Expanding Safe Hospital Access for Overdose Care in Lebanon
Vol 28/1, 2026, pp. 105-112 PDF
Michelle Wazan, Tatyana Sleiman, Dima El Hajj, and Ramzi Haddad
Abstract
In Lebanon, the criminalization of drug use and the misapplication of ministerial directives have led hospitals to report overdose cases to law enforcement, deterring people who use drugs from seeking urgent medical care and increasing the risk of preventable death. This paper examines overdose response as a right to health issue, using civil society advocacy in Lebanon to illustrate how law enforcement involvement in health care settings undermines access to emergency care. Drawing on repeated nationwide mappings of hospital practices when receiving overdose cases conducted between 2016 and 2024, the paper documents patterns of compliance and noncompliance with Ministry of Public Health directives prohibiting the reporting of overdoses to the police. While sustained advocacy has contributed to multiple policy milestones, including ministerial and syndicate circulars reaffirming hospitals’ duty of care without police involvement, implementation has remained uneven. Although more hospitals have stopped reporting overdose cases to the police, continued reporting remains tied to limited staff awareness, fear of liability, and stigmatizing attitudes toward people who use drugs. The Lebanese case highlights both the critical role and the structural limits of civil society monitoring in safeguarding access to emergency medical care under conditions of criminalization, crisis, and weak accountability. We argue that incremental protective policies are insufficient where emergency care remains entangled with punitive drug policy.
Introduction
The United Nations Office on Drugs and Crime World Drug Report 2025 estimates that 316 million people used an illicit drug in 2023, representing a 28% increase over the past decade.[1] Drug overdoses remain a critical global public health issue, with an estimated 100,000–150,000 cases annually, placing a significant burden on health systems.[2]
Despite these alarming figures, evidence consistently shows that emergency services are often not contacted during drug-related emergencies. Studies in Canada have found that emergency services are called in less than half of overdose cases.[3] Fear of police presence, potential criminal charges, and negative past encounters with law enforcement are cited as key barriers.[4] In the United States, a survey examining incarceration in a county jail within six hours following an emergency medical service response reported that 21% of people experiencing stimulant-involved overdoses were subsequently incarcerated.[5] Together, these findings underscore the significant role that law enforcement involvement plays in shaping health decisions, ultimately increasing the risk of overdose-related mortality.
In response to this reluctance to seek emergency care, several countries have introduced legal protections aimed at encouraging calls for help during overdoses. One prominent example is “good Samaritan” laws (GSLs) adopted by numerous US states that provide limited immunity from arrest or prosecution for drug possession when emergency services are contacted.[6] Evidence suggests that jurisdictions implementing GSLs experience a 14% lower incidence of overdose-related fatalities compared to those that have not implemented such laws.[7] However, persistent deterrents remain in jurisdictions where GSLs are passed.[8] Studies continue to document fears related to police presence at overdose scenes, risk of arrest, and limited knowledge of or trust in GSLs.[9]
In Lebanon, where the use of drugs and possession for personal use is criminalized and carries prison sanctions of up to three years, data on drug use prevalence and overdose rates are scarce. The most recent estimates suggest that there are 9,000 people nationwide who inject drugs.[10] In 2015, the estimated number of people who injected drugs in Greater Beirut was approximately 3,000.[11] More than 195 individuals reported having experienced a non-fatal opioid overdose in the same year.[12] In Lebanon, the risk of overdose is closely linked to incarceration, prior treatment experiences, and repeated arrests, reflecting interconnected risks faced by communities of people who use drugs and providing critical context for examining the country’s overdose response.[13]
The International Guidelines on Human Rights and Drug Policy, endorsed by several United Nations agencies, affirm that, in line with the right to health under international human rights law, particularly the Universal Declaration of Human Rights and the International Covenant on Economic, Social and Cultural Rights, states must ensure that individuals who experience or witness an overdose are protected from criminal prosecution or punishment when seeking medical assistance.[14] These standards clarify that people who use drugs hold an inalienable right to health and that states, including Lebanon, are obligated to ensure safe access to emergency medical care during overdoses.
Nevertheless, criminalization reinforces stigma and discrimination that extends beyond the criminal justice system into health care settings, effectively “undermin[ing] access to services for people who use drugs.”[15] Criminalization thus impedes the enjoyment of human rights, including access to emergency medical services.
Over the past two decades, the legal framework governing overdose reporting to law enforcement in Lebanon has evolved, yet significant implementation challenges persist. In 2006, the Ministry of Interior issued Circular 55/1, requiring hospitals to report emergency cases resulting from “harm caused by others” to the Internal Security Forces.[16] Although this provision does not apply to overdose or drug-related cases, its vague wording, coupled with entrenched stigma, has led many hospitals to report drug overdoses to law enforcement. As a result, police have visited emergency departments to interrogate or arrest patients following overdose events. This practice has fostered a climate of fear that discourages people who use drugs from seeking urgent medical care, increasing the risk of preventable death. A 2015 unpublished survey conducted by Skoun—a harm reduction and outpatient treatment center operating in Lebanon since 2003—among 300 service users of harm reduction centers in Lebanon found that 57% of those who had experienced an overdose did not seek hospital care during their first overdose for fear of arrest.
To mitigate the documented harms of criminalization, public health and human rights experts have increasingly advocated for the decriminalization of drug use as part of a rights-based approach to drug policy. Decriminalization is widely understood to reduce barriers to harm reduction services, including access to emergency medical care, and to improve health outcomes.[17] The United Nations Committee on Economic, Social and Cultural Rights has repeatedly linked the criminalization of drug use to impediments to the right to health and to increased engagement in risky practices that increase the likelihood of drug-related emergencies.[18] The recognition of these harms has led a growing number of countries and jurisdictions to pursue varying drug use decriminalization models.[19] Portugal is frequently cited as a leading example of decriminalization, where results have shown a significant decrease in overdose deaths since 2001.[20]
This paper uses advocacy conducted in Lebanon as a case study to examine how legal ambiguity, institutional practices, and stigma converge to undermine access to emergency care and to explain why overdose-linked protective policies are insufficient without broader structural reform. In doing so, it contributes to ongoing debates on drug policy and human rights by foregrounding overdose response as a site where the consequences of criminalization are both immediate and fatal.
Civil society advocacy and monitoring in Lebanon
Survey of service users
In 2015, in response to growing concerns among service users and their families about overdose, Skoun conducted a survey among 300 service users of harm reduction centers operating in Lebanon to better understand drivers and obstacles to emergency-seeking behavior. The survey found that 35% of service users had overdosed and that 49% knew someone who had overdosed. Among those who overdosed, 57% did not go to a hospital the first time they overdosed, 21% did not go the second time they overdosed, and 13.3% refrained from going to a hospital on their third overdose. The main stated reason for this reluctance was fear of arrest. Of those who reported going to the hospital or knowing someone who overdosed and went to the hospital, 32% reported that the police were called.
As a result of these findings, and in partnership with Embrace—a Lebanese nongovernmental organization working on mental health and suicide prevention—and the National Mental Health Program at the Ministry of Public Health, Skoun held a panel in 2016 with ministerial representatives as well as representatives from two major hospitals in Lebanon to discuss the life-threatening consequences of the misapplication of the ministry’s 2006 circular. The panel’s conclusion was that reporting overdose cases to the police contravened the Hippocratic Oath and violated medical ethics. Accordingly, the Ministry of Public Health released Circular 44/2016 to clarify that overdose cases fall outside the scope of Circular 55/1, since they do not constitute “harm caused by others.”[21] However, even after this clarification, many hospitals continued to disregard the policy.
In 2016, Skoun launched a series of initiatives to ensure safe and timely access to emergency medical care—without fear of arrest—in cases of overdose for people residing in Lebanon. These efforts consist of conducting repeated mappings of hospitals to document those that implement the ministerial directives, as well as advocating with decision-makers and governmental entities to secure additional guarantees and directives that protect the rights of people who use drugs when accessing health care services.
“Safe hospitals” mapping
To assess the implementation of the Ministry of Public Health’s Circular 44/2016 prohibiting the reporting of overdose cases to law enforcement, Skoun initiated repeated mappings of hospital practices across Lebanon beginning in 2016. The initial 2016 mapping served as a pilot phase, through which the methodology was refined, with subsequent rounds from 2018 onward producing more consistent and reliable data. The mappings aimed to document whether hospitals report overdose and drug-related emergencies to law enforcement upon admission to emergency departments and to identify patterns of compliance, noncompliance, and underlying justifications. The number of hospitals successfully reached varied across mapping rounds due to a variety of factors, including non-response and broader health system disruptions, particularly in the context of Lebanon’s overlapping economic and political crises (see Table 1). In the first round, Skoun targeted all 141 private and public hospitals listed on the Ministry of Public Health’s website; subsequent rounds targeted the 133 hospitals that responded during the first round. The final sample reflects those that were reachable and responsive at the time of data collection.

The mappings were conducted through structured phone surveys by Skoun’s outreach team using a standardized questionnaire focused on reporting practices for overdose and drug-related emergencies, as well as awareness of relevant ministerial circulars. The unit of analysis was the hospital. Interviews were conducted with the most senior emergency department staff available, typically one or two individuals per hospital (a senior doctor or a senior emergency room nurse), as they are the primary decision-makers regarding whether to report cases to law enforcement. In some instances, emergency staff indicated that such decisions required referral to hospital administration, in which case Skoun contacted the administration directly. This purposive selection aimed to capture institutional practice through those with decision-making authority, rather than to survey a representative sample of all emergency department staff.
A hospital was classified as “safe” for people who use drugs if overdose and drug-related emergency cases were not reported to law enforcement, irrespective of staff familiarity with the circulars themselves. This classification was used as an operational proxy for whether individuals could seek care without risk of legal repercussions. Where reporting occurred, reasons and areas of concern were documented. In cases where multiple respondents were interviewed within the same institution and provided contradictory responses, the hospital was conservatively classified as “unsafe,” reflecting the potential risk faced by individuals in practice.
In parallel with data collection, the mappings served an advocacy and accountability function. Hospitals that were unaware of the circulars were informed of their content and of the human rights and health implications of reporting overdose cases. Copies of the relevant directives were shared with emergency staff and hospital administrations to foster internal dissemination and compliance.
Once identified, lists of hospitals that did not report overdose cases were compiled and disseminated through social media and harm reduction networks to enable people who use drugs to access emergency care without fear of arrest.
Repeated mappings were conducted between 2016 and 2024, with interruptions during periods of compounded crisis, economic collapse, the COVID-19 pandemic, and intensified conflict, allowing for the observation over time of trends in compliance and institutional practice.
Growth of a national network of “safe hospitals”
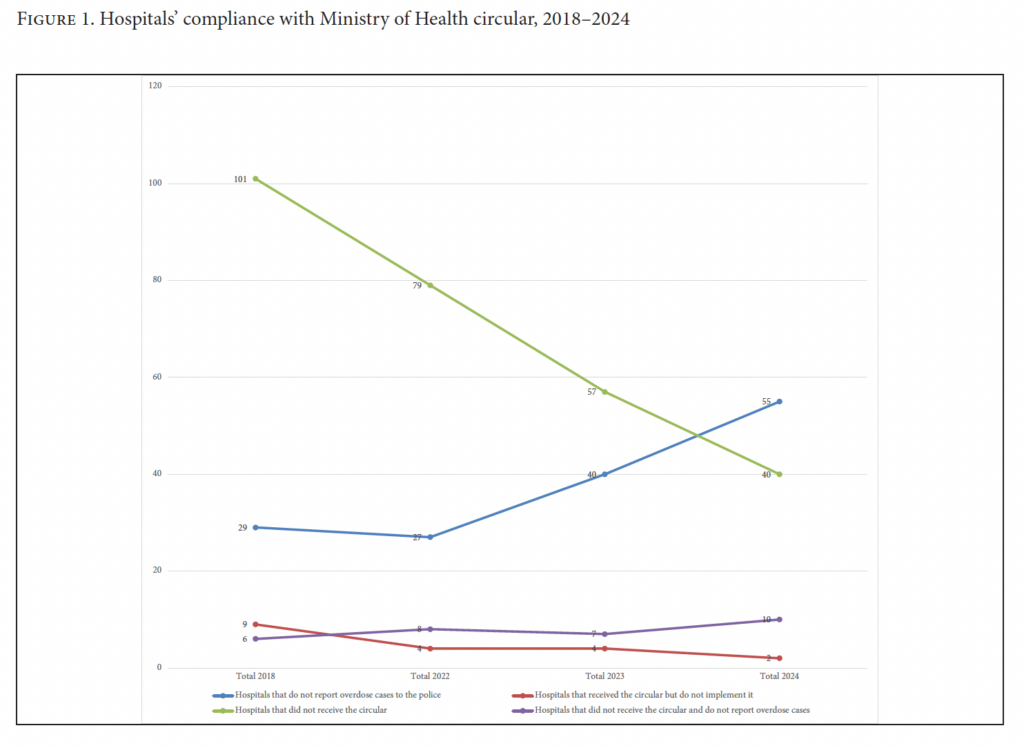
Figure 1 shows that after 2018, there was a sharp increase in the percentage of hospitals considered “safe” and a sharp decrease in the number of hospitals declaring not to have received the Ministry of Health’s 2016 circular. The number of hospitals that received the circular but nevertheless continued to report overdose cases to the police decreased between 2018 and 2024.
The mappings coincided with sustained advocacy that led to additional normative measures reinforcing the right of people who use drugs to access emergency medical care. The increase in the number of hospitals refraining from reporting overdoses appears to be driven by three factors: the issuance of complementary circulars in 2019 by the Ministry of Public Health and the Ministry of Interior clarifying non-reporting obligations and law enforcement jurisdiction; the repetition of mappings, which reinforced awareness of these obligations among hospital staff; and the 2024 circular issued by the Syndicate of Hospitals, which provided further institutional reassurance to hospital administrations. These measures directly responded to concerns raised by hospitals during the mappings and were pursued through targeted advocacy with relevant stakeholders.
Reasons for continued reporting
Despite the increase in the number of “safe hospitals,” structural impediments to the implementation of the circular persisted. Over the years, interviews with staff in private and governmental hospitals revealed a consistent pattern of reporting overdose cases to law enforcement, often driven by lack of awareness of the Ministry of Public Health and Ministry of Interior circulars and a widespread belief, sometimes driven by social and political pressure, that notifying the police is part of their duty. Hospital staff often expressed worry that they would face prosecution for not reporting or that the hospital would be legally liable for the same reasons. A hospital director echoed the social and political pressures they face, with one explaining that “the tongue of people is stronger than the law” and another admitting fear of media exposure: “If someone dies of an overdose and [we] didn’t report, what will the media say?”
Additional justifications for reporting included suspicion of suicide attempts or poisoning, patient agitation, or behavior deemed unusual. Many respondents conflated overdose and drug use with violence, stating that they report cases when “[the patients] are violent, or if they come alone and stay for a long time,” or claiming that they report because drug use suggests accompanying criminal activity, as reflected in comments such as “because this person might be harming someone else.”
In heavily militarized areas, hospital staff noted that “having the Army at the hospital checkpoint means we must report” or “there is a police checkpoint at the entrance, they already know.” Regular oversight by security agencies was also cited. For instance, one hospital highlighted that local law enforcement “regularly comes in to check on what’s happening and ask about death cases and overdose cases.” Several admitted reporting to multiple parties, including hospital security, the Lebanese Army’s Intelligence Directorate, the Internal Security Forces’ intelligence unit, and the General Security Directorate, raising serious concerns about breaches of patient confidentiality.
Stigmatizing opinions and attitudes among medical staff members are particularly concerning because they directly hinder access to medical services but could also translate into defiance of the Ministry of Public Health’s circulars. One staff member argued that “these circulars are a mistake, and these cases should be reported to the police, if not to arrest them, at least to take them to treatment.” Another declared more harshly that “people who use drugs should be killed … it’s against religion, and they’re harming others and might harm children.” Surprisingly, that staff member worked at a hospital that did not report overdose cases to the police, yet he was adamant about expressing his disagreement with the hospital’s policy during the survey.
Mapping in crisis and conflict
The economic collapse of Lebanon triggered a severe medical brain drain in 2021, with approximately 40% of physicians and 30% of nurses leaving the country.[22] This exodus contributed to high staff turnover and fragmented awareness of ministerial directives among emergency department personnel. As of 2022, the results of the mappings documented disruptions in the continuity of overdose response practices within health care institutions, reflected in inconsistent compliance across mapping cycles. Hospitals previously identified as “safe” no longer appeared on “safe hospitals” list due to staff changes, hospital closures, or the suspension of emergency departments. Conflict escalation starting in late 2023 further affected health care institutions, demonstrating that in contexts of crisis and conflict, protection directives are ineffective without sustained institutionalization, monitoring, and reinforcement.
Advocacy
Skoun’s advocacy efforts were informed by findings from its repeated mappings and targeted institutions identified as central to addressing health care workers’ fears and institutional hesitations around non-reporting. In 2019, following sustained advocacy, the Ministry of Public Health reiterated its directives through Circular 76/2019, reaffirming that hospitals should refrain from reporting overdose cases to the police. The Ministry of Interior subsequently issued a complementary circular addressed to law enforcement agencies, clarifying that overdose cases reported by hospitals fall outside their mandate and explicitly acknowledging the right to health of people who use drugs.
Subsequent mappings conducted between 2022 and 2024 demonstrated that despite these directives, continued advocacy remained necessary. In August 2024, Skoun engaged key stakeholders to strengthen dissemination and monitoring of the circulars, resulting in the Syndicate of Hospitals issuing Circular 22/2024 reminding all private hospitals of their duty of care and of their obligations under the ministerial directives. In parallel, Skoun launched a video addressed to health care workers, emphasizing their role in safeguarding the lives of people who use drugs and reinforcing compliance with non-reporting policies.[23]
Lessons learned
The Lebanese case illustrates how criminalization continues to produce adverse health outcomes even where policies formally seek to mitigate its effects. Protective policies, while necessary, are insufficient when they are not embedded within institutional practice. The mapping of “safe hospitals” revealed that ministerial directives prohibiting the reporting of overdoses to law enforcement were often not integrated into hospital protocols, staff training, or internal accountability mechanisms. This lack of institutionalization undermined continuity, weakened knowledge among health care workers, and allowed discretionary and arbitrary practices to persist. This is particularly relevant in a context of crisis and conflict where staff turnover is high.
The absence of systematic monitoring and enforcement by relevant ministries further weakened accountability, allowing hospitals to selectively interpret or disregard official guidance with few consequences. While Skoun’s mapping played a critical role in disseminating life-saving information and reminding health care institutions of their obligations, it also exposed the limits of civil society action in the absence of formal state endorsement. In several cases, hospital administrations questioned the legitimacy of a nongovernmental organization to assess or publicize compliance with ministerial directives.
At a deeper level, the Lebanese example underscores how criminalization operates not only through law but through social norms and professional cultures. Moralizing attitudes among health care workers toward people who use drugs reinforce fear, stigma, and discriminatory practices, effectively reproducing the harms of criminalization within health institutions themselves. This dynamic captures the core harm of punitive drug policy in the context of health: Even where protective policies exist, criminalization reshapes perceptions of deservingness, trust, and care, ultimately placing lives at risk.
Finally, it was not possible to assess the impact of protection directives and the growing network of “safe hospitals” on overdose-related mortality, as drug overdoses remain systematically underreported due to stigma and the absence of consistent data collection mechanisms.
Conclusion
Across jurisdictions that criminalize drug use and possession, evidence shows that protection directives aimed at safeguarding the fundamental right to health of people who use drugs are insufficient on their own. While contexts and contributing factors may vary, the common denominator remains the criminalization of drug use. Punitive drug policies continue to shape health-seeking behavior and health outcomes. In a context of criminalization, overdose deaths can result from foreseeable and preventable rights violations. Only by embracing evidence-based and rights-based approaches to drugs can states reduce overdose mortality, protect human dignity, and uphold their international commitments.
Michelle Wazan, LLB, is drug policy program manager at Skoun Lebanese Addictions Center, Beirut, Lebanon.
Tatyana Sleiman, MSc, is executive director of Skoun Lebanese Addictions Center, Beirut, Lebanon.
Dima El Hajj is a master of public health candidate at the American University of Beirut, Lebanon.
Ramzi Haddad, MD, is a professor of psychiatry at the Lebanese University, Beirut, Lebanon.
Please address correspondence to Ramzi Haddad. Email: ramzi.hadd@gmail.com.
Competing interests: None declared.
Copyright © 2026 Wazan, Sleiman, El Hajj, and Haddad. This is an open access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] United Nations Office on Drugs and Crime, World Drug Report 2025 (2025).
[2] World Health Organization, Global Status Report on Alcohol and Health and Treatment of Substance Use Disorders (2024).
[3] K. M. Follett, A. Piscitelli, M. Parkinson, et al., “Barriers to Calling 9-1-1 During Overdose Emergencies in a Canadian Context,” Critical Social Work 15/1 (2014).
[4] S. Bozat-Emre, S. G. Marshall, C. Zhong, et al., “Lessons Learned from Launching the Manitoba Take-Home Naloxone Program,” Health Promotion and Chronic Disease Prevention in Canada 38/6 (2018).
[5] B. Ray, B. J. Hedden, J. J. Carroll, et al., “Prevalence and Correlates of Incarceration Following Emergency Medical Services Response to Overdose,” Drug and Alcohol Dependence 238 (2022).
[6] H. Nguyen and B. R. Parker, “Assessing the Effectiveness of New York’s 911 Good Samaritan Law: Evidence from a Natural Experiment,” International Journal of Drug Policy 58 (2018).
[7] S. Moallef and K. Hayashi, “The Effectiveness of Drug-Related Good Samaritan Laws: A Review of the Literature,” International Journal of Drug Policy 90 (2021).
[8] E. Van der Meulen, S. K. H. Chu, and J. Butler-McPhee, “‘That’s Why People Don’t Call 911’: Ending Routine Police Attendance at Drug Overdoses,” International Journal of Drug Policy 88 (2021).
[9] H. Byles, N. Sedaghat, N. Rider, et al., “Barriers to Calling Emergency Services Among People Who Use Substances in the Event of Overdose: A Scoping Review,” International Journal of Drug Policy 132 (2024).
[10] Middle East and North Africa Harm Reduction Association, Assessment of Situation and Response of Drug Use and Its Harms in the Middle East and North Africa (2024).
[11] Middle East and North Africa Harm Reduction Association. Project Crossroads: Size Estimation, Risk Behavior Assessment, and Disease Prevalence Among Key Populations in Lebanon (2015).
[12] Ministry of Public Health, National Report on Drug Situation in Lebanon (2017).
[13] Middle East and North Africa Harm Reduction Association (2024, see note 10).
[14] United Nations Development Programme, World Health Organization, Joint United Nations Programme on HIV/AIDS, Office of the United Nations High Commissioner for Human Rights, International Guidelines on Human Rights and Drug Policy (2019).
[15] Joint United Nations Programme on HIV/AIDS, Health, Rights and Drugs: Harm Reduction, Decriminalization and Zero Discrimination for People Who Use Drugs (2019).
[16] Skoun, Impediments to the Right to Life: Monitoring Overdose Reception Practices in Emergency Rooms Across Lebanese Hospitals (2023), https://www.skoun.org/storage/publications/nexAOvzIec9ooBqSNJTVtBIwYyNKBspmz6zzRHJx.pdf.
[17] Public Health Degrees, “The Decriminalization of Drugs and Public Health” (March 28, 2026), https://www.publichealthdegrees.org/resources/drugs-decriminalization-and-public-health/.
[18] United Nations General Assembly, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN Doc. A/65/255 (2010).
[19] Talking Drugs, “Drug Decriminalisation Across the World,” https://decriminalisation-map.talkingdrugs.org.uk/.
[20] Drug Policy Alliance, Drug Decriminalization in Portugal: Learning from a Health and Human-Centered Approach (2023).
[21] Skoun (2023, see note 16).
[22] World Health Organization Regional Office for the Eastern Mediterranean, “Joint Statement by Dr Tedros Adhanom Ghebreyesus, WHO Director General, and Dr Ahmed Al Mandhari, Regional Director for the Eastern Mediterranean, on Lebanon” (September 19, 2021), https://www.emro.who.int/media/news/joint-statement-by-dr-tedros-adhanom-ghebreyesus-who-director-general-and-dr-ahmed-al-mandhari-regional-director-for-the-eastern-mediterranean-on-lebanon.html.
[23] Skoun, “Skoun Overdose Awareness Campaign 2024,” YouTube (August 29, 2024), https://www.youtube.com/watch?v=wtRLfvpL0vM.