A Meta-Narrative Literature Synthesis and Framework to Guide Future Evaluation of Legal Empowerment Interventions
Katherine Footer, Michael Windle, Laura Ferguson, Jordan Hatcher, Carrie Lyons, Emma Gorin, Anne L. Stangl, Steven Golub, Sofia Gruskin, and Stefan Baral
Abstract
Legal empowerment is increasingly recognized as a key approach for addressing socio-structural determinants of health and promoting the well-being and human rights of vulnerable populations. Legal empowerment seeks to increase people’s capacity to understand and use the law. However, limited consensus remains on the effectiveness of legal empowerment interventions in optimizing health outcomes. Leveraging a meta-narrative approach, we synthesized literature describing how legal empowerment interventions have been operationalized and empirically studied with respect to health determinants. The studies included here document diverse legal empowerment approaches and highlight how interventions changed the context surrounding the health of vulnerable populations. The absence of robust conceptualization, operationalization, and measurement of the risk contexts in which legal empowerment approaches operate limits the clarity with which interventions’ impact on health can be ascertained. Despite this, legal empowerment is a promising approach to address the health of marginalized populations. To foster support between the fields of legal empowerment and health, we explore the limitations in study design and measurement of the existing evidence base; such scrutiny could strengthen the rigor of future research. This paper provides a guide to the socio-structural levels across which legal empowerment interventions impact health outcomes in order to inform future interventions.
Introduction
The World Health Organization (WHO) Commission on Social Determinants of Health (CSDH) identified improved living and working conditions and access to health care as fundamental to health equity.[1] The CSDH has highlighted the importance of tackling socio-structural drivers, including norms, policies, laws, and processes of governance, that tolerate or promote inequitable distributions of power and social resources.[2] Within this framework, legal empowerment is gaining recognition as a critical approach that provides a mechanism for individuals and communities to address structural barriers to health and human rights through improved access to justice—broadly defined to include access to public health and other services unjustly denied despite relevant rights and availability of adequate resources.[3]
Whether law is conceptualized as an enabling or limiting mechanism for rights holders or part of a more complex governance framework, it is deeply embedded within social, economic, and political processes. The health of vulnerable populations such as sex workers, people who inject drugs, men who have sex with men, ethnic minorities, and people living with HIV can be substantially impacted by their legal environment. These populations experience health inequities stemming from structural factors, including: stigma, discrimination, social and economic marginalization, criminal sanctions, and violence.[4]
Public health law studies have contributed to our understanding of how human rights and laws affect environments, behaviors, and health outcomes.[5] Studies have focused on how the legal environment can harm the health of vulnerable populations. For example, discriminatory laws affecting people living with HIV have been shown to reinforce social stigmas and be associated with increased violence and reduced health care access.[6] Discriminatory laws and systematic human rights abuses affecting ethnic minorities have also been linked to poorer health outcomes, including higher prevalence of maternal health risks and gender-based violence.[7] These examples emphasize the law as a determinant of health and demonstrate that legal institutions often institutionalize inequities and contradict expectations of equality. This inverse relationship between the law’s ability to recognize rights and its capacity to vindicate them is central to legal empowerment efforts. Recently, public health research has focused increasingly on law as a predominantly negative health determinant of vulnerable populations, focusing less on how law can be used to positively impact health.[8]
Legal empowerment has gained prominence as a framework for strengthening individuals’ capacity to exercise their rights, with implications for their health and well-being.[9] The United Nations Development Programme and the World Bank Group have supported access to justice and rule of law programs around the world.[10] Legal empowerment is a concept that has emerged in support of access to justice, a broader initiative that has evolved over time and continues to lack a common definition. The United Nations Development Programme defines access to justice as the ability of disadvantaged groups to prevent and overcome poverty by seeking a remedy through the justice system for grievances, in accordance with human rights principles.[11] As articulated by the Commission on Legal Empowerment and the Poor, legal empowerment is rooted in an enabling human rights framework, whereby vulnerable people gain understanding and control of their legal entitlements.[12]
Legal empowerment is identified by the use of laws, legal systems/institutions, and services for socio-structural change. Interventions commonly encompass nontraditional forms of assistance and redress, such as access to community paralegals or customary law remedies.[13] They also include assisting the disadvantaged with nontraditional mechanisms such as monitoring health services constrained by corruption, entrenched bureaucracy, gender bias, and other forms of discrimination to bolster their responsiveness and efficacy.
With the increasing focus on legal empowerment, it is essential to understand the evidence base supporting these approaches. We conducted a meta-narrative review of the literature to identify legal empowerment interventions addressing health-related outcomes. Its objectives were to document the legal empowerment approaches used and the health domains and socio-structural levels addressed by these interventions, and to describe their impact.
Methods
Search strategy and selection criteria
To identify legal empowerment interventions targeting health-related outcomes, we adapted a meta-narrative review of the literature, following the RAMESES review standards.[14] The RAMESES approach involves an initial scoping of the literature, broader systematic searches of electronic databases, selection and appraisal of papers, and data extraction.[15] The method is particularly appropriate where a topic spans multiple disciplines, limiting the utility of a systematic review and meta-analysis.
Definition of terms
For this review, we adapted Golub’s expansive definition of legal empowerment: “the use of law and rights to help increase disadvantaged populations’ control over their lives.”[16] We included interventions that sought to increase access and participation in legal processes, including initiatives that sought to change formalized laws and policies, as well as the systems and institutions that create, enforce, and implement those laws. In line with Goodwin and Maru (2014), our definition of legal empowerment required a process component, namely the expansion of people’s ability to engage with law-making processes as a result of the intervention.[17] Finally, we adopted a definition of health-related outcomes that included health outcomes (such as infectious diseases and mental health outcomes), proximal individual or interpersonal level health behaviors (such as substance use and interpersonal violence), and socio-structural determinants (such as stigma, laws, and policies) that are risk factors for more proximal health outcomes.
Inclusion criteria
An article had to meet the following criteria for inclusion:
- Published in a peer-reviewed journal or grey literature publication (including thesis publications) between 2002 and 2015.
- Evaluation of an intervention for legal empowerment (as defined above) and its impact on a health-related outcome (as defined above).
- Studies could be of any design from any country.
- Studies could involve any population.
- Studies had to be available in full in English.
- As the objective of the meta-narrative was to identify the impact of legal empowerment interventions on health outcomes through the identification of broad health dimensions, sources were not excluded based on quality. However, studies were excluded if none of the intervention components addressed a health-related outcome.
Screening and data abstraction
This review followed the RAMESES review standard.[18] The first step, scoping, is the process of identifying key relevant background publications broader in scope than the inclusion criteria of the final review. We identified publications in public health law, health and human rights, and social epidemiology through the study team’s internal expertise. The list was expanded through consultation with external experts in legal empowerment and public health law, and review of relevance-based searches of Westlaw, PubMed, Scopus, Embase, Sociofile, POPLINE, GlobalHealth (OVID), and PAIS International. Next, a list of publications was created by tracing the citations from the background publications forwards and backwards, using Scopus for peer-reviewed literature and Google Scholar for grey literature.[19] A full list of search terms and databases used is included in the supplementary files.
The first and second reviewer (MW and ID) did parallel screening of titles found in the completed search. If the article was deemed relevant by at least one reviewer, the abstract was retrieved. Next, the first and third reviewer (MW and IH) screened the abstract for relevant information. If one or both reviewers selected the abstract, the full article was reviewed. The first author served as a tie breaker and discussed discrepancies in order to reach consensus on whether to include an article. This review process allowed for inclusion of documents emergent in the full text review and abstraction process but not identified in the initial scoping and sampling. The first and second author read all articles and reached consensus on each paper. All papers selected were appraised alongside data abstraction using a standardized abstraction form (see supplementary files).
Data synthesis
We analyzed the final list of articles through a meta-narrative approach as it allows for different types of data and methods from diverse disciplines to be analyzed together.[20] This approach allowed for the inclusion of both quantitative and qualitative studies, which is not feasible in traditional systematic reviews. Initially, thematic analyses were conducted by the first author to identify broad themes within the interventions and outcome measures. Through the analytic process, the applicability of a socio-ecological model was examined to characterize how different types of legal empowerment processes address contextual risk factors for proximal health outcomes. Within the expansion of people’s use and enjoyment of the law, the common themes of implementation at the grassroots level of legal empowerment interventions were “participatory legal empowerment strategies” and “institutional reform strategies” primarily occurring at the state level (see Table 3). We also identified whether the interventions were conducted as part of broader strategies (for example, community-based monitoring systems).
For all interventions, we present whether individual, interpersonal, or structural outcomes were considered in the study, using an adapted socio-ecological model to guide data abstraction. Socio-ecological models are particularly useful for understanding the contexts which influence disease acquisition across intersecting levels of influence, including individual (such as attitudes and behaviors), interpersonal (such as social support), community (such as social participation) and legal (such as local, state, and national laws).[21]
Table 1. Summary of legal empowerment intervention designs
| Author(s) | Design of legal empowerment intervention(s) |
| Abdikeeva et al., 2013 | Four NGOs carrying out a range of access-to-justice strategies with the collective goal of improving Roma health and human rights by (1) addressing systemic impediments to health care and (2) developing tools to bring about positive legislative changes. |
| Barendrecht et al., 2013 | Paralegal program to help disadvantaged communities resolve disputes and legal problems in Nicaragua. |
| Beattie et al., 2010; Beattie et al., 2014; Gurnani et al., 2011 | Multi-layered violence intervention targeting policy makers, secondary stakeholders including police, lawyers, and media, and primary stakeholders as part of a wider HIV prevention program in India. |
| Beletsky et al., 2011 | Police-level intervention on police legal knowledge, syringe access attitudes, and ability to address needle stick injuries in the United States. |
| Beletsky et al., 2012 | Introduction of national policy to prohibit police interference with public health outreach, targeting IDU and sex workers. Policy backed by public health and human rights groups’ programmatic activities to support the policy in Kyrgyzstan. |
| Beletsky et al., 2013 | Structural intervention to integrate HIV-prevention training into police officer training in Kyrgyzstan. |
| Biradavolu et al., 2009 | Structural intervention to mobilize sex workers and address context-specific factors contributing to HIV vulnerability in India. |
| Bluthenthal et al., 2008 | Legalization and provision for syringe exchange programs in the United States. |
| Dworkin et al., 2014; Lu et al., 2013 | NGO community-led land and property rights intervention in rural Kenya to address women’s disinheritance and its role in the spread of HIV among women. |
| Gruskin et al., 2013 | Three NGOs offering legal integration programs, which look to integrate legal services into existing health care settings in Kenya. |
| Hughes et al., 2007 | Law 30/2000, passed as a response to high prevalence of persons who inject drugs (PWID) in Portugal, accomplished several goals: (1) decriminalized use, possession, and acquisition of all types of illicit substance for personal use; (2) formally abandoned punitive exercise of police power as the state response to substance use, and moved that response to the public health sector; and (3) removed substantial barriers to the exercise of constitutionally protected rights by substance-using persons. |
| Kigodi et al., 2013 | NGO program with trained paralegals offering legal knowledge, support, referrals, and advice to help women navigate legal cases and resolve conflict outside of the formal justice system in Tanzania. |
| Jardine et al., 2012 | Passage of national HIV law including measures affecting police at ward level in Vietnam. |
| Kohrt et al., 2015 | Educational intervention for police, targeting knowledge of mental health and law relevant to mental health users in Liberia. |
| Mac Dowell, 2003 | Strategic litigation and advocacy on behalf of persons living with HIV/AIDS (PLWHA) in Venezuelan human rights courts, leading to (1) amendments to the 1999 Constitution to remove barriers for PLWHA enjoyment of right to protection of health under 1961 Constitution, and (2) expansion of access to treatment. |
| Midford et al., 2002 | Intervention to implement a new model for illicit drug law enforcement that emphasizes harm reduction at a community level in Australia. |
Table 2: Summary of studies evaluating health-related outcomes of legal empowerment interventions, 2002-15, by author, country, and population
| Reference | Country | Target population | Method/data gathering | Sample size | Sampling | Aim/objective/purpose of study |
| Abdikeeva et al., 2013 | Serbia, Romania, Macedonia | Roma | Review of Open Society Foundations (OSF) Legal Empowerment programs in Roma communities. | N/A | N/A | Proposal for a framework for the qualitative evaluation of legal empowerment, documentation and advocacy; media advocacy; and strategic litigation. Proposal suggests collecting data at four impact levels (NGO capacity, to individual accountability, to changes in law and policy, and to the effect on communities at large). |
| Barendrecht et al., 2013 | Nicaragua | Disadvantaged persons, particularly those benefiting from informal conflict resolutions and reductions in domestic violence. | Mixed methods; prospective ecological study | 480 pre-exposure; 1000 post-exposure;
36 qualitative | Random, augmented by quota sampling to match basic national demographics | Evaluation of the effect of access to justice programs on prevalence of legal needs, legal services use, and legal empowerment. |
| Beattie et al., 2014 | India | Female sex workers | Quantitative; two cross-sectional integrated behavioral-biological assessment surveys | 1975; 1934 | Cluster sampling (FSW who sold sex at home, brothels, lodges, or dabhas); time-location sampling (street-based FSW) | Assessment of the impact of community mobilization on HIV and STI prevalence, HIV risk behaviors, and collective and individual power among FSWs. |
| Beattie et al., 2010 | India | FSW | Quantitative; cross-sectional, combining anonymous polling booth surveys (PBS) and face-to-face integrated behavioral-biological assessments (IBBA) over a multi-year period | 7,638 PBS;
3,852 IBBA | Random, cluster, and time-location cluster for both PBS and IBBA. | Evaluation of structural intervention on policy makers, secondary stakeholders (such as police), and FSWs, modifying the relationship between violence and FSW condom use, STI/HIV risk. |
| Beletsky et al., 2011 | United States | PWID | Quantitative; cross-sectional pre- and post-interventions survey of police | 94 pre-training;
| Not specified | Evaluation of the effect of police-level intervention on police legal knowledge, syringe access attitudes, and ability to address needle stick injuries. |
| Beletsky et al., 2012 | Kyrgyzstan | PWID | Quantitative; cross-sectional post-intervention survey of police | 319 law enforcement officers | Purposive | Assessment of links between Instruction 417 knowledge and
legal and public health knowledge, attitudes towards harm reduction programs, and intended practices targeting vulnerable groups. |
| Beletsky et al., 2013 | Kyrgyzstan | PWID | Quantitative; cross-sectional post-intervention survey of police | 313 law enforcement officers | Purposive | Evaluation of the effect of police level trainings on legal and public health knowledge, positive attitudes toward public health programs and policies, occupational safety awareness, and intended practices. |
| Biradavolu et al., 2009 | India | FSW | Qualitative; interviews and ethnographic observations with FSWs, NGO staff, and other actors (lawyers, police). | 26 NGO staff meetings;
12 Crisis International team meetings; 60 CBO community meetings; 6 legal literacy sessions; 3 advocacy sessions in police stations; Interviews 75 FSW; 11 NGO staff; 36 other actors. | Not specified | Analysis of effect of interventions of community-based organization interventions on police practices affecting HIV risk. |
| Bluthenthal et al., 2008 | United States | PWID | Quantitative; multivariate analysis of changes pre- and post-legal intervention | 24 programs | Purposive | Assessment of effect of legalization of syringe exchange programs on syringe exchange, syringe exchange budgets, and police harassment of program staff and clients. |
| Dworkin et al., 2014 | Kenya | Women | Qualitative; in-depth interviews with program leaders and implementers. Implementers randomly selected from inclusive list. | 50 | Random | Identification of the strategies that were used to prevent, mediate, and resolve property rights violations program was designed to reduce women’s HIV risk at the community level by protecting and enhancing women’s access to and ownership of land. |
| Gruskin et al., 2013 | Kenya | Health service users, particularly PLWHA | Mixed-methods; program evaluation | Not provided | Purposive | Evaluation of three Open Society-funded legal integration programs providing LE interventions in health care settings, particularly PLWHA. |
| Gurnani et al., 2011 | India | FSW | Quantitative; program evaluation | N/A; program consists of 83 project sites; 169 drop-in centers; and 619 STI clinics. | N/A; standardized, routine program monitoring indicators analyzed for entire intervention; daily tracking of news articles concerning HIV/AIDS and FSWs has been conducted manually by media monitors in selected districts. | Evaluation of effect of structural intervention on policy makers, secondary stakeholders (such as police), and FSWs on service provision, service uptake, and positive media reports on HIV and FSW. |
| Hughes et al., 2007 | Portugal | PWID | Mixed-methods; including review of evaluative reports, and key informant interviews | 11 | Not given | Assessment of the impact of legislation ending use of penal sanctions for drug possession and introducing a system of referral to Commissions for the Dissuasion of Drug Addiction, through stakeholder perceptions of major impacts, successes, and challenges in adopting decriminalization, and patterns of drug use. |
| Kigodi et al., 2013 | Tanzania | Women | Qualitative; including interviews, focus groups, observations, and secondary data sources. | 31 interviews; 4 focus groups | Convenience | Exploration of the effects of legal services for women and children surviving GBV and other gendered injustices. |
| Jardine et al., 2012 | Vietnam | PLWHA, PWID | Qualitative, post-intervention interviews | 13 interviews with law enforcement personnel; 27 semi-structured questionnaires with street level police | Not given | Assessment of influence of regulation on ward level police regarding harm reduction in order to better target education and structural change. |
| Kohrt et al., 2015 | Liberia | Mental health services users (MHSUs) | Qualitative and quantitative, pre- and post-intervention interviews. | 14 law enforcement personnel | Not given | Assessment of education intervention on police knowledge of mental health, attitudes toward MHSUs, and law relevant to MHSUs. |
| Lu et al., 2013 | Kenya | Women | Qualitative; post-intervention interviews | 20 | Not given | Identification of facilitators and inhibitors to implementation of intervention reducing HIV risk by promoting property rights of women. |
| Mac Dowell, 2003 | Venezuela | PLWHA | Legal policy review | N/A | N/A | Review of the effect of changes Venezuela’s Constitution in 1961 and 1999, and legislation guaranteeing rights to ART and HIV treatment on numbers enrolled in treatment and compliance by |
| Midford et al.,
2002 | Australia | PWID | Mixed method; observations, police focus groups, interviews with key informants and participants; survey with police, review of media | 9 focus groups with police officers; 301 police officer post-training survey | Purposive sampling | Investigation of the implementation and impact of structural intervention on drug harm. |
| Reference | Access to justice strategy | Outcome measure | |||||||||||||||||||
| Legal empowerment strategies | Complimentary strategies to legal empowerment (1) | Institutional reform strategies | Part of broader strategy | Individual | Inter-Pers. | Structural | |||||||||||||||
| Educ. | Para
legal | Legal
Aid | Cust.
Law | Health
Law Int. | Conflict
Res. | Partic.
Human Rights | Citizen
Partic. | Comm.
Monitor. | Comm.
Mobil. | Comm. Media | Litigat. | Police
Train. | Law
Change | Comm.
Outcome | Health Sys. | Legal
Sys. | Macro
Struct. | ||||
| Abdikeeva et al., 2013 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Barendrecht et al., 2013 | ✓ | ✓ | ✓ | ||||||||||||||||||
| Beattie et al., 2010 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓(2) | ✓ | ||||||||||||
| Beattie et al., 2014 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓(2) | ✓ | ||||||||||||
| Beletsky et al., 2012 | ✓ | ✓ | |||||||||||||||||||
| Beletsky et al., 2013 | ✓ | ✓ | |||||||||||||||||||
| Beletsky et al., 2011 | ✓ | ✓ | |||||||||||||||||||
| Biradavolu et al., 2009 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| Bluthenthal et al., 2008 | ✓ | ✓ | ✓ | ||||||||||||||||||
| Dworkin et al., 2014 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||
| Gruskin et al., 2013 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| Gurnani et al., 2011 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||
| Hughes et al., 2007 | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||
| Kigodi et al., 2013 | ✓ | ✓ | |||||||||||||||||||
| Jardine et al., 2012 | ✓ | ✓ | ✓ | ||||||||||||||||||
| Kohrt et al., 2015 | ✓ | ✓ | ✓ | ||||||||||||||||||
| Lu et al., 2013 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||
| Mac Dowell, 2003 | ✓ | ✓ | ✓ | ||||||||||||||||||
| Midford et al., 2002 | ✓ | ✓ | |||||||||||||||||||
Findings
The scoping process yielded 67 key background documents, including both grey and peer-reviewed literature (Figure 1). From the analysis of citations of this initial list, we identified 2,261 articles for review, of which 19 met our inclusion criteria (Figure 1). The articles described the results of 16 different legal empowerment interventions on health outcomes (Table 1). One intervention was considered by three articles, and another by two.
Figure 1. Flow chart of search strategy
Study populations
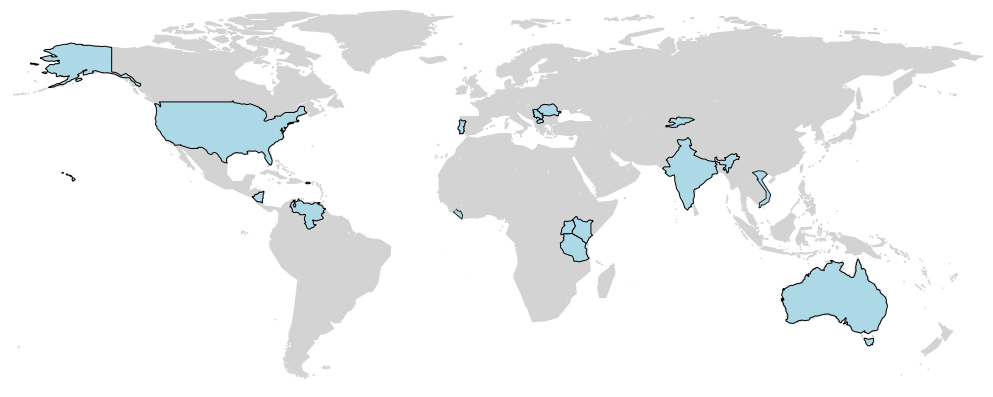
While there was at least one study from each continent, overall coverage was very limited, highlighting the small number of studies in general (Figure 2). The studies also included a wide range of different vulnerable populations (Table 2). The variety of populations reinforces the range of people that could benefit from legal empowerment interventions.
Figure 2. Distribution of legal empowerment interventions from the 19 studies
Legal empowerment interventions
Interventions in the review employed a range of access strategies appropriate to the socio-legal context in which communities live.[22] We categorized legal empowerment interventions as either “participatory” legal empowerment approaches or “institutional reform” approaches. Five (26%) studies used only participatory legal empowerment approaches and nine (47%) used only an institutional reform approach (Table 3).[23] The remaining five (26%) used both approaches.[24]
Crucial to participatory legal empowerment-focused interventions are people’s participation and active engagement in the entire process (such as paralegal programs and community legal and rights education). Legal empowerment approaches that involve institutional reform processes were characterized as being more top down, while still linked to the expansion of people’s involvement with lawmaking processes.[25] Building on this taxonomy of “participatory” and “institutional” legal empowerment approaches, we set out typologies of intervention under these two classifications, improving the conceptual understanding of the legal empowerment interventions.
Within the participatory legal empowerment strategies, we identified eight emergent themes (Table 3). These were interventions that included improved legal and human rights knowledge (n=7 studies); the training of community-based paralegals (n= 5 studies); citizen participation in governance (n=4 studies); informal conflict resolution (n=3 studies); the hiring of legal aid lawyers (n=2 studies); customary law strengthening (n=2 studies); integration of legal services into health care (n=2 studies); participatory documentation of human rights violations (n=1 study).[26] Of the studies using participatory legal empowerment strategies, six combined these efforts with complementary community-based approaches (either monitoring systems, mobilization, or media strategies), and four were integrated into larger interventions.[27]
Within the institutional reform approaches, we identified three key themes. These were the training of police forces in their interactions with vulnerable populations (n=7); changes to law or policy to reduce discrimination or increase access to justice for at-risk populations (n= 4); and the use of strategic litigation (n=1 study).[28]
Most efforts to measure legal empowerment focused primarily on descriptions of interventions and measurement of intervention exposure. Many studies were excluded because they focused exclusively on measuring exposure to an intervention, without attempting to assess the relevance to health. Nine of the 15 studies measured exposure at a programmatic level or as part of the study design. This included reporting the number of legal cases in progress or completed; participation in group workshops or meetings; program records and routine data (for example, clients receiving paralegal services); general service provision and uptake of intervention by the community; police knowledge of law and completion of police training.[29]
Study design and measures
Studies representing varying types of methodological approaches were included: qualitative (n=6, 26%), quantitative (n=7, 37%) and mixed method (n=4, 27%), with two studies being a legal and programmatic policy review, respectively (13%).[30] The majority of quantitative studies were cross-sectional and only recorded exposure to the intervention and the outcome of interest at a single time point. Two studies included data before and after intervention exposure; however, none included a single cohort followed through time.[31]
Studies differed substantially in the health-related measure of impact. These could be grouped into individual level health outcomes or health-related risk behavior, interpersonal outcomes that assess the impact of interventions on health-related interactions between individuals (in particular, interpersonal violence), and structural measures.
Forty-two percent of studies considered individual-level health related outcomes (n=8), with all but two considering behavior change. Of the five individual level studies that focused on behavior change, one looked at changes in HIV/STI related risk behaviors (condom use) and STI infection, and five examined changes in legal knowledge and rights awareness.[32] Two of the five studies that considered behavior change also reported on individual level empowerment, of which one measured “self-efficacy” around condom use within the context of HIV prevention.[33] In addition, one paper reported on changes in drug use and drug-related disease and death.[34] Three studies considered interpersonal violence. One looked at violence as a proxy for HIV-related health outcomes, while the others looked at reductions in violence as an outcome in and of itself.[35]
Four studies considered community-level change.[36] Only one study, a complex community intervention (of which legal empowerment was one component), included a validated measure based on recognized constructs, in this case “collective power.”[37] Another two studies measured prevalence of “community conflicts” post intervention and changes in community attitudes around women’s legal property rights.[38] Changes at the health system level were reported in seven studies (36%), most of which looked at health care access and reported different indicators including access to health insurance, provision of drug treatment, access to HIV treatment, and access to needle exchange programming.[39] Three studies measured rights awareness and changes in the health care setting. One study looked at partnering between health providers and police.[40]
Structural changes to institutional/legal systems were considered the outcome in eight (42%) of the papers; these were conceptualized as changes to the operation of legal institutions (that is, police practices and judicial decision making). All the studies measured changes in police practices or knowledge, which included measuring the impact of harm reduction trainings and changes to the law on policing of people who inject drugs and sex workers; the enforcement of previously ignored due process laws; knowledge around mental health; and the level and quality of cooperation between police and health agencies.[41]
Finally, changes in macro-structural factors tied to health were considered in three of the studies through changes to the law, national educational curricula, and state fulfillment of legal obligations.[42]
Intervention impact
All eight of the studies that considered an individual-level determinant found evidence that a legal empowerment intervention had a positive impact on health or on a socio-structural determinant relevant to a more proximal health outcome. Five of these studies reported evidence of a legal empowerment intervention’s impact on increased legal knowledge and rights awareness (hypothesized as being relevant to HIV prevention) and reduction in stigma and discrimination.[43] Two reported increased individual empowerment; one of these measured this increase quantitatively, finding that female sex workers who were highly exposed to a broad intervention—which included a legal empowerment component—were significantly more likely than women with low exposure to the intervention to be tested for HIV, use condoms regularly, and test positive for chlamydia or gonorrhea.[44] Notably, this study measured exposure to a range of HIV interventions including peer navigation, which was supported by legal empowerment strategies implemented previously, illustrating the complex nature of assessing the impact of any single measure. One paper reported a national decline in substance use and drug-related deaths in Portugal following a change in the law intended to expand access to harm reduction services for people who inject drugs.[45]
Of the three studies looking at interpersonal violence, two found positive changes associated with a legal empowerment intervention. These studies evaluated a multi-layered violence intervention in India, which included institutional legal empowerment components targeting the sensitization of police and lawyers. The studies found reductions in the proportion of female sex workers reporting violence post-intervention, as well as female sex workers supported in seeking redress in more than 90% of 4,600 incidents of reported violence.[46] Finally, a study evaluating a paralegal community program in Nicaragua found a drop in the perceived prevalence of violence in both the intervention area and the control area.[47] Interestingly, the study hypothesized that this drop in both areas may have been the result of an introduction in Nicaragua of a comprehensive law against violence to women.[48]
All four of the studies that measured community-level changes reported increased community mobilization relevant to more proximal health outcomes.[49] In one paper, this community mobilization was associated with increased uptake in HIV/STI-related services (although legal empowerment was not a key exposure in the intervention).[50] One study looking at a community paralegal intervention found a reduction in the prevalence of “community conflicts” post intervention, relevant to community level “well-being.”[51] Another study, evaluating a community-led property rights intervention in Kenya, found improvement in community attitudes around women’s legal property rights and entitlements relevant to HIV prevention strategies.[52]
Of seven studies considering changes at the health care system level, four reported increased access to health-related services as a result of the intervention.[53] Two reported increased rights awareness in the health care setting which was hypothesized, based on the literature, to have an impact on mitigating discrimination.[54] One found an intervention increased collaboration between health professionals and the police, important to improved health outcomes for people with mental health problems in Liberia.[55]
Of the papers measuring structural changes, a positive increase in police knowledge (particularly around harm reduction) and practices towards people who inject drugs was observed in seven of the eight studies. This included an increase in referrals of people who inject drugs to health agencies (adjusted odds ratio (aOR) 2.21, 95% CI: 1.33-3.9), a decline in police harassment, and reduced police intent to confiscate syringes following training.[56] Two interventions designed to improve collaboration between health services and law enforcement found increased cooperation, relevant to the health and well-being of PWID and those with mental illness.[57] Legal changes prohibiting police interference with harm reduction programming in Kyrgyzstan was significantly associated with better knowledge of and attitudes to harm reduction programming (aOR=1.84, 95% CI:1.12-3.00).[58] Conversely, in Vietnam, similar changes to the law did not result in positive changes to police behavior, suggesting the importance of incorporating police training as part of any law reform.[59]
In the three studies that documented changes at the macro structural level, one reported that participatory human rights activities by the Serbian Roma population brought about laws that expanded health care access to include them, exemplifying how community-led advocacy can bring about structural changes relevant to health.[60] The other two involved a change to the law: the decriminalization of certain drugs in Portugal was followed by the inclusion of drug education in the national educational curricula; the law guaranteeing rights to antiretroviral therapy in Venezuela was associated with access to adequate treatment for people living with HIV.[61]
Methodological limitations to study designs
Notably, none of the studies followed a single cohort through time, which would have provided an opportunity to measure changes over time. Studies relied on serial cross-sectional assessments or the comparison of different populations (for example, pre- and post-intervention).
Studies evaluating broader, more complex interventions were limited in that they could not explore the impact attributable to legal empowerment specifically.[62] To properly understand the role of legal empowerment, we need studies that are appropriately powered to assess the contribution of legal empowerment in the context of broader interventions. One study used a prospective ecological design to evaluate the impact of a paralegal/mediator program.[63] However, care should be taken when interpreting the results of ecological studies, as they can be subject to ecological fallacy. Overall, the sampling strategies used to recruit study participants were poorly described or not described at all. Where they were available, studies typically relied on convenience approaches that may induce selection bias and limit generalizability. Finally, the studies included in this review predominantly considered the impact of legal empowerment interventions on social and structural influences relevant to health. There was often limited clarity around defining these higher order determinants of risk, mitigating the value of the findings as actionable data for interpreting the impact of legal empowerment to improve proximal health determinants.
Current gaps and opportunities
Health inequities are hypothesized as arising from intersecting social-structural determinants, particularly for vulnerable populations. Law is recognized as a structural factor that can negatively impact vulnerable populations. Consistent data in multiple fields including social epidemiology, health and human rights, and public health law research have increased the focus on law as an important socio-structural determinant of health.[64] Legal empowerment interventions offer an important means of expanding people’s individual and collective enjoyment of their legal rights, which we suggest has positive implications across socio-structural levels and a potential effect on health and health equity. These findings suggest that there is an opportunity for implementing and disseminating studies formally evaluating the impact of legal empowerment interventions on health-related outcomes. Moreover, there is utility in studying optimal strategies to implement legal empowerment interventions. Gruskin et al. provide a useful example of a program monitoring study that included a human rights logic model to aid evaluation and reporting on health-related outcomes. The study highlights how implementation evaluations of legal empowerment interventions can be grounded in a clearly articulated human rights-based approach.[65]
Randomized control trials are the gold standard in intervention studies but are increasingly difficult to implement given the movement toward multiple combined intervention packages. Moreover, RCTs can be difficult to design, necessitating community-level randomization which limits feasibility and appropriateness. In addition, where the intervention applies to the entire population (that is, change in the law), randomization is not possible.[66] The studies included in this review rely heavily on qualitative data, which is important in understanding an intervention’s impact in context and helping inform quantitative indicator development. However, while we adopt WHO’s pragmatic approach of evidence being judged on “fitness to purpose” as opposed to “strict traditional hierarchies of evidence,” the lack of more diverse evidence hampers the recognition of legal empowerment as a key access to justice strategy for improving health and health equity.[67] Possible approaches include the use of regression-discontinuity study designs that offer comparable internal validity to randomized trials, but are unique in the method of participant assignment, using a pre- and post-test program comparison strategy.[68]
This review also raises the importance of articulating implementation and outcome measures. Similar to other types of structural intervention, individual-focused behavior change is a popular pathway to measure. However, individual level constructs such as self-efficacy and stigma are important under-utilized measurement domains relevant to legal empowerment interventions, with validated indicators that could demonstrate more nuanced and rigorous pathways that mediate health outcomes.[69] One study in this review sought to measure legal empowerment as an individual-level process outcome, using a subjective measure of a person’s perceived confidence to solve potential future legal problems.[70] More rigorously operationalizing legal empowerment as an individual and community level construct is essential to document the complex pathways by which it may bring about change. The studies reviewed often hint at interpersonal and structural processes, but not in a way that links them to recognized conceptual constructs and measurable indicators.
Furthermore, to better capture change at the institutional and macro-level, it is necessary to better integrate large health and legal data sets into study design. The methodologies required for this remain under-developed and constitute an area ripe for rigorous innovation. Our studies highlight the absence of a number of vulnerable populations, including transgender persons and men who have sex with men. There undoubtedly exist more legal empowerment interventions at a grassroots level with a range of vulnerable populations—though with limited formal documentation—highlighting the need for continuing investment in more rigorous evaluation.
A conceptual framework to guide evaluations of health outcomes of access to justice interventions
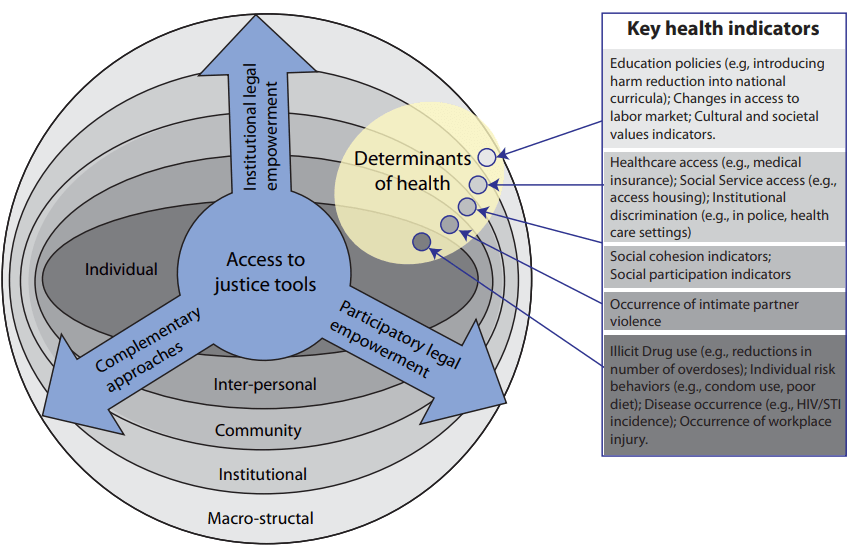
This review used a definition of legal empowerment put forward by Golub, 2013, with the intention of providing the broadest conceptualization from which to commence our meta-narrative. Our analysis and synthesis allowed for the distillation of a more refined typology of legal empowerment processes and approaches. Using a socio-ecological model to guide data abstraction helped contextualize the health impact of legal empowerment interventions, mapping them across the socio-ecological dimensions of individual, interpersonal, community, institutional, and macrostructural. After critical reflection on the definitional, practical, and measurement aspects of legal empowerment, we present a framework that: a) provides a refined typology of legal empowerment approaches that promote access to justice and b) links these approaches to five layers of socio-ecological health risk (Figure 3). The framework presented is not a prescriptive list of mediators and health outcomes. Rather, it is intended to help researchers and practitioners of legal empowerment to begin to contextualize how legal empowerment as an access to justice approach can impact health and begin to generate discussion on the most important and attainable outcomes to measure (Figure 3). The legal empowerment approaches set out by the framework have also been defined in this paper, along with complementary approaches often found to accompany legal empowerment strategies (Box 1).
Figure 3 A framework linking justice approaches to health outcomes
Box 1. Access to justice tools
| Participatory legal empowerment strategies |
| Legal and human rights education: Education of vulnerable populations on their legal and human rights options. |
| Community-based paralegal: A community-based person with some legal knowledge and skills that they use for the benefit of their community. Particularly important in deformalizing the justice system for communities. |
| Customary law strengthening: Working with local populations on strengthening customary law approaches, including ensuring that customary structures do not discriminate against women or socially exclude a population. |
| Legal aid: Free or inexpensive advice, assistance, or representation concerning the law from a person with formal legal training and qualifications. |
| Integration of legal services into health care: this can involve the integration of relevant legal services into health care settings (such as HIV clinics and hospices) and enables health care providers to connect their patients to legal assistance. |
| Informal conflict resolution: A process that can take on a variety of forms, but is used to solve problems without having to resort to more formal grievance and complaint processes. |
| Participatory human rights documentation and advocacy: Involves the documentation of human rights violations and advocacy that is undertaken by, or includes those affected. |
| Citizen participation in governance: Ordinary citizens being actively involved in assessing their own needs and participating in projects that alter governance structures (such as improving transparency in local government or bringing about a policy change). |
| Legal empowerment institutional
reform strategies |
| Strategic litigation: The selection of cases intended to achieve broad change at the level of law, policy, practice, or social discourse for the benefit of a vulnerable group. |
| Police training: Training for law-enforcement institutions that improves people’s access to correct legal process. |
| Changes to law or policy: Work with lawmakers to change law or policy to reduce discrimination against vulnerable populations or increase access to justice. |
| Complementary legal empowerment strategies |
| Community-based monitoring system: Provides a form of community oversight around changes to or introduction of a social or health program. Members of an affected community are involved in tracking change and local impacts, from which they can generate demands, suggestions, critiques, and data that can be acted upon. |
| Community mobilization: A process through which action is stimulated by a community itself, or by others, that is planned, carried out, and evaluated by a community’s individuals, groups, and organizations on a participatory and sustained basis to improve health, hygiene, and education levels, so as to enhance the overall standard of living in the community. |
| Media-based strategies: Print and news media, social media, video documentaries, radio talk shows, and live events in the community can help disseminate legal information to socially excluded groups, promote the accountability of state actors, and contribute to sensitizing the broader public. Communications and media techniques can both strengthen a program’s other advocacy efforts and enhance its overall impact. |
Limitations of the meta-narrative review
Including four fields (social epidemiology, health and human rights, public health law research and international development literature) in the initial scoping and chain-referral process was intended to ensure that our findings represented the work of a diverse range of disciplines. However, the review focused particularly on legal empowerment’s relevance to health, and as such, the limited pool of papers reflects the scope of the review’s objective and is not intended to reflect the broader legal empowerment intervention literature that exists. A meta-narrative review was used to ensure that a range of approaches were included. For instance, this led the study team to revisit the inclusion of police trainings as a legal intervention that fit within an overarching legal empowerment narrative. The process of teasing out approaches was not intended to result in an exhaustive inventory of publications.
Given the diversity of interventions and outcomes, a meta-analysis was not possible. We could therefore not conduct pooled analyses to quantify the association we observed. Even at the level of individual studies, the quality of the evidence was severely hampered by the choice of methods, as discussed earlier. Finally, a noteworthy limitation to the synthesis of some studies concerned the decision to include a number of complex interventions, of which legal empowerment was only one component.
Conclusion
Legal empowerment is a diverse and rich tool for increasing access to justice. However, the health benefits of this intervention approach remain understudied, especially where interventions are focused on “participatory” legal empowerment strategies at a grassroots level. There is a lack of clarity about the relationship between the socio-structural factors that are the target of most legal empowerment interventions and more proximal health risks and outcomes. Legal empowerment interventions are by nature difficult to evaluate where change is sought at a community or structural level. Even when assessing individual-level change, determining how increased legal knowledge and rights awareness influences health requires explicit attention to legal empowerment as a key measurable variable on an equal footing to the inclusion of other socio- and attitudinal factors (such as stigma and self-efficacy), variables which themselves lack explicit consideration. We have proposed a framework that seeks to clarify the types of legal empowerment approach, the levels across which interventions may take effect, and potential measurable variables.
Acknowledgment
This work was supported by the Law and Health Initiative of the Open Society Foundations
Katherine Footer, MSc, LLB is an assistant scientist in the Center for Public Health and Human Rights, Department of Epidemiology, Department of Health Behavior and Society, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Michael Windle, JD is a doctoral research assistant in the Center for Public Health and Human Rights, Department of Epidemiology, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Laura Ferguson, PhD, MSc, MA is director of Program on Global Health & Human Rights, Institute for Global Health, University of Southern California, CA, USA.
Jordan Hatcher, MPH is a research assistant in the Center for Public Health and Human Rights, Department of Epidemiology, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Carrie Lyons, MPH is a senior research Coordinator at the Center for Public Health and Human Rights, Department of Epidemiology, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Emma Gorin, is a research assistant in the Department of International Health, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Anne L. Stangl, PhD MPH is a senior behavioral scientist in the Department of Global Health, International Center for Research on Women, Washington, DC, USA.
Steven Golub, JD is a development consultant for the Development Consultant, Guidance Committee of the Namati Global Legal Empowerment Network, CITY, COUNTRY.
Sofia Gruskin, JD, MIA is director of Program on Global Health & Human Rights, Institute for Global Health, University of Southern California, CITY, CA, USA.
Stefan Baral, MD MPH MBA is an associate professor in the Center for Public Health and Human Rights, Department of Epidemiology, Johns Hopkins School of Public Health, Baltimore, MD, USA.
Please address correspondence to Katherine Footer. Email: kfooter1@jhu.edu.
Competing interests: None declared.
Copyright © 2018 Footer, Windle, Ferguson, Hatcher, Lyons, Gorin, Stangl, Golub, Gruskin, and Baral. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- WHO Commission on Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the commission on social determinants of health (Geneva: World Health Organization, 2008).
- Ibid.
- Open Society Foundation, Bringing justice to health: The impact of legal empowerment projects on public health (2013); S. Golub, The past, present and possible future of legal empowerment: One practitioner’s perspective (Washington/The Hague: World Justice Project/Hague Institute for the Internationalisation of Law, 2012); R. L. Nobleman, “Addressing access to justice as a social determinant of health,” Health Law Journal 21/2014), p. 49.
- M. R. Decker, A. L. Crago, S. K. Chu et al., “Human rights violations against sex workers: Burden and effect on HIV,” Lancet 385/9963 (2015), pp.186-199; K. Lunze, F. I. Lunze, A. Raj et al., “Stigma and human rights abuses against people who inject drugs in Russia—a qualitative investigation to inform policy and public health strategies,” PLoS One 10/8 (2015), p.e0136030.
- S. Burris, L. Beletsky, J. A. Burleson et al., “Do criminal laws influence HIV risk behavior? An empirical trial,” Arizona State Law Journal (2007); C. S. Davis and L. Beletsky, “Bundling occupational safety with harm reduction information as a feasible method for improving police receptiveness to syringe access programs: Evidence from three U.S. cities,” Harm Reduction Journal 6 (2009), p.16; A. Krusi, T. Kerr, C. Taylor et al., “‘They won’t change it back in their heads that we’re trash’: The intersection of sex work-related stigma and evolving policing strategies,” Sociology of Health & Illness 38/7 (2016), pp. 1137-1150; B. Tenni, J. Carpenter, and N. Thomson, “Arresting HIV: Fostering partnerships between sex workers and police to reduce HIV risk and promote professionalization within policing institutions: A realist review,” PLoS One 10/10 (2015), pp. e0134900; UNAIDS, Report on the global AIDS epidemic (Geneva: United Nations, 2006).
- C. L. Galletly and S. D. Pinkerton, “Conflicting messages: How criminal hiv disclosure laws undermine public health efforts to control the spread of HIV,” AIDS Behavior 10/5 (2006), pp. 451-461; R. S. Lee, A. Kochman, and K. J. Sikkema, “Internalized stigma among people living with HIV-AIDS,” AIDS and Behavior 6/4 (2002), pp. 309-319.
- S. Hajioff and M. Mckee, “The health of the Roma people: A review of the published literature,” Journal of Epidemiology and Community Health 54/11 (2000), pp. 864-869.
- United Nations Development Programme, Global commission on HIV and the law: Risks, rights, and health (New York: UNDP, 2012); K. M. Blankenship and S. Koester, “Criminal law, policing policy, and HIV risk in female street sex workers and injection drug users,” The Journal of Law, Medicine, and Ethics 30/4 (2002), pp.548-559; Decker et al. (See note 4); D. Werb, E. Wood, W. Small et al., “Effects of police confiscation of illicit drugs and syringes among injection drug users in Vancouver,” International Journal of Drug Policy 19/4 (2008), pp. 332-338; E. Wood, T. Kerr, W. Small et al., “The impact of a police presence on access to needle exchange programs,” Journal of Acquired Immune Deficiency Syndromes 34/1 (2003), pp. 116-118.
- Open Society Foundation (See note 3).
- Commission on Legal Empowerment of the Poor and United Nations Development Program, Making the law work for everyone, (New York: UNDP, 2008); Maru, Access to justice and legal empowerment: A review of World Bank practice, Working paper (2009).
- United National Development Programme Regional Centre for Europe and the CIS, Strengthening judicial integrity through enhanced access to justice (UNDP, 2013).
- Maru (See note 10).
- J. Borg, A. K. Bergman, and P. O. Ostergren, “Is ‘legal empowerment of the poor’ relevant to people with disabilities in developing countries? An empirical and normative review,” Global Health Action 6 (2013), p.22854.
- G. Wong, T. Greenhalgh, G. Westhorp et al., “Rameses publication standards: Realist syntheses,” BMC Medicine 11 (2013), pp. 21.
- Ibid.
- Golub (See note 3).
- L. Goodwin and V. Maru, What do we know about legal empowerment? Mapping the evidence (Namati.org, 2014); Maru (See note 10).
- Wong et al. (See note 14).
- T. Greenhalgh, G. Wong, G. Westhorp et al., “Protocol—realist and meta-narrative evidence synthesis: Evolving standards (rameses),” BMC Medical Research Methodology 11 (2011), p.115; Wong et al. (See note 14).
- Wong et al. (See note 14).
- S. Baral, C. H. Logie, A. Grosso et al., “Modified social ecological model: A tool to guide the assessment of the risks and risk contexts of HIV epidemics,” BMC Public Health 13 (2013), p. 482; K. R. McLeroy, D. Bibeau, A. Steckler et al., “An ecological perspective on health promotion programs,” Health Education Quarterly 15/4 (1988), pp. 351-377.
- Sheldrick, “Access to justice and legal empowerment as vehicles of poverty alleviation: Governance challenges to linking legal structures to social change,” (Centre for International Sustainable Development Law, 2012).
- M. Barendrecht, M. Kokke, M. Gramatikov et al., “Impact assessment of the facilitadores judiciales programme in Nicaragua,” WIDER Working Paper 2013/113 (Helsinki: UNU-WIDER, 2013); L. Beletsky, A. Agrawal, B. Moreau et al., “Police training to align law enforcement and HIV prevention: Preliminary evidence from the field,” American Journal of Public Health 101/11 (2011), pp.2012-5; L. Beletsky, R. Thomas, N. Shumskaya et al., “Police education as a component of national HIV response: Lessons from Kyrgyzstan,” Drug and Alcohol Dependence 132 Supplement 1 (2013), pp. S48-52; L. Beletsky, R. Thomas, M. Smelyanskaya et al., “Policy reform to shift the health and human rights environment for vulnerable groups: The case of Kyrgyzstan’s instruction 417,” Health and Human Rights 14/2 (2012), pp. 34-48; R. N. Bluthenthal, K. G. Heinzerling, R. Anderson et al., “Approval of syringe exchange programs in California: Results from a local approach to HIV prevention,” American Journal of Public Health 98/2 (2008), pp. 278-283; S. L. Dworkin, T. Lu, S. Grabe et al., “What community-level strategies are needed to secure women’s property rights in western Kenya? Laying the groundwork for a future structural HIV prevention intervention,” AIDS Care 26/6 (2014), pp.754-7; S. Gruskin, K. Safreed-Harmon, T. Ezer et al., “Access to justice: Evaluating law, health and human rights programmes in Kenya,” Journal of the International AIDS Society 16/3 Supplement 2 (2013), pp.18726; C. Hughes and A. Stevens, The effects of decriminalization of drug use in Portugal (The Beckley Foundation Drug Policy Programme, 2007); M. Jardine, N. Crofts, G. Monaghan et al., “Harm reduction and law enforcement in Vietnam: Influences on street policing,” Harm Reduction Journal 9 (2012), p.27; H. Kigodi, “Paralegal services and the fight against gender-based violence and other gendered injustices in Tanzania,” (2013); B. A. Kohrt, E. Blasingame, M. T. Compton et al., “Adapting the crisis intervention team (cit) model of police-mental health collaboration in a low-income, post-conflict country: Curriculum development in Liberia, west Africa,” American Journal of Public Health 105/3 (2015), pp.e73-80; T. Lu, L. Zwicker, Z. Kwena et al., “Assessing barriers and facilitators of implementing an integrated HIV prevention and property rights program in western Kenya,” AIDS Education and Prevention 25/2 (2013), pp.151-163; E. Mac Dowell, “Juridical action for the protection of collective rights and its legal impact: A case study,” The Journal of Law, Medicine, and Ethics 30 (2002), pp. 644-654; R. Midford, “Cops, drugs and the community: Establishing consultative harm reduction structures in two western Australian locations,” The International Journal of Drug Policy 13 (2002), pp.185-192.
- A. Abdikeeva, T. Ezer, and A. Covaci, “Assessing legal advocacy to advance Roma health in Macedonia, Romania, and Serbia,” European Journal of Health Law 20/5 (2013), pp. 471-486; T. S. Beattie, P. Bhattacharjee, B. M. Ramesh et al., “Violence against female sex workers in Karnataka state, south India: Impact on health, and reductions in violence following an intervention program,” BMC Public Health 10 (2010), p. 476; T. S. Beattie, H. L. Mohan, P. Bhattacharjee et al., “Community mobilization and empowerment of female sex workers in Karnataka state, south India: Associations with HIV and sexually transmitted infection risk,” American Journal of Public Health 104/8 (2014), pp. 1516-1525; M. R. Biradavolu, S. Burris, A. George et al., “Can sex workers regulate police? Learning from an HIV prevention project for sex workers in southern India,” Social Science & Medicine 68/8 (2009), pp. 1541-1547; V. Gurnani, T. S. Beattie, P. Bhattacharjee et al., “An integrated structural intervention to reduce vulnerability to HIV and sexually transmitted infections among female sex workers in Karnataka state, south India,” BMC Public Health 11 (2011), p. 755.
- Goodwin and Maru (See note 17).
- Abdikeeva et al. (See note 24); Barendrecht et al. (See note 23); Beattie et al. (2010, See note 24); Beattie et al. (2014, see note 24); Biradavolu et al. (See note 24); Dworkin et al. (See note 23); Gruskin et al. (See note 23); Gurnani et al. (See note 24); Kigodi (See note 23); Lu et al. (See note 23).
- Abdikeeva et al. (See note 24); Beattie et al. (2010, see note 24); Beattie et al. (2014, see note 24); Biradavolu et al. (See note 24); Dworkin et al. (See note 23); Gurnani et al. (See note 24).
- Abdikeeva et al. (See note 24); Beattie et al. (2010, see note 24); Beattie et al. (2014, see note 24); Beletsky et al. (2011, see note 23); Beletsky et al. (2013, see note 23); Biradavolu et al. (See note 24); Bluthenthal et al. (See note 23); Gurnani et al. (See note 24); Hughes and Stevens (See note 23); Jardine et al. (See note 23); Kohrt et al. (See note 23).
- Abdikeeva et al. (See note 24); Beattie et al. (2010, see note 24); Beattie et al. (2014, see note 24); Beletsky et al. (2011, see note 23); Beletsky et al. (2013 see note 23); Biradavolu et al. (See note 24); Gruskin et al. (See note 23); Gurnani et al. (See note 24); Lu et al. (See note 23).
- Abdikeeva et al. (See note 24); Barendrecht (See note 23); Beattie et al. (2010, see note 24); Beattie et al. (2014, see note 24); Beletsky et al. (2011, see note 23); Beletsky et al. (2012, see note 23); Beletsky et al. (2013, see note 23); Biradavolu et al. (See note 24); Bluthenthal et al. (See note 23); Dworkin et al. (See note 23); Gruskin et al. (See note 23); Gurnani et al. (See note 24); Hughes and Stevens (See note 23); Jardine et al. (See note 23); Kigodi (See note 23); Kohrt et al. (See note 23); Lu et al. (See note 23); Midford (See note 23).
- Barendrecht (See note 23); Beattie et al. (2010, see note 24).
- Abdikeeva et al. (See note 24); Beattie et al. (2014, see note 24); Dworkin et al. (See note 23); Gruskin et al. (See note 23); Kigodi (See note 23); Lu et al. (See note 23).
- Beattie et al. (2014, see note 24); Gruskin et al. (See note 23).
- Hughes and Stevens (See note 23).
- Beattie et al. (2010, see note 24); Gruskin et al. (See note 23); Gurnani et al. (See note 24).
- Barendrecht (See note 23); Beattie et al. (2014, see note 24); Lu et al. (See note 23).
- Beattie et al. (2014, see note 24).
- Barendrecht (See note 23); Lu et al. (See note 23).
- Abdikeeva et al. (See note 24); Bluthenthal et al. (See note 23); Hughes and Stevens (See note 23); Mac Dowell (See note 23).
- Kohrt et al. (See note 23).
- Beletsky et al. (2011, see note 23); Beletsky et al. (2012, see note 23); Beletsky et al. (2013, see note 23); Biradavolu et al. (See note 24); Bluthenthal et al. (See note 23); Jardine et al. (See note 23); Kohrt et al. (See note 23); Midford (See note 23).
- Abdikeeva et al. (See note 24); Hughes and Stevens (See note 23); Mac Dowell (See note 23).
- Abdikeeva et al. (See note 24); Dworkin et al. (See note 23); Gruskin et al. (See note 23); Kigodi (See note 23); Lu et al. (See note 23).
- Beattie et al. (2014, see note 24); Gruskin et al. (See note 23).
- Hughes and Stevens (See note 23).
- Beattie et al. (2010, see note 24); Gurnani et al. (See note 24).
- Barendrecht (See note 23).
- Ibid.
- Ibid.; Abdikeeva et al (See note 24); Beattie et al. (2014, see note 24); Lu et al. (See note 23).
- Beattie et al. (2014, see note 24).
- Barendrecht (See note 23).
- Lu et al. (See note 23).
- Abdikeeva et al. (See note 24); Bluthenthal et al. (See note 23); Hughes and Stevens (See note 23); Mac Dowell (See note 23).
- Gruskin et al. (See note 23); Lu et al. (See note 23).
- Kohrt et al. (See note 23).
- Beletsky et al. (2013, see note 23); Bluthenthal et al. (See note 23).
- Kohrt et al. (See note 23); Midford (See note 23).
- Beletsky et al. (2012, see note 23).
- Jardine et al. (See note 23).
- Abdikeeva et al. (See note 24).
- Hughes and Stevens (See note 23); Mac Dowell (See note 23).
- Beattie et al. (2010, see note 24); Beattie et al. (2014, see note 24).
- Barendrecht (See note 23).
- K. M. Blankenship, S. R. Friedman, S. Dworkin et al., “Structural interventions: Concepts, challenges and opportunities for research,” Journal of Urban Health 83/1 (2006), pp. 59-72; S. Burris, “Law in a social determinants strategy: A public health law research perspective,” Public Health Reports 126 Supplement 3 (2011), pp. 22-27; S. Burris, A. C. Wagenaar, J. Swanson et al., “Making the case for laws that improve health: A framework for public health law research,” The Milbank Quarterly 88/2 (2010), pp.169-210; S. El Feki, T. Avafia, T. M. Fidalgo et al., “The global commission on HIV and the law: Recommendations for legal reform to promote sexual and reproductive health and rights,” Reproductive Health Matters 22/44 (2014), pp. 125-136; L. Gable, L. O. Gostin, and J. G. Hodge, Jr., “HIV/AIDS, reproductive and sexual health, and the law,” American Journal of Public Health 98/10 (2008), pp. 1779-1786; G. R. Gupta, J. O. Parkhurst, J. A. Ogden et al., “Structural approaches to HIV prevention,” Lancet 372/9640 (2008), pp. 764-775; A. M. Robertson, R. S. Garfein, K. D. Wagner et al., “Evaluating the impact of Mexico’s drug policy reforms on people who inject drugs in Tijuana, B.C., Mexico, and San Diego, CA, United States: A binational mixed methods research agenda,” Harm Reduction Journal 11 (2014), p. 4.
- Gruskin et al. (See note 23).
- Beletsky et al. (2011, see note 23); Beletsky et al. (2012, see note 23); Beletsky et al. (2013, see note 23); Hughes and Stevens (See note 23).
- WHO Commission on Social Determinants of Health (See note 1).
- J. Bor, E. Moscoe, P. Mutevedzi et al., “Regression discontinuity designs in epidemiology: Causal inference without randomized trials,” Epidemiology 25/5 (2014), pp. 729-737.
- A. Bandura, “Guide for constructing self-efficacy scales,” Self-Efficacy Beliefs of Adolescents 5 (2006), 307-337; V. A. Earnshaw and S. R. Chaudoir, “From conceptualizing to measuring HIV stigma: A review of HIV stigma mechanism measures,” AIDS and Behavior 13/6 (2009), pp. 1160-1177; A. D. Forsyth and M. P. Carey, “Measuring self-efficacy in the context of HIV risk reduction: Research challenges and recommendations,” Health Psychology 17/6 (1998), pp. 559-568; S. C. Kalichman, L. C. Simbayi, A. Cloete et al., “Measuring AIDS stigmas in people living with HIV/AIDS: The internalized AIDS-related stigma scale,” AIDS Care 21/1 (2009), pp. 87-93.
- Barendrecht (See note 23).