A Human Right-Based Approach to Dealing with Adverse Events in Residential Care Facilities
Vol 26/1, 2024, pp. 115-127 PDF
Niall McGrane, Laura Behan, and Laura M. Keyes
Abstract
Managing residential care facilities (RCFs) includes the ability to manage adverse events while maintaining a human rights-based approach to care and support. Literature investigating rights-based approaches in RCFs is scarce; therefore, an investigation of the current approach will inform improvements. This study sought to identify whether RCFs in Ireland upheld a rights-based approach during the course of adverse events by analyzing notifications of adverse events from 2021 taken from the Database of Statutory Notifications from Social Care in Ireland. Data analysis was conducted independently by two researchers. Notifications of adverse events were coded according to whether the human rights principles of fairness, respect, equality, dignity, and autonomy were upheld or violated during the adverse event and its subsequent management. There was some evidence of violations, including staff violations during adverse events and their management, as well as residents violating fellow residents’ autonomy, respect, and dignity in notifications of “serious injury” and “allegations of abuse.” However, overall, good practice was identified, with residents’ human rights upheld by staff. Our findings indicate that a rights-based approach to care and support is being upheld during adverse events and their management, which may indicate that such an approach to care and support has been adopted in RCFs in Ireland.
Introduction
Human rights are the basic rights and freedoms that all people should enjoy. They are protected under the Universal Declaration of Human Rights and the European Convention on Human Rights.[1] How these rights are understood and applied so that people with disabilities can fully enjoy their human rights is further addressed in the Convention on the Rights of Persons with Disabilities.[2] A convention on the rights of older persons has not been adopted to date but has been advocated for in the academic literature.[3] Respect for human rights is also implicit within many published codes of conduct and ethics of health and social care professionals.[4] A human rights-based approach to health care and to social care can be considered as adherence to the underlying principles in human rights instruments.
A rights-based approach to delivering care and support for people with disability and older persons ensures that their human rights are protected and supported while availing of health care and social care.[5] Residential care facilities (RCFs) provide health care and social care in the form of accommodation, nursing, and supportive services to people who cannot live independently. In Ireland, RCFs can encompass nursing homes, supportive care facilities, residential homes, rehabilitation centers, and palliative care centers, among other facilities. The care provided by RCFs encompasses both health care and social care and can range from full nursing care to assisted living and from full-time care to respite. Embedding a rights-based approach in the service culture of RCFs ensures that people availing of services are treated with fairness, dignity, respect, and equality and that they can participate fully in decisions about their own care.
The human rights principles outlined in legislation are often used to make up frameworks that can serve as practical tools to guide the implementation of a rights-based approach in practice without the need for knowledge of human rights legislation.[6] Frameworks such as the PANEL principles (participation, accountability, nondiscrimination, and equality) and the FREDA principles (fairness, respect, equality, dignity, and autonomy) have been adopted by national regulators of health and social care to promote and monitor a rights-based approach.[7] Ireland’s Health Information and Quality Authority has published rights-based guidance for RCFs underpinned by the FREDA principles.[8] These tools can also be used by health and social care regulators and researchers to assess for a rights-based approach in health and social care settings.
RCFs are typically regulated with the goal of maintaining and improving the quality of care and safeguarding residents.[9] Regulation can improve the quality and standard of care by implementing improvements across all regulated organizations and by focusing on poorly performing organizations.[10] A rights-based approach to caring for older persons and for people with disability has been called for in the literature.[11] It is a strategic objective of the regulators of RCFs in Ireland and elsewhere, who, in addition to promoting a rights-based approach, identify, challenge, and report on breaches of rights in health and social care services.[12]
A common aspect of regulating RCFs is the statutory mandate to notify the regulator of adverse events, as is the case in Ireland.[13] Statutory notifications from RCFs in Ireland, similar to other jurisdictions, provide detail on the incident, the actions taken by the RCF, and the outcome.[14] They include valuable information that is utilized to assess compliance with regulations, assess levels of risk to residents, and monitor the quality of care and support provided. Analyzing statutory notification data can provide insight into the approach to care and support taken during the management of adverse events in RCFs. This can inform quality improvement across the system.[15] Analyzing notifications can also identify system failures and contributing factors that can inform risk management recommendations and opportunities for quality improvement.[16] Adverse events are complex, can have multiple contributing factors, and are high-stress situations for both residents and staff.[17]
There is a scarcity of literature investigating a rights-based approach in social care and analyzing adverse events, specifically in RCFs. Reviewing statutory notifications provides a method to investigate the approach taken to care and support in health and social care settings. In this light, we designed a study reviewing and analyzing the narratives that are part of statutory notifications of adverse events from RCFs in order to identify if FREDA principles were being violated or upheld during the course of adverse events and their management. This can help inform interventions aimed at improving the quality and safety of RCFs.
Methods
Context
In Ireland, the regulation of RCFs is the responsibility of the chief inspector of social services of the Health Information and Quality Authority. The regulator receives statutory notifications of adverse events from all RCFs that detail the circumstances of the incident, the number of residents involved, and the actions taken by the RCF throughout the adverse event.[18] The free-text data contained in each notification are entered by staff members of the RCF submitting the notification and by the regulatory inspector that reviewed the notification. The nine types of notifications mandated in Ireland are “unexpected death,” “outbreak of infectious disease,” “COVID-19 outbreak,” “serious injury to residents,” “unexplained absence of residents,” “allegations of abuse,” “staff misconduct,” “staff under professional review,” and any “fire, loss of service or unplanned evacuation.” The regulator must be notified of these adverse events within three days of their occurrence. Quarterly reporting is also mandated. Such notifications must describe the RCF’s use of restraints, its operation of fire safety equipment, and the occurrence of theft, non-serious injuries, pressure sores, and expected deaths in the facility. These quarterly notifications differ fundamentally from the three-day notifications because they take a trend approach to monitoring care and safety rather than one based on individual incidents.
We used the Database of Statutory Notifications from Social Care in Ireland 2013–2021 as the basis for our analysis.[19] This database is a comprehensive national repository of all notifications received by the regulator. Each notification received by the regulator is risk rated by the inspector responsible for monitoring the center that submitted the notification. The risk rating is a combination of two values: the risk likelihood and the risk impact. Both of these values range from 1 (lowest risk) to 5 (highest risk). These values are multiplied to derive the risk rating for the notification. The risk rating is color-coded as follows: green=1–3, yellow=4–6, orange=8–12, and red=15–25.
Sample
In order to draw a representative sample that included all service types (n=4; RCFs for older people, RCFs for adults with disabilities, RCFs for children with disabilities, and RCFs for people of all ages with disability), notification types (n=9), and risk rating colors (n=4), we stratified the sample by service type, notification type, and risk rating color. Upon receipt, each notification is assigned a reference number. Notifications received in 2021 (total n=39,336) were extracted from the Database of Statutory Notifications from Social Care in Ireland. Quarterly notifications were excluded from the analysis (n=15,357). Using the random number generator in Microsoft Excel, we drew the top two of each type of notification, stratified as above. Not all types of notifications or risk ratings were received from each type of service. Thus, this method resulted in a total of 194 notifications in our sample for analysis.
Data analysis
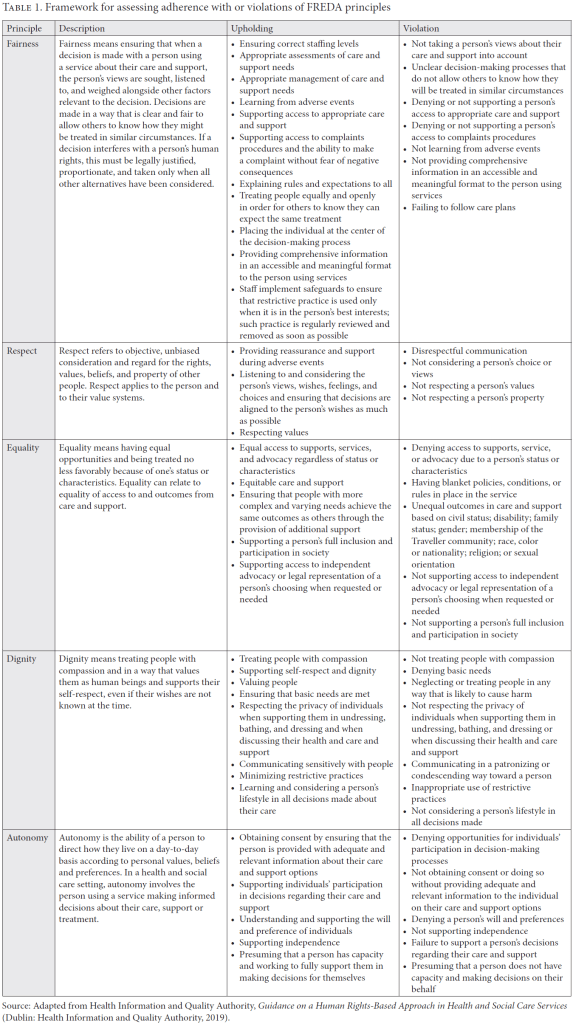
Data were imported into NVivo 1.3 (QSR International) for analysis. The free-text data describing the circumstances surrounding the incident were analyzed independently by two researchers. Line-by-line coding was completed through a deductive approach for each notification in the sample, looking for violations and upholding of the FREDA principles during the adverse event and its management. Both researchers together devised a decision-making framework, assisted by the Health Information and Quality Authority’s published guidance on a rights-based approach to care and support (Table 1).[20] This framework illustrates how each FREDA principle could be violated or upheld. This framework was applied independently to each notification.
Incidents could be coded to one or more of the FREDA principles if one or more were violated or upheld. Each incident was also classified as involving either staff upholding or violating principles, or resident peers upholding or violating principles. Each incident was also classified as to whether it occurred during the adverse event or during the management of the adverse event.
The researchers met to compare the results of their analyses. Disagreements were resolved through discussion or by the involvement of a third researcher. Results are presented as a narrative review of each FREDA principle, with consideration of the notification type and supported by verbatim quotes from the notification. This study is reported in line with the Standards for Reporting Qualitative Research.[21]
Results
The sample drawn consisted of 194 notifications of adverse events, constituting 0.81% of all three-day notifications received in 2021. Table 2 contains a breakdown of the sample, including totals for each stratification by risk rating and percentages of these totals. Notifications of COVID-19 outbreaks were the only notification type in our sample to contain notifications submitted by all types of RCFs and include all risk rating colors (n=32).

Fairness
There was evidence of the principle of fairness being upheld by staff in the management of adverse events in all but notifications of “staff being under professional review.” Examples of upholding fairness included ensuring the correct staffing (“adequate staffing levels remaining, with use of relief & over-time” [NOT-0455444]); appropriate assessments and management of care and support needs (“Effective care planning and interventions in place to support the high risk of fracture, equipment and manual handing procedures and plans in place” [NOT-0413405]); learning from adverse events (“Additional Supervision and ‘early warning/indication’ measures have been put in place, to seek to ensure a non-reoccurrence” [NOT-0480060]); supporting access to appropriate care and support (“A social story was prepared and read to BM09 to inform her that she would be going to the hospital” [NOT-0386103]); supporting access to complaints procedures (“the residents [sic] has been met and a statement of account taken. The residents [sic] understands the issue is being taken seriously” [NOT-0495511]); and explaining rules and expectations and treating people equally (“notified families and residents of these restrictions” [NOT-0513341]).
Violations of fairness by staff in the sample were rare but were found in notifications of “serious injury,” “unexplained absence,” and “fire, service loss or unplanned evacuation.” These violations of fairness included inadequate staffing (“not all staff were on duty as per the planned roster” [NOT-0421817]); not supporting access to the required care (“Resident overnight without medical treatment and/or pain relief and injury not noted until next staff member came on duty” [NOT-0435668]); and not learning from the adverse event (“No details of actions taken to reduce risk of recurrence outlined in notification form” [NOT-0456168]).
Respect
There was a lot of evidence of the principle of respect being upheld by staff in the management of adverse events in all but notifications of “staff under professional review.” The most common manner of upholding respect was by providing reassurance and support to residents in the management of an adverse event, both verbally and physically (“emotional support offered by way of conversation, back and hand rubs” [NOT-0386103]). Respect in communication was also evident (“Social stories were completed with the residents to communicate the loss of water and change in plans” [NOT-0513252]). Respect for choices was also evident in the management of an adverse event (“It was explained to XXX that they were positive for COVID-19, XXX expressed that they did not want to be transferred to hospital and that they wanted to stay” [NOT-0496881] and “XXX and YYY were brought out of the center for activities of their own choosing” [NOT-0441808]). Respect for privacy and values was also evident (“attempted to prevent fellow resident entering as XXXX was undressed from the waist down” [NOT-0386103] and “to be examined by a female physician” [NOT-0375386]).
Violations of respect were evident in notifications of “serious injury,” “allegations of abuse,” and “staff misconduct.” The vast majority of these violations, excluding those in notifications of “staff misconduct,” involved peer-on-peer interactions and were relatively minor physical altercations (“Resident XXXXXX tried to knock the dessert out of their hand and threw a spoon at Resident YYYYYY” [NOT-0430676]) or verbal violations of respect (“the other resident said ‘shut the fuck up, don’t talk to me, go away’” [NOT-0413804]). Staff violations of respect involved disrespectful communication (“staff member alleged to have shouted at a resident” [NOT-0495511]); violations of privacy (“carer had made inappropriate comments and exposed resident inappropriately” [NOT-0418805]); and disrespect in their actions (“staff member has allegedly made the resident feel uncomfortable about calling out for assistance as he presents as annoyed and frustrated when he responds. He is reported to also take longer than needed to respond” [NOT-0456947]).
Equality
Upholding the principle of equality was evident in the management of “outbreaks of infectious disease,” “serious injury,” “unexplained absence,” and “staff misconduct.” Only one violation of equality by staff was identified. This was in a notification of “staff misconduct.”
Evidence of equal treatment with regard to medical concerns was evident (“All residents symptomatic have been reviewed by GP and referred to Dietician” [NOT-0453528]), as was evidence of facilitating equal access to medical treatment (“resident was brought to the A and E where she was met by members of the staff team from the residential service” [NOT-0458542]) and advocacy (“Residents have been offered further supports of contacting an advocate or an identified representative” [NOT-0426556]). Only one instance of a violation of equality was found in a notification of “staff misconduct,” where equal access to care was denied: (“Staff failed to follow protocol around head injury, in particular, failure to get appropriate medical advice following a head injury” [NOT-0417548].)
Dignity
Upholding the principle of dignity was evident in all adverse event notifications except notifications of “unexpected death” and “unexplained absence.” There was evidence of residents being treated with compassion (“Compassionate visits occurring and virtual calls with family” [NOT-0453528] and “additional measures we were putting [sic] in place such as familiar staff only to support resident” [NOT-0497781]) and with value (“nurse who had been assisting her managed to hold her at this stage and prevented the resident from falling to the ground” [NOT-0468320]). Dignity was upheld by staff supporting residents’ self-respect (“care staff remained outside the partly opened door allowing for her privacy” [NOT-0458967]); ensuring that basic needs were met (“Staff ensured person was cleansed & dignity maintained” [NOT-0458967]); and comforting residents in the event of an adverse event (“Emotional first aid and support to regulate” [NOT-0433644]).
Staff violating the principle of dignity was evident in notifications of “serious injury” (“Resident overnight without medical treatment and/or pain relief and injury not noted until next staff member came on duty” [NOT-0435668]); “allegations of abuse” (“Resident XXXXXX had not been brought to the toilet between the hours of 10: 30 and 18:30” [NOT-0414757]); “staff misconduct” (“staff member was being aggressive and verbally abusive towards the resident” [NOT-0441070]); “staff under professional review” (“non-adherence to controls in place including lack of social distancing, overstaying time allocated for visit and not wearing a face shield” [NOT-0421899]); and “fire, service loss or unplanned evacuation” (“they could not bath/shower for one day” [NOT-0513252]).
Violations of dignity also occurred in peer-on-peer interactions and were reported only in notifications of “serious injury” (“Resident XXXX sustained 3 knife wounds, inflicted by peer” [NOT-0442910]) and “allegations of abuse” (“Staff then witnessed XXX intimidatingly staring at YYY and said ‘Shut up’, in a threatening tone. XXX picked up his walking stick and struck YYY with an upwards motion making contact with YYY left wrist” [NOT-0470480]).
Autonomy
Staff supporting and promoting the principle of autonomy was evident in the sample in all but notifications of “outbreaks of infectious disease,” “staff misconduct,” and “staff under professional review.” Obtaining consent and supporting informed decisions about their own care was evident (“advised for hospital transfer to rule out injury- resident agreeable” [NOT-0456217]), even if it was against what had been advised (“resident is refusing to comply with full medical advice, in that he is refusing to wear the boot at night” [NOT-051879405]). Supporting participation in decisions made on care and support was evident (“handover at 8 am with consultation with XXXX so he can plan his daily activity” [NOT-0457704]). Understating and supporting the will and preferences of residents was evident (“resident wishes to contact family when choosing to do so” [NOT-0491340]) and (“requested to go out on the bus which staff facilitated and he got a takeaway which he appeared to enjoy” [NOT-0431685]). Supporting independence was also evident in the sample (“Resident went on a planned outing unaccompanied as per protocol” [NOT-0462696]).
Incidents of staff violating autonomy occurred in notifications of “unexplained absence,” “allegations of abuse,” and “staff misconduct.” Violations included restrictive practices (“restrictions now in place for minimum of one month, no friend visits, no internet access, no use of smart phone. House doors locked at all times, no independent shopping trips” [NOT-0447579]); failure to support decisions regarding care (“The advocate neglected to facilitate the resident’s stated wishes when they agreed to the advocate visiting” [NOT-0491401]); and failing to facilitate care plans (“A staff member is alleged to have fed a service user in a manner that did not adhere to a resident specific FEDS plan” [NOT-0426556]).
Human rights-based approach during the adverse event and its management
The vast majority of adverse events in our sample contained examples of staff upholding a rights-based approach to care and support in the management of an adverse event. There were numerous examples of staff upholding all of the FREDA principles in each type of adverse event notification, excluding “staff under professional review.” There was also evidence of staff upholding each FREDA principle during the adverse event, although not as numerous as in the management of an incident.
Violations of the FREDA principles occurred mainly in the adverse event itself (and not in the management of such events), where there was evidence of violations of all five principles. In the management of such events, there was evidence only of the violation of autonomy and fairness.
Staff and peer-on-peer evidence
In the majority of notifications in our sample, staff upheld a rights-based approach when managing adverse events and during events. There were a small number of notifications containing staff violations of the FREDA principles, with the majority being notifications of “staff misconduct.”
Peer-on-peer interactions were responsible for violations of respect, dignity, and autonomy, and these were in notifications of “serious injury” and “allegations of abuse.”
Discussion
Summary of findings
Notifications of adverse events from RCFs in Ireland contained evidence that a rights-based approach to care and support is being upheld by staff during adverse events and their management. RCF staff upholding FREDA principles was evident in all types of notifications except for notifications of “staff under professional review.” Although there were examples of the FREDA principles being violated by staff, these were few in number, and no violations were identified in notifications of “unexpected death,” “outbreaks of infectious diseases,” and “outbreaks of COVID-19.” Evidence of residents violating their fellow residents’ autonomy, respect, and dignity were observed, but only in notifications of “serious injury” and “allegations of abuse.”
Statutory notifications from RCFs in Ireland, similar to other jurisdictions, provide detail on the incident, the actions taken by the RCF, and the outcome.[22] This valuable information can be utilized in a variety of ways: assessing compliance with regulations, assessing risk, monitoring quality of care, or providing insight into the approach to care and support taken during the management of adverse events. Adverse events are complex, can have multiple contributing factors, and are high-stress situations for both residents and staff.[23] Evidence of a rights-based approach during times of high stress may indicate that a rights-based approach to care and support in general has been widely adopted in RCFs in Ireland. Staff ensuring that the FREDA principles are protected and supported during adverse events may point toward a rights-based approach being embedded in the service culture. Conversely, an adverse event—being complex, a time of high stress, and out of the ordinary—may be the only time a rights-based approach is taken.
This is the first study to rely on notifications of adverse events to investigate whether a rights-based approach is being implemented in RCFs, and there is a scarcity of literature that investigates experiences of a rights-based approach in social care. Applying the same FREDA framework used here to other data sources, such as inspection reports or investigations of complaints received by the regulator, may provide insight into the approach taken by RCFs during the routine care and support of everyday life. In support of our finding, a review of rights-based approaches in mental health and disability and dementia care settings indicated that a rights-based approach can be successfully implemented and is of benefit to those receiving treatment.[24] A study published in 2020 that used regulator inspection reports to investigate human rights in RCFs for people with an intellectual disability in Ireland indicated that a rights-based approach had not been implemented.[25] This study, which developed its own human rights framework based on the United Nations Convention on the Rights of Persons with Disabilities, indicated that restrictive practices are in use and that residents are subject to abuse, neglect and isolation and are not empowered.[26] In contrast, our study indicates that a rights-based approach to care and support is being embraced by RCFs. This contrasting finding may be because our focus was on acute incidents and not routine care, using adverse event notification data instead of inspection reports. This suggests that the presence of a rights-based approach during adverse events may not translate to the presence of a rights-based approach in routine care and support. In support of this lack of generalizability, a study using the same database as our study investigated the use of restrictive practices in nursing homes in Ireland and showed the indiscriminate use of restrictive practices in RCFs, suggesting that the FREDA principles are being violated.[27] The measurement of the implementation or impact of a rights-based approach is not simple, however, as measuring typical health outcomes does not capture the effects of a rights-based approach to health care and to social care, and statutory notifications do not portray the everyday approach to care and support.[28]
Human rights legislation, codes of professional conduct, and national standards advocate for a shift away from a paternal approach to care and support toward a rights-based approach.[29] There has also been a call in the literature to implement a rights-based approach to health care and social care since the United Nations outlined the need for a rights-based approach in all of its agencies.[30] Education on human rights for health care professionals and care workers can improve decision-making skills in practice.[31] Educating the public can also benefit those being cared for and supported in RCFs, as it can provide confidence to question the nature and quality of care for older people.[32] A review, published in 2015, on the impact of human rights legislation in health care and social care in England and Wales, however, indicated that a rights-based approach was not realized. The author of this review states that the Human Rights in Healthcare Programme, which was introduced in 2005, had not led to a shift away from a paternalistic approach to care and support toward a rights-based approach.[33] The author argues that the development of human rights-based resources has had a beneficial effect but that the overall implementation has not been as successful, for a multitude of reasons.
The people being cared for in RCFs are residents, not patients, and the goal of care differs from other health care services. While there is substantial research into adverse events in acute settings, there is a paucity of data and research relating to adverse events in other settings, including RCFs.[34] In RCFs, a rights-based approach may result in compromises being made that would not be made in acute services and this, in certain circumstances, may cause a disparity in risk management and conflict with restrictive practices aimed at reducing the risk of adverse events. Adverse events in RCFs are complex and can have multiple causes, and striking the balance between risk management, control, and monitoring and the promotion of autonomy, liberty, independence, choice, comfort, quality of life, and positive risk taking may explain some of the violations of the FREDA principles that were evident in our sample. There are competing demands of empowerment and the duty of care for staff; however, staff have a responsibility to, and not a responsibility for, residents.[35] In nursing practice studies, it has been identified that challenges can arise when practitioners need to achieve a balance between upholding the human rights of individuals while protecting these individuals’ health and well-being and maintaining their duty of care as practitioners.[36] This has also been identified with supporting people who are at risk and may lack the capacity to make a decision but still require their human rights to be upheld.[37]
The comprehensive reporting of adverse events is important for understanding the event and for learning by both those reporting and those receiving notifications.[38] Identifying violations of the FREDA principles by staff in statutory notifications of adverse events can assist RCFs and the regulator in the further implementation of a rights-based approach and in making the elimination of violations of FREDA principles by staff potentially achievable. Violations of FREDA principles in notifications of “staff misconduct” suggest that the RCFs are aware of violations from staff and are actually upholding the FREDA principles and implementing a rights-based approach by reporting these violations. However, the complete elimination of violations during resident-to-resident interactions may not be achievable, as is the case in almost all situations where people live with other people. Monitoring for patterns of these interactions and taking preventative action, however, would help reduce incidents of violations of dignity and respect by fellow residents.
Strengths and limitations
To the best of our knowledge, this is the first investigation of the use of a rights-based approach to care and support in RCFs. Our work is also unique in that it utilized notifications of adverse events to the regulator to investigate the approach to care and support during adverse events. The sample was extracted from the Database of Statutory Notifications from Social Care in Ireland, a national database that contains all notifications of adverse events received by the regulator from RCFs in Ireland commencing in 2013.[39] This national database may not be complete, as it may not contain every adverse event that occurs in RCFs in Ireland. However, the risk of this is low given that reporting adverse events to the regulator is legally required and RCFs are monitored and inspected. Our sample was stratified for types of notifications, types of RCFs and risk ratings, ensuring that a large representative sample was analyzed.
The free-text data in statutory notifications are written by RCF employees and regulatory inspectors. This is both a strength and a limitation. Using data contained in notifications means that the data collection method is commensurate across events and no bias was introduced by the researchers in its collection. Notifications are, however, a single point of view that include personal opinions and biases and are influenced by the culture of the RCF.[40] Those completing forms may attempt to put their best foot forward and not apportion blame or reveal a non-rights-based approach to the management of the adverse event. Although the form is the same for everyone, the language, terminology, and writing skills are not. Establishing an evidence base on the implementation of a rights-based approach requires the use of a variety of study designs using a range of sources. These include audits, regulatory inspection reports, focus groups with residents and staff, and observational studies.
The interpretation of the FREDA principles and the framework for coding the notifications was devised by the authors without input from service providers or from residents of RCFs. Their input on the interpretation of the FREDA principles in the development of the framework may have resulted in a different framework. The findings presented are therefore limited to our interpretation of the FREDA principles. That said, the framework was devised using the Health Information and Quality Authority’s guidance on a rights-based approach to care and support, which was published in 2019.[41] This meant that stakeholders had over two years to become familiar with the Health Information and Quality Authority’s interpretation of the FREDA principles.
The authors who performed the analysis were experienced in the method and complemented each other in their experience of the fields of care, statutory notifications, and human rights. A third researcher strengthened the analysis by resolving any disagreements. The sampling strategy was developed by researchers with in-depth knowledge of the nuances of adverse events in RCFs and the nuances in the provision of care and support in RCFs. As a result, the sample should reflect the approach taken during adverse events in RCFs in Ireland.
Conclusion
Our analysis of a sample of notifications received by the social care regulator in Ireland detailing adverse events in RCFs indicates that a rights-based approach to care and support is being upheld during adverse events. There was evidence of violations of human rights by staff and by residents, but these were minor in nature and few in number. In RCFs, there are competing demands to promote a rights-based approach and to avoid harm or injury that are not present in other health care services, such as acute care, which may explain the violations by staff. In these situations where human rights are competing with risk management, staff need to consider the applicability and weighting of each right within that situation and their duty of care to ensure safety and fairness for all residents. While eliminating violations of human rights by staff is potentially achievable, eliminating violations during resident-to-resident interactions may not be. Monitoring for patterns of these interactions and taking preventative action, however, would help ensure that residents’ human rights are upheld in RCFs.
Ethics
We did not seek ethical approval for this analysis given that it is a secondary analysis of routinely collected regulatory data pertaining to events as opposed to individuals. The data do not contain any identifiable personal data.
Niall McGrane, PhD, is a regulatory researcher at the Health Information and Quality Authority, Dublin, Ireland.
Laura Behan, PhD, is a senior regulatory researcher at the Health Information and Quality Authority, Cork, Ireland.
Laura M. Keyes, PhD, is a regulatory practice and researcher manager at the Health Information and Quality Authority, Cork, Ireland.
Please address correspondence to Niall McGrane. Email: nmcgrane@hiqa.ie.
Competing interests: The authors are employed as researchers by the health and social care regulator of Ireland.
Copyright © 2024 McGrane, Behan, and Keyes. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/bync/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948); European Convention on Human Rights, European Treaty Series No. 5 (1950).
[2] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006); M. A. Stein, P. Stein, D. Weiss, and R. Lang, “Convention on the Rights of Persons with Disabilities,” European Journal of Health Law 14/3 (2007).
[3] I. Doron and I. Apter, The Debate around the Need for an International Convention on the Rights of Older Persons,” Gerontologist 50/5 (2010); C. Peisah, C. de Mendonça Lima, H. Verbeek, and K. Rabheru, “IPA and WPA-SOAP Joint Statement on the Rights of Older Persons with Mental Health Conditions and Psychosocial Disabilities,” International Psychogeriatrics 34/11 (2022); C. Peisah, E. L. Sampson, K. Rabheru, et al., “The Human Rights of Older People with Mental Health Conditions and Psychosocial Disability to a Good Death and Dying Well,” American Journal of Geriatric Psychiatry 29/10 (2021).
[4] Irish Association of Social Workers, Code of Practice (Dublin: Irish Association of Social Workers, 2020); Nursing and Midwifery Board of Ireland, Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives (Dublin: Nursing and Midwifery Board of Ireland, 2021); Irish Medical Council, Guide to Professional Conduct and Ethics, 8th edition (Dublin: Irish Medical Council, 2019).
[5] M. J. Curtice and T. Exworthy, “FREDA: A Human Rights-Based Approach to Healthcare,” Psychiatrist 34/4 (2010).
[6] Ibid.
[7] Scottish Human Rights Commission, Health and Social Care Alliance, and NHS Health Scotland, Human Rights in Health and Social Care: Putting it into Practice; Case Studies from Scotland (Scotland: Scottish Human Rights Commission, 2019); Health Information and Quality Authority, Guidance on a Human Rights-Based Approach in Health and Social Care Services (Dublin: Health Information and Quality Authority, 2019); Quality Care Commission, Our Human Rights Approach for How We Regulate Health and Social Care Services (London: Quality Care Commission, 2019).
[8] Health Information and Quality Authority (2019, see note 7).
[9] K. Walshe and A. Boyd, “Designing Regulation: A Review,” Regulation 3/2 (2007).
[10] Ibid.
[11] Peisah et al. (2022, see note 3); Peisah et al. (2021, see note 3); Walshe and Boyd (see note 9); N. Rushford and D. Harvey, “Dementia as a Disability and Human Rights Issue,” Healthcare Papers 16/2 (2016); E. Evans, S. Howlett, T. Kremser, et al., “Service Development for Intellectual Disability Mental Health: A Human Rights Approach,” Journal of Intellectual Disability Research 56/11 (2012); D. Banerjee, K. Rabheru, C. A. de Mendonca Lima, and G. Ivbijaro, “Role of Dignity in Mental Healthcare: Impact on Ageism and Human Rights of Older Persons,” American Journal of Geriatric Psychiatry 29/10 (2021); S. Fitzgerald, L. Behan, S. McCarty, et al., “Translating a Human Rights-based Approach into Health and Social Care Practice,” Journal of Social Care 3/1 (2020).
[12] Health Information and Quality Authority, Annual Report (Dublin: Health Information and Quality Authority, 2022); Scottish Human Rights Commission et al. (see note 7); Quality Care Commission (see note 7); Health Information and Quality Authority (2019, see note 7).
[13] Australian Government, Aged Care Quality and Safety Commission Act 2018 (2018); Government of Ireland. Care and Welfare of Residents in Designated Centres for Older People Regulations 2013 (2013); Government of Ireland, Care and Support of Residents in Designated Centres for Persons (Children and Adults) with Disabilities) Regulations 2013 (2013); Government of Northern Ireland, Article 23 (7)(d) The Health and Social Services (Quality, Improvement and Regulation) Order 2003 (2003); Government of the United Kingdom, Health and Social Care Act 2008 (2008); S. Abimbola, J. Negin, A. L. Martiniuk, and S. Jan, “Institutional Analysis of Health System Governance,” Health Policy Plan 32/9 (2017).
[14] Government of Ireland, Care and Welfare of Residents (see note 13); Government of Ireland, Care and Support of Residents (see note 13); Government of Northern Ireland (see note 13).
[15] N. McGrane, S. O’Regan, P. Dunbar, et al., “Management and Reporting of Safety Incidents by Residential Care Facilities in Ireland: A Thematic Analysis of Statutory Notifications,” Health and Social Care in the Community 30/6 (2002); I. Leistikow, S. Mulder, J. Vesseur, and P. Robben, “Learning from Incidents in Healthcare: The Journey, Not the Arrival, Matters,” BMJ Quality and Safety 26/3 (2017).
[16] N. McGrane, P. Dunbar, and L. M. Keyes, “Contributing Factors to Adverse Events in Long-Term Care Facilities in Ireland: A Content Analysis,” Journal of the American Medical Directors Association 25/4 (2024).
[17] Ibid.; R. Amalberti, D. Benhamou, Y. Auroy, and L. Degos, “Adverse Events in Medicine: Easy to Count, Complicated to Understand, and Complex to Prevent,” Journal of Biomedical Informatics 44/3 (2011); A. Cobos-Vargas, P. Pérez-Pérez, M. Núñez-Núñez, et al., “Second Victim Support at the Core of Severe Adverse Event Investigation,” International Journal of Environmental Research and Public Health 19/24 (2022).
[18] Government of Ireland, Care and Welfare of Residents (see note 13); Government of Ireland, Care and Support of Residents (see note 13); Government of Ireland, Health Act 2007 (2007).
[19] S. O’Regan, N. McGrane, P. Dunbar, et al., “Public Reporting of Adverse Events from Long-Term Care Facilities for Older Persons and People with Disability in Ireland 2013–2019: Development of an Openly Accessible Database and Descriptive Analyses,” Journal of the American Medical Directors Association 23/8 (2022).
[20] Health Information and Quality Authority (2019, see note 7).
[21] B. C. O’Brien, I. B. Harris, T. J. Beckman, et al., “Standards for Reporting Qualitative Research: A Synthesis of Recommendations,” Academic Medicine: Journal of the Association of American Medical Colleges 89/9 (2014).
[22] Government of Ireland, Care and Welfare of Residents (see note 13); Government of Ireland, Care and Support of Residents (see note 13); Government of Northern Ireland (see note 13).
[23] McGrane et al. (see note 16); Amalberti et al. (see note 17); Cobos-Vargas (see note 17).
[24] S. Porsdam Mann, V. J. Bradley, and B. J. Sahakian, “Human Rights-Based Approaches to Mental Health: A Review of Programs,” Health and Human Rights Journal 18/1 (2016).
[25] K. Murphy and E. Bantry-White, “Behind Closed Doors: Human Rights in Residential Care for People with an Intellectual Disability in Ireland,” Disability and Society 36/5 (2021).
[26] Ibid.
[27] World Health Organization, Global Priorities for Patient Safety Research (Geneva: World Health Organization, 2009).
[28] L. Dyer, “A Review of the Impact of the Human Rights in Healthcare Programme in England and Wales,” Health and Human Rights Journal 17/2 (2015).
[29] R. Newham, A. Hewison, J. Graves, and A. Boyal, “Human Rights Education in Patient Care: A Literature Review and Critical Discussion,” Nursing Ethics 28/2 (2021).
[30] United Nations Development Group, The Human Rights Based Approach to Development Cooperation: Towards a Common Understanding among UN Agencies (New York: United Nations, 2003).
[31] S. Every-Palmer, L. Kininmonth, G. Newton-Howes, and S. Gordon, “Applying Human Rights and Reducing Coercion in Psychiatry following Service User-Led Education: A Qualitative Study,” Health and Human Rights Journal 23/2 (2021); P. Hunt, A. E. Yamin, and F. Bustreo, “Making the Case: What Is the Evidence of Impact of Applying Human Rights-Based Approaches to Health?,” Health and Human Rights Journal 17/2 (2015); Dyer (see note 28).
[32] T. Jessop and C. Peisah, ‘Human Rights and Empowerment in Aged Care: Restraint, Consent and Dying with Dignity,” International Journal of Environmental Research and Public Health 18/15 (2021).
[33] Dyer (see note 28).
[34] World Health Organization (see note 27).
[35] S. Baxter and H. Carr, “Walking the Tightrope: The Balance Between Duty of Care, Human Rights and Capacity,” Housing, Care and Support 10/3 (2007).
[36] C. Cole, S. Wellard, and J. Mummery, “Problematising Autonomy and Advocacy in Nursing,” Nursing Ethics 21/5 (2014); R. Griffith and C. Tengnah, “The Influence of Human Rights on District Nurse Practice,” British Journal of Community Nursing 14/10 (2010).
[37] Baxter and Carr (see note 35).
[38] C. Macrae, “The Problem with Incident Reporting,” BMJ Quality and Safety 25 (2015).
[39] O’Regan et al. (see note 19); Health Information and Quality Authority, Database of Statutory Notifications from Social Care in Ireland (unpublished database).
[40] Macrae (see note 38).
[41] Health Information and Quality Authority (2019, see note 7).