ALMA-ATA at 40: Civil Society Continues the Commitment to Health for All
Leigh K. Haynes and Julia Robinson
With the Alma-Ata Declaration, the world committed to achieving “health for all by the year 2000”, designating this “a most important world-wide social goal.” It identified primary health care as the principal strategy to reach this goal and highlighted the necessity for action from not only the health sector but also other social and economic sectors (Section I, Section X). In the subsequent four decades, those called to action by the declaration have shown varied levels of commitment to its principles. While governments and private sector actors have often supported and implemented policies and programming inconsistent with the declaration, much of civil society has continued to work toward comprehensive primary health care and the promise of health for all.
Since 1978, many governments have embraced policies grounded in neoliberal ideology to achieve their goals, including expanding health care services. However, in high- and low-income countries alike, these policies have steadily opened the door for private companies, whose foremost interest is profit, to enter the ‘healthcare market’ rather than expand the public, equitable provision of health care. In European countries, we’ve recently seen austerity measures erode universal healthcare as governments turn to private companies to deliver health services rather than public providers. Similarly, in developing countries with fragile health systems, international development policy has sometimes favored the adoption of a model of private health care, including user fees at the point of service, rather than a policy of investing in public systems. Further, international trade agreements threaten increases in drug prices and pre-emption of governments’ regulatory power over their own health systems. Such policies have led to staunch inequities in access to health care and in health outcomes, especially among poor people and those who live in rural areas (for example, as in Sweden). By relying so heavily on the private sector, governments are shirking their right to health obligations, as agreed in international conventions. They are also failing to prioritize primary health care, a central tenet of the declaration.
Alma-Ata called for governments and international organizations to work with communities to plan and implement health care (Section IV). But organizations have often undermined this principle by imposing a Northern-led model of development that employs outside “technical experts” and consultants to “fix” problems the health sector faces in low- and middle-income countries, rather than involving local communities in decision-making and capacity building to address the root causes of the problems. A disproportionate amount of official development aid is directed to international NGOs and consulting firms, rather than national governments, local authorities, and civil society. Much of this aid goes back to donor countries in the form of salaries, overhead, and other expenses or through tied aid and private sector investment. Finally, vertical programming and donor interests do not always coincide with the interests of local people and their health rights. Brain drain frequently leaves communities with few or no health workers and, due to poor community consultation, the health services provided may not be those most needed.
Despite these shortcomings, civil society groups of activists, academics, health care workers, trade unions, and so many others around the world have maintained a commitment to securing health for all through universally accessible primary health care. Working at every level, from local to global, such groups pressure governments and international organizations to make policy that works toward achieving the right to health. This civil action takes place in communities, in the gaps left by the health system, and it provides primary and other essential health services to people who would otherwise be overlooked.

In the United States, where the prohibitive costs of primary care make it inaccessible for many, groups like the HOPE Campaign have arisen to build a broad movement to move toward the vision of health for all. The HOPE Campaign organizes marches, rallies, education activities, and demonstrations at legislative offices to achieve National Improved Medicare for All. They advocate for legislation which “would create a national health insurance that covers every person living in the United States with comprehensive benefits from birth to death”.
In the European Union, where corporate influence has resulted in a “creeping privatization” of health care, the European Network against Privatization and Commercialization of Health and Social Protection has emerged. This network of individuals, organizations, healthcare users, and providers, works to defend universal health care, social protection, and solidarity-based financing across Europe. It recently launched a year-long campaign, leading up to the 2019 European elections. Through this campaign, the network aims to stop candidates for EU Parliament from being influenced by multinational pharmaceutical companies, private insurance, and other vested interests. It speaks out against policies that would further deteriorate the right to health.
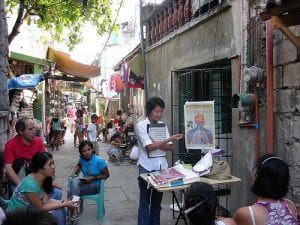
Civil society also works at grassroots levels to provide much needed primary health care where there are shortages of health care providers. An example in the Philippines, is the Council for Health and Development—a network of community-based health programs (CBHP). They train volunteer Community Health Workers (left) who provide education and health care, including first aid, disease prevention, and treatment of common illnesses. CHWs serve as an important nexus between clinic-based doctors and nurses, and individuals who live in circumstances that prevent them from seeking care.
In an effort to improve the quality of primary health care services in underserved communities, the Community of Practitioners on Accountability and Social Action in Health (COPASAH) brings together “grassroots practitioners” from across the globe to share experiences that will improve their practices. Identifying the need for practical education, COPASAH facilitates bottom-up learning between these practitioners, based on their own experiences, and builds a body of practical knowledge so these communities receive the quality care that is their right. COPASAH also works with practitioners to empower local communities to determine and demand health services that are culturally appropriate, and of adequate quality.
Many organizations provide essential health services in the wake of inhumane treatment of vulnerable people. Doctors of the World provides primary health care and psychological services to asylum seekers who live in poor conditions in camps across Europe. Sea-Watch organizes search and rescue missions for migrants in the Mediterranean Sea and has a medical crew on its ships to provide emergency care. Other organizations step in to fulfill homeless people’s right to health care; for example, the Street Medicine Institute works in the United States and is expanding services to other parts of the world.
Despite policies and programming that prove detrimental to the right to health, civil society remains steadfast in its commitment to the principles of the Alma-Ata Declaration to achieve health for all. And during times of increasing economic inequality, social exclusion, environmental degradation, war, divisive politics, and other circumstances that harm people’s health, its actions are crucial. Governments must be held accountable in their duty to protect and fulfill everyone’s right to health. The voice and experience of civil society, which is close to those most affected, is an important part of that accountability, and it should be heavily weighted in policymaking and health systems planning. Formalizing civil society roles in government, international NGOs, and donor structures, is one way of placing the people’s priorities at the center so their pressing needs are not overlooked. Such actions put us on the path envisioned by the Alma-Ata Declaration: a path toward achieving health for all and an equitable and just future for everyone.
Leigh Haynes is a PhD researcher at the Faculty of Pharmacy and Medicine at the Vrije Universiteit Brussel and a member of the People’s Health Movement-USA. Email: leigh.haynes@vub.ac.be
Julia Robinson is a clinical instructor in the Department of Global Health at the University of Washington, lead of advocacy and Cote d’Ivoire programs at Health Alliance International, and the North America steering council co-representative for the People’s Health Movement.