The Right to Science as a Guidepost for Fair Access to COVID-19 Vaccines: Investigating the Interpretive Role of the United Nations Committee on Economic, Social and Cultural Rights
Volume 24/2, December 2022, pp. 191-204 | PDF
Katrina Perehudoff and Jennifer Sellin
Abstract
Facing the unmet need for new, affordable medicines for public health crises, how should states’ duty to ensure that everyone shares in the benefits of science be understood in relation to pandemic vaccine supply, and how has the United Nations Committee on Economic, Social and Cultural Rights monitored the implementation of this right? In this paper, we examine the contours and content of state obligations with regard to pandemic vaccine supply under the right to science (article 15(1)(b) of the International Covenant on Economic, Social and Cultural Rights), focusing on three aspects of state obligations: mobilizing public resources for developing and disseminating the benefits of scientific progress in areas of public health need; preventing unreasonably high medicines prices; and international cooperation, particularly in a globalized health emergency. The committee regularly assesses state parties’ implementation of their obligations under the covenant, culminating in the issuing of concluding observations, which often serve as a basis for the next round of periodic reporting by states and can thereby direct future state action. Our analysis of the committee’s concluding observations reveals that the committee has inconsistently applied its own guidance on the right to science regarding medicines and intellectual property in these monitoring exercises. These findings inform a rights-based response to medical innovation for health crises and advance the Sustainable Development Goal target on medicines research and development.
Introduction
The right to participate in and enjoy the benefits of scientific progress and its applications (“right to science”) has recently emerged and been lauded as potentially transforming persistent theoretical debates and practical societal challenges in science policy.[1] One of these persistent debates is where duties lie to develop and make widely accessible lifesaving medical technologies, particularly in a health emergency. Ongoing health crises (from HIV/AIDS to the Avian flu) and localized epidemics (e.g., tuberculosis, malaria, and vaccine-preventable diseases) illustrate the intrinsic link between the preservation of human dignity and policy decisions about which medical products to prioritize for development, financing, and distribution, and on what terms. A rights-based response requires states—working individually and cooperating globally—to adequately resource and prioritize biomedical research and development (R&D) in the public interest and equitably distribute the resulting goods. By many measures, gaps in government oversight of previous public health crises have translated into life-threatening failures to develop needed vaccines and therapeutics (termed “medicines”), and in delays in these products reaching people at risk.[2]
The recently unearthed right to science has the unique potential to guide state action and international cooperation on biomedical innovation. The right to science is found in a range of sources, most notably the 1948 Universal Declaration of Human Rights, whose article 27(1) provides that “everyone has the right … to share in scientific advancement and its benefits,” and the 1966 International Covenant on Economic, Social and Cultural Rights (ICESCR), which enshrines the right to science in article 15(1)(b).[3] With 171 ratifying states, the ICESCR imposes legal obligations on the majority of the world’s governments to translate the commitments embodied in the ICESCR into domestic law, policy, and practice.
Article 15(1)(b) recognizes everyone’s right “to enjoy the benefits of scientific progress and its applications.” The “benefits” of science are widespread and cover “the material results of the applications of scientific research, such as vaccinations,” as well as the “scientific knowledge and information directly deriving from scientific activity.”[4] Together with the concept of progressive realization in article 2(1) of the ICESCR, scientific progress conveys the idea of a positive impact on human welfare and is seen as an instrument for human benefit.[5] To explicate state parties’ obligations under article 15(1)(b), this provision must be read with reference to its paragraphs (2)–(4) and article 2 of the covenant. States must progressively achieve the full realization of the right to science and must take immediate steps within a “reasonably short period of time.”[6] State parties have an obligation to respect, protect, and fulfill the right to science.[7]
How should states’ duty to ensure that everyone shares in the benefits of science be understood in relation to pandemic vaccine supply, and how has the United Nations (UN) Committee on Economic, Social and Cultural Rights monitored the implementation of this right? These questions gained a sense of global urgency due to the COVID-19 pandemic (declared in March 2020) and the elaboration of the right to science by the committee in General Comment 25 (adopted in April 2020). Since its inception, the right to science has been rather neglected within international human rights law, being referred to by some scholars as a “sleeping beauty.”[8] Only in the last two decades has the (academic) debate slowly focused on this right. The 2009 Venice Statement on the Right to Enjoy the Benefits of Scientific Progress and Its Applications, the result of expert meetings initiated by the UN Educational, Scientific and Cultural Organization, was a first important step toward the elucidation of the right’s normative content and state obligations.[9]
This paper uses the COVID-19 pandemic as a “laboratory” to examine the contours and content of state obligations with regard to pandemic vaccine supply under the right to science, and a kind of “sandbox” to understand to what extent this global health crisis has informed the Committee on Economic, Social and Cultural Rights’ ongoing interpretation of the right to science, as articulated in its concluding observations on state parties’ reports. Section two briefly outlines why biomedical R&D tends to be neglected in medical fields such as pandemic pathogens. Section three traces the evolution of state obligations for regulating biomedical R&D in the instructive general comments of the Committee on Economic, Social and Cultural Rights. Section four continues this examination from the perspective of the right to science, pinpointing three salient aspects of state obligations: public financing for biomedical R&D; preventing unreasonably high medicines prices; and international cooperation. Section five compares the committee’s monitoring of state action before and during the COVID-19 pandemic to assess the extent to which the committee has applied its own interpretation of state duties under the right to science in relation to COVID-19 vaccines. These findings inform a rights-based response to medical innovation for health crises and advance the Sustainable Development Goal target on medicines R&D.[10]
Why is R&D neglected in certain medical fields?
The current biomedical R&D model incentivizes innovation by rewarding inventors with a time-limited market monopoly for producing, using, and selling their end product. These monopoly rewards, enforced through intellectual property rights (IPRs) (such as patents) and other exclusivities granted by states, effectively prevent competition and enable the owner to largely set the price and production terms of its product. Intellectual property (IP) is argued to stimulate innovation by allowing developers to recoup their investments in R&D. These same incentives tend to draw medicines to the market for “profitable” diseases, characterized as affecting large or wealthy populations with certainty. One of the criticisms of such a market-based R&D model is that it fails to incentivize new medicines for unprofitable conditions or populations, sometimes termed “neglected fields.”
For nearly two decades, coronavirus infections (causing severe acute respiratory syndrome, Middle East respiratory syndrome, and COVID-19) have been overlooked by market-driven pharmaceutical R&D despite the fact they caused pandemics in 2002, 2012, and 2020.[11] When the COVID-19 pandemic struck in March 2020, there was still no marketed coronavirus vaccine. Pandemic pathogens (e.g., Ebola, coronaviruses) are forgotten by private biomedical R&D because they may or may not strike, leading to uncertainty about potential profits. The number of vaccine producers globally has declined in the last two decades, and notably in the public sector, further concentrating and privatizing global vaccine development and manufacturing capacity.[12] The result was clear already in the 2009 swine flu pandemic, and again in the COVID-19 pandemic, when limited vaccine manufacturing capacity and lack of a global mechanism to allocate supplies fairly triggered a global race for scarce supplies. Wealthy states crowded out governments unwilling or unable to pay to be first in the distribution line, receiving more doses faster than states dependent on donations.[13] In response, a coalition of states proposed at the World Trade Organization (WTO) a time-bound waiver to the protection of patents and other forms of IP needed to manufacture products for the prevention, containment, and treatment of COVID-19. Rather than an IP waiver, a declaration affirming the existing flexibilities in the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) was adopted at the 12th WTO Ministerial Conference in June 2022.
States have several regulatory tools by which they can shape the market for new medicines needed for health emergencies.[14] Public financing of the private R&D process is one policy measure that should be paired with access conditionalities for the resulting medicine. Managing IP is another policy option that rests in states’ sovereign power to grant or override patents and other forms of IP and exclusivities related to medicines in order to protect public health. Another, more transformative, policy option is adapting the innovation model so the costs of R&D are “delinked” from the production and prices of the resulting medicine. This range of public policy responses to securing access to medical countermeasures to a pandemic raises important questions about the scope and contours of states’ human rights obligations to protect and promote the right to science in response to a health emergency.
Access to medicines: The evolution in the Committee on Economic, Social and Cultural Rights’ general comments
Public health emergencies and access to medicines generally are human rights issues. Depending on the nature and enforceability of these rights, their implementation may be monitored by various bodies, including the Committee on Economic, Social and Cultural Rights, the Committee on the Rights of the Child, the Committee on the Rights of Persons with Disabilities, the Human Rights Committee, and domestic human rights agencies. Given this paper’s focus on the ICESCR, this section focuses on the evolution of the Committee on Economic, Social and Cultural Rights’ interpretation of access to medicines as part of the rights to health and to science.
In one of its first general comments, the committee stated that state parties are not acting in compliance with their human rights obligations where significant parts of their population do not have access to essential primary health care.[15] A decade later, in its General Comment 14 on the right to health issued in 2000, the committee clarified that public health goods must be available, (economically) accessible, scientifically and medically appropriate, and of good quality and that states subsequently have a minimum core obligation to provide essential medicines.[16] Although not specifically referring to health emergencies, it explained that states’ duty to provide health care includes promoting medical research, immunization programs against major infectious diseases, and measures to prevent, treat, and control epidemic diseases.[17] Yet it did not detail how states should go about achieving this, except for reiterating the importance of international cooperation.[18] Rather, the committee’s approach was focused predominantly on the state’s obligation of result, specifically to ensure that essential public health goods, such as medicines, are developed and made available and accessible without discrimination.[19] In other words, in its efforts to delineate and operationalize the right to health for states, the committee identified the destination (provision of essential medicines for all) without addressing possible roadblocks or signaling possible detours to more efficiently and effectively reach this end goal.
The nature of science and especially the state’s role in promoting science has significantly changed since the adoption of the ICESCR more than 50 years ago. (Bio)medical and pharmaceutical research is now largely a commercial enterprise, and that has affected the research objectives, priorities, processes, and outcomes of science.[20] However, despite the growing role of the private sector in the protection and promotion of health rights, the committee has provided sparse guidance to states about how to regulate the business sector with regard to (bio)medical R&D, beyond instructing states to facilitate the private sector to discharge its human rights responsibilities related to health.[21] Although, therewith, it has acknowledged the critical role of the state in shaping the environment so that nonstate actors contribute to the realization of the covenant’s rights.
In 2005, the committee issued another general comment addressing the tension in the Universal Declaration of Human Rights and ICESCR between the seemingly competing notions of the protection of authors’ rights and the right of all to benefit from scientific advancement.[22] At the outset, General Comment 17 resolutely outlines that authors’ rights cannot and must not be conflated with IPRs.[23] It starts to unpack the role of the state in maintaining an R&D system that fosters the realization of human rights, including access to affordable medicines. For example, states are required to prevent the use of scientific and technical advances for purposes contrary to human rights and dignity. As a result, they can exclude “inventions from patentability whenever their commercialization would jeopardize the full realization of these rights.”[24] Moreover, it reaffirms the state’s duty to regulate the human rights responsibilities of the “private business sector, private research sector, and other non-State actors.”[25] Importantly, in relation to IPRs, the general comment asserts that the private interests of authors should not be unduly favored over the interests of the public. States have a core obligation “to strike an adequate balance” between authors’ rights and other rights recognized by the covenant.[26] The general comment, though, does not detail how such an adequate balance should be struck, except by noting that any national or international IP regime should not impede the state’s ability to comply with its core obligations and that states have “a duty to prevent unreasonably high costs for access to essential medicines, … from undermining the rights of large segments of the population to health.”[27] In its subsequent general comment on sexual and reproductive health, issued in 2016, the committee does provide a concrete recommendation to ensure that IP regimes do not “impede access to medicines, diagnostics or related technologies,” namely by incorporating “to the fullest extent any safeguards and flexibilities” contained within international IP treaties, such as TRIPS and the Doha Declaration on TRIPS and Public Health.[28]
Since then, the committee has acknowledged the active role that states play in structuring the current biomedical R&D model and its relationship to the high prices of end products. General Comment 24 on state obligations toward economic, social, and cultural rights in the context of business activities, issued in 2017, recognizes for the first time that states are actors “designing a framework on [IPRs],” which must be consistent with human rights standards.[29] The committee links states’ role in shaping the IP system with their duty to ensure that IPRs result in neither a “denial or restriction of everyone’s access to essential medicines” that is crucial for the enjoyment of health rights.[30]
Over time, the committee’s interpretations have increasingly recognized the different dimensions of state obligations to ensure access to medicines. General Comment 25 on science and economic, social, and cultural rights continues that evolution. Notably, and unsurprisingly considering the timing, it also addresses state duties during a pandemic, a dimension that previously was not touched on by the committee.
State obligations under the right to science
State action on R&D efforts for medicines needed in health emergencies must take account of all relevant human rights, including the right to health and the right to science, among others. The Committee on Economic, Social and Cultural Rights qualifies the right to science as having an intrinsic value and an instrumental value as an essential tool to realize the right to health, among others.[31] This paper focuses on the nascent right to science as a real-time guidance for designing and executing medicines R&D for public health crises, as it offers us a “global ethical discourse” to balance potentially conflicting interests.[32]
In general terms, the scope of the right to science is wide-ranging. It requires from state parties that science in the broadest sense, and its benefits and material applications, such as vaccines, be available, accessible, of quality, and acceptable. This is also evident from article 15(2) of the ICESCR, which clarifies that all necessary steps must be taken for “the conservation, the development and the diffusion of science.” Required state action, therefore, encompasses everything from ensuring that science is taking place, to adequately regulating the scientific process to minimize risk, and subsequently widely disseminating the results and benefits of that process, in particular serving the needs of marginalized groups. This section takes a closer look at three illustrative but non-exhaustive dimensions of state duties fundamental for assessing state action on medicines for health emergencies that can be derived from, but are not limited to, the right to science: (1) adequate financial support for R&D of public importance; (2) preventing unreasonably high costs for access to essential medicines; and (3) international cooperation, which acts as a cross-cutting aspect that transverses the foregoing obligations. These three elements are crucial for a rights-based response to health emergencies. Moreover, they are, to varying degrees, linked to states’ core obligations under the ICESCR.
Nonstate actors have an essential role to play in developing and diffusing scientific progress. Since the inclusion of the right to share in scientific advancement in the Universal Declaration of Human Rights, the nature of doing science has fundamentally changed. Biomedical and pharmaceutical (multinational) corporations are now major players in health R&D and innovation, and are key actors that contribute to, or impact, essential medicines being globally available, accessible, and affordable. As a result, there is—rightly so—increased attention on outlining the human rights responsibilities of (pharmaceutical) corporations.[33] Even so, the committee maintains a clear focus on states as the primary duty bearers, neglecting the separate responsibilities of nonstate actors. Therefore, the analysis below focuses on the duties of states as elaborated by the committee in its newest General Comment 25 on science and economic, social, and cultural rights.
Adequate financial support for R&D of public importance
As stated above, and similarly to other economic, social, and cultural rights, the committee finds that the right to science encompasses the following: availability, accessibility, quality, acceptability, and the protection of scientific freedom.[34] States have “a positive duty to actively promote the advancement of science through, inter alia, education and investment in science and technology.”[35] That requires, among other things, creating an enabling and participatory environment, as well as allocating appropriate resources in budgets.[36] The committee has identified the obligation to develop a national framework law and to adopt and implement a national strategy or plan of action as a prioritized core obligation.[37]
In the context of a health emergency, the duty to fulfill the right to science therefore demands appropriate financing for R&D to ensure that needed medical products are available and subsequently (economically) accessible. The committee has confirmed that states have a core obligation to “ensure that in the allocation of public resources, priority is given to research in areas where there is the greatest need for scientific progress in health … and the well-being of the population, especially with regard to vulnerable and marginalized groups.”[38] It needs no elaboration why a safe and effective vaccine against an infectious disease outbreak is absolutely crucial to safeguard the right to health and a range of other economic, social, and cultural rights, considering both the short- and long-term impacts of health crises on health systems and economies around the world. Consequently, states should provide adequate financial support for R&D for public health threats, either through national efforts or, if necessary, by resorting to international and technical cooperation.
Moreover, when governments fund science, they must take special care, within the funding structures and processes, to ensure that the results are widely disseminated and accessible.[39] By referring to both development and diffusion, article 15(2) of the ICESCR recognizes that the state’s duty to promote, facilitate, and support science—the development element—is closely connected to the duty to ensure that everyone has access to the benefits of science—the diffusion element.[40]
Preventing unreasonably high costs for access to essential medicines
Broad dissemination is needed to ensure that everyone has equal access to the benefits of science, especially when they are instrumental for the enjoyment of other economic, social, and cultural rights.[41] The committee recognized early on that the right to health requires state action to ensure that essential medicines are affordable. The right to science reinforces the idea that access to medicines for future health crises not be unduly inhibited by their cost, especially for vulnerable and marginalized groups. New medicines for health crises should therefore, as far as possible, be “accessible and affordable”—which requires that states use their maximum available resources to overcome any hurdles that individuals may face when trying to benefit from new medical applications and technologies.[42] States have core obligations to eliminate laws, policies, and practices “that unjustifiably limit access by individuals or particular groups to facilities, services, goods and information related to science, scientific knowledge and its applications,” as well as to take positive measures to ensure access to those applications of scientific progress “that are critical to the enjoyment of the right to health.”[43]
The state, however, is by no means the only or even the most dominant actor that affects individuals’ access to affordable essential medicines. The privatization of (bio)medical and pharmaceutical research has significantly impacted the manner in which science is conducted, facilitated, and promoted, as well as the role of the state in that regard. States’ duty to protect takes on special importance, as the privatization of science should not result in the enjoyment of economic, social, and cultural rights being made “conditional on the ability to pay.”[44] Particularly the development of national and international IP regimes associated with private scientific research can have negative effects on the enjoyment of access to the benefits of scientific progress. The right to science has a complex relationship with IP protection.[45] The committee acknowledges that IP protection intends to provide incentives to innovate, while at the same recognizing that IPRs can result in distortions in the funding of science, limitations to the sharing of scientific information and research (e.g., data exclusivity provisions), and significant obstacles for persons trying to access the benefits of science.[46]
To incite a positive effect of IP on access to the benefits of science, states should (at least) take the following steps. First, as elaborated above, states should provide adequate financial support for R&D of public importance to counter distortions of funding associated with IP. The right to science also encourages states to make use of other incentives, such as “market entry awards,” which introduce the notion of “de-linkage.”[47]
Second, states must take steps to ensure the “social dimension” of IP—in other words, the capacity of IP to promote the realization of economic, social, and cultural rights in national legislation and international agreements on IP.[48] The committee reiterates that “States parties have a duty to prevent unreasonably high costs for access to essential medicines.”[49] Therefore, states must work toward a balance between the protection of IP, on the one hand, and access to and sharing of scientific knowledge and its applications, especially those linked to the right to health, on the other. Accordingly, the right to science becomes a significant mediator between human rights, especially the right to health, and IP protection.[50] In striking this balance, the private interests of authors should not be unduly favored over the public interest in enjoying access to their productions. Moreover, the obligations of states under IP treaties must not compromise the implementation of their human rights obligations.[51] Thus, to ensure access to essential medicines, especially for the most disadvantaged, the committee asserts that states should use all flexibilities found in the TRIPS Agreement as confirmed by the Doha Declaration on the TRIPS Agreement and Public Health.[52] For example, states should refrain from granting disproportionately lengthy terms of patent protection for new medicines and should make use of compulsory licensing so as to promote the production of cheaper generic medicines.[53] The UN Special Rapporteur on cultural rights has also recommended the use of patent pools.[54]
The cross-cutting obligation of international cooperation
Health is, generally, recognized as a global and shared responsibility.[55] This recognition is, for example, evidenced by article 44 of the World Health Organization’s International Health Regulations, which is widely accepted, including by all World Health Organization members. Global health emergencies are prime examples of the necessity for a collective global response. Consequently, the state’s human rights duties outlined above must be read in light of the cross-cutting obligation of international cooperation.
The duty of international cooperation, specifically to promote an enabling global environment for the advancement of science, flows from articles 55–56 of the UN Charter and article 2(1) of the ICESCR and is reinforced by article 15(4) of the ICESCR, which recognizes “the benefits to be derived from the encouragement and development of international contacts and cooperation in the scientific fields.”[56] Notably, states have a core obligation to “foster the development of international contacts and cooperation in the scientific field.”[57] In addition, all states should contribute, to the maximum of their available resources, to the common task of developing science.[58] The right to science acknowledges that science is a global good but that deep international disparities in science and technology continue to exist among states.[59] Consequently, the committee recognizes the responsibilities of particularly developed states to contribute to the development of science and technology and to share the benefits and applications of scientific progress with low- and middle-income countries.[60]
The committee already acknowledges this in its interpretation of the right to health, where it notes that states should undertake “individual and joint efforts to, inter alia, make available relevant technologies, using and improving epidemiological surveillance and data collection on a disaggregated basis, the implementation or enhancement of immunization programmes and other strategies for infectious disease control.”[61]
The international community has a “collective responsibility,” while developed states have a “special responsibility,” to assist developing states with regard to diseases that are easily transmissible beyond borders.[62] The right to science clarifies that “access to research results and their applications should be regulated in a form that allows developing countries and their citizens adequate access to [essential medicines] in an affordable manner.”[63] Moreover, states should share the benefits and applications resulting from scientific progress and its applications with the international community, particularly with developing countries, communities living in poverty, and groups with special needs and vulnerabilities.[64] Notably, a “stronger commitment” to international cooperation is required when combating pandemics.[65] The general comment, however, gives little guidance on how states should discharge this obligation. Benefits and applications should be shared “with due incentives and regulations.”[66] States should share scientific information about potential pathogens and improve early warning systems.[67]
In conclusion, General Comment 25 builds on and deepens the committee’s previous interpretations of the ICESCR’s rights. It offers a starting point to assess state action in relation to pandemic vaccine supply. The next section examines to what extent the COVID-19 pandemic has informed the committee’s understanding of the right to science as articulated in its concluding observations on state parties’ periodic reports.
Monitoring the right to science
Treaty monitoring bodies are important actors for holding states accountable to their human rights obligations. The Committee on Economic, Social and Cultural Rights regularly assesses state parties’ implementation of their obligations under the ICESCR through the reporting procedure. The committee offers specific guidance to states reporting on their actions; in relation to the right to science, the committee’s 2009 guidelines invite states to
- Indicate:
(a) The measures taken to ensure affordable access to the benefits of scientific progress and its applications for everyone, including disadvantaged and marginalized individuals and groups; and
(b) The measures taken to prevent the use of scientific and technical progress for purposes which are contrary to the enjoyment of human dignity and human rights
.…
- Indicate the measures taken for the conservation, development and diffusion of science and culture and to encourage and develop international contacts and co-operation in the scientific and cultural fields.[68]
In this monitoring process, states submit periodic reports to the committee every five years detailing their actions taken to realize covenant rights. These periodic reports are considered alongside submissions from other treaty bodies and independent sources (e.g., nonstate actors, which may submit shadow reports).[69] After considering all information received, the committee publishes its concluding observations highlighting positive aspects and areas of concern. There is a feedback loop by which concluding observations often serve as a basis for the next round of periodic reporting by states. Benjamin Meier et al. confirm that states’ subsequent reports on public health topics and right to health norms are “largely responsive” to the issues highlighted in previous sets of concluding observations.[70] In this way, the committee can influence state accountability toward covenant rights, provided that both the treaty monitoring body and state parties effectively report on salient human rights relevant for health. A study of the state reports submitted to the committee between 1992 and 2013 found that this was not always the case. Over 21 years, 114 states reported on the right to science in their reports, while 51 state parties did not.[71] A more recent study identified that of the 170 state parties that have submitted reports (139 in total), the great majority (129) have reported taking specific measures to implement the right to science.[72]
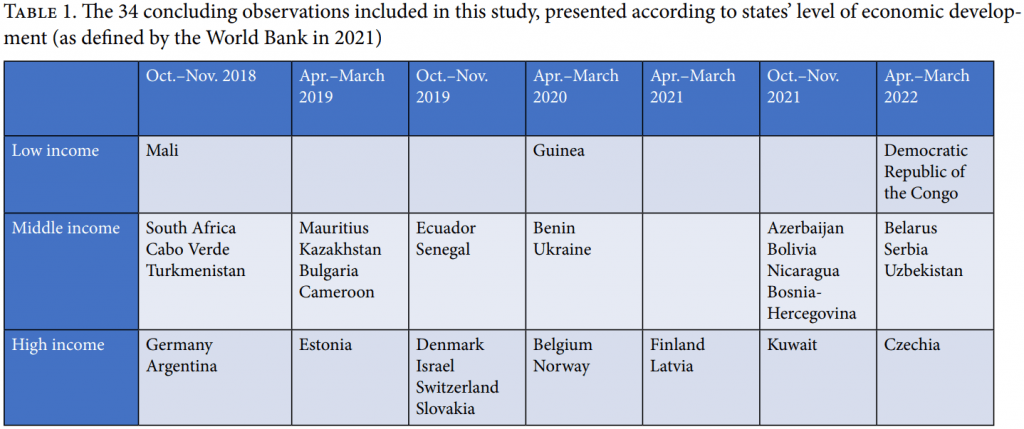
This section presents the findings of an analysis of references to medicines as part of the right to science in all 34 of the committee’s concluding observations of state reports published between 2018 and 2022 (see Table 1). This period was selected because it includes a series of concluding observations before and (just) after the COVID-19 pandemic was declared in March 2020. It is noteworthy that the committee members who authored General Comment 25 are also those who monitored state parties between 2020 and 2022. Consequently, we hypothesize that the committee would be highly inclined to reference its General Comment 25 in subsequent concluding observations.
Within each monitoring report, relevant passages were identified by an automated search for the terms “scien,” “vacc,” “health,” and “technol,” followed by a manual check of the hits for references to the right to science and its components. Our analysis reveals the relative importance of the right to science in the committee’s practice of monitoring state compliance between 2018 and 2022.
Pre-COVID-19 (2018–2019)
Prior to COVID-19, the committee’s assessment of state action with respect to article 15 of the ICESCR was generally limited to cultural aspects of the right to science (such as respect for minority or Indigenous languages) or digital rights such as access to the internet.[73] In our sample, few explicit references are made to “science” as part of the right to science, and where they do exist, those references are either rather vague or surprisingly specific.[74] None of the pre-pandemic concluding observations comment on the right to science’s role with respect to facilitating and promoting biomedical R&D or the availability and accessibility of vaccines or medicines during a crisis.
“Post”-COVID-19 (2020–2022)
In relation to vaccines, the right to science is mentioned in half of the concluding observations published after March/April 2020 (n=6 out of 12 states), and in none adopted in March or April 2020, when the COVID-19 pandemic was declared and General Comment 25 was published. Adopting a general comment may have been an impetus for the committee to more formally and explicitly refer to the right to science and make recommendations for state action in subsequent concluding remarks.
However, when it comes to specific recommendations for state action, few of the concluding observations in 2021 and 2022 actually addressed global vaccine inequity in comparable terms to General Comment 25. Among the most obvious references are the committee’s notes that Uzbekistan, Latvia, and Finland have not played an “active role” (or indicated they would play an active role in the future) “in advocating for universal, equitable and affordable access to COVID-19 vaccines and drugs in regional and international organizations” they are members of.[75] Following this statement, the committee makes explicit reference to arts. 2(1), 12, and 15 of the ICESCR.[76] Moreover, the committee urges these states to
make every effort to exercise [their] leverage in regional and international organizations of which [they are] a member to advocate for universal, equitable and affordable access to COVID-19 vaccines and drugs, including through the possibility of supporting the proposals made at the World Trade Organization of establishing a temporary waiver for some intellectual property rights for vaccines at least for as long as the pandemic continues.[77]
In a number of its concluding observations, the committee simply calls on the state to “pay particular attention” to General Comment 25 or to the committee’s earlier statements on the COVID-19 pandemic and economic, social, and cultural rights, or to ensure equitable access to COVID-19 vaccines.[78] Curiously, no reference is made either to the right to science or General Comment 25 in concluding observations published alongside the above recommendations in November 2021 (Bolivia) or in March/April 2022 (Belarus, Czechia, Democratic Republic of the Congo, and Serbia). Whereas the European Union block was a notable opponent to the original waiver proposal circulated at the WTO in October 2020, the committee missed the opportunity to address this opposition in its March 2022 concluding observations on Czechia, which is a member of the European Union.[79]
The committee has promoted international collaboration in relation to COVID-19 vaccines in its concluding observations. For example, it praised Kuwait’s “support to COVAX, the vaccines pillar of the Access to COVID-19 Tools Accelerator” while “regretting”
the lack of information on specific measures taken by the State party to ensure that the projects that it engages in take into account the principle of universal access to science and technology (art. 15).[80]
Consequently, it recommended that Kuwait integrate the right to science “into its plans to develop a knowledge economy in the framework of its ‘New Kuwait’ vision, as well as to any other projects it implements on the national or international levels.”[81] In other instances, the committee has made vague references encouraging the state to take account of paragraph 82 of General Comment 25 on international cooperation in a pandemic, and the committee’s statement on COVID-19 vaccination, international cooperation, and IP.[82] In response to Finland, the committee paid extra attention to international cooperation, remarking that in relation to access to COVID-19 vaccines and drugs, the state should take account of paragraph 39 of General Comment 14 on international cooperation in the context of the right to health.[83] Moreover, the committee “regrets the State party’s slow progress towards reaching the internationally agreed target for official development assistance (art. 2 (1)),” a statement that the committee has made before in its concluding observations on high-income countries, although the committee’s following recommendations for official development assistance do not specifically relate to the COVID-19 pandemic.[84]
Besides addressing issues of global drug development and international cooperation, the committee has used its concluding observations to address domestic inequities that can be related to vaccines, such as “the challenges faced by disadvantaged and marginalized groups to access to culture and the benefit of scientific research,” unequal access to COVID-19 vaccines, the “lack of access to information” that has failed to prevent the spread of COVID-19, and the limited access to health care for refugees, asylum seekers, and migrants, impairing effective measures to contain COVID-19 in reception centers.[85]
Finally, accountability is a key characteristic of the committee’s monitoring process. States receive specific recommendations from the committee and are instructed to follow up within a given time frame by presenting information about the implementation of those recommendations. In our sample, Finland was the only country to receive specific follow-up instructions related to its efforts to leverage its membership of regional and international organizations to advocate for “universal, equitable, and affordable access to COVID-19 vaccines and drugs,” including the possibility of supporting the waiver proposal.[86] Curiously, other countries in a similar position as Finland (e.g., Czechia) are not held to the same degree of accountability on this matter by the committee.
Conclusion
Fifty-four years after its birth in the ICESCR, the right to science has come of age in the Committee on Economic, Social and Cultural Rights’ General Comment 25. This authoritative interpretation moves states’ human rights obligations concerning access to new medicines beyond the IP-health protection deadlock. With this in mind, this paper has examined how states’ duty to ensure that everyone shares in the benefits of science should be understood, and the extent to which the committee has assessed state action on COVID-19 vaccines using its own interpretation of state duties under the right to science. The committee emphasizes the importance of mobilizing public resources for developing and disseminating the benefits of scientific progress in areas of public health need, delinking R&D costs from medicine prices, and safeguarding the “social function” of IP. Special attention is given to states’ cross-cutting duty of international cooperation, particularly in a globalized health emergency. However, our analysis of the committee’s concluding observations reveals that the committee has inconsistently applied its own standards regarding medicines and IP in these monitoring exercises to hold states to account. This research reveals a need to strengthen the link between the normative development of the right to science (in General Comment 25) and the ICESCR’s monitoring exercises. The Committee on Economic, Social and Cultural Rights plays a key role in clarifying the existing norms in the field of health and human rights. Its concluding observations should, at the very least, direct states’ attention to the recent General Comment 25 and its implications for state action on medicines in global health crises. Given the dearth of global fora for monitoring international cooperation to realize human rights, the committee should hold states to account on matters of global solidarity for access to the benefits of scientific progress (e.g., pandemic medicines).
Acknowledgments
This work was supported in part by a grant from Unitaid to the Pharmaceutical Accountability Foundation and Medicines Law & Policy.
Katrina Perehudoff, MSc, LLM, PhD, is an assistant professor at the Law Centre for Health and Life at the Faculty of Law, University of Amsterdam, Netherlands. She is affiliated with the Amsterdam Institute of Global Health & Development, Netherlands; the World Health Organization Collaborating Centre for Governance, Accountability, and Transparency in the Pharmaceutical Sector at the University of Toronto, Canada; and Medicines Law & Policy, Amsterdam, Netherlands.
Jennifer Sellin, LLM, PhD, is an assistant professor in the Department of International and European Law and a member of the Maastricht Centre for Human Rights at the Faculty of Law, Maastricht University, Netherlands.
Please address correspondence to Katrina Perehudoff. Email: s.k.perehudoff@uva.nl.
Competing interests: None declared.
Copyright © 2022 Perehudoff and Sellin. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original authors and source are credited.
References
[1] S. Porsdam Mann, H. Porsdam, and Y. Donders, “‘Sleeping Beauty’: The Right to Science as a Global Ethical Discourse,” Human Rights Quarterly 42/2 (2020), pp. 332–333.
[2] H. Brandswell, “Against All Odds”: The Inside Story of How Scientists across Three Continents Produced an Ebola Vaccine,” Statnews (January 7, 2020), https://www.statnews.com/2020/01/07/inside-story-scientists-produced-world-first-ebola-vaccine/; M. Herder, J. E. Graham, and R. Gold, “From Discovery to Delivery: Public Sector Development of the rVSV-ZEBOV Ebola Vaccine,” Journal of Law and the Biosciences 7/1 (2020), p. 1.
[3] This paper uses the term “right to science” despite the term not capturing the full meaning of the right.
[4] Committee on Economic, Social and Cultural Rights, General Comment No. 25, UN Doc. E/C.12/GC/25 (2020), para. 8.
[5] Human Rights Council, Report of the UN Special Rapporteur in the Field of Cultural Rights, Farida Shaheed, UN Doc. A/HRC/20/26 (2012), para. 24.
[6] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 23.
[7] Ibid., paras. 43–50.
[8] Porsdam Mann et al. (see note 1), pp. 332–333; W. A. Schabas, “Looking Back: How the Founders Considered Science and Progress in Their Relation to Human Rights,” European Journal of Human Rights 2015/4 (2015), p. 504.
[9] UNESCO, The Right to Enjoy the Benefits of Scientific Progress and Its Applications (Venice: UNESCO, 2009).
[10] See generally S. Porsdam Mann and M. M. Schmid, “Health Research Priority Setting: State Obligations and the Human Right to Science,” American Journal of Bioethics 18/11 (2020), p. 33.
[11] E. Padron-Regalado, “Vaccines for SARS-CoV-2: Lessons from Other Coronavirus Strains,” Infectious Diseases and Therapies 9/2 (2020), p. 255.
[12] J. Hendriks, “Technology Transfer in Human Vaccinology: A Retrospective Review on Public Sector Contributions in a Privatizing Science Field,” Vaccine 30/44 (2012), p. 6230; S. Blume, “The Erosion of Public Sector Vaccine Production: The Case of the Netherlands,” in C. Holmberg, S. Blume, and P. Greenough (eds), The Politics of Vaccination: A Global History (Manchester: Manchester University Press, 2017), p. 148.
[13] M. Turner, “Vaccine Procurement during An Influenza Pandemic and the Role of Advance Purchase Agreements: Lessons from 2009-H1N1,” Global Public Health 11/3 (2016), p. 322.
[14] K. Perehudoff, E. ‘t Hoen, K. Mara, et al., “A Pandemic Treaty for Equitable Global Access to Medical Countermeasures: Seven Recommendations for Sharing Intellectual Property, Know-How and Technology,” BMJ Global Health 7 (2016), pp. 2–4.
[15] Committee on Economic, Social and Cultural Rights, General Comment No. 3, UN Doc. E/1991/23 (1990), para. 10.
[16] Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc E/C.12/2000/4 (2000), paras. 12, 43(d). Similarly, Committee on Economic, Social and Cultural Rights, General Comment No. 22, UN Doc. E/C.12/GC/22 (2016), para. 49(g).
[17] Committee on Economic, Social and Cultural Rights (2000, see note 16), paras. 36, 44(b)–(c).
[18] Ibid., para. 40.
[19] Ibid., para. 12; Committee on Economic, Social and Cultural Rights (2016, see note 16), paras. 12–21.
[20] A. R. Chapman, “Towards an Understanding of the Right to Enjoy the Benefits of Scientific Progress and Its Applications,” Journal of Human Rights 8/1 (2009), pp. 1, 8.
[21] Committee on Economic, Social and Cultural Rights (2000, see note 16), para. 42.
[22] Porsdam Mann (see note 1), pp. 332, 339.
[23] Committee on Economic, Social and Cultural Rights, General Comment No. 17, UN Doc. E/C.12/GC/17 (2006), paras. 1–3. See further Human Rights Council (2012, see note 5), para. 57; United Nations General Assembly, Report of the UN Special Rapporteur in the Field of Cultural Rights, UN Doc. A/70/279 (2015), para. 90; A. Plomer, “IP Rights and Human Rights: What History Tells Us and Why It Matters,” in H. Porsdam and S. Porsdam Mann (eds), The Right to Science: Then and Now (Cambridge: Cambridge University Press 2022), pp. 58–60.
[24] Committee on Economic, Social and Cultural Rights (2006, see note 23), para. 35.
[25] Ibid., para. 55.
[26] Ibid., para. 39(e).
[27] Ibid., para. 35.
[28] Committee on Economic, Social and Cultural Rights (2016, see note 16), para. 51.
[29] Committee on Economic, Social and Cultural Rights, General Comment No. 24, UN Doc. E/C.12/GC/24 (2017), para. 24.
[30] Ibid.
[31] Committee on Economic, Social and Cultural Rights (2020, see note 4), paras. 63, 67.
[32] Porsdam Mann (see note 1), pp. 332, 356.
[33] Human Rights Council, Report of the UN Special Representative to the Secretary General on the Issue of Human Rights and Transnational Corporations and Other Business Enterprises, Annex; Guiding Principles on Business and Human Rights: Implementing the United Nations “Protect, Respect, and Remedy” Framework, UN Doc. A/HRC/17/31 (2011); United Nations General Assembly, Report of the UN Special Rapporteur on the Right to Health, Annex; Human Rights Guidelines for Pharmaceutical Companies in relation to Access to Medicines, UN Doc. A/63/263 (2008).
[34] Committee on Economic, Social and Cultural Rights (2020, see note 4), paras. 16–20.
[35] Ibid., para. 46.
[36] Ibid.
[37] Ibid., para. 52.
[38] Ibid.
[39] United Nations General Assembly (2015, see note 23), para. 109.
[40] M. Frick, I. Henry, and E. Lessen, “Falling Short of the Rights to Health and Scientific Progress: Inadequate TB Drug Research and Access,” Health and Human Rights Journal 18/1 (2016), pp. 9–10.
[41] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 17.
[42] Ibid., para. 47.
[43] Ibid., para. 52.
[44] Committee on Economic, Social and Cultural Rights (2017, see note 29), para. 22.
[45] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 60.
[46] Ibid., para. 61.
[47] Ibid., para. 62; Human Rights Council (2012, see note 5), para. 34; United Nations General Assembly (2015, see note 23), para. 108.
[48] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 62.
[49] Ibid.
[50] Ibid., para. 69.
[51] United Nations General Assembly (2015, see note 23), para. 89.
[52] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 69. See also Human Rights Council (2012, see note 5), paras. 58–61; United Nations General Assembly (2015, see note 23), paras. 63–70; International Commission of Jurists, Human Rights Obligations of States Not to Impede the Proposed COVID-19 TRIPS Waiver: Expert Legal Opinion (Geneva: International Commission of Jurists, November 2021).
[53] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 69.
[54] Human Rights Council (2012, see note 5), para. 62.
[55] Committee on Economic, Social and Cultural Rights (2000, see note 16), para. 5; United Nations Department of Economic and Social Affairs, “Sustainable Development Goals No. 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages,” https://sdgs.un.org/goals/goal3.
[56] Committee on Economic, Social and Cultural Rights (2020, see note 4) para. 77.
[57] Ibid., para. 52.
[58] Ibid., para. 48.
[59] UNESCO (see note 9), para. 4.
[60] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 79. See also Human Rights Council (2012, see note 5), para. 68.
[61] Committee on Economic, Social and Cultural Rights (2000, see note 16) para. 16.
[62] Ibid., para. 40.
[63] Committee on Economic, Social and Cultural Rights (2020, see note 4), para. 79.
[64] Ibid., para. 80.
[65] Ibid., para. 82.
[66] Ibid., para. 80.
[67] Ibid., para. 82.
[68] United Nations, Compilation of Guidelines on the Form and Content of Reports to Be Submitted by States Parties to the International Human Rights Treaties, UN Doc. HRI/GEN/2/Rev.6 (2009), pp. 41–42.
[69] Office of the United Nations High Commissioner for Human Rights, “Follow-Up to Concluding Observations,” https://www.ohchr.org/en/treaty-bodies/follow-concluding-observations.
[70] B. M. Meier, M. De Milliano, A. Chakrabarti, and Y. Kim, “Accountability for the Human Right to Health through Treaty Monitoring: Human Rights Treaty Bodies and the Influence of Concluding Observations,” Global Public Health 13/11 (2018), pp. 1558–1576.
[71] J. M. Wyndham, M. W. Vitullo, K. Kraska, et al., Giving Meaning to the Right to Science: A Global and Multidisciplinary Approach (American Association for the Advancement of Science, 2017), pp. 24–25.
[72] R. Yotova and B. M. Knoppers, “The Right to Benefit from Science and Its Implications for Genomic Data Sharing,” European Journal of International Law 31/2 (2020), p. 679.
[73] Committee on Economic, Social and Cultural Rights, Concluding Observations: Mauritius, UN Doc. E/C.12/MUS/CO/5 (2019), paras. 61–62; Committee on Economic, Social and Cultural Rights, Concluding Observations: Estonia, UN Doc. E/C.12/EST/CO/3 (2019), paras. 50–53.
[74] Committee on Economic, Social and Cultural Rights, Concluding Observations: Kazakhstan, UN Doc. E/C.12/KAZ/CO/2 (2019), para. 51; Committee on Economic, Social and Cultural Rights, Concluding Observations: Slovakia, UN Doc. E/C.12/SVK/CO/3 (2019), para. 61.
[75] Committee on Economic, Social and Cultural Rights, Concluding Observations: Uzbekistan, UN Doc. E/C.12/UZB/CO/3 (2022), para. 44; Committee on Economic, Social and Cultural Rights, Concluding Observations: Latvia, UN Doc. E/C.12/LVA/CO/2 (2021), para. 40; Committee on Economic, Social and Cultural Rights, Concluding Observations: Finland, UN Doc. E/C.12/FIN/CO/7 (2021), para. 8.
[76] Ibid.
[77] Committee on Economic, Social and Cultural Rights (2022, see note 75), para. 44(b); Committee on Economic, Social and Cultural Rights (2021, Latvia, see note 75), para. 41(e); Committee on Economic, Social and Cultural Rights (2021, Finland see note 75), para. 9.
[78] Committee on Economic, Social and Cultural Rights, Concluding Observations: Azerbaijan, UN Doc. E/C.12/AZE/CO/4 (2021), para. 45(d); Concluding Observations: Kuwait, UN Doc. E/C.12/KWT/CO/3 (2021), para. 41; Committee on Economic, Social and Cultural Rights, Concluding Observations: Bosnia and Herzegovina, UN Doc. E/C.12/BIH/CO/3 (2021), para. 44(d); Committee on Economic, Social and Cultural Rights (2022, see note 75), para. 44(c); Committee on Economic, Social and Cultural Rights (2021, Finland see note 75), para. 9.
[79] J. Kohler, A. Wong, and L. Tailor, “Improving Access to COVID-19 Vaccines: An Analysis of TRIPS Waiver Discourse among WTO Members, Civil Society Organizations, and Pharmaceutical Industry Stakeholders,” Health and Human Rights Journal 24/2 (2022).
[80] Committee on Economic, Social and Cultural Rights (2021, Kuwait, see note 78), para. 40.
[81] Ibid., para. 41.
[82] Committee on Economic, Social and Cultural Rights (2022, see note 75), para. 44(c); Committee on Economic, Social and Cultural Rights (2021, Finland, see note 75), para. 9; Committee on Economic, Social and Cultural Rights (2021, Azerbaijan, see note 78), para. 45(d).
[83] Committee on Economic, Social and Cultural Rights (2021, Finland, see note 75), para. 9.
[84] Ibid., para. 10.
[85] Committee on Economic, Social and Cultural Rights, Concluding Observations: Czechia, UN Doc. E/C.12/CZE/CO/3 (2022), para. 50; Committee on Economic, Social and Cultural Rights, Concluding Observations: Serbia, UN Doc. E/C.12/SRB/CO/3 (2022), para. 20(a); Committee on Economic, Social and Cultural Rights, Concluding Observations: Nicaragua, UN Doc. E/C.12/NIC/CO/5 (2021), para. 42; Committee on Economic, Social and Cultural Rights (2021, Bosnia and Herzegovina, see note 78), paras. 20–21(c).
[86] Committee on Economic, Social and Cultural Rights (2021, Finland, see note 75), para. 54.