Emotional Difficulties and Experiences of Stigma Among Persons with Lymphatic Filariasis in Plateau State, Nigeria
Jibril Abdulmalik, Emeka Nwefoh, James Obindo, Samuel Dakwak, Motunrayo Ayobola, John Umaru, Elisha Samuel, Christopher Ogoshi, and Julian Eaton
Introduction
Lymphatic filariasis (LF) is a chronic and disfiguring condition that can lead to significant disability.1 Global estimates project that infection with the filarial parasite, which causes LF, is present in at least 120 million persons, with about 40 million people exhibiting clinical symptoms and signs.2 Thus, the condition is now recognized as a public health priority, along with other neglected tropical diseases (NTDs).3
This recognition has led to concerted efforts to eliminate the threat of LF and other NTDs, such as the launch of the Global Programme to Eliminate LF by 2020.4 A combined approach using several initiatives—including the use of mass drug administration campaigns as preventive chemotherapy in endemic areas, the provision of effective treatment for infected persons, and sustainable water, sanitation, and hygiene programs—has been deployed globally with successful results. The prevalence of LF in Nigeria ranges from 14% to 32%, depending on the region.5 Over 106 million people in the country have been found to be at risk of LF, making Nigeria the country with the largest at-risk population in Africa.6 Nonetheless, significant progress is being made with respect to mass drug administration across endemic regions and treatment for affected persons. Indeed, two North Central states of Nigeria that were previously endemic for LF (Plateau and Nassarawa) recently met criteria to stop statewide mass drug administration for LF—the very first states in Nigeria to achieve this feat.7 Despite this progress in prevention efforts, individuals already affected must live with the long-term consequences of the disease.
Increasingly, NTDs, including LF, have been recognized as being associated with a reduced quality of life as a result of social exclusion, stigma, and discrimination.8 Stigma is the result of a real or perceived difference that causes affected individuals or groups to be identified as inferior. It pertains to “any attribute, trait or disorder that marks an individual as being unacceptably different from the accepted norm, and that elicits some form of community sanction”.9 Such traits or attributes include physical deformity, disease condition, gender, sexual orientation, and ethnicity, among others. Discrimination—also described as enacted stigma—is a closely associated concept that describes unfair and unjust treatment. Thus, stigma is best seen as a composite of three issues: (1) ignorance of a condition or people; (2) prejudice manifesting as fear, anxiety, and avoidance; and (3) discrimination resulting in systematic disadvantages in various domains of life, including work life, home and personal life, community participation, and access to health care.10
Several studies have explored stigma and its associated socioeconomic consequences among affected persons living with LF and other NTDs, but there is a paucity of studies seeking to understand the stigma, associated experiences of exclusion and discrimination, and emotional reactions and consequences among persons living with LF in Nigeria, despite the country having the largest disease burden in Africa.11 Recent estimates conservatively estimate that 50% of clinical patients with LF have co-morbid depression.12 Others have also postulated that stigma and discrimination lead to co-morbid mental health problems and to a reduction in health-related quality of life.13 The wider burden of LF is therefore likely to be considerably higher if these co-morbidities are taken into account.
Furthermore, the spirit of the Sustainable Development Goals (SDGs) is to “leave no one behind,” thus emphasizing the importance of equity as a consideration in international development. LF and other NTDs are known to disproportionately affect the most disadvantaged: the rural poor with reduced access to health care services and clean potable water.14 Such marginalized groups tend to have little power, and therefore a human rights-based approach should be an important consideration in efforts to combat LF and other NTDs. Nigeria has ratified most international treaties and conventions that provide a framework for respecting these rights, such as the International Covenant on Economic, Social and Cultural Rights, the Convention on the Rights of Persons with Disabilities, and the African Charter on Human and Peoples’ Rights. Unfortunately, implementation has been very weak, making the realization of these rights a challenge for marginalized communities, including those with NTDs.
Thus, although previous studies from Nigeria have described the epidemiological and clinical characteristics of LF, the experiences of stigma, discrimination, and associated mental health challenges remain unclear for individuals living with this disease in Nigeria. A better understanding of such experiences is an important first step upon which to premise advocacy for a rights-based approach to address the identified problems. Our study sought to fill this gap. Specifically, it explored three aspects: (1) sociocultural perceptions and beliefs around LF, as experienced by persons affected by LF; (2) stigma experiences associated with LF, as well as the disease’s impact on daily functioning, including work, family and community life, and enjoyment of human rights; and (3) the emotional and mental health consequences of the disease, as well as the coping strategies used by persons living with LF.
Study methodology
Study setting
Our study was conducted in Plateau State, across the five sites of Jos, Nyes, Amper, Dadur, and Gwam Lar, which are a combination of urban and rural communities that are endemic for LF. The communities are agrarian, with high levels of poverty and limited access to health services and social amenities, including potable water. The Carter Centre, in partnership with the state government of Plateau, has organized them into catchment groups for the provision of treatment. Thus, they provided a readily available convenience sample for our study. We utilized this pre-existing organization into catchment areas to identify designated treatment clinics that are in close proximity to each community, where patients can receive wound management, antibiotics and anti-fungal creams (for infections), and analgesia (for pain relief).
Sampling and recruitment procedures
We used a combination of purposive and snowball sampling methods to recruit participants. We approached all individuals who presented at the designated clinics in each of the five communities on the specified medication collection days (following a month’s notice sent to them) and explained the study to them. All consenting patients were recruited and were also asked to nominate other individuals who might have useful information. We then approached these nominated individuals to encourage their participation as well. Efforts were made to ensure representativeness across gender and location (urban/rural). The inclusion criteria included a diagnosis of LF, the presence of lymphedema (with or without hydrocele), and an age of 18 years and above. Those who could neither understand nor speak English or the local Hausa languages were excluded. While most communities in north central Nigeria understand Hausa, they retain their specific ethnic identities and language, and a few may not understand the Hausa language.
Data collection methods
We employed three qualitative methods, with different strengths, to ensure comprehensive and in-depth coverage of the study objectives. In total, we conducted eight focus group discussions, six key informant interviews, and seven McGill Illness Narrative Interviews (MINIs).15 In addition to using a facilitator and note-taker at each session, we recorded the sessions using audio recording equipment. The key informant interviews provided in-depth but broad descriptions of the situation of persons living with LF, while the MINIs provided personalized insight into the lived experiences of those affected by LF. The focus group discussions aimed to achieve consensus from the respective groups about the experiences of affected persons.
Focus group discussions
We conducted eight focus group discussions, each of which included six to eight participants who were affected by LF according to the criteria above. Special care was taken to ensure relative homogeneity within each group (urban/rural and gender) in order to promote free conversation and enhance the chances of attaining consensus around issues of discussion. Each session began by introducing the topic and then initiated a discussion using a topic guide that was synthesized from previous research. The focus groups explored five broad themes: commonly held views about LF within the community; experiences of being treated differently (e.g., stigma and discrimination) on account of LF; emotional reactions to stigma and discrimination; experiences of support and encouragement; and what participants would like to see change for the better.
Key informant interviews
We conducted key informant interviews with six respondents across the five sites. These interviews were focused on gaining a deep understanding of the research issues from individuals with extensive experience and knowledge of the subject. One of the respondents did not have LF but had more than two decades of field experience and first-hand involvement caring for persons with LF in one of the clinics. The other five respondents had lived with LF for at least five years and were identified by their peers as very well informed. Indeed, three of these five were serving unofficially as volunteers to provide peer support to other affected persons. For this method, it was not critical to achieve a representative sample; rather, the purpose was to select persons who were identified as clearly knowledgeable and experienced with regard to LF in these communities.
McGill Illness Narrative Interviews
Persons identified either from the focus group discussions or via the snowball approach as having experienced significant stigma, life events, or psychological consequences as a result of their status as persons affected by LF were approached for the MINIs.16 The MINI is a qualitative interview schedule for investigating meanings and experiences related to a specific illness—in this case, LF. The interviewee is asked to talk about the health problem in terms of a timeline of events that explores causes, symptoms and signs, effects, and what the person did or is doing about the problem, including seeking care in the formal biomedical system or with non-biomedical healers. MINIs have been found to be culturally valid and have been previously utilized to explore experiences of perinatal depression in Nigeria.17
Data coding and analysis
We transcribed and translated into English the audiotapes of the interviews, paying special attention to removing mentions of people’s names and descriptions of specific individuals who may be identifiable from such descriptions. This task was performed by Samuel Dakwak, a clinical psychologist and a native Hausa speaker, and reviewed by Jibril Abdulmalik for accuracy. Back translation of randomly selected portions was performed by Abdulmalik to ensure that the meanings were retained.
The final transcript data was analyzed based on the qualitative content analysis method, using a sequential combination of deductive and inductive coding.18 Two experienced qualitative researchers (Jibril Abdulmalik and Motunrayo Ayobola) independently performed this. Both researchers subsequently harmonized their themes and reconciled areas of disagreement.
Specifically, the qualitative data coding and analysis entailed the following steps:
- A set of codes based on a previous review of the literature was prepared for use in interrogating the data (deductive coding).
- An initial read-through of all the transcripts was performed to gain a feel for the responses and important themes that were immediately striking (inductive coding). Aspects or concepts that were unclear necessitated listening to the audio tapes again to gain appropriate insight into the intended meanings of the participants.
- A thematic codebook was prepared as the final coding template for data analysis.
- The transcripts were uploaded into the Atlas.ti software, and the transcripts were read and assigned thematic codes and memos within the software.
- The software was utilized to pull, aggregate, and display salient quotations and segments for individual codes and themes.
Ethical considerations
We obtained ethical clearance from the Ethics and Research Committee of the University of Jos Teaching Hospital. Privacy and confidentiality were ensured for all participants in the interview settings, and these issues were discussed prior to conducting the interviews. Written informed consent was also obtained from the participants. Those of us who conducted the interviews are experienced mental health clinicians (a psychiatrist and a clinical psychologist, each with several years of clinical experience), and where we identified respondents who required psychological interventions, qualified professionals on our team provided the respondents with brief psychosocial support and then referred them for ongoing care at the University of Jos Teaching Hospital. Furthermore, all participants were screened for depression as part of an associated study evaluating the prevalence and correlates of depression, and which included the provision of treatment for identified persons.19 Any participants who screened positive for depression in that study were referred for follow-up care.
Results
Sociodemographic profile of respondents
Out of a total of 93 patients seen at the five sites, 69 respondents (74.2%) provided consent and were interviewed. Four respondents who provided consent were excluded due to language difficulties, while the others did not satisfy the inclusion criteria and were therefore excluded. The participants with language difficulties were unlikely to have different experiences of the illness, as they were living within their own communities and could speak their local dialects. While the qualitative methods employed do not demand large sample sizes, the high proportion of participants recruited for the study promoted the achievement of saturation for this sampled group, and the subsequent analysis of results confirmed this.20 There were slightly more female participants (37) than male ones (32). The age of the participants ranged from 20 to 80 years, with a mean age of 53.8 years (SD=15.93). The results are presented below following the outline of our research themes.
Community perceptions of LF
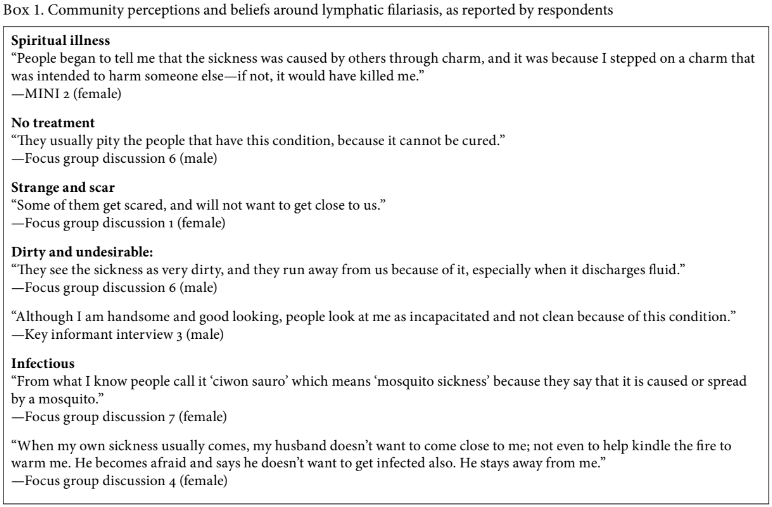
According to respondents, the most common belief about the cause of LF in their communities is that it is a spiritually inflicted illness that affects individuals who have stepped on a charm that was placed on the ground by their enemies. Thus, it is viewed with some apprehension, and community members wish to be far removed from affected individuals in order to reduce the chances of the charms somehow affecting them as well.
Other commonly expressed perceptions include views that LF is a strange, scary, and poorly understood illness; that affected persons are dirty and foul smelling; that it is an infectious condition caused by mosquitoes; and that it is an incurable disease (see Box 1).
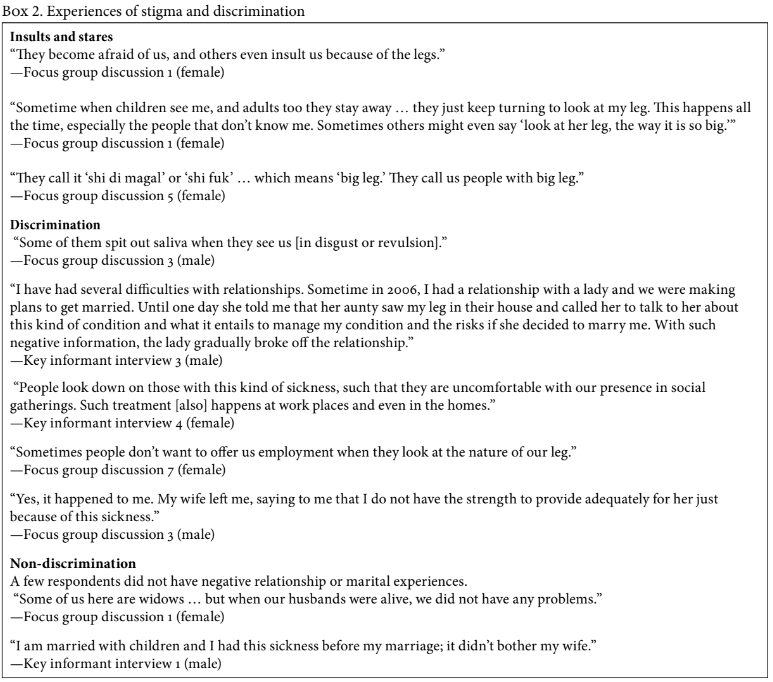
Experiences of stigma and discrimination
Nearly all respondents revealed personal experiences of stigma and discrimination that included being shunned, receiving embarrassing stares and insults, and being viewed as inferior on account of the disability. Social interactions—including the ability to find a marital partner, the quality of marital relationships, and participation in social events—were all negatively affected by the presence of LF for the majority of the respondents. These experiences, however, were directly linked to the severity of the illness, as individuals with minimal leg swellings could escape negative attention, unlike those with severe and disfiguring leg swellings (see Box 2).
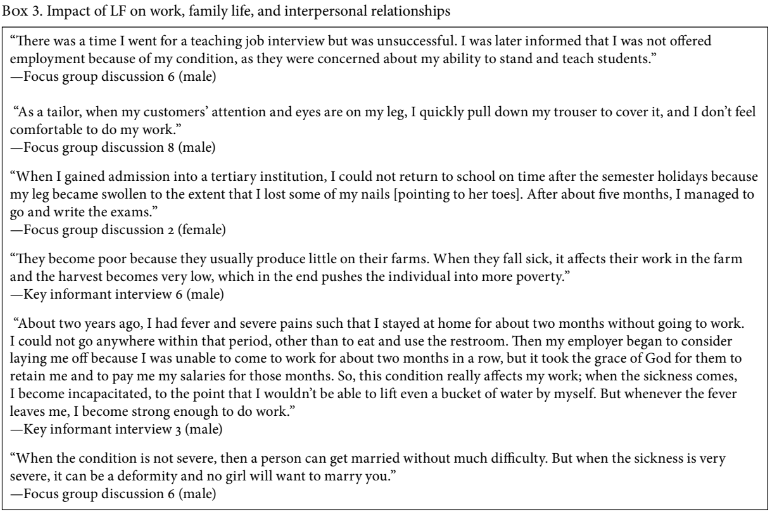
Impact of LF on work, family life, and interpersonal relationships
The presence of LF restricts affected individuals’ ability to obtain employment or perform optimally at work or in school. This is especially true during periods when the person suffers acute attacks characterized by debilitating pain and fever, which may last for weeks. Thus, the individual may be forced to miss long spells of school or work. Furthermore, those who are self-employed, such as craftspeople and traders, also notice that people stop buying from them once they see their swollen legs. However, a few respondents did not report a negative social impact, especially with respect to family life, as they enjoyed good support from their spouses, family members, and members of the community (see Box 3).
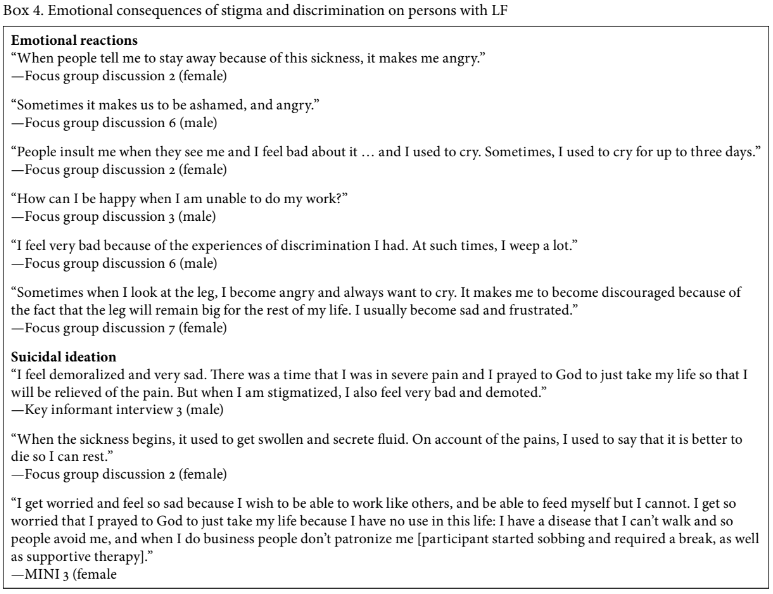
Emotional consequences of stigma and discrimination for persons with LF
The most commonly reported emotions were feelings of sadness, shame, and hopelessness on account of the negative life experiences. Other individuals experienced anger, frustration, worries, and suicidal ideations. These emotions were usually described as time bound—lasting for a few days or weeks—and most commonly occurring either in the aftermath of acute infections or following stigmatizing and discriminatory experiences (see Box 4).
Personal coping strategies and family and community support
Three broad categories of coping mechanisms emerged from the data: personal strategies, family support, and community support.
Personal strategies: Participants responded to their circumstances in a number of practical ways, including social withdrawal, in order to avoid awkward encounters and to avoid the need to wear long clothes that cover their feet, thus preventing stares. In addition, respondents reported a number of cultural rationalizations, such as resignation to fate and seeking solace in their faith in God. A few described turning to alcohol and drugs. Finally, some described their need to beg on the streets as a result of their lack of other economic opportunities.
“I have to dress and cover the leg well—if not, people will not want to be close to me.” —Focus group discussion 3 (male)
“It [LF] is the will of God. He can afflict anyone with sickness. So, I look up to God for help.” —Focus group discussion 5 (female)
Family: Support and encouragement from family members was also an important way for some respondents to cope.
“It was my family members that have been washing and dressing my wounds each morning during that period. In fact, our children were very happy for me and were even singing out of joy, when I eventually began walking with the aid of a walking stick after eight months of being bed-ridden. They were very happy for me.” —Focus group discussion 1 (female)
“I know my family supported me all the way and they encouraged me when I was going to the hospital, and they have been there for me in my condition. My family has been very supportive.”—Key informant interview 4 (female)
Community: Some respondents described being helped by their communities through support, encouragement, and financial aid. Religious bodies, especially women’s church groups, provided regular visits, prayers, emotional support, and financial contributions to individuals with LF.
“The women fellowship of my church and other people gave me money as a form of assistance because of this condition. And I used the money to go to the hospital.” —Key informant interview 5 (female)
“The people of my own village supported and encouraged me … It is only people that are not from our community that did not [support me].”—Focus group discussion 1 (female)
Respondents reported receiving free medications and general health counseling from the Carter Centre but were unaware of any governmental support at the local, state, or federal level for persons with LF.
The majority of respondents indicated that they had initially sought treatment from traditional healers—to no avail and often at considerable expense—before eventually arriving at the designated clinics where the Carter Centre provided free treatment services. The counseling services at these clinics were aimed at providing information about medications and general health care issues; there was no systematic or coordinated manner of identifying or providing interventions for emotional and other mental health difficulties experienced by individuals with LF.
Changes desired by persons with LF
The most pronounced wish of respondents was the discovery of a definitive solution for the physical disfigurement of their limbs so their lives could return to normal. Another recommendation was public awareness campaigns to increase the level of community understanding of LF and to reduce stigma and discrimination. Free and regularly available medications were also mentioned, as medications are sometimes either unavailable or available only for a fee. The respondents specifically requested opportunities to earn a livelihood and care for themselves independently. Given that they could no longer farm successfully, several respondents wanted the opportunity to receive government benefits such as supported employment, small loans to start a business, and other forms of welfare support. Such benefits are currently not available in Nigeria, apart from through charitable donations, which are not regular
Discussion
Perceptions of LF within communities
The perceptions of LF reported by respondents reflected a mix of accurate information (such as knowledge that LF is an infection that may be transmitted by mosquitoes) and inaccurate information (such as the belief that it is a spiritual illness caused by “enemies”). This is in line with earlier reports from developing countries.21 The pervasive nature of misconceptions about the causative mechanism for LF may have a negative impact on the effectiveness of prevention and eradication efforts. However, it is salient to note the overlap between the perception of LF as a form of spiritual affliction that can spread to others and the biomedical fact that it is an infectious condition that can be transmitted among people living in close proximity. This link may be exploited in public awareness campaigns.
Stigma experiences and impact on functioning
A central theme from our study’s results is respondents’ overwhelmingly negative experiences of stigma and discrimination. Similar findings have also been reported for other NTDs, such as leprosy, which also has physical and cutaneous signs that are strongly associated with stigma and poor mental health outcomes.22
The social exclusion experienced by respondents resulted in high levels of disability, as many of them could not complete their education, secure employment, hold down jobs, engage in farming, or engage in business. These findings agree with earlier reports about the psychosocial consequences for persons with LF from low- and middle-income countries.23 Indeed, another study illustrated how stigma and disability from LF not only resulted in social isolation and avoidance behavior (linked to self-stigma) but also led to reduced career aspirations and a downward spiral into poverty.24
Another salient finding was the association between increased levels of stigma and the severity of the disease—those with minimal swellings managed to get by with as near normal lives as possible, while those with more severe disability were unable to hide their condition and had more negative experiences in their social interactions. A recent study reported a similar observation about this association.25 Enacted stigma is more pronounced with greater severity of the disease and obvious physical deformities. This, in turn, can exacerbate the felt stigma of affected individuals.26
However, it is pertinent to note that some respondents had positive stories of spousal, family, and community support, which greatly enhanced their ability to cope. This positive finding in the face of widespread stigma has also been reported by previous studies.27 Other coping strategies were both negative and positive. Examples of negative coping strategies were social withdrawal and isolation, street begging, and resorting to alcohol and drugs. The positive coping styles of resignation to fate, drawing comfort from religious beliefs, and use of loose clothing that covers the legs and feet demonstrate adaptation to the challenging realities faced in everyday life. These coping strategies hold promise for future research efforts aimed at developing simple psychological interventions to counter stigma. Such efforts are much more effective if they take cultural beliefs into account. Furthermore, a multimodal approach that looks at individual factors as well as community and other contextual factors is more likely to be effective.28
Emotional consequences
The most common emotional reactions were suggestive of anxiety and depressive illness. A subset of this project with the same study population utilized standardized assessment instruments and found a 20% prevalence of depression in this population, which is high compared with the lifetime prevalence of 3.2% in the country’s general population.29 The presence of depressive symptoms in this study was also associated with expressions of suicidal ideation (but there were no reported suicidal attempts in this study). These findings are supported by the high prevalence of depression reported among individuals with LF from other studies, estimated at 70% in Togo and 97% in India.30
A recent review highlighted the extent of co-morbid mental illnesses among persons with NTDs such as LF. This is supported by a report which clearly illustrate how the experiences of stigma and discrimination, as well as other attendant social disadvantages among persons with NTDs (including LF), predispose them to mental health problems.31 Furthermore, while the initial burden of disability-adjusted life years (DALYs) attributed to LF (taking account of physical disabilities only) in the Global Burden of Disease Study of 2010 was estimated at 2.78 million DALYs, a more recent calculation of the attributable burden due to depressive illness alone among persons with LF puts the figure at about 5.09 million DALYs.32 This doubling of the attributable burden of disease has important consequences for public health planning and resource prioritization. It is also worthy to note that the significant caregiver burden and impact on families as illustrated by our study results are often not captured in attributable disease burden calculations. The emotional toll and its resultant burden on these individuals and their communities deserve attention and urgent intervention—especially since the physical disfigurement, once established, is usually lifelong.
Using a human rights-based approach
The association between LF (and other NTDs) and poverty and social disadvantage—such as difficulties with access to health, education, and employment—has been reported elsewhere.33 Our findings support these observations: respondents reported difficulties in accessing their rights to health, education, and work, as well as meaningfully participating in their communities.34 Their relative lack of power means that there are few opportunities for them to engage in democratic processes to advocate for their rights.
While the government of Nigeria has ratified several pertinent international conventions, such as the International Covenant on Economic, Social and Cultural Rights and the Convention on the Rights of Persons with Disabilities, these instruments lack legislative muscle since they have not been domesticated by the National Assembly. Indeed, section 12(1) of the Nigerian Constitution states that “[n]o treaty between the Federation and other countries shall have the force of law except to the extent to which any such treaty has been enacted into law by the National Assembly.”35 People affected by NTDs are poorly represented in the national disability federation (the Joint National Association of Persons With Disabilities), which has a mandate to engage in reporting under the Convention on the Rights of Persons with Disabilities.
A holistic approach to addressing the individual and structural discrimination faced by affected persons and their communities entails domesticating relevant legal instruments in order to guarantee and protect these persons’ rights as enshrined in international and regional law.
The SDGs also provide opportunities for promoting the rights of persons with LF in Nigeria and reducing their experiences of stigma, discrimination, and social exclusion. As stated earlier, one overarching principle of the SDGs is a commitment to “leave no one behind”, which might be achieved through the application of Universal Health Coverage, without financial hardships.36 Considering that LF and other NTDs are most prevalent in poor populations, the success or failure of the universal health coverage paradigm within the SDGs can be measured against the extent of its effectiveness in reaching persons with NTDs.37 In specific terms, SDGs 1, 2, 3, 4, 6, 10, and 16 lend themselves to the cause of promoting the human rights of persons with LF and other NTDs in Nigeria and elsewhere.38
SDG 1 aims to end poverty in all its forms, which stands to have an impact on the vulnerable population of persons (and their families) living with LF and other NTDs. Indeed, it has been proposed that LF is simultaneously an outcome and a driver of poverty.39 SDG 2 aspires to “end hunger, achieve food security and improve nutrition and promote sustainable agriculture”; this is directly relevant to the Nigerian communities where LF is endemic, such as our study population. Participants were mainly farmers, and even those who had other vocations still maintained family farms on a subsistence basis. Episodes of painful infections of their limbs frequently interfered with their farming activities, resulting in reduced agricultural production and worsening food security while pushing them into poverty.
SDG 3 aims to achieve health for all, including persons with NTDs. SDG 4 aspires to achieve inclusive and equitable quality education and promote lifelong learning opportunities for all. This is particularly relevant for our study’s participants, who described how their experience with LF had disrupted their educational pursuits, particularly during episodes of acute and painful infections. SDG 6 focuses on ensuring the availability and sustainable management of water and sanitation for all, which is pertinent for all persons with NTDs.
Lastly, SDGs 10 and 16 have clear human rights implications for persons with LF and other NTDs and should be utilized to advocate for their rights. Goal 10 calls for addressing inequalities; here, the majority of affected persons are the rural poor, whose needs are often not prioritized. Reducing inequalities should translate into an improvement in their status in society and an overall reduction in their experience of stigma. Goal 16 calls on governments to “promote peaceful and inclusive societies for sustainable development, provide access to justice for all and build effective, accountable and inclusive institutions at all levels.” Ensuring the inclusion of persons with LF and other NTDs in Nigeria will necessarily cut across several areas, including health care, social services, economic empowerment, and community participation. Health sector inclusiveness will entail not only the provision of physical therapies and interventions but also support for their mental health needs.
In order to achieve this health sector inclusiveness, the Nigerian government needs to provide training for health workers that allows them to identify and provide interventions for mental health problems among persons with LF and other NTDs. This could be via improvements in the integration of mental health into primary health care services (mental health is the ninth pillar of primary care in Nigeria). The World Health Organization’s Mental Health Gap Action Programme Intervention Guide, which has been contextualized and piloted in Nigeria, provides a useful manual for this implementation.40 In addition, the World Health Organization’s QualityRights program, focused on realizing meaningful access to rights in mental health services, has also been piloted in Nigeria.41 These and other resources can support the development of self-help groups that can advocate for their rights. Such groups may play a role in expanding community education and outreach programs to improve individuals’ knowledge and reduce stigma and discrimination. In addition, these groups also play a role in advocacy for the protection and promotion of their rights by the government.
Lastly, it is clear that current efforts to tackle LF and other NTDs—which are focused predominantly on mass drug administration for the prevention of disease transmission—neglect important associated rights (including the right to physical and mental health care, the right to live and participate fully in community life, and the right to education) of people affected by NTDs. The SDGs provide opportunities to advance the cause of persons living with LF and other NTDs through their commitment to Universal Health Coverage, which ensures that all populations, including those living with NTDs, have access to health care.
Conclusion
Given the pervasive stigma and discrimination experienced by persons affected by LF, and the associated emotional consequences, interventions that address stigma and the psychosocial consequences of this condition must be considered an essential component of LF-related services. Such interventions can be supported through the enactment of a legislative framework that promotes and protects the human rights of affected citizens. The training of health workers, the provision of accessible services via primary care, and public education campaigns are additional steps that can be taken by the government and civil society organizations alike.
The screening, identification, and treatment of mental health needs, as well as social and economic inclusion, should gain prominence as rights-based considerations during policy discussions on contemporary challenges for LF in particular and NTDs in general.
Acknowledgments
The authors acknowledge the support of the Health and Development Support Programme and the Carter Center, which provided access to their programs in Nigeria. We also gratefully acknowledge the contribution of Toyin Aderemi of CBM’s country office in Nigeria to the success of this project.
Jibril Abdulmalik is a senior lecturer at the Department of Psychiatry, University of Ibadan, Nigeria.
Emeka Nwefoh is mental health advisor at the CBM Country Co-ordination Office, Abuja, Nigeria.
James Obindo is an associate professor at the Department of Psychiatry, University of Jos, Nigeria.
Samuel Dakwak is a lecturer at the department of General and Applied Psychology, University of Jos, Nigeria.
Motunrayo Ayobola is a doctoral student at the Department of Sociology, University of Ibadan, Nigeria.
John Umaru is deputy director for Plateau/Nassarawa States Integrated Health Programmes at the Carter Centre, Jos, Nigeria.
Elisha Samuel is administrative and human resources manager at the Health and Development Support Programme, Jos, Nigeria.
Christopher Ogoshi is Programme Coordinator at the Health and Development Support Programme, Jos, Nigeria.
Julian Eaton is Senior Mental Health Advisor at CBM International and Assistant Professor at London School of Hygiene and Tropical Medicine, UK.
Please address correspondence to Jibril Abdulmalik. Email: jfutprints@yahoo.com.
Competing interests: None declared.
Copyright © 2018 Abdulmalik, Nwefoh, Obindo, Dakwak, Ayobola, Umaru, Samuel, Ogoshi, and Eaton. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- World Health Organization, Working to overcome the global impact of neglected tropical diseases (Geneva: WHO, 2010).
- World Health Organization, Managing morbidity and preventing disability in the Global Programme to Eliminate Lymphatic Filariasis: WHO position statement (Geneva: WHO, 2011).
- M. Zeldenryk, M. Gray, R. Speare, et al., “The emerging story of disability associated with lymphatic filariasis: A critical review,” PLoS Neglected Tropical Diseases 5/12 (2011).
- World Health Organization, Global Programme to Eliminate Lymphatic Filariasis: Progress report 2000–2009 and strategic plan 2010–2020 (Geneva: WHO, 2010).
- N. Okorie, G. O. Ademowo, Y. Saka, et al., “Lymphatic filariasis in Nigeria: Micro-stratification overlap mapping (MOM) as a prerequisite for cost-effective resource utilization in control and surveillance,” PLoS Neglected Tropical Diseases 7/9 (2013); C. Okonofua, O. Morenikeji, and O. Salawu, “Lymphatic filariasis and associated morbidities in rural communities of Ogun State, Southwestern Nigeria,” Travel Medicine and Infectious Disease 12/1 (2014), pp. 95–101; E. A. Omudu and J. O. Ochoga, “Clinical epidemiology of lymphatic filariasis and community practices and perceptions amongst the Ado people of Benue State, Nigeria,” African Journalof Infectious Diseases 5/2 (2011), pp. 47–53.
- Brady, “Seventh meeting of the Global Alliance to Eliminate Lymphatic Filariasis: Reaching the vision by scaling up, scaling down, and reaching out,” Parasites and Vectors 7/46 (2014).
- Eigege, D. S. Evans, G. S. Noland, et al. “Criteria to stop mass drug administration for lymphatic filariasishave been achieved throughout Plateau and Nasarawa States, Nigeria,” American Journal of Tropical Medicine and Hygiene 97/3 (2017), pp. 677–680.
- K. Kumari, K. T. Harichandrakumar, L. K. Das, and K. Krishnamoorthy, “Physical and psychological burden due to lymphatic filariasis as perceived by patients and medical experts,” Tropical Medicine and International Health 10/6 (2005), pp. 567–573; C. K. Ahorlu, S. K. Dunyo, G. Asamoah, and P. E. Simonsen, “Consequences of hydrocele and the benefits of hydrocelectomy: A qualitative study in lymphatic filariasis endemic communities on the coast of Ghana,” Acta Tropica 80/3 (2001), pp. 215–221; R. S. Wijesinghe, A. R. Wickremasinghe, S. Ekanayake, and M. S. Perera, “Physical disability and psychosocial impact due to chronic filarial lymphoedema in Sri Lanka,” Filaria Journal 6/4 (2007)
- Goffman, Stigma: Notes on the management of spoiled identity (Harmondsworth, Middlesex: Penguin Books, 1963); G. Scambler, “Stigma and disease: Changing paradigms,” Lancet 352/9133 (1988), pp. 1054–1055.
- Thornicroft, D. Rose, A. Kassam, and N. Sartorius, “Stigma: Ignorance, prejudice or discrimination?,” British Journal of Psychiatry 190/3 (2007), pp. 192–193.
- Zeldenryk et al. (see note 3); T. Cassidy, C. M. Worrell, K. Little, et al., “Experiences of a community-based lymphedema management program for lymphatic filariasis in Odisha State, India: An analysis of focus group discussions with patients, families, community members and program volunteers,” Plos Neglected Tropical Diseases 10/2 (2016); K. Hofstraat and W. H. van Brakel, “Social stigma towards neglected tropical diseases: A systematic review,” International Health 8 (2016), pp. i53–i70; M. G. Weiss, “Stigma: Formulating concepts and priorities for a public health agenda,” Tropical Medicine and International Health 12 (2007), p. 17; B. Person, L. K. Bartholomew, M. Gyapong, D. G. Addiss, and B. van den Borne, “Health-related stigma among women with lymphatic filariasis from the Dominican Republic and Ghana,” Social Science and Medicine 68/1 (2009), pp. 30–38.
- G. N. Ton, C. Mackenzie, and D. H. Molyneux, “The burden of mental health in lymphatic filariasis,” Infectious Diseases of Poverty 4 (2015), p. 34.
- Litt, M. C. Baker, and D. Molyneux, “Neglected tropical diseases and mental health: A perspective on comorbidity,” Trends in Parasitology 28/5 (2012), pp. 195–201; K. T. Harichandrakumar and M. Kumaran, “Health related quality of life (HRQoL) among patients with lymphatic filariasis,” International Journal of Health Sciences and Research 7/3 (2017), pp. 256–268.
- World Health Organization, Working to overcome the global impact of neglected tropical diseases: First WHO report on neglected tropical diseases (Geneva: WHO, 2010); P. J. Hotez, A. Fenwick, L. Savioli, and D. H. Molyneux, “Rescuing the bottom billion through control of neglected tropical diseases,” Lancet 373/9674 (2009), pp. 1570–1575; J. Sun and J. Amon, “Addressing inequity: Neglected tropical diseases and human rights,” Health and Human Rights Journal 20/1 (2018).
- Groleau, A. Young, and L. J. Kirmayer, “The McGill Illness Narrative Interview (MINI): An interview schedule to elicit meanings and modes of reasoning related to illness experience,” Transcultural Psychiatry 43/4 (2006), pp. 671–691.
- Adeponle, D. Groleau, L. Kola, et al., “Perinatal depression in Nigeria: Perspectives of women, family caregivers and health care providers,” International Journal of Mental Health Systems(2017).
- Y. Cho and E. Lee, “Reducing confusion about grounded theory and qualitative content analysis: Similarities and differences,” Qualitative Report 19/64 (2014), pp. 1–20.
- Obindo, J. Abdulmalik, E. Nwefoh, et al., “Prevalence of depression and associated clinical and socio-demographic factors in people living with lymphatic filariasis in Plateau State, Nigeria,” PLoS Neglected Tropical Diseases 11/6 (2017).
- A. Bowen, “Naturalistic inquiry and the saturation concept: A research note,” Qualitative Research 8 (2008), p. 137.
- V. Babu, S. Mishra, and A. N. Nayak, “Marriage, sex, and hydrocele: An ethnographic study on the effect of filarial hydrocele on conjugal life and marriageability from Orissa, India,” PLoS Neglected Tropical Diseases 3/4 (2009), p. e414; A. Tsutsumi, T. Izutsu, A. M. Islam, et al., “The quality of life, mental health, and perceived stigma of leprosy patients in Bangladesh,” Social Science and Medicine 64/12 (2007), pp. 2443–2453; Ahorlu et al. (2001, see note 8).
- Tsutsumi et al. (see note 21).
- Person, D. Addiss, L. K. Bartholomew, et al., “Can it be that god does not remember me: A qualitative study on the psychological distress, suffering, and coping of Dominican women with chronic filarial lymphedema and elephantiasis of the leg,” Health Care for Women International 29/4 (2008), pp. 349–365; M. Gyapong, J. O. Gyapong, S. Adjei, et al., “Filariasis in northern Ghana: Some cultural beliefs and practices and their implications for disease control,” Social Science and Medicine 43/2 (1996), pp. 235–242; C. K. Ahorlu, S. K. Dunyo, K. A. Koram, et al., “Lymphatic filariasis related perceptions and practices on the coast of Ghana: Implications for prevention and control,” Acta Tropica 73/3 (1999), pp. 251–261; Kumari et al. (see note 8); M. Perera, M. Whitehead, D. Molyneux, et al., “Neglected patients with a neglected disease? A qualitative study of lymphatic filariasis,” PLoS Neglected Tropical Diseases 1/2 (2007), p. e128; J. Coreil, G. Mayard, J. Louis-Charles, and D. Addiss, “Filarial elephantiasis among Haitian women: Social context and behavioural factors in treatment,” Tropical Medicine and International Health 3/6 (1998), pp. 467–473; M. G. Weiss, “Stigma and the social burden of neglected tropical diseases,” PLoS Neglected Tropical Diseases 2/5 (2008), p. e237.
- Perera et al. (see note 23).
- Kumari et al. (see note 8).
- Scambler (see note 9).
- Gyapong et al. (see note 23); Ahorlu et al. (1999, see note 23); Coreil et al. (see note 23).
- Weiss (2008, see note 23).
- Obindo et al. (see note 19); R. C. Kessler, N. A. Sampson, P. Berglund, et al., “Anxious and non-anxious major depressive disorder in the World Health Organization World Mental Health Surveys,” Epidemiology and Psychiatric Sciences 24/3 (2015), pp. 210–226.
- A. Richard, E. Mathieu, D. G. Addiss, and Y. K. Sodahlon, “A survey of treatment practices and burden of lymphoedema in Togo,” Transactions of the Royal Society of Tropical Medicine and Hygiene 101 (2007), pp. 391–397; Constitution of the Federal Republic of Nigeria (1999).
- Litt et al. (see note 13).
- Ton et al. (see note 12).
- World Health Organization (2010, see note 14); Hotez et al. (see note 14); Sun and Amon (see note 14).
- Sun and Amon (see note 14).
- K. Suma, R. K. Shenoy, and V. Kumaraswami, “A qualitative study of the perceptions, practices and socio-psychological suffering related to chronic brugian filariasis in Kerala, southern India,” Annals of Tropical Medicine and Parasitology 97/8 (2003), pp. 839–845.
- World Health Organization, Fourth WHO report on neglected tropical diseases: Integrating neglected tropical diseases into global health and development (Geneva: WHO, 2017).
- Fürst, P. Salari, L. M. Llamas, et al., “Global health policy and neglected tropical diseases: Then, now, and in the years to come,” PLoS Neglected Tropical Diseases
- N. Durrheim, S. Wynd, B. Liese, and J. O. Gyapong, “Lymphatic filariasis endemicity—an indicator of poverty?” Tropical Medicine and International Health 9 (2004), pp. 843–845.
- Abdulmalik, L. Kola, W. Fadahunsi, et al., “Country contextualization of the mental health gap action programme intervention guide: A case study from Nigeria,” PLoS Med. 10/8 (2013), p. e1001501; O. Gureje, J. Abdulmalik, L. Kola, et al., “Integrating mental health into primary care in Nigeria: Report of a demonstration project using the mental health gap action programme intervention guide,” BMC Health Services Research 15 (2015).
- Abdulmalik et al. (see note 39); Gureje et al. (see note 39).
- World Health Organization, QualityRights tool kit to assess and improve quality and human rights in mental health and social care facilities (Geneva: WHO, 2012).