Well-Being Under Structural Constraints of Political Instability in the Israeli-Occupied West Bank: A Cross-Sectional Study
Vol 28/1, 2026, pp. 85-103 PDF
Rula Ghandour, Abdullatif Husseini, Shiraz Nasr, and Rita Giacaman
Abstract
The well-being of Palestinians living under prolonged Israeli occupation is deeply conditioned by the structures of deprivation and control that shape daily life. Using data from 3,000 adults residing in refugee camps and surrounding urban areas of the West Bank, this study examines how deprivation, political violence, and human rights violations relate to well-being as measured by the World Health Organization-Five Well-Being Index. Nearly three-quarters of respondents (73.8%) reported poor well-being. Material deprivation showed the strongest association with well-being: Those reporting low or moderate deprivation had 1.7- and 2.4-fold higher odds of poor well-being, respectively. Household exposure to political violence was associated with higher odds of poor well-being with an odds ratio (OR) of 1.35, while human rights violations by the Israeli military and the Palestinian Authority was associated with higher odds of poor well-being with an OR of 1.51 and 1.72, respectively. An interaction between locality and displacement revealed that stable camp residents had lower odds of poor well-being, while those displaced from camps had the highest risk. These findings show that in the West Bank of the Israeli-occupied Palestinian territory, well-being reflects the social geography of inequality, where displacement, deprivation, and ongoing political violence transform daily existence into a struggle for security and dignity, rendering the right to health inseparable from the right to live freely and safely.
Introduction
The well-being of populations living under chronic political instability is profoundly shaped by the structural constraints in which they live.[1] In the Israeli-occupied Palestinian territory (oPt), decades of Israeli military occupation have fragmented land and services, breaking the country into disconnected pieces and creating overlapping political, economic, and social constraints that define the daily lives of Palestinians. Restrictions on movement, widespread unemployment, land confiscation, and unequal control over resources have produced a system of structural constraints that extends far beyond direct violence and violations.[2] These constraints interact to inhibit people’s opportunities and systematically undermine their physical and mental health.[3]
Within this context, human rights violations are widespread. Here, human rights refer to standards that define how persons should be treated.[4] In contexts of military occupation and armed conflict, the primary focus of the human rights discourse is on the relationship between the state and individuals, including how state agents observe or violate human rights under conditions of military occupation and, in the case of armed conflict, how protections are expressed in international humanitarian law.[5] Under the prolonged Israeli military occupation of the Palestinian territory, such violations have become embedded within the social, economic, and institutional fabric of daily life, producing what can be described as structural constraints on well-being.[6] Human rights violations in the oPt are various and are manifested through restrictions on movement, economic marginalization, spatial segregation, and unequal access to resources—conditions that constrain life opportunities and systematically undermine well-being.[7]
Published research related to the oPt has also largely prioritized exposure to political violence and its effect on health and well-being.[8] Although the political conditions that Palestinians endure under Israeli occupation and colonization are particularly harsh—affecting all aspects of life and generally undermining both well-being and physical health—exposure to political violence is not the only form of harm to which Palestinians, and others worldwide, are subjected. Evidence shows that violence from family and community members, over and above the violence perpetrated by the Israeli military and the Palestinian Authority, is also important and contributes to the suffering that Palestinians experience throughout their lives.[9] This suffering produces what we call the invisible wounds inside a person, which can negatively influence health and well-being and need to be considered when examining the effects of violation, regardless of the perpetrator.[10]
Deprivation is another key dimension of harm in this context, encompassing the material, economic, social, and political restrictions that shape daily life under prolonged political instability. In the oPt, deprivation is not limited to poverty or lack of resources but also includes restricted movement, limited access to services, political fragmentation, and constraints on freedom and dignity.[11]
These personal and collective experiences of deprivation and violence reinforce cycles of vulnerability and limit opportunities for recovery and well-being.[12] In this sense, deprivation itself can be understood as a chronic violation of the rights to health, security, and dignity, linking inequalities directly to human rights violations.
This study builds on a research trajectory that we at the Institute of Community and Public Health at Birzeit University have pursued over the past several years. Our work has sought to understand how political instability, exposure to political violence, and deprivation interact with human rights violations to shape health and well-being among Palestinians living under occupation. This broader approach situates well-being as a reflection of structural constraints, including deprivation, gendered power relations, and prolonged political instability.
This study forms part of a broader research project that investigates the well-being of adults living in the West Bank of the oPt and the factors associated with their well-being, as assessed through participant reports using the World Health Organization-Five Well-Being Index (WHO-5). The study also examines the relationship between these well-being reports and human rights violations by four categories of potential perpetrators, using a locally developed and validated instrument that understands human rights violations in an ecological and locally grounded way and captures violations across family, community, governing authority, and military occupation levels. In addition, the study assesses exposure to political violence, deprivation, and other demographic and socioeconomic characteristics and how they are linked to well-being. In doing so, the study illuminates how persistent human rights violations, deprivation, and political instability together shape the well-being of Palestinians living under one of the world’s most enduring military occupations.
Methods
This is a cross-sectional study conducted between June 15 and July 31, 2025, in Palestinian refugee camps and surrounding urban areas in the north, center, and south of the Israeli-occupied West Bank. We used the World Health Organization’s framework on the social determinants of health to guide our understanding of how political, economic, social, and material conditions shape well-being.[13] We also drew on the socio-ecological framework to conceptualize the multilayered nature of human rights violations and to organize the measured variables across personal, household, community and locality, and broader contextual levels. This framework is rooted in Urie Bronfenbrenner’s ecological systems theory from the 1970s and was later adapted to the health sciences in the 1980s; it conceptualizes health as shaped by interacting influences across multiple levels, including intrapersonal, interpersonal, institutional, community, and policy levels.[14]
We examined human rights violations across different social and political levels, including violations attributed to family, community, the Palestinian Authority, and the Israeli military occupation.[15] Personal-level variables included age, sex, marital status, number of children, education, employment status, and chronic disease. Household-level variables included household exposure to political violence and material deprivation. Community- and locality-level variables included governorate, locality, refugee status, displacement, and community-level human rights violations. Broader contextual variables included human rights violations by the Palestinian Authority and the Israeli military occupation, sociopolitical deprivation, and Oslo area classification. The study did not aim to measure all levels of the socio-ecological framework exhaustively, such as personal behaviors or policy-level variables; rather, we used the framework to support a layered interpretation of exposure and to organize the variables measured in this survey.
Target population and sample
The study population included Palestinian men and women aged 18 years or older who lived in one of six areas across the northern, central, and southern regions of the West Bank. These areas included three Palestinian refugee camps and their surrounding urban areas. In the north, we selected the Jenin refugee camp and the surrounding urban area of Jenin City. In the center, we selected the al-Am’ari refugee camp for its proximity to the twin cities of Ramallah and al-Bireh. In the south, we selected al-Dheisheh refugee camp and the surrounding urban area of Bethlehem city.
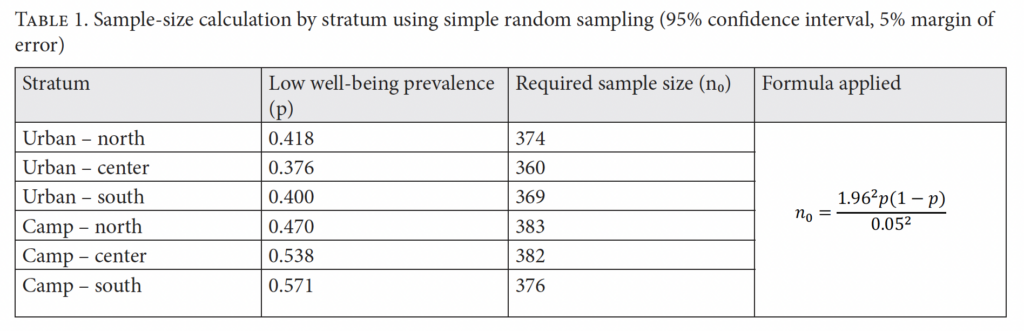
The sample size was calculated separately for each of the six strata using a simple random sampling formula, based on the estimated prevalence of poor well-being from a 2022 study, a 95% confidence level, and a 5% margin of error.[16] The initial minimum required sample size across the strata was 2,244 participants (see Table 1). To account for the clustered sampling design, we increased this by 20%, resulting in a minimum required sample of approximately 2,693 participants. We therefore targeted 3,000 participants, with approximately 500 participants sampled from each stratum.
Data collection
Within each stratum in the central and southern regions and the urban regions in the north, we selected clusters using systematic random sampling based on Palestinian Central Bureau of Statistics enumeration units. We then systematically selected households within each cluster and selected one participant per household using the Kish table. In the Jenin refugee camp, household selection differed due to large-scale displacement following the 2023 war on Gaza and the subsequent escalation of Israeli military violence in the West Bank. Data collection relied on displacement lists obtained from the camp’s popular committee, as approximately 75% of camp residents were displaced at the time of the study. Sampling within and outside the camp was conducted proportionally to cluster size to achieve the target sample size for each stratum. Data were collected by trained fieldworkers using electronic tablets and the Kobo Toolbox platform.
Study instrument
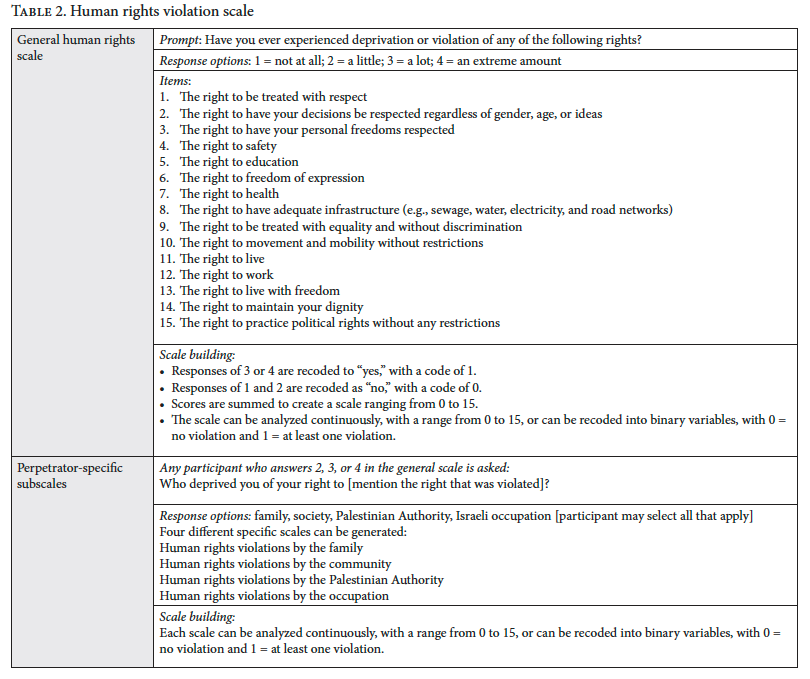
We assessed well-being using the validated Arabic version of WHO-5. Item scores were summed, transformed to a 0–100 scale, and then dichotomized into poor versus good well-being using a cut-off score of 50.[17] Human rights violations were measured using locally developed instruments, including a general human rights violations scale and four perpetrator-specific subscales. In this analysis, human rights violations refer to reported violations across four perpetrator levels—family, community, Palestinian Authority, and Israeli military occupation—capturing exposure across different social and political contexts. Each scale included up to 15 items reflecting violations relevant to the specific context or ecological level. Scale scores represented the number of reported violations and were recoded into binary variables, with 0 indicating no reported violations and 1 indicating the presence of at least one violation.[18]
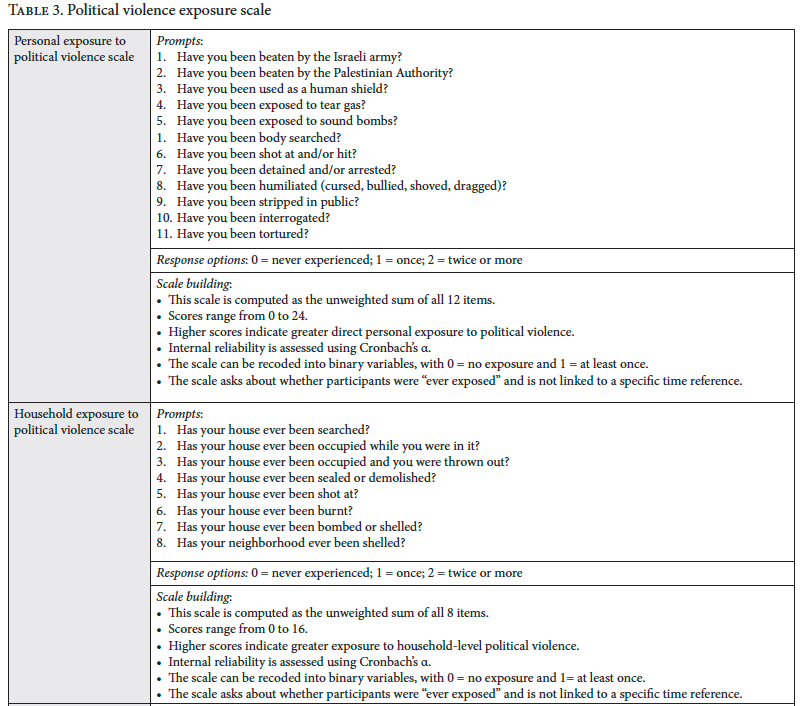
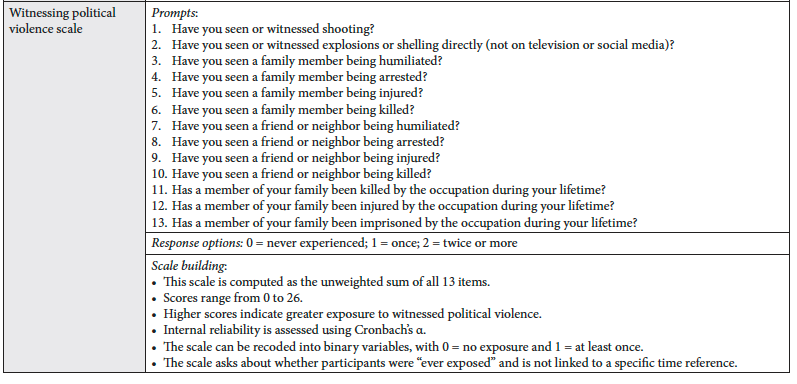
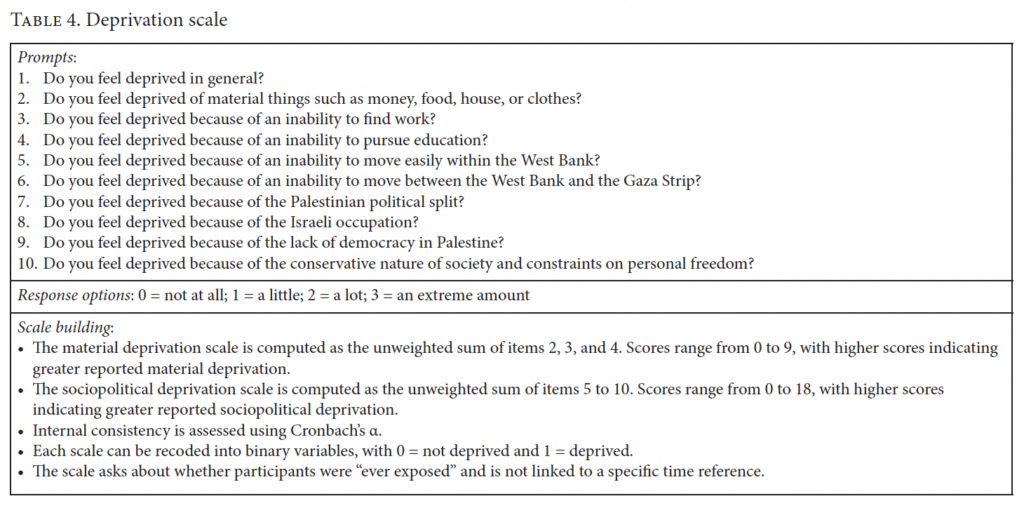
We also used a scale measuring exposure to political violence, which captures personal and household exposure to political violence, as well as exposure through witnessing political violence. For each reported exposure, participants were asked to identify the perpetrator, with response options including the Palestinian Authority, the Israeli military occupation, and Israeli settlers.[19] Additionally, we used a nine-item deprivation scale with two main subscales: sociopolitical deprivation and material deprivation.[20] All of these scales were developed by the Institute of Community and Public Health, building on qualitative research, and were piloted and validated using factor analysis to ensure validity and reliability. Detailed scale items are presented in Tables 2, 3, and 4.
The instrument also included several demographic and socioeconomic variables, including age group (18–24, 25–40, 41–60, 61–92), sex (man, woman), marital status (never married, currently married, widowed/divorced), number of children (none, 1–3, 4–6, 7 or more), and education level (less than higher education (Tawjihi), passed Tawjihi, post-Tawjihi). Additional variables included work status (working, unemployed, housewife, other), reported economic status (excellent/good, less than good, bad), governorate (Jenin, Ramallah and al-Bireh, Bethlehem), locality (urban, refugee camp), and area classification based on the Oslo Accords of 1995 (Area A, Area B, Area C).[21] Questions on displacement in the past two years, refugee status, health insurance coverage, and the presence of chronic disease were also included. Fieldworkers were trained in administering the research instruments following piloting to ensure clarity, relevance, timing, reliability, and consistency.
Statistical analysis
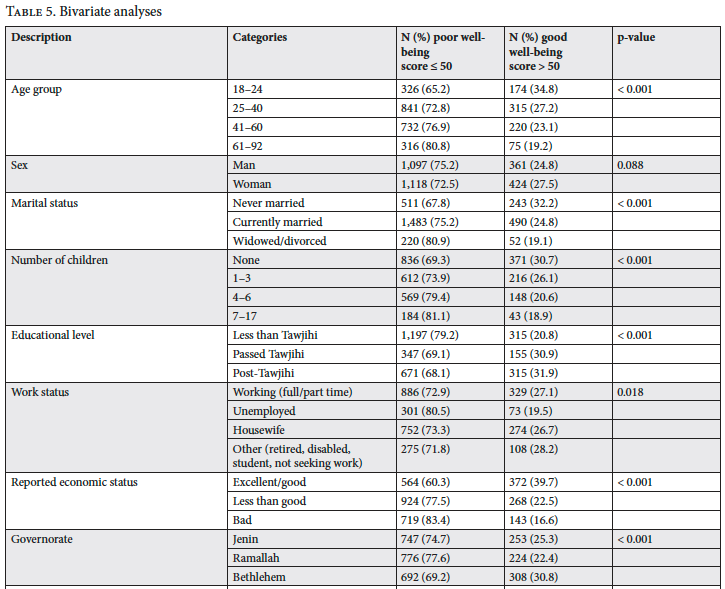
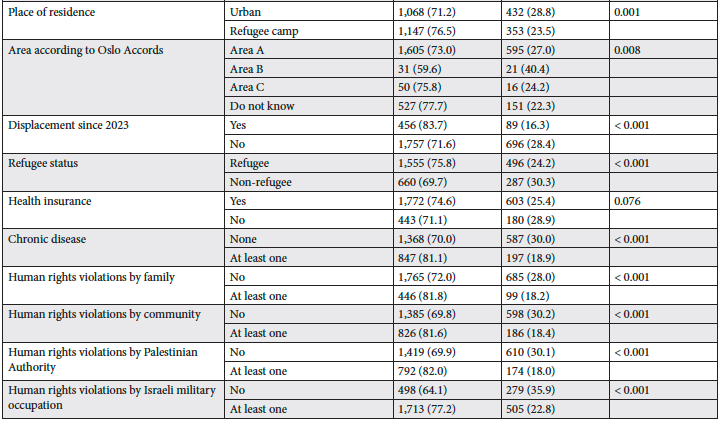
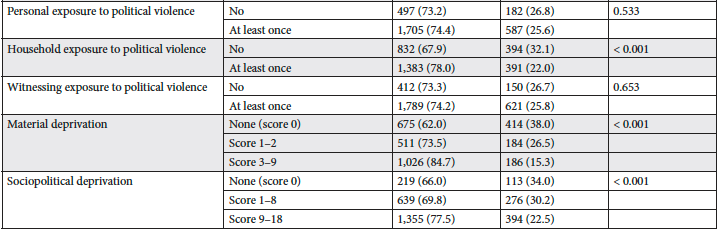
Descriptive (univariate) analyses were first performed to summarize participants’ demographic, socioeconomic, and health characteristics. Bivariate analyses were then conducted to examine the associations between each independent variable and the WHO-5 well-being outcome, using chi-square tests (see Table 5). WHO-5 was analyzed as a binary variable. Independent variables were selected based on the socio-ecological framework and the World Health Organization’s framework on the social determinants of health, encompassing factors at the personal, household, community, and broader contextual levels. Scales measuring exposure to political violence and human rights violations were recoded as binary indicators (0 = not exposed, 1 = ever exposed), while deprivation items were analyzed as ordinal variables. A factor analysis of the deprivation items yielded two distinct components: material deprivation and sociopolitical deprivation.
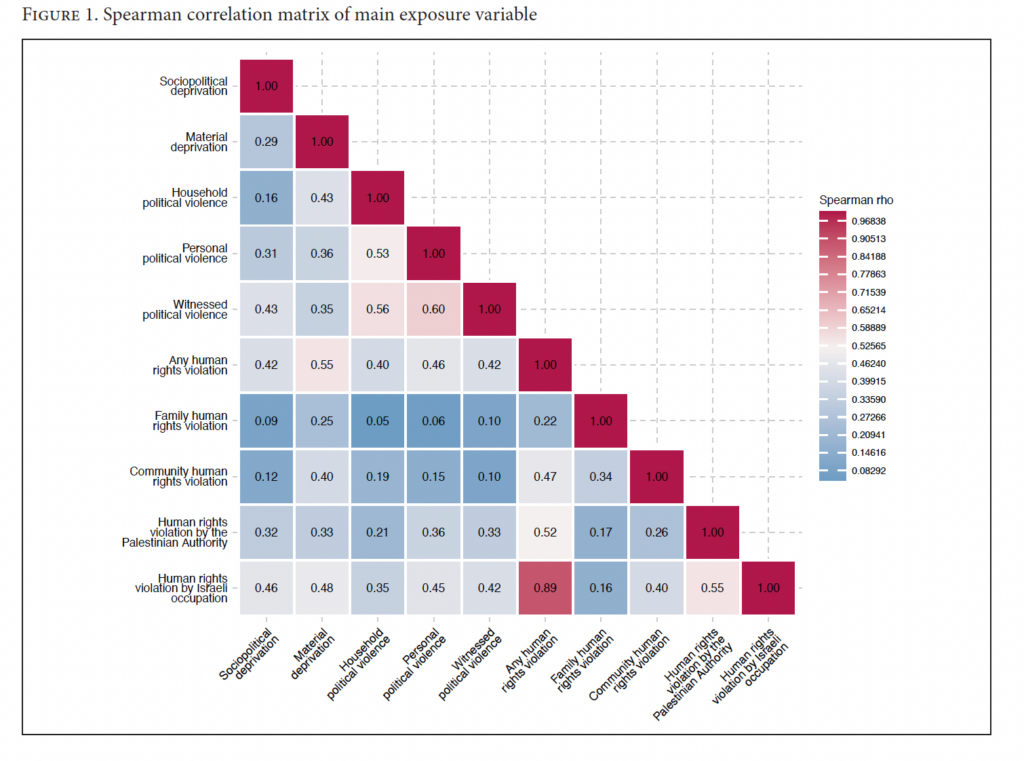
All multi-item scales demonstrated acceptable internal consistency, with Cronbach’s alpha values higher than 0.65. A multiple binary logistic regression model was then fitted to identify independent predictors of poor well-being. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Correlations between deprivation, political violence, and human rights violation variables were examined, and multicollinearity diagnostics were assessed before fitting the final multivariate model. Variance inflation factors were within acceptable limits, suggesting that multicollinearity was not a concern in the final model. A Spearman correlation heat map was also generated to visually assess the degree of overlap between these variables (see Figure 1). All analyses were conducted using Stata 18.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee at the Institute of Community and Public Health, Birzeit University (Ref. 2025(2-1)). Verbal informed consent was obtained from all participants in accordance with Birzeit University’s ethical guidelines on confidentiality, anonymity, and voluntary participation.
Results
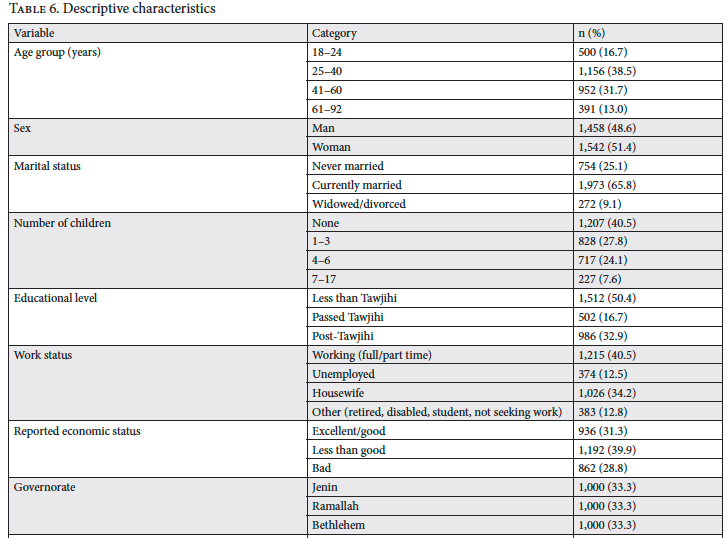
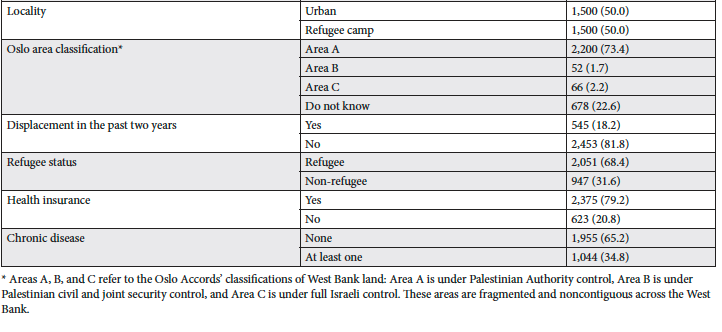
Of the 3,147 persons invited to participate, 3,000 consented (95.3%). The mean age was 41 ± 24 years; most were aged 25–40 (38.5%) or 41–60 (31.7%), and 51.4% were women. Most participants were married (65.8%), and about half had fewer than four children. Half had less than a high school education, and 40.5% were employed, while 34.2% were housewives. Economically, 31.3% reported good or better status, 39.9% less than good, and 28.8% bad compared with people around them. Participants were evenly distributed across Jenin, Ramallah, and Bethlehem, with half living in urban areas and half in refugee camps or displaced settings. Most lived in Area A (73.4%); 18.2% had been displaced in the past two years; 68.4% were registered refugees; 79.2% had health insurance; and approximately one-third reported being diagnosed with a chronic illness. (See Table 6.)
As shown in Figure 2, most participants (77.1%) reported experiencing at least one form of human rights violation. Violations by family members were the least common, reported by 18.2% of participants, followed by violations by the Palestinian Authority (32.3%) and the community (33.8%). The most frequently reported human rights violation was by the Israeli military occupation (74.1%). With regard to exposure to political violence, 77.1% of participants reported at least one personal exposure to such violence. Nearly 60% of participants reported household-level exposure, and 81.1% reported directly witnessing political violence outside the media. Moderate to high material deprivation was reported by 40.5% of study participants, and 58.4% reported moderate to high levels of sociopolitical deprivation.
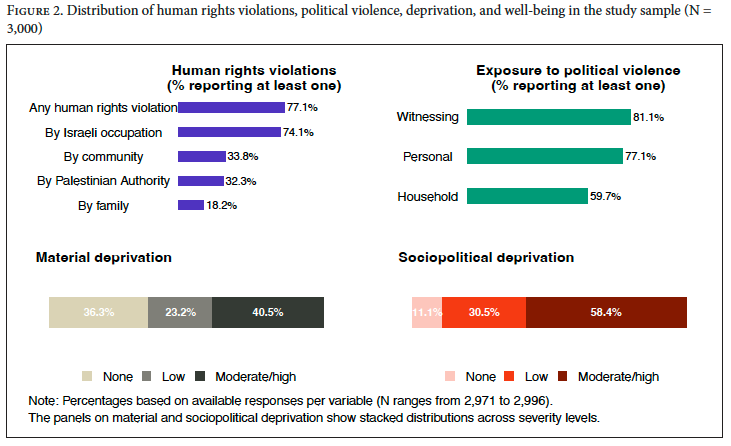
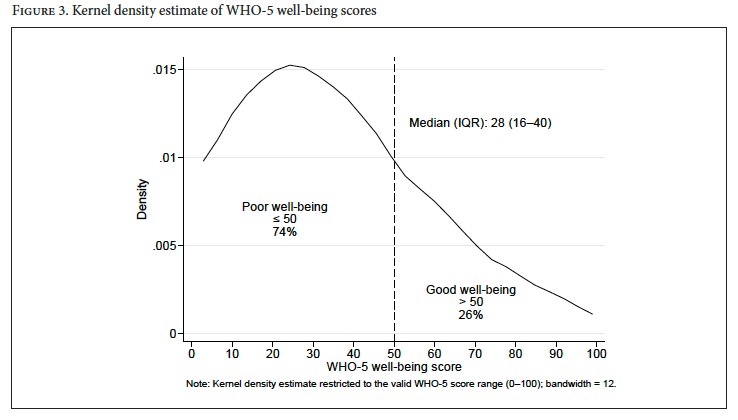
Figure 3 shows a smoothed kernel density distribution of WHO-5 scores, with the curve peaking at lower scores and gradually declining toward higher scores. The median WHO-5 score was 28, with an interquartile range of 16–52, and 74% of participants scored ≤ 50, indicating low well-being, while 26% scored > 50, indicating good or moderate well-being.
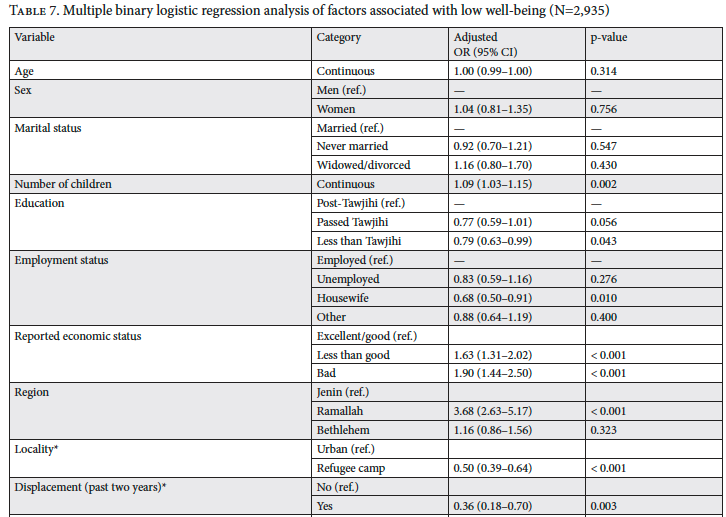
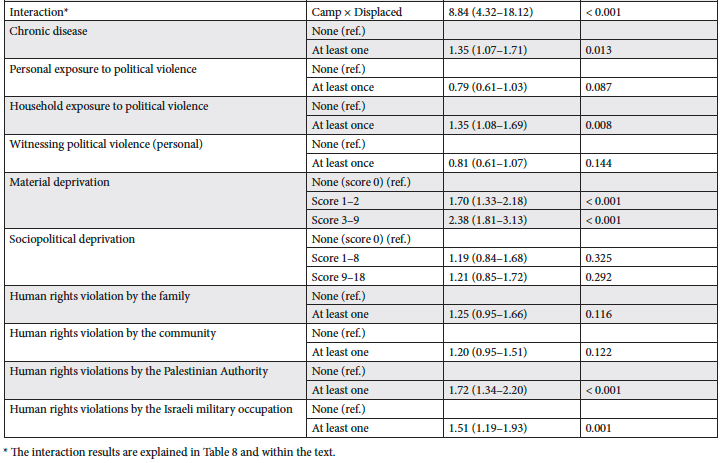
The multivariate logistic regression showed that having more children increased the odds of poor well-being (OR = 1.09, 95% CI: 1.03–1.15). Secondary education (OR = 0.79, 95% CI: 0.63–0.99) and being a housewife (OR = 0.68, 95% CI: 0.50–0.91) were associated with lower odds compared with post-secondary education and employment, respectively. Poorer economic status was strongly associated with poor well-being, with higher odds among those reporting “less than good” (OR = 1.63, 95% CI: 1.31–2.02) and “bad” conditions (OR = 1.90, 95% CI: 1.44–2.50). Region was also significant, as residents of Ramallah and al-Bireh had higher odds of poor well-being than those in Jenin (OR = 3.68, 95% CI: 2.63–5.17).
Having at least one chronic illness was associated with higher odds of poor well-being (OR = 1.35, 95% CI: 1.07–1.71). Among forms of political violence, only household exposure was significantly associated with poor well-being (OR = 1.35, 95% CI: 1.08–1.69), whereas personal exposure or witnessing violence was not. Material deprivation showed a strong gradient: low deprivation was associated with higher odds of poor well-being (OR = 1.70, 95% CI: 1.33–2.18), increasing to more than twofold among those with moderate to high deprivation (OR = 2.38, 95% CI: 1.81–3.13). Sociopolitical deprivation was not significant. Exposure to human rights violations was also associated with poor well-being, including violations by the Palestinian Authority (OR = 1.72, 95% CI: 1.34–2.20) and the Israeli military (OR = 1.51, 95% CI: 1.19–1.93) (Table 7).
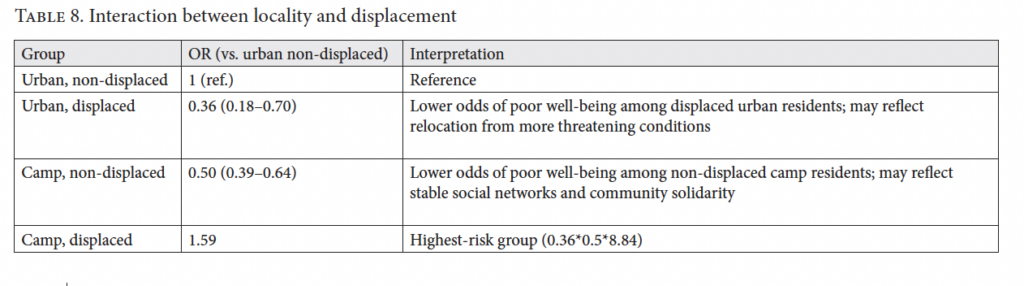
Our findings showed a significant interaction between residence locality and displacement status in relation to well-being. Urban non-displaced participants served as the reference group. Compared with this group, displaced urban residents had lower odds of poor well-being (OR = 0.36, p = 0.003), as did residents of stable refugee camps who were not recently displaced (OR = 0.50, p < 0.001). In contrast, participants originating from refugee camps who had been displaced within the past two years had higher odds of poor well-being (combined OR = 1.59, p < 0.001), reflecting the combined effects of camp origin, displacement, and their interaction (Table 8).
Discussion
In this study, we found high levels of poor well-being among adults living in three Palestinian refugee camps and their surrounding urban areas in the West Bank, with nearly three-quarters reporting poor well-being. These findings emerged during a period of intensified political violence, coinciding with the war on the Gaza Strip that began in late 2023. The results highlight the central role of economic and material conditions in shaping well-being. Poorer well-being was associated with lower economic status, higher levels of material deprivation, residence in the central West Bank, and specific combinations of locality and displacement status, particularly among displaced refugee camp residents. Household exposure to political violence and human rights violations—whether by the Palestinian Authority or the Israeli military occupation—was also associated with poorer well-being, underscoring how direct exposure to violence and violations permeates everyday family life. At the personal level, living with a chronic disease or condition was likewise associated with lower well-being.
As noted above, nearly three-quarters of study participants reported poor well-being, a high estimate compared with other national and regional studies, but comparable to findings from areas with high war intensity or high levels of political instability. For example, an earlier study in the oPt found that 33.8% of adults reported poor well-being based on the WHO-5 Index during a period without significant political escalation in the West Bank (2012–2013).[22] A cross-sectional study from Syria, conducted during the Syrian conflict that began in 2011, found a drastic decline in mental well-being compared to previous years. Key indicators from the study, which analyzed data from 2008 to 2015, showed a 41.4% increase in negative emotions and a 50% reduction in life satisfaction. Additionally, hope levels declined significantly, reflecting a pervasive sense of despair among the study population.[23] Similarly, a study in northern Uganda found that approximately 75% of internally displaced persons reported experiencing “overthinking,” a condition linked to trauma that can lead to severe mental health issues.[24] These studies, along with our study, illustrate how political instability and war can dramatically deteriorate mental well-being.
In our study, the assessment of structural constraints emphasized that place matters. Regional differences emerged even after adjusting for socioeconomic and political variables. Residents of Ramallah and al-Bireh Governorate, in the central West Bank, had markedly higher odds of low well-being compared with those living in Jenin, in the northern West Bank. Although Ramallah and al-Bireh Governorate is the administrative and economic center of the West Bank, it is also characterized by extreme socioeconomic stratification, high living costs, the dense presence of Palestinian Authority structures, and frequent Israeli military offensives and invasions, factors that generate daily stressors and uncertainty.[25] In contrast, Jenin Governorate in the northern West Bank and Bethlehem Governorate in the southern West Bank are characterized by strong community cohesion, extended kinship networks, and shared collective coping mechanisms that might act as social buffers that help sustain well-being despite high levels of political violence and other structural constraints.[26]
Regression results also showed significant spatial disparities in well-being. The interaction between locality of residence, defined as urban area or refugee camp, and displacement status showed a differentiated pattern of vulnerability that cannot be understood without considering the social meaning of place in the West Bank. People living in urban areas who were displaced from their original place of residence showed lower odds of low well-being compared with urban residents who were not displaced. This might reflect a possibility that this displacement was associated with a move to a relatively safer urban neighborhood, with improved security and greater access to resources, which temporarily enhanced their well-being despite the hardship of the displacement.[27] This finding should not be interpreted as displacement being protective in itself. Rather, it may indicate that some displaced urban residents had moved away from more threatening or insecure conditions and that their reported well-being reflected relative relief from prior fear, threats, or exposure to violence.
Our results also showed that refugee camp residents who were not displaced, primarily those in the central and southern West Bank, had lower odds of poor well-being than non-displaced urban residents. This finding may reflect the protective role of social cohesion and community-based solidarity in refugee camps, which tend to provide emotional and practical support under chronic adversity. Studies from Palestine and elsewhere have similarly documented this protective role. A qualitative study conducted in West Bank refugee camps during the COVID-19 pandemic found that strong community engagement and collaboration among local refugee camp committees fostered solidarity and acted as a protective factor for residents’ psychological well-being. The study suggests that the social fabric and collective organization within refugee camps can provide a sense of security and belonging that helps buffer the effects of chronic stress and instability.[28] Similarly, a study in Cameroon found that internally displaced persons with higher levels of community solidarity reported improved psychological health outcomes and greater community satisfaction and that this solidarity served as a protective factor against psychological distress. The findings suggest that the social cohesion fostered within these communities provides essential emotional and practical support, which is crucial in mitigating the adverse effects of displacement.[29]
In contrast, people who had been living in Palestinian refugee camps and were displaced, primarily from the northern refugee camps, had the highest combined odds of low well-being. This group experienced displacement from environments that are typically protective to them. Expulsion from socially dense, collectively organized communities into more fragmented and uncertain settings may involve the sudden loss of a major psychosocial resource, which could worsen well-being among Palestinians experiencing forced displacement.[30] This pattern challenges dominant global displacement frameworks, which often conceptualize displacement as uniformly harmful or focus predominantly on material losses while overlooking the protective role of stable social ecologies.[31] Our findings suggest that the impact of displacement is deeply conditioned by the characteristics of the place from which people are uprooted and the structural conditions of the places to which they relocate.
Moreover, our results highlight that material deprivation and poor relative economic status consistently predicted lower well-being. This finding is consistent with extensive evidence from the oPt and other settings suggesting that material deprivation, rather than sociopolitical deprivation, is the strongest and most consistent determinant of mental health and subjective well-being. In the oPt, evidence indicates that both material and subjective deprivation exert powerful effects on psychological well-being.[32] Similarly, a global meta-review confirmed that material and subjective deprivation were stronger predictors of depression and low well-being than social or political variables.[33] A study in Switzerland found that restricted standards of living were significantly associated with poorer psychological health even among the employed population, showing that deprivation impacts well-being independently of employment status.[34] Research in Ethiopia and Indonesia has further shown that perceived low social and economic status strongly correlates with poorer mental health among adolescents and families, independent of structural constraints.[35] In a study in Wales, researchers using a large population survey to assess how financial strain shapes psychological well-being found that persons experiencing material deprivation had nearly double the prevalence of low well-being compared with those who were financially secure, showing how economic hardship alone can generate a substantial mental health burden.[36] Together, this evidence suggests that the lived experience of economic scarcity and comparison to others profoundly affects psychological well-being. The consistent pattern across contexts confirms that material deprivation functions as a core structural determinant of mental health in protracted crises.
While material deprivation clearly undermines well-being by limiting access to basic needs and security, its effects are deeply intertwined with exposure to political violence, which shapes daily life in the West Bank of the oPt. Our findings indicate that household exposure to political violence, rather than personal experience or witnessing political violence, was the key predictor of well-being, suggesting that the impact of war and political instability in the oPt is collective as well as personal. This aligns with broader evidence showing that violence echoes through families, communities, and shared living environments, creating a sustained atmosphere of fear and insecurity. Earlier evidence from a large survey of Palestinian adolescents similarly found that while both personal and collective exposure to political violence worsened mental health, collective or household exposure affected psychological well-being through shared instability and disrupted social functioning.[37]
Similarly, research across Palestinian households has found that human insecurity and economic deprivation, experiences typically shared within families, have stronger associations with depressive-like symptoms and trauma-related stress than does direct personal exposure to violence.[38] Household exposure magnifies psychological burden because family members’ suffering through displacement, loss, or violence extends trauma into the collective emotional fabric of the home, deepening feelings of helplessness and loss of control.[39] This pattern mirrors global findings from other conflict zones, where collective or familial trauma predicts more persistent and severe distress than isolated personal experiences because it erodes the social and emotional support systems essential for resilience and recovery.[40]
The negative association between household exposure to political violence and people’s well-being in the oPt becomes more complex when human rights violations are understood as an embedded part of that exposure. Violations stemming from both internal and external sources—family, community, the Palestinian Authority, and the Israeli military occupation—collectively shape the psychosocial environment.[41] Although family- or community-level human rights violations were not significantly associated with poor well-being in our study, this does not mean that these violations are unimportant; rather, this may reflect the strong cohesion and mutual support within Palestinian families and communities in this population, which often buffer the psychological impact of interpersonal or localized stressors. In contrast, violations committed by governing or occupying authorities showed stronger associations with poor well-being and may overwhelm these coping mechanisms by targeting entire households and communities through systemic and prolonged oppression. Studies confirm that persistent human rights abuses, such as arbitrary arrests, home demolitions, and mobility restrictions, undermine well-being and create chronic insecurity, which predicts depression, trauma, and a sense of “being broken or destroyed” among Palestinians.[42] Therefore, human rights violations, especially when enacted by authorities or occupying powers, extend beyond physical harm, institutionalizing poor psychological well-being and reinforcing the cycle of collective distress already rooted in household exposure.
It is important to note that some personal-level characteristics, such as age and sex, were not significantly associated with well-being in this study, while chronic illness, poorer economic status, and material deprivation remained important predictors. This pattern suggests that well-being in the Palestinian context is shaped less by fixed demographic characteristics than by socioeconomic, collective, and political conditions. In most high-income and low- and middle-income country settings, higher education, income, and social capital are consistently associated with better self-rated health and subjective well-being, even among people with chronic illness.[43] Studies show that disparities in well-being are often explained by socioeconomic resources and access to care rather than illness alone.[44] However, the significance of chronic illness in Palestine reflects the intersection of health vulnerability and structural deprivation. Under conditions of prolonged occupation, movement restrictions, economic instability, and health care shortages, managing chronic disease becomes a source of continuous psychological distress rather than simply a medical concern.[45]
Research in the oPt and other politically constrained and conflict-affected contexts has shown that barriers to health care access, medication shortages, and the erosion of medical infrastructure exacerbate both physical suffering and emotional strain.[46] This is consistent with findings from other protracted crises, such as Ethiopia, where anxiety and depression among displaced populations are better explained by displacement frequency and social support than by demographic characteristics.[47] Taken together, these findings suggest that in the Palestinian context, chronic illness functions as both a medical and psychosocial burden, reflecting how enduring instability transforms health vulnerability into a continuous source of stress that reinforces broader cycles of collective distress.
Conclusion
This study has shown that in the Palestinian context, well-being is shaped by cumulative socioeconomic and political vulnerabilities. Consistent with earlier research, our study suggests that daily stressors, material deprivation, poverty, and political violence are far stronger predictors of well-being than most fixed demographic characteristics, such as age and sex.[48] Our findings show that displacement, poverty, political violence, and human rights violations are powerful structural and political determinants of low well-being. Displacement, however, is not uniformly harmful; its effects depend on social and spatial contexts. Long-lasting Palestinian refugee camps often provide cohesive environments that buffer against distress, whereas displacement from such protective spaces, combined with ongoing instability, deepens psychological suffering.[49] These patterns highlight that place, stability, and collective belonging are critical dimensions of health under prolonged occupation.
While addressing structural constraints that undermine health and well-being remains essential, this may be difficult to target or achieve under current political and social conditions. Still, there are practical steps that can help reduce daily hardship and promote well-being. Strengthening social protection systems is important for easing material deprivation, especially for displaced families who remain excluded from formal safety nets. Supporting community-based networks of solidarity and collective strength can also help sustain psychosocial well-being during ongoing adversity. Integrating contextually and culturally appropriate mental health care into primary care, through community-led and locally grounded approaches, may further promote recovery and preserve dignity in local settings.
Improving well-being in Palestine requires recognizing that displacement, fragmentation, and continuing political violence are not only political or social issues but central public health concerns. The right to health depends on addressing long-term structural constraints, in addition to enhancing the collective strength of communities to protect life and dignity under occupation.
Strengths and limitations
This study has several strengths. We relied on a large, diverse sample and used locally validated measures that captured the lived realities of Palestinians under occupation. By integrating the socio-ecological framework and the World Health Organization’s framework on the social determinants of health, we highlighted how structural constraints affecting groups in the population, rather than personal traits affecting individuals, shape well-being. However, the purposive sampling limits generalizability, and the cross-sectional design prevents causal inference. Self-reported data may involve bias, and mobility restrictions constrained access to some areas.
In relation to exposure to political violence, although the survey captured the reported perpetrator of political violence, including Israeli settlers, settler violence was not analyzed separately in this paper because the selected study locations were more directly exposed to military occupation practices, while settler violence is more geographically concentrated in specific areas of the West Bank and was less frequently reported in our sample.
Funding
This paper was partially supported by the Open Society Foundations (grant number OR2024-95119).
Rula Ghandour, PhD, is an assistant professor in public health at the Institute of Community and Public Health, Birzeit University, occupied Palestinian territory.
Abdullatif Husseini, PhD, is a full professor of epidemiology and public health at the Institute of Community and Public Health and the Salim Edde Chair in Community and Public Health, Birzeit University, occupied Palestinian territory.
Shiraz Nasr, MS, is an academic researcher at the Institute of Community and Public Health, Birzeit University, occupied Palestinian territory.
Rita Giacaman, PhD, is a full professor of public health, Institute of Community and Public Health, Birzeit University, occupied Palestinian territory.
Please address correspondence to Rula Ghandour. Email: rghandour@birzeit.edu.
Competing interests: None declared.
Copyright © 2026 Ghandour, Husseini, Nasr, and Giacaman. This is an open access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] C. A. Sousa, “Political Violence, Collective Functioning and Health: A Review of the Literature,” Medicine, Conflict and Survival 29/3 (2013).
[2] O. Tanous, “Structural Violence and Its Effects on Children Living in War and Armed Conflict Zones: A Palestinian Perspective,” International Journal of Health Services 52/1 (2022).
[3] W. Hammoudeh, S. Mitwalli, R. Kafri, et al., “The Mental Health Impact of Multiple Deprivations Under Protracted Conflict: A Multi-Level Study in the Occupied Palestinian Territory,” PLOS Global Public Health 2/12 (2022); C. McNeely, B. K. Barber, C. Spellings, et al., “Prediction of Health with Human Insecurity and Chronic Economic Constraints in the Occupied Palestinian Territory: A Cross-Sectional Survey,” Lancet 382/S25 (2013).
[4] H. Schmitz and K. Sikkink, “International Human Rights,” in W. Carlsnaes, T. Risse, and B. A. Simmons (eds), Handbook of International Relations, 2nd edition (Sage, 2013).
[5] S. Sivakumaran, “Re-Envisaging the International Law of Internal Armed Conflict,” European Journal of International Law 22/1 (2011); S. C. S. Guerra, L. E. Nagle, and Á. S. F. da Silva, “Human Rights Violations Perpetrated by State Agents in Military Occupations: Analysis of the Incursion of International Human Rights Law to the Normative Territory of the Armed Conflicts,” Revista Opinião Jurídica 19/32 (2021).
[6] Tanous (see note 2); McNeely et al. (see note 3).
[7] Tanous (see note 2).
[8] R. Giacaman, H. S. Shannon, H. Saab, et al., “Individual and Collective Exposure to Political Violence: Palestinian Adolescents Coping with Conflict,” European Journal of Public Health 17/4 (2007).
[9] R. Giacaman, R. Ghandour, and W. Hammoudeh, “Measuring Human Rights Violations from an Ecological Perspective Using a Locally Generated Instrument: A Cross-Sectional Study of Palestinians in the Israeli-Occupied West Bank,” Frontiers in Public Health 13 (2025).
[10] R. Giacaman, “Reframing Public Health in Wartime: From the Biomedical Model to the ‘Wounds Inside’,” Journal of Palestine Studies 47/2 (2018).
[11] Hammoudeh et al. (see note 3).
[12] K. Bates, T. Leone, R. Ghandour, et al., “Women’s Health in the Occupied Palestinian Territories: Contextual Influences on Subjective and Objective Health Measures,” PLOS One 12/10 (2017); Hammoudeh et al. (see note 3); McNeely et al. (see note 3).
[13] World Health Organization, “A Conceptual Framework for Action on the Social Determinants of Health,” Discussion Paper (2010).
[14] S. D. Golden and J. A. L. Earp, “Social Ecological Approaches to Individuals and Their Contexts: Twenty Years of Health Education and Behavior Health Promotion Interventions,” Health Education & Behavior 39/3 (2012).
[15] Giacaman et al. (2025, see note 9).
[16] Ibid.
[17] C. W. Topp, S. D. Østergaard, S. Søndergaard, and P. Bech, “The WHO-5 Well-Being Index: A Systematic Review of the Literature,” Psychotherapy and Psychosomatics 84/3 (2015).
[18] R. Ladadwa, S. Nasr, and R. Giacaman, Investigating Human Rights Violations Experienced by Palestinians on the West Bank of the Occupied Palestinian Territory (Opt) (Institute of Community and Public Health, Birzeit University, 2022); Giacaman et al. (2025, see note 9).
[19] Giacaman et al. (2007, see note 8).
[20] Hammoudeh et al. (see note 3).
[21] Giacaman et al. (2025, see note 9).
[22] N. Harsha, L. Ziq, R. Ghandour, and R. Giacaman, “Well-Being and Associated Factors Among Adults in the Occupied Palestinian Territory (Opt),” Health and Quality of Life Outcomes 14/1 (2016).
[23] F. Cheung, A. Kube, L. Tay, et al., “The Impact of the Syrian Conflict on Population Well-Being,” Nature Communications 11 (2020).
[24] B. Roberts, V. N. Odong, J. Browne, et al., “An Exploration of Social Determinants of Health Amongst Internally Displaced Persons in Northern Uganda,” Conflict and Health 3 (2009).
[25] L. Taraki, “Urban Modernity on the Periphery: A New Middle Class Reinvents the Palestinian City,” Social Text 26/2 (2008).
[26] I. Kawachi and L. F. Berkman, “Social Ties and Mental Health,” Journal of Urban Health 78/3 (2001).
[27] A. Nikuze, R. Sliuzas, J. Flacke, and M. van Maarseveen, “Livelihood Impacts of Displacement and Resettlement on Informal Households: A Case Study from Kigali, Rwanda,” Habitat International 86 (2019).
[28] L. Shakhshir and W. Hammoudeh, “Responding to the COVID-19 in West Bank Palestine Refugee Camps: Lessons and Role of Community Engagement,” BMC Public Health 25/1 (2025).
[29] A. E. Tassang, S. Guoqing, T. Y. Akintunde, et al., “Social Integration, Solidarity, and Psychological Health of Internally Displaced Persons in Cameroon: Exploring the Role of Community Satisfaction,” Heliyon 9/10 (2023).
[30] Y. E. Masri, “72 Years of Homemaking in Waiting Zones: Lebanon’s ‘Permanently Temporary’ Palestinian Refugee Camps,” Frontiers in Sociology 5 (2020); Y. El-Zakka and J. L. Diab, “Youth Development and Spatial Configurations: Socio-Spatial Inequalities in Palestinian Refugee Camps in Lebanon,” Frontiers in Sociology 8 (2023).
[31] M. Porter and N. Haslam, “Predisplacement and Postdisplacement Factors Associated with Mental Health of Refugees and Internally Displaced Persons: A Meta-Analysis,” JAMA 294/5 (2005).
[32] Hammoudeh et al. (see note 3).
[33] I. Dougall, M. Vasiljevic, J. D. Wright, and M. Weick, “How, When, and Why Is Social Class Linked to Mental Health and Wellbeing? A Systematic Meta-Review,” Social Science & Medicine 343 (2024).
[34] S. Vetter, J. Endrass, I. Schweizer, et al., “The Effects of Economic Deprivation on Psychological Well-Being among the Working Population of Switzerland,” BMC Public Health 6 (2006).
[35] C. Owens and C. Hadley, “Subjective Social Status and Mental Health Among Adolescents in Ethiopia: Evidence from a Panel Study,” SSM – Population Health 22 (2023); I. Borualogo, S. Kusdiyati, and H. Wahyudi, “Subjective Well-Being and Material Deprivation During COVID-19 Pandemic: A Study in Children and Adolescents in Indonesia,” Jurnal Psikologi (2022).
[36] J. Allen, A. Cotter-Roberts, O. Darlington, et al., “Understanding Health Inequalities in Wales Using the Blinder-Oaxaca Decomposition Method,” Frontiers in Public Health 10 (2022).
[37] Giacaman et al. (2007, see note 8).
[38] McNeely et al. (see note 3).
[39] B. K. Barber, C. McNeely, J. A. Olsen, et al., “Effect of Chronic Exposure to Humiliation on Wellbeing in the Occupied Palestinian Territory: An Event-History Analysis,” Lancet 382/S7 (2013).
[40] Hammoudeh et al. (see note 3).
[41] Giacaman et al. (2025, see note 9).
[42] A. Christian, O. Sanuade, M. Okyere, and K. Adjaye-Gbewonyo, “Social Capital Is Associated with Improved Subjective Well-Being of Older Adults with Chronic Non-Communicable Disease in Six Low- and Middle-Income Countries,” Globalization and Health 16/1 (2020).
[43] K. Hauck, S. Martin, and P. Smith, “Priorities for Action on the Social Determinants of Health: Empirical Evidence on the Strongest Associations with Life Expectancy in 54 Low-Income Countries, 1990–2012,” Social Science & Medicine 167 (2016).
[44] A. Lohana, A. Gulati, J. Kumar, et al., “The Silent Victims: How the Israel-Palestine War Impacts the Management of Chronic Kidney Disease and End-Stage Renal Disease Patients,” Cureus 16/3 (2024).
[45] R. Giacaman, R. Khatib, L. Shabaneh, et al., “Health Status and Health Services in the Occupied Palestinian Territory,” Lancet 373/9666 (2009); Bates et al. (see note 12).
[46] Giacaman et al. (2009, see note 45); Bates et al. (see note 12).
[47] S. Bekeko, F. Mekonnen, and R. E. Teklu, “Post-Traumatic Stress Disorder, Depression, Anxiety, and Their Predictors Among Internally Displaced Persons in a Conflict-Affected Area of Metekel Zone, Northwest Ethiopia: Structural Equation Modeling,” Frontiers in Psychiatry 16 (2025).
[48] K. E. Miller and A. Rasmussen, “War Exposure, Daily Stressors, and Mental Health in Conflict and Post-Conflict Settings: Bridging the Divide between Trauma-Focused and Psychosocial Frameworks,” Social Science & Medicine 70/1 (2010).
[49] Cheung et al. (see note 23); Tassang et al. (see note 29).