Kenya’s cash transfer program: Protecting the health and human rights of orphans and vulnerable children
John H. Bryant
Health and Human Rights 11/2
Published December 2009
Abstract
In Kenya, as in other countries of sub-Saharan Africa heavily burdened by HIV/AIDS, orphans and vulnerable children (OVC) face poverty and despair. There is an urgent need to provide a comprehensive response that supports families and communities in their efforts to care for children and safeguard their rights. The government of Kenya has established a cash transfer program that delivers financial and social support directly to the poorest households containing OVC, with special concern for those children with or affected by HIV/AIDS. The Kenyan effort builds on lessons drawn from research and program development on cash transfers in Latin America, Asia, and Africa, and the Kenyan program offers an opportunity to examine the challenges faced by Kenya, and its responses in the context of international experiences. This paper — based on observation of and interviews with key actors involved in the origins, development, evaluation, and continued strengthening of Kenya’s cash transfer program and on the analysis of technical program documents obtained from those key actors — describes the Kenyan cash transfer program in light of human rights issues as they relate to children’s health. It offers one example of how caring for society’s most vulnerable members is a collective responsibility to be shared by a country’s government, local citizens, and the international community.
Introduction
Magnitude of the crisis
There are an estimated 32.8 million people living in Kenya, of whom 16.9 million are children under 18 years of age. Over 53% of Kenya’s population lives under the poverty line, suggesting that an estimated 9 million children are in urgent need of support, though the number may be higher as the actual number of children living under the poverty line is unknown. An estimated 12% of all Kenyan children under 18 years of age — 1.8 million — are orphans. According to Kenyan government estimates, AIDS alone has killed one or both parents of 700,000 of the country’s children.1
Due to the ongoing tragedy of poverty, fragmented development, and HIV/AIDS, increasing numbers of Kenyan children are growing up without adequate support, care, and protection.2 In Kenya, as across the sub-Saharan African region, families and communities continue to care for the majority of these orphans and vulnerable children (OVC), but many families face severe economic constraints that limit their ability to meet children’s needs.3 Orphans may suffer additional vulnerability compared with other children, for example in nutrition and access to education, although evidence on these patterns is mixed.4 While the Kenyan project described in this paper targeted resources to those children who lived in the poorest families of each community — as determined by communal public meetings (see below) — recent research expands the category of children who must be seen as vulnerable by stressing that all children living in communities affected by poverty and HIV/AIDS face serious threats to their well-being and healthy development.5 Where HIV/AIDS and poverty converge, all children risk being denied their basic human rights to such necessities as shelter, food, clean water, health care, and education.6
There is an urgent need to provide a more comprehensive response that supports families and communities to not only care for their children but also to safeguard the rights of those children. This paper describes in detail one such response — that of an ongoing cash transfer program in Kenya — in light of human rights issues as they relate to the health of children.
This paper is based on observation and on interviews with key actors involved in the origins, development, evaluation, and continued strengthening of Kenya’s Cash Transfer Programme for Orphans and Vulnerable Children; the paper is also based on the analysis of technical program documents obtained from those key actors. The bulk of the documentation reviewed has not been formally published. A primary aim of the research was to capture practitioners’ perspectives on the processes that gave rise to the cash transfer program and that have shaped the early phases of the program’s implementation. Interactions with key informants involved in numerous aspects of the cash transfer program (CTP) provided opportunities for understanding the overall process. We particularly focused on the dynamics of interactions among the diverse organizations involved in the CTP development process and on the issues reflected in internal program documents.7 We reviewed those dynamics, also considering how the CTP, with increasing government support, evolved over time.
We first briefly summarize the context of the human rights of the child as they pertain to Kenya and recent research supporting cash transfers as an effective tool for social protection. We then describe the Kenyan cash transfer program and discuss the results of a baseline survey report evaluating the program thus far. Throughout each section, and summarized in the concluding reflections, we identify gains and shortfalls, with special attention to ways in which Kenya’s approach may provide lessons for other countries in sub-Saharan Africa.
Rights of the child
International human rights instruments have long recognized social protection as a fundamental human right. Most notably, rights for all citizens are enshrined in Articles 22 and 25 of the United Nations Universal Declaration of Human Rights (1948): “Everyone as a member of society, has a right to social security… [and] to a standard of living adequate for the health and well-being of himself and his family, including food, clothing, housing, medical care and necessary social services.”8
The United Nations Convention on the Rights of the Child goes even further to protect the rights of society’s most vulnerable individuals — its children. The Convention protects children’s rights by setting non-negotiable standards and obligations in health care; education; and legal, civil, and social services. The Convention reaffirms the responsibility of the State in the protection of children’s rights, without discrimination of any kind and through the adoption of all appropriate legislative, administrative, and budgetary measures and any other measures that may be necessary.
For the government of Kenya, improving the lives of Kenya’s most vulnerable children is not only a legal and moral imperative but is also a practical and affordable possibility. The government-funded Cash Transfer Programme for Orphans and Vulnerable Children, described below, is assisting just a small fraction of those most in need. However, it has the potential to improve the lives of hundreds of thousands of Kenya’s children, lifting them out of a place of deprivation and despair. Kenya’s economy is fairly robust, growing at a pace faster than population growth. Yet, if the government is to deliver such a social protection scheme nationally and over the long term, it will need support from the international community, particularly given the impacts of the recent global economic downturn. The CTP advances an exciting new vision of social justice in Kenya. It recognizes that caring for society’s most vulnerable members is a collective responsibility to be shared by a country’s government, local citizens, and the international community.9
The growing movement toward social protection
The international trend toward investing in social protection in poor countries has reached sub-Saharan Africa, taking on new urgency as HIV/AIDS interacts with other drivers of poverty to simultaneously destabilize livelihood systems and family and community safety nets.10
Social transfers are regular and predictable transfers, often in the form of cash, provided by the state as part of a social contract with its citizens. They include child support grants, orphan care grants, disability grants, social pensions, and transfers to poor households, among others. Their objective is to alleviate poverty, provide social protection, or reduce economic vulnerability. Some cash transfers may be unconditional; others are conditional, aimed to promote particular behaviors, such as school attendance or regular health checkups.
Cash transfers have played a key role in reducing poverty in industrialized nations for more than 50 years, but until the past decade, cash transfers were thought to be unaffordable or impossible to deliver in poorer countries. Since the 1990s, however, large-scale cash transfer schemes have been launched in a growing number of developing countries, including Brazil, Colombia, Honduras, Mexico, Nicaragua, and South Africa. Increasingly, these schemes are being seen as a right of citizenship, and evidence is growing that they can help tackle hunger, increase living standards, and improve the education and health of the poorest families.11
In their extensive review of the evidence for the potential impact of cash transfer programs to strengthen families, Michelle Adato and Lucy Bassett argued in 2008 that “cash transfers have demonstrated a strong potential to reduce poverty and strengthen children’s education, health, and nutrition, and thus can form a central part of a social protection strategy for families affected by HIV and AIDS.”12 Their paper is one of many issued by the Joint Learning Initiative on Children and HIV/AIDS (JLICA), an independent, interdisciplinary network of policy makers, practitioners, community leaders, activists, researchers, and people living with HIV/AIDS that worked together to improve the well-being of HIV-affected children, their families, and their communities.13 Adato and Bassett’s argument, which supports our findings in the Kenya cash transfer program, is based on evidence from (1) studies in several large-scale, well-established transfer programs in southern Africa; (2) studies from newer, smaller cash transfer programs in southern and eastern Africa; (3) modeling of impacts of cash transfers in sub-Saharan Africa; and (4) studies of conditional cash transfers in Latin America and Asia.14
Kenya’s efforts to develop a cash transfer program have also benefited from the support of several international research initiatives and organizations. UNICEF has been strongly supportive of the government of Kenya’s CTP efforts, providing encouragement at a policy level, strong technical guidance, and necessary financial support. UNICEF’s role in supporting cash transfer activities is also documented in a number of technical papers, both domestic (within Kenya) and international, that are relevant to the Kenyan cash transfer project.15
The Kenyan response: A brief background
In 2004, the Hon. Moody Awori, Vice-President of Kenya, suggested the introduction of a cash transfer program as a way to meet the needs of the country’s increasing number of children made vulnerable due to poverty and HIV/AIDS. The concept had been discussed in a number of forums by a wide range of organizations and was generating increasing support. A first version of a national action plan for orphans and vulnerable children was developed that same year and was followed by the establishment of a national steering committee for actions aimed at orphans and vulnerable children, which is chaired by the Permanent Secretary in the Ministry of Home Affairs. The idea grew closer to becoming a reality when a proposal to set up a cash transfer program was developed by the Ministry of Home Affairs. UNICEF provided funds and technical support to help the government develop the program.
Kenya’s Cash Transfer Programme for Orphans and Vulnerable Children delivers cash to families, which they can use to pay for food, clothes, and services such as education and health. The aim of the program is to keep orphans and vulnerable children within their families and communities and to promote their development. It is important to note that the program was not intended to address poverty as a primary objective. It is intended, rather, as a rights-based program that has as a primary goal fostering orphans and other vulnerable children and supporting the development of their potential (human capital).
The cash transfer program in Kenya
Phase One: The pilot program
Phase One of the program was initiated in December 2004 with 500 of the poorest families in three districts spread throughout the country — Nairobi, Kwale, and Garissa — with each family receiving KSh500 (approximately US$6.50) per month.16 The aim of the pilot project was to learn lessons on the selection procedures and transaction costs that could be used to design a small program that could be scaled up nationwide.
The beneficiary families were selected through an open process that used government and community structures at the district and local levels. Communities developed their own criteria for selecting beneficiaries, using broad guidelines provided by UNICEF. A list of vulnerable children was then agreed upon in open barazas (public meetings). Almost all (98%) of the recipient households identified contained an OVC, that is, they contained an orphan, a sick child, or a child considered at risk due to a chronically sick caregiver.
Funds were transferred from a UNICEF bank account to the Ministry of Home Affairs and, from there, to a government account at the district level. District Children’s Officers withdrew cash from these accounts and delivered it to families in great secrecy or with armed escorts provided by the police for security reasons (post offices would later become the location of funds.) Families were free to choose how to use the money they received.
In April 2005, five months into the project, the Ministry of Home Affairs, UNICEF, and the World Bank hosted a workshop to examine key lessons learned from Phase One that would be used to shape a larger program. Participants included teams from each district (community representatives, members of the Area Advisory Council, and the District Children’s Officers); officials from the Department of Children’s Services (DCS) and other government agencies (the Ministry of Health, the Ministry of Education, and the National AIDS Control Council, among others); and other interested partners, including the Swedish International Development Cooperation Agency (SIDA) and the UK Department for International Development (DFID).
Participants in the workshop reported that Phase One of the scheme had a positive impact on the welfare of the beneficiaries and had improved access to education, health, and nutrition, but they added that there was a strong need to increase the number of recipients. The workshop highlighted some other key findings:
Beneficiaries reported that they used the money mainly on items such as food, school uniforms, textbooks, and cooking oil. However, beneficiaries added that the amount of funds was not enough to cover the full extent of the family’s basic needs.
According to beneficiaries, it was felt that those receiving cash subsidies should ensure that school-aged children in the household attend school, that the children have birth certificates, and that the children’s health and nutritional status be improved. As a result of the workshop, the communities decided that the previous unconditional pilot program should have conditions to avoid misuse of the transfers.
As a result of Phase One, children who had HIV were receiving antiretroviral (ARV) treatment, which they had not been able to afford previously (ARV treatment was not free at that time).
Other household members were benefiting from the cash subsidy. Between 30% and 50% of adult members of the beneficiary households were HIV positive or had developed AIDS and, anecdotally, data reported by workshop participants also identified that part of the cash transfers was used to buy ARVs.
During the development of Phase One, there was growing political pressure to expand the program to other areas. As part of this first phase, the Department of Children’s Services started implementing the learned lessons in 10 additional districts (Bungoma, Trnas Nzoia, Nayndarua, Nyeri, Nakuru, Meru North, Siaya, Kisii Central, Mombasa, and Machakos) with around 5,000 additional families. The purpose of implementing the program in these additional districts was to test the capacity of the government to develop such a program in a larger number of districts and to test different targeting and implementation mechanisms and procedures.
Phase Two: Strengthening capacities to assist more families
Experts in setting up cash transfer programs on a national scale in Latin America were recruited to refine targeting procedures, design a Management and Information System (MIS), and develop a comprehensive operations manual that outlines all processes, cycles, and instruments with concrete guidelines for all actors in the program. A Secretariat was also created within the Department of Children’s Services that is dedicated to managing the expanded program.
Scaling up
The enrollment process for Phase Two began in March 2007. The main objective of Phase Two was to assess and evaluate different operational mechanisms and conditions to identify the most effective ways to keep children in their families and within their communities. As Phase Two began, a household survey was conducted as a baseline for the impact evaluation. The program was rolled out in stages with the payments beginning in May. By August, all of the 10,500 enrolled orphans and vulnerable children in 17 districts were receiving their entitlements.
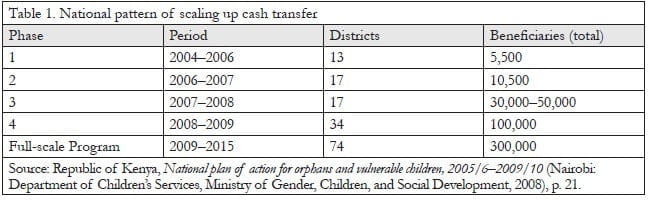
As seen in Table 1, the pilot was scaled up to 50,000 children in Phase Three and to 100,000 children in Phase Four. The overall target population of the program is 300,000 orphans and vulnerable children in 74 districts, which is at the national scale, to be achieved in the years 2009 to 2015.
During Phases One and Two, key issues in program effectiveness included targeting households, the question of attaching conditions to cash transfers, monitoring and evaluation (M&E), and fostering effective collaborations. The following discussion is limited to the details of administration and evaluation for Phases One and Two.
Targeting households
Poor areas with high HIV prevalence were chosen for Phase Two. Targeting, implementation, and monitoring were all done through a hierarchical structure of volunteer committees. The Area Advisory Council created a District OVC Sub-Committee (DOSC) to be in charge of supporting the implementation of the cash transfer program. The DOSC sensitized various groups on the program. The DOSC was also in charge of creating, training, and supervising Location OVC Committees (LOC).
Who was eligible? To qualify for the program, a household had to be poor, contain orphans or vulnerable children under 18 years of age, and not be receiving benefits under another program, either in cash or in kind. Information was collected on a standardized form and was then entered into the program’s MIS — a computerized database — that identified households that were possibly ineligible.
Enumerators were then selected to visit families and collect more extensive information on eligible households. A comprehensive questionnaire was designed to help ensure that all relevant information was collected to assess and verify a household’s degree of poverty and vulnerability. The data from this second round was entered into the MIS, which then ranked extremely vulnerable households, beginning with the most vulnerable.
Since the targeting process identified more eligible families than could be covered with actual program resources, a ranking system was developed to identify and rank the most vulnerable families. It is important to note, however, that targeting will be a continuing process that will need to respond to the dynamic nature of vulnerability as well as to the resources available for the program. Currently, the ranking system ranks household in this order, from highest priority to lowest: 1) child-headed households, 2) eldest-headed households, 3) households with larger numbers of orphans and vulnerable children, and 4) all other households with orphans and vulnerable children.
Prioritized eligible household lists were sent back to the community for validation. Each list was then presented and approved in a public baraza. If there was consensus in the baraza that some cases should be reviewed, the LOC, supported by the DOSC, reviewed these cases. This was the last chance for determining if the household belonged in the program. The final approved list of selected households and the reviewed cases were sent to the Office of the Vice President and to the Ministry of Home Affairs to be entered into the MIS for enrollment in the program.
Attaching conditions to receipt of benefits
A key question in any cash transfer program is whether a scaled-up program should attach conditions to the receipt of the money. Attaching conditions makes the program more expensive to deliver; the question is whether this extra expense is worthwhile — do these conditions make an important difference to children? Or would these funds be better spent if distributed to more families?
In the Kenyan program, it was decided that some households (about half) would be subject to conditions (attendance of all eligible children in primary school and attendance of younger children at health centers for immunizations and other health interventions). Other beneficiaries, in particular those who live in areas with limited access to education and health services, would receive the subsidies without conditions.
A household survey was used to collect baseline data on beneficiary and non-beneficiary households in areas where the program operates and was also used to collect the same data from comparison control groups (households in non-beneficiary areas). Once all of the data is complete, two follow-up surveys will make it possible to test the effectiveness of attaching conditions (see Baseline Survey Report section below).
Once households were enrolled, they received information about the program, including on their entitlements and their responsibilities. Those families who chose to participate were registered as beneficiaries. All enrolled households received an identification card and training on basic operational processes, including how to collect payments and, if conditions were attached, how they could access necessary services.
Approximately every four months, a volunteer visited the beneficiary households. These volunteers were from the community and trained to orient the family on issues related to compliance with conditions, collection of benefits, and any other problems they may have. The visit also served the purpose of identifying potential problems affecting a given household that may require specialized assistance. This is an important aspect of the social support of poor families.
The benefit of KSh1,500 per household each month takes into consideration the national average per capita income (KSh2,800) per month. The amount of cash is not intended to cover all of a child’s expenses but to ensure that the households are able to foster their children and cover part of their basic food, health, and education costs. This helps families meet the children’s immediate needs and invest in their development so they can break the poverty cycle.
The distribution process during Phase One was described above. During subsequent phases the post office was and is designated to be in charge of receiving the funds and the list of beneficiaries in order to distribute payment to them every one to two months.
Monitoring and evaluation
Monitoring was carried out throughout each program cycle to review (1) financial issues (program costs and expenses, budget); (2) administrative issues (performance of institutions linked to the program, quality of education and health services being provided); and (3) progress achieved (that is, the number of enrolled families, paid beneficiaries, and so forth) as compared to original plans. This enabled the Ministry of Home Affairs to identify problems and issues arising during the course of each stage and to make necessary adjustments. At the local level, the LOC monitored the performance of the program, making sure that the entitlements were being received and that families were assuming their responsibilities. A mechanism was also in place to receive and address complaints about payment and the quality of education and health services.
In addition to internal monitoring, a comprehensive operational and impact evaluation was built into Phase Two to evaluate three key areas:
- the welfare of and impact on the beneficiaries;
- the operational effectiveness of the program, including a cost evaluation; and
- the extent to which the program reached those in greatest need.
The evaluation, carried out by an independent team of researchers and an external firm, included quantitative household surveys, quantitative community surveys, qualitative focus group discussions with beneficiaries and other community members, in depth interviews with beneficiaries and those responsible for program implementation, an operational review, and a costing study. The Baseline Survey Report, described in the next section, was the first of the program’s planned evaluations. The lessons learned from this comprehensive external evaluation enabled important program modifications to be made, both in the conceptual design and the practical operation, before the program was scaled up in Phase Three.
Linking people to services to maximize impact
Collaboration and coordination with other service providers and complementary programs ensured that households were able to access and benefit from essential services, including education, health care, and birth registration. Guidelines were established with the Ministries of Education and Health to monitor and promote compliance with conditions and to clearly outline the responsibilities of participating schools (formal and non-formal; public and private) and health facilities (public or private; faith-based or mobile). Headmasters, teachers, and OVC officers at participating schools were trained by District Education Officers to collect and forward information on school registration and attendance. Information on health facility visits was collected by directors and health providers, who were trained by District Medical Officers of Health. Data from schools and health facilities were sent within established time frames to the District Children Officers who entered it into the MIS. An agreement between the Ministry of Home Affairs and the Civil Registrar, the agency responsible for issuing national identity cards and birth and death certificates, will facilitate the enrollment process. This will expedite bureaucratic procedures for beneficiaries to obtain national identity cards and necessary birth and death certificates.
Home visits further promote the well-being of families and the delivery of essential services. Trained volunteers visited beneficiary households to conduct awareness-raising sessions on vital health and family issues, including nutrition, child and maternal health, and prevention and treatment of chronic illness, such as malaria and HIV/AIDS. Working closely with the community, these volunteers also linked people up with local services, provided by the government, NGOs, community-based organizations, and faith-based organizations. HIV-positive household members were referred to programs that provide free access to ARVs. Awareness-raising sessions were part of the program for both groups (with and without conditions) and enabled the program to maximize all existing resources in the community.
Affordability and financial sustainability
Kenya is well positioned to take the Cash Transfer Programme for Orphans and Vulnerable Children to scale. The country’s GDP grew at a rate of 5.1% in 2006/7, with an increase to 5.5% in the following years, although the full effects of the recent global economic downturn remain to be seen. Tax revenues have increased significantly in recent years, with over US$7 billion collected in taxes last year alone. After more than a decade of stagnation, the country is experiencing a period of real growth.
Although the program clearly does not meet the needs of all 1.8 million of Kenya’s orphans, scaling the program up to meet the cash transfer program goal is clearly affordable. To cover 300,000 orphans and vulnerable children across the country would cost a small fraction — 0.6% — of Kenya’s total 2006/7 budget and just 0.12% of GDP.
Scaling up is also practical. Existing methods of delivering food and services to families in a piecemeal fashion through NGOs are less efficient and costly, with administrative costs often ranging between 40% and 60%. In contrast, a national cash transfer program would not only reach many more children in a systematic way, but experience from other countries demonstrates that the administrative costs for such full-scale programs average about 10%.17
While the goal is for the Kenyan government to fully manage and fund the program, co-financing by international development partners will be necessary for a transitional period and to ensure its sustainability. The government has demonstrated its financial commitment by ensuring that the cash transfer program is integrated into the annual budget, and in 2006/7 the government committed US$56 million to the scheme. UNICEF, DFID, SIDA, and the World Bank are also investing in developing the technical and human capacity of the Kenyan government to take this to scale.
The momentum must not stop here. Parliamentarians can play a pivotal role in supporting this program. As leaders and elected officials, they have a mandate and political responsibility to act in the best interests of their constituents. They also command the influence and resources to make it happen. Donor partners can do their part by providing additional resources to help share the costs of going to scale and assisting Kenya in mounting this tremendous and vital undertaking.
Despite the challenges posed by the recent global economic instability, this is a period of opportunity for Kenya. Many questions will be answered over the next few years to determine whether the Cash Transfer Programme for Orphans and Vulnerable Children can be expanded into a comprehensive system of social protection that will reach not just the country’s neediest children but all chronically poor and vulnerable households. Many choices will also have to be made — choices that have the potential to make a real difference in the future and fate of millions of Kenyan citizens. Margaret Basigwa, Deputy Director of Children’s Services, Office of the Vice President and Ministry of Home Affairs, emphasized the importance of making these choices soon:
We need to take care of our children to make sure this country has a future. Each person can do something to make a difference in a child’s life. We are all responsible and we should all pool together to support the orphans and vulnerable children.18
Given the special opportunities offered by the cash transfer program, it is essential to carefully evaluate the process that is underway in order to support the practical steps that are necessary to advance the program to its full potential.
How well is it working? The baseline survey report
OVC-CT Program operational and impact evaluation
Even as the program continued to scale up, Phase Two of the Pilot Program, “Strengthening Capacities to Assist More Families,” was independently evaluated as a basis for deciding whether, and how, the program should be scaled up to a national level. Oxford Policy Management was contracted to undertake the evaluation, which is described in this section.19
The core of the evaluation was a community-based controlled trial, with information collected using household and community interviews. The questionnaires captured information on a number of measures of the welfare of the children and their households. The evaluation was designed to compare program and control households at baseline and at follow-up some 18 to 24 months later, and this comparison will be used to assess the impact of the program. The evaluation was further designed to compare the impact of imposing conditions along with cash transfer as compared to cash transfers alone.
The evaluation covers Nyanza (Kisumu, Suba, Homa Bay, and Migori districts), Nairobi, Kwale, and Garissa, with four locations per district: two participating in the program intervention and two acting as controls. The allocation of intervention and control status and whether or not conditions were imposed was done randomly.
Conditions were imposed in Homa Bay, Kisumu, and Kwale; there were no conditions imposed in Garissa, Migori, and Suba. In Nairobi, conditions were imposed in one location (Kirigu), but not in the other (Dandora B).
The field work for the baseline quantitative survey was conducted between March and August 2007 by Research Solutions Limited using questionnaires in Swahili, Luo, and Somali. This survey covered only OVC households. Information was collected on program recipients, on control households that were selected to be comparable to the recipients, and on other OVC households in the study locations. Some 2,759 households were interviewed and included in the sample for analysis.
The survey collected information on a range of measures of welfare in the study population. They included measures of household consumption expenditure that can be used to assess income poverty and included information on assets owned, housing conditions, the education and employment of adults in the households, and other socioeconomic characteristics. They also included information on child welfare measures, including nutritional status, immunization, illness, health care-seeking behavior, school enrollment and attendance, child work, and birth registration.
Below is a summary of the findings of the baseline survey, the characteristics of the program recipients and the control population, and an assessment of these two groups in terms of similarity. The baseline levels of key indicators presented here form the basis for the impact evaluation. We also offer a brief analysis of the extent to which the program has managed to identify and enroll its target group, including how successfully it has included poor OVC households.
Basic characteristics of OVC and program recipients
The program has set up its activities and identified recipients in all of the evaluation locations. At the time of the baseline survey, the program was reaching 21% of OVC households and 22% of OVC in the evaluation locations. Almost all OVC households contain orphans (96%). A significant fraction of households also have a chronically ill caregiver or child. It is estimated that only 75% of children in OVC households are actually orphans or vulnerable children, since these households may also contain children who are not classed as OVC.
A parent was most likely to be the main caregiver of OVC, reflecting the fact that single orphans are much more common than double orphans. Grandparents were also quite often the main caregivers for OVC, with 18% being cared for by a grandparent. Around 22% of OVC caregivers in the study population as a whole were over 60, reflecting the important role of grandparents in caring for OVC. The proportion reached 37% in recipient households, due to the priority given to the most elderly caregivers by the program.
Targeting of the program
In addition to collecting information on the consumption (income poverty) of the OVC households, the survey also collected information on the household characteristics that were used by the program to identify the eligible households and to prioritize certain households in the selection of recipients. Together, this information means that the analysis could assess whether recipients were selected in accordance with program rules and whether poor OVC households were selected as recipients.
On many welfare indicators, recipients were on average somewhat more disadvantaged than the rest of the OVC population in their locations. Recipient households generally had poorer quality housing, fewer assets, and lower levels of education among adults than non-recipient households. They were more likely to have malnourished children, although some other health indicators and school enrollment appeared to be slightly better.
The analysis looked at the program’s coverage of poor OVC households, using household consumption levels as the measure of income poverty. Although, as noted earlier, the program was not intended to address poverty as a primary objective — and selection of districts where the program operates was not based on poverty criteria — the program decided, nevertheless, to target support to poor OVC households with limited resources, using household characteristics identified by the community. Due to limited funds, the program also introduced an additional prioritization process to select the most vulnerable households from all households identified as eligible.
This additional prioritization complicates the analysis of poverty targeting. At the time of the baseline survey, some 21% of OVC households were identified for inclusion in the program. One element of the analysis therefore looked at how effectively the program managed to select the poorest 21% of OVC households, on the basis that they can be considered the most vulnerable. The analysis shows that 38% of recipients were below the US$1 per day poverty line and 84% were below the US$2 line. These figures show that many program recipients were in some sense “poor.” They also show that the manner in which many recipients were considered to be poor is very sensitive to the poverty line that is chosen.
An analysis of the program’s targeting effectiveness identified difficulties in directing resources to the poorest OVC households. Only around one quarter of the poorest households were selected for inclusion in the program (at the time of the baseline survey). This reflects the limited coverage of the program due to budget constraints and the fact that the program selection process has not managed to identify the poorest recipients consistently. As a result, a large fraction of the poorest OVC households did not benefit from the program and will not in the future unless the targeting procedures are improved.
The subsequent enrollment of all eligible households in the period following the baseline survey would have resulted in increased coverage of the poorest since it would have increased coverage as a whole. However, it is clear that the existing targeting system is not very effective at ensuring that, for any given level of coverage, the poorest OVC households are selected. In other words, a significant fraction of less-poor households were being covered by the program. Three quarters of recipients were not from the poorest 21% of households. The analysis shows that the differences between the poorest and the better-off households were not trivial: the average consumption level in the top fifth of households was almost five times that of the poorest, and support given to a better-off household is support denied to a poorer household. Overall, some 41% of recipients were in the poorest third of OVC households within their location, while 28% came from the top (better-off) third. Determining how to identify and enroll the poorest OVC households remains a very important challenge to the CTP philosophy and management process.
A detailed analysis of the targeting process shows that there are two elements to the problem. The first element is that the allocation of the number of recipients to be included in the program between districts does not closely reflect the distribution of poor OVC households. If coverage is to be expanded, the program needs to develop policies and procedures for allocating the number of recipients geographically based on estimates of need. The second element is that the recipient selection process within each district and location is not sufficiently effective at identifying the poorest OVC households. The poverty criteria used to identify households as poor are not sufficiently sensitive to effectively determine the severity of household poverty. In fact, as reported by the program, the criteria used appear to exclude very few households. The subsequent prioritization process used to select the most vulnerable for inclusion, based on the age of the caregiver, does help to include more poor households, but there is room to strengthen this process further.
It seems likely that some form of poverty targeting will remain part of the program’s operations in the future. The issue of defining and identifying poor OVC households is an important ongoing issue that the program will need to address.
At some point during these ongoing processes, there will also need to be consideration and further discussion of the differences between the effective application of the cash transfer program on the basis of human rights (a “human rights approach”) as contrasted with a response based on a situation of poverty. Here, we see two contrasting perspectives. One would be to see the two approaches — rights-based and poverty-oriented — as competitive, calling for a choice between them. The other would be to see the two approaches as complementary. While we strongly favor a rights-based approach, there is no denying the importance of poverty as a crucial factor impeding social development of these communities. The challenge, therefore, is to bring together skillful approaches to enhancing a rights-based approach, and simultaneously addressing the burdens of poverty, both of these addressed in an evolving context of Kenya’s cash transfer program.
Concluding reflections
There is no doubting the importance of this effort by the government of Kenya to develop cash transfer programs for enhancing the well-being of orphans and vulnerable children living in poverty in Kenya. The ways in which the many relevant components of the government and the larger society, together with local communities, have joined efforts to ensure the adequacy of planning and of responsive actions relating to the needs of the truly poor and vulnerable of the society are especially impressive.
Although the efforts are impressive, it remains clear that there are faults that require correction in the targeting system of identifying and responding to the needs of the poorest households. The history of the program to date suggests that Kenya, given its explicit commitment to maintaining the rights of the child, will be responsive to the need for corrective actions. As we look at the ways in which Kenya is addressing these problems, it is apparent that it has been both challenging and complex, with calls for responses from virtually every corner of the government and the society. Addressing these challenges requires addressing two particular problems the program faces. The first is that of selecting the recipient households — those that are the poorest and in greatest need. The second is developing the programmatic structures and processes necessary to deliver the benefits and to monitor the processes and outcomes. Each of these two steps has multiple complexities, and it is one of the great strengths of the Kenyan government that it has responded with diligence, insight, resources, and enhanced commitment.
Kenya’s cash transfer program offers an encouraging model in these times of intensified debate around efforts to address the needs of deprived people in poor countries. The development of primary health care systems, basic educational systems, and agricultural initiatives so often fall short of expectations. It is gratifying to know the impact of cash transfer programs on the poor and needy of the world and to know how to scale up and improve the effectiveness of such programs. And to see African governments and partner organizations coping with the burdens of poverty, inequities, and human need is gratifying indeed.
Acknowledgments
Special thanks for helpful support from Carlos Alviar, Cash Transfer Programme Officer, UNICEF, Kenya; Mary Mbuga, Assistant Director, Children’s Services, Ministry of Gender, Children and Social Development, Kenya; Katherine Kimotho, Child Protection Officer, Specialist OVC, UNICEF, Kenya; and the JLICA team.
John H. Bryant, MD, is Senior Faculty Associate at the Johns Hopkins School of Public Health, Department of International Health; Adjunct Associate Professor at the University of Virginia, Department of Public Health Sciences; and Adjunct Professor at the Great Lakes University of Kisumu, Kenya.
Please address correspondence to the author at 250 Pantops Mountain Road, Apt. 5223, Charlottesville, Virginia 22911, email: jbryant@wcbr.us.
References
1. Facing the crisis together: The government of Kenya’s Cash Transfer Programme for Orphans and Vulnerable Children, 2007. This is a working document used within the governmental organizations to facilitate the functioning of the cash transfer program. It was made available to the author by UNICEF. Source of the data: Republic of Kenya, National plan of action for orphans and vulnerable children 2005/6–2009/10 (Nairobi: Department of Children’s Services, Ministry of Gender, Children, and Social Development, 2008).
2. Ibid., pp. 4 and 9.
3. Joint Learning Initiative on Children and HIV/AIDS (JLICA), Home truths: Facing the facts on children, AIDS, and poverty (Boston/Geneva: JLICA, 2009). Available at http://www.jlica.org/resources/publications.php.
4. K. Johnson, “Who is the vulnerable child? Using data from DHS and MICS to identify vulnerable children in the era of HIV/AIDS,” (presentation at the Fourth Global Partners Forum on Children Affected by HIV/AIDS, Dublin, Republic of Ireland, October 6–7, 2008). This presentation summarized results from a comprehensive 2008 analysis of data on children’s vulnerability in a range of countries in sub-Saharan Africa. The analysis was performed by UNICEF and Macro International.
5. L. Richter, L. Sherr, and C. Desmond, An obvious truth: Children affected by HIV and AIDS are best cared for in functional families with basic income security, access to health care and education, and support from kin and community, Synthesis report, Joint Learning Initiative on Children and HIV/AIDS (JLICA) Learning Group 1: Strengthening Families (Boston/Geneva: JLICA, 2009). Available at http://www.jlica.org/userfiles/file/JLICA_LG1_FINAL%281%29.pdf?PHPSESSID=7d0431e2b2093b7b05ea96098b72ec90; L. Sherr, “Strengthening families through HIV/AIDS prevention, treatment, care and support,” Technical report, Joint Learning Initiative on Children and HIV/AIDS (JLICA) Learning Group 1: Strengthening Families, (Boston/Geneva: JLICA, 2008). Available at http://www.jlica.org/userfiles/file/Sherr%20Strengthening%20families%20through%20prevention,%20treatment,%20.pdf?PHPSESSID=7d0431e2b2093b7b05ea96098b72ec90; JLICA (see note 3).
6. JLICA (see note 3); Richter et al. (see note 5).
7. CTP program documents supplied by key informants and discussed during interviews included the following: Facing the crisis together (see note 1); Acacia Consultants Ltd., Evaluation of cash transfer programme in Nairobi, Kwale and Garissa Districts (Acacia Consultants/UNICEF Kenya Country Office, February 2007); A. Hurrell, P. Ward, and F. Merttens, Kenya OVC-CT Programme operational and impact evaluation. Baseline survey report (Oxford, UK: Oxford Policy Management, July 2008); K. Allen, P. Campbell, S. Chatterjee, et al., Can the Kenyan State put the 300,000 most vulnerable children in the country on a cash transfer programme by the end of 2010? UNICEF Division of Policy and Planning Working Paper (New York: UNICEF, May 2007). Available at http://www.unicef.org/socialpolicy/files/Can_the_Kenyan_State_put_300K_Most_Vulnerable_Children_on_Cash(3).pdf; Ayala Consulting Company, Operations manual: Cash Transfer Programme for OVC (Ayala Consulting Co./Republic of Kenya, Office of the Vice President and Ministry of Home Affairs, October 2007); World Bank, Project appraisal document on a proposed credit to the Republic of Kenya for a cash transfer for orphans and vulnerable children project, February 17, 2009 (Nairobi: Africa Regional Office, February 2009). Available at http://www-wds.worldbank.org/external/default/main?pagePK=64193027&piPK=64187937&theSitePK=523679&menuPK=64187510&searchMenuPK=64187283&siteName=WDS&entityID=000333038_20090304234001.
8. Universal Declaration of Human Rights, G. A. Res. 217A (III) (1948), Art. 22 and 25. Available at http://www.un.org/en/documents/udhr/.
9. Facing the crisis together (see note 1), p. 2.
10. M. Adato and L. Bassett, What is the potential of cash transfers to strengthen families affected by HIV and AIDS? A Review of the evidence on impacts and key policy debates, Technical report, Joint Learning Initiative on Children and HIV/AIDS, Learning Group 1: Strengthening Families (Boston/Geneva: JLICA, 2008). Available at http://www.jlica.org/userfiles/file/Adato%20&%20Bassett%20What%20is%20the%20role%20of%20cash%20transfers%20to%20streng.pdf.
11. Ibid., p. 5.
12. Ibid., p. 179.
13. JLICA (see note 3).
14. Adato and Bassett (see note 5), p. 179.
15. In addition to the resources cited in note 7, see, for example, UNICEF, The impact of social cash transfers on children affected by HIV and AIDS (New York: UNICEF, 2007).
16. The pilot program began with the selection of 500 of the poorest families, although the program literature often refers to “500 children.” Both terms are correct in this case. The program goal is expressed in terms of the number of OVC who will benefit. But these gains are sought in the context of the families. The main concerns are the well-being of the children and that they are cared for in the family context.
17. “Evidence from around the world demonstrates that the administrative costs of national cash transfer programs can cost less than 10 percent of total cost. In contrast, small NGOs, the traditional channel for delivering support, may spend 40–60 percent of their budget on administrative costs.” World Bank (see note 7), p. 18, footnote 35.
18. Facing the crisis together (see note 1), p. 16.
19. Hurrell et al. (see note 7).