A Needle in a Haystack? Human Rights Framing at the World Trade Organization for Access to COVID-19 Vaccines
Volume 24/2, December 2022, pp. 141-157 | PDF
Katrina Perehudoff, Heba Qazilbash, and Kai Figueras de Vries
Abstract
How and why is implicit and explicit human rights language used by World Trade Organization (WTO) negotiators in debates about intellectual property, know-how, and technology needed to manufacture COVID-19 vaccines, and how do these findings compare with negotiators’ human rights framing in 2001? Sampling 26 WTO members and two groups of members, this study uses document analysis and six key informant interviews with WTO negotiators, a representative of the WTO Secretariat, and a nonstate actor. In WTO debates about COVID-19 medicines, negotiators scarcely used human rights frames (e.g., “human rights” or “right to health”). Supporters used both human rights frames and implicit language (e.g., “equity,” “affordability,” and “solidarity”) to garner support for the TRIPS waiver proposal, while opponents and WTO members with undetermined positions on the waiver used only implicit language to advocate for alternative proposals. WTO negotiators use human rights frames to appeal to previously agreed language about state obligations; for coherence between their domestic values and policy on one hand, and their global policy positions on the other; and to catalyze public support for the waiver proposal beyond the WTO. This mixed-methods design yields a rich contextual understanding of the modern role of human rights language in trade negotiations relevant for public health.
Introduction
In the last two years, the world has witnessed drastic inequitable access to COVID-19 vaccines and other medical countermeasures whereby some high-income countries secured priority access to vaccine supplies, often to the detriment of access in low- and middle-income countries. These unjust outcomes occurred against the backdrop of international human rights law, which includes states’ “minimum core obligation” to provide access to essential medicines on a nondiscriminatory basis, including through international assistance (article 12 of the International Covenant on Economic, Social, and Cultural Rights (ICESCR)).[1] The provision of essential medicines is part of states’ duty to fulfill their legal obligations and is also critical for the realization of other social rights (e.g., the right to social security (article 9 of the ICESCR) and the right to enjoy the benefits of science (article 15 of the ICESCR)). Therefore, the provision of essential medicines is interdependent on the full spectrum of civil, political, economic, and cultural rights (e.g., right to life (article 6 of the International Covenant on Civil and Political Rights)). With 171 and 173 state parties (respectively), the ICESCR and International Covenant on Civil and Political Rights enshrine human rights standards that most states have legally committed to realizing and agreed to be held accountable to.[2]
These stark inequities in access are sustained, in part, by vaccines being commodified on the global market within international trade law, namely the World Trade Organization’s (WTO) Agreement on Trade-Related Aspects of Intellectual Property (TRIPS Agreement), which establishes global standards for the protection of intellectual property (IP). Priority access to vaccines for wealthy and powerful countries is sustained by three key shortcomings of the COVID-19 pandemic response in relation to vaccines. First, the IP, knowledge, and know-how needed to increase vaccine production and supplies has not been voluntarily shared with other manufacturers by the private sector in a timely fashion.[3] Second, there is no “lever” in international law to mandate private companies to share the manufacturing know-how needed to produce vaccines. This shortcoming exists in global laws even though access to vaccines is part of the human rights to health and science (articles 12 and 15 of the ICESCR) and even though the TRIPS Agreement promotes the social and economic development aims of IP protection (article 7) and permits states to take measures to protect public health (article 8). The principle of systemic integration requires that these two bodies of international law be interpreted in harmony (article 31.3(c) of the Vienna Convention on the Law of Treaties). Third, manufacturing capacity is concentrated in a few world regions, and there is no (current) global consensus on how to distribute scarce vaccine supplies.
The WTO is one lawmaking fora where alternative approaches to the above shortcomings of the pandemic response were hotly debated. In October 2020, India and South Africa proposed to WTO members a measure of last resort, considering the general unwillingness of COVID-19 vaccine developers to voluntarily license or share their IP, knowledge, and know-how.[4] India and South Africa’s proposal, which garnered support from 65 cosponsors, sought a temporary waiver from certain provisions of the TRIPS Agreement (e.g., patents, trade secrets, and copyright and industrial designs) in relation to products for the prevention, containment, and treatment of COVID-19.[5] Achieving such a waiver to the TRIPS Agreement would be no small feat, as such a decision would require consensus among all WTO members. Counterproposals came from the United States and the European Union, increasing the pressure to convince fellow negotiators (i.e., representatives of WTO member governments) of the merits of one proposal and the drawbacks of the others.[6]
Frames are ideas, symbols, or narratives that apply a set of values to an issue.[7] For example, WTO negotiators may frame a trade issue as a matter of stimulating economic growth or promoting global development. Using a particular policy frame for a problem implies the set of solutions that are perceived as being coherent with the underlying values and goal.[8] The purpose of framing in the context of international negotiations is “to (re-)define and (de-)legitimise” different problems and proposals to address them.[9] Negotiators seek to establish a “dominant frame” through argumentation and persuasion, which Jutta Joachim suggests can convey an important source of power, alongside the economic and military power that some states wield.[10] For example, in the 2000s HIV/AIDS epidemic, a coalition of developing countries—veritable underdogs in terms of economic and trade power—succeeded in reframing the debate about IP and access to medicines at the WTO, in part, by engaging a human rights frame within and outside the WTO.[11] This success contributed to the adoption of the Doha Declaration on the TRIPS Agreement and Public Health by WTO members, reaffirming states’ right to use IP flexibilities to protect public health. Herein lies an important nuance: in the context of the WTO, members have a right to use IP flexibilities, whereas in the context of international human rights law, states have a duty to use IP flexibilities in order to provide essential medicines (when all other measures have failed) as part of the right to health.[12]
This paper considers a human rights frame to be the explicit or implicit use of language derived from human rights law. A human rights frame has much to offer WTO negotiators advocating for their proposal(s) to address IP and COVID-19 vaccine inequity. Referencing the importance of access to medicines in international human rights law re-prioritizes state action to address health needs over the protection of medicines as private property.[13] Human rights law also invokes a set of legal obligations on states, and measures for accountability. International human rights law offers both a normative and a legal framework for state action. It establishes legal standards for access to medicines that have been mirrored or adapted in domestic constitutional law and framework legislation for universal health coverage.[14] In some cases, references in domestic law to access to medicines as part of the right to health have enabled domestic courts to redress violations of this right.[15]
Despite the potential utility of a human rights frame for trade negotiators, explicit references to human rights were noticeably absent from South Africa and India’s initial waiver proposal in October 2020.[16] This observation raises questions about the modern role of human rights language in trade negotiations relevant for public health. Therefore, this study assesses how and why human rights framing is used by WTO negotiators in debates about IP, know-how, and technology needed for COVID-19 vaccines, and how these findings compare with human rights framing by WTO negotiators in the lead-up to the 2001 Doha Declaration.
The research questions are as follows:
- In communications at WTO about IP and COVID-19 vaccines:
- Which explicit and implicit human rights terms were used by WTO negotiators, and with what frequency?
- How did WTO negotiators use these terms in relation to state obligations?
- Why did WTO negotiators choose to use this language?
- What similarities and differences can be observed in how WTO negotiators’ use explicit human rights language in the context of WTO debates on IP and access to medicines in 2001 and 2020–2022?
Methodology
This mixed-methods case study of the human rights language used in WTO debates about IP and access to medicines is informed by framing theory and social constructivist approaches to international relations. Social constructivist theories argue that reality is a mediated process constructed through language and social interactions, rather than an objective truth.[17] In public health policy, issues become important when actors engage in strategic social construction, advancing claims regarding what deserves to be a policy issue and which range of solutions ought to be considered. [18] Thus, health policy actors use different frames to strategically influence (i.e., “introduce, undermine or change”) the perception of policy issues in order to advance their own interests.[19]
We selected the WTO waiver proposal as a case study to understand the modern role of human rights language in health-related trade negotiations because this issue is contentious, timely, and of global relevance. The WTO’s forefathers gave “diplomacy and economics” precedence over other concerns, suggesting that WTO negotiations are among the least likely fora where human rights framing would be used.[20] Moreover, in June 2022, the 12th Ministerial Conference reached a compromise decision on the COVID-19 vaccines aspects of the waiver proposal, meaning that these discussions are fresh in negotiators’ minds. As a point of comparison, we selected the 2001 WTO proceedings on IP and access to medicines leading up to the Doha Declaration.
Normative framework
The normative framework that guides this research and informs the concept of human rights language is drawn from the nature of state obligations, the rights to health and to science (articles 2, 12, and 15 of the ICESCR), and the ICESCR’s authoritative interpretation of state duties emanating from these rights (see Table 1).[21]
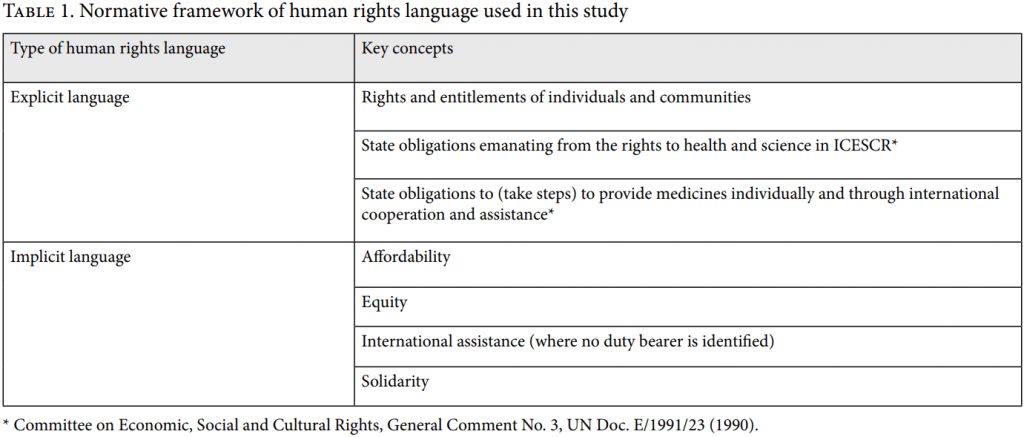
Explicit language
The human rights to health and science are interdependent on one another and other human rights such as the right to life. The rights to health and science bestow entitlements on each individual by virtue of their human dignity. Access to medicines is integral to exercise one’s freedom to control one’s own health and to enjoy one’s right to equal access to a system of health protection.[22]
The state duty to provide essential medicines, undertaking measures to prevent and treat disease, and ensuring nondiscriminatory access to health facilities, goods, and services are part of states’ “minimum core obligations,” as well as states’ duty to fulfill the rights to health and to social security. Additionally, the right to science requires states to direct public funding toward research and development in areas of public health need; to prevent unreasonably high medicines prices, such as by safeguarding the “social function” of IP; and to engage in international cooperation for the dissemination of new technologies.[23] States should use all the flexibilities in the TRIPS Agreement to increase vaccine production and ensure global access to a COVID-19 vaccine.[24] Consequently, under the ICESCR, states have a duty to use TRIPS flexibilities to make medicines available when other measures have failed. (This contrasts with the WTO’s trade regime, where members have a right to use TRIPS flexibilities to protect public health.) States should progressively realize these duties using a maximum of their available resources to move “expeditiously and effectively as possible” toward these goals.[25] To fully realize these rights, states have a duty to individually take steps and a duty to provide ”international assistance and cooperation,” including economic and technical cooperation.[26] States should also consider these legal obligations as members of international organizations and when entering into multilateral agreements.[27] Although states hold the primary responsibility to realize these obligations, they are shared with the international community and the private sector.[28] Explicit language (with regard to state obligations) is that which identifies explicit state duties to take steps to provide essential medicines or to engage in international assistance or cooperation.
Implicit language
Affordability is an element of the right to health that imposes the duty on states to ensure “economic accessibility” by making health goods, as well as scientific progress and its applications, affordable for all.[29] States are encouraged to disseminate access to research and its applications to allow developing countries and their citizens to access medical products.[30]
Equity is linked to the core obligation of states to ensure the “equitable distribution” of health services and goods, as well as to the concept of nondiscrimination and ensuring that health services and goods are affordable and available for all, including socially disadvantaged or marginalized groups.[31]
Implicit language (with regard to international assistance) is that which makes general calls for international assistance or cooperation without identifying who the duty bearer is.
International solidarity is a “foundational principle” of international law with legal roots in the universal notion that states have positive duties of cooperation for “harmonious international life.”[32] As outlined by the United Nations Independent Expert on human rights and international solidarity, international solidarity is a legally binding state duty in relation to infectious disease control and response to public health emergencies (article 44 of the International Health Regulations).[33] Although the term “solidarity” is not derived from international human rights law, the concept of international solidarity is closely linked with international assistance required to realize social rights.[34]
Selection of WTO members
Three considerations guided our purposive sample of WTO members. First, we included the members most likely to use human rights language in relation to this topic. These were countries that used explicit human rights references in their official WTO communications in 2001 or 2020–2022 about IP and access to medicines.
The second criterion was the representativeness of different positions on the waiver proposal, which was determined according to Jillian Kohler et al.’s classification of members’ positions.[35] Two members supporting, opposing, and with an undetermined position on the waiver proposal were included regardless of their human rights framing, in addition to the “most likely” members. WTO members were classified as “supporters” if they sponsored or expressed support for the proposal, whereas they were considered “opponents” if they stated their objections to the proposal. WTO members with an undetermined position did not make any clear statement expressing either support or objection to the proposal.
The third criterion was representativeness of all income economies. This consideration led to the inclusion of two additional BRICS members with emerging markets and corresponding economic power to balance out the other income economies included using the first two criteria.
Sources and analysis
Official statements from WTO members were collected from WTO’s website according to our eligibility criteria. Documents were searched using NVivo to identify explicit or implicit human rights language derived from the normative framework as shown in Table 1. Text was excluded that was unrelated to access to medicines, such as pandemic lockdowns. Two authors first confirmed whether the hits were relevant to access to medicines, then quantified and described the results to research questions 1a–b and 2.
Semi-structured interviews were conducted in English with key informants in June and July 2022 via Zoom. Ethical approval was granted by the University of Amsterdam’s Faculty of Law. Eligible key informants were WTO negotiators, representatives of the WTO Secretariat, and nonstate actors observing WTO debates. Informants were purposively sampled through the networks of the authors. The interview guide was tailored to each informant; it aimed to clarify, confirm, or contest the results of the content analysis and previous interviews, as well as to deepen their meaning. All interviews were audio recorded (with permission), transcribed, and pseudo-anonymized by two authors. All authors analyzed the transcripts iteratively through close reading and used inductive coding to identify and describe themes that answered research question 1c.
Results
This analysis is based on a sample of 26 WTO members and two groups of members using 35 unique WTO documents regarding IP and access to medicines and key informant interviews with a nonstate actor, a representative of the WTO Secretariat, and four WTO negotiators: one opposing the waiver proposal, one with an undetermined position on the waiver proposal, and two supporting the waiver proposal.
Explicit language
Few explicit human rights references appeared in members’ official communications in relation to IP and COVID-19 vaccines. When explicit human rights language was used by negotiators, it was concentrated around January–March 2021 and peaked in September 2021 (see Figure 1).
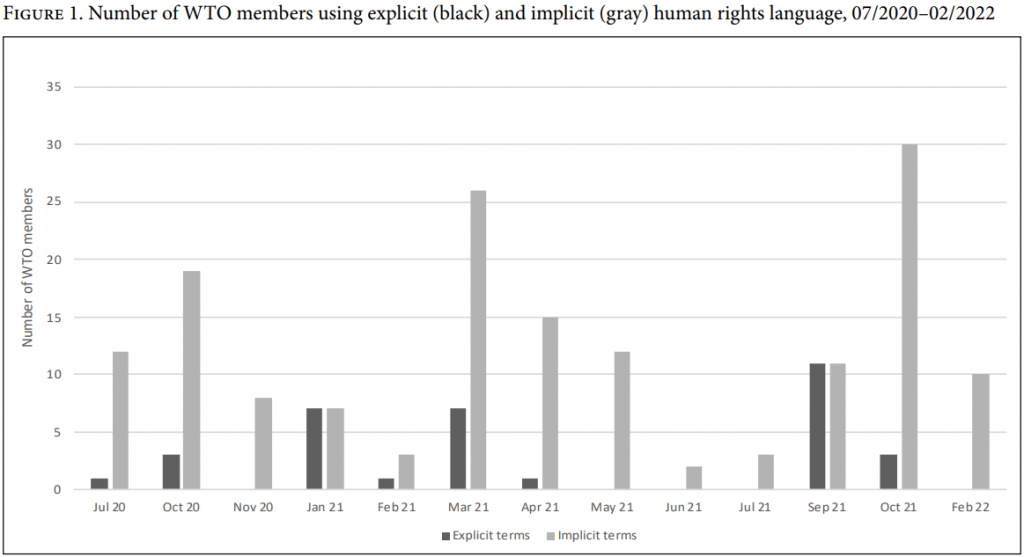
Although explicit references were missing from the initial waiver proposal (October 2020), the sponsors introduced an explicit human rights argument to their clarification about the waiver proposal in September 2021, stating:
[The] adoption of a TRIPS waiver acts as an important political, moral and economic lever towards encouraging solutions aimed at global equitable access to COVID-19 health products and technologies including vaccines, therapeutics and diagnostics, which is in the wider interest of the global public. This outcome is also consistent with the Covenant on Economic, Social and Cultural Rights, especially Article 12 which recognizes the “human right of everyone to the enjoyment of the highest attainable standard of physical and mental health” and obligating the taking of steps to fully realize this right, including “those necessary for … the prevention, treatment and control of epidemics, endemics, … and other diseases.”[36]
In this communication, a human rights justification for the waiver proposal is one of several arguments the supporters present, suggesting that it does not hold particular primacy over other “ethical, epidemiological, and economic” considerations mentioned in the same context.[37] Nor do explicit state obligations flow from this appeal to a human rights frame.
Of those members using explicit human rights language, the most frequently used terms were “human rights” and the “right to health.” Only Indonesia and Bolivia referenced the “right to life” alongside the “right to health.”[38] No member referenced the “right to science,” although Costa Rica’s statement about the World Health Organization’s COVID-19 Technology Access Pool at a TRIPS Council meeting (February 2021) mirrored the Committee on Economic, Social and Cultural Rights’ guidance for states on the right to science.[39]
Explicit references were usually employed by supporters, often appealing to the human rights obligations that most WTO members have (by virtue of being state parties to the ICESCR). Supporters linked those obligations with the imperative to support the waiver proposal. For example, Bolivia underscored at a TRIPS Council meeting (July 2021) that the overall objective of a waiver is the preservation of human lives, which necessitates
adopting timely and appropriate measures so that the privileges and the rights which are recorded [sic] to pharmaceutical industries do not override the rights we have to life, to health, the right to develop our economies.[40]
Bolivian negotiators asserted the primacy of human rights as a justification for establishing a “humanitarian waiver,” and then they appealed to WTO members’ “responsibility” to adopt a decision that “may change the reality experienced by millions of people on the ground throughout the world.”[41] This is the only case we identified where a negotiator explicitly referenced the phrase “human rights” in association with the concept that states have positive responsibilities to act.
WTO members advocating for alternative, voluntary approaches (to the waiver proposal) to scale-up COVID-19 vaccine access did not use explicit human rights language to rally support for their positions.
Motivations for using explicit human rights language
Key informants explained that several factors motivated explicit references to human rights.
First, citing international human rights law and specific human rights is part of a strategy to leverage all possible arguments and “agreed language” in order to convince members of the waiver proposal’s importance. One supporter reported to us that “when you are negotiating, you use all the arguments you can use, the same reasoning on the other side, but usually it is a lot more credible if you use something that has already been agreed on.”
Second, human rights framing resonates with the world and is therefore useful to incorporate into the WTO waiver proposal debate as a public relations endeavor. Most informants we interviewed confirmed the importance of building a public narrative around a given issue at WTO in order to generate support from a wider audience beyond WTO. Human rights language assists in these public communications because, as one supporter explained to us, they need to build a narrative to “present the situation in the best light,” and human rights are suited to this task because they are “something viewed positively by [our] citizens and the general public.” This strategic narrative shaping was described by an opponent as “manipulating the larger audience[’s] ignorance about how the [IP] system effectively works.” Using human rights language at the WTO had a ripple effect beyond the WTO, reaching “the very capitals of some of the members that until the very end opposed the waiver,” according to a supporter of the waiver proposal.
Third, an “intermestic” approach, in which domestic policy is linked to international policy, motivates some negotiators to draw inspiration for their WTO discourse from those human rights principles and language in their domestic legal orders. Idea construction is an important element of an intermestic approach.[42] Dyah Kurniawati explains that, in line with a constructivist perspective, in an intermestic approach “international norms will be more easily internalized and legitimized in domestic policy if they touch on the values, identity, or beliefs of domestic actors.”[43] As one supporter explained to us:
If we talk in the international forum, it has to represent our interest and our values domestically. At the same time, when we are negotiating in the international forum then we also bring it back domestically.
Motivations for omitting explicit human rights language
Key informants offered several explanations for why WTO negotiators may not explicitly reference human rights.
First, the WTO’s trade mandate is a “semi-independent” legal regime, which was acknowledged by all key informants. Curiously, the respondents did not explicitly acknowledge the principle of systemic integration in international law, which requires in the case of pharmaceuticals that the TRIPS Agreement and United Nations human rights treaties be interpreted in harmony. Moreover, according to several respondents, the unique mandates of different international organizations in Geneva give rise to the fragmented internal organization of some Geneva missions. Three negotiators explained to us that the internal structure of their missions mirrors the distinct mandates of the international organizations they engage in, with one arm dealing with trade or economy (e.g., a mission to WTO), while another handles human rights (e.g., a mission to the United Nations). Negotiators we interviewed justified omitting human rights framing from their WTO discourse because of this internal fragmentation, with one negotiator explaining it means they would be “less tempted” to consider or use human rights narratives in their dealings at WTO regarding sensitive topics, such as the waiver proposal.
Second, some WTO members have “sensitivities” to human rights arguments, as they are concerned about a political discussion of IP and health emerging in an “unprotected environment,” such as the Human Rights Council. An “unprotected environment” is a policymaking forum where the protection of IP is a primary aim, often over other societal concerns that, if prioritized, could threaten the economic interests of states with large pharmaceutical industries.
Third, one negotiator implied that explicit human rights language at the WTO is not necessary because human rights principles are implicit to the organization’s work in general, and specifically on access to medicines. “The idea of a right to health and WTO being [responsive] to a health emergency was always there, but … I do not recall any kind of references to human rights law,” this negotiator outlined. Additionally, a WTO representative and negotiator confirmed to us that, in their views, human rights language is intrinsic to members’ right to use TRIPS flexibilities.
Implicit language
Implicit human rights language was used by WTO negotiators in more documents than explicit references. Implicit references were used in WTO communications throughout the debates on IP and COVID-19 vaccines (see Figure 1).
Terms related to “affordability” and “equity” were frequently used together, sometimes with comparable frequency by supporters and opponents.[44] For example, terms related to “equity” were used in a comparable number of WTO documents by South Africa (in 12 out of the 16 documents in which South Africa is quoted) as the European Union (in 11 out of 17 documents). “International cooperation” and similar terms were the least frequent among all implicit human rights language. The term “solidarity” was used at least once by most members in our sample, and in some cases, opponents and supporters used the term in a comparable number of documents (e.g., in 3 out of 17 documents in which the European Union is quoted versus 5 out of 16 documents in which India in quoted).
WTO negotiators use these implicit terms in statements appealing to WTO members’ duties and responsibilities. Negotiators cited the “collective responsibility” to make global trade an instrument for pandemic containment and recovery, and a “duty and responsibility” to prioritize a response that can help save lives.[45] Other negotiators referenced the “responsibility” of WTO members to facilitate knowledge sharing and research for containment and treatment of COVID-19 and to promote equitable and affordable access to products against COVID-19, and a “shared responsibility” of WTO members to collaborate to ensure that IP doesn’t pose a barrier to research, development, manufacture, and supply of medical products for COVID-19.[46] Some WTO negotiators mirrored the Committee on Economic, Social and Cultural Rights’ language by referring to governments’ “core obligations of protecting public health and ensuring access to medicines for all.”[47]
There is no consensus among key informants in our sample about whether these implicit terms can be equated with human rights language. A WTO representative noted that the question as to whether words, such as solidarity, constitute human rights language has not been discussed in recent negotiations. Yet the respondent nevertheless considers phrases such as “vaccine equity” and “solidarity” as related to human rights.
Taking a different perspective, one supporter we spoke to concluded that “of course” terms such as equity, solidarity, and international assistance are human rights language, explaining that these terms arise from the field of human rights and are relevant beyond that domain. According to this supporter, human rights language overlaps with the supporter’s practical policy objectives of expanding and diversifying vaccine production in order to end the pandemic and save lives, which illustrates “the real impact and relevance” of human rights framing.
In our interviews, a WTO representative and a negotiator both indicated that the “right to protect public health” and references to the TRIPS flexibilities signify human rights language. These principles are found in the TRIPS Agreement (articles 7–8) and are reaffirmed in the Doha Declaration (“WTO members’ right to protect public health and, in particular, to promote access to medicines for all”). Members that mentioned the “right to protect public health” in their WTO communications generally did not use explicit human rights language, except for South Africa. Although the “right to protect public health” is not necessarily a human right, our respondents considered that the former phrase is implicitly linked to human rights language. WTO negotiators may feel more comfortable referencing states’ “right to protect public health” (compared to human rights language) because this phrase echoes the principles of the TRIPS Agreement (article 8).[48]
Motivations for using implicit human rights language
Negotiators used implicit human rights language to advance their member’s particular interests regarding access to medicines and IP.
Supporters employed these terms to call for “constructive engagement” with the proposal and to generate support among negotiators for it.[49] They also used this language to contest the effectiveness of voluntary options (“voluntary, secretive, limited and restrictive licensing has failed to leverage global expertise and capacity to scale-up manufacturing and deliver equitable access”).[50]
Opponents used these implicit phrases to promote the existing TRIPS flexibilities and to advocate for voluntary mechanisms, such as the ACT-Accelerator or collaboration with industry to incentivize and increase production capacity.[51] In a TRIPS Council meeting (February 2021), South Africa stated that
high-minded language on solidarity and global public goods, however, has not been matched by tangible steps to share know-how and intellectual property rights to facilitate deep technology transfer in the COVID-19 response.[52]
Furthermore, one supporter explained to us that opponents to the proposal may use this implicit language as part of a strategy to ease domestic pressure on negotiators. According to this supporter, some negotiators have taken positions on the waiver proposal that, in effect, represented the interests of “big business” and were contrary to the majority opinion of their own constituents. The supporter explained that in these situations, implicit human rights terms were instrumentalized by negotiators to appease the constituents whose interests were not being accurately represented at the WTO. This instrumentalization was echoed by a nonstate actor we spoke to, who noted that “maybe initially it [the word solidarity] was very welcome but then, after a while, it lost its meaning to me, as … a tick[ing]-the-box sort of thing.”
Comparison with 2001
Comparable numbers of WTO members in our sample used explicit human rights language at least once in WTO discussions about IP and HIV/AIDS (14 members or groups) or COVID-19 medicines (12 members or groups) (see Table 2). Four members in our sample (Egypt, South Africa, Tanzania, and Zimbabwe) adopted an explicit human rights frame for the first time in their WTO communications about IP and COVID-19 vaccines, whereas in the same communications about COVID-19, four members (Brazil, Chile, Dominican Republic, and Ecuador) abandoned the explicit human rights language they once used in 2001.
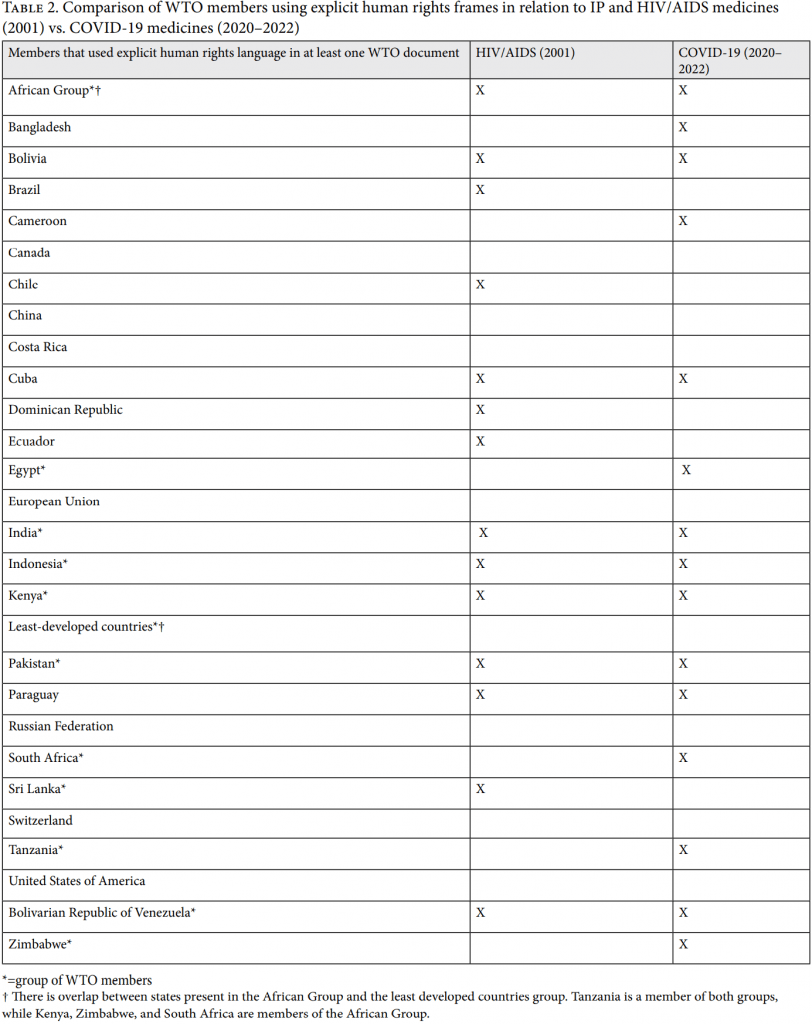
A WTO representative observed that human rights language was used differently in the WTO discussions in 2001 compared to 2020–2022. First, the 2001 discussion focused on the interpretation of the basic principles and objectives of the TRIPS Agreement (articles 7 and 8) in light of human rights. Although these principles and objectives were mentioned in 2020–2022, they were not addressed in direct relation to human rights. Second, a central debate in 2001 was whether public health should have primacy over IP, and human rights language helped shape some negotiators’ arguments; however, this debate in general was less present in 2020–2022.
Members using explicit references in 2001 frequently associated human rights with state obligations regarding health protection, the interpretation of the TRIPS Agreement, or both. For example, at a TRIPS Council meeting (November 2001), Indonesia advanced the understanding that the human rights to life and to health implicate state responsibilities for the prevention and treatment of diseases. Indonesian negotiators further advocated that protecting those human rights “was not just the responsibility of national governments but, to a certain extent, should be the universal responsibility of all people of the world,” suggesting the importance of international collaboration.[53]
Discussion
This research assesses how and why human rights framing is used by WTO negotiators in debates about IP and COVID-19 vaccines, and how these findings compare to negotiators’ WTO discourse in the 2001 HIV/AIDS epidemic. We found that WTO negotiators used little explicit human rights language in relation to IP and COVID-19 vaccines. Supporters used both explicit and implicit human rights references to garner support for the waiver proposal, while opponents and members with undetermined positions on the waiver used only implicit language to advocate for alternative proposals. A comparable number of WTO members used explicit human rights framing in 2001 and 2020–2022.
Reflecting on human rights framing at WTO
This study revealed that WTO negotiators use explicit human rights frames to appeal to previously agreed language about state obligations; to ensure consistency between their domestic values, principles, and policy, and their policy positions on a global stage (“intermestic approach”); and to galvanize public support for the waiver proposal beyond the WTO.
These findings support the idea of a feedback loop between WTO negotiators on the one hand, and civil society and public opinion outside the WTO on the other.[54] In this loop, WTO negotiators by their own admission may use a human rights frame to catalyze external support for a given proposal. Yet, equally important, external actors can also inform WTO negotiators about the human rights implications of their work, which may be reflected in their subsequent discourse. The latter is one reason why many waiver sponsors applied a human rights frame for the first time in their September 2021 discourse about the waiver proposal.[55] Consequently, the role of civil society organizations in the narratives of WTO negotiators should not be underestimated. Kohler et al. found that these organizations were the only stakeholder to consistently frame COVID-19 vaccine inequality as a human rights issue.[56]
Position and determinants of human rights language at the WTO
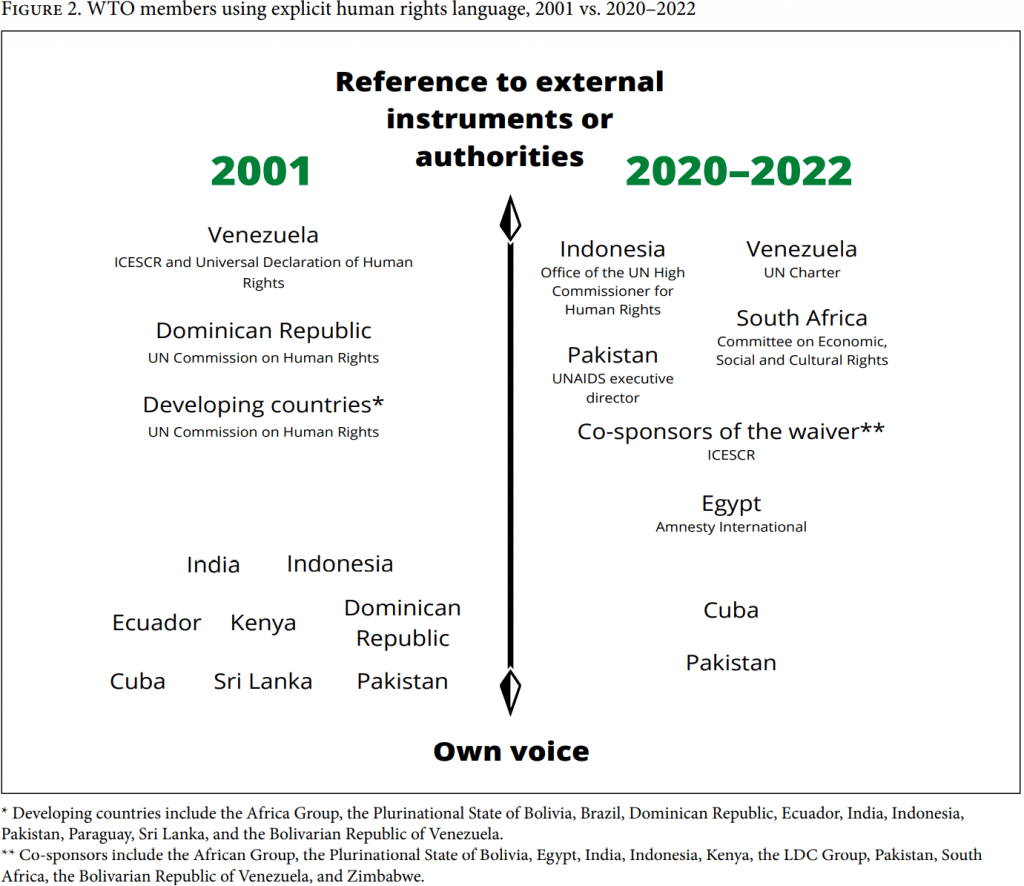
The negotiators who used explicit human rights framing tended to cite human rights instruments and authorities external to the WTO in 2020–2022, whereas in 2001 they made explicit human rights claims in their own voice (meaning, by expressing the state’s position without reference to external experts, authorities, or other legal instruments in their oral or written remarks) (see Figure 2). The precise intention behind these strategies should be further explored to elucidate how human rights frames are used in trade diplomacy.
The idea of bringing coherence to a state’s domestic and international policy spheres suggests that WTO members with a constitutional right to health would be more likely than those without such a right to use an explicit human rights frame in WTO negotiations about IP and public health. However, several states in our sample with strong constitutional protections for health and medicines disprove this hypothesis (e.g., Brazil, Dominican Republic, and Ecuador).[57]
This research shows that five states—three with an undetermined position on the waiver (Brazil, Chile, and Ecuador) and two that support the waiver (Dominican Republic and Sri Lanka)—ceased using explicit human rights language between 2001 and 2020. We interpret this finding to be more of a reflection of the states’ domestic political and economic circumstances than a suggestion that human rights language has diminished in importance. One reason for this shift could be changes in the domestic political economy of pharmaceuticals, where, for example, states needed access to the IP, know-how, or data to locally produce medicines to address the HIV/AIDS epidemic that was not needed by those states to address the COVID-19 pandemic. For example, in 2001, Brazil was a high-profile negotiating state in the WTO special session and the Doha rounds, where it used explicit human rights language coinciding with its pursuit of clarifications of the TRIPS Agreement in order to leverage its domestic manufacturing capacity to produce generic versions of HIV/AIDS medicines. In 2020, Brazilian leveraged its robust domestic capacity to produce vaccines by negotiating technology transfer agreements with Astra Zeneca (at the federal level) and China’s Sinovac (at the state level) for the local manufacture of those COVID-19 vaccines.[58] Consequently, a TRIPS waiver was of little added value to Brazil’s domestic response; therefore, Brazil was not a proponent of the waiver proposal, which limited the need to use all persuasive devices (e.g., human rights language) in Brazil’s toolbox. More generally, another reason for WTO negotiators to cease using human rights language in the 2020–2022 pandemic is the domestic and regional political shifts from the socially oriented post-dictatorial governments of the 1990s–2000s to the current right-leaning governments (e.g., Brazil, Chile, and Ecuador).
Domestic political and economic considerations could also be the reason that five WTO members (Bangladesh, Cameroon, Egypt, South Africa, and Tanzania) started using explicit human rights language in their own statements (i.e. not as part of a group, such as the African Group) for the first time in WTO pharmaceutical IP debates in 2020–2022. For example, South Africa refrained from assuming a high-profile role in the 2001 WTO debates, particularly the special session. The state also avoided using explicit human rights language in its own 2001 statements at WTO (beyond its membership of the African Group). These decisions could have been influenced by residual political and economic effects of the 1990s anti-apartheid sanctions and embargoes against South Africa.
Many of the states that used explicit human rights language in 2001 and 2020–2022 (e.g., Bolivia, Cuba, Kenya, Indonesia, and Paraguay) enshrine health as a human right in their domestic constitutions, which is consistent with other research on the determinants of human rights frames in domestic pharmaceutical IP debates.[59] Yet our findings suggest that domestic policy and economic realities may have more influence on state narratives about pharmaceuticals at the WTO than the values and human rights norms enshrined in states’ respective domestic constitutions. For example, both South Africa and Brazil enshrine an enforceable right to health; yet both of these states have avoided explicit human rights language when discussing pharmaceutical access at the WTO at some point in the last two decades. Taken together, these findings suggest that a constitutional right to health is supportive but not decisive for states to use human rights language in pharmaceutical IP debates at the WTO.
Our research investigates the use of human rights language in pharmaceutical IP debates at the WTO amid a policy climate that is “increasingly hostile—or at least indifferent—to human rights” in matters of global health.[60] It may be that explicit human rights language is seen as a weak or “emotional” argument (the latter was suggested by one of our respondents), rather than a persuasive argument. Nevertheless, even though this research shows that human rights language is used by fewer WTO members in relation to pharmaceutical IP in 2020–2022 than in 2001, those WTO members that do invoke human rights in 2020–2022 tend to make explicit reference to human rights legal instruments (see Figure 2). This suggests that those states are conscious of their own legal obligations stemming from these treaties and that those legal obligations are born by all state parties, which was corroborated by one of our respondents.
Contesting reasons why WTO negotiators avoid human rights language
Our key informants, and the broader literature on this subject, contest some of the justifications we report for WTO negotiators to avoid using a human rights frame.
First, the claim that the WTO is semi-independent, or “self-contained,” of other international fora is discounted by Holger Hestermeyer, who points to the application of “other norms of international law” in the WTO regime, the references in the TRIPS Agreement to other international conventions, and the WTO’s Dispute Settlement Understanding (article 3.2) that allows WTO panels and the Appellate Body to reference international law outside WTO agreements.[61]
Our study revealed a porous barrier between the WTO and other international legal regimes that allows for selective cross-fertilization of norms and language, depending on the member’s own interests. This porous barrier is necessary for systemic integration and the reduction of fragmentation in international law; however, our research shows that WTO negotiators appear to be taking haphazard and inconsistent steps toward harmonious interpretation in the field of pharmaceuticals and public health. Most respondents acknowledge that WTO negotiators sometimes reference other norms or interpretive tools from external political or legal regimes (e.g., United Nations, G20, and the African Union). Key informants viewed this strategy with some skepticism, particularly when language was drawn from external regimes with a narrow membership (e.g., G20). According to one negotiator who was interviewed, it would be more appropriate to introduce language from the ICESCR (with 171 state parties, most of which are WTO members). This corroborates Hestermeyer’s contested proposal based on the Vienna Convention to interpret that “the international law rule binds at least a large number of the WTO Members.”[62] No clear distinction is made between which references to external legal orders are permissible in WTO negotiations, and which are not.
Second, the claim that WTO negotiators avoid human rights framing due to the fragmented institutional mandates of their missions in Geneva was contested by some key informants. One supporter, whose mission operates in a similar fashion, rejected this idea, explaining that a fractured institutional mandate does not justify WTO negotiators suddenly disregarding the majority opinion of their constituents and instead advancing the interests of their domestic pharmaceutical industry at the WTO—a phenomenon that has been reported by other scholars.[63]
Strengths and limitations, and policy implications
One strength of this study is the explicit normative framework derived from international human rights law, and its application by at least two authors of this paper. Another strength is the mixed-methods design, which responds to previous critiques of human rights discourse analysis by yielding a deeper, contextual understanding of the reasons for and intentions behind the use of some human rights terms.[64] In addition, the key informants represented each position on the waiver proposal, and their responses generally corroborated one another, as the results show. The limitations of this research include restricted public access to some WTO documents, fewer WTO documents available for 2001 (compared to 2020–2022), and disparate periods of comparison (one year/2001 versus two years/2020–2022). These limitations may have impacted the results of the content analysis; however, key informants corroborated the findings of our content analysis.
This study has identified arguments and counterarguments for using a human rights frame in WTO discussions on IP and access to medicines. These arguments may be relevant for WTO negotiators and observers seeking to influence the outcome of the forthcoming negotiations on COVID-19 therapeutics and diagnostics, as well as on broader issues of trade and public health.
Supplemental information
Additional details regarding the methodology and key findings are available through doi: 10.21942/uva.21666845.
Acknowledgments
We thank the key informants who participated in this research, Ellen ‘t Hoen and Pramiti Parwani for their comments on an earlier version of this manuscript, and the participants of the Connaught Global Challenge paper development workshop on May 17, 2022, for their helpful feedback. This work was supported in part by a Connaught Global Challenges grant, “Advancing Rights-Based Access to COVID-19 Vaccines as Part of Universal Health Coverage,” to Lisa Forman and by a grant from Unitaid to Medicines Law & Policy.
Katrina Perehudoff, MSc, LLM, PhD, is an assistant professor at the Law Centre for Health and Life at the Faculty of Law, University of Amsterdam, Netherlands. She is affiliated with the Amsterdam Institute of Global Health & Development, Netherlands; the Amsterdam Centre for European Law and Governance; the Amsterdam Centre for European Studies; the World Health Organization Collaborating Centre for Governance, Accountability, and Transparency in the Pharmaceutical Sector at the University of Toronto, Canada; and Medicines Law & Policy, Amsterdam, Netherlands.
Heba Qazilbash, BSc (Hons), is an MPH candidate at the Dalla Lana School of Public Health at the University of Toronto, Canada.
Kai Figueras de Vries, BA, is an LLM candidate at the University of Amsterdam’s Faculty of Law and the chair of the Amsterdam chapter of Universities Allied for Essential Medicines, Netherlands.
Please address correspondence to Katrina Perehudoff. Email: katrina.perehudoff@gmail.com
Competing interests: None declared.
Copyright © 2022 Perehudoff, Qazilbash, and de Vries. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original authors and source are credited.
References
[1] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966); Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000).
[2] United Nations, “Status of Treaties,” https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-3&chapter=4&clang=_en; K. Perehudoff and L. Forman, “What Constitutes ‘Reasonable’ State Action on Core Obligations? Considering a Right to Health Framework to Provide Essential Medicines,” Journal of Human Rights Practice 11/1 (2019).
[3] K. Perehudoff, E. ‘t Hoen, K. Mara, et al., “A Pandemic Treaty for Equitable Global Access to Medical Countermeasures: Seven Recommendations for Sharing Intellectual Property, Know-How and Technology,” BMJ Global Health 7 (2022).
[4] TRIPS Waiver Proposal at the WTO, “Waiver from Certain Provisions of the TRIPS Agreement for the Prevention, Containment, and Treatment of COVID-19,” IP/C/W/669 (October 2020).
[5] Revised TRIPS Waiver Proposal at the WTO, “Waiver from Certain Provisions of the TRIPS Agreement for the Prevention, Containment, and Treatment of COVID-19 Revised Decision Text,” IP/C/W/669.Rev1 (May 2021).
[6] Counterproposal from the United States, “Supporting the Timely and Efficient Release of Global Goods through Accelerated Implementation of the WTO Trade Facilitation Agreement,” G/TFA/W/25/Rev.6 (May 2021); counterproposal from the European Union, “Urgent Trade Policy Responses to the COVID-19 Crisis,” WT/GC/231 (June 2021).
[7] C. McInnes and K. Lee, “Framing and Global Health Governance: Key Findings,” Global Public Health 7/Suppl 2 (2012).
[8] Ibid.
[9] J. Joachim, “Framing Issues and Seizing Opportunities: The UN, NGOs, and Women’s Rights,” International Studies Quarterly 47/2 (2003), p. 269; J. S. Odell and S. K. Sell, “Reframing the Issue: The WTO Coalition on Intellectual Property and Public Health, 2001,” Negotiating Trade: Developing Countries in the WTO and NAFTA 85 (2006).
[10] Joachim (see note 9).
[11] Odell and Sell (see note 9), p. 88; E. George, “The Human Right to Health and HIV/AIDS: South Africa and South-South Cooperation to Reframe Global Intellectual Property Principles and Promote Access to Essential Medicines,” Indiana Journal of Global Legal Studies 18/1 (2011); D. Matthews, Intellectual Property, Human Rights and Development: The Role of NGOs and Social Movements (Cheltenham: Edward Elgar Publishing, 2011).
[12] K. Perehudoff and L. Forman, “What Constitutes ‘Reasonable’ State Action on Core Obligations? Considering a Right to Health Framework to Provide Essential Medicines,” Journal of Human Rights Practice 11/1 (2019); E. ‘t Hoen, Practical Applications of the Flexibilities of the Agreement on Trade-Related Aspects of Intellectual Property Rights: Lessons beyond HIV for Access to New Essential Medicines, https://medicineslawandpolicy.org/wp-content/uploads/2018/03/EllentHoen_dissertatie_Practical_Implications_2018.pdf.
[13] L. Forman, “‘Rights’ and Wrongs: What Utility for the Right to Health in Reforming Trade Rules on Medicines?,” Health and Human Rights Journal 10 (2008), p. 39.
[14] S. K. Perehudoff, B. Toebes, and H. Hogerzeil, “Essential Medicines in National Constitutions: Progress since 2008,” Health and Human Rights Journal 18/1 (2016), p. 141; S. K. Perehudoff, N. V. Alexandrov, and H. V. Hogerzeil, “Legislating for Universal Access to Medicines: A Rights-Based Cross-National Comparison of UHC Laws in 16 Countries,” Health Policy and Planning 34/Suppl 3 (2019).
[15] O. F. Norheim and B. M. Wilson, “Health Rights Litigation and Access to Medicines: Priority Classification of Successful Cases from Costa Rica’s Constitutional Chamber of the Supreme Court,” Health and Human Rights Journal 16 (2014), p. 47.
[16] Ibid.; TRIPS Waiver Proposal (see note 4).
[17] J. Shiffman, “A Social Explanation for the Rise and Fall of Global Health Issues,” Bulletin of the World Health Organization 87/8 (2009).
[18] Ibid.
[19] McInnes and Lee (see note 7), pp. S195–S196; S. Rushton and O. D. Williams, “Frames, Paradigms and Power: Global Health Policy-Making under Neoliberalism,” Global Society 26/2 (2012).
[20] H. Hestermeyer, “Access to Medicine as a Human Right in the WTO Order,” in H. Holger Hestermeyer (ed), Human Rights and the WTO: The Case of Patents and Access to Medicines (Oxford: Oxford University Press, 2007), pp. 210–211.
[21] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966); Committee on Economic, Social and Cultural Rights (2000, see note 1); Committee on Economic, Social and Cultural Rights, General Comment No. 17, UN Doc. E/C.12/GC/17 (2006); Committee on Economic, Social and Cultural Rights, General Comment No. 25, UN Doc. E/C.12/GC/25 (2020).
[22] Committee on Economic, Social and Cultural Rights (2000, see note 1), para. 1.
[23] Committee on Economic, Social and Cultural Rights (2020, see note 21); K. Perehudoff and J. Sellin, “The Right to Science as a Guidepost for Fair Access to COVID-19 Vaccines: Investigating the Interpretive Role of the United Nations Committee on Economic, Social and Cultural Rights,” Health and Human Rights Journal 24/2 (2022).
[24] Committee on Economic, Social and Cultural Rights, Statement on Universal Affordable Vaccination against Coronavirus Disease (COVID-19), International Cooperation, and Intellectual Property, UN Doc. E/C.12/2021/1 (2021); Committee on Economic, Social and Cultural Rights (2020, see note 21), para. 69.
[25] Committee on Economic, Social and Cultural Rights (2000, see note 1), para. 31.
[26] Ibid., para. 38; Committee on Economic, Social and Cultural Rights (2006, see note 21), para. 40; Committee on Economic, Social and Cultural Rights (2020, see note 21), para. 51; International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 2.
[27] Committee on Economic, Social and Cultural Rights (2000, see note 1), paras. 39, 50.
[28] Ibid., paras. 42, 45.
[29] Ibid., para. 12(b).
[30] Ibid., para. 79.
[31] Ibid., para. 43(e).
[32] United Nations, Charter of the United Nations, 1 UNTS XVI (1945), arts. 55–56; Office of the United Nations High Commissioner for Human Rights, “Independent Expert on Human Rights and International Solidarity,” www.ohchr.org/en/special-procedures/ie-international-solidarity.
[33] Human Rights Council, Report of the Independent Expert on Human Rights and International Solidarity, Obiora Chinedu Okafor, on International Solidarity in Aid of the Realization of Human Rights during and after the Coronavirus Disease (COVID-19) Pandemic, UN Doc. A/HRC/47/31 (2021), paras. 26–27.
[34] Ibid.
[35] J. Kohler, A. Wong, and L. Tailor, “Improving Access to COVID-19 Vaccines: An Analysis of TRIPS Waiver Discourse among WTO Members, Civil Society Organizations, and Pharmaceutical Industry Stakeholders,” Health and Human Rights Journal 24/2 (2022).
[36] WTO Communication, IP/C/W/684 (September 2021), para. 6.
[37] Ibid., paras. 5, 7.
[38] WTO General Council Meeting, WT/GC/M/190 (March 2021); TRIPS Council Meeting, IP/C/M/99/Add.1 (July 2021).
[39] Committee on Economic, Social and Cultural Rights (2020, see note 21), para. 16; TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), paras. 998, 1002.
[40] TRIPS Council Meeting (2021, see note 38), para. 27.
[41] Ibid., para. 28.
[42] D. E. Kurniawati, “Intermestic Approach: A Methodological Alternative in Studying Policy Change,” PCD Journal 5, no. 1 (2017).
[43] Ibid., p. 168.
[44] TRIPS Council Meeting, IP/C/M/95/Add.1 (October 2020), para. 533.
[45] Switzerland at TRIPS Council Meeting, IP/C/M/98/Add.1 (July 2020), para. 368; India at TRIPS Council Meeting, IP/C/M/99/Add.1 (July 2021), para. 874; India at TRIPS Council Meeting, IP/C/M/103/Add.1 (February 2022), para. 301.
[46] India at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 874; India at TRIPS Council Meeting IP/C/M/103/Add.1 (February 2022), para. 301; Chad on behalf of the LDC Group at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 1217; Tanzania at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 1460; Nigeria at TRIPS Council Meeting, IP/C/M/97/Add.1 (April 2021), para. 127.
[47] Nigeria at TRIPS Council Meeting, IP/C/M/96/Add.1 (April 2021), para. 127.
[48] E. ‘t Hoen, “Protecting Public Health through Technology Transfer: The Unfulfilled Promise of the TRIPS Agreement,” Health and Human Rights Journal 24/2 (2022).
[49] Bangladesh at TRIPS Council Meeting, IP/C/M/103/Add.1 (February 2022), para. 87; South Africa at TRIPS Council Meeting, IP/C/M/103/Add.1 (February 2022), para. 405; Communication to the TRIPS Council, IP/C/W/672 (January 2021), para. 151.
[50] South Africa at TRIPS Council Meeting, IP/C/M/97/Add.1 (April 2021), para. 15.
[51] Canada at TRIPS Council Meeting, IP/C/M/99/Add.1 (July 2021), para. 1113; EU at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 1036; United States at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 533.
[52] South Africa at TRIPS Council Meeting, IP/C/M/96/Add.1 (February 2021), para. 853.
[53] TRIPS Council Meeting, IP/C/M/33 (November 2001), para. 166.
[54] J. Smith, C. Mallouris, K. Lee, and T. Alfvén, “The Role of Civil Society Organizations in Monitoring the Global AIDS Response,” AIDS and Behavior 21/1 (2017).
[55] WTO Communication, IP/C/W/684 (September 2021), para. 6.
[56] Kohler et al. (see note 35).
[57] Perehudoff et al. (2016, see note 14).
[58] E. M. da Fonseca, K. C. Shadlen, and F. I. Bastos, “The Politics of COVID-19 Vaccination in Middle-Income Countries: Lessons from Brazil,” Social Science and Medicine 281 (2021).
[59] M. K. Land, “Human Rights Frames in IP Contests,” in R. Dreyfuss and C. Rodríguez-Garavito (eds), Balancing Wealth and Health: Global Law and the Battle over Intellectual Property and Access to Medicines in Latin America (New York: Oxford University Press, 2014).
[60] J. Enoch and P. Piot, “Human Rights in the Fourth Decade of the HIV/AIDS Response: An Inspiring Legacy and Urgent Imperative,” Health and Human Rights Journal 19/2 (2017).
[61] Hestermeyer (see note 20), p. 212.
[62] Ibid., pp. 221–222.
[63] A. Kapczynski, “The Right to Medicines in an Age of Neoliberalism,” Humanity: An International Journal of Human Rights, Humanitarianism and Development 10/1 (2019), pp. 86–88; Kohler et al. (see note 35).
[64] C. Williams and A. Blaiklock, “Human Rights Discourse in the Sustainable Development Agenda Avoids Obligations and Entitlements: Comment on ‘Rights Language in the Sustainable Development Agenda; Has Right to Health Discourse and Norms Shaped Health Goals?’,” International Journal of Health Policy and Management 5/6 (2016).