Case Study: Degree of Integration of Disability Rights Into Allied Health Professional Education
Claire Bowley, Ann-Mason Furmage, Kanchan Marcus, and Stephanie D. Short
Abstract
Persons with disabilities are vulnerable to rights violations when accessing health care, including allied health care. However, the commitment of allied health professional education to disability rights has not been researched. This study is the first to investigate the extent to which disability rights principles are integrated into allied health competencies and education. Specifically, this paper explores the extent to which disability rights principles are integrated into the competencies and education of the six allied health professions taught by the University of Sydney’s Faculty of Health Sciences. The study brings to light facilitators and barriers to professional curriculum renewal, and recommendations for future health professional education. This case study reveals that three allied health professions—exercise physiology, physiotherapy, and radiography—incorporate a rights-based approach to a lesser degree than the other three—speech pathology, occupational therapy, and rehabilitation counseling. We refer to this as an “allied health continuum.” The paper concludes that there is considerable scope for the allied health professions to strengthen human rights-based education and care provision through ethical codes of conduct, competencies, curriculum renewal, accreditation, and registration requirements, with the aim of reducing rights violations experienced by persons with disabilities when accessing allied health care.
Academic institutions can… ensure that professional training courses include adequate information about disability, based on human rights principles.1
Introduction
The UN Convention on the Rights of Persons with Disabilities (the Convention) promotes and protects the “equal enjoyment of all human rights and fundamental freedoms by all persons with disabilities.”2 This imposes obligations on states to develop rights-based approaches in the planning and provision of health care for persons with disabilities.3 As Australia ratified the Convention in 2008, the Australian government is legally obliged to ensure that all Australian persons with disabilities enjoy their human rights within the context of health care.4
This study was conducted as a first step toward holding universities to account in implementing their obligations under the Convention in the context of allied health professional education. The case study was conducted in the University of Sydney’s Faculty of Heath Sciences, which provides education across six allied health professional disciplines: exercise physiology, occupational therapy, physiotherapy, radiography, rehabilitation counseling, and speech pathology.5 The University of Sydney has demonstrated a commitment to the rights of persons with disabilities in the education of allied health care professionals, as the Faculty of Health Sciences 2011–2015 Strategic Plan is underpinned by the “values embedded in the moral and legal framework of the United Nations Convention on the Rights of Persons with Disabilities (2006).”6
Despite such commitments, persons with disabilities have reportedly faced rights violations when attempting to access health care.7 As a consequence, the World Health Organization (WHO) and the World Bank recommended in World report on disability 2011 that universities “ensure that professional training courses include adequate information about disability, based on human rights principles.”8 This recommendation was the springboard for this study. As a starting point, we reviewed grey and academic literature, exploring the nature and extent to which human rights are incorporated within allied health professional competencies and education in Australia and internationally.
Health professional competencies
Competencies published by the peak governing bodies of the six allied health professions under investigation recognize the importance of human rights in their practice. However, some professions—most notably, occupational therapy and rehabilitation counseling—exhibit a greater interest in human rights and the rights-based approach to persons with disabilities than others.
The World Federation of Occupational Therapists position statement on human rights asserts that all humans have the right to participate in occupations that enable them to fulfill their potential and experience satisfaction.9 Occupational therapists have also demonstrated an interest in the right of all persons to participate in meaningful occupations that contribute positively to their well-being, which has been applied to persons with disabilities.10 Additionally, the Australian Society of Rehabilitation Counsellors and the Rehabilitation Counselling Association of Australasia recognize that rehabilitation counselors ought to respect the rights of persons with disabilities by facilitating independence and providing accessible and non-discriminatory services.11
The professions of speech pathology and physiotherapy also recognize the importance of human rights, but it is less clear how far this extends to persons with disabilities.12 The extent to which radiography and exercise physiology adopt a focus on the rights of persons with disabilities is not evident.13
To our knowledge, no previous research has compared the degree to which allied health professional competency documents exhibit a rights-based approach to disability and rehabilitation.
Health professional education
Several studies conducted in the United Kingdom and United States are relevant to this study.14 Vincent and colleagues surveyed 156 medical students from 26 medical schools in the UK.15 While 57% of these students thought that human rights issues were important, only 20% indicated that human rights were included in their education. Chamberlain surveyed 51 individuals responsible for teaching ethics and law to nursing students in the UK.16 The majority of respondents taught only 10 of the 16 surveyed human rights issues.
In the US, Sonis and colleagues surveyed 113 coordinators of compulsory bioethics units of study in medical schools.17 Using a similar survey to Chamberlain, Sonis and colleagues found that medical schools only included approximately seven of the 16 human rights issues.18 Additionally, Brenner reviewed the curricula of 28 graduate schools of public health and 15 masters of public health programs in the US, as well as 34 international schools of public health, for the inclusion of human rights units.19 Within these schools, Brenner and colleagues identified only eight units that focused on human rights. More recently, Cotter and colleagues surveyed the deans from 108 medical and public health schools in the US.20 Only 37% of the surveyed schools had offered some level of human rights education during the past academic year, and time constraints (82%), lack of qualified instructors (41%), and lack of funding (34%) were perceived as barriers to teaching about human rights.
Furthermore, Shakespeare and Kleine’s 2013 analytical overview of interventions that have been conducted to improve health professional education on disability unearthed “some evidence that medical and health science training might actually distance practitioners from a holistic or human rights approach to disability, because it may lead to a reductionist, problem-centered approach.”21 Interestingly, the exclusion criteria employed in this useful study excluded clinical studies and papers solely concerned with improving teaching in rehabilitation sciences. It is relevant to note, too, that while this overview cited some papers relevant to allied health professional education about disability, many people, including those who would not be classed as people with disabilities, need rehabilitation (for example, after sports injury). It would be interesting to know what proportion of allied health professionals’ clients are disabled people with long-term impairment, as that would make the exclusion of the rights-based approach very relevant.
Findings from the literature indicate that human rights principles are not always incorporated into medical, nursing, and public health curricula. More importantly, the incorporation of education about the rights of persons with disabilities within allied health curricula remains under-researched.
The current study
This study intended to rectify this omission in the literature, by exploring the degree to which the competencies and education of the six allied health professions taught by the University of Sydney’s Faculty of Health Sciences respect the rights of persons with disabilities.
The study aimed to:
- investigate the nature and extent to which allied health professional competencies exhibit a rights-based approach towards working with people with disabilities;
- investigate the nature and extent to which allied health professional education respects the rights of persons with disabilities; and,
- explicate the facilitators, barriers, and recommendations for the progressive incorporation of human rights principles within health professional education more generally.
Method
Data collection
Allied health professional competency documents and education documents were collected and interviews conducted with coordinators of units that focused on disability rights. The use of three data sources was used to reduce bias through methodological triangulation. Field notes detailing potential impacts on the reliability of the data were recorded before and after data collection.22
Allied health professional competency documents
The Allied Health Professions Australia’s (AHPA) website was reviewed to identify the Australian peak governing bodies for the six allied health professions:
- Exercise and Sports Science Australia;
- Occupational Therapy Australia;
- Speech Pathology Australia; and
- The Australian Physiotherapy Association.
As AHPA does not represent rehabilitation counseling and radiography, their Australian peak governing bodies were identified through a Google search:
- The Australian Institute of Radiography; and
- The Rehabilitation Counselling Association of Australasia.
The websites were searched systematically for documents outlining the professions’ codes of ethics. Where no code of ethics was available, codes of conduct were collected.
Allied health professional education documents
Summaries of all units taught by the six allied health disciplines were obtained from the university’s website.
For those units whose summary referred to disability, unit outlines describing the learning aims were obtained through telephone and/or email contact with the unit coordinators and/or program directors.
Coordinator interviews of units focusing on disability rights
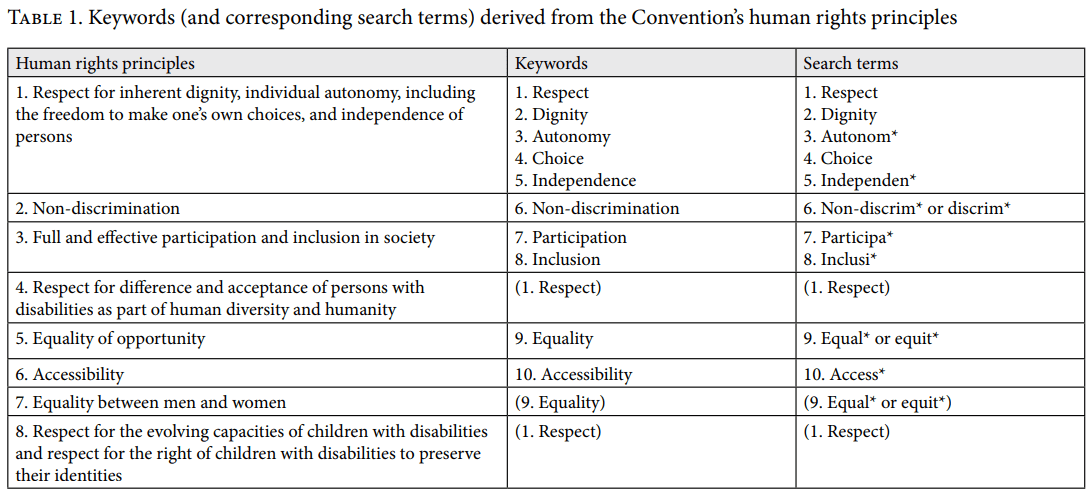
Individuals who coordinated a unit that focused on disability rights were invited via email to participate in 30-minute semi-structured telephone interviews. Units were considered to have focused on disability rights if their outline included the keywords “disability and human rights” or “disability” and at least two keywords from the Convention’s eight general principles (Table 1).23
In cases where unit coordinators were no longer at the university, outlines from 2015 were used. If the 2015 units were identified as focusing on disability rights and were taught during the first semester of 2015, coordinators were similarly invited to participate. Interviews were conducted using an interview guide, from a previous pilot study.24 The interview guide included closed-ended and open-ended questions, and was divided into five sections:
- enrolment details;
- formal curriculum;
- informal curriculum;
- supports and barriers; and
- comments and suggestions.
Questions were designed to explore the nature and extent to which education focused on disability rights, and the supports, barriers, and recommendations for future incorporation of human rights within health professional education. The interviewer recorded responses in writing on the interview guide, and they were then typed into an electronic interview guide post-interview. Typed interview transcripts were emailed to participants for member checking.25
Data analysis
A mixed-methods design using quantitative and qualitative analytical approaches was used, as there are few studies reviewing human rights within health professional competencies and education and therefore no obvious agreement on the best approaches to use.26 The approaches that were used included a quantitative keyword search and qualitative content analysis.27 The use of two approaches reduced bias through methodological triangulation.28
Quantitative data analysis
A quantitative keyword search of the competency and education documents was used to investigate the extent to which the six professions focus on disability rights.
Keywords included ‘disability’ and ‘human rights’ (human right* and/or right*), as well as ten keywords from the Convention’s eight general principles (Table 1).29 The number of keywords referred to by each document was calculated. Keywords were only included in the final count if they referred to the expectations of health professionals when working with their clients and/or to the content taught within units of study.
Qualitative data analysis
Competency documents, education documents, and member-checked interview transcripts were analyzed using a qualitative content analysis to investigate the nature of the competencies and education provided.
Competency documents, education documents, and interview transcripts were read multiple times to gain a sense of the whole. Content that referred specifically to the expectations of health professionals when working with their clients and/or to the content taught within units was included in the analyses. Using an inductive approach, selected content was then divided into meaning units, condensed, and abstracted and labeled with a code. After content from each document was coded, all codes were reviewed before proceeding to the next document. Codes that referred to human rights were sorted into sub-categories and categories, which were then arranged into an overarching human rights theme. Keywords from the Convention’s eight general principles were used as a theoretical framework.30 An audit trail detailing decisions made during data analysis was recorded, and education documents and interview transcripts were de-identified to protect participants’ confidentiality.31
The University of Sydney’s Human Research Ethics Committee provided ethical approval for this study (Project No. 2015/460).
Results
Allied health professional competencies
The following competency documents were collected for analysis.
- Occupational Therapy Australia’s code of ethics.32
- Rehabilitation Counselling Association of Australasia’s code of professional ethics for rehabilitation counselors.33
- Speech Pathology Australia’s code of ethics.34
- Australian Physiotherapy Association’s code of conduct.35
- Australian Institute of Radiography’s code of ethics.36
- Exercise and Sports Science Australia’s code of professional conduct and ethical practice.37
Table 2 shows the quantitative keyword results. Independence, participation, and inclusion were the least referenced keywords. Rehabilitation counseling and speech pathology were the only disciplines to refer specifically to persons with disabilities. Rehabilitation counseling included the most keywords from the Convention’s eight general principles (eight out of ten), closely followed by occupational therapy, speech pathology, and physiotherapy, which all included seven out of ten keywords.38
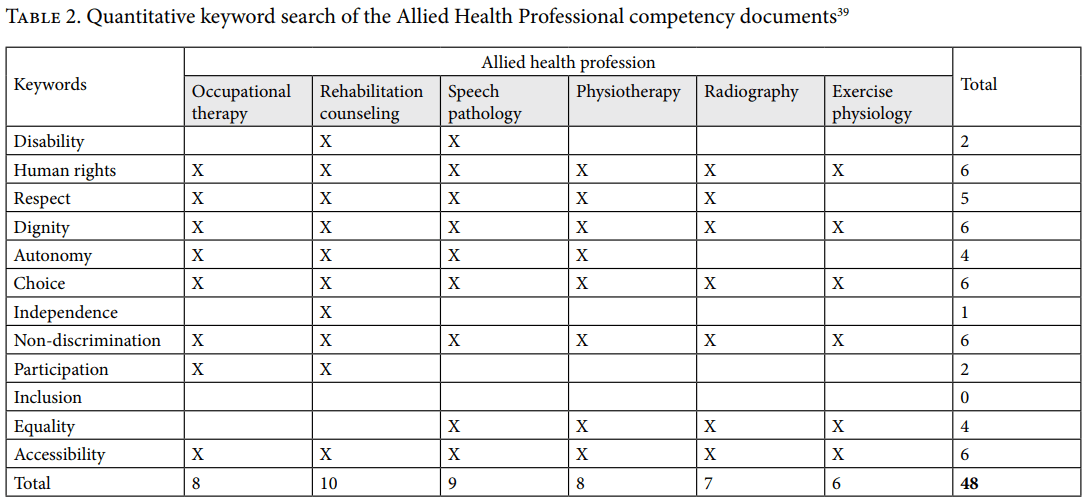
Total refers to the number of keywords included in the competency documents, within (vertical) and between (horizontal) documents. The white rows indicate the ten keywords from the Convention’s eight general principles.
Qualitative analysis of documents
The keyword ‘respect’ is recognized in the competency documents of all the allied health professions with the exception of exercise physiology. The documents that do refer to respect assert that health professionals are committed to practice in a manner that respects client’s rights (for example, dignity and autonomy), as well as client’s personal (for example, their health needs) and contextual factors (for example, their culture). The code of ethics from Speech Pathology Australia states, “we respect the rights and dignity of our clients and we respect the context in which they live.”
Dignity is acknowledged within all competency documents, as all health professionals are expected to promote the dignity of their clients by adhering to procedures and legislation that protect privacy and confidentiality. The code of conduct from the Australian Physiotherapy Association states, “members shall protect the confidentiality and privacy of client health information.”
Most of the professions’ documents assert that health professionals should respect and promote their clients right to autonomy; the exceptions are radiography and exercise physiology. Occupational therapy’s competency document states that autonomy implies patients are: “active participants in any decision regarding their involvement in services,” and the rehabilitation counseling competency documents asserts that rehabilitation counselors will advocate for their clients during situations where autonomy is reduced (for example, during involuntary admission to hospital).
Choice is recognized in all competency documents, as all the health professionals are expected to ensure clients are able to make informed choices (for example, informed on the likely benefits, risks, and costs of services). Health professionals are also expected to uphold their client’s rights to withdraw from treatment, seek a second opinion, and determine who will be provided with their personal information.
Independence was only acknowledged by rehabilitation counseling, where rehabilitation counselors are expected to support their clients: “efforts at self-advocacy both on an individual and an organizational level.”
While all documents assert that allied health professionals shall provide non-discriminatory services, rehabilitation counseling and speech pathology are the only professions to refer specifically to persons with disabilities. The Australian Institute of Radiography’s code of ethics states that radiographers shall: “ensure the provision of non- discriminatory services to all people regardless of age, colour, gender, sexual orientation, religious affiliation, political allegiances, type of illness, ethnicity, race, and mental or physical status.”
Participation is recognized by occupational therapy and rehabilitation counseling, where both professions ought to ensure clients are: “afforded the opportunity for full participation in their own treatment team.”
Inclusion is not recognized in any competency document.
The right to equality is recognized in most competency documents; the exceptions are occupational therapy and rehabilitation counseling. The competency documents that do refer to equality assert that health professionals are obliged to ensure equitable availability of health care services and resources.
All of the allied health professions expect professionals to ensure that clients are able to access their personal information and services, including physical and attitudinal access. The code of professional conduct and ethical practice for Exercise and Sports Science Australia states: “An exercise and sports science professional must… uphold the Client’s right to gain access to the necessary level of health care.”
Disability in allied health professional education
Of the 349 units taught by the Faculty of Health Sciences in 2014, only 24 (7%) of the unit summaries included the keyword ‘disability’ (Table 3).
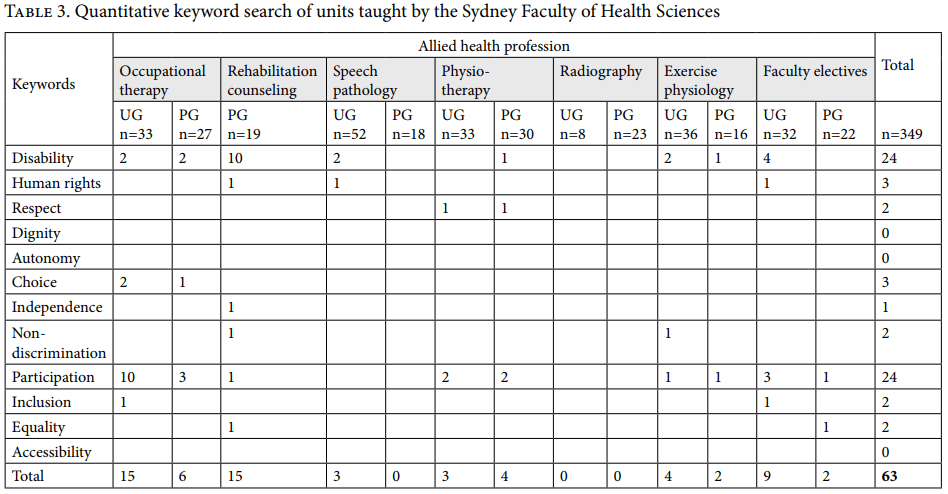
Total refers to the number of unit summaries that referred to the keywords, within (vertical) and between disciplines (horizontal). The white rows indicate the keywords from the Convention’s eight general principles.40 UG = undergraduate. PG = postgraduate.
Unit outlines for the 24 unit summaries that referred to disability were obtained and analyzed using a quantitative keyword search. Of these 24 units, 14 were identified to focus on disability rights (Table 5); including units from occupational therapy, rehabilitation counseling, and speech pathology.
Across all unit outlines, human rights, participation, inclusion, and accessibility were the most frequently referenced keywords; followed by choice, independence, non-discrimination, and equality. Respect, dignity, and autonomy were the least referenced keywords.
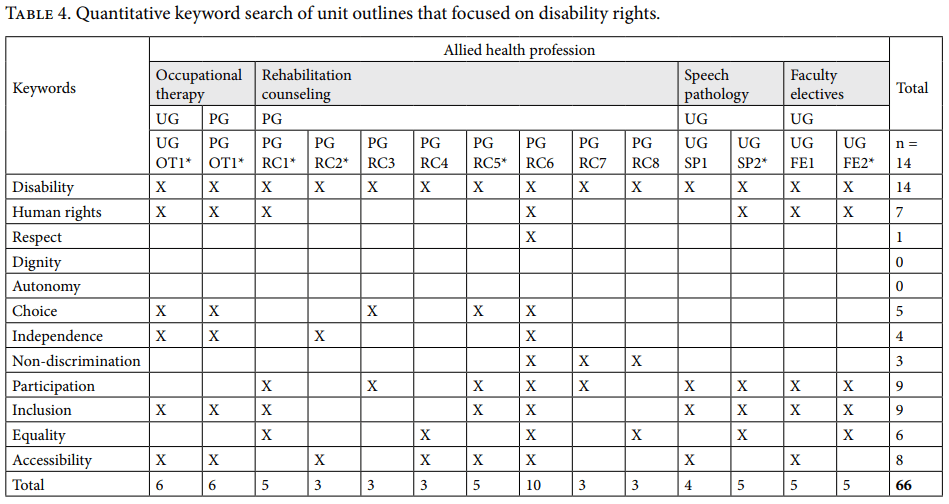
Total refers to the number of keywords referred to in the unit outlines, within (vertical) and between units (horizontal). The white rows indicate the keywords from the Convention’s eight general principles.41 UG = undergraduate. PG = postgraduate. * = units whose coordinators participated in interviews.
Qualitative interviews
A qualitative content analysis was conducted to analyze the content of units whose coordinators participated in interviews, which included interview transcripts and corresponding unit outlines.
Coordinators of seven of the 14 units that referred to disability rights participated in interviews (50% response rate). As some units were taught across disciplines and levels (that is, undergraduate and postgraduate), four interviews were completed. All interviewees (“subjects”) referred to all ten keywords from the Convention’s eight general principles, outlined below.42
Subject 1 challenged students to respect the rights of persons with intellectual disabilities to take risks (that is, dignity of risk), to express their autonomy (for example, the right to explore their sexuality) and to respect children with intellectual disabilities. Subject 1 also presented active support as a therapeutic approach used to increase client’s choice and independence. Subject 2 challenged students to consider the how they might respect the dignity and autonomy of persons with disabilities to make independent choices, with a particular focus on access to services; where respect was considered to be “interwoven through the entire subject (unit).” Subject 3 focused on respecting the dignity and autonomy of persons with disabilities, through its focus on the Independent Living Movement’s message that persons with disabilities have a right to make independent choices regarding education, employment and housing, with assistance when required. Subject 4 challenged students to consider how they might respect the dignity and autonomy of persons with disabilities to make independent and informed choices, with a particular focus on employment. This subject also urged health professionals to respect their client’s personal factors (for example, diversity) and contextual factors (for example, culture).
Subject 1 recognized the right for non-discrimination in the education and criminal justice systems, and active support was presented as a therapeutic approach that supports people “to participate fully (with support) in domestic and community life.” Additionally, personal and contextual factors that affect participation in domestic, community, vocational, and leisure activities were explored. This subject also focused on the inclusion and participation of children within education, and the inclusion and participation of adults in transition to adulthood, employment, retirement, and end of life supports. Subjects 2, 3, and 4 focused on the rights of persons with disabilities to access non-discriminatory communities, services and employment that encourage participation and inclusion.
Subjects 1 and 4 focused on equality of opportunity within the workplace. Subject 4 specifically taught students about workplace assessments and interventions that aim to increase employment equality and accessibility, in addition to the gendered and cultural aspects of employment participation. Subject 1 also explored physical and attitudinal factors that affect access to services, including a specific focus on issues of service accessibility for persons with intellectual disabilities living in rural areas. Subject 2 included a service learning component, which focused on providing accessible services that enhance the community participation of persons with disabilities, adding to the recognition of persons with disabilities as “equal members in their communities.” Additionally, subject 2 explored the rights of persons with disabilities for equal access to health resources and considered gendered aspects of access in terms of health seeking behaviors. Subject 3 provided information regarding the inequalities persons with disabilities face, including inequalities that occur between men and women. Additionally, subject 3 required students to complete a physical and attitudinal accessibility inventory of a community space (for example, a restaurant, university, or workplace), which assisted students to develop skills in advocating for the accessibility rights of persons with disabilities.
Subjects 1, 2, and 3 referred to legislation relevant to the rights of persons with disabilities, including the Convention.
Subjects 1 and 3 taught students how to recognize human rights violations, which “are sometimes subtle and not always obvious.”
Subjects 1, 3, and 4 challenged students to consider how a rights-based approach might be incorporated into practice. For example, Subject 1 involved a project where students worked therapeutically with an individual with an intellectual disability.
Facilitators, barriers, and recommendations
Unit coordinators identified a variety of factors that support the incorporation of disability rights within curricula:
- heads of disciplines;
- colleagues;
- students of the units themselves;
- the faculty’s external advisory committee;
- admissions policies to recruit educationally disadvantaged students;
- methods of teaching and learning that emphasis a rights-based approach (for example, client-centeredness); and
- awareness that “there is a move to audit disability teaching within the faculty.”
Supportive factors were particularly evident for rehabilitation counseling, as it was described as having “a major focus on this topic; more so than more clinically-focused Disciplines.”
Unit coordinators also identified a variety of barriers to incorporating disability rights into curricula:
- competition for time;
- lack of focus on encouraging and supporting persons with disabilities to complete the courses;
- “lack of awareness for the importance of human rights and a “medical model” focus is instead used”; and,
- “Systematic barriers to people talking, interacting and sharing across Faculties.”
Three of the four coordinators were not aware of other units that incorporated disability rights. However, the occupational therapy coordinator stated that they do embed human rights principles within their teaching in other occupational therapy units. The coordinator who was aware of other units that incorporated disability rights was aware of units within their own profession, rehabilitation counseling.
Unit coordinators made the following comments regarding the future incorporation of human rights principles into health professional education.
- “Attitudes around rights, choice, control, participation and inclusion for all people should be at the heart of all teaching,” not just for persons with disabilities;
- The medical model, while it has its purpose, does not always ascribe to a rights-based approach;
- The faculty should develop specific units of study on human rights that all students from all disciplines ought to complete;
- “They are trying to do this with Indigenous studies–they should do the same with rights”; and,
- “There is no one size fits all approach” when educating health professional students about the rights of persons with disabilities.
Discussion
Allied health professional competencies
We can first conclude that the commitment to human rights is recognized within the Australian competency documents relevant to the allied health professions under investigation, with some slight variation between professions.
This analysis of Australian competency documents was followed up with empirical investigations conducted in a case study within the Faculty of Health Sciences at the University of Sydney in Australia. These results cannot be generalized beyond Australia or this particular faculty. The quantitative analysis found that rehabilitation counseling and speech pathology competency documents included the highest number of keywords, and were also the only professions to refer specifically to persons with disabilities. These two professions were closely followed by occupational therapy and physiotherapy, and next by radiography and exercise physiology. These varying levels of commitment have implications for practice and education. Given the multidisciplinary nature of health care, it is important that all health professionals share a similar commitment to human rights if health care is to be truly rights-focused.43 The variations between professions suggest that this might not be the case. As governing bodies influence what is included within health professional education curricula, it is possible that varying levels of commitment will similarly influence the extent to which allied health professional education focuses on human rights principles.44
Findings from the qualitative analysis suggest that all the allied professions under investigation are committed to practice that respects and upholds their clients’ rights to dignity (that is, privacy and confidentiality), informed choice, non-discrimination, and accessibility. However, most professions overlooked the rights to independence, participation, and inclusion. Therefore, allied health professionals may not be explicitly aware of their obligations to promote and protect these human rights. This has significant implications for practice, as it may mean persons with disabilities are particularly vulnerable to violations of the rights to express their independence (for example, in terms of self-care) and for participation and inclusion (for example, in decisions regarding their treatment). When reviewing these findings, radiography and exercise physiology again demonstrated the weakest commitment to practice that upholds human rights principles.
An allied health professional continuum
While acknowledging the limitations of the study, we have identified the emergence of a continuum within the allied health professions under review, which reflects the extent to which they integrate disability rights principles. We suggest this continuum should be subject to further verification or falsification. We also recognize that: the codes of ethic and conduct are not the only documents that outline health professional practice; curricula documents do not include all content that is presented within units of study; and that disability can be referred to with different terms (for example, the Convention on the rights of persons with disabilities defines persons with disabilities as persons with long-term impairments).
Quantitative results revealed that of the 349 units taught across all allied health professional disciplines in 2014, only 24 were identified as focusing on disability. No units from postgraduate speech pathology, undergraduate physiotherapy, or radiography referred to disability, let alone to disability rights. Of the 24 units that did refer to disability, 14 focused specifically on disability rights. These 14 units were taught within the rehabilitation counseling, occupational therapy, and speech pathology disciplines.
These findings may suggest that the education provided in physiotherapy, radiography, and exercise physiology may not be equipping students to promote and protect the rights of persons with disabilities. This possible educational neglect provides insight into why persons with disabilities might experience rights violations when attempting to access health care.45 These findings are comparable to conclusions drawn from previous research, which suggested that human rights are not always successfully incorporated into medical, nursing, and public health curricula.46
While the quantitative analysis appeared to suggest that respect, dignity, autonomy, and non-discrimination were largely overlooked, qualitative results suggested that all interviewed subjects referred to all ten keywords from the Convention’s eight general principles.47 These findings reflect the fact that content taught within units is not always listed in curricula documents, and suggests that the interviews allowed the researchers to gain a greater understanding of the content that was taught by the allied health disciplines. Unit coordinators indicated that human rights were integrated as a theme within all interviewed units and were presented as relevant to a range of settings (for example health care, education, and employment). This integrated approach was evident during the interviews, as most coordinators had difficulty talking about one human right without referring to another. These findings have positive implications for practice, as they suggest that when the university’s allied health education does include a focus on disability rights, this focus is broad, integrated, and applicable to a range of practice areas. The interviews support conclusions drawn from research conducted by Chamberlain in nursing education, which noted that there is room for improvement in the incorporation of human rights principles into health professional education.48
Facilitators, barriers, and recommendations
Unit coordinators identified a range of factors that support the teaching of human rights, particularly within rehabilitation counseling. This study also unearthed a range of barriers. The most interesting barrier was the existence of systematic barriers to people interacting and sharing across faculties, with medicine, nursing, pharmacy, and so on. As allied health professionals are expected to work collaboratively as part of multidisciplinary teams, allied health disciplines within universities should work collaboratively in their efforts to educate future health professionals.49 In support of this claim, one unit coordinator recommended that the faculty develop specific units on human rights and health that students from all health profession courses should undertake.
The study also suggests that a more biomedical model of disability, while it has its value, does not always incorporate a rights-based approach. Given that physiotherapy, exercise physiology, and radiography are arguably the most biomedically oriented professions of the six allied health professions, it is possible that this orientation creates a barrier to incorporating a rights-based approach within their competencies and education. Following this interpretation, we propose a continuum regarding the extent to which the six allied health professions respect the rights of persons with disabilities in this case study (Figure 1).

Implications for future research
Given that human rights principles are recognized to varying degrees within the competency documents of the six allied health professions under investigation, it is recommended that peak governing bodies review their competency documents to ensure that they are in fact meeting their obligations under the Convention. It is additionally recommended that universities strive to develop curricula that reflect their commitment to the rights of persons with disabilities, which is multidisciplinary in nature. Future research should investigate the effectiveness of such education, measured using pre/post assessment. Future research could also compare allied health professional education with competencies to medicine and nursing, and public health, as these professionals also play significant roles in multidisciplinary health care teams and in the care of persons with disabilities.50
Limitations
Findings from this case study should be understood within the context of several limitations. Codes of ethics and conduct are not the only documents that outline health professional practice expectations (for example, graduate competencies), and other organizations also provide guidelines for health professional practice within Australia (for example, the Australian Health Practitioner Regulation Agency). Additionally, curricula documents do not include all content that is presented within units, and disability can be referred to with different terms (for example, impairment, condition, disease, illness, or using diagnostic labels). Furthermore, interviews were only completed with coordinators of 50% of the units identified as focusing on disability rights, and results from interviews suggested that human rights principles were taught in additional units not identified in the keyword search. Therefore, this case study may have underestimated the commitment of the allied health profession educators to respect the rights of persons with disabilities.
Conclusion
This is the first study undertaken to investigate the commitment of allied health professions to human rights-based education. Results from this empirical case study indicate that allied health professional competencies recognize the relevance of human rights principles to health professional practice, to varying degrees. It identifies an allied health continuum in the Faculty of Health Sciences at the University of Sydney, with rehabilitation counseling and occupational therapy providing evidence of a stronger commitment to human rights principles than speech pathology, physiotherapy, exercise physiology, and radiography. This study suggests that allied health professional education may not be equipping students adequately to promote and protect the rights of their clients with disabilities. Allied health professional governing bodies and universities have a legal obligation under the Convention to ensure that health professional practice and education respect the rights of persons with disabilities. The authors hope this study will enable progress toward that goal, with the aim of reducing human rights violations experienced by persons with disabilities when accessing allied health care.
Claire Bowley, MOT, is an occupational therapist at Unique Kids Clinic, New South Wales, Australia.
Ann-Mason Furmage is a disability advocate and member of the Occupational Therapy External Advisory Committee, Faculty of Health Sciences, University of Sydney, New South Wales, Australia.
Kanchan Marcus is a research assistant in the Faculty of Health Sciences at the University of Sydney, New South Wales, Australia.
Stephanie D. Short, DipPhty, MSc, PhD, is a health sociologist in behavioral and social sciences in health, Faculty of Health Sciences, University of Sydney, New South Wales, Australia.
Please address correspondence to Stephanie Short. Email: stephanie.short@sydney.edu.au
References
1. World Health Organization, World Bank. World report on disability (Geneva: WHO; 2011).
2. UN General Assembly. Convention on the rights of persons with disabilities. 2006.
3. D. Skempes, G. Stucki, and J. Bickenback, “Health-related rehabilitation and human rights: Analyzing States’ obligations under the United Nations Convention on the rights of persons with disabilities,” Archives of Physical Medicine and Rehabilitation 96 (2015), pp.163-173.
4. Australian Human Rights Commission, Australia and the universal declaration on human rights. Available at: https://www.humanrights.gov.au/publications/australia-and-universal-declaration-human-rights.
5. The University of Sydney, Our courses. 2014). Available at http://sydney.edu.au/health-sciences/future-students/courses/index.shtml.
6. The University of Sydney. Strategic plan 2011-2015. In: Sciences FoH, editor. 2011.
7. National People with Disabilities and Carer Council, Shut out: The experience of people with disabilities and their families in Australia, National Disability Strategy Consultation Report. In: Department of Families H, Community Services and Indigenous Affairs, editor (Canberra, ACT: Australian Government, 2009).
8. WHO (2011, See note 1).
9. World Federation of Occupational Therapists, Position statement: Human rights (2006). WFOT_Position_Statement_Human_Rights_CM2006. Available at WFOT.org.
10. K. W. Hammell, “Quality of life, participation and occupational rights: A capabilities perspective,” Australian Occupational Therapy Journal 62/2 (2015), pp.78-85.
11. Rehabilitation Counseling Association of Australasia, Code of professional ethics for rehabilitation counselors (Moonee Beach, NSW: Rehabilitation Counseling Association of Australasia, 2013).
12. World Confederation for Physical Therapy, WCPT endorsement: The united nations convention on the rights of persons with disabilities, 2015.
13. Australian Institute of Radiography, Professional practice standards for the accredited practitoner (Melbourne, Victoria: Australian Institute of Radiography, 2013).
14. A. Vincent, D. Forrest, S. Ferguson, “Human rights and medical education,” The Lancet 343/8910 (1994), pp.1435-1435.
15. Ibid.
16. M. Chamberlain, “Human rights education for nursing students,” Nursing Ethics 8/3 (2001), pp.211-222.
17. J. Sonis, D. W. Gorenflo, P. Jha, C. Williams, “Teaching of human rights in US medical schools,” JAMA 276/20 (1996), pp.1676-1678.
18. Chamberlain (2001, See note 16).
19 J. Brenner, “Human rights education in public health graduate schools: 1996 survey,” Health and Human Rights Journal 2/1 (1996), pp.129-139.
20. L.E. Cotter, J. Chevrier, W.N. El-Nachef, R. Radhakrishna, et al. “Health and Human Rights Education in U.S. Schools of Medicine and Public Health: Current Status and Future Challenges, “ PLoS ONE 4/3(2009): e4916. Available at https://doi.org/10.1371/journal.pone.0004916.
21. T. Shakespeare and I. Kleine, “Educating health professionals about disability: A review of interventions,” Health and Social Care Education 2/2 (2013), pp. 20-37.
22. M. Curtin and E. Fossey, “Appraising the trustworthiness of qualitative studies: Guidelines for occupational therapists,” Australian Occupational Therapy Journal 54/2 (2007), pp. 88-94.
23. UN General Assembly (2006, see note 2).
24. S. Short, C. Chapparo, R. Madden, et al, Human rights: 8 principles for curriculum renewal in health. 2011). Available at http://sydney.edu.au/social-inclusion/grants-program/grant-recipients/2011/division-of-health-sciences.shtml.
25. Curtin (2007, see note 22).
26. R. B. Johnson and A. J. Onwuegbuzie, “Mixed methods research: A research paradigm whose time has come,” Educational Researcher 33/7 (2004), pp.14-26.
27. U. H. Graneheim and B. Lundman, “Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness,” Nurse Education Today 24/2 (2004), pp.105-112.
28. Curtin (2007, see note 22).
29. UN General Assembly (2006, see note 2).
30. Ibid.
31. Curtin (2007, see note 22).
32. Occupational Therapy Australia, Code of ethics (Fitzroy, Victoria: Occupational Therapy Australia, 2014).
33. Rehabilitation Counseling Association of Australasia (2013, see note 11).
34. Speech Pathology Australia, Code of ethics (Melbourne, Victoria: The Speech Pathology Association of Australia Limited, 2010).
35. Australian Physiotherapy Association, APA code of conduct (Camberwell, Victoria: Australian Physiotherapy Association, 2008).
36. Australian Institute of Radiography, Code of ethics (Melbourne, Victoria: Australian Institute of Radiography, 2002).
37. Exercise and Sports Science Australia, Code of professional conduct and ethical practice: Version 2 (Albion, Queensland: Exercise & Sports Science Australia, 2014).
38. UN General Assembly (2006, see note 2).
39. Ibid.
40. Ibid.
41. Ibid.
42. Ibid.
43. Australian Medicare Local Alliance, Guide to allied health professions in the primary care setting (Canberra, ACT: Australian Medicare Local Alliance, 2013).
44. Rehabilitation Counseling Association of Australasia, About RCAA. Available at http://www.rcaa.org.au/about-rcaa.
45. WHO (2011, see note 1).
46. Cotter et al. (2009, see note 20).
47. UN General Assembly (2006, see note 2).
48. Chamberlain (2001, see note 16).
49. Australian Medicare Local Alliance (2013, see note 42).
50. Australian Nursing and Midwifery Federation, ANMF position statement: Care for people living with a disability (Melbourne, Victoria: Australian Nursing and Midwifery Federation, 2015).