Political Contestation of the Right to Health in the United States: Eighty Years of Conservative Opposition to Health and Human Rights
Vol 28/1, 2026, pp. 179-197 PDF
Benjamin Mason Meier and Darby McBride
Abstract
The United States stands apart from other nations in opposing the right to health under international law, with longstanding conservative opposition to a human right to health holding back policy efforts to realize health care and underlying determinants of health—at home and throughout the world. Over the past 80 years, American conservative ideology has presented persistent political obstacles to the advancement of health as a human right, challenging who is entitled to rights and what those rights entail. This ideological opposition has reframed health as a narrow privilege for some rather than an expansive right for all. Examining the historical evolution of the right to health since the end of World War II, this paper analyzes how shifting conservative opposition over the years has undermined human rights in health policy and culminated in existential challenges for health systems. The paper concludes that the guarantee of health as a human right must be codified as a defining principle of American democracy, enshrining constitutive commitments to health as a foundation for a healthier future under law.
Introduction
The advancement of health as a human right has long been challenged in the United States by conservative ideologies, which have sought to limit the right to health in domestic policy and global governance. While the justifications for this opposition have shifted over time and across political parties—alternatively grounded in individualism, neoliberalism, and nationalism—US conservative opposition has persisted through the years, presenting recurring obstacles to the development and implementation of the right to health. This enduring ideological opposition to the right to health in US policy has expanded in scope and impact with the rise of right-wing populist nationalism, as the US government is now taking rapid steps to limit health and human rights in domestic and global health policy, presenting an existential challenge to the foundational notion of health as a human right. To understand these current retrogressive measures, it is imperative to examine historical American opposition to the right to health, with past failures to progressively realize human rights in health policy offering lessons to shape future advocacy to ensure health as a human right.
The right to health encompasses interconnected freedoms and entitlements that support the realization of health care and underlying determinants of health. These government responsibilities for health have come to be codified under international law, shifting the public health debate from political aspiration to binding obligation. Through the evolving development of the right to health under international law, the US government has worked with other states under the United Nations (UN) to establish a common global vision for public health. Yet, in stark contrast to the progressive trajectory of other high-income nations, this US advancement of the right to health has faced continuing conservative opposition over who is entitled to rights and what rights should be upheld by the state—with this opposition framing health as a privilege of wealth rather than a fundamental right for all. Such ideological opposition has repeatedly limited health advancements in US policy, reflecting an American interpretation of human rights that has constrained the notion of health as a universal human right and an essential government responsibility. This selective US conceptualization of rights holders and state obligations in health has shaped conservative opposition over the past 80 years, with past obstacles to the right to health now presenting new challenges for the US public health system, in foreign health assistance, and through global health governance.
This paper analyzes the long evolution of the right to health in US policy, examining the persistent opposition of American conservative ideology that has laid the foundation for the current US abandonment of human rights in domestic and global health policy. Beginning in the aftermath of World War II, the first section frames early US efforts to establish human rights and public health as central to a new international order. However, in contrast with the health policy trajectory in other high-income nations, this postwar vision for health and human rights faced early challenges from American conservatives, with the second section detailing this opposition amid Cold War tensions. The third section examines the increasing politicization of health in the United States, beginning in the 1980s amid a surge of Republican Party support for neoliberal economic policies and conservative religious ideologies and giving rise to new Republican attacks on Democratic health initiatives and global health governance. The 21st century reshaped this Republican attack on the right to health, with the fourth section investigating how the securitization of health amid the US “War on Terror” reframed global health engagement as either a security imperative or religious charity.
Despite an unprecedented expansion of domestic health care access under the 2010 Affordable Care Act, this Democratic effort to progressively realize access to health coverage reignited sweeping Republican attacks on health policy, leading into the 2016 election of President Trump. The fifth section traces the populist policies of the first Trump administration, considering the lasting implications of the US rejection of the right to health amid the COVID-19 response. Despite subsequent efforts to address determinants of health under the Biden administration, President Trump would return to office following the 2024 election, with this right-wing populist governance now threatening public health science, human rights protections, and global health institutions. These ongoing populist attacks on health and human rights, a culmination of past conservative opposition, will outlast this administration. In responding to these longstanding political obstacles to the right to health, threatening universal rights and health entitlements, this paper concludes that ideological constraints on the right to health will endure in US conservativism until health is reconceptualized under US law as a fundamental human right and a central foundation of American democracy.
Roosevelt’s dream of health for all as a human right
The initial conceptualization of a right to health under international law arose in the context of World War II, as the United States positioned itself in the allied fight against tyrannical governments as a beacon for the advancement of individual freedoms, international institutions, and health protections.[1] However, postwar efforts to codify health and human rights were stymied by conservative attacks on health-related human rights and opposition to universal health care systems.
From “four freedoms” to human rights
Even before the United States entered World War II, US President Franklin Delano Roosevelt proclaimed to the world in January 1941 that the postwar era would be founded on four “essential human freedoms”: freedom of speech, freedom of religion, freedom from fear, and freedom from want.[2] The last of these “Four Freedoms”—freedom from want—heralded a state obligation to provide for the health of its peoples. As the Great Depression and ensuing World War transformed the United States, Roosevelt cited this “freedom from want” as central to a “Second Bill of Rights,” looking to uphold economic and social rights as central to a “New Deal” under US law, with the understanding that “a necessitous man is not a free man.”[3] Roosevelt intended this Second Bill of Rights to serve as a constitutive commitment—rather than a constitutional amendment—embedding new responsibilities into American institutions and values.[4] While proclaiming such values as universal, extending across all nations, Roosevelt sought to ensure these rights in the United States, calling on Congress in his 1944 State of the Union address to enshrine “the right to adequate medical care and the opportunity to achieve and enjoy good health.”[5] Drawing from this conceptualization of social and economic guarantees, the United States worked with allied nations to establish human rights as a foundation of global governance.[6]
Developing human rights to advance health
The Charter of the United Nations—signed by nations in June 1945, just after the passing of President Roosevelt—would be the first international treaty to codify human rights, with human rights serving as one of the central pillars of UN governance.[7] Framing health among these human rights, states sought to develop a specialized health agency under the UN. The United States would host the final International Health Conference to establish this new UN health agency, with US President Harry Truman echoing Roosevelt and imploring representatives in his opening message to see health as a right:
The right to adequate medical care and the opportunity to achieve and enjoy good health should be available to all people. For this objective I can assure you is in the interest and the support of the United States.[8]
Through the unprecedented declaration that “the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being,” the July 1946 Constitution of the World Health Organization established the mandate of the World Health Organization (WHO) as the “directing and coordinating authority on international health work.”[9] The founding states of WHO envisioned an expansive role for human rights in realizing “a state of complete physical, mental and social well-being and not merely the absence of disease of infirmity.”[10]
In advancing these rights through the UN, former US First Lady Eleanor Roosevelt was instrumental in shaping the postwar human rights framework through the 1948 Universal Declaration of Human Rights (UDHR). Following the death of her husband, President Truman appointed Eleanor Roosevelt as a delegate to the newly established UN, where she was elected chair of the Human Rights Commission in 1946—and came to be known as the “First Lady of the World.”[11] Roosevelt led delegates in developing the UDHR, which framed a human right to “a standard of living” adequate for health, encompassing both a right to medical care and underlying determinants of health.[12]
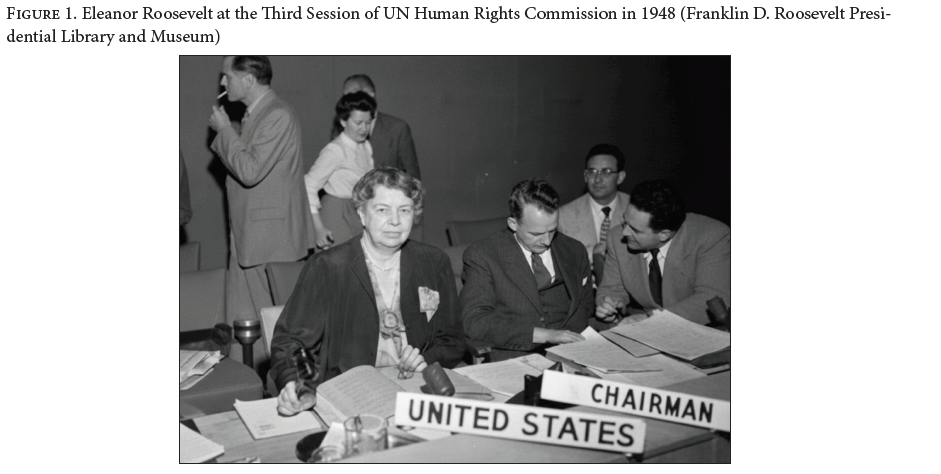
However, Roosevelt’s rights-based vision was not embraced throughout the US government.[13] Conservative politicians across political parties opposed efforts to expand international human rights law beyond civil and political rights, as the comprehensive vision of rights in the UDHR was seen as a threat to US institutions of racial segregation and a ploy for the international advancement of communist ideals.[14] These conservative critics attacked Roosevelt as a “menace to liberty” and an “un-American communist,” and the electoral impact of these attacks shifted US policies in ways that limited the realization of the right to health.[15]
Abandoning universal health care
Even as President Truman became the first US president to propose a comprehensive national health plan—outlining in 1945 a five-point program to advance medical education, health insurance, and public health services—this effort to realize universal health care for all Americans was abandoned amid rising conservative opposition. Nations across the Western world were rapidly rebuilding from the destruction of World War II through the development of national health systems, as seen in the British establishment of the National Health Service to provide free care to all “ordinarily residents” (British citizens and permanent residents, with specific provisions for visitors, refugees, and asylum seekers).[16] However, without US congressional support for universal guarantees of health, the United States instead pursued incremental efforts to expand segregated health care systems through the 1946 Hospital Survey and Construction Act, funding hospitals in underserved communities in exchange for the provision of free emergency care.[17] With the US Congress shifting to Republican control in the 1946 midterm elections, breaking up the “New Deal coalition” that sought to protect social security for the working classes over the previous decade, the United States abandoned comprehensive health insurance efforts similar to those of postwar European nations.[18] This solidifying conservative opposition to universal health care found support from medical practitioners in the American Medical Association, which feared a loss of physician profits under “fee-for-service” care.[19]
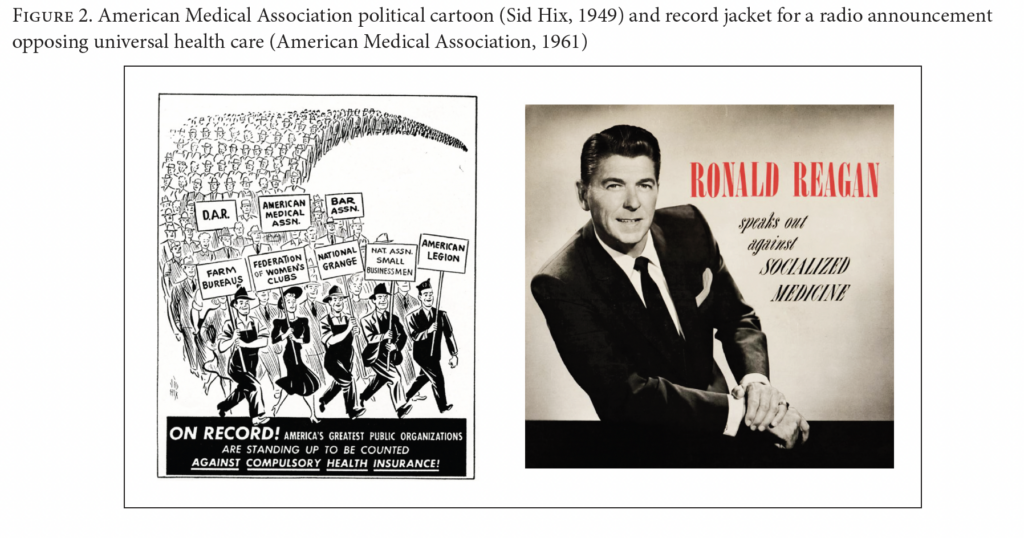
The American Medical Association developed nationwide campaigns against universal health care, equating health insurance subsidies and government health insurance with “socialized medicine.” This coordinated conservative opposition undermined health reform efforts and challenged the right to health at home and abroad.[20]
Conservative opposition to “socialized medicine”
Attacks against “socialized medicine” became a hallmark of US health policy. Undercutting the UDHR’s promise of universal human rights, the international development of health-related rights would be challenged by Cold War divisions between Western capitalist democracies and Soviet communist regimes, with the US government looking to prevent the rise of “health rights” as a basis to contain the spread of communism.[21] Following the 1952 election of Republican President Dwight D. Eisenhower, the United States withdrew from the development of international human rights treaties, abandoning UN cooperation to codify international standards in order to prioritize ideological conflict amid the Cold War.[22] These Cold War divisions impacted both the conceptualization of the right to health under international law and the implementation of human rights in US health policy.[23]
Cold War politics
Soviet criticism of US health inequalities fueled conservative challenges to the very idea of health as a universal entitlement to be progressively realized through government action. Questioning whether health was a genuine human right or merely a political aspiration, the United States pushed for the codification of international legal obligations only for civil and political rights, individual freedoms from government intrusion that were long protected by the US Constitution.[24] This US rejection of health-related rights contributed to the temporary withdrawal of Soviet states from WHO, with the Soviet Union arguing in February 1949 that its withdrawal was forced by WHO’s lack of focus on the underlying economic and social determinants of health.[25] Without Soviet engagement, international efforts to address social determinants of health would have no voice in World Health Assembly debates, shifting WHO toward disease eradication initiatives and limiting efforts to examine public health under a rights-based framework.[26]
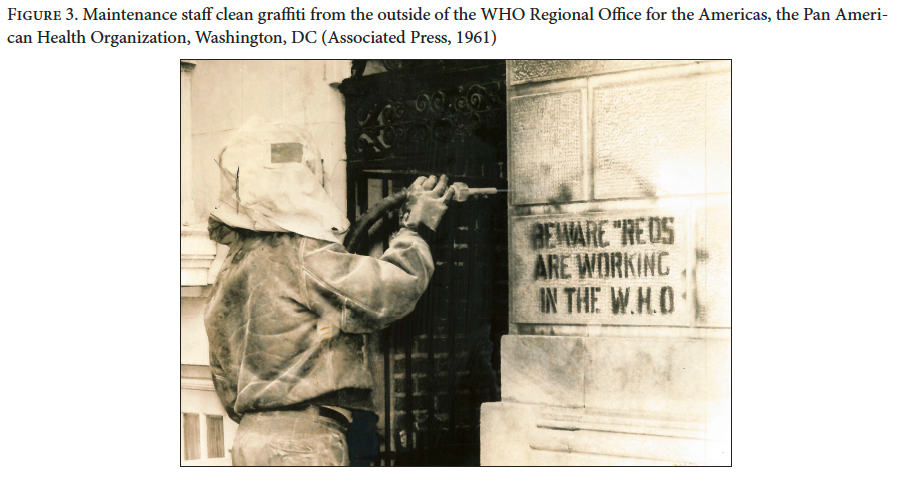
Even as Soviet states returned to WHO, the United States sought to contain the influence of communist (so-called “red”) health initiatives—through both bilateral assistance to advance public health and multilateral influence to limit the right to health. With the United States pursuing bilateral health assistance to undermine the influence of “communist health initiatives,” Democratic President John F. Kennedy’s establishment of the United States Agency for International Development (USAID) in 1961 galvanized US foreign assistance for public health in low-income nations.[27] However, the rise of USAID was met by conservative opposition, as conservatives in Congress rapidly called for a “retrenchment in aid,” framing USAID as a waste of taxpayer resources to “placate ungrateful nations.”[28] Facing political opposition at home to advancing health abroad, the United States pushed WHO to abandon UN negotiations to codify the right to health under international law. Such US opposition to expansive Soviet proposals resulted in a constrained individual right to the “highest attainable standard of health” under the 1966 International Covenant on Economic, Social and Cultural Rights.[29] Challenged by US political pressure, WHO’s repeated proclamations of the “non-political” nature of public health and its attempts to avoid political debates on human rights limited multilateral efforts to achieve universal health care throughout the world.[30]
Opposition to universal health care
By the mid-1960s, worldwide attention was again focused on health inequalities as a violation of human rights. The fight for human rights in the United States became intertwined with the struggle for racial equality, with Black Americans systematically denied a wide range of rights, including social and economic rights to education, housing, and health.[31] Seeking to address rising inequities through health care reforms, Democratic Presidents Kennedy and then Lyndon B. Johnson made universal health care a political priority in US policy.[32] Conservative members of Congress, however, sought to limit these universal care initiatives, condemning efforts to establish a “welfare state” as the first step in the spread of communism to all aspects of life and reducing the health policy debate from public health to medical coverage.[33] This opposition, often couched in implicitly racist terms, led President Johnson to abandon universal health care reforms and focus instead on narrower health programs for specific vulnerable populations, with interconnected 1965 legislation providing for the rights of the elderly through Medicare and the rights of the impoverished through Medicaid.[34] The American Medical Association supported this proposed government medical assistance for the elderly but actively opposed any expansion of assistance to other populations, framing efforts to ensure health care for all as compromising the control of physicians and insurance companies in setting fees.[35] While the final creation of Medicaid provided federal funding to state governments to facilitate medical coverage for impoverished Americans, compromises in congressional negotiations resulted in inadequate financing for care and state discretion on coverage, allowing health inequities and racial discrimination to persist.[36]
These divisive conservative attacks on health equity initiatives, pushing Southern white voters toward the Republican Party and leading to the narrow 1968 election of Republican President Richard Nixon, would frustrate efforts to expand welfare guarantees under the US Constitution, as US health care reform debates shifted toward the expansion of private health insurance.[37] As domestic health policy became stymied by partisan divisions, these conservative attacks extended globally, with American conservatives turning against international health policy developments under WHO governance.[38]
A “new international health order”
Following the election of a new WHO Director-General in 1973, the WHO Secretariat looked to human rights to advance public health for impoverished populations throughout the world. WHO sought to navigate tensions between the Cold War superpowers while also addressing the concerns of “developing countries,” as these long marginalized states came together to restructure international development cooperation in the pursuit of a “new international economic order.”[39] With these developing countries voting together in the World Health Assembly to advance health as a universal human right, the WHO leadership held out human rights as central to a political campaign for public health, extolling international legal obligations as a clarion call for the realization of primary health care. This renewed rights-based vision for health would shape WHO’s 1978 International Conference on Primary Health Care, in Alma-Ata, USSR. Drawing from the united advocacy of low- and middle-income countries, the resulting Declaration of Alma-Ata detailed a multisectoral imperative to address underlying determinants of public health, delineating government obligations to promote health as a human right.[40]
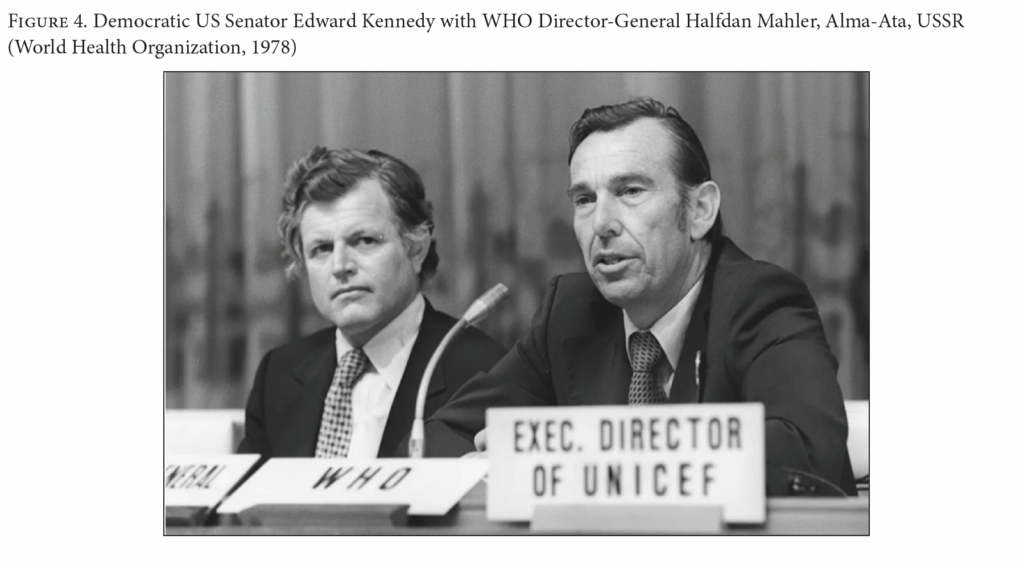
WHO leaders saw this moment as the “onset of the health revolution,” with scholars examining the Declaration of Alma-Ata as heralding a “new international health order.”[41] This new order for international health found early support in a renewed US commitment to human rights and global governance, with Democratic President Jimmy Carter inaugurating his presidency in 1977 under the commitment to “guarantee the basic right of every human being to be free from poverty and hunger and disease and political oppression.”[42] While the Carter administration continued to advance the right to health under WHO, amid broader US support for economic and social rights in the late 1970s, the 1980 election of Republican President Ronald Reagan—and with it, renewed conservative opposition to WHO’s regulatory activities—closed any opportunity to implement the Declaration of Alma-Ata and realize primary health care throughout the world.[43]
Republican attacks against public health and “global” health
The Reagan administration saw the ascendance of the “New Right” in the Republican Party, which brought together two opposing ideological tenets of conservatism: “neoliberalism,” an economic conservatism that sought freedom from government intervention, and “moralism,” a social conservatism that advanced government authority to further traditional moral and social values.[44] These contradictory conservative ideals led to inconsistencies across health policy, as US policies simultaneously liberalized the market for privatized health services and imposed right-wing religious ideologies to attack sexual and reproductive rights and LGBTQ+ populations.
Challenging WHO governance and US welfare policy
As health care became increasingly privatized under the neoliberal economic model—prioritizing free market liberalization with minimal government intervention—the Reagan administration presented new obstacles to health, treating health services as a transactional commodity rather than a fundamental right. This economic model for health, advanced forcefully by the Heritage Foundation, a conservative nongovernmental think-tank, was integrated across the US health system, as corporations gained greater control over health determinants and the government stepped back from public health, disregarding structural barriers to health for marginalized populations.[45] Although these policy shifts purported to promote economic efficiency, the subordination of human rights to market forces served to undermine primary health care, developing-nation health systems, and WHO governance.[46]
Impacting health throughout the world, the Reagan administration first pushed back against WHO regulation of commercial determinants of health, with the United States standing alone in opposition to the 1981 WHO International Code of Marketing of Breastmilk Substitutes, which aimed to regulate transnational formula corporations in order to prevent infant death.[47] Thereafter cutting back US financial support for WHO, the Reagan administration threatened the stability of WHO financing, criticizing the organization for its alleged limitation of free markets and shifting US financial commitments away from general budget support and toward targeted funding for US priorities.[48]
In applying this neoliberal model to the US health system, the “Reagan Revolution” sought the privatization and decentralization of government health programs: the US Department of Health and Human Services faced large budget cuts, the federal government provided grants directly to states for health programming, and Medicare and Medicaid eligibility were sharply reduced.[49] These neoliberal cost-cutting measures shrank the federal government’s share of the nation’s health budget, cutting Medicaid by more than 10% and welfare spending by more than 17%, at the expense of rights-based conceptions of health, with the government singling out specific groups as “unworthy” of health entitlements.[50] The Reagan administration often justified these cuts to the “welfare state” in racialized terms, repeatedly demonizing impoverished Black women as “welfare queens” who were seeking to abuse the welfare system and take from “hardworking Americans.”[51] Framing poverty as a personal moral failure rather than a foundational government responsibility, the administration narrowed the definition of health to focus only on medical care, increased barriers for impoverished Americans, and disregarded underlying determinants of health.
Religious attacks on sexual and reproductive rights
These limitations on health extended to reproduction and sexuality, as the Reagan administration looked to conservative social values to attack sexual and reproductive rights, seeking to constrain the expansion of women’s rights and reimpose traditional gender roles. Invoking conservative religious ideologies that opposed gender equality, contraception, and abortion, the administration abandoned domestic family planning programs and raised new obstacles to abortion access.[52] Such attacks on reproductive rights, responding to the 1973 US Supreme Court decision in Roe v. Wade and supported by a “moral majority” movement, were seen as central to a larger social conservative battle to protect the traditional, heterosexual “nuclear family” and preserve the patriarchal, male-dominated familial dynamic.[53] This politicization of women’s rights impacted health throughout the world, as the United States sought to block foreign assistance to any organization that performed, promoted, or discussed abortions in any country. Announcing this policy shift at the 1984 International Conference on Population in Mexico City, the so-called Mexico City Policy (or Global Gag Rule) constrained family planning programs throughout the world and expanded the administration’s attacks on reproductive rights globally.[54]
With these attacks extending to sexual rights, the Reagan administration’s inaction in the early days of the HIV/AIDS response reflected an explicit rejection of the rights of gay, bisexual, and transgender populations that were disproportionately impacted by the disease.[55] The administration saw these populations as morally “sinful” and, through this right-wing religious lens, rejected the equal dignity and rights of affected populations—stigmatizing vulnerable communities, denying timely information, and neglecting the right to health.[56] Six years after the first cases were identified, WHO was rallying the world to develop a rights-based Global Strategy for the Prevention and Control of AIDS, but—with more than 20,000 Americans already dead—President Reagan still had not publicly said the word “AIDS.”[57] Despite repeated pleas from affected populations asserting a human right to government support, the administration continued to attribute the disease to a “gay lifestyle,” denying necessary research, care, and support amid the rapid rise of a pandemic threat.[58] This targeted health neglect at home was extended by neoliberal development policies that exacerbated health inequities globally.
Neoliberal health reforms amid structural adjustment programs
Shifts under the Reagan administration furthered the “neoliberal era” in economic development policy, as US-led international financial institutions exacerbated health disparities within and between countries. This “Washington Consensus” of neoliberal policies—seeking to liberalize the economies of developing countries through deregulation, marketization, privatization, and decentralization—decimated fragile health and social infrastructures throughout the world.[59] Pushing these neoliberal reforms on fragile governments in return for loan-based debt assistance, the International Monetary Fund demanded that low-income countries adopt “structural adjustments” that rapidly reduced government expenditures, scaling back the public health systems necessary to respond to rising health burdens. These market-oriented conservative policy reforms, undertaken to service debt without regard for human rights, limited government action to ensure basic needs.[60] Under such “structural adjustment programs,” the International Monetary Fund was able to “demand cuts in government expenditure, including axing or abolishing programmes for education, health, housing and public sector development, like sewage disposal and public housing.”[61] Even as these programs failed to stoke economic growth, the dramatic scaling back of government commitments to uphold public health left in its wake weakened national public health infrastructures unable to bear the burden of rising health challenges.[62]
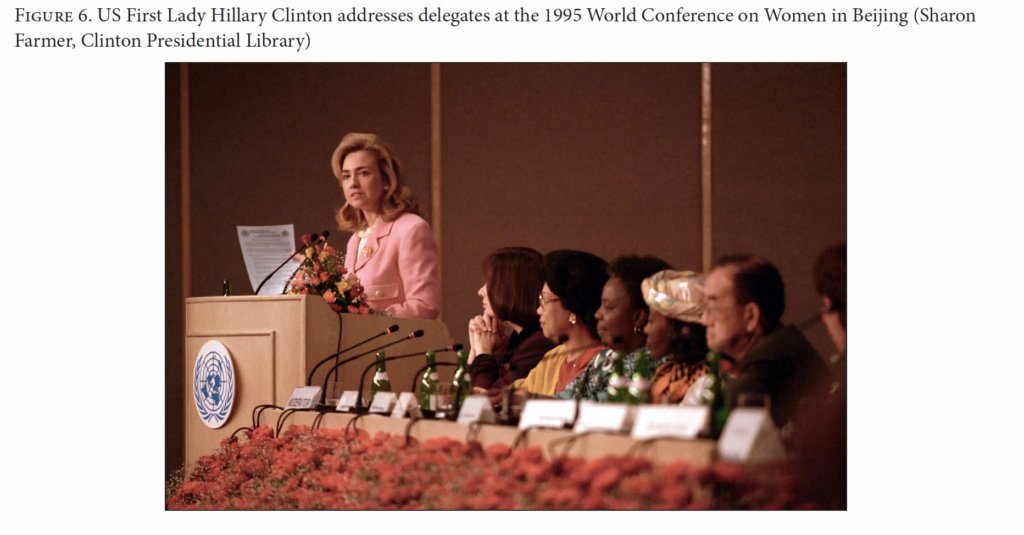
The end of the Cold War at the start of the 1990s, followed by the election of Democratic President Bill Clinton in 1992, offered the promise of ending US opposition to human rights in global health. Declaring a new post-Cold War consensus on human rights, delegates at the 1993 World Conference on Human Rights sought to bridge the divide between civil and political rights and economic, social, and cultural rights. The resulting Vienna Declaration and Programme of Action declared that all human rights are “universal, indivisible and interdependent and interrelated” and should be treated “on the same footing, and with the same emphasis.”[63] The Clinton administration, seeking to establish a “Third Way” movement at the center of the political spectrum, looked in this moment of sweeping global change to renew US leadership in multilateral health governance: playing a leading role in advancing the HIV/AIDS response through the 1994 creation of the Joint United Nations Programme on HIV/AIDS (UNAIDS); spearheading the UN’s Fourth World Conference on Women in 1995 and strengthening the United Nations Population Fund (UNFPA); and supporting a united international front against climate change through the 1997 Kyoto Protocol.[64]
Yet despite this renewed leadership and financial support, the conservative legacy of the neoliberal approach to health persisted across US political parties. When the Clinton administration sought to reform health care at home, it proposed only an incremental, market-oriented approach to universal care, prioritizing efficiencies in private health insurance coverage while conspicuously avoiding the language of human rights.[65] As Republican lawmakers and interest groups scaled back their support for the individual elements of this reform package, the comprehensive bill failed, and in the wake of this failure, Congress passed the 1997 State Children’s Health Insurance Program to provide health coverage to uninsured children whose family income was too high to qualify for Medicaid.[66] Throughout the world, the US government continued to address health as a means to economic development rather than as a right—an end unto itself. This neoliberal “health for growth” model elevated health, nutrition, and population funding under the World Bank while strengthening pharmaceutical patent protections under the World Trade Organization.[67] As authority in global health governance continued to shift from WHO to international financial institutions, the WHO Secretariat sought to reorient itself—from the unquestioned leader to a necessary coordinator in a crowded global health governance landscape.[68]
Global health security: “Compassionate conservatism” abandoned
Amid this leadership vacuum in global health governance, the global health architecture in the 21st century shifted toward greater US hegemony in global health policy, with commentators increasingly noting that “the US domestic agenda is driving the global agenda” in health.[69] Terrorist attacks against the United States realigned this rising US engagement in global health, refocusing public health through the lens of national security even as Republican President George W. Bush sought to expand lifesaving treatments abroad as a religious imperative. Yet despite this increasing Republican attention to global health, subsequent Democratic Party efforts to expand health care access in the United States would be attacked relentlessly by conservatives as a “threat to freedom,” giving rise to a new anti-government populist movement that opposed the right to health and prevailed in the 2016 US elections.
Terrorist attacks and the securitization of public health
The attacks of September 11, 2001 redefined US interests in public health, as Al-Qaeda terrorist attacks against the United States (alongside a bioterrorist “anthrax scare” in the days that followed) upended global health engagement under the Bush Administration, reframing public health as a national security imperative.[70] Although President George W. Bush had presented his administration as the foundation of a new “compassionate conservatism,” advancing social conservative values alongside government assistance to those in need, these attacks reshaped foreign policy amid a self-declared “War on Terror,” in which public health was redefined to address the fear of bioterrorism and disease “invasion.”[71] The Bush administration rapidly responded to this rising fear by developing the Model State Emergency Health Powers Act, a federal template for state public health law reforms, which was seen to prioritize the state’s police powers to protect “health security” at the expense of individual autonomy, civil liberties, and human rights.[72] The resulting state public health policy debates under this model act demonized immigrants and minority populations—especially Arab and Middle Eastern populations—as Islamic terrorist sympathizers, carriers of disease, and national security threats.[73] The War on Terror would lead to widespread violations of human rights at home and abroad, as the securitization of health was seen to require human rights limitations to protect public health, even as the United States sought to reshape foreign assistance through an unprecedented bipartisan commitment to HIV treatment.
A religious imperative for HIV treatment
The Bush administration remained eager to advance global health as a religious imperative, but it was unwilling to delegate substantive health authority to international organizations.[74] Moving away from international institutions as mechanisms for distributing lifesaving treatments, the United States bypassed these multilateral organizations in pursuing an ambitious expansion of its foreign health assistance, increasingly making US bilateral assistance a singular force in global health governance. As the G8 established the Global Fund to Fight AIDS, Tuberculosis and Malaria in 2001, the US government was rapidly moving to create new health institutions outside of the UN system, over which it would have greater control.[75] This bilateral approach to humanitarian assistance found bipartisan support in 2003 through the President’s Emergency Plan for AIDS Relief (PEPFAR), which would become a principal mechanism of US global health funding.
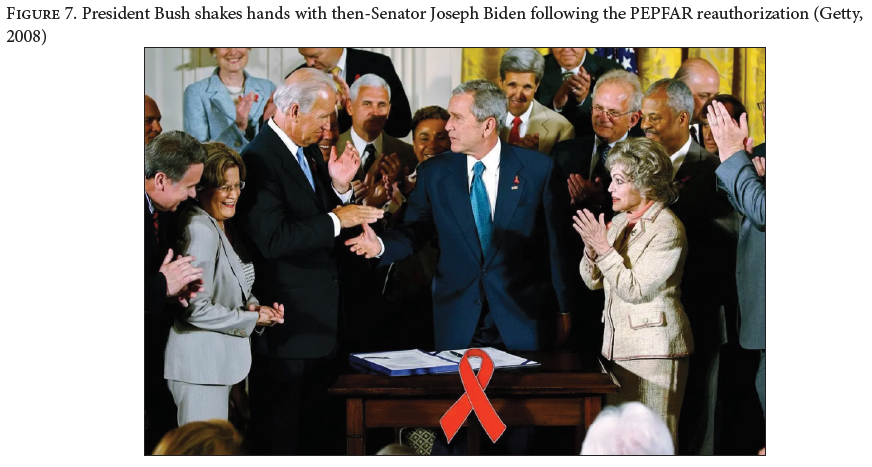
The launch of PEPFAR represented an unprecedented Republican commitment to scaling up programs for the care and treatment of HIV. Although PEPFAR was not presented as a basis to realize the right to health, bipartisan support for this initiative increased US government spending on a scale that rivaled any other American effort in global health, serving as the largest commitment by any nation to fight a single disease.[76]
The Democratic dream of universal health care gives rise to right-wing populism
The election of President Barack Obama presented the opportunity to achieve a longstanding Democratic Party goal: universal health care for all Americans. Revitalizing debates on the “moral commitment” of government to secure the health of every American, the 2010 Patient Protection and Affordable Care Act (ACA) advanced the realization of health as a human right, marking the most expansive reform of the US health care system in decades.[77] Yet while the ACA offered an unprecedented expansion of access to health care services, drawing from progressive rights-based health reforms across US states, it did not stray from the neoliberal market-based approach, working through private health insurance systems to expand access to health coverage.[78] Despite this market-based approach, with roots in past Republican proposals, the Republican Party nevertheless attacked the “Obamacare” legislation as a threat to freedom and a violation of the US Constitution.[79] Even though the Obama administration intentionally avoided justifying its policy reforms through a commitment to rights and freedoms, never invoking human rights to frame congressional debates, the ACA reflected a comprehensive effort to rein in insurance costs and improve equitable health outcomes, bringing the United States closer to other nations in realizing a right to health care.[80]
Following the passage of the ACA, President Obama harkened back to President Roosevelt in speaking before the UN General Assembly, declaring explicitly that “freedom from want is a basic human right,” as the 2011 US report to the UN’s Universal Periodic Review heralded the enactment of the ACA as a reflection of America’s commitment to progressively realize the right to health.[81] Beyond this advancement of government responsibility for health care at home, human rights became a renewed focus of US policy to advance health throughout the world, as President Obama strengthened global health policy through a coordinated strategy for US engagement with global health security.[82] This proclaimed commitment to human rights offered a moral justification for US bilateral leadership in building the capacity of African health institutions and for US multilateral support in developing global resolutions to advance universal health coverage, sexual and reproductive health, and climate change mitigation.[83] Human rights had become a foundation for renewed US leadership in public health; however, these health policy advancements galvanized populist opposition, as conservative activists, under the banner of a “Tea Party” revolution, relentlessly attacked government efforts to expand access to health as a fundamental threat to freedom.[84] The Trump presidential campaign adopted this populist rhetoric in attacking the ACA, riding a right-wing populist wave to capture the Republican nomination, with the 2016 US election turning on opposition to health care reforms and leading to profound transitions in public health policy.[85]
The populist threat to public health
The first Trump administration threatened the human rights that underlie public health, in the United States and throughout the world. Rejecting the fundamental notion that all people are equal in dignity, the administration rapidly pursued discriminatory policies that targeted marginalized populations, denied health services, and redefined “unalienable rights.”[86] The administration also attacked the foundations of health policy, pursuing cuts in health research, prioritization of corporate deregulation, and withdrawal from global initiatives.[87] These violations of human rights, challenges to public health, and isolationism in international affairs undermined the US government’s response to the COVID-19 pandemic. The failures of the pandemic response shaped the 2020 election, after which the Biden administration sought to renew US leadership in global health and human rights. Yet the 2024 elections again presented an existential crossroads for the United States, offering divergent paths for continuing US engagement with health and human rights.
Violating human rights, undermining health science, and rejecting global governance
With populist leadership dividing the United States, the first Trump administration threatened universal human rights and weakened public health protections.[88] President Trump opened his presidency in January 2017 by issuing an executive order to establish a “Muslim ban” that restricted refugees and immigrants from seven Muslim-majority countries, and these political attacks on immigrants would expand in the years that followed, as the government prosecuted migrants, separated families, and uprooted lives.[89] Undermining domestic public health systems, the administration pre-empted state public health laws while reducing the power of federal health agencies to prevent disease and promote health.[90] This populist threat to human rights and public health extended globally through isolationist policies, with the Trump administration reducing foreign assistance, flouting international norms, abandoning international partnerships, and weakening international organizations.[91] As seen in attacks on sexual and reproductive health and rights, President Trump expanded the “Global Gag Rule” to restrict American reproductive health assistance, closed US programs addressing HIV/AIDS, maternal and child health, and LGBTQ+ health, and withheld funding to the UNFPA.[92] Advancing an “America First” foreign policy, the administration rejected a range of international policies and organizations, as the United States withdrew from several UN agencies and abandoned global efforts to address the cataclysmic threat of climate change under the Paris Agreement.[93] These attacks on human rights, public health, and global governance proved catastrophic in responding to the COVID-19 pandemic.
Challenging international human rights amid a public health emergency
When faced with this new threat, the administration reacted with division and discrimination. The president referred to COVID-19 as the “Chinese virus” (in ways that stoked attacks against Asian Americans), dismissed public health data and expertise (initially denying the severity of the disease before rejecting prevention measures, promoting unproven treatments, and attacking health officials), and undermined international collaboration through global governance (initially halting WHO funding before calling for US withdrawal from WHO).[94] Abandoning global health governance in responding to a shared health crisis, the Trump administration rejected WHO public health guidance, instituted international travel bans, and blocked health data sharing in the pandemic response.[95] Isolated in facing this public health emergency, the administration pursued repressive measures in ways that undercut democratic guarantees, neglected vulnerable populations, and exacerbated health inequities in violation of human rights obligations.[96] In an effort to redefine rights to reflect administration priorities, the US government’s newly established Commission on Unalienable Rights released a 2020 report that sought to delimit human rights to a narrow conceptualization of rights rooted in a Christian interpretation of natural law, disregarding subsequent advancements of rights under international law (that protect women, children, and minorities), promoting religious freedom as a paramount right, and refuting the human rights that underlie health.[97] Advancing this redefinition of rights globally, the administration in 2020 introduced the Geneva Consensus Declaration as a basis to form an international coalition of conservative countries that would work together to reorient women’s health around conservative values, explicitly rejecting abortion as a human right.[98] These compounding policies weakened US influence in international affairs, constrained the global response to the COVID-19 pandemic, and threatened the international vision of human rights, with the future of health and human rights hanging in the balance.
A fleeting moment of renewed leadership
The 2020 election of President Joseph Biden provided a brief opening to reinstate US leadership as a basis for human rights, public health, and global solidarity. Following a contentious presidential campaign amid a catastrophic pandemic response—a response that had already seen millions of lives lost and left the United States dangerously disconnected from its past international leadership—the public health and human rights communities sought to support the rebuilding task ahead.[99] Yet even as President Biden looked to reshape US leadership under the right to health, the United States continued to be impacted by health inequities driven by the COVID-19 pandemic.[100] The Biden administration immediately sought to reintegrate human rights into public health through value-based care, prioritizing scientific integrity, health equity, and evidence-based policymaking.[101] Advancing health globally, the administration reversed the US withdrawal from WHO, repealed the Global Gag Rule, reauthorized PEPFAR, rejoined the Paris Climate Agreement, and took unprecedented steps to mitigate the climate threat through the Inflation Reduction Act of 2022.[102] Given the detrimental global health impacts of COVID-19, the US government increased bilateral foreign assistance for health and joined with other WHO member states to strengthen pandemic preparedness multilaterally through 2024 amendments to the International Health Regulations and negotiations that led to the 2025 WHO Pandemic Agreement.[103]
However, health and human rights continued to face systematic obstacles as the 2024 US elections approached, with the Trump campaign explicitly threatening to confront the public health scientists, human rights protections, and global governance institutions that underlie health in the United States and throughout the world.[104] This destructive vision for a second Trump administration was laid out in detail by the Heritage Foundation in its “Project 2025” manifesto, which presented a detailed path to consolidate right-wing power in the US government by reshaping democratic principles, reducing the government workforce, and withdrawing from global governance in ways that would threaten health and human rights.[105] That vision is now rapidly being carried out in US policy.
Conclusion
Eighty years of conservative opposition to the notion of health as a human right, challenging who is entitled to rights and what those rights include, have led to this uncertain moment, as the Trump administration attacks public health science, fundamental human rights, and global health governance. These attacks are not an aberration but a culmination, extending past conservative opposition to its ultimate policy solution: the end of health as a human right. Rather than reframing or reducing existing institutions of health and human rights, as seen in past conservative administrations, this administration now seeks to destroy the very institutions that shape the realization of the right to health, eviscerating scientific research structures, persecuting human rights defenders, and abandoning global health engagement.[106] In the absence of congressional action, the administration’s rapid reshaping of US health policy—through the rejection of health expertise, defunding of scientific research, deregulation of harmful industries, privatization of health services, abandonment of foreign assistance, and withdrawal from global governance—will exacerbate health challenges in the United States and threaten millions throughout the world.[107] This decline of US leadership to promote health and human rights will outlive the present administration, undermining health outcomes for generations and widening health inequities at home and abroad.
These attacks on the right to health should be seen as undermining core American values, where health is a foundational underpinning of rights enshrined in the US Constitution and Bill of Rights. While not explicitly enumerated in the nation’s founding documents, principles of individual freedom, a core American value, cannot exist without public health.[108] Presidents have recognized this before. Facing the twin challenges of the Great Depression and World War II, President Roosevelt explicitly proclaimed that the “land of the free” cannot ensure freedom when people live in want.[109] The US government serves to uphold that freedom from want by ensuring the conditions essential for public health. The right to health must be seen not just as an international obligation but as a foundation of American democracy. Supporting this foundation in 1944, Roosevelt called for a Second Bill of Rights, not to challenge the original Bill of Rights but to build on its foundations by guaranteeing the opportunity to achieve good health. Ensuring this equality of opportunity today will require a social minimum for all individuals and a rights-based allocation of resources for health.[110]
It will be necessary for the United States to enshrine the right to health as central to American democracy, looking to both federal and state laws to unite the nation to realize the highest attainable standard of health. With more than 110 countries already guaranteeing specific rights for the progressive realization of health, the right to health is widely codified as a core value, explicit right, or fundamental entitlement in national constitutions and foundational documents across the world.[111] Within the United States, a rising number of states have already developed constitutional and legislative entitlements to ensure health-related rights for those whose rights are not protected by the federal government.[112] This evolving recognition of the right to health has raised a nationwide imperative, learning from past opposition, to recognize the right to health as a core government commitment. Such constitutive commitments under domestic law will be necessary to make the right to health a reality in the United States, building on past movements to overcome continuing conservative opposition.[113] In this rising American movement to ensure the right to health, there is a crucial role for the political engagement of public health leaders, building a national campaign to ensure that health for all can become a unifying vision to define America’s future.
Benjamin Mason Meier is a professor of global health policy at the University of North Carolina at Chapel Hill, United States.
Darby McBride is a student in the Community and Global Public Health Program at the Gillings School of Global Public Health, University of North Carolina at Chapel Hill, United States.
Please address correspondence to Benjamin Mason Meier. Email: bmeier@unc.edu.
Competing interests: None declared.
Copyright © 2026 Meier and McBride. This is an open access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (http://creativecommons.org/licenses/bync/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] L. Henkin, The Age of Rights (Columbia University Press, 1990).
[2] S. I. Rosenman (ed), The Public Papers and Addresses of Franklin D. Roosevelt: 1940 (Macmillan, 1941), p. 672.
[3] M. R. DiNunzio, Franklin D. Roosevelt and the Third American Revolution (Bloomsbury, 2011).
[4] C. Sunstein, The Second Bill of Rights (Basic Books, 2009).
[5] F. D. Roosevelt, “Message on the State of the Union,” Congressional Records 55/57 (1944).
[6] D. J. Whelan and J. Donnelly, “The West, Economic and Social Rights, and the Global Human Rights Regime: Setting the Record Straight,” Human Rights Quarterly 29/908 (2007).
[7] E. R. Stettinius, “Human Rights in the United Nations Charter,” Annals of the American Academy of Political and Social Science 243/1 (1946).
[8] Official Records of the World Health Organization No. 2: Proceedings and Final Acts of the International Health Conference Held in New York from 19 June to 22 July 1946 (1948), p. 31 (emphasis in original).
[9] Constitution of the World Health Organization (1946).
[10] Ibid., preamble.
[11] M. A. Glendon, A World Made New: Eleanor Roosevelt and the Universal Declaration of Human Rights (Random House, 2001).
[12] These Rights and Freedoms (United Nations Department of Public Information, 1950).
[13] A. M. Black, “Eleanor Roosevelt and the Universal Declaration of Human Rights,” OAH Magazine of History 22/28 (2008).
[14] C. Eagleton, “The United States and the United Nations,” in Annual Survey of American Law (1952).
[15] C. Anderson, Eyes off the Prize: The United Nations and the African American Struggle for Human Rights (Cambridge University Press, 2009).
[16] Social Insurance and Allied Services: Report by Sir William Beveridge (Inter-Departmental Commission on Social Insurance and Allied Services, 1942).
[17] G. W. Bachman and L. Meriam, The Issue of Compulsory Health Insurance: A Study Prepared at the Request of Senator H. Alexander Smith, Chairman of the Subcommittee on Health of the Senate Committee on Labor and Public Welfare (Brookings Institution, 1948).
[18] New York Academy of Medicine, Medicine in the Changing Order (Commonwealth Fund, 1947).
[19] M. M. Peon, Harry S. Truman Versus the Medical Lobby (University of Missouri Press, 1979).
[20] “The American Medical Association: Power, Purpose, and Politics in Organized Medicine,” Yale Law Journal 63/937 (1954).
[21] A. E. Birn, “Health and Human Rights: Historical Perspectives and Political Challenges,” Journal of Public Health Policy 29/1 (2008).
[22] L. Henkin, “The United Nations and Human Rights,” International Organization 19/3 (1965).
[23] A. E. Yamin, “The Right to Health Under International Law and Its Relevance to the United States,” American Journal of Public Health 95/7 (2005).
[24] P. Alston, “The United Nations’ Specialized Agencies and Implementation of the International Covenant on Economic, Social and Cultural Rights,” Columbia Journal of Transnational Law 18/79 (1979).
[25] C. E. Allen, “World Health and World Politics,” Intelligence Organization 27/41 (1950).
[26] C. Osakwe, Participation of the Soviet Union in Universal International Organizations: A Political and Legal Analysis of Soviet Strategies and Aspirations Inside ILO, UNESCO and WHO (Sijthoff, 1972).
[27] Statement by Henry R. Labouisse, Head of the Task Force on June 21, 1961, before the Senate Hearings on the International Development and Security Act of 1961 (US Government Printing Office, 1961).
[28] U. Mahajani, “Kennedy and the Strategy of Aid: The Clay Report and After,” Western Political Quarterly 18/3 (1965).
[29] B. M. Meier and L. M. Mori, “The Highest Attainable Standard: Advancing a Collective Human Right to Public Health,” Columbia Human Rights Law Review 37/1 (2005).
[30] B. M. Meier, “Global Health Governance and the Contentious Politics of Human Rights: Mainstreaming the Right to Health for Public Health Advancement,” Stanford Journal of International Law 46/1 (2010).
[31] Anderson (see note 15).
[32] M. F. Davis, Brutal Need: Lawyers and the Welfare Rights Movement, 1960–1973 (Yale University Press, 1995).
[33] T. Marmor, “The Politics of U.S. Health System Reform,” Conference Series-Federal Reserve Bank of Boston (1969).
[34] R. Stevens, “History and Health Policy in the United States: The Making of a Health Care Industry, 1948–2008,” Social History of Medicine 21/461 (2008).
[35] E. R. Annis, “Government Health Care: First the Aged, Then Everyone,” Current History 45/104 (1963).
[36] K. Davis, “Achievements and Problems of Medicaid,” Public Health Reports 91/4 (1976).
[37] B. Hoffman, Health Care for Some: Rights and Rationing in the United States Since 1930 (University of Chicago Press, 2012).
[38] F. Quimby, The Politics of Global Health: Prepared for the Subcommittee on National Security Policy and Scientific Developments of the Committee on Foreign Affairs, U.S. House of Representatives (US Government Printing Office, 1971).
[39] N. Chorev, The World Health Organization Between North and South (Cornell University Press, 2012).
[40] S. Litsios, “The Long and Difficult Road to Alma-Ata: A Personal Reflection,” International Journal of Health Services 32/4 (2002).
[41] T. Lambo, “Towards Justice in Health,” World Health 4 (1979); C. Pannenborg, A New International Health Order: An Inquiry into the International Relations of World Health and Medical Care (Sijthoff and Noordhoff, 1979).
[42] “Inaugural Address of Jimmy Carter,” Avalon Project, https://avalon.law.yale.edu/20th_century/carter.asp.
[43] P. Bourne, New Directions in International Health Cooperation: A Report to the President (US Government Printing Office, 1978); K. Mingst, “The United States and the World Health Organization,” in M. P. Karns and K. A. Mingst (eds), The United States and Multilateral Institutions: Patterns of Changing Instrumentality and Influence (Routledge, 1990).
[44] W. P. Brandon, “Two Kinds of Conservatism in US Health Policy: The Reagan Record,” in C. Altenstetter and S. C. Haywood (eds), Comparative Health Policy and the New Right (Palgrave Macmillan, 1991).
[45] L. J. McAndrews, The Presidents and the Poor: America Battles Poverty (University Press of Kansas, 2018).
[46] J. Starrels, The World Health Organization: Resisting Third World Ideological Pressures (Heritage Foundation, 1985).
[47] K. Sikkink, “Codes of Conduct for Transnational Corporations: The Case of the WHO/UNICEF Code,” International Organization 40/815 (1986).
[48] M. Cueto, T. Brown, and E. Fee, The World Health Organization: A History (Cambridge University Press, 2019).
[49] L. D. Brown, Health Policy in the Reagan Administration: A Critical Appraisal (Brookings, 1984).
[50] S. Danziger and R. Haveman, “The Reagan Administration’s Budget Cuts: Their Impact on the Poor,” IRP Reprint 24 (1981).
[51] K. Stallard, B. Ehrenreich, and H. Sklar, Poverty in the American Dream (South End Press, 1983).
[52] J. L. Finkle and B. B. Crane, “Ideology and Politics at Mexico City: The United States at the 1984 International Conference on Population,” Population and Development Review 11/1 (1985).
[53] R. P. Petchesky, “Antiabortion, Antifeminism, and the Rise of the New Right,” Feminist Studies 7/206 (1981).
[54] “The International Conference on Population, 1984,” Population and Development Review 10/755 (1984).
[55] L. O. Gostin and Z. Lazzarini, Human Rights and Public Health in the AIDS Pandemic (Oxford University Press, 1997).
[56] J. Mann and D. Tarantola, “Responding to HIV/AIDS: A Historical Perspective,” Health and Human Rights 2/5 (1998).
[57] N. Krieger and R. Appleman, “The Politics of AIDS” in AIDS: The Politics of Survival (Baywood Publishing Company, 1994).
[58] D. Altman, “HIV, Homophobia, and Human Rights,” Health and Human Rights 2/4 (1998).
[59] J. Yong, J. V. Millen, A. Irwin, and J. Gershman, Dying for Growth: Global Inequality and the Health of the Poor (Common Courage Press, 2000).
[60] R. Falk, “Interpreting the Interaction of Global Markets and Human Right,” in A. Brysk (ed), Globalization and Human Rights (University of California Press, 2002).
[61] T. Evans, “A Human Right to Health,” Third World Quarterly 23/2 (2002).
[62] D. P. Fidler, International Law and Infectious Diseases (Oxford University Press, 1999).
[63] World Conference on Human Rights, Vienna Declaration and Programme of Action, UN Doc. A/CONF.157/23 (1993).
[64] C. Campbell and B. A. Rockman, “Third Way Leadership, Old Way Government: Blair, Clinton and the Power to Govern,” British Journal of Politics and International Relations 3/1 (2001); Board on International Health, Institute of Medicine, America’s Vital Interest in Global Health: Protecting Our People, Enhancing Our Economy, and Advancing Our International Interests (National Academy Press, 1997).
[65] A. R. Chapman, Health Care Reform: A Human Rights Approach (Georgetown University Press, 1994).
[66] E. D. Kinney, “Recognition of the International Human Rights to Health and Health Care in the United States,” Rutgers Law Review 60/335 (2007).
[67] World Health Organization, Macroeconomics and Health: Investing in Health for Economic Development (2001), https://www.who.int/publications/i/item/924154550X; R. P. Petchesky, Global Prescriptions: Gendering Health and Human Rights (Zed Books, 2003); L. Forman, “Trade Rules, Intellectual Property, and the Right to Health,” Ethics and International Affairs 21/3 (2007).
[68] T. M. Brown, M. Cueto, and E. Fee, “The World Health Organization and the Transition from ‘International’ to ‘Global’ Public Health,” American Journal of Public Health 96/62 (2006).
[69] I. Kickbusch, “Influence and Opportunity: Reflections on the US role in Global Public Health,” Health Affairs 21/131 (2002).
[70] J. M. Hughes and J. L. Gerberding, “Anthrax Bioterrorism: Lessons Learned and Future Directions,” CDC Emerging Infectious Diseases 8/10 (2002); A. S. Khan, “Public Health Preparedness and Response in the USA Since 9/11: A National Health Security Imperative,” Lancet 378/1460 (2011).
[71] L. O. Gostin, “Public Health Law in an Age of Terrorism: Rethinking Individual Rights and Common Goods,” Health Affairs 21/79 (2002).
[72] G. J. Annas, “Bioterrorism, Public Health, and Civil Liberties,” New England Journal of Medicine 346/1337 (2002).
[73] N. B. King, “The Influence of Anxiety: September 11, Bioterrorism, and American Public Health,” Journal of the History of Medicine and Allied Sciences 58/4 (2003).
[74] J. Kassalow, Why Health Is Important to U.S. Foreign Policy (Council on Foreign Relations, 2001).
[75] Brown et al. (see note 68).
[76] E. J. Emanuel, “PEPFAR and Maximizing the Effects of Global Health Assistance,” JAMA 307/20 (2012).
[77] A. Rudiger and B. M. Meier, “A Rights-Based Approach to Health Care Reform,” in E. Beracochea, C. Weinstein, and D. P. Evans (eds), Rights-Based Approaches to Public Health (Springer, 2011).
[78] G. MacNaughton, M. McGill, A. Jakubec, et al., “Engaging Human Rights Norms to Realize Universal Health Care in Massachusetts, USA,” Health and Human Rights 20/2 (2018).
[79] S. Butler, “Don’t Blame Heritage for ObamaCare Mandate,” Heritage Foundation (February 6, 2012), https://www.heritage.org/health-care-reform/commentary/dont-blame-heritage-obamacare-mandate.
[80] C. Ho, Normalizing an American Right to Health (Oxford University Press, 2023).
[81] B. M. Meier and L. Gable, “US Efforts to Realise the Right to Health Through the Patient Protection and Affordable Care Act,” Human Rights Law Review 13/1 (2013).
[82] C. McInnes, A. Kamradt-Scott, K. Lee, et al., The Transformation of Global Health Governance (Palgrave Macmillan, 2014).
[83] L. O. Gostin and E. Friedman, “A Retrospective and Prospective Analysis of the West African Ebola Virus Disease Epidemic: Robust National Health Systems at the Foundation and an Empowered WHO at the Apex,” Lancet 385/9980 (2015).
[84] K. Arceneaux and S. P. Nicholson, “Who Wants to Have a Tea Party? The Who, What, and Why of the Tea Party Movement,” Political Science and Politics 45/4 (2012).
[85] J. Geyman, “Crisis in U.S. Health Care: Corporate Power Still Blocks Reform,” International Journal of Health Services 48/1 (2017).
[86] M. Rise, “On American Values, Unalienable Rights, and Human Rights: Some Reflections on the Pompeo Commission,” Ethics and International Affairs 34/1 (2020).
[87] J. M. Sharfstein, “Science and the Trump Administration,” JAMA 318/14 (2017).
[88] D. W. Drezner, “Present at the Destruction: The Trump Administration and the Foreign Policy Bureaucracy,” Journal of Politics 81/2 (2019).
[89] The White House, “Executive Order Protecting the Nation from Foreign Terrorist Entry into the United States,” (2017), https://trumpwhitehouse.archives.gov/presidential-actions/executive-order-protecting-nation-foreign-terrorist-entry-united-states-2/; S. Woolhandler, D. U. Himmelstein, S. Ahmed, et al., “Public Policy and Health in the Trump Era,” Lancet 397/10275 (2021).
[90] J. G. Hodge, M. Morcelle, S. Wetter, et al., “Public Health Preemption: Constitutional Affronts to Public Health Innovations,” Ohio State Law Journal 79/4 (2018).
[91] F. Quigley, “Trump-Pence Attack on Healthcare Challenged at Its Roots,” Health and Human Rights (October 8, 2019), https://www.hhrjournal.org/2019/10/08/trump-pence-attack-on-healthcare-challenged-at-its-roots/.
[92] A. Ahmed and T. McGovern, “Sexual and Reproductive Health and Rights: Advancing Human Rights to Protect Bodily Autonomy and Sexuality,” in L. O. Gostin and B. M. Meier (eds), Global Health Law and Policy: Ensuring Justice for a Healthier World (Oxford University Press, 2023).
[93] The White House, “President Donald J. Trump at the United Nations General Assembly: Outlining an America First Foreign Policy” (September 20, 2017), https://trumpwhitehouse.archives.gov/briefings-statements/president-donald-j-trump-united-nations-general-assembly-outlining-america-first-foreign-policy/; C. Amirfar and A. Singh, “The Trump Administration and the ‘Unmaking’ of International Agreements,” Harvard International Law Journal 59/443 (2018).
[94] C. R. Williams, J. G. Kestenbaum, and B. M. Meier, “Populist Nationalism Threatens Health and Human Rights in the COVID-19 Response,” American Journal Public Health 110/12 (2020).
[95] S. Sekalala, L. Forman, R. Habibi, et al., “Health and Human Rights Are Inextricably Linked in the COVID-19 Response,” BMJ Global Health 5 (2020).
[96] L. O. Gostin, A. Constantin, and B. M. Meier, “Global Health and Human Rights in the Age of Populism,” in L. O. Gostin and B. M. Meier (eds), Foundations of Global Health and Human Rights (Oxford University Press, 2020).
[97] “Report of the Commission of Unalienable Rights,” (2020) https://www.state.gov/wp-content/uploads/2020/07/Draft-Report-of-the-Commission-on-Unalienable-Rights.pdf.
[98] L. Morgan, “Anti-Abortion Strategizing and the Afterlife of the Geneva Consensus Declaration,” Developing World Bioethics 23 (2023).
[99] B. M. Meier, L. Hango, V. Matus, et al., “Health and Human Rights in the New American Administration,” Health and Human Rights (December 20, 2020), https://www.hhrjournal.org/2020/12/20/health-and-human-rights-in-the-new-american-administration/.
[100] B. J. Stark, “Inequality, COVID-19, and International Human Rights: Whose Lives Matter?,” Journal of International and Comparative Law 27/2 (2021).
[101] R. L. Haffajee and B. D. Sommers, “Evidence-Based Health Policy in the Biden-Harris Administration,” JAMA Health Forum 2/7 (2021).
[102] X. Becerra, “U.S. HHS Secretary Becerra: Remarks at the 74th World Health Assembly,” US Mission to International Organizations in Geneva (2021).
[103] L. Pace and S. C. Kim, “Strengthening Global Health Security Under the Biden-Harris Administration,” Journal of Law, Medicine and Ethics 53/1 (2025).
[104] B. M. Meier, A. E. L. Palmquist, M. Dockery, et al., “The 2024 U.S. Elections: Global Health Policy at a Crossroads,” Journal of Law, Medicine and Ethics 52/498 (2024).
[105] Heritage Foundation, Project 2025 Presidential Transition Project (2023); C. Piroddi, L. Gilby, M. Koivusalo, et al., “The Hegemony of Far-Right Populism, Project 2025, and the Dangers Ahead for Science and Public Health,” International Journal of Social Determinants of Health and Health Services (2025).
[106] J. J. Amon, “Free Speech, the Right to Health, and Genocide,” Health and Human Rights 27/1 (2025).
[107] U.S Department of State, America First Global Health Strategy (2025), https://www.state.gov/america-first-global-health-strategy; J. S. Morrison and L. O. Gostin, “Promise and Gaps in America First Strategy for Global Health,” BMJ 391 (2025); S. Halabi, L. O. Gostin, K. Wontumi, et al., “Science and Public Health in the Trump Era: The Dismantling of Evidence and Institutions, and Proposals for Reconstruction,” Journal of Health Politics, Policy and Law 51/2 (2026).
[108] W. Parmet, Constitutional Contagion: COVID, the Courts, and Public Health (Cambridge University Press, 2023).
[109] Sunstein (see note 4).
[110] S. Moyn, Not Enough: Human Rights in an Unequal World (Harvard University Press, 2018).
[111] J. Heymann, A. Cassola, A. Raub, and L. Mishi, “Constitutional Rights to Health, Public Health and Medical Care: The Status of Health Protections in 191 Countries,” International Journal for Research, Policy and Practice 8/6 (2013).
[112] G. MacNaughton, F. Haigh, M. McGill, et al. “The Impact of Human Rights on Universalizing Health Care in Vermont, USA,” Health and Human Rights 17/2 (2015); A. Rudiger, “Human Rights and the Political Economy of Universal Health Care,” Health and Human Rights 18/2 (2016).
[113] L. O. Gostin, T. Daniely, H. E. Huffstetler, et al., “The Shibboleth of Human Rights in Public Health,” Lancet Public Health 5/471 (2020).