EDITORIAL Health in the Courts of Latin America
Octávio Luiz Motta Ferraz
To address any complex issue in a large and diverse geographical region of the world is always a daunting and risky task. Latin America is no exception. Despite the semblance of uniformity that the use of the term “Latin American” often misleadingly imparts, the truth is that there is no such thing as a homogeneous bloc of countries occupying the territory running from the border between the United States and Mexico down to Uruguay, plus a few islands in the Caribbean Sea. Not even a single language is shared, let alone a broader “Latin American culture.”
We are dealing with a large region spanning 20 million square kilometers (13% of the earth’s land surface), including very poor countries such as Haiti, middle-income ones such as Peru, Colombia, and Brazil, and relatively wealthy ones such as Uruguay and Argentina. There are democracies at different levels of maturity and stability alongside authoritarian regimes, as well as a diverse range of political-economic systems, from socialist Cuba to economically liberal Chile.[1] Health systems also vary significantly in their structures (from national health services in Brazil to social security and public insurance schemes in Mexico and Colombia), coverage, and quality. As an influential historian has recently claimed, the idea of Latin America should have probably vanished by now. But he also acknowledges that “[t]he term is here to stay, and it is important.”[2]
The topic addressed in this special section—the judicial enforcement of health rights—inevitably reflects this remarkable diversity. Despite some interesting common trends, no “Latin American model” of health litigation emerges, unsurprisingly, from the growing but still limited studies of the past few decades (including those published in this issue). On the contrary, there is significant variety in terms of the magnitude of the phenomenon, its main characteristics, its potential causes, the impact it has on equity and health systems, and the emerging initiatives in reaction to the phenomenon.
Why Latin America?
What seems to unite many in Latin America and beyond is the perception that health litigation is particularly acute and often problematic in the region. Concern with the rise of health litigation is of course not unique to Latin America, but some of the traditional worries about judges interfering in the realm of public policy seem more intense in that region. This is due largely to what some describe as an “explosion” of litigation experienced in some of the region’s countries (thousands of cases in Costa Rica, and hundreds of thousands in Colombia and Brazil) and a heightened disposition of judges to enforce the right to health through strong remedies in comparison to non-Latin American countries.[3]
Studying judicialization in Latin America therefore seems to provide an ideal opportunity for us to extract broader lessons about this growing phenomenon, which is affecting an increasing number of countries throughout the world.[4]
Yet the literature on the topic, both in Latin American languages and in English, though growing, is still rather limited and, additionally, beset by the lack of a clear analytical framework to guide us in identifying the salient issues in need of empirical research and in drawing more robust conclusions that may assist in potential reform if and where it is needed.
The inspiration for this special section was the desire to enhance the body of research dedicated to understanding the phenomenon of health litigation as it relates to both of these aspects—in other words, not only regarding the specific knowledge about what goes on in specific countries but also with regard to refining our analytical framework to assess the phenomenon wherever it occurs.
The importance of context and empirical data
Right to health litigation has attracted the attention of scholars, policy makers, politicians, and the general public for two interrelated reasons. Both have to do with the involvement of the courts in the realm of public policy in general and health policy in particular. The first relates to what we might call the democratic legitimacy of that involvement and pits those who see it as always inappropriate—a frontal breach of the principle of separation of powers—against those for whom the very recognition of health as a legal right, especially when done through the constitution, automatically legitimizes the participation of courts.[5] The latter disagree among themselves, however, about the exact manner in which courts ought to intervene, with proposals ranging from more deferential and procedural approaches to more assertive and substantive ones.[6] The second line of reasoning has to do with what actually happens when courts interfere—that is, the impacts, good or bad, of judicialization. Some have drawn attention to the potentially negative effects of judicial involvement, such as distortions of rational health policies and the worsening of health inequities.[7] Others have stressed the role that judicialization can play in enhancing state accountability and citizens’ participation, especially in the health systems of countries where democratic control is weaker.[8]
I believe that the effects of right to health litigation, as with any complex phenomenon, can be both positive and negative and are likely to vary significantly from country to country. The legitimacy of courts’ involvement in health policy is also strongly dependent, in my view, on highly contextual factors related to the operation of courts (including the impacts of judicialization) and, more broadly, the structure and operation of the political and health systems of particular countries. The legitimacy question therefore cannot be settled in isolation from these empirical and contextual factors as if it were a matter of pure normative theory—that is, of determining the correct meaning of the principle of separation of powers.[9]
Latin America illustrates this point nicely. It seems increasingly clear from emerging empirical data that the judicialization of health in different Latin American countries reveals quite different pictures concerning both legitimacy and impacts. Take, for instance, Costa Rica and Brazil. We know that in both countries claims for medicines make up a large proportion of right to health litigation, that these claims are overwhelmingly individual in nature, that courts are very receptive (in other words, the success rates are quite high), and that a significant proportion of these medicines are not incorporated into the public health system, often for not passing mainstream priority-setting criteria.[10] Yet it would be a mistake to jump to the conclusion that, in both places, judicialization is therefore mostly illegitimate and produces largely negative impacts.
We need to know much more about each of these countries to build a comprehensive picture of judicialization—and once we have that, important differences are likely to emerge. Moreover, such differences may (I would even say are likely to) lead to different conclusions about the legitimacy and impacts of judicialization in these countries.
A few brief examples may help us here. Whereas in Costa Rica anyone can petition the Sala IV (the chamber of the Supreme Court that deals with right to health litigation) directly and without the need to be represented by a lawyer, in Brazil legal representation is compulsory: cases must start in local courts and can go all the way up to the Supreme Federal Tribunal, the fourth and last instance of the judicial system, in a lengthy and costly process. These differences in the judicial system are likely to result in easier access to courts in Costa Rica, which, in turn, will likely affect the socioeconomic profile of claimants, or those who benefit directly from successful litigation.
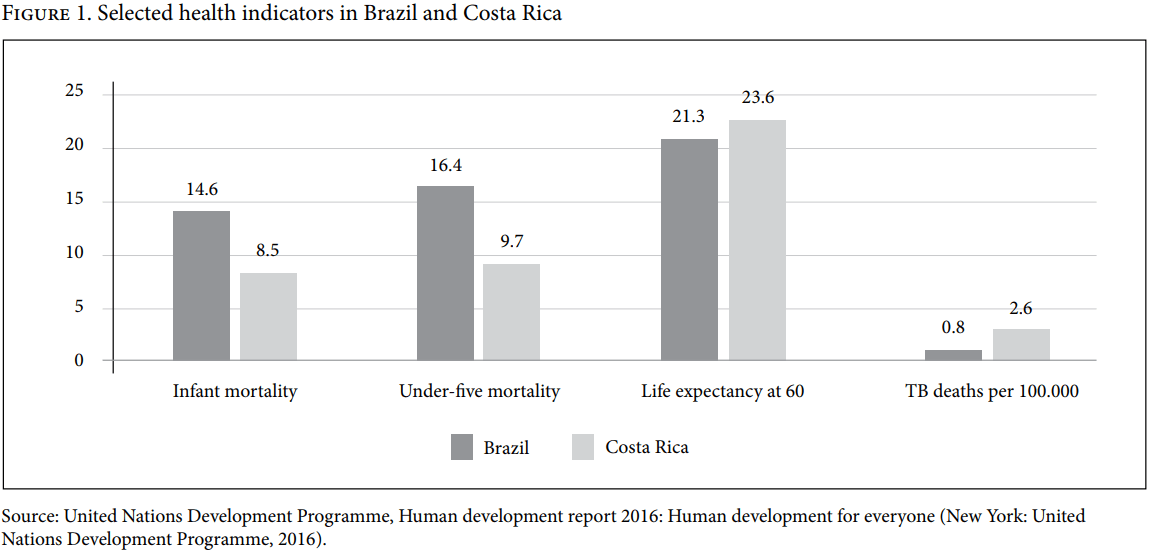
Other important differences related to the operation of the health system seem relevant. As empirical data show, Costa Rica displays a strong commitment, at least in comparative terms, to the funding of its health system. Government health expenditure is consistently around 7% of the gross domestic product (GDP), almost double the upper-middle-income country average. In per capita terms, this amounts to almost US$1,000 (in terms of purchasing power parity), which is more than two-and-a-half times the upper-middle-income country average and one-and-a-half times the global average. As a result, out-of-pocket expenditure is low and private health insurance plays a very small role, about 1% of total health sector financing, which is much lower than the upper-middle-income country average of 7% and the global average of 15%.[11] In Brazil, despite the constitutional recognition of health as a fundamental right (in contrast to Costa Rica) and the largest state-funded national health service in the world in terms of beneficiaries (the Unified Health System), the funding commitment is much weaker. Government health expenditure barely reaches 4% of GDP, amounting to around US$400 in per capita terms, significantly lower than Costa Rica.[12] Given such funding disparities, it is not surprising that Costa Rica’s public health system is much more comprehensive than that of Brazil, despite the fact that both are upper-middle-income countries with similar levels of wealth (both around US$14,000 GDP per capita). It is plausible to assume that the greater comprehensiveness of Costa Rica’s health system is partly responsible for the better health of the Costa Rican population. Brazil is indeed well behind Costa Rica in many important health indicators, as illustrated in Figure 1.
Differences in the operation of the health system, such as those just highlighted, are also relevant for a comprehensive and robust analysis and assessment of the legitimacy and impacts of right to health litigation in specific countries. As Olman Rodríguez Loaiza, Sigrid Morales, Ole Frithjof Norheim, and Bruce M. Wilson plausibly claim in their paper in this special issue, given Costa Rica’s reasonably well-funded, comprehensive, and well-functioning health system, it seems difficult to conclude that the high volume of right to health litigation in that country is “a response to an ineffectual, inefficient health care system.” But the same hypothesis cannot be discarded so easily in Brazil and other countries.
These are just two brief examples of how variables in the structure and operation of the judicial and health systems of different countries will likely affect the analysis and assessment of the legitimacy and impacts of the judicialization of health. Even within the same country, especially if it is large and diverse (Brazil immediately comes to mind), the judicialization of health is likely to display different characteristics across subnational regions.[13]
Which data are relevant?
The still limited but growing number of in-depth studies of countries and regions within countries, especially those with reliable empirical data, are very important for those pursuing a better understanding of the judicialization of health. Some of the papers in this special issue add to this welcome trend. Loaiza et al.’s contribution analyzes all 98 successful medication cases filed in Costa Rica in 2016 in light of priority-setting criteria from the public health literature on the topic. According to these criteria—which combine severity of the health condition, effectiveness, and cost-effectiveness—medication (or any other health intervention) can be classified into four priority groups: high, medium, low, and experimental. They find that 62% of the successful cases fall into groups that the public health literature would consider of clearly low priority—that is, low-priority (53%) and experimental drugs (9%). Another interesting finding of their study is that these medications share some common characteristics: “they are new on the market, have a very high cost compared to their benefits (often 3–5 times Costa Rica’s GDP per capita), target severe conditions such as cancer or rare diseases, and are similarly disputed in countries with much higher levels of health care spending (such as the UK and Norway).”
Lucía Berro Pizzarossa, Katrina Perehudoff, and José Castela Forte’s article on Uruguay is another important and welcome contribution along similar lines, and on a country that has featured much less in the literature than some of its counterparts. They look at a sample of 42 judicial claims (amparos) for medicines decided in Uruguay in 2015. As also found in studies in Brazil, Colombia, and Costa Rica, the success rate in these claims was high (74%), as was the percentage of claims for “off-formulary” drugs (drugs not incorporated into the medicines lists of the Uruguayan health system). Although they do not perform the same analysis of priority carried out by Loaiza et al., they do report that in at least eight claims (19% of their sample), drugs assessed and rejected by the Uruguayan health system as cost-ineffective (namely cetuximab, lenalidomide, and sorafenib) were nonetheless granted by the courts. These and another three drugs in the ten most claimed and granted in Uruguayan courts (abiraterone, ibrutinib, and TDM1–trastuzumab) are also in Loaiza et al.’s Costa Rican study. The first five are classified as low priority, and the last as medium priority.
The analytical framework of these two studies reveals a promising way forward in our quest to better understand judicialization’s legitimacy and impacts. Knowing exactly what health benefits are claimed in court, whether they are part of the health package offered in the country, and how they rank in terms of priority-setting criteria is an essential precondition for a solid analysis of the phenomenon. It would be very welcome if future studies from other countries experiencing high levels of health litigation collected such data.
Both studies reach plausible conclusions about the potential negative effects of court orders that grant off-formulary and low-priority interventions. Loaiza et al. highlight two: (1) it may become more difficult for the health system to negotiate price reductions, and (2) individuals suffering from similar conditions may receive unequal treatment if judicial orders end up benefiting only those who go to court. Pizzarossa et al. emphasize this second risk further: “successful plaintiffs inevitably receive and consume more health system resources than those who do not seek treatment through the courts.”
But it is also important to be aware of the limitations of this analytical framework. It provides merely a crucial starting point for discussion, not a final verdict of the legitimacy and impacts of judicialization. As Loaiza et al. appropriately warn, their suggested priority-setting criteria is not a “gold standard.” Although there is growing consensus in the literature about what should be taken into consideration when setting priority in health (such as the severity of the condition, effectiveness of treatment, and cost-effectiveness of treatment), “reasonable people may disagree on their relative weight and on the classification of new medications.”
This brings up what is perhaps the most difficult obstacle in the effort to find an appropriate framework to evaluate the legitimacy and impacts of judicialization. When disagreement about priority setting is rife, as it tends to be in most complex fields —and health is certainly one of them—how to determine the correctness of specific priority-setting decisions?[14] This is fundamentally what judges are being called on to do in all these cases in Costa Rica, Uruguay, and other countries where plaintiffs challenge the health system’s refusal to provide them with a certain health benefit. If we accept, as I think we must, that disagreement is bound to happen in many cases, then the question becomes whether and how courts should interfere with the decisions made by the public authorities in charge of running the health system on behalf of the population.
This is, of course, the perennial and intractable issue raised by courts’ increasing involvement in social policy that I mentioned earlier. All other contributions to this special issue grapple with it from different and interesting perspectives.
What role for courts?
The difficulty—or impossibility in the view of many—is thus to define the exact content of the right to health in terms of the specific health benefits individuals are entitled to under conditions of resource limitation and disagreement about priority-setting criteria. Should the courts get involved? If so, how?
Christopher Newdick and Keith Syrett have both been grappling with these questions for a long time and have already made seminal contributions to the debate.[15] In their papers in this issue, they explore innovative frameworks and approaches to their longstanding concerns about judicialization.
Newdick’s paper starts with a bleak warning. If we thought that setting priorities in health was an intractable task, it is going to become even harder in the future. This is due to pressures on both sides of the equation: fewer resources due to diminishing revenue-raising capacity of states under the grips of austerity and increasing health needs due to higher longevity and chronic illnesses among populations. In such a context, he argues, judges will be called on even more often to resolve the intensifying distributive tensions that are likely to arise. His aim is not to present a solution but rather to offer what he calls a “resource allocation rights matrix” to assist in the debate. The matrix combines two core dichotomies (individual versus community rights and substantive versus procedural remedies) to produce four possible conceptions of the right to health and corresponding remedies: community rights and procedural remedies; individual rights and procedural remedies; community rights and substantive remedies; and individual rights and substantive remedies. Given the inescapability of opportunity costs generated by the need to set priorities, he argues that the logic of community rights and procedural remedies, which draws strongly on Norman Daniels and James Sabin’s accountability for reasonableness framework, is the most compelling, while the individual rights and substantive remedies logic, prevalent in some Latin American countries, is the least. But he clarifies that the former should not always prevail over the others. Special circumstances may call for the other approaches, such as exceptional clinical reasons (individual/procedural), serious cases of hardship for entire groups (community/substantive), and limited trust between resource allocators and the judiciary (substantive/individual). He helpfully illustrates each of these approaches with concrete examples from different jurisdictions across the world and finishes by arguing, persuasively in my view, that his matrix helps illuminate the costs and benefits of judicial policy and urging judges to be more transparent about which approach they adopt and why. This seems to chime with both Loaiza et al.’s and Pizzarossa et al.’s papers, which question the lack of coherent justification in decisions in Costa Rica and Uruguay. Moreover, both adopt what Newdick would call the individual rights and substantive remedy approach, the most problematic one in his view.
Syrett’s article calls for the “[d]evelopment and clarification of the normative basis of the right to health in a manner which would enable courts to respond sensitively and appropriately to conditions of scarcity.” This would entail, in his view, finding a “middle ground” between the two prevalent extremes: one that rejects the very possibility or usefulness of a rights-based approach to health and thus “seems to attach insufficient weight to the right [to health] as a claim in law,” and another that sees that right as an absolute claim and thus “accords insufficient weight to the opportunity costs of giving effect to the right.” Such task, he admits, is “manifestly a highly demanding [one],” yet cannot be avoided in a climate of ever-growing contestation and litigation about access to scarce health resources, not only in Latin America but across the globe. In his exploratory endeavor, he looks into the prospects for proportionality, a “relational” conception of rights, and a “deliberative democracy” role for courts as potential “pathways through which this challenge might be addressed.” All face important challenges, as he admits, but could, with further development, provide a sound basis for progress.
Out of the three pathways proposed by Syrett, proportionality seems to me the most problematic. Some have persuasively criticized its usefulness in yielding specific answers even to the classical bilateral conflicts involved in civil liberties (for example, liberty versus security, and freedom of expression versus privacy).[16] In polycentric distributive conflicts such as those involved in social and economic rights, the likelihood of indeterminate results seems significantly higher. Proportionality thus seems incapable of either replacing or adding to the priority-setting criteria and the disagreement around them, discussed above. The relational reading of the right to health seems very plausible to me and in line with cherished public health ideas of equity and community or public interest. Yet, as Syrett properly alerts, “many will doubt whether this approach is consonant with ideas of rights at all.” The deliberative democracy pathway, rather than an alternative to the other two, seems more like a compromise that may be able to incorporate what Syrett calls a “culture of justification” embedded in the other two, “permitting proper judicial consideration of the interconnectedness of individual rights to health care and obligations to the community in circumstances of scarcity.” Yet, as Syrett admits, it would need much further development and testing than he is able to provide in his contribution.
Aquiles Ignacio Arrieta-Gómez’s contribution on Colombia provides interesting insights from someone who has witnessed, from the inside, the workings of one of the most innovative and respected constitutional courts. He provides a detailed account of the landmark Decision T-760 of 2008, a structural ruling on the right to health in which the court ordered the state to remedy the inequality that existed between the more comprehensive contributory system and the subsidized system, which had lower benefits coverage. He also describes setbacks that followed T-760 but concludes, on a positive note, that the decision had at least three positive effects: “it helped establish the constitutional roots of the right to health and its justiciability (a living reform of the Constitution); it guaranteed better access to necessary health services; and it ensured that public health policies are rights oriented, including through the promotion of reasonable limits and public participation in decision making.”
Judicialization beyond courts
The two contributions focused on Brazil, by Danielle da Costa Leite Borges and Regiane Garcia, invite us to lift our gaze from courts in order to see some important developments happening elsewhere, often neglected in the literature on judicialization.
Borges’s piece discusses improvements in what she calls “health governance,” which health litigation has indirectly helped promote. She focusses on two fronts: (1) the creation of the National Commission for the Incorporation of Technologies in the Public Health System in 2012 and (2) several local and national initiatives aimed at reducing the need for litigation through different types of cooperation between the executive and judiciary. As she persuasively argues, “the creation of [the national commission] brought substantial improvements to the institutionalization of [health technology assessment], especially as compared to the old decision-making process.” The system has become “more transparent, participatory, and accountable,” which, in her view, “can contribute to the advancement of fairness in the health system … by making drugs available to the population at large and not only to individual claimants.” In terms of judicial-administrative cooperation, she highlights two recent initiatives: the creation of “advisory health committees” composed of permanent civil servants of the state health authority in the fields of medicine, nursing, pharmacy, nutrition, and management to provide technical advice to judges in right to health claims, and the establishment of mediation and conciliation centers, where health claims are mediated by a social worker who connects health authorities and claimants to assess the merits of the claim and try to reach a solution out of court. Both were initially adopted in the state of Rio de Janeiro but are now being extended to other states in the country. As Borges argues, although these developments are still too recent and not much data are available on them, they hold the potential to improve the fairness and efficiency of the Brazilian public health system and to contribute to the “dejudicialization” of health—that is, to decrease the large number of cases that end up in Brazilian courts.
It is interesting to note, here, that Loaiza et al.’s contribution also discusses a similar new process that has been adopted in Costa Rica. The authors are actually able to empirically test whether involving outside medical expertise has improved the Sala IV’s health rights jurisprudence by comparing successful health rights litigation claims for medications before and after the rollout of this process. Their conclusion is that it has not, but the blame seems to lie more on the type of the expertise used (the Cochrane review, which does not include cost-effectiveness analysis) than in the judges, who tend “to follow the vast majority of these recommendations.” A similar study on Brazil when data becomes available would be very welcome.
Garcia’s piece focuses on an aspect of the right to health that seems even less discussed in the literature on judicialization: the participation of citizens in health policy decisions. After arguing that participation is a legal right both in Brazilian and international law, she goes on to describe the results of her doctoral empirical research project on the functioning of the Brazilian National Health Council (NHC), the participatory body created to comply with the requirement of “community participation” established in article 198 of the Constitution. Through naturalistic observations of NHC meetings and semi-structured interviews with various NHC members during 2012–2015, she attempted to shed light on three main questions: “whether the composition of the NHC facilitated citizen participation, whether the NHC was successful in considering group needs and systemic concerns, and whether the law hinders the NHC’s ability to carry out its mandate.” Her tentative conclusion, necessarily limited by the scope of her research (“a small-scale study focusing on the experiences of 26 NHC members”), is that the NHC is a “particularly important mechanism for participation because it facilitates the inclusion of marginalized communities and the consideration of system-wide concerns.”
Whether these concerns are then translated into concrete health policies and lead to improved access and better population health is something that Garcia was not able to establish but seems important to determine through future research. Given the strong, and perhaps growing, body of opinion (see Newdick, Syrett, and Pizzarossa et al. in this issue) that courts should at least review the reasonableness of allocative decisions and that one of the crucial criteria is “participation,” we ought to know much more than we currently do about the working and effectiveness of institutional mechanisms for participation such as the Brazilian NHC studied by Garcia.
Sofía Charvel, Fernanda Cobo, Silvana Larrea, and Juliana Baglietto’s contribution also looks beyond the courts. They conduct a useful mapping of the legal instruments on priority setting in Brazil, Costa Rica, Chile, and Mexico with a view to determine the extent to which each reflects the elements of transparency, relevance, review and revision, and oversight and supervision, which they take from Daniels and Sabin’s accountability for reasonableness framework and Sarah Clark and Albert Weale’s social values framework. Their conclusion is that while all four countries fulfill these elements to some degree, there is significant variability in how they do so and improvements are needed in several areas. Perhaps the most homogenous findings are on the element of transparency. As the authors state, “it is difficult to find the information online and … the information is not updated as required by law.” Moreover, the fragmentation of priority-setting systems—in other words, the lack of a single priority-setting mechanism—“makes even more complex the task of understanding how priority setting is performed.” In all other elements, variations and gaps are found in different countries, leading the authors to invite “countries to improve their legal frameworks.” This mapping and analysis of the legal framework is certainly interesting and valuable, yet one should avoid conclusions about the actual fairness of priority-setting institutional mechanisms based only on what the law states. As those familiar with social-legal scholarship could argue, “law on the books” can and often does diverge from “law in action.” Analysis of how priority setting actually takes place in each country is therefore important to allow us to know how effective these legal frameworks really are.
International accountability
Most Latin American countries have recognized the right to health not only in their domestic law (often in the constitution) but also through international treaties, such as the International Covenant on Economic, Social and Cultural Rights and the Protocol of San Salvador of the Organization of American States. Moreover, out of the current 23 countries that have ratified the Optional Protocol to the International Covenant on Economic, Social and Cultural Rights—an important new complaint mechanism—no fewer than 7 are from Latin America (Argentina, Uruguay, Bolivia, Ecuador, Costa Rica, El Salvador, and Honduras), and another 4 have signed but not yet ratified the treaty (Chile, Paraguay, Venezuela, and Guatemala).
Judicialization studies tend to focus on national courts, for several understandable reasons. The explosion of litigation in some countries takes place in these courts; many countries have included the right to health in their national constitutions, and domestic courts tend to focus on constitutional norms rather than international law; and the debate on the legal status and force of international human rights law, especially in the field of social and economic rights, still rages. Nonetheless, domestic courts in some countries are paying increasing attention to international human rights law, and it may thus become more relevant to look into the role of international human rights law when studying judicialization. This may be particularly so in those countries that have ratified the Optional Protocol to the International Covenant on Economic, Social and Cultural Rights and have thereby agreed to be subject to recommendations following the adjudication of individual or group complaints.
Pizzarossa et al.’s study of Uruguay, one of the first countries to ratify the Optional Protocol, uses the interpretation of the United Nations Committee on Economic, Social and Cultural Rights regarding minimum core obligations and non-discrimination as their framework to evaluate judicialization in that country. They seem to find the Uruguayan courts wanting in both areas when it comes to granting off-formulary low-priority drugs to claimants.
Another contribution to this issue that focuses on international law is that of Laura Pautassi. She studies the reports submitted by seven countries (Bolivia, Colombia, Ecuador, El Salvador, Mexico, Paraguay, and Uruguay) to the working group responsible for examining state parties’ compliance with the Protocol of San Salvador, as well as the observations and recommendations made by the working group’s experts. Her focus is on what she calls the “cross-cutting” category of access to justice, which she claims is a “key component of the right to health.” It is interesting that in a region known for its high volume of litigation, one of her main findings is that there is “a lack of recognition regarding the need to ‘enable’ access to justice.” This seems to reinforce the point about the significant diversity of the phenomenon across Latin America.
Health improvement in Latin America: The role of rights and litigation
Most Latin American countries have made progress in the past three decades in terms of the well-being of their populations—some have made considerable progress, others not as much. In terms of the Human Development Index (HDI), the only country still in the “low human development” group is Haiti (0.493 in 2015), but even that represents an almost 20% improvement over its 1990s situation (0.408). All other countries are well above 0.55, the threshold for “medium human development”; many are in the “high human development” group (that is, above 0.7); and some score as high as 0.827 (Argentina) and 0.847 (Chile), placing them in the “very high human development” bracket. When we focus on the health components of the HDI, we also see significant progress. In life expectancy, for instance, no Latin American country is below 60 anymore, with Haiti (54.6 in 1990 and 63.1 today) and Bolivia (55.1 in 1990 and 68.7 today) having improved their situations. In addition, life expectancy in Chile (82), Costa Rica (79.6), and Cuba (79.6) is above that of the United States (79.2) and similar to that of the United Kingdom (80.8). Most other Latin American countries clutter around 75 and 76, with the regional average at 75.2. Infant mortality has also fallen significantly: Haiti has decreased from a staggering 101 per 1,000 live births in 1990 to 52.2 today; Bolivia from 85.6 to 30.6; and Guatemala from 59.8 to 24.3. All other Latin American countries have rates under 20 (indeed, Uruguay, Costa Rica, and Cuba have rates under 10).
It is of course true that these are country averages that disguise inequalities—sometimes significant ones—among the population. Yet the scale of some of the progress is such that it could not have happened without improving the lives of those at the bottom of the socioeconomic pyramid as well.
That progress has occurred everywhere, that it varies among countries, and that there is still a lot to be done in all of them is clear. What is much more complex to establish is whether the right to health has had any role and, if so, of what precise nature, in such progress. Here, we must distinguish between three different ways in which the right to health may feature in such an impact analysis: as a moral claim, as a legal right, and as a justiciable guarantee. As a moral claim, the right to health imposes moral duties on society to ensure that the right is respected. This is how the right to health has been invoked, for instance, at least since the 1940s, most notably in the 1946 Constitution of the World Health Organization and, later, in the 1978 Declaration of Alma-Ata. When transformed into a legal right (“legalization”), as most countries have increasingly done since the 1970s through either the ratification of international treaties or the adoption of domestic legal instruments (often the national constitution), that moral claim becomes part of the law—it acquires a legal status that, depending on the context in which it operates, may add some clarity and strength to the moral idea. As a justiciable guarantee, it is supposed to acquire a further layer of potential protection through the possibility of being invoked in courts (“judicialization”).
It seems clear that the right to health as a moral idea has played a significant role in the improvement of the health conditions of the population in Latin America described above. As Rifat Atun et al. show, the pioneering health system reforms in Latin America—aiming “to expand access to health services, improve health outcome, and increase financial risk protection”—were strongly inspired by the idea of health as a human or a citizen’s right, and such reforms have played a direct role in the improvement of the health outcomes of the population. To quote the authors:
Along with economic development and rising incomes, improvements in health systems and universal health coverage have contributed to improved health outcomes for women (reduced maternal mortality ratio) and children (reduced under-5 and infant mortality rates … ) and for communicable diseases such as malaria, neglected tropical diseases, and tuberculosis, which predominantly affect the poor.[17]
Whether the legalization and judicialization of the right to health can strengthen or accelerate the progress is less clear. Some of the most comprehensive and high-quality health systems in the world are in countries where the right to health has not been expressly legalized via domestic legislation (for example, the United Kingdom), suggesting that, at least in those countries, legalization may not be an important determinant of respect for the right to health. In many Latin American countries, however, there is a widespread belief that legalization, particularly through the constitution (“constitutionalization”), provides further protection to the moral idea of health as a human right and further guarantees against recalcitrant governments. The same is often thought of judicialization. If the government is unwilling to comply with its duties correlated to the right to health, citizens can go to the judiciary to force implementation. If that option is not available (that is, if the right to health is non-justiciable), an important source of motivation for the state to comply with its duties is thought to be lost.
The problem is that the real world of health policy practice and, in particular, priority setting (that is, the allocation of limited resources among virtually unlimited and growing health needs) is much more complicated than the neat theoretical universe of rights and duties. As briefly discussed above, such complexity affects significantly our ability to reach a consensus on the correctness of specific priority-settings decisions or, to put it in legal terms, our ability to determine with precision the content of the right to health. This in turn makes the assessment of the legitimacy and impacts of the phenomenon of judicialization more difficult.
However, this complexity should not demotivate us from continuing the effort of collecting and analyzing more data and refining our analytical framework to help us better understand this fascinating phenomenon. The contributions of this special issue take us further in that direction.
Acknowledgment
Some of the papers in this special section were presented during two conferences in 2017, at Georgetown and King’s College London law schools. The guest editors are grateful to both law schools for the funding provided.
Octávio Luiz Motta Ferraz is a reader in transnational law, co-director of the Transnational Law Institute, and an affiliate of the Brazil Institute at King’s College London. He was formerly a senior research officer for the United Nations Special Rapporteur on the right to health.
Please address correspondence to Octávio Luiz Motta Ferraz. Email: octavio.ferraz@kcl.ac.uk.
Competing interests: None declared.
Copyright © 2018 Motta Ferraz. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1]. See 2018 Index of Economic Freedom, Index: Central, South America show mixed progress on economic freedom (January 14, 2014). Available at https://www.heritage.org/index/press-release-south-america.
[2]. M. Tenorio-Trillo, Latin America: The allure and power of an idea (Chicago: University of Chicago Press, 2017), p. 3.
[3]. R. Iunes, L. Cubillos-Turriago, and M. L. Escobar, Universal health coverage and litigation in Latin America (Washington, DC: World Bank, 2012).
[4]. A. E. Yamin and S. Gloppen (eds), Litigating health rights: Can courts bring more justice to health? (Cambridge, MA: Harvard University Press), pp. 76, 87–88.
[5]. M. Tushnet, Weak courts, strong rights: Judicial review and social welfare rights in comparative constitutional law (Princeton, NJ: Princeton University Press, 2008), pp. 227, 264.
[6]. J. King, Judging social rights (Cambridge: Cambridge University Press, 2012).
[7]. O. Ferraz, “The right to health in the courts of Brazil: Worsening health inequities?,” Health and Human Rights Journal 11/2 (2009), pp. 33–45.
[8]. A. E. Yamin and F. Lander, “Implementing a circle of accountability: A framework for judiciaries in enforcing health-related rights,” Journal of Human Rights 14/3 (2015), pp. 312–331.
[9]. O. L. M. Ferraz, “Harming the poor through social rights litigation,” Texas Law Review 89/7 (2011), pp. 1643–1668.
[10]. O. F. Norheim and B. M. Wilson, “Health rights litigation and access to medicines: Priority classification of successful cases from Costa Rica’s Constitutional Chamber of the Supreme Court,” Health and Human Rights Journal 16/2 (2014), pp. 47–61; see also their contribution in this issue.
[11]. P. Slon, Universal health coverage assessment: Costa Rica (Ottawa: Global Network for Health Equity, 2017). Available at http://gnhe.org/blog/wp-content/uploads/2015/05/GNHE-UHC-assessment_CostaRica.pdf.
[12]. United Nations Development Programme, Human development report 2016: Human development for everyone (New York: United Nations Development Programme, 2016).
[13]. For a recent discussion of divergence in findings within Brazil, see the exchange between O. L. M. Ferraz, “Moving the debate forward in right to health litigation,” Health and Human Rights Journal 18/2 (2016), pp. 265–268 and J. Biehl, M. P. Socal, and J. J. Amon, “Response: On the heterogeneity and politics of the judicialization of health in Brazil,” Health and Human Rights Journal 18/2 (2016), pp. 269–271.
[14]. G. Calabresi and P. Bobbitt, Tragic choices (New York: W. W. Norton and Company, 1978).
[15]. C. Newdick, Who should we treat? Rights, rationing, and resources in the NHS (Oxford: Oxford University Press, 2005); K. Syrett, Law, legitimacy and the rationing of health care: A contextual and comparative perspective (Cambridge: Cambridge University Press, 2008).
[16]. For a good discussion, see V. Afonso da Silva, “Comparing the incommensurable: Constitutional principles, balancing and rational decision,” Oxford Journal of Legal Studies 31/2 (2011), pp. 273–301.
[17]. R. Atun, L. O. Monteiro de Andrade, G. Almeida, et al., “Health-system reform and universal health coverage in Latin America,” Lancet 385/9974 (2015), pp. 1230–1247.