Revisiting Health Rights Litigation and Access to Medications in Costa Rica: Preliminary Evidence from the Cochrane Collaboration Reform
Olman Rodríguez Loaiza, Sigrid Morales, Ole Frithjof Norheim, and Bruce M. Wilson
Abstract
In response to the incremental creation of an expansive constitutional right to health in Costa Rica, the country’s rights-friendly constitutional chamber of the Supreme Court (known as the Sala IV) unleashed a flood of litigation for medications, treatments, and other health care issues. This development was met by widespread criticism from within the health sector, which complained that the court’s jurisprudence routinely elevated the right to health above financial considerations, thus posing a threat to the financial well-being of the state-run health care system.[1] Further, a 2014 study by Ole Frithjof Norheim and Bruce Wilson examining successful health rights litigation revealed that more than 70% of favorable rulings were for low-priority medications, suggesting a lack of fairness in access to medications in Costa Rica.[2] To address some of these criticisms, the Sala IV initiated a partnership in 2014 with the Cochrane Collaboration to incorporate medical expert evaluations into its decision-making process for claims seeking access to medications. This article examines the court’s reformed decision-making process to determine whether the increased reliance on medical expertise has changed health rights jurisprudence. We reviewed all medication claims from 2016 and classified the successful cases into four groups using standard priority-setting criteria. We then compared these results with rulings issued in 2008, prior to the court’s reform (and the year analyzed in Norheim and Wilson’s study). Our analysis reveals that under the court’s new rules, the probability of winning a medication lawsuit has increased significantly; moreover, the percentage of rulings granting experimental medications has declined while the percentage granting high-priority medications has increased. Based on these results, in comparison to the court’s pre-reform jurisprudence, we can tentatively conclude that the new process has led to some minor gains in fairness.
Introduction
Starting in the mid-1990s, many Latin American countries witnessed an increased use of litigation to claim access to medical procedures and medications.[3] This judicialization of health care made courts “key actors of health policy” and generated an apparent conflict between two ethical imperatives: fair, efficient health spending priorities and individuals’ health rights.[4] The rapid increase in litigation for health rights was met by criticism from some national health system leaders who claimed that court decisions distorted their budgets, undermined the ability of national health systems to rationally allocate scarce resources, impaired the overall performance of health systems, and undermined these systems’ solvency.[5] Magistrates often pushed back, stating that court intervention is justified when “administrative inefficiencies or prioritization processes of health services fail to protect an individual’s right” and rejecting the idea that “access to care should be determined by the price mechanism.”[6]
While the judicialization of health care became a reality in many countries around the world, one court in particular came under intense criticism for its health rights jurisprudence: the Constitutional Chamber of the Supreme Court of Costa Rica (Sala Constitucional or Sala Cuarta, commonly written as Sala IV).[7] Costa Rica’s state-owned and -funded health care system, administered by the Costa Rican Social Security Fund (Caja Costarricense de Seguro Social, commonly referred to as the Caja), loudly and frequently complained that Sala IV health rights decisions harmed its capacity to manage the health system’s resources in a fair and efficient manner and that the magistrates lacked the medical training and knowledge necessary to issue rational, medically informed health-related rulings.[8] Two of this paper’s authors made an earlier contribution to this ongoing debate on ballooning health rights litigation.[9] Using standard priority-setting criteria, we examined the technical aspects of the court’s decisions in order to evaluate whether these decisions led to more fairness in access to medications. We found that in 2008, over 70% of the court’s decisions favoring litigants’ claims were for medications classified as “low priority,” while less than 3% of the decisions were for medications classified as “high priority” (these criteria are explained further below).
While that article did not address the financial impact of medication claims or non-medication health rights claims (which include requests for access to clinics or to treatments such as surgeries), or the suitability of health rights litigation, it concluded that in the case of Costa Rica, litigation does not necessarily lead to more fairness in access to medication. We noted that Sala IV magistrates, while strongly defending their constitutional right to decide health rights cases, were cognizant of the criticism leveled at the court’s lack of medical expertise and its deference to the opinions of claimants’ treating doctors. As a result, the court, with the support of the World Bank Institute, sought to expand its access to medical expertise through a technical cooperation agreement with the Cochrane Collaboration. The goal was to add a new layer of independent medical expert assessment that could inform and improve the fairness of Sala IV decisions on medication cases.[10] It is the development of this new process currently used by the court in the deliberation of health rights litigation that is of interest here. We analyze whether the new process involving outside medical expertise has improved the court’s health rights jurisprudence using priority-setting criteria. Little is known about the potential impact of medical expert assessment on jurisprudence and priority setting for new medications in any country. This article examines this new process in Costa Rica and compares successful health rights litigation claims for medications before (2008) and after (2016) the reform.
The article proceeds as follows. We first contextualize and describe the Costa Rican health care system, how it became judicialized from the mid-1990s onward, and how the Sala IV created an explicit constitutional right to health and gave little consideration to the economic impact of its decisions. We then detail the Sala IV’s process for deciding medication cases that developed over two decades prior to the initiation of the court’s reformed decision-making process, which includes an additional layer of expert medical opinion. Next, we examine the impact of the new process through a priority-setting evaluation of all 108 medication cases decided by the Sala IV in 2016 (the only full year under the rules of the new process), which allows us to better understand who benefits and how much they benefit compared to other patients.[11] We then compare these priority-setting results with those of the pre-reform process outlined in Norheim and Wilson’s 2014 study. Lastly, we present our conclusions concerning the impact of the Cochrane Collaboration and the new layer of expert opinion on the Sala IV’s medication-related jurisprudence and suggest areas of future research to further investigate the impact of the judicialization of health care in Costa Rica and beyond.
Costa Rica
Costa Rica is a small, upper-middle-income, largely urban Central American country, with a population of approximately 4.9 million.[12] The country has long stood out as one of the most democratic countries in the Americas for its universal adult franchise and free and fair elections held every four years without interruption or challenge since 1953.[13] The country enjoys an expansive public welfare system that includes education, insurance, pensions, and a well-funded public health system that received 6.8% of the gross domestic product (GDP) in 2014, which is among the top 30 highest state expenditures on public health in the world and almost double the Latin American average.[14] The country also has some of the highest social indicator values in Latin America, including a very high life expectancy (79.6 years), a Human Development Index score of 0.776 (66th highest in the world), and a low poverty rate (20.5%).[15] A region-wide United Nations report notes that Costa Rica is one of only two countries in the Americas with “optimal access” to basic medications and enjoys almost universal health care coverage.[16]
Courts and health rights
The judicialization of health in Costa Rica was therefore not a response to an ineffectual, inefficient health care system. Rather, it took place in the context of a well-functioning, effective, universal health care system that facilitated the attainment of impressive health statistics. Litigation claiming a right to health care began to emerge slowly in the mid-1990s and then expanded very rapidly in the late 1990s, and was sparked by two consecutive events: First, a judicial reform in 1989 created a constitutional chamber of the Supreme Court (the Sala IV), which opened a very accessible legal arena allowing anyone to approach the court to seek protection of his or her rights. Second, the inability or unwillingness of the public health system to respond to the HIV/AIDS epidemic in the 1990s pushed people living with HIV and AIDS to use the newly created court to seek medical help; this was a response to the public health care system’s routinely voiced argument that antiretroviral medications were not a cure, were too expensive, and should not be provided.[17]
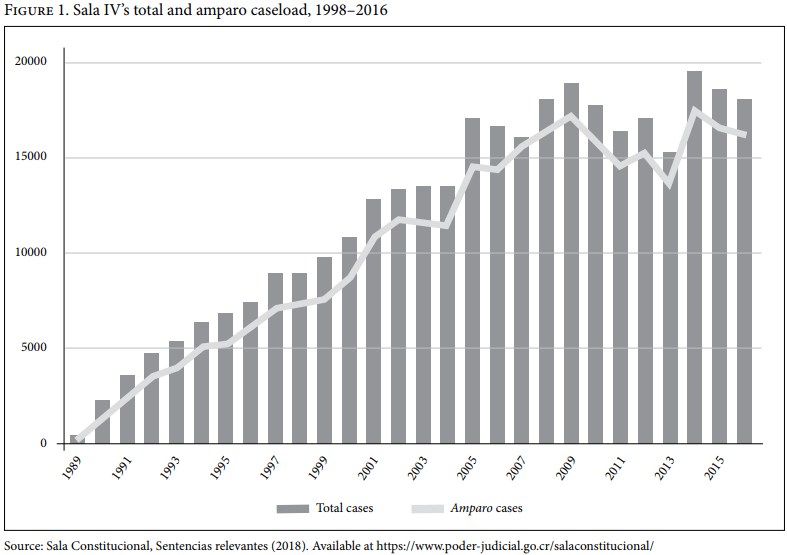
The creation of the Sala IV and its profound impact on the country’s polity has been covered extensively elsewhere.[18] In short, it was a watershed event that transformed the country’s superior court from a dormant institution that exercised little oversight of the other branches of government and had little interest in hearing cases on individuals’ constitutional rights into one of the most powerful and assertive courts in the Americas.[19] Once it was rolled out in late 1989, the Sala IV immediately discarded the Supreme Court’s strict legal formality and accepted amparo cases (writs of protection) from anyone in the country regardless of that person’s age, sex, income, nationality, or ethnic origin. Filing a case before the Sala IV requires no lawyers, no fees, and very few hurdles. The court renders decisions quickly, and its decisions are binding on all people and institutions, with the exception of the court itself. The speed with which the court became a logical and recognizable venue to challenge perceived injustices is illustrated in Figure 1: the Sala IV’s caseload increased from fewer than 2,300 cases in 1990 (its first full year of operation) to almost 20,000 in 2014, before settling at approximately 18,000 cases per year thereafter. Individuals using the simple, low-cost writ of amparo account for more than 80% of all cases before the Sala IV.[20]
In the court’s early years, health rights cases were not part of its rapidly expanding docket. This was in part because the health system functioned well and, perhaps more importantly, because the Constitution lacked an explicitly encoded right to health. Yet, over the years, the court gradually and deliberately created an expansive right to health by building on explicit articles in the Constitution, including the protection of human life (article 21) and the right to social security protection (article 73), as well as international instruments to which Costa Rica was a signatory.[21] Under Costa Rican law, international instruments have an “almost supra constitutional value,” which allows the Sala IV to amplify and add to the existing explicit rights contained in the Constitution.[22] By the mid-1990s, court jurisprudence effectively created an expansive, justiciable “fundamental right” to health, but with explicit financial limitations that the court considered in its rulings. By way of an example, in 1992 the Sala IV rejected an amparo claim filed by the president of the Association for the Struggle against AIDS, Jacobo Schifter, on behalf of people living with HIV/AIDS, demanding that the public health care system provide free access to azidothymidine. The court’s unanimous decision accepted the Caja’s argument that azidothymidine was not a cure for HIV/AIDS and that “the cost of purchasing the drug implies a very large sacrifice for [the Caja], which does not have a budget committed to such ends.”[23] The court noted the ethical dilemma of requiring the purchase of azidothymidine, pointing out that other people in similarly delicate or terminal situations had no access to budget allocations for their medications. It argued that this “aspect cannot be left unnoticed, as there are certain diseases for which there are still no budgets committed to them and, from that perspective, to demand that the Caja disregard certain other programs to assist those suffering from AIDS, no matter how hard it seems, is not reasonable.”[24]
In 1997, however, the court changed tracks, issuing a decision ordering antiretroviral medications to be provided to people living with HIV/AIDS.[25] As a result, the previously slow stream of health rights cases quickly became a flood and ushered in the full judicialization of health care in Costa Rica. According to Carlos Zamora, an actuarial scientist at the Caja, the 1997 HIV/AIDS decision was central to the development of the Sala IV’s right to health jurisprudence; the legal arguments “served as a model that has shaped the field of health rights.”[26] In its decision, the court articulated its most expansive understanding of the right to health: “What good are the rest of the rights and guarantees … if a person cannot count on the right to life and health assured?”[27] In the years following this decision, the court increasingly and consistently dismissed the Caja’s arguments that some medications were prohibitively expensive and should not be provided. Finally, in 2007, it issued a decision categorically stating that the Caja could not use “eminently economic reasons” to decline to fill a patient’s prescription when the prescribed medicine falls outside the Caja’s official list of medications (LOM).[28] The rapid growth in successful health rights litigation sparked a growing chorus of complaints concerning the financial burden on the Caja, which was forced to pay for medications that its own medical experts had already evaluated and declined to include in the LOM.[29]
Studies of the financial impact of the court’s decisions repeatedly invalidate the Caja’s allegation that costs incurred from compliance with these decisions are bankrupting the health system or causing an unwanted re-equilibration of expenditures. Indeed, a 2009 study sponsored by the Caja itself revealed that the total cost of providing all successfully litigated medications amounted to less than 1% of the institution’s medication budget.[30] Similar studies undertaken by other researchers, not affiliated with the Caja, corroborate the Caja’s initial results.
The new process for constitutional health rights adjudication for medications
The 2014 article closes by noting that the Sala IV recognized its lack of medical technical expertise and initiated a collaborative program with an international agency, the Cochrane Collaboration, with the support of the World Bank Institute.[31] The Cochrane Collaboration, named for Scottish doctor Archie Cochrane, is a UK-based not-for-profit international collaboration of 37,000 medical experts from over 130 countries. The experts collaborate to “produce credible, accessible health information that is free from commercial sponsorship and other conflicts of interest.”[32] This partnership allowed the court access to evidence-based medicine databases in the Cochrane library that could be used in cases where the lawsuit involved a claim for a specific medication. As part of the agreement, in mid-2014, two groups of law clerks from the Sala IV—including two of the authors of this article (Morales and Rodriguez)—and forensic doctors attended a two-week workshop on how to use the Cochrane Library and other medical databases to assess medications that were the subject of litigation. It is noteworthy that Cochrane reviews typically summarize only the quality of evidence for a proven treatment effect of a new medication. A comprehensive health technology assessment (HTA) is necessary for a full assessment of evidence on cost-effectiveness and other organizational and ethical aspects of introducing the new technology in question. To overcome some of these limitations, the training was designed to teach law clerks to read and understand the latest available scientific evidence, how to interpret medical data and statistics, and how to analyze the benefits and weaknesses of specific medications for patients.
In the second half of 2015, the Sala IV implemented its new procedure for medication cases, which effectively diminished the court’s previous reliance on the testimony of patients’ treating physicians rather than evidence from the Caja.[33] The process replaced a “dogmatic approach of a medical case by a treating physician” with one more reliant on evidence-based medicine.[34] This system has proven a novel way to substantiate health rights cases before rendering a final ruling and to publicly address the criticisms leveled against the Sala IV’s health rights jurisprudence for being technically and scientifically uniformed. This new approach to medication cases is not the result of an amendment to Costa Rica’s legal framework; rather, it is a court-led initiative to improve the court’s performance using evidentiary rules that allow it to find new facts or information, at no cost to claimants, to deliver fair and balanced decisions.
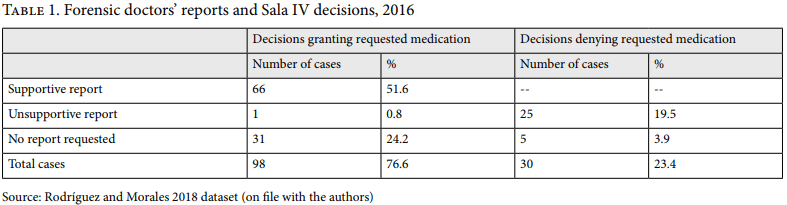
The new process begins when a treating doctor prescribes a medication for a patient that is not part of the official LOM drawn up by the Caja’s pharmacopoeia committee. In order to litigate for this medication, both the patient and the physician must be part of the Caja health care system; moreover, a claim may be filed with the Sala IV only after all appeals processes in the Caja have been exhausted. Under the court’s pre-reform process, Sala IV magistrates tended to accept the evidence presented by the treating doctor as santa palabra (indisputable) and decide in favor of the patient under the belief that the treating doctor knows the patient’s particular medical situation best. The new process follows the same path as the old one to the extent that cases are filed with the Sala IV and the court then requests relevant supporting evidentiary and argumentative documents from the Caja and the patient’s treating doctor before deciding the case. In its post-reform process, however, the court might reject the case for technical reasons, refer it to the medicatura forense (forensic clinic), or issue a decision without requesting an external report for further evaluation. As Table 1 shows, in 2016, the first full year of the reformed process, approximately 72% of all medication cases included a request for a forensic doctor’s report, while 28% of cases did not.
If the court requests a report from one of the ten forensic units around the country, a Caja medical forensic doctor will provide a written evaluation. The assigned doctor must study the patient’s medical records, perform a full physical examination of the patient, and evaluate the appropriateness of the claimed medication using international medical databases. Once this is complete, the doctor must send a written report to the Sala IV with his or her expert opinion concerning the competing claims of the treating doctor and the Caja with regard to the appropriateness of the medication for the patient in question. The court uses this report in its decision-making process. As Table 1 shows, the court overwhelmingly accepts the conclusions of forensic doctors: in 2016, Sala IV magistrates accepted all forensic doctors’ reports, with the exception of one case in which the court overruled an unsupportive report.
Data
Although the court’s new process for deciding medication cases started with training workshops in mid-2014, implementation lagged until the second half of the following year. Thus, we elected to focus on all cases litigated in 2016, the only year thus far in which the court has operated under the new Cochrane Collaboration rules and for which complete data are available. We examined all 128 cases presented to the Sala IV that year claiming a specific medication and extracted information for the 98 cases for which the court issued a favorable ruling. We then used the same framework for priority classification that Norheim and Wilson used in their 2014 study. This framework is based on fairness and efficiency criteria from the public health and priority-setting literature.[35]
Priority group I = High-priority interventions
Priority group II = Medium-priority interventions
Priority group III = Low-priority interventions
Priority group IV = Experimental interventions
According to this framework, an intervention for a given condition is assigned high priority if the condition is severe (in terms of lost life years or the loss of quality of life in the absence of the drug in question); if the intervention is highly effective (in terms of improved health in terms of life years or quality of life); and if the intervention is reasonably cost-effective. The measure of effectiveness used in most HTA reports and cost-effectiveness studies is the quality-adjusted life year (QALY). To preserve comparability with Norheim and Wilson’s 2014 study, we used the same thresholds for cost-effectiveness (incremental cost per QALY gained):
cost-effective: < GDP per capita
intermediate: > GDP per capita < 3 x GDP per capita
not cost-effective: > 3 x GDP per capita
More recently, this classification has been criticized, and an alternative suggestion is to classify interventions as cost-effective if the incremental cost per QALY gained is below 0.5 GDP per capita.[36]
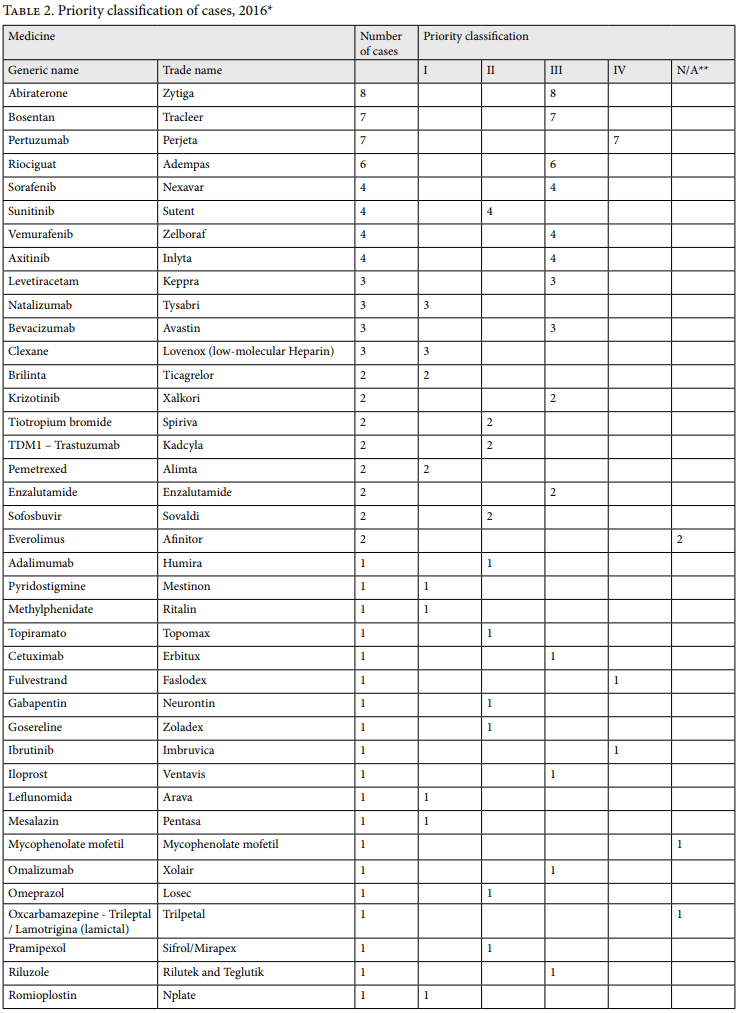
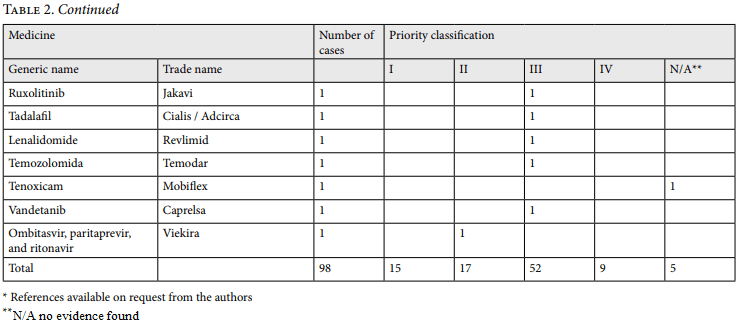
In addition, the framework’s definition of “experimental interventions” refers to interventions judged as experimental according to independent experts (such as the Cochrane Collaboration) or trusted health technology assessment agencies (such as the National Institute of Health Care Excellence in the UK). Table 2 provides a breakdown of our classification of the 2016 cases.
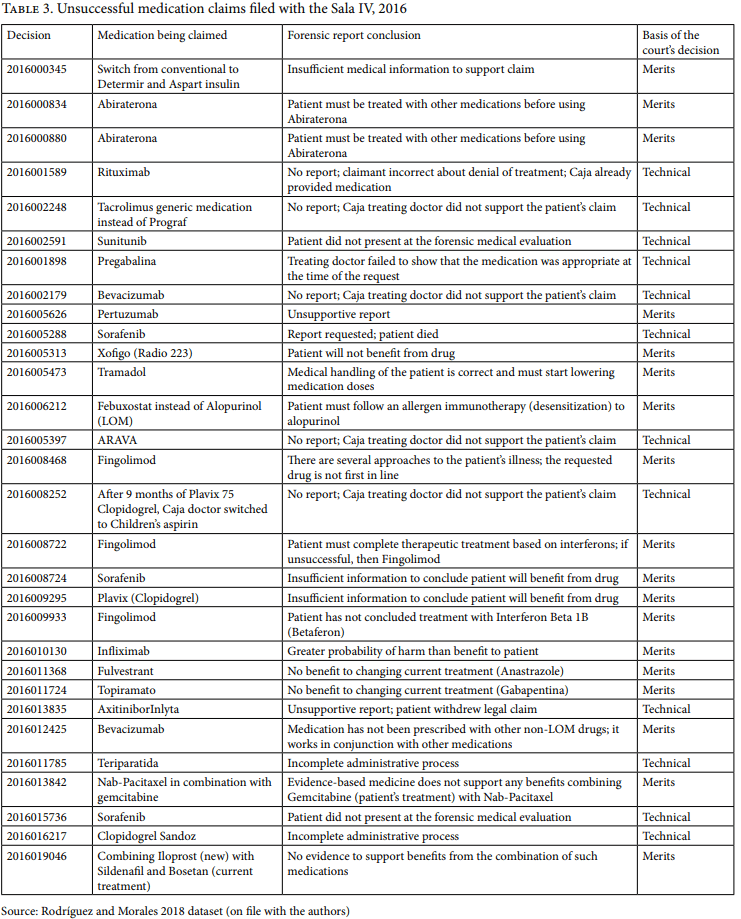
Before we consider the results of the Sala IV’s new process for deciding medication cases, a brief comment on the 23% unfavorable rulings (shown in Table 3) is in order, as it helps highlight the significance of forensic reports for the court’s decision making. Of the 30 unfavorable rulings, 26 received unsupportive forensic reports; final court decisions accepted the findings of 25 of those cases. The unsupportive reports detail that evidence-based medicine shows limited benefits to the patients of the medications claimed, that the required Caja medication protocol has not yet been completed, or that the patient’s medical examination reveals possible harm from the claimed medication. For the remaining five unsuccessful cases, no report was requested. Those five cases were rejected for a variety of technicalities, such as the patient filing the case without the support of his or her treating doctor, the patient’s death, and the patient’s failure to attend the required medical examination at the forensic clinic.
Results
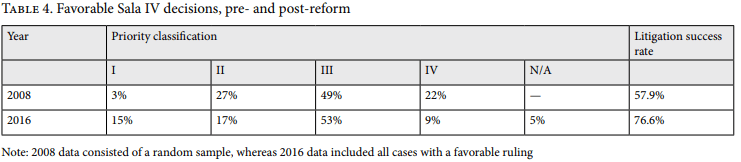
Of the 98 successful medication cases (in other words, those with favorable rulings) filed in 2016, 15% fell into priority group I, 17% fell into group II, 53% fell into group III, 9% fell into group IV, and 5% were unclassifiable (see Table 4). This means that 62% of successful cases could be classified as being of clearly low priority (groups III and IV) by common standards. Medications that were assigned low priority share some common characteristics: they are new on the market, have a very high cost compared to their benefits (often 3–5 times Costa Rica’s per capita GDP), target severe conditions such as cancer or rare diseases, and are similarly disputed in countries with much higher levels of health care spending (such as the UK and Norway).
Discussion
Table 4 presents the priority classifications of successful medication claims from 2008 and 2016—that is, cases filed both before and after the rollout of the Sala IV’s new system relying on independent expert advice. We found that a lower proportion of experimental cases were successful in 2016 (9%) compared to 2008 (22%). The proportion of high-priority cases increased from 3% in 2008 to 15% in 2016, while the proportion of medium-priority cases went down. Low-priority cases remained relatively stable between the two periods.
Although many other factors may explain this change, the reduction in successful cases for experimental drugs could be a result of more thorough, independent expert assessment. From a health systems and health policy perspective, this change might indicate a positive development. Yet we find that the proportion of low-priority medications is high (more than 50%) and relatively stable. These are medications that are typically new on the market, are not reimbursed in the public system, and have very high prices and low cost-effectiveness. This finding is unsurprising, since Cochrane reviews do not include considerations on cost-effectiveness and the court still maintains its belief that its decisions do not impose undue financial costs on the Caja’s medications budget. A comprehensive HTA is needed for an assessment of evidence on cost-effectiveness. One possible interpretation of the results concerning successful cases is that the court is better informed than before about whether a new medication is proven to be effective, but not better informed about its cost-effectiveness. Another interpretation might be that the court has this information but chooses not to take it into account. The low-priority medications are well known in the HTA and priority-setting literature from Europe, such as in the UK and Norway. Several of them have not been prioritized in these countries, or at least not before undergoing substantial price reductions. Information about their cost-effectiveness in a European context is relative easy to find from HTA databases.
We note two possibly negative implications from our findings. First, favorable court decisions for very costly new medications may undermine the opportunity for the Caja to engage in price negotiations with pharmaceutical companies. European countries have been successful in obtaining substantial price reductions through the strict and systematic use of comprehensive HTAs and through a clear system for priority setting. This favor patients in the long run, as lower prices benefit the health system and, as a consequence, its users. Second, we found fewer successful cases than one would expect based on the incidence of certain diseases that require particular medications. One possible interpretation is that many other patients in similar situations may not have received the treatment in question. Historically, though, the Caja has sometimes updated its LOM in response to increasing numbers of successful amparos seeking specific medications. For example, after the successful 1997 antiretroviral case and the following avalanche of cases, the Caja included antiretroviral medications in the LOM, thus extending coverage to people who did not go to court. It is also possible that patients who would have been denied access to non-LOM medications via litigation might have received them from the Caja through an administrative procedure instead. Indeed, the Caja can and does provide non-LOM medications to patients on a case-by-case basis. The cases that end up at the Sala IV tend to be the more difficult ones, such as those in which a local Caja committee might side with the treating doctor but the central Caja committee might reject that recommendation and deny the medication. Thus, it is difficult to know what the exact budget impact of the low number of successful cases for each type of medication might be or to assess whether that impact is negative from a health system, legal, and ethical perspective: it is not entirely clear if persons with the same condition are necessarily being treated equally. Another way to look at the issue is that if a patient wins access to a specific medication for his or her condition, then a similarly situated patient denied that medication by the Caja will be able to subsequently litigate for the same medication.
Finally, this study suggests that the court may need to go beyond the Cochrane Collaboration and undertake comprehensive HTAs to evaluate whether a particular drug should be prioritized. Such evaluations are easily available from many countries, and the same drugs are assessed everywhere. This challenge is not national but international. A regional collaboration for rapid HTAs, horizon scanning, and translation of HTAs from other countries and a review of their recommendations could improve the situation further. Involving the Cochrane Collaboration and forensic doctors is a positive first step, but more can be done.
Strengths and limitations
Although this article is, to the best of our knowledge, the first to evaluate Sala IV decisions from a priority-setting perspective both before and after the court’s reform expanding the use of evidence-based medicine, our findings should be interpreted with caution. Due to lack of detailed information, we classified the cases according to typical outcomes for the average patient in need of the relevant medication. Particular individual circumstances that could, on medical grounds, favor or disfavor the person in question were not taken into account.
We would also like to note that the court is not obligated to request expert medical advice on each case or to follow the recommendations contained in those reports. However, the court tends to follow the vast majority of these recommendations when requested; and when such reports are not requested, it generally follows the recommendation of the patient’s treating doctor (as was the case before the Cochrane Collaboration reforms). But our study concerns the question only of fairness and not of costs, and it is limited to claims for medications not included in the Caja’s official list of medications. While medications are an important and potentially expensive subcategory of health rights cases, they are not the universe of those cases. Litigation for surgeries, other treatments, and waiting lists is growing rapidly and taking up more of the court’s docket, but for these cases the court does not request third-party expert reports to inform its decisions.
Our method is based on available evidence, and we use explicit criteria grounded in theories of fair priority setting in health. Our assessment, interpretation, and classification of the evidence into priority groups involves discretion. There is some agreement on priority criteria, but reasonable people may disagree on their relative weight and on the classification of new medications. Every system of priority classification is bound to be controversial. Therefore, we do not regard our classification as the “gold standard,” and we invite further independent scrutiny; nonetheless, we believe our conclusions to be relatively reasonable. Finally, we would like to note that priority classification is based on data from other countries. Issues related to variability and comparability of cost, process, and use of health personnel may limit the transferability of results from HTAs in one country to another. However, some of the new medications appear to have such low cost-effectiveness that it is unlikely that national studies would change the conclusion.
Acknowledgments
The authors wish to thank Fernando Castillo Víquez, Fernando Cruz Castro, Paul Rueda Leal, Nancy Hernandez López, José Paulino Hernandez Gutiérrez, Evelyn Villarreal, Kattia Salas, Kerstin Hamann, Luis Ardón Acuña, Marcela Calderón Barrantes, Franz Vega Zúñiga, Josette Bogantes Rojas, Pablo David Navarro Villalobos, Mario Tristan, Yuri Baidal, and the Health and Human Rights Journal’s anonymous referees for their insights and comments.
Olman Rodríguez Loaiza is a law clerk at the Constitutional Chamber of the Supreme Court of Costa Rica, San José, Costa Rica.
Sigrid Morales is a law clerk at the Constitutional Chamber of the Supreme Court of Costa Rica, San José, Costa Rica.
Ole Frithjof Norheim is a professor at the University of Bergen, Norway.
Bruce M. Wilson is a professor at the University of Central Florida, Orlando, USA, and an associated senior researcher at the Chr. Michelsen Institute, Bergen, Norway.
Please address correspondence to Bruce M. Wilson. Email: bruce.wilson@ucf.edu.
Competing interests: None declared.
Copyright © 2018 Rodríguez, Morales, Norheim, and Wilson. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1]. R. A. Navarro Fallas, Derecho a la salud: un análisis a la luz del derecho internacional, el ordenamiento jurídico costarricense y la jurisprudencia constitucional (San José: Editorial Juricentro, 2010).
[2]. O. F. Norheim and B. M. Wilson, “Health rights litigation and access to medicines: Priority classification of successful cases from Costa Rica’s Constitutional Chamber of the Supreme Court,” Health and Human Rights 16/2 (2014).
[3]. L. Cubillos, M-L. Escobar, S. Pavlovic, and R. Iunes, “Universal health coverage and litigation in Latin America,” Journal of Health Organisation and Management 26 (2012), pp. 390–406.
[4]. A. Yamin and S. Gloppen (eds), Litigating health rights: Can courts bring more justice to health? (Cambridge, MA: Harvard University Press, 2011); Cubillos et al. (see note 3), p. 403; B. Rumbold, R. Baker, O. Ferraz, et al., “Universal health coverage, priority setting, and the human right to health,” Lancet 390/10095 (2017), pp. 712–714.
[5]. E. Lamprea, “The judicialization of health care: A Global South perspective,” Annual Review of Law and Social Science 13 (2017), pp. 431–449; O. Ferraz, “Brazil: Health inequalities, rights and courts,” in A. Yamin and S. Gloppen (eds), Litigating health rights: Can courts bring more justice to health? (Cambridge, MA: Harvard University Press, 2011).
[6]. Cubillos et al. (see note 3), p. 392; A. Yamin “Power, suffering, and courts,” in A. Yamin and S. Gloppen (eds), Litigating health rights: Can courts bring more justice to health? (Cambridge, MA: Harvard University Press, 2011), p. 334.
[7]. See, for example, the Gaceta Medica de Costa Rica 7/2 (2007); B. M. Wilson, “The causes and consequences of health rights litigation in Costa Rica,” in A. Yamin and S. Gloppen (eds), Litigating health rights: Can courts bring more justice to health? (Cambridge, MA: Harvard University Press, 2011).
[8]. J. D. Romero, “Sala Constitucional y Caja Costarricense de Seguro Social,” Gaceta Medica de Costa Rica 7/2 (2007), pp. 124–129.
[9]. Norheim and Wilson (see note 2).
[10]. Cooperación Técnica entre la Sala Constitucional de Costa Rica y la Colaboración Cochrane (2014). Available at http://youtu.be/-FTUHIunv8?list=UU5pGw_JyZ1daGCnX-MlCtDvg; Observatorio Judicial, Sala Constitucional y médicos forenses se capacitan. Available at https://www.poder-judicial.go.cr/observatoriojudicial/vol169/capacitacion/cap2.html.
[11]. A. Yamin and O. Norheim, “Taking equality seriously: Applying human rights frameworks to priority setting in health,” Human Rights Quarterly 36 (2014), pp. 296–324.
[12]. World Population Review, Costa Rica population 2018 (2018). Available at http://worldpopulationreview.com/countries/costa-rica-population.
[13]. Freedom House, Costa Rica (2018). Available at https://freedomhouse.org/report/freedom-world/2018/costa-rica.
[14]. World Bank, Health expenditure, public (% of GDP) (2018). Available at https://data.worldbank.org/indicator/SH.XPD.PUBL.ZS.
[15]. World Health Organization, Life expectancy at birth, 2000–2015 (2018). Available at http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/tablet/atlas.html; United Nations Development Programme, 2016 Human Development Report (2016). Available at http://hdr.undp.org/en/countries/profiles/CRI; World Bank, Poverty headcount ratio at national poverty lines (% of population (2017). Available at https://data.worldbank.org/indicator/SI.POV.NAHC.
[16]. Wilson (2011, see note 7), p. 133.
[17]. See, for example, B. M. Wilson, “Claiming Individual rights through a constitutional court: The example of gays in Costa Rica,” International Journal of Constitutional Law 5 (2007), pp. 242–257.
[18]. See, for example, C. J. Gutiérrez Gutiérrez, “La constitución 50 años después,” in C. J. Gutiérrez Gutiérrez et al. (eds), Temas claves de la constitución política: investigaciones jurídicas (San José: Editorial Investigaciones Jurídicas, 1999), or, more recently, B. M. Wilson, “Enforcing Rights and exercising an accountability function: Costa Rica’s Constitutional Court,” in G. Helmke and J. Rios-Figueroa (eds), Courts in Latin America (New York: Cambridge University Press, 2011), pp. 55–80.
[19]. S. Gloppen, B. Wilson, R. Gargarella, et al., Courts and power in Latin America and Africa (New York: Palgrave Macmillan, 2010).
[20]. Sala Constitucional, Sentencias relevantes (2018). Available at https://www.poder-judicial.go.cr/salaconstitucional.
[21]. K. Vargas López, “El desarrollo del derecho a la salud por parte de la Sala Constitucional y su influencia en el sistema público de salud en Costa Rica,” Master’s thesis (Ciudad Universitario Rodrigo Facio, San José, Costa Rica, 2010).
[22]. L. F. Solano Carrera, “Derecho fundamental a la salud,” Gaceta Médica de Costa Rica 9/2 (2007), pp. 141–50; R. Navarro Fallas, Derecho a la salud (San José: Editorial Juricentro, 2010); F. Cruz Castro, “Costa Rica’s constitutional jurisprudence, its political importance and international human rights law: Examination of some decisions,” Duquesne Law Review 45/3 (2006–2007), pp. 557–576.
[23]. Sala Constitucional, Resolución 280-92 (1992).
[24]. Ibid.
[25]. Sala Constitucional, Resolución 5934-97 (1997).
[26]. C. Zamora Zamora, “Los recursos de amparo y los recursos de constitucionalidad con la Caja de 1989 a 2008,” Caja Costarricense de Seguridad Social, Dirección Actuarial, working paper (2010).
[27]. Sala Constitucional, Resolución 5934-97 (1997).
[28]. Sala Constitucional, Resolución 2007-00043 (2007).
[29]. H. V. Hogerzeil, M. Samson, J. V. Casanovas, and L. Rahmani-Ocora, “Is access to essential medicines as part of the fulfilment of the right to health enforceable through the courts?” Lancet 368/9532 (2006), pp. 305–311.
[30]. A. Chaves Matamoros, “Derecho a la salud pública: papel de la Sala Constitucional” (Escuela de Salud Pública de la Facultad de Medicina de la Universidad de Costa Rica, August 26, 2010); A. Chaves Matamoros, “Segundo Encuentro Costarricense Sobre Judicialización de la Salud y Sistemas e Salud” (2013).
[31]. Norheim and Wilson (see note 2).
[32]. Cochrane, About us. Available at www.cochrane.org/about-us.
[33]. Romero (see note 8).
[34]. F. Castillo V., “Derecho a la salud: Recientes evoluciones de la jurisprudencia constitucional.” Available at https://www.poder-judicial.go.cr/salaconstitucional/images/cefcca/Documentos/Derechoalasalud/CONFERENCIADERECHOALASALUD.pdf.
[35]. World Health Organization, Making fair choices on the path to universal health coverage: Final report of the WHO Consultative Group on Equity and Universal Health Coverage (Geneva: World Health Organization, 2014); O. F. Norheim, “Ethical priority setting for universal health coverage: Challenges in deciding upon fair distribution of health services,” BMC Medicine (2016).
[36]. B. Woods, P. Revill, M. Sculpher, and K. Claxton, “Country-level cost-effectiveness thresholds: Initial estimates and the need for further research,” Value Health 19/8 (2016), pp. 929–935.