From International Commitments to Local Practice: Examining Staff Attitudes Toward Human Rights in Lithuanian Mental Health Care Facilities
Vol 28/1, 2026, pp. 125-139 PDF
Ugnė Grigaitė, Gintaras Šumskas, Eglė Šumskienė, Karilė Levickaitė, Jurga Mataitytė-Diržienė, and Jūratė Charenkova
Abstract
This study explores the attitudes of mental health care professionals in Lithuania toward human rights principles, provisions, and standards as defined by the United Nations Convention on the Rights of Persons with Disabilities (CRPD) and their application in mental health care. Employing a mixed-methods convergent design, the study integrates survey data (n = 390) with qualitative findings from six focus groups with professionals and service users (n = 36). The results reveal notable differences across professional roles, institutional settings, and experience levels. Medical psychologists consistently demonstrated more human rights-supportive attitudes, while nurse assistants and professionals in large inpatient facilities were more likely to endorse coercive practices and question the full implementation of rights in practice. Additionally, mid-career professionals and those working in smaller facilities expressed greater openness to reform and the practical utility of the CRPD. Qualitative findings further highlighted systemic barriers such as stigma, biomedical dominance, and resource constraints. These findings underscore the importance of targeted training, institutional reform, and sustained political will to align Lithuania’s mental health care services with international human rights standards. Further longitudinal research is warranted to examine how attitudes toward human rights in mental health care evolve, especially in response to policy changes, reforms, and targeted training initiatives.
Introduction
Across the world, people with mental health conditions or psychosocial disabilities often face stigma, discrimination, and limitations on their political, civil, social, and economic rights.[1] Fostering their human rights is essential to advancing overall well-being. Mental health care professionals have a key role in this process: They are responsible for ensuring that human rights principles guide mental health care interventions.[2] In light of recent global crises affecting health, economic stability, and social justice, it is more important than ever to recognize and prioritize the rights of persons who use mental health care services.[3]
The United Nations Convention on the Rights of Persons with Disabilities (CRPD) has significantly reshaped the global understanding, implementation, and protection of the rights of people with psychosocial disabilities.[4] Its core aim is to ensure that all individuals with mental health conditions and disabilities fully and equally enjoy their human rights and fundamental freedoms, while also promoting respect for their inherent dignity.[5]
Although human rights in mental health care have only recently begun to receive broader recognition, their importance is increasingly acknowledged across the world.[6] While human dignity is a foundational principle, research indicates that it is not always safeguarded or promoted within mental health systems and services.[7] The World Psychiatric Association has highlighted the protection of human rights in mental health care as one of its primary concerns.[8]
In the past decade, growing recognition of the rights of persons with mental health conditions and psychosocial disabilities has brought traditional psychiatric practices under scrutiny.[9] A key point of contention within the human rights community is whether coercive interventions, such as involuntary hospitalization and treatment, can ever be considered compatible with human rights standards.[10] Some mental health care professionals and advocates argue that such practices may be justified if they are necessary, proportionate, and implemented with strong legal safeguards.[11] Others maintain that coercion is inherently a violation of human rights and can never be justified.[12] This ongoing debate has led to a significant standstill in the human rights discourse, often referred to as the “Geneva impasse.”[13] A relatively new direction in academic research on the promotion of human rights in mental health care may offer a way to resolve this impasse, which has dominated discussions in the field in recent years.[14]
In the case of Lithuania, the government ratified the CRPD and its Optional Protocol in 2010, prompting significant legal and systemic reforms, including updates to quality standards for services within the health care system. A clear political commitment to improving mental health care and protecting human rights is reflected in the 19th Government Program of 2024. These priorities are further embedded in national development strategies, which outline specific targets to be achieved by 2030. Key goals include strengthening mental health literacy, combating stigma, improving primary-level mental health care, expanding and diversifying specialized outpatient services, and streamlining inpatient care. According to the Ministry of Health, these objectives are central to the ongoing reform of Lithuania’s health care sector.
Since 2021, Lithuania has been conducting human rights monitoring in mental health care facilities using the QualityRights methodology of the World Health Organization (WHO), which aims to support countries in reforming their health care systems to be more person-centered, recovery-oriented, and respectful of human rights.[15] The initiative aims to drive lasting change in attitudes and practices, empowering stakeholders to promote dignity, rights, and recovery for individuals with mental health conditions and disabilities.[16] In 2023, Lithuania’s Ministries of Health and Social Security and Labor adopted official guidelines for assessing, monitoring, and providing methodological support to ensure that mental health and social care services meet human rights standards, demonstrating a firm national commitment to improving both the quality of services and the protection of human rights.
Although some progress has been made globally, stigmatizing attitudes and human rights violations continue to occur within mental health care facilities.[17] Across many countries, mental health care professionals face significant barriers to implementing practices grounded in human rights, often working within systems shaped by paternalistic values. For example, in Spain, mental health care professionals cite a lack of financial and human resources, limited social support, and the persistence of paternalistic and biomedical models as key obstacles to upholding service users’ human rights; they also identify stronger professional training as a potential pathway to address these issues.[18] Across South American countries, progress has been made in reducing coercive practices, but further improvements in service quality are still needed.[19] Recognizing the role of human rights in supporting the well-being of both service users and professionals is essential for advancing these standards. In India, implementing new mental health legislation faces major hurdles due to underfunded services, insufficient social support, and a shortage of trained personnel; sustained political will is critical to improving care quality and protecting human rights.[20]
On a global scale, achieving human rights-based mental health care requires much broader and ongoing commitment from health care providers, families, social stakeholders, policy makers, and the wider public.[21] Emerging evidence suggests that professionals’ attitudes play a critical role in shaping everyday practices, including the use of coercion, respect for autonomy, and support for decision-making. Studies have shown that stigmatizing or paternalistic attitudes among mental health professionals are associated with the persistence of rights-restrictive practices, whereas more rights-oriented attitudes are linked to improved quality of care and recovery-oriented approaches.[22] Studies have shown that personal attitudes and socially constructed norms strongly influence whether professionals intend to apply human rights principles and standards in their work.[23] As a result, mental health care practitioners frequently encounter challenges when striving to uphold human rights in their day-to-day practice.[24]
In Lithuania, too, despite recent progress and initiatives, deeply entrenched stigmatizing attitudes continue to pose a major barrier to the effective realization of the rights of people with mental health conditions and psychosocial disabilities. This issue is particularly evident in national assessments of the mental health care system.[25] A study commissioned by the Mental Health Centre at the Lithuanian Institute of Hygiene found that discriminatory and human rights-averse views are still widespread among the general public and mental health care professionals.[26]
Until the present study, no research in Lithuania had specifically examined mental health care professionals’ attitudes toward human rights principles or their implementation in practice. Our study addresses that gap by evaluating these professionals’ views on human rights in everyday service delivery. Lithuania’s mental health system is undergoing a transition from institutional to community-based care, reflecting broader dynamics seen in Central and Eastern Europe. That said, rather than aiming for direct generalizability, the study contributes to the limited empirical evidence on how professionals’ attitudes are shaped by training, institutional culture, and reform processes, while offering context-sensitive insights to inform comparative research on the barriers and enabling conditions affecting human rights implementation.
The specific objectives of this paper are as follows:
- to evaluate how mental health care professionals perceive the principles, provisions, and standards for ensuring human rights as defined by the CRPD, and how these are applied within mental health care services;
- to assess professionals’ attitudes toward potential reforms in mental health care services, whether organizational, managerial, or clinical, that would bring practices into greater alignment with the CRPD principles, provisions, and standards; and
- to explore the associations between, on the one hand, professionals’ attitudes toward human rights and service reforms and, on the other, their sociodemographic characteristics, as well as the organizational features of the facilities in which they work.
Methods
Study design
We utilized a convergent mixed-methods design.[27] The quantitative component involved a survey administered online, by telephone, and in person by the market research company RAIT.[28] It provided statistical insights into the prevalence and patterns of human rights implementation and professionals’ attitudes. The qualitative component was exploratory and grounded in an experiential framework.[29] It included six focus group discussions with mental health care professionals and service users, as well as open-ended questions within the survey.[30] Including qualitative methods enabled a deeper investigation of participants’ attitudes and the underlying reasons behind the quantitative findings.[31] They also captured subtle systemic and sociocultural dynamics, as well as other human factors, that numbers alone may not reveal.[32]
This paper is part of a broader study titled “Protection of Human Rights in Mental Healthcare Facilities,” for which the research team developed a methodology based on the human rights standards outlined in the CRPD, along with relevant tools from the WHO QualityRights initiative.[33]
Survey
Drawing on the CRPD and the methodological tools developed under the WHO QualityRights initiative, we developed a survey questionnaire consisting of 30 closed-ended questions and two open-ended questions. Ten questions were dedicated to collecting sociodemographic and workplace-related data; another 10 questions were formulated to evaluate participants’ knowledge of relevant human rights principles, provisions, and standards, as well as their relevance to mental health care; and a further 10 questions were used to evaluate participants’ attitudes toward human rights and reforms in mental health care services. (Supplementary materials are available from the authors, including Supplementary Table 1 on the collected sociodemographic and workplace-related data, and Supplementary Tables 2, 3, and 4 on the specific questions and attitudinal statements presented in the survey.)
Additionally, the two open-ended questions in the survey asked participants, “What do you know about the CRPD, and what are its key principles, provisions, and standards relevant to providing mental health care services?” and “What should be changed or improved first and without delay in the provision of mental health care services in Lithuania to implement human rights?”
For the specific analysis presented in this paper, we drew on the responses to 20 closed-ended questions, including 10 sociodemographic questions, and one open-ended question. These were the questions focused specifically on participants’ “attitudes” rather than their “knowledge.”
We collected the data using three survey formats:
- Online survey: Participants completed the questionnaire independently online. The survey was distributed through email invitations sent to health care institutions and representatives of target groups; links shared in professional social media groups; phone calls to health care institutions inviting participation; and snowball sampling.
- Telephone survey: Participants were contacted directly and invited to answer the questionnaire over the phone. Trained interviewers read the survey questions aloud and recorded participants’ responses in real time. This format helped reach professionals who may not have had access to or who preferred not to use the online format.
- Self-administered paper-based survey: Participants completed printed questionnaires independently. Paper surveys were delivered to staff representatives of several hospitals, who then distributed them to members of the target group.
Focus groups
The fifth and sixth authors conducted six focus group discussions (FGDs), each involving an average of six participants, for a total of 36 participants. We used FGDs as a qualitative method to explore participants’ experiences, perceptions, and opinions in greater depth, allowing for a detailed examination of key themes and the underlying factors shaping them.
Five FGDs were conducted online with mental health care service providers via Microsoft Teams platform. One FGD with service users was held in person in Vilnius. Although the primary focus of the study was on professionals’ attitudes, the inclusion of service users helped contextualize those attitudes by relating them to lived experiences of care and to the everyday realization of human rights within mental health services.
We used purposive sampling to select FGD participants, which helped ensure a diverse representation of service providers across different institutions, professions, levels of care (inpatient and outpatient), and geographic regions. Professionals from Vilnius, Kaunas, Klaipėda, Alytus, Šiauliai, and Panevėžys took part. We recruited participants through email and telephone. The service user group included individuals with at least five years of experience using mental health services and who reported no recent deterioration in their mental health at the time of the study. (Participants’ sociodemographic information is summarized in Supplementary Table 5, available from the authors).
The FGDs lasted approximately 90 minutes each and took place between October and November 2024. They were guided by a semi-structured protocol that included a set of guiding questions but allowed facilitators flexibility when participants introduced personally meaningful topics. In such cases, the conversation was allowed to flow naturally before being gently steered back to the core discussion points. Throughout the sessions, the research team made conscious efforts to foster a psychologically safe and supportive environment. The facilitators acted as active listeners, using questions primarily to encourage reflection, clarify responses, and guide the dialogue, while prioritizing participants’ voices and experiences.
All discussions were audio-recorded, transcribed verbatim, and analyzed using reflexive thematic analysis.
Quantitative data analysis
We analyzed the survey data to examine relationships between participants’ attitudes toward mental health care practices and human rights, particularly in the context of Lithuania’s implementation of the CRPD. We assessed responses by gender, age, professional experience, workplace location, and institution type and size. Descriptive statistics included absolute (n) and relative (%) frequencies for categorical variables. We tested bivariate associations using the chi-square or Fisher’s exact tests, as appropriate. Our main method was binary logistic regression, in which 10 attitudinal statements served as dependent variables and were dichotomized into agreement versus non-agreement. We included sociodemographic and workplace characteristics as independent variables and estimated odds ratios (Exp(b)). We applied a significance level of α = 0.05 and conducted analyses using SPSS.
Qualitative data analysis
We conducted a reflexive thematic analysis of the qualitative survey data and focus groups using the MAXQDA software. The first author repeatedly reviewed the open-ended responses and transcripts, coded text segments, and organized them into themes using an inductive approach. We then formulated and reviewed the themes as a team, discussing and refining them in light of emerging patterns both within and across thematic categories.
Data integration strategy
In this mixed-methods study, we employed a convergent data integration strategy to ensure a comprehensive understanding of the research topic. We collected and analyzed quantitative and qualitative data separately but concurrently and brought together the findings during the interpretation phase. This allowed us to compare, contrast, and complement statistical patterns with narrative insights, enriching the overall analysis. Integration took place at the level of interpretation and discussion, where themes emerging from FGDs and open-ended survey responses were used to contextualize and explain trends observed in the quantitative data.
This strategy facilitated a more nuanced exploration of human rights implementation in mental health care facilities, ensuring that both measurable outcomes and the lived experiences of participants informed our conclusions.
Research team and reflexivity
The authors of this study contribute a diverse range of personal and professional expertise spanning the fields of human rights, mental health, disability, public health, health care service evaluation, academic scholarship, and civic activism. Several of us have been directly involved in advancing the rights of persons with mental health conditions and psychosocial disabilities in Lithuania, including through work on deinstitutionalization, monitoring human rights conditions in mental health and social care institutions, and advocacy related to the implementation of the CRPD. This multidisciplinary background is a key asset, consistent with the principles and values of qualitative research, which acknowledge and harness researchers’ subjectivity as an integral part of the research process. Rather than aiming for neutrality, we acknowledge that our perspectives shape how data are collected, interpreted, and understood.[34]
The study is therefore informed by a shared commitment to a human rights-based and recovery-oriented approach to mental health care, taking a critical stance toward practices that restrict autonomy, such as involuntary treatment, institutionalization, and limits on legal capacity. These normative commitments shaped how we interpreted concepts such as risk, care, and protection and may have influenced the analysis, particularly when examining practices normalized within psychiatric systems. At the same time, our experience within and alongside mental health services fostered awareness of the structural, legal, and ethical constraints faced by professionals. This dual positioning—both critical of and engaged with these systems—enabled the examination of tensions between human rights standards and everyday clinical practice without reducing them to individual attitudes alone.
We actively practiced reflexivity throughout the research process. We engaged in ongoing discussions to examine how our values, assumptions, and professional positions shaped data collection, coding, and interpretation. Particular attention was given to moments where participants’ perspectives diverged from our own, ensuring that these views were presented accurately even when they did not fully align with a human rights-based analytical framework. This approach balanced a critical human rights lens with methodological rigor, transparency, and respect for the field’s complexity.
Research ethics
All research participants provided their informed consent to participate. All personal information and any data shared by participants in the survey or during the focus groups were treated as strictly confidential and were accessible only to members of the research team involved in data collection and analysis.
To protect participants’ privacy, we do not use the real names of individuals, locations, or institutions in this paper or any other publications arising from the study. When describing participants, we provide only general sociodemographic information.
Ethical approval for the study was obtained from the Ethics Committee for Research Compliance of the Institute of Sociology and Social Work and the Institute of Educational Sciences, Faculty of Philosophy, Vilnius University (Protocol No. (1.13E)250000-KT-162, September 25, 2024).
Results
Quantitative results
A total of 390 mental health care professionals participated in the survey, including psychiatrists, medical psychologists, social workers, nurses and nurse assistants working in the mental health care sector. Of these, 89 participants completed paper-based questionnaires, 84 participated via telephone interviews, and 217 filled out the online survey.
Figure 1 shows the general distribution of attitudinal statements and their evaluation by professional group.
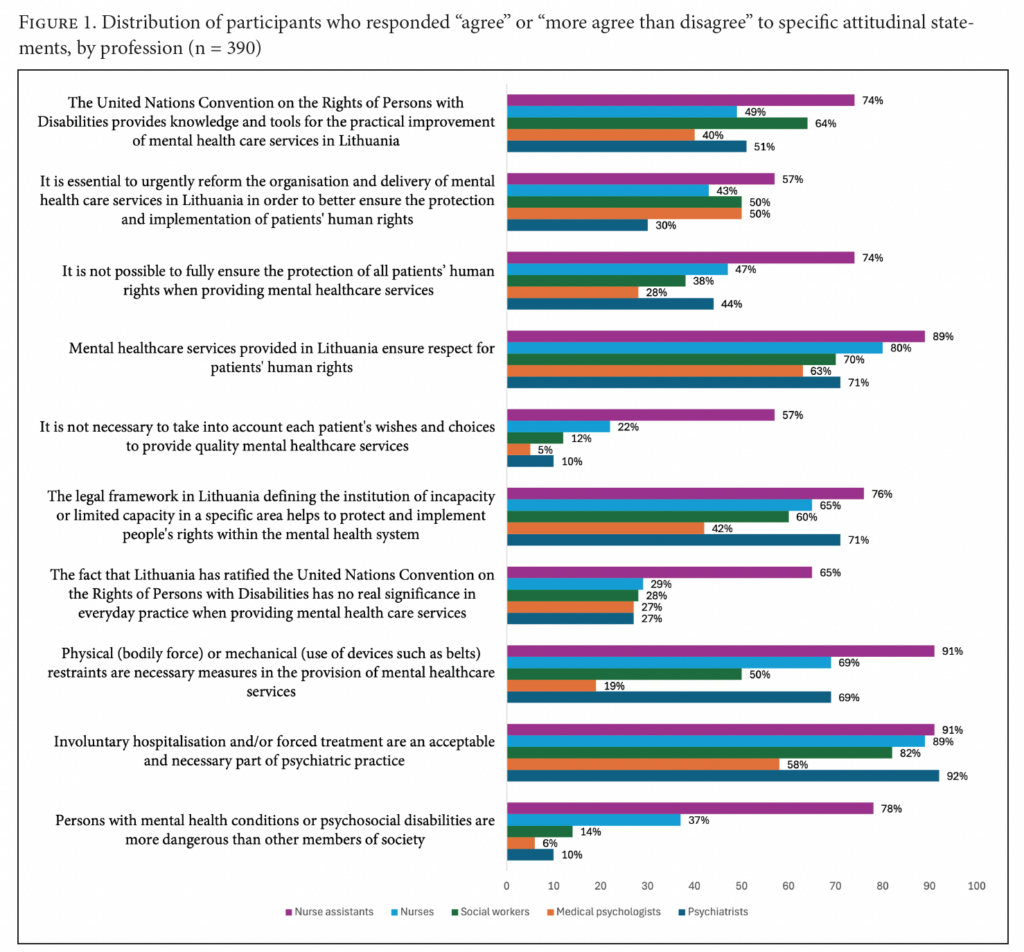
Statistically significant results reveal that medical psychologists show the lowest agreement with stigmatizing or coercive practices, such as the belief that people with psychosocial disabilities are dangerous (Exp(b) = 0.116, p < 0.0001) or that involuntary treatment and restraints are necessary (Exp(b) = 0.107, p < 0.0001). Psychiatrists and social workers also demonstrate lower agreement with stigmatizing views in some cases. In contrast, nurses (Exp(b) = 2.225, p = 0.019) and nurse assistants (Exp(b) = 4.719, p = 0.005) are more likely to agree with statements endorsing coercive measures, such as the use of physical or mechanical restraints.
Professionals working in public psychiatric inpatient settings are more likely to support coercive measures and hold stigmatizing views (Exp(b) = 2.877, p = 0.001). In contrast, those based in public mental health centers tend to disagree with such statements (Exp(b) = 0.353, p = 0.001). Staff in institutions with more than 200 beds are more likely to perceive persons with mental health conditions as dangerous (Exp(b) = 6.274, p < 0.001) and see physical or mechanical restraints as necessary (Exp(b) = 3.221, p < 0.001). Further, professionals in institutions with more than 200 beds (Exp(b) = 2.524, p = 0.016) and those in institutions with more than 200 employees (Exp(b) = 2.929, p = 0.012) are more likely to support restrictions on people’s legal capacity.
Those with 6–10 years of professional experience are significantly less likely to agree with the need for involuntary hospitalization (Exp(b) = 0.224, p = 0.001). Professionals aged 26–35 are less likely to believe that the ratification of the CRPD has no practical significance (Exp(b) = 0.318, p = 0.036). Professionals from larger facilities are more likely to agree with statements suggesting a limited impact of the CRPD (Exp(b) = 2.524, p = 0.016) and the need for coercive measures (Exp(b) = 3.221, p < 0.001).
Moreover, results show that medical psychologists consistently express more rights-oriented views. They are significantly less likely to agree with statements suggesting that patient choices are not essential for quality care (Exp(b) = 0.195, p = 0.003), that human rights are already well protected in Lithuania (Exp(b) = 0.427, p = 0.008), or that full human rights protection in practice is impossible (Exp(b) = 0.438, p = 0.007). On the contrary, nurse assistants show higher agreement with more skeptical or system-supportive statements across multiple areas, including the perceived impossibility of fully ensuring human rights (Exp(b) = 3.158, p < 0.000) and believing that it is not necessary to take into account each patient’s wishes and choices in order to provide quality mental health care services (Exp(b) = 4.689, p < 0.000).
Qualitative results
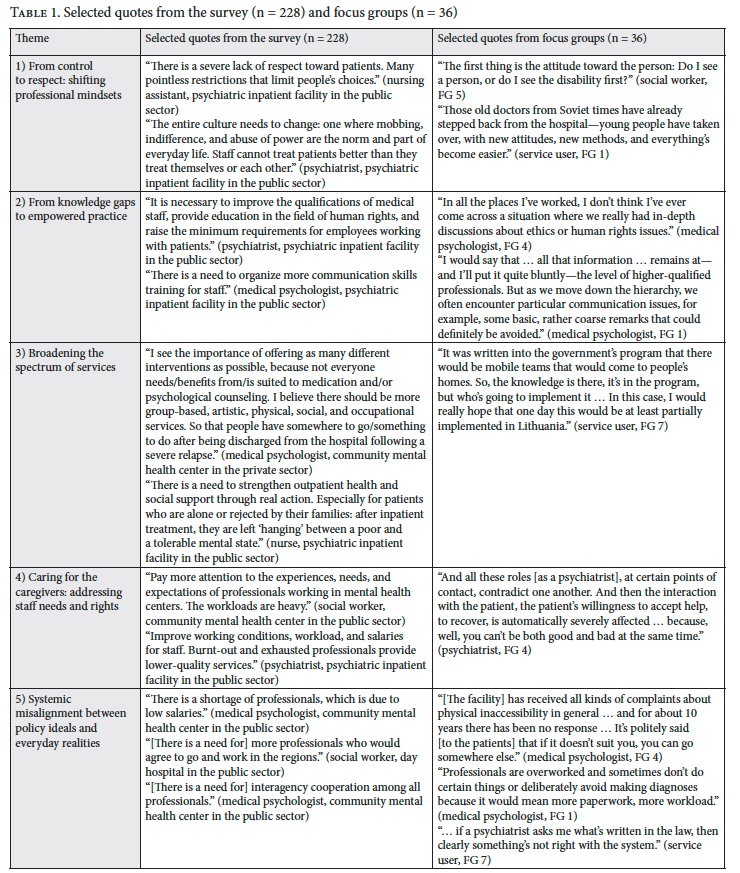
Some survey participants (n = 228) provided their opinions on what should be changed or improved in the provision of mental health care services in Lithuania to implement human rights. Our analysis of their answers in conjunction with the results of the six focus groups revealed five main themes:
- From control to respect: shifting professional mindsets
- From knowledge gaps to empowered practice
- Broadening the spectrum of services
- Caring for the caregivers: addressing staff needs and rights
- Systemic misalignment between policy ideals and everyday realities
Themes
- From control to respect: shifting professional mindsets
The first theme captures a critically needed transformation identified by both professionals and service users in the study. Rather than merely describing attitudes, this theme reveals how these attitudes are actively constructed and negotiated within institutional cultures. Many professionals acknowledged the need to move away from paternalistic attitudes and toward a human rights-based approach in mental health care. This includes rethinking the culture of care, reducing stigma, and promoting respect in everyday interactions with patients and colleagues alike. Participants highlighted the limited autonomy often experienced by service users, calling for greater involvement in care planning, supported decision-making, and the recognition of their preferences. These accounts illustrate a tension between normative commitments to human rights and the persistence of routinized practices that limit autonomy.
Service users, in turn, pointed to persistent gaps in the system, such as professionals’ lack of competence in communicating legal rights. The quality of care, as perceived by service users, varies significantly between facilities, with some settings demonstrating exemplary communication and shared decision-making. This variability underscores the uneven translation of human rights principles into practice across different institutional contexts.
Many service users also underscored the importance of generational change in the medical workforce, expressing hope that younger professionals would bring more progressive attitudes. Practices such as physical restraint in hospitals were described with fear and disapproval, further reinforcing the demand for humane, empowering, and rights-based approaches.
- From knowledge gaps to empowered practice
The second theme highlights a persistent disconnect between human rights principles and their practical application in mental health care, rooted in the fragmented education of professionals. This theme extends beyond identifying knowledge gaps by demonstrating how limited or informal knowledge translates into inconsistent and sometimes contradictory practices. While professionals across disciplines acknowledged the importance of human rights, many lacked a clear understanding of the CRPD, with most learning about it only through informal channels, occasional training, or workplace audits.
Psychiatrists, psychologists, and nursing staff frequently operate without explicit reference to the CRPD, often relying on ethical intuition rather than structured knowledge. This reliance on individual judgment contributes to variability in practice and reflects the absence of a shared, system-wide human rights framework. As a result, rights such as informed consent, privacy, freedom from coercion, and access to appropriate care are not consistently upheld.
Professionals strongly emphasized the need for targeted, ongoing education for all staff, especially for older professionals and nursing personnel, as well as the need to embed the CRPD into institutional policies, job regulations, and academic curricula. Despite these challenges, some professionals (particularly social workers and nurses) demonstrated proactive engagement by independently organizing training and promoting awareness. These examples highlight the presence of agency and bottom-up efforts for change, even within structurally constrained environments.
- Broadening the spectrum of services
The third theme reflects a strong call from both professionals and service users for more diverse, accessible, and person-centered mental health care services. It illuminates how current service limitations directly shape experiences of exclusion, dependency, and restricted choice. Professionals emphasized the need to expand day hospital options, outpatient services, and continuous services (particularly in underserved regions) and to strengthen interdisciplinary, team-based care models.
There was a shared emphasis on increasing the availability of nonmedical interventions, such as psychotherapy and social support, especially for individuals for whom medication is not appropriate.
Service users expressed a desire for more holistic and recovery-oriented services, highlighting the value of emotional support, non-pharmacological treatments, and therapeutic options that foster inclusion, autonomy, and dignity.
These perspectives demonstrate that the realization of human rights is closely linked to the availability and diversity of services rather than solely to individual professional attitudes. Participants also emphasized the value of drawing on international promising practices, such as mobile crisis teams that provide home-based support to the entire family, thereby reducing the need for hospitalization and preserving the individual’s social environment.
- Caring for the caregivers: Addressing staff needs and rights
This theme highlights the significant challenges faced by mental health care professionals in safeguarding both patient rights and their own well-being. The findings demonstrate that professionals’ attitudes and practices cannot be understood in isolation from the conditions under which they work.
Participants across professions reported overwhelming workloads, low pay, high burnout risk, unclear professional boundaries, and a lack of systemic support. Psychiatrists described the moral and professional dilemmas arising from being tasked with both therapeutic and legal responsibilities, such as participating in court proceedings related to forced treatment or legal capacity, undermining their trust-based relationship with patients.
Psychologists and social workers saw themselves as advocates and intermediaries for service users, often compensating for systemic gaps in rights protection, yet felt limited in their power to influence decisions or systemic reforms. Social workers emphasized their role in promoting human rights and social inclusion but noted increasing marginalization within interdisciplinary teams. Nurses, who spend the most time with patients, offer vital emotional and practical support, yet their role is often undervalued in discussions about rights-based care.
- Systemic misalignment between policy ideals and everyday realities
Participants identified a broad spectrum of systemic gaps that hinder the effective realization of human rights principles within mental health care services. This theme synthesizes how structural factors mediate the relationship between formal commitments to human rights and their practical implementation.
Despite policy advances and formal frameworks inspired by the CRPD, everyday practice remains fragmented and inconsistent across institutions and professionals. Key systemic challenges include chronic shortages of human and financial resources, lengthy waiting times, uneven regional service accessibility, insufficient intersectoral collaboration, data management issues, and confidentiality concerns.
While some psychiatrists noted regulatory changes and human rights audits as steps forward, many felt that these did not translate into palpable improvements in patient care. Psychologists and social workers similarly acknowledged growing awareness and training on mental health and human rights, while noting that practical application on the frontline often falls short, with lingering stigma and discriminatory attitudes affecting treatment decisions. Nurses observed positive shifts in privacy, communication, and patient-centered approaches, although these were seen as unevenly implemented. Participants also pointed to structural barriers, such as a lack of physical and informational accessibility and the complex dilemmas around legal capacity, where rights such as voting are retained symbolically while broader autonomy is restricted.
Taken together, these findings demonstrate that gaps in human rights implementation are not solely due to individual attitudes but are deeply embedded in systemic, organizational, and policy-level misalignments. Table 1 presents selected quotes illustrating each of the five themes.
Discussion
This mixed-methods study aimed to explore and assess the attitudes of mental health care professionals in Lithuania toward human rights defined in the CRPD and their application in mental health care settings. This is the first empirical study in the country to examine how professional, institutional, and sociodemographic factors influence these attitudes. Importantly, the integration of qualitative and quantitative findings allows for a more comprehensive understanding of not only what attitudes are held but also how they are constructed, negotiated, affected, and enacted within everyday practice contexts.
The study shows that profession is one of the strongest predictors of mental health care professionals’ attitudes toward patients’ human rights. Medical psychologists show the lowest agreement with stigmatizing or coercive practices, such as beliefs that people with psychosocial disabilities are dangerous or that involuntary treatment and restraints are necessary. Psychiatrists and social workers also demonstrate lower agreement with stigmatizing views in some cases. In contrast, nurses and nurse assistants are more likely to endorse coercive measures, including the need for physical or mechanical restraints.
These results are consistent with other studies, where mental health care professionals with psychological or social work training have often shown more rights-aligned attitudes, likely reflecting their training in person-centered and recovery-oriented approaches.[35] Conversely, nurses are more likely than other professionals to support coercive practices, possibly due to their frontline roles in enforcing such measures and feelings of unsafety.[36] In line with global trends, this underscores the need for targeted, specialized rights-based training, including de-escalation techniques, across professions in both academic curricula and continuous professional development.[37] The qualitative findings support this division: Professionals and service users emphasize ending paternalistic practices, fostering supported decision-making, and recognizing physical restraints as harmful, while pointing to an urgent need for humane, rights-based approaches. Beyond reinforcing quantitative patterns, these insights show how professional roles are embedded in everyday moral reasoning, highlighting tensions between care, control, and responsibility that sustain coercive practices and demonstrating that attitudes are actively negotiated within institutional and relational contexts.
Generational differences are also evident, with younger professionals less likely to believe that ratification of the CRPD has no practical significance, indicating greater sensitivity to international human rights commitments. This is contrary to some former studies, where older staff expressed lower support for coercive practices.[38] In the present study, service users expressed optimism about generational change in the workforce, linking it to more progressive attitudes and greater awareness of service users’ rights. Some findings may suggest that educational curricula are evolving to better incorporate human rights discourse, although this may also reflect broader societal changes in disability and inclusion. The qualitative data further deepen this insight, illustrating how generational shifts are experienced in practice through differences in communication styles, openness to shared decision-making, and willingness to question established hierarchies. This suggests that potential changes in attitudes are intertwined with broader cultural and systemic transformations rather than solely individual-level factors.[39]
The impact of years of professional experience revealed a nuanced pattern. Professionals with 16–20 years of experience demonstrated greater support for involuntary treatment and physical restraint, whereas those with 6–10 years of experience were less likely to endorse the need for involuntary hospitalization and other coercive measures. These findings are echoed in the qualitative data, where professionals spoke of heavy workloads, ethical dilemmas, and unclear professional boundaries, which may contribute to greater tolerance of coercive or expedient practices under the systemic pressure. The divergence observed in this study may reflect the influence of institutional culture, professional burnout, or changes in the policy environment over time.[40] Importantly, the qualitative findings illuminate the mechanisms underlying this pattern, showing how prolonged exposure to resource constraints and risk-management pressures can normalize coercive practices over time, not as a result of individual attitudes alone but as an adaptation to structural conditions.
Institutional context, including facility type and size, also shapes attitudes. In this study, professionals in public psychiatric inpatient settings were more likely to endorse coercive and stigmatizing views, while those in public mental health centers expressed more rights-supportive perspectives. This aligns with international findings showing that inpatient settings tend to foster more custodial attitudes, partly due to environmental stressors, high patient acuity, and risk-management pressures.[41] The qualitative data in this study provide critical insight into how these environments shape practice, with participants describing institutional routines, staffing shortages, and safety concerns that constrain the implementation of rights-based approaches, even when professionals express support for them.
Notably, staff in large institutions (i.e., those with more than 200 beds or employees) were more likely to simultaneously endorse both perceived legal protections and coercive measures, revealing a potentially contradictory stance. The qualitative data echoed this contradiction, with participants acknowledging a gap between legal frameworks and daily practices, shaped by fragmented services, regional disparities, and limited intersectoral coordination. This ambivalence has also been reported in other post-institutional reform contexts in Central and Eastern Europe, where human rights commitments coexist with long-standing institutional cultures and resource limitations.[42] Taken together, the qualitative and quantitative findings of this study suggest that this apparent contradiction reflects not only an attitudinal inconsistency but a systemic dissonance between policy-level commitments and practice-level realities. This underscores the importance of addressing structural conditions alongside professional attitudes.
Conclusion
In Lithuania, professionals’ attitudes toward human rights in mental health care vary meaningfully across professional roles, workplace sizes, and levels of experience. Medical psychologists and professionals in smaller institutions tend to support more rights-based approaches, while nurse assistants and those in larger facilities are more likely to endorse the current system or see limitations in the potential of human rights implementation.
These findings underscore the complex interplay between professional identity, institutional environment, and individual attitudes toward human rights in mental health care. They highlight the need for targeted interventions, such as professional training, institutional reform, and policy advocacy, to promote a stronger alignment with the principles of the CRPD. Future research should explore how specific institutional dynamics and professional development pathways influence the adoption of rights-based practices in mental health systems in different geographical and cultural environments. Moreover, further longitudinal research is warranted to examine how attitudes toward human rights in mental health care evolve, especially in response to policy changes, systemic reforms, and targeted training interventions.
Strengths and limitations
This is the first empirical study in Lithuania to examine mental health care professionals’ attitudes toward human rights principles enshrined in the CRPD, addressing a key gap in national and regional research. The convergent mixed-methods approach enabled a comprehensive understanding by integrating quantitative data with qualitative insights from focus groups. Including both professionals and service users enriched interpretation, while the inclusion of a broad range of professionals across different institution types and regions enhanced the relevance of the findings. Grounding the research in international human rights frameworks, particularly the CRPD and the WHO QualityRights initiative, further strengthened its conceptual and ethical foundation.
Despite the strengths, the study also has some limitations. Some professional groups or institutional types may be over- or under-represented. Moreover, all data were self-reported and may therefore have been influenced by social desirability bias, especially on sensitive topics such as coercion and stigma. In addition, the quantitative data were gathered using different formats (telephone, online, and self-administered paper questionnaires), which may have introduced interviewer effects or mode-related variations in how openly participants responded. Finally, some subsamples in the analysis were small, which may have affected the stability of statistical estimates in the logistic regression models.
Funding
This study was conducted as part of the project “Attitudes of Healthcare Facilities’ Employees Toward Human Rights Principles Based on the United Nations Convention on the Rights of Persons with Disabilities,” funded by the Public Health Promotion Fund administered by the Ministry of Health of the Republic of Lithuania (Ref. No. (1.78 MR) SU-1773/S-145) and implemented by Vilnius University together with the nongovernmental organization Mental Health Perspectives (www.perspektyvos.org).
Ugnė Grigaitė, PhD, is a project manager and researcher at Mental Health Perspectives, Vilnius, Lithuania, and an integrated member at the Comprehensive Health Research Centre, Lisbon Institute of Global Mental Health, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal.
Gintaras Šumskas, PhD, is an associate professor at Vytautas Magnus University, Kaunas, Lithuania.
Eglė Šumskienė, PhD, is a professor at the Institute of Sociology and Social Work, Faculty of Philosophy, Vilnius University, Vilnius, Lithuania.
Karilė Levickaitė, MA, is a director at Mental Health Perspectives, Vilnius, Lithuania.
Jurga Mataitytė-Diržienė, PhD, is an associate professor at the Institute of Sociology and Social Work, Faculty of Philosophy, Vilnius University, Vilnius, Lithuania.
Jūratė Charenkova, PhD, is an associate professor at the Institute of Sociology and Social Work, Faculty of Philosophy, Vilnius University, Vilnius, Lithuania.
Please address correspondence to Ugnė Grigaitė. Email: ugne.grigaite@nms.unl.pt.
Competing interests: None declared.
Copyright © 2026 Grigaitė, Šumskas, Šumskienė, Levickaitė, Mataitytė-Diržienė, and Charenkova. This is an open access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] A. A. Mahdanian, M. Laporta, N. Drew Bold, et al., “Human Rights in Mental Healthcare: A Review of Current Global Situation,” International Review of Psychiatry 35/2 (2023).
[2] C. A. A. Ventura, W. Austin, B. S. Carrara, and E. S. de Brito, “Nursing Care in Mental Health: Human Rights and Ethical Issues,” Nursing Ethics 28/4 (2021).
[3] J. Probert, “Moving Toward a Human Rights Approach to Mental Health,” Community Mental Health Journal 57/8 (2021).
[4] P. Harpur, “Embracing the New Disability Rights Paradigm: The Importance of the Convention on the Rights of Persons with Disabilities,” Disability and Society 27/1 (2012).
[5] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006).
[6] Human Rights Council, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN Doc. A/HRC/35/21 (2017); M. Funk and N. Drew, “WHO QualityRights: Transforming Mental Health Services,” Lancet Psychiatry 4/11 (2017); M. Funk and N. Drew Bold, “WHO’s QualityRights Initiative: Transforming Services and Promoting Rights in Mental Health,” Health and Human Rights 22/1 (2020).
[7] Ventura et al. (see note 2).
[8] H. Herrman, J. Allan, S. Galderisi, et al., “Alternatives to Coercion in Mental Health Care: WPA Position Statement and Call to Action,” World Psychiatry 2/1 (2022).
[9] M. Aragonés-Calleja and V. Sánchez-Martínez, “Evidence Synthesis on Coercion in Mental Health: An Umbrella Review,” International Journal of Mental Health Nursing 33/2 (2024); S. Every-Palmer, L. Kininmonth, G. Newton-Howes, and S. Gordon, “Applying Human Rights and Reducing Coercion in Psychiatry Following Service User-Led Education: A Qualitative Study,” Health and Human Rights 23/2 (2021).
[10] Aragonés-Calleja and Sánchez-Martínez (see note 9); M. Chieze, C. Clavien, S. Kaiser, and S. Hurst, “Coercive Measures in Psychiatry: A Review of Ethical Arguments,” Frontiers in Psychiatry 12 (2021).
[11] G. Danzer and A. Wilkus-Stone, “The Give and Take of Freedom: The Role of Involuntary Hospitalization and Treatment in Recovery from Mental Illness,” Bulletin of the Menninger Clinic 79/3 (2015).
[12] K. Sugiura, F. Mahomed, S. Saxena, and V. Patel, “An End to Coercion: Rights and Decision-Making in Mental Health Care,” Bulletin of the World Health Organization 98/1 (2020).
[13] W. Martin and S. Gurbai, “Surveying the Geneva Impasse: Coercive Care and Human Rights,” International Journal of Law and Psychiatry 64 (2019).
[14] B. McSherry, P. Gooding, and Y. Maker, “Human Rights Promotion and the ‘Geneva Impasse’ in Mental Healthcare: Scoping Review,” BJPsych Open 9/3 (2023).
[15] Funk and Drew Bold (2020, see note 6); U. Grigaitė, K. Levickaitė, D. Juodkaitė, and N. Goštautaitė-Midttun, “Promoting Human Rights-Based Deinstitutionalization in Lithuania by Applying the World Health Organization’s QualityRights Assessments,” International Journal for Quality in Health Care 37/1 (2025).
[16] World Health Organization, “QualityRights Materials for Training, Guidance and Transformation” (November 12, 2019), https://www.who.int/publications/i/item/who-qualityrights-guidance-and-training-tools.
[17] Mahdanian et al. (see note 1).
[18] C. Febles-Arévalo, J. J. Martín-Domínguez, R. García-Montesdeoca, et al., “Care Quality from the Perspective of Human Rights as Perceived by Mental Health Professionals in Gran Canaria: A Qualitative Study” (2023).
[19] C. I. Aviles González, D. M. Cerchiaro Fernández, M. E. Guerra Muñoz, et al., “Mental Health Professionals’ Perception of Respect for Human Rights and Organizational Well-Being in Three Countries of South America,” International Journal of Environmental Research and Public Health 21/2 (2024).
[20] B. D. Kelly, “Psychiatric Services, Mental Health Law, and Human Rights,” Indian Journal of Medical Research 156 (2022).
[21] M. G. Carta and D. Bhugra, “Human Rights and Mental Health: Critical Challenges for Health Professionals, Users, and Citizens,” International Review of Psychiatry 35 (2023).
[22] P. Doedens, J. Vermeulen, L. Lou Boyette, et al., “Influence of Nursing Staff Attitudes and Characteristics on the Use of Coercive Measures in Acute Mental Health Services: A Systematic Review,” Journal of Psychiatric and Mental Health Nursing 27/4 (2020).
[23] S. Davis Le Brun, S. Butchard, P. Kinderman, et al., “Applying the Theory of Planned Behaviour to Understand Mental Health Professionals’ Intentions to Work Using a Human Rights-Based Approach in Acute Inpatient Settings,” Journal of Mental Health 33/3 (2023).
[24] Ventura et al. (see note 2).
[25] D. Wijker, P. Sillitti, and E. Hewlett, “The Provision of Community-Based Mental Health Care in Lithuania,” OECD Health Working Paper No. 143 (2022), https://www.oecd.org/en/publications/the-provision-of-community-base-mental-health-care-in-lithuania_18de24d5-en.html.
[26] N. Grigutytė, M. Jakubauskienė, and K. Levickaitė, “Stigmatizuojančios Lietuvos gyventojų nuostatos psichikos sveikatos srityje – tyrimo ataskaita” (2022).
[27] J. W. Creswell and V. L. Plano-Clark, Designing and Conducting Mixed Methods Research, 3rd Edition (Sage Publications, 2017).
[28] P. Dodemaide, L. Joubert, N. Hill, and M. Merolli, “Online Survey Design and Social Media,” in ACM International Conference Proceeding Series, Association for Computing Machinery (2020).
[29] S. Hall, Representation: Cultural Representations and Signifying Practices (Sage Publications, 1997).
[30] V. Braun, V. Clarke, E. Boulton, et al., “The Online Survey as a Qualitative Research Tool,” International Journal of Social Research Methodology 24/6 (2021).
[31] M. M. Hennink, I. Hutter, and A. Bailey, Qualitative Research Methods (Sage Publications, 2020).
[32] Creswell and Plano-Clark (see note 27); L. C. Houghton and A. Paniagua-Avila, “Why and How Epidemiologists Should Use Mixed Methods,” Epidemiology 34/2 (2023).
[33] E. Šumskienė, U. Grigaitė, K. Levickaitė, et al., Žmogaus teisių apsauga psichikos sveikatos priežiūros įstaigose (Vilnius University Press, 2025); Funk and Drew Bold (2020, see note 6); World Health Organization (2019, see note 16); World Health Organization, WHO QualityRights Toolkit: Assessing and Improving Quality and Human Rights in Mental Health and Social Care Facilities (2012).
[34] V. Braun, V. Clarke, N. Hayfield, et al., “Doing Reflexive Thematic Analysis,” in S. Bager-Charleson and A. McBeath (eds), Supporting Research in Counselling and Psychotherapy: Qualitative, Quantitative, and Mixed Methods Research (Palgrave Macmillan, 2022); V. Braun and V. Clarke, “Thematic Analysis,” in F. Maggino (ed), Encyclopedia of Quality of Life and Well-Being Research (Springer, 2022); B. Gough and A. Madill, “Subjectivity in Psychological Science: From Problem to Prospect,” Psychological Methods 17/3 (2012).
[35] F. Agudelo-Hernández, H. Vélez-Botero, and M. C. González-Morales, “Human Rights Education and Attitudes Toward Mental Health Among Psychology, Medical, and Social Work Students,” Stigma and Health (2024).
[36] Doedens et al. (see note 22).
[37] F. Begum, “Human Rights and Mental Health: A Review of Current Awareness and Emerging Developments,” Saudi Journal of Nursing and Health Care 7/9 (2024).
[38] I. Galbert, A. N. Azab, Z. Kaplan, and L. Nusbaum, “Staff Attitudes and Perceptions Towards the Use of Coercive Measures in Psychiatric Patients,” International Journal of Mental Health Nursing 32/1 (2023).
[39] D. O. Aluh, J. M. Caldas de Almeida, D. Richter, and R. Whittington, “Coercion in Contemporary Mental Health Services: Key Concepts, Historical Development and Contextual Factors,” in N. Hallett, R. Whittington, D. Richter, and E. Eneje (eds), Coercion and Violence in Mental Health Settings: Causes, Consequences, Management, 2nd edition (Springer Nature Switzerland, 2024).
[40] Human Rights Council (see note 6).
[41] World Health Organization, Guidance on Community Mental Health Services: Promoting Person-Centred and Rights-Based Approaches (2021).
[42] World Health Organization Regional Office for Europe, Mental Health, Human Rights and Standards of Care: Assessment of the Quality of Institutional Care for Adults with Psychosocial and Intellectual Disabilities in the WHO European Region (2018).