VIEWPOINT Upholding Human Rights in the Wake of COVID-19: Time to Strengthen Pharmaceutical Accountability
Volume 24/2, December 2022, pp. 205-209 | PDF
Rosalind Turkie
Introduction
Pharmaceutical companies have the power and the responsibility to help governments realize the human right to health for all, yet there are egregious examples—such as the recent COVID-19 pandemic—where companies have violated these responsibilities. The Pharmaceutical Accountability Foundation, a nonprofit organization based in the Netherlands, argues that it is time to hold drug companies accountable for their excessive pricing policies and abuse of the intellectual property framework.[1] As a first step toward accountability, the foundation developed a monitoring and evaluation scorecard to measure pharmaceutical companies’ compliance with human rights during the COVID-19 pandemic. The results of this scorecard, published in June 2022, demonstrate that stronger regulation is needed to obtain better adherence to human rights in the pharmaceutical field (see Figure 1). We propose a legal standard in Dutch law—a requirement for a duty of care—as a promising avenue for enforcing the pharmaceutical industry’s human rights responsibilities, which has been difficult until now.
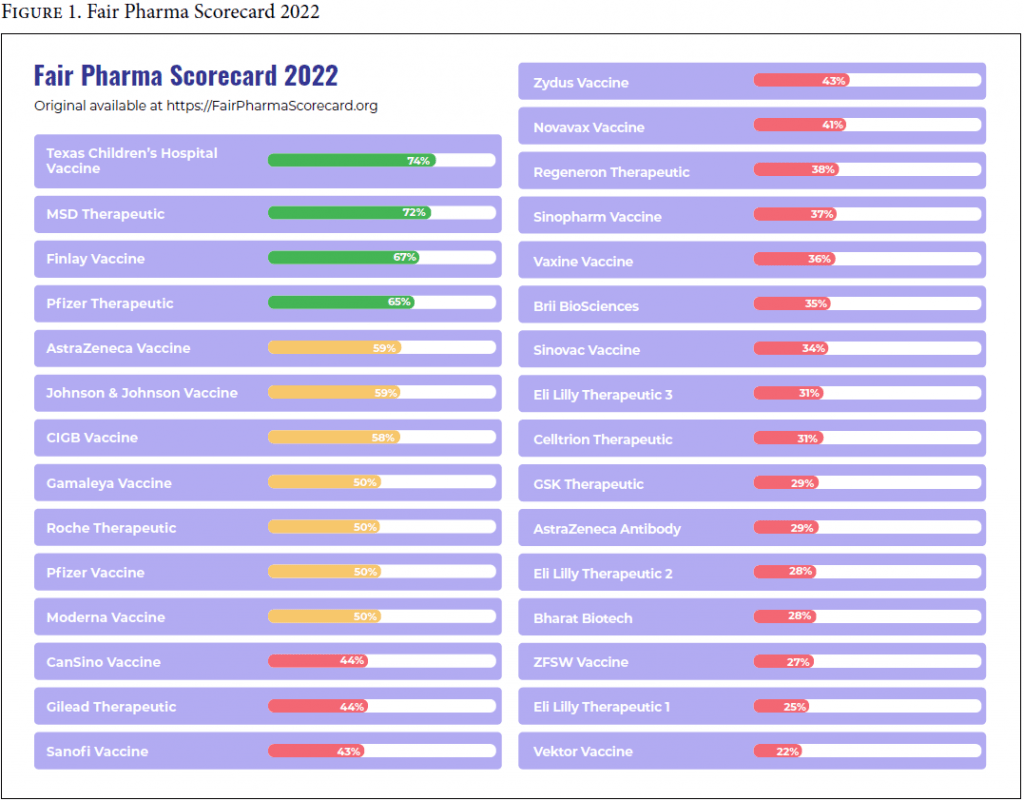
Figure 1. Fair Pharma Scorecard 2022
Pharmaceutical companies and access to medicines: Key players, limited accountability
Ensuring access to essential medicines is part of the core obligations imposed on governments under the right to the highest attainable standard of health.[2] However, private companies cannot be held directly accountable for failing to uphold the right to health, unless national law allows for this. The United Nations Guiding Principles on Business and Human Rights, endorsed by the Human Rights Council in 2011, clarify that businesses have a secondary set of nonbinding responsibilities to respect human rights.[3] These principles have been largely acknowledged by major pharmaceutical companies around the world.
Pharmaceutical companies play an essential role in countries’ health care systems by researching and developing new drugs to treat or prevent new and existing diseases. Governments across Europe outsource the development, production, and sale of medicines to such companies, without imposing conditions on the results.[4] Access to medicines is thus no longer controlled by the state but largely by the private pharmaceutical sector. Although governments are required to regulate private companies when their activities interfere with human rights, in practice this is challenging. International law does not provide mechanisms for enforcing pharmaceutical companies’ human rights responsibilities, which has led to their poor implementation.
A first step toward accountability: Global monitoring and evaluation
In June 2022, the Pharmaceutical Accountability Foundation assessed the roots of global COVID-19 vaccine and therapeutics inequality through its publication of the Fair Pharma Scorecard, which evaluates how producers of COVID-19 vaccines and therapeutics performed according to international human rights principles during the pandemic.[5] The scorecard assessment is based on the Human Rights Guidelines for Pharmaceutical Companies, developed by Paul Hunt, the 2002–2008 United Nations Special Rapporteur on the right to health.[6] The foundation adapted these guidelines into a framework for monitoring and evaluating pharmaceutical companies’ behavior and then used this framework to score companies on four categories—accountability, equity, international cooperation, and transparency—divided into 19 criteria of equal weight (see Table 1). We used a three-point scale to score information on company behavior. All companies with a COVID-19 vaccine or therapeutic marketed in any country were selected for scoring, resulting in 26 companies being scored on 30 products. Data collection took place through structured internet searches, crowdsourcing information from civil society and professional organizations, and direct consultation with the companies. Each company was informed of its score and invited to comment and provide additional information prior to publication of the scorecard.
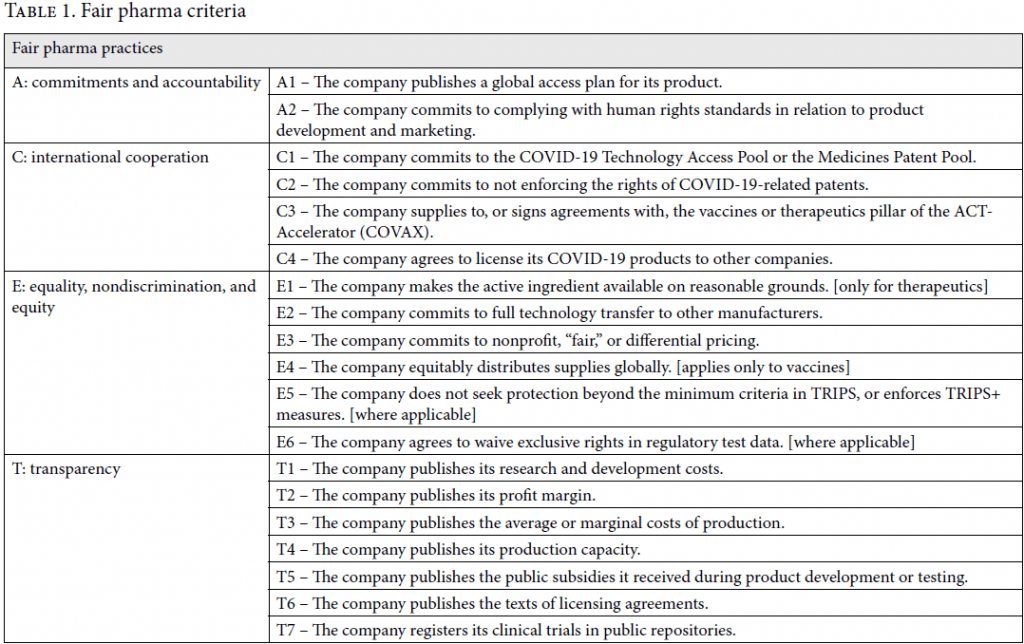
Table 1. Fair pharma criteria
The Fair Pharma Scorecard: An indicator of good and bad practices
The scorecard results show that several pharmaceutical companies acknowledge some form of responsibility for human rights: 9 out of 26 companies publicly accept the United Nations Guiding Principles on Business and Human Rights on their websites or publish their own human rights policy documents. Despite this, 19 companies scored poorly overall, showing that pharmaceutical companies largely failed to comply with human rights principles during the pandemic. The scorecard is a useful tool for pointing out the areas in which companies perform well and those where they are failing. For example, while 20 companies publish their production capacity, only 6 score full points for fair or differential pricing practices and for distributing their product equitably. Only two companies have committed to the COVID-19 Technology Access Pool or the Medicines Patent Pool—pooling mechanisms for the sharing of technology and medical products—showing a generalized lack of willingness to share intellectual property, knowledge, and data in global solidarity. Our World in Data estimates that today, for every 100 people in high-income countries, 214 vaccines have been administered, but in low-income countries, this figure drops to 31 doses—meaning that seven times more vaccines have been administered in high-income countries.[7] Although many variables were involved in the global allocation of COVID-19 vaccines, the scorecard suggests that increased compliance with human rights norms by drug companies during the pandemic could have contributed to a more equitable global vaccine coverage.
The need for legal accountability mechanisms
Notably, all 26 companies scored full points for publishing their clinical trial results—a legal requirement in most countries, and the only criterion matched by binding norms. This suggests that translating human rights principles into “hard” law may achieve higher compliance rates than relying on “soft” enforcement mechanisms. Reinforcing this is the fact that companies often refuse to release raw data after publication of the initial trial results, as access to these data—not assessed in the scorecard—is not effectively covered by existing legislation. Full transparency is therefore probably achievable only when required by law.
Overall, the scorecard shows that drug companies need to improve their adherence to human rights principles in order to respect the right to health. It also suggests that this will require going beyond moral and ethical responsibilities through the establishment of binding accountability mechanisms. Legal avenues to hold pharmaceutical companies directly accountable for infringements of the right to health are required at both the international and the domestic level. National law has the advantage of being directly enforceable within the concerned state and can address the problem at its source. Moreover, successful domestic policies can then become the source of “legal transplants” from one state to another. Recent developments in Dutch case law suggest that domestic litigation in the Netherlands could be successful in establishing strong norms for holding the pharmaceutical industry accountable.
Next steps for pharmaceutical accountability: The Dutch example
The Dutch civil courts are a promising avenue for enforcing pharmaceutical human rights responsibilities at the national level. In 2021, the District Court of the Hague held a private company liable for violating its duty of care in the unprecedented Milieudefensie v. Shell judgment.[8] Relying on article 6:162 of the Dutch Civil Code, containing an “unwritten” standard of care, the court held that private companies have individual obligations to act in accordance with generally accepted norms of social conduct—including human rights.[9] A new Dutch precedent could be created for pharmaceutical companies, using the same provision to create accountability for noncompliance with human rights. A company could then be held liable under Dutch law, for example, for the excessive pricing of medicines resulting in the displacement of health care budgets. Displaced budgets refers to the opportunity costs in health systems with finite health care budgets, meaning that public funds spent in one area (for example, expensive medicines) prevents financing for treating patients in another area and hinders the realization of their right to health. Generating a legal precedent that flouting human rights is not socially acceptable is one way of realizing the judicial enforcement of the right to health at the national level and could inspire other civil law systems to similarly strengthen pharmaceutical accountability in their jurisdictions.
Conclusion
The Fair Pharma Scorecard quantifies pharmaceutical companies’ compliance with human rights principles during the COVID-19 pandemic. The overall picture is that pharmaceutical companies are not sufficiently adhering to certain human rights norms that are essential to the realization of the right to health. The results clearly indicate the need for robust accountability mechanisms in this field: failure to establish these will entrench health inequalities among the world’s most vulnerable populations. Accountability through national law may be easier to implement than international approaches and, if successful, can inspire other states to adopt similar approaches to the problem. Strategic litigation in the Netherlands is one way to bring accountability in this sector and ensure that pharmaceutical companies’ influence on public health systems facilitates equitable access to medicines worldwide, as the Dutch courts have shown that they are willing to hold private companies accountable for not complying with their social duty of care. It is now time to test this principle on the pharmaceutical industry.
Disclaimer
The Pharmaceutical Accountability Foundation is funded by Unitaid, and this article was submitted as part of the foundation’s funding deliverables. Unitaid had no role in the study design. The author has not been paid to write this article by a pharmaceutical company or any other agency. The author was not precluded from accessing data in the study and accepts responsibility to submit for publication.
Acknowledgments
I would like to thank Wilbert Bannenberg, chairperson of the Pharmaceutical Accountability Foundation, for his technical support and writing assistance. I am also grateful to Katrina Perehudoff, Brigit Toebes, Tegan Insoll, and Jennifer Sellin for their valuable feedback.
Rosalind Turkie, LLM, is a human rights researcher at the Pharmaceutical Accountability Foundation, Amsterdam, Netherlands.
Please address correspondence to the author. Email: GCCP@farmaterverantwoording.nl.
Competing interests: None declared.
Copyright © 2022 Turkie. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original authors and source are credited.
References
[1] Pharmaceutical Accountability Foundation, “Fair Pharma Scorecard” (June 2022), https://fairpharmascorecard.org.
[2] Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000).
[3] Office of the United Nations High Commissioner for Human Rights, Guiding Principles on Business and Human Rights, UN Doc. HR/PUB/11/04 (2011).
[4] See, for example, O. Dyer, “COVID-19: Moderna Seeks to Exclude US Government Scientists from Vaccine Patents, Despite Public Investment,” BMJ (Novemer 12, 2021).
[5] See Pharmaceutical Accountability Foundation (see note 1).
[6] United Nations General Assembly, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN Doc. A/63/263 (2008).
[7] See Our World in Data, “Cumulative COVID-19 Vaccinations per 100 People,” https://ourworldindata.org/grapher/covid-vaccination-doses-per-capita?tab=table.
[8] Milieudefensie et al v. Royal Dutch Shell (May 26, 2021) ECLI:NL:RBDHA:2021:5337.
[9] Burgerlijk Wetboek (Civil Code) (1992), art. 6:162.