Access to Justice in Health Matters: An Analysis Based on the Monitoring Mechanisms of the Inter-American System
Laura Pautassi
Abstract
This article analyzes how states are complying with their periodic reporting obligations under the Protocol of San Salvador (PSS) in one specific area: access to justice as a key component of the right to health. The sources of information for this analysis are seven reports submitted by the States parties, together with the observations and final recommendations made by the experts of the monitoring mechanism of the PSS. The reports are based on progress indicators, a group of indicators that the states must use to measure progress in compliance with its rights obligations. This system of indicators presents the cross-cutting category “access to justice,” which allows the identification of each branch of government’s involvement in the design of a health system and the guarantees of judicial protection of the right to health. The analysis focuses on the articulation of the empirical evidence presented by the States in the context of protection and fulfillment of the right to health, identifying progress made or limitations faced in the compliance with state responsibilities. The main findings reveal the weakness of the current mechanisms of access to justice in health and the reticence of the judiciary to take an active role towards accountability.
Introduction
Latin American states widely recognize the right to health. Most of these countries include a specific mention to the right to health in their constitutions and have ratified international agreements: the International Covenant on Economic, Social and Cultural Rights (ICESCR) and the Additional Protocol to the American Convention on Human Rights in the Area of Economic, Social and Cultural rights (ESCR), known as the Protocol of San Salvador (PSS).
ICESCR (1966) is a binding instrument for 18 Latin American states, while the PSS was opened for signature in 1988, came into effect in 1999, and has so far been ratified by 16 states. In both cases, the definition of the right to health is largely similar. While ICESCR states that the right to health is “the right of all persons to enjoy the highest possible level of physical and mental health” (Art. 12.1), the PSS defines it as “the enjoyment of the highest level of physical, mental and social well-being” (Art. 10.1). These instruments also require states to take similar measures, such as healthy working conditions and prevention, treatment, and medical assistance, with the purpose of guaranteeing the full effectiveness of this right. As a result of the work carried out by United Nations monitoring mechanisms such as the Committee of the ICESCR and the Office of the High Commissioner of the United Nations for Human Rights (OHCHR), the State parties reached a new consensus regarding the forms of verifying compliance with obligations related to the right to health. The necessary framework for the incorporation of human rights indicators was the result of the work of special rapporteurs, in particular the first special rapporteur for the right to health, Paul Hunt, who strongly emphasized the need to develop progress indicators to measure compliance with the right to health.[1] Subsequent documents from the United Nations supported his position.[2]
At the regional level, the Inter-American Human Rights System (IHRS) made a key contribution through the 2005 Resolution of the General Assembly of the Organization of American States (OAS), which established that the monitoring mechanism of the PSS would be designed through human rights indicators, more precisely “progress indicators,” as described in the following section.[3] In 2007, another resolution of the general assembly established that the monitoring mechanism will be called the Working Group responsible for examining periodic reports of State parties to the Protocol of San Salvador (WGPSS) and be comprised of two independent experts, four governmental experts, and two members of the Inter-American Commission on Human Rights (IACHR).[4]
This milestone was the first step in an unprecedented process, which involved the design and implementation of a mechanism that combines obligations, accountability, and empirical evidence for eight rights: health, education, social security, work, trade union rights, adequate food, environment, and cultural rights. The system of progress indicators also takes into account guarantees for the protection of children and adolescents and elderly and disabled persons, while also incorporating a gender perspective and the recognition of indigenous populations and ethnic groups in a cross-cutting manner.
In order to analyze this innovative tool for measuring State parties’ compliance with the right to health, in section 3, I look at all seven countries that have to date been evaluated by the Working Group of the Protocol of San Salvador (WGPSS), the body in charge of monitoring the national reports. These countries are Bolivia, Colombia, Ecuador, El Salvador, México, Paraguay, and Uruguay.[5] For each country report, the analysis involves the states’ responses to the requested indicators regarding access to justice and the identification of the guarantees of justiciability in health matters. The sources of information are the reports submitted by the State parties and the observations and final recommendations made by Working Group experts.
Section 4 focuses on the shortcomings of information from the states, specifically regarding access to justice in health. Lastly, some key findings are presented on the conclusions.
Support in the evidence: progress indicators
This section will describe the PSS system of progress indicators in terms of the cross-cutting category of access to justice within the right to health. As mentioned above, the PSS defines the right to health in a very similar way to ICESCR; therefore, the interpretive standards and the general observations made by the ICESCR Committee have been a relevant source for the elaboration of the PSS progress indicators.
The scope, content, and measures to be adopted by the State parties to the PSS in terms of the right to health require elements that allow the verification of coverage, universality, integrality, progressive realization, and non-regression, among other relevant information.[6]
Progress indicators relate to social or development indicators regarding the sources of information, such as national statistics, census data, and surveys. However, their distinctive feature compared to development and other indicators lies in the fact that the unit of measurement is every economic, social, and cultural right (such as the right to health) defined in the PSS.
This analytical exercise requires the identification of different human rights dimensions, which in turn are translated into categories and variables to be observed. This process presents many complexities, since the purpose is not only to quantify the extent of the policies adopted or laws passed, but also to qualify the state conduct in complying with its obligations. There is particular focus on quality, quantity, adequacy, availability, diversity, and universality.
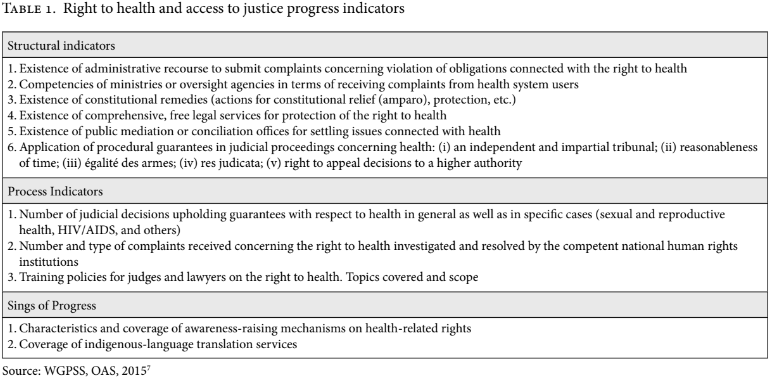
Progress indicators defined by the PSS are divided into structural, process, and results indicators. Structural indicators reflect the ratification of international legal instruments and provide information on how the State party organizes its institutions and legal system to meet its international obligations. Process indicators seek to measure the quality and extent of the state’s efforts to implement rights by tracking the scope, coverage, and content of strategies or policies designed to accomplish the goals necessary for the realization of a given right. Result indicators seek to measure the actual impact of government programs and interventions, offering a quantitatively verifiable and comparable measurement of the performance of the state in terms of the progressive realization of rights. In the case of the PSS follow-up mechanism, there has been advances in incorporating qualitative signs of progress into the three types of indicators described.
This methodology focuses on eight rights (health, social security, education, adequate food, healthy environment, benefits of culture, work, and trade union rights) and also on the state’s obligations to respect, protect, and guarantee these rights. Other categories were developed in order to complete the system of indicators: institutional design adopted, financial context and budgetary commitment and state capacities. Finally, the conceptual framework is completed by the fundamental human rights principles: equality and nondiscrimination, social participation and accountability, access to information and to the justice system.
The General Assembly of the OAS requires compliance with the information required by the indicators.[7] All data thus produced by the State parties also advances the Sustainable Development Goals agenda.
The system designed by the Working Group of Protocol of San Salvador (WGPSS) requests 714 indicators in total. Specifically regarding the right to health, the WGPSS requests 85 indicators, as well as signs of qualitative progress (see Table 1).
The information that State parties submit under this recently created monitoring process provides a baseline for further measurement of progress. State parties must report every three years, which means that as of 2019 there will be a flow of relevant information that will allow a detailed analysis of the different elements involved in the compliance with the ICESCR.
On the other hand, as the WGPSS points out in its reports, the official information submitted by the states is the only element of analysis. Said reports do not necessarily cover the states’ “degree of compliance” with their obligations to the right to health, rather only how those states are “reporting” to an international human rights mechanism, such as the one devised under the PSS. The WGPSS therefore bases its evaluation only on the information received officially by each state. While the WGPSS does take alternative civil society reports (shadow reports) into consideration as control elements for the mechanism, these shadow reports are not part of the State party’s evaluation procedure.
Access to justice for health matters according to the State parties’ reports
This section analyzes the seven national reports submitted to the PSS monitoring mechanism, as well as the recommendations the WGPSS made regarding access to justice in health matters. The interest in analyzing the reports submitted by the State parties is that this is the only information that the states themselves show and provide, in light of a binding mechanism and in response to their international obligations regarding the right to health.
Bolivia
Bolivia is a particular case, insofar as its definition as a plurinational and intercultural state, based on its constitution of 2009, establishes in Article 18 that:
I. Every person has the right to health.
II. The state guarantees the inclusion and access to health for all persons, without any exclusion or discrimination.
III. There shall be a single health system, which shall be universal, free, equitable, intra-cultural, intercultural, and participatory, with quality, kindness, and social control.
Subsequent articles acknowledge that the health system should be universal and free, and should respect the Bolivian world view and the traditional practices of the nations and rural and/or native indigenous people. Articles 35 through 44 expressly and widely recognize the right to health and social security. The WGPSS pointed out that Bolivia presented a project related to the strengthening of access to justice and prevention of violence against women in indigenous populations and communities; and in rural, native and afro-descendant communities. The Working Group experts expressed:
The state should advance in a prompt and timely manner the implementation of this project understanding that it represents the first step to increasing the guarantees to access to justice, in this case of women who are victims of violence, but it is the hope that they be incorporated in the various fields of guarantees of economic, social and cultural rights.[9]
The lack of information submitted by the state of Bolivia with regard to indicators of access to justice in health is noteworthy. The report only mentions that, with regards to administrative matters, complaints must be filed with the Ministry of Health, the Ombuds office, or the medical school. Complaints must be submitted via a form that is available in person and on the Ministry of Health website. This is all the information that it offers in terms of access to justice in health.
The WGPSS has therefore indicated that in future, Bolivia should provide information regarding:
- number of judicial decisions that have granted guarantees in health generally and in specific cases (such as those dealing with sexual and reproductive health, treatment for people living with HIV/AIDS),
- number of complaints related to the right to health received, investigated, and resolved by the competent national human rights institutions, and
- policies for training judges and lawyers in right to health matters, topic coverage, and scope.
Colombia
Colombia recognizes the right to health for children and adolescents (Articles 44 and 50 of the constitution) and the protection of and the assistance for elderly people (Article 46) where the state guarantees “the services of integral social security and food subsidies in the cases of indigence”. In 2009, Article 49 was amended to establish that “public health and environmental protection are public services under the responsibility of the State. All individuals are guaranteed access to the services that promote, protect and restore health.”
Colombia submitted more complete information than Bolivia regarding indicators related to access to justice. First, the state indicated that the National Health Superintendence (“Supersalud”) receives petitions related to the General Health Social Security System, and that there are other administrative bodies for filing complaints: the Ministry of Health and Protection, Ombuds office, and national attorney general’s office; offices of the district and municipal attorneys of Bogota; and departmental, district, and municipal health departments. According to the report, the Ombudsman office registered the requests for counseling, attention, and intervention for violation of the right to health due to the deficiency in care provided by the territorial authorities and service providers. It states that health is the most frequent complaint received by this organism: Supersalud received a total of 239,584 petitions, complaints, and requests for information submitted in 2011.
With regard to conflict resolution, Supersalud has a delegate for the jurisdiction and conciliation procedures, who has been implementing conciliation as an alternative mechanism for conflict resolution between actors of the health service and acting as judge and mediator in these reconciliations. The state report adds that it offers conciliation workshops in different departments of the country as a strategy to offer this “tool as an alternative mechanism for conflicts as opposed to the judicial route and in a more expeditious manner allowing for the standardization of the flow of the resources of the General Health Social Security System.” The official information indicates that in 2010, 1,403 conciliation agreements were signed.
With regard to writ for protection of constitutional rights, Colombia states that “constitutional actions are becoming the best alternative that the Colombians have to assert their rights before the different entities when a fundamental right has been violated.” The report indicates that in 2011, 105,947 writs were filed invoking the right to health. However, background information was not provided, and neither was the scope or degree of the resolution of these actions.
In the Colombian case, it is particularly striking that the state affirms in its report that the “constitutional action (tutela) has constituted the best alternative for Colombians to claim their rights before the different entities when fundamental rights are violated.” The potential of using indicators to monitor rights can be seen here, as it allows the identification of this type of response, and shows how the state itself recognizes the limits of its own health system.[10]
On the indicator requested by the WGPSS for procedural legal guarantees in matters of health, Colombia reports that the current judicial career system permits entrance based on merits to judges, court magistrates, and employees. In the high courts, magistrates are elected for a fixed period of eight years and cannot be reelected. There is also a training program at the Lara Bonilla Law School that specializes in labor and is mainly directed at labor magistrates and judges regarding international work standards, judicial practice in social security for health, and judicial practice in pensions.
It is interesting to note that Colombia is the only state that has submitted information about the length of time involved in administrative procedures related to health issues. They indicate that such procedures take twice as long as labor lawsuits.
However, the state indicates that “during 2012, in the writs for protection of constitutional rights that invoked the right to health, 80.27% of the judicial decisions in the lower court were decided in favor of the protection of the right.” They did not provide more information, including the source of this calculation or the motives for which the writs were granted. Nevertheless, these tendencies seem to indicate an excessive use of the writ for protection of constitutional rights for purposes of the realization of the right to health.
The WGPSS highlighted the overall high degree of response to the requested indicators, particularly the Comprehensive Information System for Social Protection (SISPRO) that “makes available to the public the results reached in terms of health statistics and indicators of the sector.” The WGPSS pointed out that Colombia has
“proceedings that allow filing of complaints for noncompliance with the right to health, as well as public offices for mediation or conciliation. Likewise, it recognizes that the access to the justice system is free and that the Judiciary is independent and autonomous; in addition to the fact that there are in-depth courses for magistrates.”
Therefore, the WGPSS has made specific mention of the information submitted in matters of access to justice regarding health matters.
Ecuador
Ecuador established in Article 32 of its 2008 Constitution that
health is a right guaranteed by the State and whose fulfillment is linked to the exercise of other rights, among which the right to water, food, education, sports, work, social security, healthy environments and others that support the good way of living.
Subsequent constitutional articles recognize that priority and specialized care in public and private sectors shall be given to: elderly persons; children; pregnant women; people with disabilities; people in prison; people with high-complexity illnesses; and/or people in situations of risk; and victims of domestic or sexual violence, child abuse, and natural or manmade disasters.[11]
Ecuador specifically reports that pursuant to Article 191 of the constitution, the responsible for filing complaints to guarantee the protection of the right to health is the office of the Attorney for the Defense of the People, a decentralized entity of the judicial function which offers free legal services and representation for those who cannot hire a lawyer. Likewise, the obligatory nature of guaranteeing access to justice is extended to universities.[12]
Ecuador states that it has 775 public defenders and 10 free legal advice offices in the country.[13] The Ombuds office reports that 2,079 consultations occurred between 2013 and 2015, most of which related to the right to health. Although there is a general description that the consultation related to the “right to health and good living,” the WGPSS pointed out that the State party made the effort to specify gender, education level, and ethnic background of each person who submitted an inquiry. Most inquiries were made by mixed-race individuals, followed by Afro-Ecuadorians. It remains uncertain whether many of the consultants may not have declared their indigenous origin.
The state declared that the judicial council registered 63 mediation centers on a national level, 14 of which are public centers and 49 private. In its official report, the state informed that “no cases related with the right to health have been registered but they were able to be addressed as they dealt with admissible matters.” It is noteworthy to show how the state admits its own inaction in terms of guarantees or protection of rights. Finally, regarding the indicator for policies for training judges and lawyers in matters of the right to health, Ecuador points out that the Ministry of Public Health and the judicial council are working on an inter-institutional agreement to train judges and lawyers in matters of the right to health.
When responding to the structural indicator related to the application of procedural guarantees in judicial proceedings in matters of health, the state asserts that the constitution establishes from Articles 75 to 82 the rights to protection, among which are the independence and impartiality of tribunals, reasonable time period, equality of arms and avenues for appeals of decision to upper courts.[14] However, Ecuador responds that on a national level, as of April 2016 “they have not processed any information about the number of legal decisions that have granted health guarantees.”
The Ministry of Public Health implemented the model of comprehensive health care that prioritizes primary care, prevention, and promotion of health with citizen participation, including a National Department of Human Rights, Gender, and Inclusion at the Ministry of Public Health, which forms part of the national Vice-Ministry for the Promotion of Health, and whose purpose is to implement public policies for the protection of the right to health.
In turn, the state provided summaries of two cases before the Inter-American Court of Human Rights (IACHR) against the Ecuadorian state. Both cases are in the supervision stage of compliance with judgment and a provincial court in Pichincha regarding HIV and sexual and reproductive health. The first case, Gonzales Lluy and others v. Ecuador, referred to the state’s international responsibility for infringement of the right to dignity and personal integrity of the victim.[15]
It concerns a child who in 1998 contracted HIV through a blood transfusion carried out when she was three years old, and the multiple discriminations she endured as a result. The state reports that as of January 2014, the child had guaranteed access to health and medical services, including medical and psychological treatment and medications, as well as a scholarship for graduate and post-graduate studies and recognition of the state’s international responsibility.[16]
The other case reported is that of Laura Alban Cornejo, who in 1987 was admitted to Hospital Metropolitano in Quito with clinical evidence of bacterial meningitis. A resident prescribed an injection of 10 milligrams of morphine to treat the patient’s excruciating pain. Five days later, the patient died. On November 22, 2007, the IACHR ruled that the authorities did not provide the proper guarantees in response to the complaint filed by the victim’s parents, and did not initiate a timely investigation into her death. The state recognized the lack of a prompt, diligent investigation. Ten years after the judgment, Ecuador reported that “it has established rules and public policies aimed at preventing the facts that occurred in this case and guaranteeing expeditious and diligent legal proceedings.”
The reports analyzed by the WGPSS are based on the official information submitted by each State party. In the case of Ecuador, the state admitted that several cases were brought before the IACHR and that the right to health must be directly justiciable before the IACHR.
Ecuador reported that 26 cases related to the right to health were registered as having been received, investigated, and resolved.[17] Recognizing the presumed violation of rights, these complaints are directed to the Human Rights, Gender and Inclusion Directorate of the Ministry of Health, and an investigative process is carried out. The state indicates that “the investigations carried out in these cases also serve as an input for making improvements within the National Health System.” They also note that the Ministry of Public Health, through the directorate, is in the first phase of implementing the “Model of Management of Requirements and Citizen Complaints to improve the Health Service,” an online system that organizes and manages citizen requests, generates information on the main problems for the development of favorable public policies, and is a tool for improving service quality.
El Salvador
Article 65 of the constitution states:
The health of the inhabitants of the Republic constitutes a public good. The State and people are obligated to see to its conservation and restoration. The State shall determine the national health policy and control and supervise its application.[18]
Thereafter, the state commits to free assistance to all persons without resources and sets the foundation for the organization of health benefits. Throughout El Salvador’s report and in accordance with the WGPSS evaluation, the state highlights the formulation of a five-year plan that seeks to progressively ensure universal health coverage. Furthermore, the report mentions the Intercultural Health Plan, initiated in 2011, in context of the Ministry of Health consultation of the national health policy for indigenous communities. It also notes advances in services for individuals who are elderly, mentally ill, or have a physical or mental disability. However, it notes with concern that the average coverage in the country only reaches 25% of the entire population and requires an increase in health resources.
Regarding access to justice, El Salvador indicates that between 2010 and 2015, the Ministry of Health processed 1,365 complaints. Most of these complaints were resolved, but the report does not indicate in whose favor.
Based on information from the Secretariat of the Constitutional Court of the Supreme Court, El Salvador indicated that from 2010-2014 there were 53 constitutional suits, judicial actions, and procedures for protection of rights. Thirty-one have a final judgement for habeas corpus and protection measures, mostly due to lack of medical treatment or assistance, provision of medications, or interruption of pregnancy due to imminent danger of death for the woman.
The state points out an “amparo” case specifically related to the right to life and to sexual reproductive health that was dismissed on May 28, 2013.[19] The judgment indicates that
all the fundamental rights possess the same hierarchy despite the fact that article 1 paragraph 2 of the constitution establishes that women cannot allege the right to their own body or to the right to interruption of pregnancy. Decision compatible with the Constitutional and Democratic Rule of Law.[20]
In clear opposition, the WGPSS has emphatically indicated that El Salvador must review its policy on sexual and reproductive health with the participation of civil society. In particular, it encourages El Salvador to review the legislation regarding the absolute criminalization of abortion, taking into consideration a comprehensive vision of human rights in line with recommendations of other international and regional protection organisms.
Finally, the report points out that the State party does not have a training policy for judges and lawyers in matters of right to health.
Mexico
Mexico is a federal state that ensures on a constitutional level “access to health services through the expansion of coverage of the national system” with recognition of the principles of equality and nondiscrimination and the rights of the indigenous people. In its report submitted to the WGPSS, the state indicates that the administrative body competent for receiving health complaints is the National Medical Arbitration Commission (CONAMED) together with the National Commission of Human Rights and the State Commissions of Human Rights.
The state reports that the National Commission on Human Rights received 4,616 complaints regarding violations of the right to health in 2012, while in 2011 they registered 4,310 omissions without providing further information about the resolution.[21]
Although the constitution contemplates procedural guarantees in Articles 14 and 17, as well as in federal civil procedural code and amparo law, among other laws, the population has alarmingly limited access to the writ of protection of constitutional rights. According to the state report, there are only four protection proceedings under review, regarding attention of persons with HIV (2014); disability (2014) and two cases regarding civil responsibility for medical negligence in private hospitals. The report adds that there are two actions of unconstitutionality (decriminalization of abortion in the Federal District and another regarding the law for protection of people with autism); a constitutional controversy (challenging the law on health and medical care services for family violence, sexual violence, and violence against women), and an administrative protection suit (regarding the right to health of a community in Mini Numa, Guerrero). Clearly, according to the report, the exercise of protection actions in health matters is highly insufficient. While this may be partially due to problems accessing the appropriate information, it is imperative to promote increased active surveillance to guarantee the access to justice in health and to underscore the state’s responsibilities, in line with the recommendations of the WGPSS in its final observations.
Paraguay
The constitution of Paraguay recognizes that “The State will protect and promote health as a fundamental right of the person and in the interest of the community.”[22] Thereafter, the constitution establishes that the state shall promote a national health system under a commitment of integrality, including “social well-being” on the basis of strategies based on “health education and community participation.”[23]
However, the State party’s report does not present any indicators for access to justice in health. In general terms, the indicators presented regarding the right to health are very weak.[24] The state’s report focuses the information provided on the National Service of Eradication of Malaria, including other programs referred to specific diseases. Given that this is a key organism in the health structure, the lack of answers referred to health indicators raises several concerns. No information was obtained from the report regarding guarantees of access to justice for health matters.
The WGPSS has described in its final recommendations the lack of information presented in relation to the right to health by Paraguay as an omission requiring the experts to resort to complementary sources. It also warns about the high rates of maternal mortality, adolescent pregnancy, and HIV/AIDS. Also, it strongly emphasizes the state’s obligation to be accountable and to provide guarantees to access to information.
It is interesting to note that some information can be accessed through a search in the Ministry of Health Social Well-Being website, which has a portal for open data, in addition to a site for reporting corruption.[25] However, there is no information providing evidence of the ministry having taken action. The Ministry of Justice notes the existence of a human rights observatory publishing a series of protocols, including the protocol for the access to justice for people with psychosocial disabilities, for the elderly, and for the transgender population, among others.[26] Likewise, there is a portal of information and services where citizens can access information on the judicial branch.[27] It is equally interesting that the state has developed the SIMORE Monitoring and Recommendation System aimed at facilitating the search for international human rights recommendations, but only from the international system of protection and not the Inter-American system.
In other words, although there is no detailed information or evaluation indicators, this does not mean that there is a complete absence of information, but rather that the State party has failed to report it to the WGPSS. This is no minor detail, given the relevance of the binding mechanisms in international monitoring procedures.
Uruguay
Article 44 of the constitution of Uruguay establishes the responsibilities of the state in health matters and provides that “All the inhabitants have the duty to take care of their health, as well as to get treatment in the case of sickness.” In its report, the state notes its efforts to increase this limited conceptualization of the right to health by approving law 18.211/07 of the National Integrated Health System. This law seeks to implement structural changes in the management model for the health system, and is based on the universality of access, coverage and increase in the investment and budgetary contributions.
In relation to guarantees to access to justice for right to health, Uruguay reported on the organization of the system but not on the results obtained. It indicated that there are administrative bodies to receive complaints under the responsibility of the Ministry of Health, in particular in the area of user support. It also indicated frequent use of the writ of protection for cases involving supply of expensive medications, but does not report how many writs are presented per year. In relation to the request regarding the number of judicial decisions, the state indicated that “Of the information processed by the judicial branch there is no information available regarding human rights matters.”
The WGPPS particularly stressed that the state should report the number, frequency, type of lawsuit, resolution, execution, and compliance with the judgment, among other indicators. Likewise, the WGPSS indicated that the state should break down the information provided using a gender and diversity perspective, and highlighted the need to make a more determined effort in order to obtain better performances in health. On the other hand, the monitoring mechanisms is a reminder, in line with the demands of the civil society organizations, of the need to direct a larger quantity of specific resources in matters of sexual and reproductive health towards the health sector in order to guarantee the implementation of the laws in force. Among other actions, this should provide for the training of health personnel and the information on reproductive rights for women and men.
It is worth noting that Uruguay, a state with significant development in its social security system and particularly the health system, which is expressed in the national report in other indicators, does not provide information on guarantees to access to justice. Although this is a common problem in the reports submitted by countries analyzed in this paper, it is important to point out the relevance of this information when planning and implementing public policies for access to justice.
Shortcomings in information and protection mechanisms provided
Evidence from the reports submitted by the State parties before the WGPSS show an alarming lack of information regarding the realization of the right to health and the cross-cutting category of access to justice, when compared to other categories covered by the system of progress indicators. This lack of information has not enabled a systematic evaluation of the judicial systems at domestic level, a problem that is common to all State parties. In general, only judgments from the high courts of justice are available; however, little is known about the extent to which procedures for receiving complaints are effective, or remedies for damage compensation are available. Furthermore, little information is provided regarding the length and cost of judicial procedures, information which is central to analyze access to justice.
In spite of this information deficit, some conclusions can be drawn from this sample of almost half of the State parties (7) that are part of the PSS (16).
First, the information provided in the first round of evaluation shows the potential strength of this instrument. Also, it highlights the current deficits and shortcoming in the protection available for the right to health. The evident contrast between the wide constitutional recognition of the right to health and the inability to present indicators for access to justice unveils an important gap shared by all the transversal categories included in this system.
Even in the case of the countries that present more information, such as Colombia, the resistance of the judiciary to be evaluated or be held accountable is evident. In most cases, the State parties did not submit information regarding procedural guarantees, which is the sixth structural indicator mentioned in Table 1.
States failed to report regarding the respect and guarantees of: (i) an independent and impartial tribunal; (ii) reasonableness of times; (iii) equality of arms; (iv) res judicata; and (v) right to appeal decisions to a higher authority. Such a situation, connected to the weakness in administrative procedures to guarantee the right to health (whether in the ministries of health or other supervisory institutions) shows the lack of guarantee to access to health as highlighted by the WGPSS in its final observations. Lack of information extended to the State parties’ failure to report whether any training was available for magistrates and judges regarding the right to health, and to the indicator of process related to state capacities.
Access to health services requires compliance with minimum procedures of due process, and this is a requirement for progress in guarantees to access to the right. Therefore, each State party must be accountable to its citizens regarding the time required by judicial procedures, transparency and access to information, opportunities for involvement of beneficiaries of the health system, legal frameworks applicable, and objective and reasonable criteria for awarding services and benefits. Finally, state accountability should include information on the possibility to submit complaints related to abuses or arbitrary health service rejections, including the indicators that allow the monitoring system to evaluate the degree of compliance with state obligations.
In the specific field of access to justice in health, the lack of information on demands for accountability to the judiciary is all too evident. Failing to provide the necessary information constitutes a regression of the state’s obligations regarding the exercise of the judiciary’s functions. State authorities could argue that the problem lies not in the state actions but in the manner in which the PSS indicators were developed or in the current inaccessibility of data due to lacking sources of information. Accepting this argument, the future failure to develop the necessary sources of information to address the requirements of the PSS and other reporting mechanisms would expose the State parties’ inaction to abide by its international obligations for the realization and protection of human rights.
Two additional remarks should be made. First, the WGPSS, like other committees and follow-up mechanism, does not compare countries nor does it establish a ranking among them. Each country is a unit of analysis itself. Second, through this exercise, the WGPSS is setting the baseline and in 2019 will be able to measure progressivity for all State parties.
Meanwhile, in terms of citizen and civil society participation, access and dissemination of information on PSS goals is a tool to promote government accountability. In this regard, the WGPSS insists that civil society organizations and specialized agencies submit reports in order to contribute information to the mechanism. Such information provided by civil society organizations is a powerful instrument to contrast the official data presented by states.
Conclusion
The article described the mechanism for monitoring social rights in the Americas, focusing on the cross-cutting indicator of access to justice in relation to the right to health. Then, it analyzes of the reports submitted by seven countries, evidencing the contrast between the indicators requested and the information submitted. The challenges, deficits, and potentialities of this mechanism were also identified.
The main findings of the experience analyzed refers to two substantive aspects. First, it addresses the centrality of monitoring access to justice in the broad sense that has been defined in the indicators, since it is normally not considered a “piece of information” generally informed by the public administration. Repeatedly, rights are included in governmental speeches and to a lesser extent are used to justify programs and policies, more often than not in an improper and narrative manner, without including its minimum standards. In particular, there is a lack of recognition regarding the need to “enable” access to justice. The mere fact that the State parties have not been able to provide information in a national compliance report—even though such information could often be available—is an indication of the deficiency in the state capacities and accountability and the lack of any record regarding the justiciability of ESCR. In other cases, the delay in the resolution of lawsuits from one forum to another also demands an explanation which as of today is not available.
The second aspect to be noted refers to the importance to reinforce and improve the forms of measurement of compliance with rights. The possibility of including empirical evidence to measure progression as an essential standard for evaluating judicial action has the power to correct the “case by case” practices and move towards mechanisms that examine the health system in its entirety and promote its adjustment to constitutional and international standards. The preparation of the national report based on progress indicators questions not only the ministries of foreign affairs, but also forms an interjurisdictional instance (that is, a collaborative work among different ministries), as some states are beginning to develop. This procedure surpasses the “mere compliance report” and constitutes a fundamental step to treating the right to health in a comprehensive manner.
In other words, access to justice to enhance the right to health requires not only an evaluation of the rules of procedure that could favor or limit the models of judicial intervention, or even the availability of empirical evidence through new sources of information. Rather, access to justice could be served by a monitoring process based on indicators showing the need to implement a wide discussion agenda regarding the institutional designs that have an impact on the possibility of the courts and the judicial tribunals of complying with a relevant role in the control of governmental policies.[28] In this sense, the experience initiated by the PSS monitoring system, which is to be strengthened in the years to come, will contribute to a better understanding of the necessary system of protection of rights, based on empirical information. Therefore, the regular use of indicators as a mechanism of state control will enable the design of rights-based public policies.
The regional experience shows that many collective cases allowed structural problems of the health sector to be handled more adequately, and in some cases, enabled a better transfer between the judicial decision and the political system. Having information available and evaluating the state’s actions is an indispensable condition to guaranteeing better health policies. Progress indicators are presented as connecting vessels between the organization of the health sector and access to justice in a feedback that strengthens rather than obstructs channels of cooperation with the essential participation of the citizens and rights-holders.
Laura Cecilia Pautassi, PhD, is a researcher for the Scientific and Technical Research Council (Consejo de Investigaciones Científicas y Técnicas (CONICET) in Buenos Aires, Argentina, a tenured researcher at the Ambrosio Gioja Legal and Social Research Institute (Instituto de Investigaciones Jurídicas y Sociales A. Gioja) in Buenos Aires, Argentina, and a professor at the University of Buenos Aires/UBA Law School, Buenos Aires, Argentina.
Please address correspondence to laurapautassi@derecho.uba.ar.
Competing interests: None declared.
Copyright © 2018 Pautassi. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1]. P. Hunt, Economic, social and cultural rights. Report of Special Rapporteur on the right to everyone to enjoy the highest possible level of physical and mental health, UN Human Rights Committee, Doc E/CN. 4/2006/48 (March 3, 2006), K. Tomaševski, Human rights obligations: making education available, accessible, acceptable and adaptable”, Education Primers, Nº 3, (Gothenburg, Sweden: Novum Grafiska AB, 2001).
[2]. UN Office of the High Commissioner for Human Rights, Report on Indicators for Promoting and Monitoring the Implementation of Human Rights, UN Doc. No. HRI/MC/2008/3 (2008); and UN Office of the High Commissioner for Human Rights, Human Rights Indicators. A Guide to Measurement and Implementation. UN Doc. No. HR/PUB/12/5 (Geneva and New York, 2012).
[3]. Organization of American States, Standards for the preparation of the periodic reports pursuant to the Protocol of San Salvador, AG/RES 2074 (XXXV-O/05).
[4]. Protocol of San Salvador: Working Group. http://www.oas.org/en/sare/social-inclusion/protocol-ssv/working-group.asp
[5]. National state reports to the WGPPS (in Spanish). Available at: http://www.oas.org/es/sadye/inclusion-social/protocolo-ssv/
[6]. V. Abramovich and L. Pautassi, The measurement of rights in social policies, (Buenos Aires: Editores Del Puerto, 2010) contains text that refers to the definition of indicators on a regional level.
[7]. In accordance with the Resolutions of the General Assembly of the OAS: AG/RES. 2713 (XLII-O/12) and AG/RES. 2823 (XLIV-O/14) that approve progress indicators.
[8]. See http://www.oas.org/en/sare/social-inclusion/protocol-ssv/docs/pssv-indicators-en.pdf
[9]. The Mechanism for Monitoring of the Inter-American Convention to prevent, eradicate and penalize violence against Women, http://www.oas.org/es/mesecvi/
[10]. A.Yamin and Ó. Parra-Vera, “Judicial Protection of the Right to Health in Colombia: From Social Demands to Individual Claims to Public Debates”, Hastings Int’l & Comp. L. Rev. 33 (2010): 431;.
[11]. Constitution of the Republic of Ecuador, 2008. Title III.
[12]. Constitution of the Republic of Ecuador, 2008. Article 193.
[13]. Republic of Ecuador, Compliance report of the Protocol of San Salvador, First group, permanent mission of Paraguay to the OAS, (Washington, DC: April 25, 2016), p. 24.
[14]. Constitution of the Republic of Ecuador, 2008. Articles 75 and 76, paragraph 7, literal k and m).
[15]. Inter-American Court of Human Rights. Case Gonzales Lluy vs Ecuador. Available at: http://www.corteidh.or.cr/docs/casos/articulos/seriec_298_esp.pdf
[16]. Ministry of Justice, Human Rights and Cults. https://www.justicia.gob.ec/en-caso-gonzalez-lluy-el-estado-ecuatoriano-ha-emprendido-acciones-para-garantizar-acceso-a-la-salud-incluso-antes-del-fallo-de-la-corteidh/
[17]. Republic of Ecuador, op cit, 2016:33.
[18]. Constitution of El Salvador, XXXX. Article 65.
[19]. Amparo 310-2013
[20]. Referencia
[21]. In the database of the Diagnostic contained in the National Human Rights Program 2014-2018, Mexico, cited in Mexico, 2014 op. cit.
[22]. Constitution of the Republic of Paraguay, XXX. Article 68.
[23]. Constitution of the Republic of Paraguay, XXX. Article 70.
[24]. Republic of Paraguay, Compliance Report of the Protocol of San Salvador, First Group, permanent mission of Paraguay to the OSA, Washington DC, June 9, 2015. Available at http://www.oas.org/es/sadye/inclusion-social/protocolo-ssv/docs/informe-consolidado-paraguay.pdf.
[25]. Paraguay, Anti-corruption secretary. http://www.denuncias.gov.py/ssps/.
[26]. Paraguay, General Direction of Human Rights. http://www.derechoshumanos.gov.py/
[27]. Paraguay, Justice Department. https://www.paraguay.gov.py/poder-judicial
[28]. A. Yamin, “Taking the right to health seriously: implications for health systems, courts, and achieving universal health coverage.” Human Rights Quarterly 39 (2017), pp. 341–368.