the implementation of the IHR, a series of additional concerns are still present. For instance, states that have failed to implement the core capacities are no longer required to develop national implementation plans as originally required under articles 5 and 13. Additionally, the dispute settlement mechanism provided by article 56 of the IHR might be qualified as a weak one: indeed, the review committee established in relation to the H1N1 pandemic underlined how “the lack of enforceable sanctions” was “the most important structural shortcoming of the IHR.”33
Toward an integrated interpretation of the right to health and the IHR
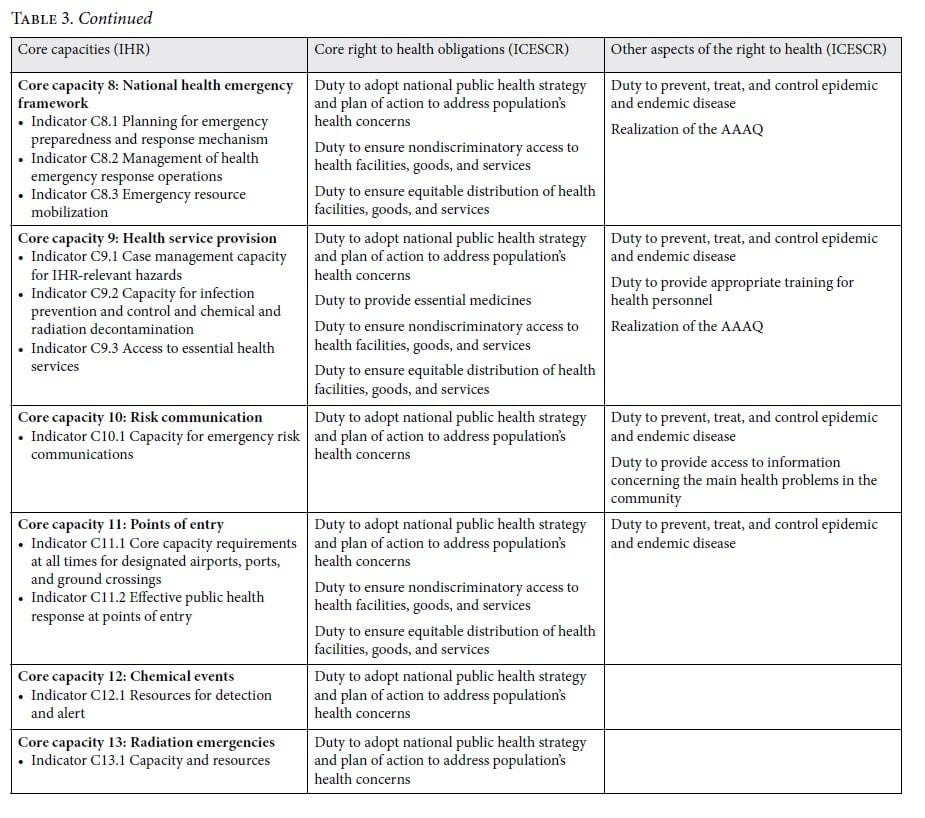
As Table 3 illustrates, there are considerable parallels between states’ obligations to have core capacities under the IHR and their “minimum core” and other obligations under the right to health. We argue in favor of more cross-fertilization between these two regimes. This regime interaction may enrich both frameworks from a normative perspective while also enhancing accountability, social justice, and public health outcomes.
Normative interaction may arise through a systemic interpretation of the IHR, whereby, according to article 31(3)(c) of the Vienna Convention on the Law of Treaties, “international standards may be interpreted in the light of any relevant rules of international law applicable in the relations between the parties.” The right to health clearly can be considered a relevant rule of international law that can assist in the interpretation of the IHR, particularly insofar as it underscores the importance of IHR duties from a human rights perspective. Table 3 offers a non-exhaustive illustration of obvious overlaps and synergies between right to health duties and IHR core capacities. For example, implementing the core obligation to ensure nondiscriminatory access to health care facilities, goods, and services would require explicit legal protection against discriminatory applications of pandemic-response legislation, such as emergency orders and lock-downs (core capacity C.1). It would also require explicit protection against discrimination in access to testing (core capacity C.5), surveillance (core capacity C.6), emergency resource mobilization (core capacity C.8), access to essential health services (core capacity C.9), and public health responses at points of entry, such as airports and border crossings (core capacity C.11).
The pressing need for strong human rights protections in these areas has been reinforced by the discriminatory applications of COVID-19 laws and policies in all of these core IHR domains, including disproportionate force in the enforcement of COVID-19 emergency orders against racial and ethnic minorities and the poor; unaffordable and unavailable testing and health care services; discriminatory enforcement of border restrictions; and failures to adequately consider nondiscrimination on the basis of disability or race in policies to address essential critical care during COVID-19 surges.34 The core obligation to ensure the equitable distribution of health care facilities, goods, and services holds similar cross-cutting relevance for many of these same parts of the IHR, including legislative frameworks and financing mechanisms (core capacity C.1), access to laboratory testing (core capacity C.5), human resources for implementation of IHR capacities (core capacity C.7), and emergency resource mobilization (core capacity C.8). Taking serious account of core right to health duties in the implementation of such IHR capacities would significantly enhance the fairness and efficacy of pandemic responses, with concrete benefits for public trust, social justice, and population health.35
At the same time, the comprehensive IHR framework gives more detail to the open-ended wording under the right to health framework and provides considerable clarification of states’ duty to prevent, treat, and control epidemic disease. For example, the core capacity requirement regarding access to essential health services during a disease outbreak (C.9) fills a key gap in core obligations under the right to health, which do not speak explicitly to this imperative.
Subsequently, recognition that the IHR core capacities might inform the content of the human right to health suggests that if states fail to comply with the IHR, they may be held accountable under the UN human rights regime (for example, the reporting procedures and individual complaint mechanisms of the CESCR, Convention on the Rights of the Child, CEDAW, and Convention on the Rights of Persons with Disabilities, as well as the UN Special Procedures). They may also be held accountable in domestic courts, as illustrated by successful human rights-based challenges to disproportionately forceful and restrictive COVID-19 lockdowns in Kenya and Malawi.36
More generally, there is an urgent need to perceive public health emergencies as a matter of international human rights obligations and accountability. The right to health means that governments should evaluate their preparedness for the next global public health emergency, whether it comes from within their own borders or from abroad. Governments should do so in close consultation with WHO, the most authoritative organization globally when it comes to infectious disease outbreaks, which has generated a wealth of expertise over the course of its existence. Given that WHO is unable to sanction, the ultimate consequence when states fail to comply with their obligations should be accountability under the UN human rights regime, in addition to domestic litigation.
Conclusion
The COVID-19 pandemic underscores the importance of more effective and more equitable disease control initiatives within and across borders. It also illustrates the challenges posed by the fragmented areas of international law relating to health and disease control. We suggest that the right to health offers principles and binding duties capable of achieving some extent of the systemic integration called for in 2006 by the International Law Commission.37 This idea finds support in international human rights law scholarship, with suggestions that the right to health could act as “a core, unifying standard” and “pillar” in international law related to health.38 As this paper indicates, taking the right to health seriously in the IHR could concretely improve the fairness and efficacy of the IHR and associated pandemic responses in ways that the COVID-19 pandemic has underscored are critically required.39 At the same time, the greater specificity of IHR duties gives more detail to the open-ended wording of the right to health, including by clarifying the state duty to prevent, treat, and control epidemic disease and suggesting that access to essential health services should appropriately be construed as a core obligation under the right to health. In particular, we hope that this analysis supports greater regime interactions in which human rights law is more seriously taken into account in the potential redesign of the IHR and in which responses to COVID-19 and future disease threats more concretely consider the right to health. This proposal is not simply legalistic: this time of significant upheaval underscores the imperative for pandemic responses to be rooted in socially just, humane, and cooperative domestic and global state actions. We believe that advancing a more integrated interpretation of the IHR and the right to health offers practical and policy-relevant pathways to achieve this outcome. This paper offers a preliminary sketch of some conceptual and institutional overlaps between these two regimes. The imperative for global health and human rights researchers is to advance this research to ensure that both the IHR and international human rights law are further developed to achieve these goals.
Acknowledgments
We thank Adriana Gonzalez for her editorial assistance. This article expands on a recent blog post by Brigit Toebes: “States’ Resilience to Future Health Emergencies: Connecting the Dots between Core Obligations and Core Capacities,” ESIL Reflections 9/2 (2020).
Brigit Toebes is Chair of Health Law in a Global Context in the Department of Transboundary Legal Studies, Faculty of Law, University of Groningen, Groningen, Netherlands.
Lisa Forman is Associate Professor and Canada Research Chair in Human Rights and Global Health Equity at the Dalla Lana School of Public Health, University of Toronto, Canada.
Giulio Bartolini is Associate Professor of International Law at Roma Tre University, Italy, and Coordinator of the EU Jean Monnet Project “Disseminating Disaster Law for Europe.”
Please address correspondence to Brigit Toebes. Email: b.c.a.toebes@rug.nl.
Competing interests: None declared.
Copyright © 2020 Toebes, Forman, and Bartolini. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction.
References
- P. Villareal, The (not so) hard side of the IHR: breaches of legal obligations (February 2020). Available at https://www.rug.nl/rechten/onderzoek/expertisecentra/ghlg/blog/the-not-so-hard-side-of-the-ihr-breaches-of-legal-obligations-26-02-2020.
- A. Buyse and R. de Lange, The Netherlands: Of rollercoasters and elephant (May 2020). Available at https://verfassungsblog.de/author/antoine-buyse.
- S. Sekalala, L. Forman, R. Habibi, and B. Meier, “Health and human rights are inextricably linked in the COVID-19 response,” BMJ Global Health 5:e003359 (2020), pp. 1–7.
- Vienna Convention on the Law of Treaties, No. 18232 (1969).
- A. L. Taylor, R. Habibi, G. L. Burci, et al., “Solidarity in the wake of COVID-19: Reimagining the International Health Regulations,” Lancet 396 (2020), pp. 82–83; R. Habibi, G. L. Burci, T. C. de Campos, et al., “Do not violate the International Health Regulations during the COVID-19 outbreak,” Lancet 395 (2020), pp. 664–666.
- United Nations Conference on International Organization, “Statement by Archbishop Spellman,” San Francisco, April 25–June 26, 1945; B. Toebes, The right to health as a human right in international law (Antwerp: Intersentia-Hart, 1999).
- Toebes (see note 6).
- Committee on Economic, Social and Cultural Rights (CESCR), General Comment No. 14, The Right to the Highest Attainable Standard of Health, UN Doc. E/C12/200/4 (2000); CESCR, General Comment No. 22, The Right to Sexual and Reproductive Health, UN Doc E/C.12/GC/22 (2016); Committee on the Rights of the Child, General Comment No. 15, The Right of the Child to the Enjoyment of the Highest Attainable Standard of Health, UN Doc. CRC/C/GC/15 (2013).
- Office of the United Nations High Commissioner for Human Rights, Status of ratification of human rights instruments interactive dashboard (2020). Available at https://indicators.ohchr.org.
- L. Gostin, “The international health regulations: Responding to public health emergencies of international concern,” in L. Gostin (ed), Global health law (Cambridge, MA: Harvard University Press, 2014), pp. 177–204.
- S. Negri, “Communicable disease control,” in G. L. Burci and B. Toebes (eds), Research handbook on global health law (Cheltenham: Edward Elgar Publishing, 2018), pp. 265–302.
- World Health Organization, International Health Regulations (2005).
- Ibid.; International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966).
- United Nations Population Fund, Programme of Action of the International Conference on Population and Development, Cairo, September 5–13, 1994, UN Doc. A/CONF.171/13 (1994); Declaration of Alma-Ata (1978).
- L. Forman, “What could a strengthened right to health bring to the post-2015 health development agenda? Interrogating the role of the minimum core concept in advancing essential global health needs,” BMC International Health and Human Rights 13/48 (2013).
- CESCR (2000, see note 8); CESCR (2016, see note 8); Committee on the Rights of the Child (see note 8); Forman (2013, see note 15); CESCR, General Comment No. 3, The Nature of States Parties’ Obligations, UN Doc. E/1991/23 (1990).
- K. Young, Constituting economic and social rights (Oxford: Oxford University Press, 2012); J. Tobin, The right to health in international law (Oxford: Oxford University Press, 2012).
- CESCR, General Comment No. 19, The Right to Social Security, UN Doc. E/C.12/GC/19 (2007); CESCR, General Comment No. 21, Right of Everyone to Take Part in Cultural Life, UN Doc. E/C.12/GC/21 (2009); CESCR, General Comment No. 25, On Science and Economic, Social and Cultural Rights, UN Doc. E/C.12/GC/25 (2020).
- Young (see note 17); Tobin (see note 17).
- Optional Protocol to the International Covenant on Economic, Social and Cultural Rights, UN Doc. A/RES/63/117 (2008).
- CESCR, Report on the Thirty-Eighth and Thirty-Ninth Sessions, UN Doc. E/C.12/2007/3 (2007).
- Ibid.
- L. Forman, “Can minimum core obligations survive a reasonableness standard? Analysing the future of right to health litigation at the United Nations Committee on Economic, Social and Cultural Rights,” Ottawa Law Review 47/2 (2016), pp. 557–573.
- CESCR (2000, see note 8).
- World Health Organization (2005, see note 12).
- L. Gostin and R. Katz, “The International Health Regulations: The governing framework for global health security,” Milbank Quarterly 94/2 (2016), pp. 264–313; G. Bartolini, Are you ready for a pandemic? The International Health Regulations put to the test of their “core capacity requirements” (June 2020). Available at https://www.ejiltalk.org/are-you-ready-for-a-pandemic-the-international-health-regulations-put-to-the-test-of-their-core-capacity-requirements.
- World Health Organization, State party self-assessment tool (2018). Available at https://apps.who.int/iris/bitstream/handle/10665/272432/WHO-WHE-CPI-2018.16-eng.pdf?sequence=1.
- Ibid.
- World Health Organization, Thematic paper on the status of country preparedness capacities (2019). Available at https://apps.who.int/gpmb/assets/thematic_papers/tr-2.pdf.
- Gostin and Katz (see note 26); A. Suthar, L. G. Allen, S. Cifuentes, et al., “Lessons learnt from implementation of the International Health Regulations: a systematic review,” Bulletin of the World Health Organization 96/2 (2018), pp. 110–121E.
- World Health Organization, Report of the Review Committee on Second Extensions for Establishing National Public Health Capacities and on IHR Implementation, WHO Doc. EB136/22 Add.1 (2015).
- World Health Organization, Joint External Evaluation (JEE) mission reports (2005). Available at https://www.who.int/ihr/procedures/mission-reports/en/; Centers for Disease Control and Prevention, The Joint External Evaluation (JEE) process: A project to assess and build global health security (2019). Available at https://www.cdc.gov/globalhealth/healthprotection/stories/global-jee-process.html.
- World Health Organization, Report of the Review Committee on the Functioning of the International Health Regulations (2005) in relation to Pandemic (H1N1) 2009, WHO Doc. A64/10 (2011).
- Human Rights Watch-India, COVID-19 lockdown puts poor at risk (2020). Available at https://www.hrw.org/news/2020/03/27/india-covid-19-lockdown-puts-poor-risk; J. Alindogan, HRW: COVID-19 lockdown violators in Philippines abused (2020). Available at https://www.aljazeera.com/news/2020/04/hrw-covid-19-lockdown-violators-philippines-abused-200429080703660; AllAfrica, Uganda: Police shoot two on Bodaboda for defying Museveni COVID-19 order (2020). Available at https://allafrica.com/stories/202003300087.html; L. Forman and J. Kohler, “Global health and human rights in the time of COVID-19: Response, restrictions and legitimacy,” Journal of Human Rights 19/5 (2020), pp. 1–10; Habibi et al. (see note 5); M. Shanouda and J. De Marinis, Proceed with caution with Ontario’s critical care triage protocol (2020). Available at https://policyoptions.irpp.org/magazines/september-2020/proceed-with-caution-with-ontarios-critical-care-triage-protocol.
- Sekalala et al. (see note 3).
- Law Society of Kenya v. Hillary Mutyambai and Ors Petition No 120 (2020); D. Pilling and J. Cotterill, Court suspends lockdown in Malawi (2020). Available at https://www.ft.com/content/b4d24171-c9ec-4ab0-bad0-55f3418c8fcb.
- International Law Commission, Fragmentation of International Law: Difficulties Arising from the Diversification and Expansion of International Law: Report of the Study Group of the International Law Commission, UN Doc. A/CN.4/L.682 (2006).
- Gostin (see note 10); B. Toebes, “Global health law: Defining the field,” in G. L. Burci and B. Toebes B (eds), Research handbook on global health law (Cheltenham: Edward Elgar Publishing, 2018), pp. 2–23.
- Human Rights Watch-India (see note 34); Alindogan (see note 34); AllAfrica (see note 34); Forman and Kohler (see note 34); Taylor et al. (see note 5).