Health Is a Human Right—at CDC?
Volume 21/1, June 2019, pp 163 – 177
Sarah S. Willen
Abstract
In 2013–14, the Smithsonian-affiliated David J. Sencer Museum at the US Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia, hosted an original exhibition with an eye-catching title: “Health Is a Human Right: Race and Place in America.” Given the American government’s entrenched resistance to health-related human rights claims, the staging of an exhibition with this title at a museum described as the public face of CDC was striking. Taking this apparent disjuncture as point of departure, this article examines the origins, aims, and content of the “Health Is A Human Right” exhibition, which attracted nearly 50,000 visitors in 2013–14. Drawing on qualitative research findings, the article engages three interrelated questions: First, how can this exhibition, in this particular locale, be reconciled—if at all—with the absence of any firm right to health commitment in the United States? Second, what does the exhibition reveal about the “social life” of health-related human rights claims? Finally, what might we learn from the exhibition about the potential role of museums and museology in sparking public engagement with health and human rights issues, especially in settings where human rights have some rhetorical power but lack legal or political traction?
Introduction
In 2013-14, the Smithsonian-affiliated David J. Sencer Museum on the main campus of the United States Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia, hosted an original exhibition with an eye-catching title, announced in bold in the opening panel: “Health Is a Human Right: Race and Place in America.” I learned of the exhibition purely by chance—by stumbling upon the website during a Google Search—in October 2013, a month after it launched. My response was a double-take: An exhibition called “Health Is a Human Right”—at CDC, the “nation’s premiere health promotion, prevention, and preparedness agency,” which operates under the federal Department of Health and Human Services?1 A few clicks through the exhibition website confirmed there was no mistake. A major exhibition—designed to chronicle the enduring health impact of over a century of discriminatory laws, policies, and practices in the United States—had been launched to commemorate the 25th anniversary of CDC’s Office of Minority Health and Healthy Equity (OMHHE). It would be on display through spring 2014.
As a medical anthropologist with a longstanding interest in health and human rights, I was intrigued—and perplexed. The staging of an exhibition with this title at the federally operated museum described as the “public face” of CDC was surprising in light of the US government’s deep resistance to human rights claims-making on American soil and the limited power of health-related human rights claims in American civil society more broadly.2 In national debates about health care reform, for instance—including those culminating in the 2010 Affordable Care Act (ACA)—health and human rights claims had failed to gather much momentum.
In the following months, and with support from its CDC creators, an ethnographic study took shape with the exhibition as its focus. In this article, I triangulate among several forms of qualitative data gathered as part of that study to engage three interrelated questions. First, how can the exhibition’s title and location in a federal government museum be reconciled, if at all, with the absence of any firm right to health commitment on the part of the United States? Second, what does this exhibition reveal about what anthropologists describe as the “social life” of health-related human rights claims, including both the surprising routes through which human rights “travel” and their prominent role as a contemporary “idiom of social justice mobilization” for health?3 Finally, what might we learn from this exhibition about the potential role of museums and museology in sparking public engagement with health and human rights issues, especially in settings where human rights have some rhetorical power but lack widespread legal or political traction?4
Before turning to the exhibition itself, let us first reflect briefly on its title and, in particular, on the fact that a US federal agency had created a major exhibition that pivoted, or at least appeared to pivot, on the claim that health is a human right. Almost 170 countries have ratified the International Covenant on Economic, Social Cultural Rights (ICESCR), but the United States is not party to the ICESCR or most other international legal instruments in which a right to health is declared or defined. Neither is a right to health articulated in the US Constitution or federal law. Instead, successive presidential administrations have avoided establishing obligations, domestic or global, in the realm of economic, social, and cultural rights.5 Moreover, the United States has a long history of advancing laws and policies that commoditize health care and privatize its provision. Globally, it has promoted these neoliberal strategies in foreign policy and through its role in international institutions like the World Bank and the International Monetary Fund.6 Civil society actors in the United States have found it difficult to stake health-related human rights claims, although the appeal of right to health claims has broadened among politically liberal segments of the American public since the 2016 presidential election cycle.7 Overall, however, the American government, and society more broadly, has yet to reckon fully with the country’s long history of health-related human rights violations against citizens and others.8
Against this backdrop, the launch of an exhibition titled, “Health Is a Human Right” at a federal museum—a well-situated venue that welcomes approximately 95,000 visitors per year, as the curator told me—raises multiple questions. Why would OMHHE choose to frame their commemorative anniversary exhibition in this way? How did the theme of human rights find expression in the exhibition? Who was the intended audience, and what response did it garner—either internally, at CDC, or from other members of the visiting public? With these questions in mind, the first aim of this article is to document and reflect on the exhibition’s origins, design, content, and objectives.
The article also has a second aim: to consider the power, and the limits, of a health and human rights framework for catalyzing discussion about health, history, and inequity in the United States. In pursuing this aim, I draw on the interdisciplinary tradition of critical human rights scholarship, which takes strong cues from anthropology and attends carefully to what Richard Wilson calls the “social life of rights.”9 From a “social life of rights” standpoint, the title and exhibition offer a unique opportunity to consider how human rights can “travel” far from their juridical origins and play new roles in distinctly non-legal settings.10 As Tine Destrooper puts it, “human rights can no longer be considered merely as a matter of international law (if this was indeed ever possible)”; rather, “there is a wide range of ways in which to employ human rights, from the use of human rights language as a tool for explicit and formal mobilization to the invocation of human rights values without direct reference to their legal and institutional grounding.”11 This orientation helps clarify both the tension and the power invoked by the exhibition’s titular claim that “health is a human right.” Rather than testing the strength or validity of such a claim in legal terms, a “social life of rights” perspective instead invites recognition that this claim is a tool that can be deployed, to different ends, by different stakeholders.
Specifically, this approach invites us to consider how the claim that “health is a human right” can function as what I describe elsewhere as an “idiom of social justice mobilization” for health: a model, or framework, for thinking about the relationship between health and (in)justice.12 The term “idiom” evokes a language—a mutually accessible way of organizing thought and consolidating interest and commitment. Arguably, some fields of research, scholarship, and practice themselves function as idioms of social justice mobilization for health: social medicine, social epidemiology, medical humanitarianism, and global health come to mind. Other idioms can better be described as models or conceptual frameworks, including the social determinants of health, the notion of health equity, the concept of structural racism, and claims of a human right to health. Alongside these disciplinary and conceptual idioms are another sort: idioms that emerge at a particular historical moment and function as “branded strateg[ies] for advancing a particular set of ethical or political commitments.”13 Examples include the Alma-Ata commitment to “Health for all by the Year 2000,” the World Health Organization’s “3 by 5 Initiative,” and the United Nations’ “Millennium Development Goals.”
From a critical human rights standpoint, these diverse idioms of social justice mobilization for health are far more than just “buzzwords.”14 Each is a powerful—and distinct—conceptual framework with its own genealogy, disciplinary orientation, and community of practice. Each takes a different tack in trying to debunk claims that health disparities are somehow “natural” or beyond the scope of human intervention. And each strives to catalyze a somewhat different kind of action. Although different idioms of social justice mobilization stand in variable relation to one another, they often are invoked together—including, at times, with other idioms that stem from very different disciplines, espouse different core principles, and advance different strategic aims.
As the CDC Museum’s exhibition clearly demonstrates, idioms of social justice mobilization seldom stand alone. Rather, different idioms of social justice mobilization for health—for instance, health equity, structural racism, social determinants of health, and the notion of a right to health—can travel together, at times complementing and clarifying one another, at other times in clear tension. When viewed through this lens, the exhibition provides an opportunity to reflect critically on the conceptual and discursive challenges of using human rights to frame conversations around health and justice in a world riven by economic inequality, political instability, and deficient leadership—especially, but by no means exclusively, in the United States.
In what follows, I begin with a brief discussion of research methods, then turn to the larger story of the exhibition, including its roots in OMHHE. I include photographs to give readers a glimpse into visitors’ experience and a sense of the exhibition’s size and scope. In concluding, I return to the article’s opening questions about how the claim that “health is a human right” can become untethered from law and juridical practice and function, instead, in the social realm—as an idiom for social justice mobilization for health. The article closes with a brief discussion of lessons we can learn from this unique exhibition about the role museums and museology might play in catalyzing public engagement with matters of health and human rights concern.
Research methods
This article draws on findings from an ethnographic study of the CDC Museum’s “Health Is a Human Right” exhibition, located in CDC’s secure federal facility in Atlanta, Georgia. Research methods included (1) three tours of the exhibition, including one curator-guided tour; (2) semi-structured interviews and multiple informal conversations with the chief architects of the exhibition—the director of OMHHE and the Sencer Museum curator—as well as other CDC staff; and (3) semi-structured interviews with two university faculty who required their students to visit the exhibition. Interviews were audio recorded, transcribed, and analyzed using the Dedoose qualitative software platform. Additional resources accessed include (4) worksheets used by the curator and her team to develop the exhibition panels; (5) the accompanying exhibition text (80 single-spaced pages); (6) audio-visual records of the exhibition, including photographs and videos; and (7) the transcript of an online discussion on a CDC staff listserv that was prompted by the exhibition.
In addition, I have followed the exhibition into its second (physical) and third (online) iterations. In 2017, CDC took the first-ever step of gifting portions of exhibition material to Georgia State University, also in Atlanta, which modified it for display at the university’s school of public health. The Georgia State library also created a condensed version that is accessible online.15
This study was deemed exempt by the Institutional Review Board at the University of Connecticut.
A celebratory exhibition
“Health Is a Human Right: Race and Place in America” was created to commemorate the 25th anniversary of OMHHE, an office established in 1988 in direct response to a 1985 landmark report issued by the US Department of Health and Human Services (HHS): the Report of the secretary’s task force on black and minority health, commonly known as the Heckler Report.16 The origins of the report, and of OMHHE, illuminate the complex ways in which science, politics, and personal values can become entangled in a manner that directly affects health policy and, ultimately, population health.
When Margaret Heckler was appointed secretary of Health and Human Services by President Ronald Reagan in 1983, the Republican from Massachusetts had no experience in public health. The impact of the eight-volume report she commissioned during her tenure, however, would be difficult to overstate. First, the Heckler Report offered the first formal recognition from HHS that vast and deep-rooted population-level health disparities exist in the United States, noting that each year, African Americans suffer 60,000 excess deaths relative to the US population as a whole. In her foreword to the volume, Heckler describes this as “a sad and significant fact.” She continues:
I felt—passionately—that it was time to decipher the message inherent in that disparity. In order to unravel the complex picture provided by our data and experience, I established a Secretarial Task Force whose broad assignment was the comprehensive investigation of the health problems of Blacks, Native Americans, Hispanics and Asian/Pacific Islanders.17
In effect, the Heckler Report explicitly defined health disparities as what would be described in early 21st century terms as “inequities”—in other words, as differences that are not simply “unnecessary and avoidable,” but “also considered unfair and unjust.”18
In the decades that followed its publication, the Heckler Report became widely recognized as “a transformative, driving force for change” not simply because of its innovative science, but also because of the way it put epidemiology and public health to work in the service of ethical aims. As one national public health leader put it, the report
influenced many milestones in the health equity movement: pivotal legislation, funding, policies, research, and initiatives focused on minority health and health equity; establishment of offices of minority health within NIH, the Centers for Disease Control and Prevention, and the Health Resources and Services Administration; more inclusive data collection techniques; dedicated institutions, centers, commissions, and state, territorial, and local offices of minority health across the country; and innovative community-level interventions.19
The establishment of the Office of Minority Health at CDC in 1988—an office whose mandate was expanded in 2011 to include health equity and again in 2018 to include women’s health—was thus one direct outcome of the Heckler Report.20 Now identified as OMHHE, its mission is to “Advance health equity and women’s health issues across the nation through CDC’s science and programs, and increase CDC’s capacity to leverage its diverse workforce and engage stakeholders toward this end.”21
Despite the Heckler Report’s resounding impact, critics saw it as a missed opportunity to define these newly documented disparities as violations of human rights. In fact, doing so would have been foreign to Heckler, whose keynote at the first International AIDS Conference in Atlanta in 1985 could not be described as comporting with human rights principles. In a departure from her prepared speech, Heckler told the assembled gathering: “We must conquer AIDS before it affects the heterosexual population and the general population…. We have a very strong public interest in stopping AIDS before it spreads outside the risk groups, before it becomes an overwhelming problem.”22
The making of the exhibition
The 25th anniversary of OMHHE, the director explained in a 2014 interview, was an important occasion to celebrate, both at CDC and for the broader public. As such, it was a key opportunity to partner with the David J. Sencer Museum, which was created in 1996 and later named to honor the agency’s longest serving director.
The museum is both accessible (after passing through a security checkpoint) and free to the public, and its 5,000 square-foot, two-level gallery is immediately visible to anyone arriving at the agency’s main entrance. The lower level contains a permanent exhibit about the history of CDC. The much larger, entry-level gallery hosts temporary exhibitions on topics ranging from specific diseases like cancer and Ebola, to vulnerable communities like refugees and physical laborers (in mining, fishing, agriculture, construction, and other industries), to more conceptual themes, such as the relationship between art and science.23 Some are visiting exhibitions, while others are created at CDC, but all use museological strategies to invite reflection on issues of social, medical, scientific, and moral concern. As the curator explained to me, the museum’s estimated 95,000 visitors per year, including nearly 50,000 to this exhibition, are diverse, including CDC staff, visiting public health professionals and experts, students, and members of the general public. “We get a lot of people that are just fascinated by CDC,” she explained. These include leisure travelers who tour the United States by RV [recreational vehicle] and, in recent years, visitors interested in The Walking Dead—a television series with scenes set at CDC headquarters.
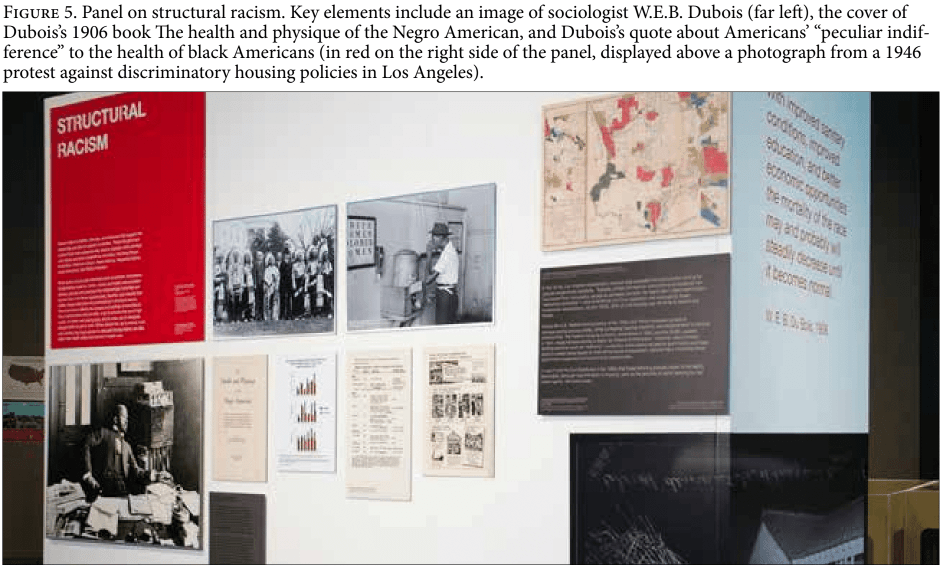
Although different in some ways from its other exhibitions, “Health Is A Human Right” was consistent with the Sencer Museum’s mission as the “public face” of CDC. According to the OMHHE director, it sought to counter the commonly held but mistaken view “that health disparities, particularly racial and ethnic health disparities, are intractable, or resistant to change.”24 She noted that strong evidence to the contrary had existed for well over a century and pointed, in particular, to the work of sociologist W.E.B. Dubois, whom I heard the curator describe on an exhibition tour as “the grandfather of the social determinants of health.” As early as 1899, Dubois expressed public dismay over the “peculiar indifference” displayed by those in power toward black Americans.25 In a 1906 passage displayed prominently in the exhibition (see Figure 6), he made the strong claim that, “With improved sanitary conditions, improved education, and better economic opportunities, the mortality of the [black] race may and probably will steadily decrease until it becomes normal.”26 While guiding a tour, the curator asked for a volunteer to read this quotation aloud.
Not unlike Dubois, who brought sociological insight to bear in critiquing racial injustices in health in his own day, the OMHHE director anchored her vision in her training as both a public health professional and an anthropologist. Her declared goals for the exhibition were to (1) clarify for visitors the root causes of health disparities; (2) put disparities into historical context; and (3) “put a face on the data” in order to help data-oriented public health professionals and community members stretch their imaginations and “really see what those disparities look like.” She also wanted to recognize the work of advocates and activists who struggle to protect themselves and their communities, especially communities marginalized and impoverished as a result of political and policy decisions. By drawing attention to activist struggles, including struggles against powerful elites, corporate entities, and even government officials, she hoped the exhibition would “dispel the idea that people facing disadvantage don’t care” about the poor conditions and concomitant health risks they endure. The final aim of the exhibition, she explained, was to “show visually how much work needs to be done” before the goals of her office will be achieved.
As federal government employees, the chief architects of the exhibition—namely, the director of OMHHE and the Sencer Museum curator—faced challenges that differ markedly from those faced by most health and human rights advocates. In particular, they grappled with the best way to reflect on raw and painful episodes in recent history “in a very responsible but pointed way … in a way that is mobilizing, that is, that’s not divisive.”
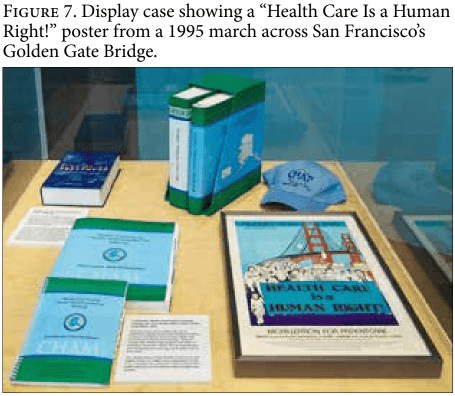
Even in 2013, when the exhibition launched, this was a tall order. Congress had passed the Obama administration’s ACA by a razor-thin majority in 2010. When implementation began in 2014, the heated national debate was ongoing. In that moment, when arguing about access to health care was highly divisive, the director saw the exhibition as an important opportunity to call attention to the broad conditions that support health, on one hand, while avoiding debates about health care, which the ACA treated as a commodity, on the other. In keeping with these goals, the exhibition approached health in a manner that extended well beyond questions of access to care. It explored the enduring impact of policy decisions on population health; the historical intertwinement of policy sectors; and watershed moments in which advocacy and activist efforts sparked new conversations, laws, ways of thinking about evidence, and modes of political action. By juxtaposing visual representations of data with photographs, videos, interactive touch screens, artifacts, and art, the exhibition historicized key events and humanized population-level processes in an effort to bring them alive for visitors. Civil rights struggles were front and center. Beyond the title and opening panel, the proposition that health is a human right appeared just once, on a poster for a 1995 march across the Golden Gate Bridge in San Francisco (Figure 7). The closest the exhibition came to staking a human rights claim involved an aspirational statement in the closing panel: “Restricted access to the conditions needed for health is a human rights issue—one that has characterized the past, but doesn’t have to be repeated in the future.”
Health, rights, and museology
The photographs included here cannot convey the detail, aesthetics, or multimedia dimensions of a major museum exhibition like this one. Nonetheless, they suggest the choices and decisions of the curator and her working group as they sought to render OMHHE’s vision both engaging and accessible.
Although the exhibition’s core vision and major funding came from OMHHE, with support from the California Endowment, the design and content were in the hands of the curator, who has curated the museum’s temporary and permanent exhibitions since 2002. Unlike most of her colleagues, she did not come to CDC with a background in public health. Trained in musicology, museum studies, and museology, she has worked as an art and history curator throughout her long career. She and a team of “subject matter experts” spent two years conducting research, planning the exhibition, and obtaining artifacts and permissions. For her, the goal of the exhibition was “to connect the dots between the social determinants of health and health outcomes.”
Where people live, and work, and how much money they make, and environmental justice, and their education, and last but not least access to health care, that is all critical to health outcomes. … [I]f nothing else, I wanted people from this exhibition to really understand those linkages.
She decided that the best way to convey these interconnections was to organize exhibit sections around different social determinants of health.
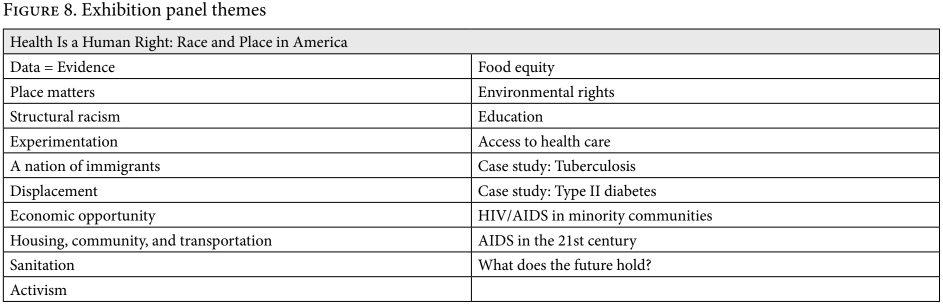
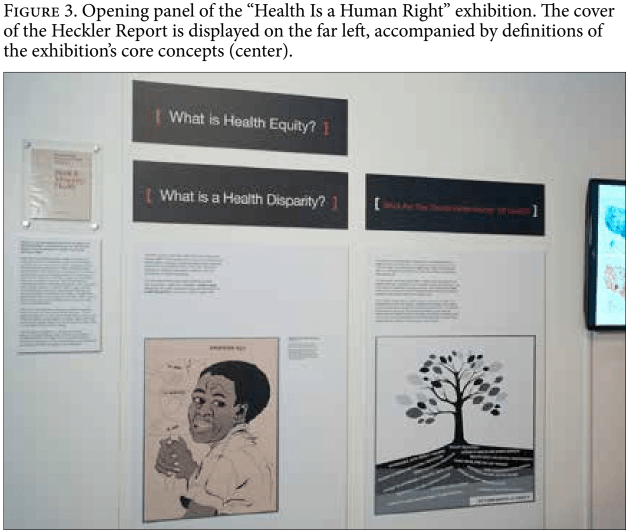
Figure 8 lists the themes and historical episodes represented in the exhibition’s 20 panels, which concentrated on 20th century events. The opening panels introduced and defined key terms and concepts like “health equity,” the “social determinants of health,” and “structural racism,” and demonstrated their relevance using visual representations and historical artifacts. Notably, the “right to health” was not among them, nor did the exhibit reference any fundamental health and human rights documents such as the UDHR, ICESCR, or General Comment 14.
From the curator’s perspective, another early panel—“Data=Evidence”—was vital. She explained: “[In] public health, and this has been drummed into me since I’ve been at CDC, if you can’t measure the problem, you can’t come up with solutions … Everything at CDC and public health is data driven and it’s evidence driven.” To assimilate the exhibition’s visual content and understand CDC’s role, she explained, visitors would need a basic familiarity with principles of scientific research and evidence.
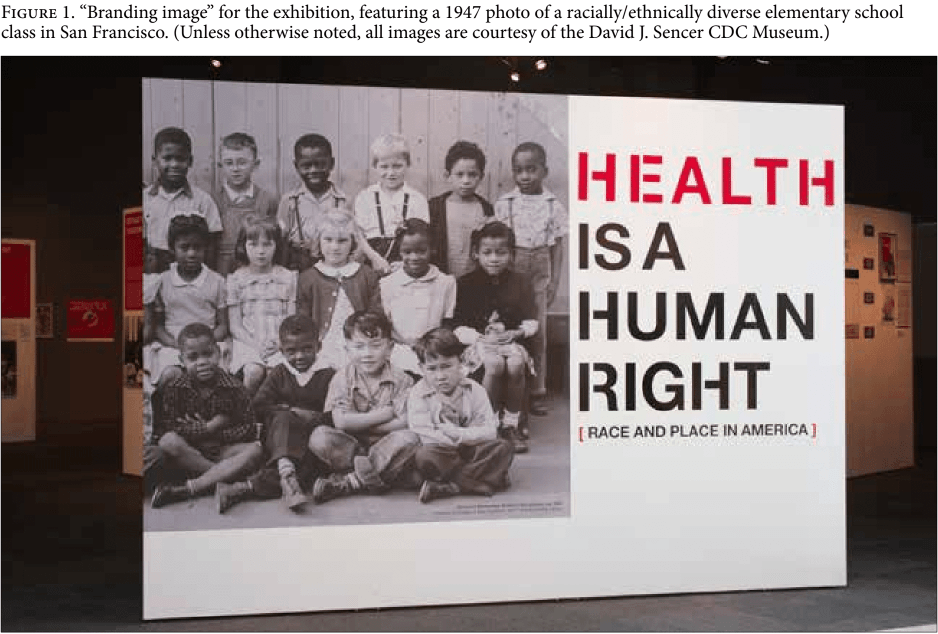
Although some issues received less attention than she would have liked—disability, for instance, and the experiences of LGBT Americans—the curator was generally pleased with the way the exhibition came together, especially with the “branding” image that greeted in-person and online visitors to the exhibition: a 1947 black-and-white photograph of a racially/ethnically diverse elementary school class in San Francisco (Figure 1). She explained:
It’s really important as an art curator, doing history, to develop visually impactful exhibitions. Most visitors won’t read much of the text, so we depend on visual strategies to tell the stories we want to convey. Case in point is Health Is a Human Right. You saw the text. I had no expectation anybody would come into this gallery and read all of it.
To transcend the limitations of text, she chose a striking, memorable image laden with historical and moral meaning. This image oriented visitors to a vision of the United States as a land of diversity, past, present, and future, she explained, and it exemplified the exhibition’s overarching moral message:
At the end of the day, it’s the children we need to care about because they represent the future. In just a few years, the United States is going to be a majority-minority country. Not only is addressing health inequities the moral thing to do, but it’s also the practical thing to do.
As the curator’s comments make clear, creating a museum exhibition like this one involves striking a balance between aesthetic, professional, and institutional considerations, as well as moral ones. To understand the design of the exhibition and its title, we need to keep in mind the role of the curator and the curatorial logic at play.
Guiding themes: Human rights violations and the power of collective action
Two key themes were especially prominent. First, although its title claim was not elaborated in the panels themselves, the resonance between health-related human rights violations and the exhibition’s content and framing concepts—“health equity,” “social determinants of health,” and “structural racism”—was unmistakable. Indeed, the exhibition was full of concrete evidence of specific instances that can be and have been described as human rights violations:
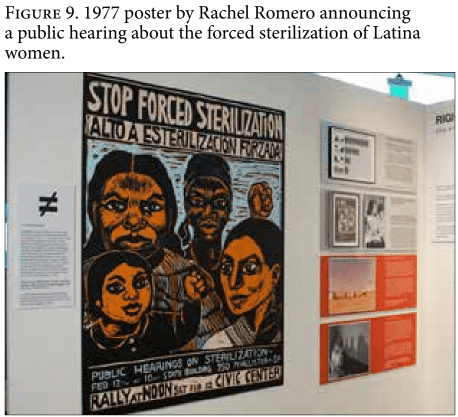
- the forced sterilization of women, many of them poor, institutionalized, and/or people of color;
- the forced relocation of American Indians from their tribal lands;
- the forced relocation of African American sharecroppers in the South;
- the internment of Japanese Americans during the Second World War; and
- medical experiments on vulnerable populations both before and after the Second World War atrocities litigated at Nuremberg, including the US Public Health Service Syphilis Study at Tuskegee, as well as the testing of isoniazid, an antibiotic developed to treat tuberculosis, on members of the Navajo nation.
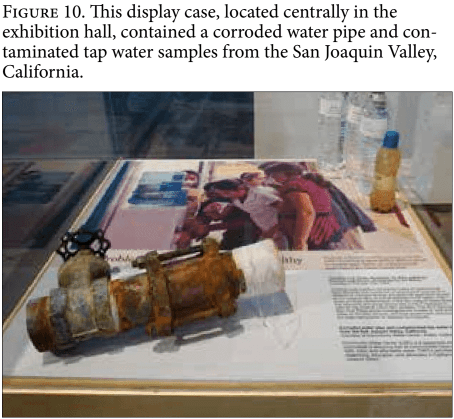
Another section, on sanitation, noted that, “Today more than 639,000 households lack indoor plumbing,” and that some people—many of them in “rural and urban communities in Alaska, southern California, rural areas of Appalachia, the colonias along the US-Mexico border, U.S. territories, and Indian reservations”—still lack access to water that is reliably safe and drinkable. Notably, the exhibition had been open to the public for more than six months on April 25, 2014—the date on which officials in Flint, Michigan, announced the city had switched its water supply from the city of Detroit to the Flint River, a decision that catalyzed a slow-moving catastrophe that continues to damage the city’s infrastructure, economy, and residents’ health.27
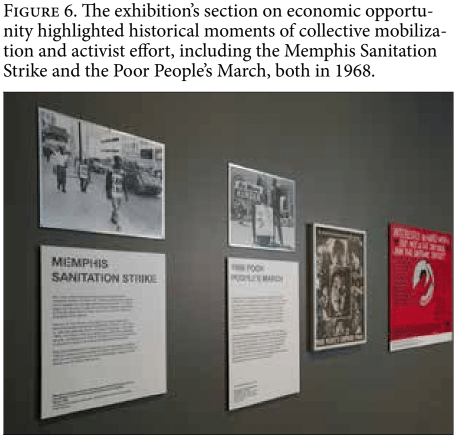
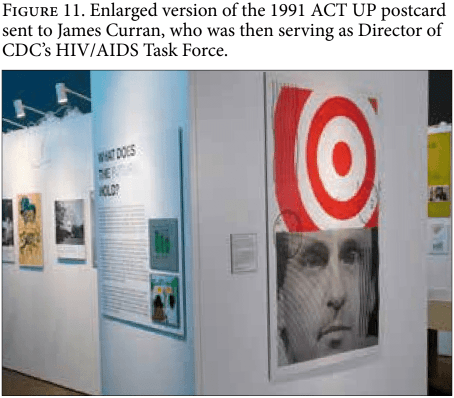
The exhibition involved a second central theme: It called attention to cases in which activists achieved change by exerting pressure on powerful actors and institutions. Exhibition panels highlighted a number of mid-century activist efforts, including the Memphis Sanitation Strike and the Poor People’s March, both of which took place in 1968. More recent movements were also featured, including a 1990-91 campaign by the AIDS activist group ACT UP. Founded in 1987 in New York, ACT UP, or the AIDS Coalition to Unleash Power, emerged as the AIDS crisis was devastating the US gay population, and before much was known about the disease. Strikingly, this section of the exhibition documents action taken by activists against CDC itself. The campaign’s signature image—of James Curran, who then served as head of CDC’s HIV/AIDS Task Force, beneath a red and white bulls-eye—was virtually impossible to miss. A caption explained:
In December 1990, ACT UP took on CDC when it staged a protest outside of the agency’s headquarters. The key issue: expansion of the case definition of AIDS to include infections specific to women and others. After the CDC protest in Atlanta, ACT UP relentlessly continued its actions, including sending 20,000 graphic postcards to Dr. James Curran, CDC’s HIV/AIDS Task Force Director [in 1991]. In 1993, once the data supported the change, CDC did expand the case definition of AIDS to reflect the fuller spectrum of the disease.
The panel text ends with requisite deference toward CDC’s reigning epistemology—that is, the impossibility of changing a case definition, or shifting the flow of resources, without rigorous scientific evidence—but it tells a very different story as well. Although the urgency and terror of the unfolding AIDS crisis may be receding into historical memory, the impact of the epidemic on the gay community in the 1980s and 1990s is difficult to overstate. Furthermore, the devastation wrought by the AIDS epidemic around the globe was a key catalyst for the health and human rights movement that exists today.28
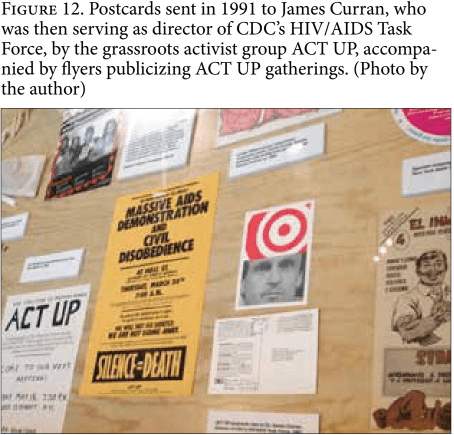
For both of these reasons, it made sense to highlight the role of grassroots and civil society activism in pushing leaders to focus on the disease. Given CDC’s central role in shaping HIV research and policy both in the United States and globally, it also made sense to display material evidence of the ACT UP campaign. Yet these goals could have been achieved quietly, for instance simply by putting campaign postcards or flyers on display (see Figure 12). The exhibition went several steps further. By giving a blown-up image of the controversial postcard central billing in the final section of the exhibition, and by contextualizing it with a passage about the tenaciousness and temerity of ACT UP activists, it conveyed another message as well: CDC is the government, and its authority is rooted in science, evidence, and power. And CDC, like the other US government agencies, is both fallible and amenable to change—including, at times, change driven by grassroots collective action.
No part of this message was cast in human rights terms. At the same time, it is consistent with both the spirit and the letter of core human rights commitments, including the right to participation and a raft of other rights enumerated in the UDHR and other key covenants and treaties.
Conclusion
In this article, I have pursued three questions and close by addressing each in turn. First, how might museums and museology spark public engagement with health and human rights issues, especially in settings where human rights hold some rhetorical power, but lack legal or political traction? As this exhibition shows, museums—especially those that use multimedia such as audio, video, interactive touch screens, and historical artifacts—are able to marshal visual and aesthetic resources that remain inaccessible to those who typically read, and write for, journals like this one. Museum exhibitions can introduce instances of health-related human rights violation, and instances of collective action and activism, to large audiences spanning different ages, life stages, and educational levels. Of course, such efforts require heavy investments of time, research, money, and human effort. They also demand the requisite professional skills, including an acute sense of visual literacy and a recognition that textual explanation is both necessary and limited in its potential impact. As more museums take up human rights concepts and themes—among them the National Center for Civil and Human Rights in Atlanta and the Canadian Museum for Human Rights in Winnipeg—it will be illuminating to reflect comparatively on the range of available tools, strategies, and successes. While there are good reasons to avoid imposing mechanisms of audit culture on aesthetic institutions, it bears mention that comparative effort may be limited by museums’ inability to systematically gather visitor reactions and feedback, as they are at the Sencer Museum.29
Second, what happens when we approach the assertion that health is a human right not simply as a juridical claim, but as a proposition with a “social life” of its own? As I propose elsewhere, the right to health should be explored ethnographically, “in all its guises: as a legal instrument, a social object, a rhetorical flourish, a node of contingent and precarious political consensus, a framework for translating theory into practice, and, finally … a contemporary idiom of social justice mobilization.”30 Many of these uses stand in tension with human rights claims rooted in legal instruments and juridical norms. For some health and human rights advocates, such non-juridical invocations are problematic. One of the Atlanta-based health and human rights experts I interviewed wondered before viewing the exhibition about the “elephant in the room”—that is, “how is the US government going to talk about health as a human right” given the “official party line … that we do not believe that such a thing … exists?” The exhibition’s inattention to “anything that anybody that has a human rights background would expect to see,” including relevant “international covenants, conventions, and treaties and monitoring bodies, and reporting mechanisms,” was described as troubling. Another expert noted after visiting the exhibition that it “doesn’t really help in terms of understanding the health and human rights linkage,” adding that “it’s okay” because “it reflects well on CDC just to have that title, and to let people know that CDC is interested in human rights.”
Whether the latter interpretation held sway among CDC staff is another question altogether. Soon after the exhibition launched, a heated, mostly anonymous debate unfolded on an internal CDC listserv in a tone that ranged from didactic, to funny, to caustic. In this online discussion, which involved approximately 15 participants (and which I was able to review some months later as a printed PDF), the exhibition itself went largely unmentioned. Central topics of debate included the new ACA legislation; proposals to redistribute wealth and associated political and ethical dilemmas; and the relevance of individual behavior and personal choice to health. Another topic of discussion involved the fundamental question prompted by the exhibition title: “Is health a human right?” Some participants in the online debate argued strongly in favor, while others took either a more ambivalent or an opposing stance. Two points were especially clear in this online conversation. First, CDC personnel hold divergent views on whether or not health is a human right. Second, it is not clear that the exhibition changed many minds. In short, the listserv debate reflected the fact that individual government agencies, like governments themselves, are not monoliths. Rather, they are comprised of individual people who hold a range of ideological positions.
This brings us to our third and final question: How can this exhibition, in this locale, be reconciled with the lack of any firm right to health commitment in the United States? From a juridical standpoint, it cannot. The exhibition “went through all of the reviews and clearances,” the OMHHE director explained, yet “it’s nothing that anyone expected to see at the CDC.” Even so, she continued, “people were happy about that.” Despite the title’s lack of legal grounding, and despite clear differences among CDC staff, the exhibition’s architects reported a strong, intuitive sense of congruence between the title and their professional aims to educate and inspire. Indeed, the title’s insistence that “health is a human right” shows how this claim can function as an idiom of social justice mobilization alongside, albeit in tension with, other idioms such as “health equity” and the “social determinants of health.” Perhaps the strongest evidence of this interpretation lies in a 2013 conversation between the curator and Michael Marmot, who chaired the WHO Special Commission on the Social Determinants of Health, and who has avoided framing his own goals in human rights terms.31 The curator recounted their conversation during his visit to the exhibition, delighting in his positive feedback: “You talk about human rights, then don’t bring it up again,” she remembered him saying. He continued: “I would have done the same.”
Acknowledgments
Thanks are due to the Human Rights Institute at the University of Connecticut for research support, to Dr. Leandris Liburd and Louise Shaw for facilitating the research that produced this essay, and to two anonymous reviewers for their critical feedback. An earlier version of this piece was presented to the Working Group on Anthropology and Population in the Department of Anthropology at Brown University.
Sarah S. Willen, PhD, MPH, is an associate professor of anthropology and director of the Research Program on Global Health and Human Rights at the Human Rights Institute, University of Connecticut, Storrs, Connecticut, United States.
Please address correspondence to Sarah S. Willen. Email: sarah.willen@uconn.edu.
Competing interests: None declared.
Copyright © 2019 Willen. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- Centers for Disease Control and Prevention, Our History – Our Story. Available at https://www.cdc.gov/about/history/index.html.
- CDC David J. Sencer Museum, About the David J. Sencer CDC Museum. Available at https://www.cdc.gov/museum/about.htm.
- R. A. Wilson, “Afterword to ‘Anthropology and human rights in a new key’: The social life of human rights,” American Anthropologist 108 (2006), pp. 77–83; S. E. Merry, “Preface,” in T. Destrooper and S. E. Merry (eds), Human rights transformation in practice (University of Pennsylvania Press, 2018); S. S. Willen, M. Knipper, C. E. Abadía-Barrero, et al., “Syndemic vulnerability and the right to health,” The Lancet 389 (2017), pp. 964–977.
- G. MacNaughton, M. McGill, A. Jakubec, et al., “Engaging human rights norms to realize universal health care in Massachusetts, USA,” Health and Human Rights Journal 20/2 (2018); M. McGill, “Human rights from the grassroots up: Vermont’s campaign for universal health care,” Health and Human Rights: An International Journal 14 (2012); A. C. Finnegan, and S. K. White, “Vermont and healthcare reform organizing: Human rights promise and praxis,” Journal of Human Rights Practice 8/1 (2016), pp. 148–170.
- W. T. Armaline, D. S. Glasberg, and B. Purkayastha, Human rights in our own backyard: Injustice and resistance in the United States (University of Pennsylvania Press, 2011); S. Hertel, and K. Libal, Human rights in the United States: Beyond exceptionalism (Cambridge University Press, 2013).
- M. Basilico, J. Weigel, A. Motgi, et al., “Health for all? Competing theories and geopolitics,” in Reimagining global health (University of California Press, 2013), pp. 74–110.
- McGill (see note 6); G. MacNaughton, and M. McGill, “Economic and social rights in the United States: Implementation without ratification,” Northeastern University Law Journal 4 (2012), p. 365; Associated Press, “Sanders unveils bill, saying ‘health care is a human right,’” New York Times, April 10, 2019.
- J. C. Carmalt, S. Zaidi, and A. E. Yamin, “Entrenched inequity: Health care in the United States,” in S. Hertel and K. Libal (eds), Human rights in the United States: Beyond exceptionalism (Cambridge University Press, 2011); A. M. Brandt, “Racism and research: The case of the Tuskegee syphilis study,” The Hastings Center Report 8/6 (1978), pp. 21–29; S. M. Reverby, “Listening to narratives from the Tuskegee syphilis study,” The Lancet 377/9778 (2011), pp. 1646–1647; S. Reverby, “Reflections on apologies and the studies in Tuskegee and Guatemala,” Ethics & Behavior 22 (2012), pp. 493–495; K. S. Ratcliff, “Health and human rights,” in W. T. Armaline, D. S. Glasberg and B. Purkayastha (eds), Human rights in our own backyard: Injustice and resistance in the United States (University of Pennsylvania Press, 2011); N. L. Novak, N. Lira, K. E. O’Connor, et al., “Disproportionate sterilization of Latinos under California’s eugenic sterilization program, 1920–1945,” American Journal of Public Health 108/5 (2018), pp. 611–613; A. Stubblefield, “‘Beyond the pale’: Tainted whiteness, cognitive disability, and eugenic sterilization,” Hypatia 22/2 (2007), pp. 162–181.
- R. Wilson (see note 3).
- S. E. Merry (see note 3); S. S. Willen, “Do ‘illegal’ migrants have a ‘right to health’? Engaging ethical theory as social practice at a Tel Aviv open clinic,” Medical Anthropology Quarterly 25/3 (2011), pp. 303–330; R. A. Wilson, and J. P. Mitchell, “Introduction: The social life of rights,” in R. A. Wilson and J. P. Mitchell (eds), Human rights in global perspective: Anthropological studies of rights, claims, and entitlements (Routledge, 2003); W. T. Armaline, D. S. Glasberg, and B. Purkayastha, The human rights enterprise: Political sociology, state power, and social movements. (Wiley, 2015); M. Goodale, “Toward a critical anthropology of human rights,” Current Anthropology 47 (2006), pp. 485–511; T. Destrooper, and S. E. Merry (eds), Human rights transformation in practice (University of Pennsylvania Press, 2018), p. 278.
- T. Destrooper, “Introduction: On Travel, Translation, and Transformation,” in S. E. Merry and T. Destrooper (eds), Human rights transformation in practice (University of Pennsylvania Press, 2018), p. 2.
- Willen et al (see note 3); Willen (see note 11); S. S. Willen, Fighting for dignity: Migrant lives at Israel’s margins (University of Pennsylvania Press, forthcoming 2019).
- Willen (see note 11), p. 306.
- A. Cornwall and K. Brock, “What do buzzwords do for development policy? A critical look at ‘participation’, ‘empowerment’ and ‘poverty reduction,’” Third World Quarterly 26/7 (2005), pp. 1043–1060; A. Cornwall, “Buzzwords and fuzzwords: Deconstructing development discourse,” Development in Practice 17/4–5 (2007), pp. 471–484; A. Rosenthal, “Weaving networks of responsibility: Community work in development programs in rural Malawi,” Medical Anthropology 31/5 (2012), pp. 420–437.
- K. Ramsey-White, “Remarks at launch event for ‘Health Is a Human Right: Race and Place in America’ at Georgia State University” (2017)
- Department of Health and Human Services, Report of the secretary’s task force on black and minority health (the Heckler Report) (DHHS, 1985).
- M. Heckler, “Secretary’s forward and charge to the task force,” in Report of the secretary’s task force on black and minority health, Volume 1 (Department of Health and Human Services, 1985).
- M. Whitehead, “The concepts and principles of equity and health,” International Journal of Health Services 22/3 (1992), pp. 429–445.
- J. N. Gracia, “Remembering Margaret Heckler’s commitment to advancing minority health,” Health Affairs Blog, 2018.
- Office of Minority Health & Health Equity, Centers for Disease Control and Prevention, “Selected achievements and milestones in CDC’s Office of Minority Health and Health Equity. May 18,” 2018.
- Office of Minority Health & Health Equity, Centers for Disease Control and Prevention, “Mission, Vision, Goals,” 2019.
- R. Shilts, And the band played on: Politics, people, and the AIDS epidemic (St. Martin’s Griffin, 2000), p. 554.
- CDC David J. Sencer Museum, Exhibitions, 2018. Available at https://www.cdc.gov/museum/exhibitions_permanent.htm.
- L. Liburd, “Remarks at launch event for ‘Health is a Human Right: Race and Place in America’ at Georgia State University” (2017).
- W. E. B. Dubois, The Philadelphia Negro (University of Pennsylvania Press, 1899).
- W. E. B. Dubois, The health and physique of the Negro American (Atlanta University Press, 1906).
- N. Gaber, “Mobilizing health metrics for the human right to water in Flint and Detroit, Michigan,” Health and Human Rights 21/1 (2019), pp. 179-189
- J. Wolff, The human right to health (Norton, 2012).
- B. Salhi and P. Brown, “Teaching Health as a Human Right in the Undergraduate Context: Challenges and Opportunities,” Health and Human Rights, 2019, 21/1 pp. 191-202.
- Willen (see note 11), p. 306.
- P. Hunt, “Missed opportunities: Human rights and the Commission on Social Determinants of Health,” Global Health Promotion 16/1_suppl (2009), pp. 36–41; A. Chapman, “Missed opportunities: The human rights gap in the report of the Commission on Social Determinants of Health,” Journal of Human Rights 10 (2011), pp. 132–150.