Evaluation of the United States’ Permitless Concealed Carry Laws and Child Health in the ECHO Cohort
CHILDREN’S RIGHT TO HEALTH, Vol 28/1, 2026, pp. 23-39 PDF
Marie L. Churchill, Emily A. Knapp, Alexander D. McCourt, Nandita Somayaji, Courtney K. Blackwell, Lyndsay A. Avalos, Kelly A. Hirko, Kaja Z. LeWinn, Johnnye Lewis, Yeyi Zhu, Alison E. Hipwell, Margaret R. Karagas, Kristen Lyall, Jody M. Ganiban, Nigel Paneth, T. Michael O’Shea, Christine C. Johnson, Carlos A. Camargo, Jr., Cassandra K. Crifasi, and Aruna Chandran, for the ECHO Cohort Consortium*
* A full list of collaborators is available from the authors.
Abstract
Firearms are the leading cause of death among children in the United States (US). As of 2023, half of US states had enacted laws allowing permitless concealed carry of firearms. Our cross-sectional study evaluated the association between permitless concealed carry laws and child general health using data from the nationwide Environmental influences on Child Health Outcomes (ECHO) Cohort collected between 2003 and 2023. Children aged 1–21 years with caregiver- or self-reported general health status were included. Secondary outcomes included child internalizing and externalizing behaviors and child stress. Regression models estimated the association of exposure to state-level permitless concealed carry laws six months prior to each outcome, adjusted for individual- and area-level covariates. One-fifth (20.9%) of the sample (n = 11,325) lived in states allowing permitless concealed carry of a handgun. Children living in these states were 25% less likely (OR: 0.75, 95% CI: 0.60, 0.95) to report excellent/very good general health and had psychological stress scores 0.21 standard deviations higher (β = 0.21, 95% CI: 0.10, 0.31) than children in other states. There was no statistically significant association with internalizing or externalizing behavior scores. Our study found that children living in states that allow permitless concealed carry of firearms had worse general health and higher stress, suggesting the need for policy changes to address gun violence as a public health and human rights crisis.
Introduction
The United States (US) has the highest rates of firearm ownership and firearm-associated homicide among high-income countries. Recent reports show a civilian firearm ownership rate of 120.5 per 100 people in 2017 (compared to 34.7 per 100 people in Canada) and a firearm-associated homicide rate of 5.4 per 100,000 population in 2023 (compared to 0.72 per 100,000 population in Canada).[1] During the COVID-19 pandemic, firearm ownership became more widespread in the United States, with 7.5 million new gun owners, exposing over 11 million additional individuals to firearms.[2] Since 2020, firearms have been the leading cause of death among US children and adolescents.[3] Beyond the individual mortality and injury associated with gun violence, spillover effects are incurred by communities. Exposure to gun violence contributes to poorer overall community health, with communities experiencing high levels of poverty, unemployment, and other disadvantages being particularly at risk.[4] Several studies have shown associations between community gun violence and adverse child mental and physical health outcomes.[5] For example, among Black, White, and Hispanic high school students in the United States, witnessing community violence was associated with increased odds of carrying a firearm, substance use, and suicide risk.[6] Moreover, a recent study from the Environmental influences on Child Health Outcomes (ECHO) Cohort showed that the odds of very good to excellent general health were 20% lower among children living in census tracts with high gun violence.[7]
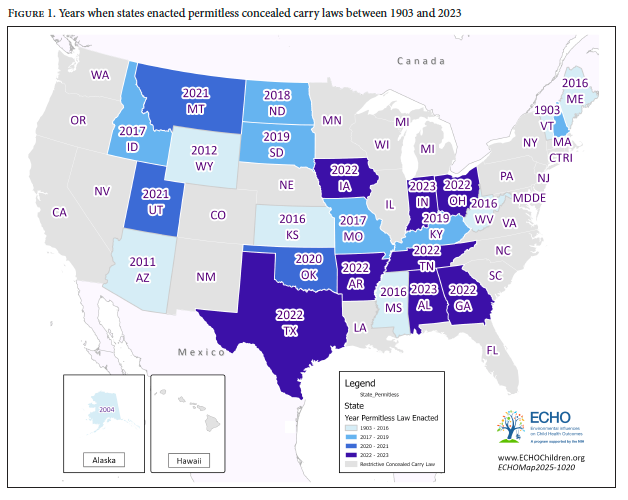
In addition to the rising rates of gun ownership in the United States, firearm laws have loosened considerably over the past 20 years. For the majority of US history, most states required gun carriers to apply for a permit, undergo background checks, obtain a license, or receive training to obtain and carry a concealed gun legally.[8] However, the number of states with permitless concealed carry laws has risen sharply since 2010, when only two states had such laws in place; by the end of 2023 (Figure 1), half of states had enacted such laws, and currently, most states (29 in total) have done so. These laws allow concealed firearms to be carried without any permitting or licensure from law enforcement or other government officials and are often linked with the removal of requirements for firearm training, placing gun owners and those around them at increased risk. A 2024 study found that states that had adopted permitless concealed carry laws and discontinued live firearm training protocols experienced an increase of 32% in gun assaults, the equivalent of 21 gun assaults per 100,000 people.[9] Furthermore, states that had abandoned the legal prohibition of gun permits to individuals convicted of a violent misdemeanor had an 8.5% increase in gun assaults compared to before the prohibition was dropped.[10] Another study found that after the legalization of carrying a concealed firearm without a permit in West Virginia, homicides and suicides increased by 48% and 22%, respectively.[11] Conversely, lower firearm mortality rates have been observed in states with more gun ownership restrictions: restrictive policies on gun ownership were associated with substantial reductions in gun-related mortality between 1991 and 2016.[12]
Permitless concealed carry laws lower barriers for legally carrying firearms in public. In some states, these laws allow younger adults (18–20 years old), individuals without gun safety training, and those who have not passed background checks to carry concealed guns in public.[13] A higher rate of gun ownership among younger adults and those not receiving a background check or training may lead to a higher rate of youth exposure to guns and gun violence.[14] This, in turn, may increase fear and stress. Exposure to gun violence is associated with posttraumatic stress symptoms among children and with increases in children’s acute mental health symptoms.[15] Higher levels of gun violence in communities stymie educational attainment and well-being: among third graders in Syracuse, New York, higher rates of neighborhood gun violence were associated with higher rates of failure on New York State’s standardized tests.[16] Among 15-year-olds from 20 large US cities, community exposure to gun homicide was associated with lower aspirations of high school graduation.[17] Studies have shown mixed results on the association between exposure to gun violence and internalizing and externalizing behaviors; to our knowledge, there have been no studies examining the effects of increased visibility of guns on child mental health outcomes.[18] It is plausible that increased exposure to guns themselves will result in poorer child health as well as manifestations of increased internalizing and externalizing behavior and reported stress.
As framed by the United Nations High Commissioner for Human Rights, gun violence is not only a public health crisis but an infringement of children’s rights to “health, education … and the right to participate in the cultural life of the community.”[19] Scholars have called out gun availability and ineffective gun control policies and regulations as key factors in the epidemic of firearm violence observed in the United States compared with other high-income countries.[20] Understanding the effects of firearm-related policies on child health and well-being is critical to addressing gun violence as a public health and human rights crisis.
Given this context, our study aimed to evaluate the impact of permitless concealed carry laws on child and adolescent health. To our knowledge, there have been no studies examining associations between permissive handgun policies and individual-level child health outcomes. We sought to fill this gap using data from the nationwide ECHO Cohort. We hypothesized that permitless concealed carry laws would be associated with lower general health status, higher internalizing (e.g., anxiety, social withdrawal) and externalizing (e.g., aggression, defiance) behavior scores, and higher stress scores among children.
Methods
Study design and participants
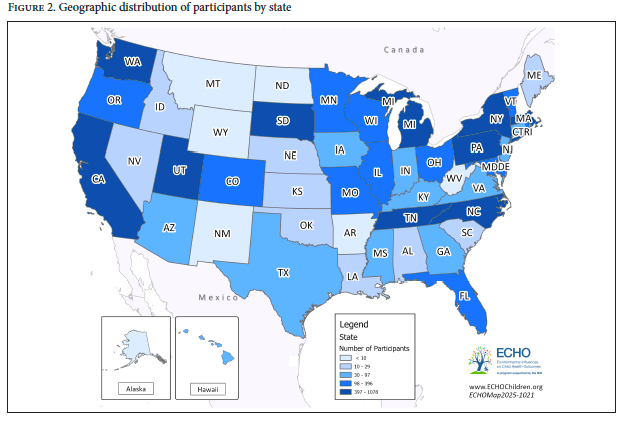
The present study leveraged data from 11,325 children participating in the ECHO Cohort, a longitudinal study of children’s health and well-being in the United States.[21] Participants in our sample were enrolled in 55 cohort sites and lived in all 50 states (Figure 2), with data collection conducted from 2003 to 2023. The ECHO Institutional Review Board or corresponding local institutional review board approved the study procedures, and written informed consent for participation was obtained. The research was performed in accordance with the Declaration of Helsinki.
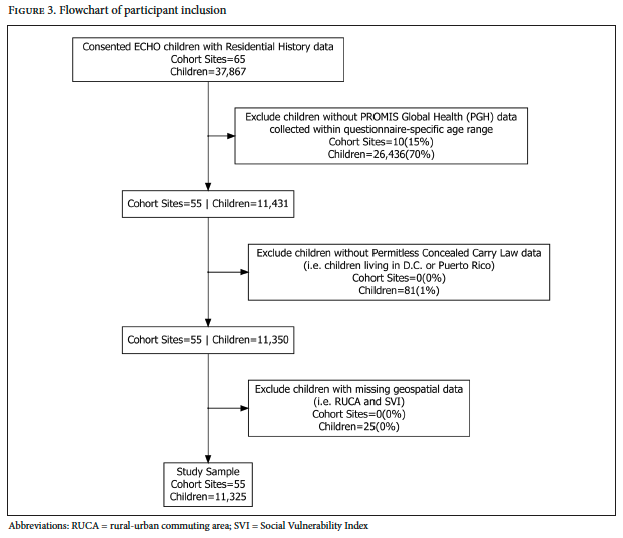
This analysis included ECHO children with (1) at least one report of the general health item from the Patient-Reported Outcomes Measurement Information System (PROMIS©) Global Health Scale, (2) a reported residential address six months prior to the PROMIS© Global Health measurement, (3) data on corresponding state- and year-specific status of permitless concealed carry law (this information was unavailable for Washington, D.C., and Puerto Rico; n = 81 participants excluded), and (4) non-missing geospatial covariates (n = 25 participants excluded) (Figure 3).[22]
Concealed carry exposure
Based on exposure to permitless concealed carry six months prior to outcome assessment, participants were categorized as either 1 (permits not required in state of residence) or 0 (permits required).[23] State-level permitless concealed carry information was obtained by researchers with the Center for Gun Violence Solutions for all 50 states from 1990 to 2023.[24]
Outcomes
Child general health. The primary outcome of interest was child general health: “In general, would you say your (child’s) health is: Excellent, Very Good, Good, Fair, or Poor.”[25] Responses were dichotomized as (1) excellent/very good and (0) poor/fair/good.[26] Child general health was reported by caregivers for children aged 1–7 years and self-reported by children aged 8–21 years.
Child behavior. Child internalizing and externalizing behavior was assessed using caregiver reports on the Child Behavior Checklist for Ages 1.5–5 and the Child Behavior Checklist for Ages 6–18, which are commonly used measures of emotional and behavioral functioning.[27] For this analysis, the internalizing (anxious, depressed, withdrawn, and somatic complaints) and externalizing (rule-breaking and aggressive behavior) broadband scale T scores were used, where higher T scores represent more problems. The two Child Behavior Checklist (CBCL) T scores, which were normed to a mean of 50 and a standard deviation (SD) of 10, were scaled for analysis to represent a 1-SD change for ease of interpretation.
Child psychological stress. Children’s stress was measured using T scores (mean 50, SD 10) calculated from responses on the pediatric and parent-proxy versions of the PROMIS© Psychological Stress Experiences (PPSE) form for ages 5–17 years.[28] The PPSE assesses a child’s thoughts and feelings of themselves and the world through questions relating to overwhelm, lack of control, and stress, with higher scores representing more stress. For the analysis, the PPSE T score was scaled by 10, the population-normed standard deviation.
Timing of outcomes and exposure. The first recorded observation was selected for analysis if multiple assessments were available. To allow for potential effects of the exposure to occur, six-month lags between the status of the permitless concealed carry law and the date of collection of each outcome were implemented.
Covariates
Individual measures. We included the following individual-level covariates: child sex (male or female), caregiver-identified child race (American Indian or Alaska Native, Asian, Black, Native Hawaiian or other Pacific Islander, White, other race, or multiple races) and ethnicity (Hispanic or non-Hispanic), age at outcome assessment, maternal education (less than high school degree, high school degree or equivalent, some college but no degree, or bachelor’s degree and above), household income (less than $30,000, $30,000–$49,999, $50,000–$74,999, $75,000–$99,999, $100,000–$199,999, or $200,000 or more), and cohort site type (sites with participants drawn from the general population, sites that recruited infants in neonatal intensive care units, sites enriched for autism spectrum disorder, or sites enriched for asthma). In addition, COVID-19 pandemic timing indicators were created (outcome collected on or after March 13, 2020, versus before March 13, 2020).
Geospatial measures. States that enact permitless concealed carry laws are likely to differ on other factors that may influence child health; therefore, we adjusted for a robust set of area-level characteristics. We included census tract-level measures of rurality using the US Department of Agriculture’s rural-urban commuting area codes and socioeconomic status (SES) using the Centers for Disease Control and Prevention/Agency for Toxic Substances and Disease Registry Social Vulnerability Index SES theme (derived from tract-level estimates of poverty, unemployment, burden of housing cost, education, and insurance).[29] We included state-level household firearm ownership estimated by RAND; state-level expansion of the Earned Income Tax Credit law (yes or no) as a proxy for state-level policies supporting families; and American Community Survey five-year estimates of median household income, population density, and total population 25 years or older with a bachelor’s degree and above.[30] All geospatial measures were linked to the tract or state of the child at the time of the exposure.
Statistical analysis
Missing data on household income (8.3%), maternal education (2.4%), child race (1.4%), and ethnicity (<1%) were imputed using multiple imputation by chained equations from the “mice” R package.[31] Results were pooled after 25 imputations, with a maximum of 10 iterations. Imputation models included our variables of interest and used family as a cluster variable to impute missing income and education, which were the same within a maternal family.
To explore the association of permitless concealed carry laws and child general health status, we employed logistic regression. Similarly, to explore the association of permitless concealed carry laws and child behavior and stress, we employed linear regressions. Covariates were selected based on prior literature, and all models were adjusted for corresponding state and year of permitless concealed carry law exposure status, COVID-19 pandemic indicator, child sex, child race and ethnicity, maternal education, household income, cohort site type, rural/urban status and socioeconomic vulnerability (Social Vulnerability Index SES), state-level Earned Income Tax Credit status, estimated firearm ownership, state median household income, population density, and population with bachelor’s degree or higher.[32] To explore potential variation in associations across cohort sites, we performed leave-one-out analyses. All analyses were run using R version 4.4.0, and an alpha-level of 0.05 was used.
Results
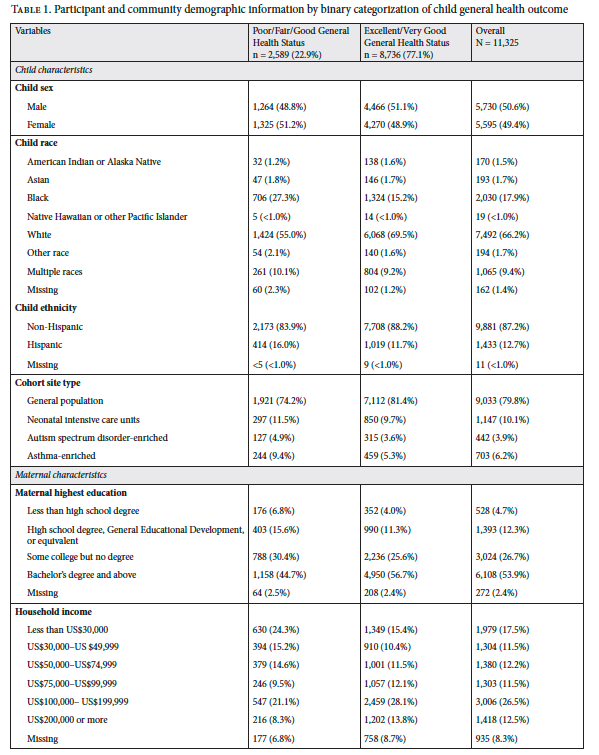
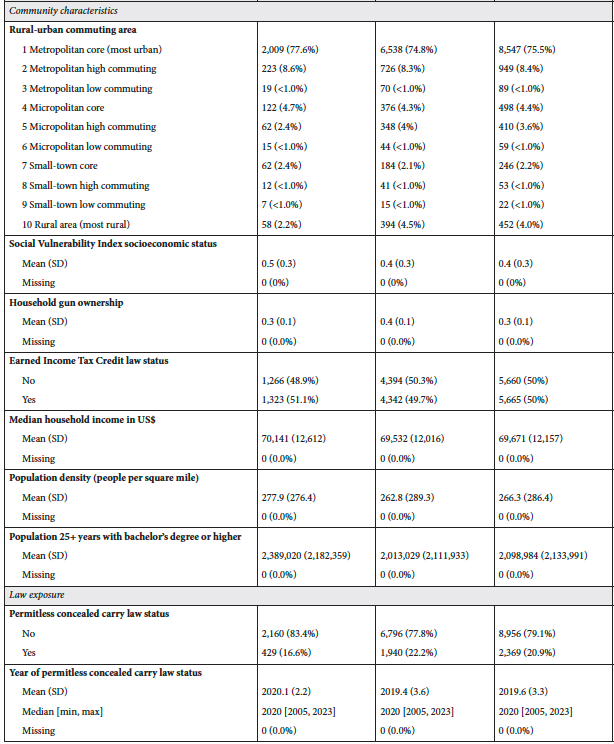
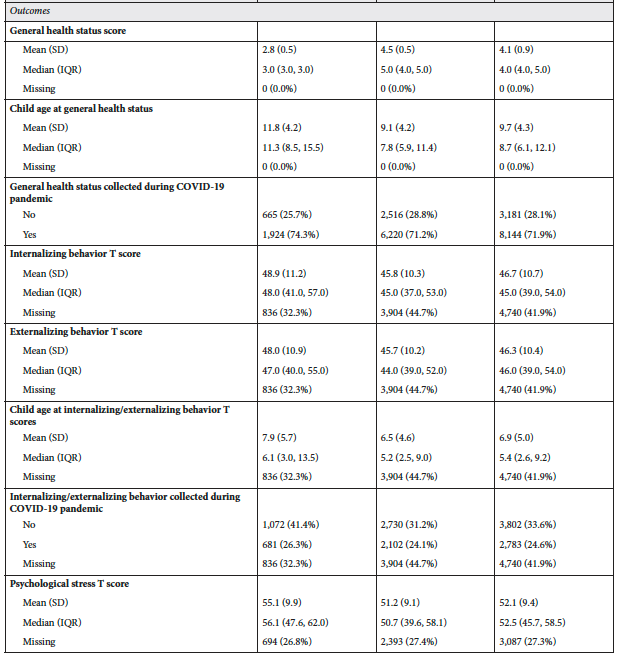
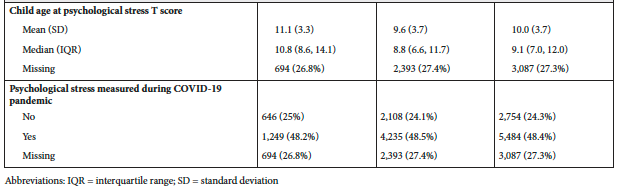
Our study population was 50.6% male and represented a diverse sample of children across race (1.5% American Indian or Alaska Native, 1.7% Asian, 17.9% Black, <1.0% Native Hawaiian or other Pacific Islander, 66.2% White, 1.7% other races, and 9.4% multiple races) and ethnicity (12.7% Hispanic) (Table 1). The majority of children had college-educated mothers (53.9% with a bachelor’s degree and above). Slightly less than a third (29.0%) reported household income of less than $50,000, whereas over a third (39.0%) reported household income of $100,000 or more. The mean age at general health assessment was 9.7 years (SD = 4.3 years), with age ranging from 1 to 21 years, and 22.9% of the sample reported low general health; the majority (71.9%) of the sample had data collected during and after the COVID-19 pandemic. One-fifth (20.9%) of the sample lived in states that allowed permitless concealed carry of a handgun (mean year 2020, years ranging from 2005 to 2023). Most participants had CBCL data (58.1%, n = 6585), with a mean internalizing T score of 46.7 (SD = 10.7) and externalizing T score of 46.3 (SD = 10.4). Slightly under three-quarters of the sample (72.7%, n = 8238) had PPSE data, with a mean PPSE T score of 52.1 (SD = 9.4). Three-quarters of the sample lived in metropolitan areas (84.6%) and had low vulnerability, with a mean Social Vulnerability Index SES score of 0.40 (SD = 0.30). Half of the sample (50.0%) lived in states with Earned Income Tax Credit laws. The average state-level gun ownership rate per household was 0.30 firearms (SD = 0.10). Overall, the states in which participants lived had a median household income of US$69,671 (SD = US$12,157) and a mean population density of 266.3 people per square mile (SD = 286.4). Additional characteristics of the subset of the study population with CBCL or PPSE outcome data are presented in Supplementary Table 1 (available from the authors).
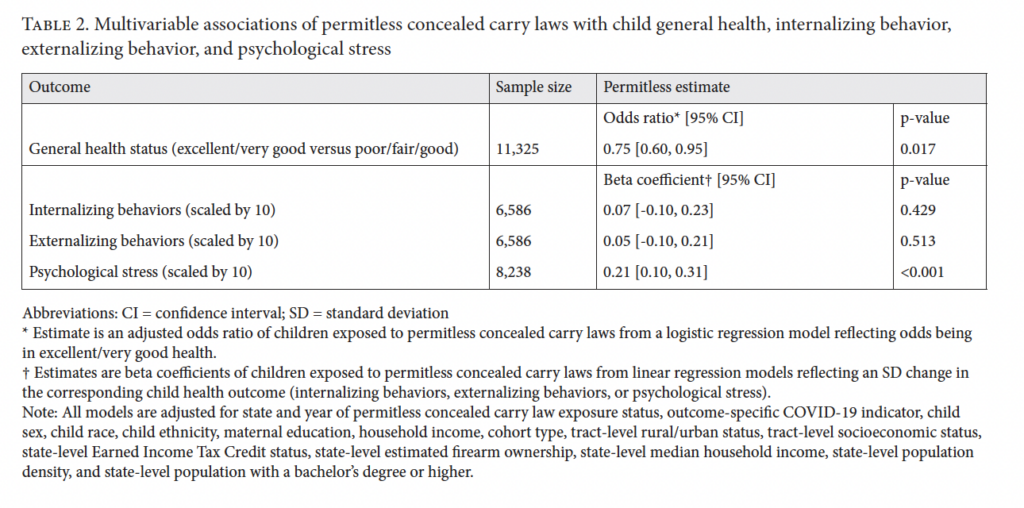
Permitless concealed carry laws were significantly associated with caregiver and self-reported child general health and psychological stress after adjusting for individual- and area-level covariates. Children exposed to permitless concealed carry laws had 25% lower odds of excellent/very good child health (adjusted odds ratio = 0.75, 95% confidence interval (CI): [0.60, 0.95]) (Table 2). Additionally, children exposed to permitless concealed carry laws had psychological stress scores 0.21 standard deviations higher (β = 0.21, 95% CI: [0.10, 0.31]). Permitless concealed carry laws were not statistically significantly associated with internalizing (β = 0.07, 95% CI: [-0.10, 0.23]) or externalizing (β = 0.05, 95% CI: [-0.10, 0.21]) scores. Analyses leaving out individual cohorts one at a time indicated that the results were robust to the influence of individual cohort sites, as CIs overlapped and the associations found were consistent in direction and magnitude (Supplementary Figures 1 and 2, available from the authors).
Discussion
Independent of area- and individual-level demographic and social characteristics, permitless concealed carry laws are associated with lower child general health status and higher levels of stress in children in a national cohort of US children. To our knowledge, this is the first large-scale examination of associations between state-level concealed carry laws and individual-level child health outcomes. We found that children living in states with permitless concealed carry laws were 25% less likely to report excellent or very good general health status. This finding was comparable to the effect size found in a similar study that explored the association of community-level gun violence with the same outcome, which found that individuals living in census tracts with high gun violence were 20% less likely to endorse excellent or very good general health status.[33] Our study also found that children living in states with permitless concealed carry laws scored 2.1 points higher on psychological stress than children living in states without these laws, which is a modest yet meaningful difference for a widespread community exposure.[34]
These findings highlight that all US children are at risk of being negatively affected by exposure to guns, and not just at risk of firearm-associated violence. In 2017, it was estimated that US civilians owned a total of 393.3 million firearms.[35] During the COVID-19 pandemic, an additional 7.5 million US adults became first-time gun owners, which in turn exposed an additional 5 million children to guns.[36] The US Bureau of Alcohol, Tobacco, Firearms and Explosives’ National Firearms Act Division processed 1.9 million firearm applications in 2019 and 3.6 million in 2023.[37] Additionally, in 2023, it was estimated that 32% of US adults owned a gun (up from 22% in 2015) and that 42% lived in a house with a gun, and in 2019, it was estimated that 6 million US adults carried loaded handguns in public daily.[38] Gun ownership in the United States is continuing to rise, and combined with the increasing visibility of guns through permitless carry laws, this increases children’s gun exposure and poses a risk that could be mitigated through policy intervention.
The direct risks of these trends are clear. Firearms are the leading cause of death among children in the United States.[39] Recent US reports show that 79% of all homicides are by firearms and that an average of seven children aged 1–17 die each day by a firearm.[40] Notably, the suicide rate among adolescents and young adults (10–24 years) increased from 2007 to 2021, and homicide rates increased from 2014 to 2021.[41] In addition, state-level permitless concealed carry laws are associated with higher rates of homicide, suicide, and gun assaults, and in general, gun death rates tend to be higher in states with weaker gun laws.[42] Moreover, the nation is trending toward more permissive gun laws, illustrated by an additional six states enacting permitless concealed carry laws since 2023 and 15 states since 2020.[43]
The indirect risks of firearms for US children are also substantial. Community gun violence has been linked to an array of mental and physical health outcomes, including increased anxiety, depression, posttraumatic stress, increased substance use, poorer test scores, and a worse outlook on the future.[44] Though gun violence varies geographically and is concentrated in certain areas, gun exposure is widespread across the nation. Our findings suggest that this exposure comes with risk to US children: living in a state with permissive gun laws was associated with poorer overall health and increased stress.
Promoting the health and well-being of children is fundamentally intertwined with protecting their rights; gun violence remains a public health crisis that not only violates the rights of victims but also has spillover effects on society as a whole.[45] While acknowledging the tension between protecting individual liberties and promoting societal safety, experts generally agree that restrictive gun laws are essential both to protect citizens from direct harm and to promote their rights to participate in all aspects of life.[46] The United Nations Convention on the Rights of the Child—adopted in 1989, ratified by nearly every nation, and signed by the United States—establishes international standards for the protection of children. The treaty declares that states are responsible for ensuring children’s rights to safety, development, and well-being.[47] Specifically, article 19 requires states to “take all appropriate legislative, administrative, social, and educational measures to protect children from physical or mental violence, injury, abuse, neglect, maltreatment, and exploitation.”[48] To meet this standard, governments are obligated to enact comprehensive laws that protect children from threats, which includes protection from gun violence. Previous evidence has linked permissive concealed carry laws to homicide, suicide, gun assaults, and gun deaths; our findings further suggest that permitless concealed carry laws represent one type of modifiable legislation that worsens child health and well-being.[49] In accordance with the Convention on the Rights of the Child, governments have a human rights duty to enact and enforce reasonable firearm regulations to protect children from harm. Permissive gun laws should therefore be viewed not only as a public health concern but also as a children’s health and children’s rights issue.
Limitations
This study has several limitations that should inform future research. First, although we had data from every state from the past two decades, we implemented a cross-sectional analysis since we did not have sufficient data to examine individuals’ health scores before and after changes in state laws. As a result, quasi-experimental and longitudinal methods that leverage specific thresholds to evaluate individuals on either side of the threshold were not feasible. We believe that such studies should be performed in the future. Second, we combined child self-reports and caregiver reports of child general health and stress to maximize the sample size. Parental and child reports of psychological constructs are not highly correlated, and combining the two may introduce measurement error. However, several published studies have combined child self-reports and caregiver reports.[50] Third, caregiver reports of preschool behaviors on the CBCL in diverse samples can be subject to measurement bias, and 31.2% of our sample had this measure, though the associations found were null.[51] Thus, due to our reliance on caregiver and self-reported measurement and measurement bias, more in-depth assessments for general health, behavioral health, and stress are needed. Last, we found that exposure to permitless concealed carry laws was associated with general health and stress but not behavior. In our sample, only 9.1% of children with CBCL data were exposed to such laws, compared to 20.9% and 18.9% with the general health and stress outcomes, respectively. It is possible that we were unable to detect an association with behavior due to the sample size. However, there may also be differences in how behavior manifests in children and how children feel. Therefore, future research that explores biological mechanisms is warranted.
Strengths
Despite these limitations, our study has many strengths, including the utilization of prospectively collected, individual-level caregiver reports and self-reports of child health in a large, geographically diverse sample representing all 50 US states. To account for unobserved differences between states that may lead to spurious associations, we included state-level effects in our models and adjusted for a robust set of state-level covariates, consistent with other studies of state-level gun policies. Due to the rich child outcome data collected in the ECHO Cohort, we were able to examine a range of health outcomes, including an overall measure of physical and mental health, behavioral outcomes, and psychological stress. Moreover, our study is one of the first to evaluate state-level gun policies on individual health outcomes, broadening our understanding of how children are negatively impacted by gun regulation.
Conclusion
Guns and gun violence are pervasive in the United States and represent a significant threat to public health. Using data from a national study of children’s health and well-being, we found that state-level permitless concealed carry laws were associated with worse general health and increased stress among children living in states with such laws. Together with findings from other studies, our results suggest that enacting more restrictive concealed carry laws is one pathway to securing children’s rights to “health, education … and the right to participate in the cultural life of the community.”[52] Following the international standard established by the Convention on the Rights of the Child, the United States has an obligation to utilize legislative avenues to promote child health, safety, and well-being.
Acknowledgments
We wish to thank our ECHO colleagues; the medical, nursing, and program staff; and the children and families participating in the ECHO Cohort. We also acknowledge Diana Steele Jones at the Duke Clinical Research Institute for editorial assistance. Jones did not receive compensation for her contributions, apart from her employment at the institute. She has provided permission to be acknowledged for her contribution.
Funding
Research reported in this publication was supported by the Environmental influences on Child Health Outcomes Program, Office of the Director, National Institutes of Health, under award numbers U2COD023375 (Coordinating Center), U24OD023382 (Data Analysis Center), U24OD023319 with co-funding from the Office of Behavioral and Social Science Research (Measurement Core), U24OD035523 (Lab Core), ES0266542 (HHEAR), U24ES026539 (HHEAR Barbara O’Brien), U2CES026533 (HHEAR Lisa Peterson), U2CES026542 (HHEAR Patrick Parsons, Kannan Kurunthacalam), U2CES030859 (HHEAR Manish Arora), U2CES030857 (HHEAR Timothy R. Fennell, Susan J. Sumner, Xiuxia Du), U2CES026555 (HHEAR Susan L. Teitelbaum), U2CES026561 (HHEAR Robert O. Wright), U2CES030851 (HHEAR Heather M. Stapleton, P. Lee Ferguson), UG3/UH3OD023251 (Akram Alshawabkeh), UH3OD023320 and UG3OD035546 (Judy Aschner), UH3OD023332 (Clancy Blair, Leonardo Trasande), UG3/UH3OD023253 (Carlos Camargo), UG3/UH3OD023248 and UG3OD035526 (Dana Dabelea), UG3/UH3OD023313 (Daphne Koinis Mitchell), UH3OD023328 (Cristiane Duarte), UH3OD023318 (Anne Dunlop), UG3/UH3OD023279 (Amy Elliott), UG3/UH3OD023289 (Assiamira Ferrara), UG3/UH3OD023282 (James Gern), UH3OD023287 (Carrie Breton), UG3/UH3OD023365 (Irva Hertz-Picciotto), UG3/UH3OD023244 (Alison Hipwell), UG3/UH3OD023275 (Margaret Karagas), UH3OD023271 and UG3OD035528 (Catherine Karr), UH3OD023347 (Barry Lester), UG3/UH3OD023389 (Leslie Leve), UG3/UH3 D035519 (Kaja LeWinn), UG3/UH3OD023344 (Debra MacKenzie), UH3OD023268 (Scott Weiss), UG3/UH3OD023288 (Cynthia McEvoy), UG3/UH3OD023342 (Kristen Lyall), UG3/UH3OD023349 (Thomas O’Connor), UH3OD023286 and UG3OD035533 (Emily Oken), UG3/UH3OD023348 (Mike O’Shea), UG3/UH3OD023285 (Jean Kerver), UG3/UH3OD023290 (Julie Herbstman), UG3/UH3OD023272 (Susan Schantz), UG3/UH3OD023249 (Joseph Stanford), UG3/UH3OD023305 (Leonardo Trasande), UG3/UH3OD023337 (Rosalind Wright), UG3OD035508 (Sheela Sathyanarayana), UG3OD035509 (Anne Marie Singh), UG3OD035513 and UG3OD035532 (Annemarie Stroustrup), UG3OD035516 and UG3OD035517 (Tina Hartert), UG3OD035518 (Jennifer Straughen), UG3OD035519 (Qi Zhao), UG3OD035521 (Katherine Rivera-Spoljaric), UG3OD035527 (Emily S. Barrett), UG3OD035540 (Monique Marie Hedderson), UG3OD035543 (Kelly J. Hunt), UG3OD035537 (Sunni L. Mumford), UG3OD035529 (Hong-Ngoc Nguyen), UG3OD035542 (Hudson Santos), UG3OD035550 (Rebecca Schmidt), UG3OD035536 (Jonathan Slaughter), and UG3OD035544 (Kristina Whitworth).
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Role of funder
The sponsor, the National Institutes of Health, participated in the overall design and implementation of the ECHO Program, which was funded as a cooperative agreement between the National Institutes of Health and grant awardees. The sponsor approved the ECHO protocol developed by the Steering Committee, as well as its amendments, including COVID-19 measures. The sponsor had no access to the central database, which was housed at the ECHO Data Analysis Center. Data management and site monitoring were performed by the ECHO Data Analysis Center and Coordinating Center. All analyses for scientific publication were performed by the study statistician, independently of the sponsor. The lead author wrote all drafts of the manuscript and made revisions based on feedback from the coauthors and the ECHO Publication Committee (a subcommittee of the ECHO Operations Committee), without input from the sponsor. The study sponsor did not review or approve the manuscript for submission to this journal.
Data availability statement
Select de-identified data from the ECHO Program are available through the NICHD Data and Specimen Hub (https://dash.nichd.nih.gov/). Information on study data not available on DASH, such as some Indigenous datasets, can be found on the ECHO study DASH web page (https://dash.nichd.nih.gov/explore/study?type=study&search=echo).
Ethics approval
The ECHO Institutional Review Board or corresponding local institutional review board approved the study procedures, and written informed consent for participation was obtained. The research was performed in accordance with the Declaration of Helsinki.
Marie L. Churchill, MS, is a senior biostatistician at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Emily A. Knapp, PhD, is an associate scientist at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Alexander D. McCourt, JD, PhD, MPH, is an assistant professor at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Nandita Somayaji, MHS, Med, is a senior research data analyst at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Courtney K. Blackwell, PhD, is an associate professor in the Department of Medical Social Sciences, Northwestern University Feinberg School of Medicine, Chicago, United States.
Lyndsay A. Avalos, PhD, MPH, is a research scientist at Kaiser Permanente Northern California, Division of Research, Oakland, United States.
Kelly A. Hirko, PhD, MPH, is an associate professor in the Department of Epidemiology and Biostatistics, College of Human Medicine, Michigan State University, East Lansing, United States.
Kaja Z. LeWinn, ScD, is a professor in the Department of Psychiatry and Behavioral Science, Child and Adolescent Division, University of California, San Francisco, United States.
Johnnye Lewis, PhD, is the professor emerita and co-director of the Community Environmental Health Program, College of Pharmacy, University of New Mexico Health Sciences Center, Albuquerque, United States.
Yeyi Zhu, PhD, is a research scientist at Kaiser Permanente Northern California, Division of Research, Oakland, United States.
Alison E. Hipwell, PhD, ClinPsyD, is a professor in the Department of Psychiatry, Psychology and Clinical and Translational Science, University of Pittsburgh, United States.
Margaret R. Karagas, PhD, is a chair and professor in the Department of Epidemiology at the Geisel School of Medicine at Dartmouth, Hanover, United States.
Kristen Lyall, ScD, is an associate professor in the Department of Epidemiology and Biostatistics, Drexel University, and AJ Drexel Autism Institute, Philadelphia, United States.
Jody M. Ganiban, PhD, is a professor in the Department of Psychological and Brain Sciences, George Washington University, Washington, DC, United States.
Nigel Paneth, MD, MPH, is a professor in the Department of Epidemiology and Biostatistics and the Department of Pediatrics and Human Development, College of Human Medicine, Michigan State University, East Lansing, United States.
T. Michael O’Shea, MPH, is a professor in the Department of Pediatrics, University of North Carolina at Chapel Hill, United States.
Christine C. Johnson, PhD, MPH, is a chair in the Department of Public Health Sciences and director of the Henry Ford Health Center for Allergy, Asthma and Immunology Research at Henry Ford Health, Detroit, United States.
Carlos A. Camargo, Jr., MD, DrPH, is the Conn Chair in Emergency Medicine at the Massachusetts General Hospital and a professor at Harvard Medical School, Boston, United States.
Cassandra K. Crifasi, PhD, MPH, is an associate professor at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Aruna Chandran, MD, MPH, is a professor at Johns Hopkins Bloomberg School of Public Health, Baltimore, United States.
Please address correspondence to Emily A. Knapp, Email: eknapp2@jhu.edu.
Competing interests: None declared.
Copyright © 2026 Churchill, Knapp, McCourt, et al. This is an open access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] World Population Review, “Gun Ownership by Country 2025,” https://worldpopulationreview.com/country-rankings/gun-ownership-by-country; National Center for Health Statistics, “National Vital Statistics System, Mortality 2018–2023,” Centers for Disease Control and Prevention, http://wonder.cdc.gov/ucd-icd10-expanded.html; S. Conroy, “Firearms and Violent Crime in Canada, 2023,” Statistics Canada, https://www150.statcan.gc.ca/n1/daily-quotidien/250225/dq250225a-eng.htm.
[2] M. Miller, W. Zhang, and D. Azrael, “Firearm Purchasing During the COVID-19 Pandemic: Results from the 2021 National Firearms Survey,” Annals of Internal Medicine 175/2 (2022).
[3] S. Villarreal, R. Kim, E. Wagner, et al., Gun Violence in the United States 2022: Examining the Burden Among Children and Teens (Center for Gun Violence Solutions, Johns Hopkins Bloomberg School of Public Health, 2024); R. Kim, E. Wagner, P. Nestadt, et al., Gun Violence in the United States 2023: Examining the Gun Suicide Epidemic (Center for Gun Violence Solutions and Center for Suicide Prevention, Johns Hopkins Bloomberg School of Public Health, 2025) .
[4] D. C. Semenza, R. Stansfield, I. A. Silver, and B. Savage, “Reciprocal Neighborhood Dynamics in Gun Violence Exposure, Community Health, and Concentrated Disadvantage in One Hundred US Cities,” Journal of Urban Health 100/6 (2023); K. J. Mitchell, V. Banyard, B. G. Taylor, et al., “Prevalence of Exposure to Someone Else’s Firearm Violence, Threats, and Risky Behavior Among a National Sample of Young People in the United States,” Frontiers in Public Health 13 (2025).
[5] C. R. Harper, J. Li, K. Sheats, M. F. Hertz, et al., “Witnessing Community Violence, Gun Carrying, and Associations with Substance Use and Suicide Risk Among High School Students—Youth Risk Behavior Survey, United States, 2021,“ Morbidity and Mortality Weekly Report 72/1 (2023); H. A. Turner, K. J. Mitchell, L. M. Jones, et al., “Gun Violence Exposure and Posttraumatic Symptoms Among Children and Youth,“ Journal of Traumatic Stress 32/6 (2019); A. Vasan, H. K. Mitchell, J. A. Fein, et al., “Association of Neighborhood Gun Violence with Mental Health-Related Pediatric Emergency Department Utilization,“ JAMA Pediatrics 175/12 (2021).
[6] Harper et al. (see note 5).
[7] N. Somayaji, E. A. Knapp, M. L. Churchill, et al., “Associations Between Neighborhood-Level Gun Violence and Child General Health Status: An ECHO Cohort Analysis,” Injury 56/11 (2025).
[8] Center for Gun Violence Solutions, Johns Hopkins Bloomberg School of Public Health, “Questions and Answers: Public Carry of Firearms, Permitless Carry and Stand Your Ground Laws” (March 18, 2025), https://publichealth.jhu.edu/center-for-gun-violence-solutions/2025/questions-and-answers-public-carry-of-firearms-permitless-carry-and-stand-your-ground-laws.
[9] M. L. Doucette, C. Crifasi, A. D. McCourt, et al., “Deregulation of Public Civilian Gun Carrying and Violent Crimes: A Longitudinal Analysis 1981–2019,” Criminology and Public Policy 23/4 (2024).
[10] Ibid.
[11] E. W. Lundstrom, J. K. Pence, and G. S. Smith, “Impact of a Permitless Concealed Firearm Carry Law in West Virginia, 1999–2015 and 2016–2020,” American Journal of Public Health 113/11 (2023).
[12] P. Sharkey and M. Kang, “The Era of Progress on Gun Mortality: State Gun Regulations and Gun Deaths from 1991 to 2016,” Epidemiology 34/6 (2023).
[13] Everytown Research & Policy, “Permitless Carry: Carrying a Concealed Gun in Public with No Permit and No Training,” Everytown for Gun Safety Support Fund (February 20, 2020), https://everytownresearch.org/report/permitless-carry-carrying-a-concealed-gun-in-public-with-no-permit-and-no-training/.
[14] B. G. Taylor, K. J. Mitchell, H. A. Turner, et al., “Prevalence of Gun Carrying and Gun Violence Victimization and Perpetration Among a Nationally Representative Sample of U.S. Youth and Young Adults,” AJPM Focus 4/1 (2025).
[15] Turner et al. (see note 5); Vasan et al. (see note 5).
[16] Turner et al. (see note 5); D. Bergen-Cico, S. D. Lane, R. H. Keefe, et al., “Community Gun Violence as a Social Determinant of Elementary School Achievement,” Social Work in Public Health 33/7–8 (2018).
[17] A. Bruns, A. J. Aubel, X. Zhang, et al., “Community Exposure to Gun Homicide and Adolescents’ Educational Aspirations,” Journal of Adolescence 96/5 (2024).
[18] C. Leibbrand, H. Hill, A. Rowhani-Rahbar, and F. Rivara, “Invisible Wounds: Community Exposure to Gun Homicides and Adolescents’ Mental Health and Behavioral Outcomes,” SSM – Population Health 12 (2020); A. M. Gard, J. Brooks-Gunn, S. S. McLanahan, et al., “Deadly Gun Violence, Neighborhood Collective Efficacy, and Adolescent Neurobehavioral Outcomes,” PNAS Nexus 1/3 (2022); X. Zhang, A. J. Aubel, A. Bruns, et al., “Heterogeneous Effects of Environmental Exposure to Gun Violence on Adolescent Problem Behavior,” Journal of Interpersonal Violence 41/9–10 (2025).
[19] Human Rights Council, Human Rights and the Regulation of Civilian Acquisition, Possession and Use of Firearms, UN Doc. A/HRC/32/21 (2016).
[20] “Gun Violence in the USA: Children’s Right to Health,” Lancet 399/10341 (2022).
[21] E. A. Knapp, A. M. Kress, C. B. Parker, et al., “The Environmental Influences on Child Health Outcomes (ECHO)-Wide Cohort,” American Journal of Epidemiology 192/8 (2023).
[22] R. D. Hays, J. B. Bjorner, D. A. Revicki, et al., “Development of Physical and Mental Health Summary Scores from the Patient-Reported Outcomes Measurement Information System (PROMIS) Global Items,” Quality of Life Research 18/7 (2009); C. B. Forrest, C. A. Tucker, U. Ravens-Sieberer, et al., “Concurrent Validity of the PROMIS Pediatric Global Health Measure,” Quality of Life Research 25/3 (2016); C. B. Forrest, K. B. Bevans, R. Pratiwadi, et al., “Development of the PROMIS Pediatric Global Health (PGH-7) Measure,” Quality of Life Research 23/4 (2014).
[23] Doucette et al. (see note 9); Center for Gun Violence Solutions, Johns Hopkins Bloomberg School of Public Health, “Regulation of Public Carry,” https://publichealth.jhu.edu/sites/default/files/2025-04/regulation-of-public-carry-factsheet.pdf.
[24] Doucette et al. (see note 9).
[25] Hays et al. (2009, see note 22); Forrest et al. (2016, see note 22); Forrest et al. (2014, see note 22).
[26] R. D. Hays, K. L. Spritzer, W. W. Thompson, and D. Cella, “U.S. General Population Estimate for ‘Excellent’ to ‘Poor’ Self-Rated Health Item,” Journal of General Internal Medicine 30/10 (2015).
[27] T. M. Achenbach and L.A. Rescorla, Manual for the ASEBA School-Age Forms and Profiles: Child Behavior Checklist for Ages 6–18, Teacher’s Report Form, Youth Self-Report: An Integrated System of Multi-Informant Assessment (Achenbach System of Empirically Based Assessment, 2001); T. M. Achenbach and L.A. Rescorla. Manual for the ASEBA Preschool Forms and Profiles: An Integrated System of Multi-Informant Assessment; Child Behavior Checklist for Ages 1 1/2–5; Language Development Survey; Caregiver-Teacher Report Form (Achenbach System of Empirically Based Assessment, 2000).
[28] K. B. Bevans, W. Gardner, K. Pajer, et al., “Qualitative Development of the PROMIS Pediatric Stress Response Item Banks,” Journal of Pediatric Psychology 38/2 (2013); K. B. Bevans, W. Gardner, K. A. Pajer, et al., “Psychometric Evaluation of the PROMIS Pediatric Psychological and Physical Stress Experiences Measures,” Journal of Pediatric Psychology 43/6 (2018).
[29] US Department of Agriculture Economic Research Service, “2020 Rural-Urban Commuting Area Codes,” https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes; US Centers for Disease Control and Prevention, “CDC/ATSDR Social Vulnerability Index (CDC/ATSDR SVI),” https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/.
[30] T. L. Schell, S. Peterson, B. G. Vegetabile, et al., “State-Level Estimates of Household Firearm Ownership,” RAND Corporation (April 22, 2020), https://www.rand.org/pubs/tools/TL354.html; S. Markowitz, K. A. Komro, M. D. Livingston, et al., “Effects of State-Level Earned Income Tax Credit Laws in the U.S. on Maternal Health Behaviors and Infant Health Outcomes,” Social Science and Medicine 194 (2017); Institute on Taxation and Economic Policy, “When Did Your State Enact an Earned Income Tax Credit (EITC)?” (April 2, 2025), https://itep.org/when-did-your-state-enact-an-earned-income-tax-credit-eitc/; US Census Bureau, “American Community Survey (ACS),” https://www.census.gov/programs-surveys/acs/news/data-releases.html.
[31] S. van Buuren and K. Groothuis-Oudshoorn, “Mice: Multivariate Imputation by Chained Equations in R,” Journal of Statistical Software 45 (2011).
[32] Somayaji et al. (see note 7); Sharkey and Kang (see note 12).
[33] Somayaji et al. (see note 7).
[34] C. B. Terwee, J. D. Peipert, R. Chapman, et al., “Minimal Important Change (MIC): A Conceptual Clarification and Systematic Review of MIC Estimates of PROMIS Measures,” Quality of Life Research 30/10 (2021).
[35] World Population Review, “Gun Ownership by Country 2026,” https://worldpopulationreview.com/country-rankings/gun-ownership-by-country.
[36] Miller et al. (see note 2).
[37] Bureau of Alcohol, Tobacco, Firearms and Explosives, “Data and Statistics,” https://www.atf.gov/resource-center/data-statistics.
[38] PEW Research Center, “For Most U.S. Gun Owners, Protection Is the Main Reason They Own a Gun” (August 16, 2023), https://www.pewresearch.org/politics/2023/08/16/for-most-u-s-gun-owners-protection-is-the-main-reason-they-own-a-gun/; A. Rowhani-Rahbar, A. Gallagher, D. Azrael, and M. Miller. “Trend in Loaded Handgun Carrying Among Adult Handgun Owners in the United States, 2015‒2019,” American Journal of Public Health 112/12 (2022); D. Azrael, L. Hepburn, D. Hemenway, and M. Miller, “The Stock and Flow of U.S. Firearms: Results from the 2015 National Firearms Survey,” RSF: The Russell Sage Foundation Journal of the Social Sciences 3/5 (2017).
[39] Villareal et al. (see note 3); Kim et al. (see note 3).
[40] Villareal et al. (see note 3); Kim et al. (see note 3).
[41] S. C. Curtin and M. F. Garnett, “Suicide and Homicide Death Rates Among Youth and Young Adults Aged 10–24: United States, 2001–2021,” National Center for Health Statistics Data Brief 471 (2023).
[42] Kim et al. (see note 3).
[43] Doucette et al. (see note 9); Center for Gun Violence Solutions, “Regulation of Public Carry” (see note 23).
[44] Vasan et al. (see note 5); Turner et al. (see note 5); Harper et al. (see note 5); Bergen-Cico et al. (see note 16); Bruns et al. (see note 17).
[45] Human Rights Council (see note 19); E. Barnert, J. Wright, C. Choi, et al., “Reimagining Children’s Rights in the US,” JAMA Pediatrics 176/12 (2022); M. Yost, K. Fernandez, E. Nelson, et al., “Gun Violence Against Children in the U.S.,” Human Rights Quarterly 46/4 (2024).
[46] R. B. Siegel and J. Blocher, “Why Regulate Guns,” Journal of Law, Medicine and Ethics 48/4 (2021).
[47] Convention on the Rights of the Child, G.A. Res. 44/25 (1989).
[48] Ibid.
[49] Kim et al. (see note 3).
[50] Somayaji et al. (see note 7).
[51] S. Zheng, M. Mansolf, M. McGrath, et al., “Measurement Bias in Caregiver-Report of Early Childhood Behavior Problems Across Demographic Factors in an ECHO-Wide Diverse Sample,” JCPP Advances 4/1 (2023).
[52] Human Rights Council (see note 19).