Assessing the Human Rights Framework on Private Health Care Actors and Economic Inequality
Vol 25/2, 2023, pp. 125-139 PDF
Rossella De Falco, Timothy Fish Hodgson, Matt McConnell, and A. Kayum Ahmed
Abstract
Private actors’ involvement in health care financing, provision, and governance contributes to economic inequality. This paper provides an overview of emerging normative trends regarding private actors’ involvement in health care by reviewing and critically analyzing international and regional human rights standards on the right to the highest attainable standard of physical and mental health. Specifically, we survey statements from United Nations human rights treaty bodies and recent jurisprudence of the African Commission on Human and Peoples’ Rights that discuss private actors’ involvement in health care. We then identify strengths and weaknesses of the current international human rights law framework to address the human rights and inequality impacts of private health care actors, before concluding with a series of recommendations to further develop existing standards.
Introduction
Over the last 40 years, the involvement of private actors in health care has steadily grown in most countries, albeit at different paces, for different reasons, and in varying social, political, and economic contexts.[1] Such private health care actors include providers (e.g., hospitals and clinics), insurance companies and sickness funds that finance health care services, and private suppliers of health care goods, such as pharmaceutical companies and medical equipment manufacturers.
In several high-income countries, private actors’ role in health care began to grow in the late 1970s and early 1980s as a part of broader neoliberal policy reforms that aimed to diminish the role of the state and expand that of the market, particularly in the provision of social services.[2] In many low- and middle-income countries, this liberalization of the health sector, which increased private actors’ involvement, was largely driven by conditionalities attached to development aid and economic stability loans, as international and regional banking systems similarly pursued policies that viewed health care as a private good.[3]
Often short of full-scale sectoral privatization, private sector involvement in health has taken a variety of intermediate shapes, including contracting and subcontracting, public-private partnerships, and various private-in-public arrangements, such as private wards in public hospitals. In this paper, these various ways in which market mechanisms have spread within health systems through privatization, liberalization, and deregulation are referred to as commercialization, an umbrella term emphasizing the market logic across these processes.[4]
The utility and social impact of health care commercialization is hotly contested by academics, public health experts, economists, and human rights practitioners.[5] Advocates for private health care markets argue that the private sector is more efficient, less bureaucratic, and more cost-effective than the public counterparts and may improve health care outcomes and quality of care.[6] Critics, meanwhile, typically argue that claims of improved health care outcomes are either exaggerated or false and that higher private sector involvement results in unfair, fragmented, and expensive health care systems.[7]
However, significant evidence suggests that health care commercialization deepens vertical, economic-based inequalities in access to health care services and medicines. In the United States, for example, a recent study found that the privatization of 258 hospitals between 2000 and 2018 resulted in a reduction in the number of low-income Medicaid patients treated, because such patients are less profitable than other groups due to lower public reimbursement rates.[8] A recent quantitative analysis of private health clinics in Kenya over 2012–2020 also found a positive association between relative income and the quality of health care received.[9] Similar pro-rich inequalities in the utilization of private medical insurance and services have been found in Ireland, Mongolia, and Nepal, among others.[10] Consistent with these trends, some traditional public health institutions have recently issued statements critical of health care commercialization. In 2023, the Lancet, a preeminent general medical journal, published a series of articles on the commercial determinants of health and how “a substantial group of commercial actors are escalating avoidable levels of ill health, planetary damage, and inequity.”[11]
Some of the most consistent critics of health care commercialization, however, have been nongovernmental human rights organizations, which have increasingly raised concerns about the impacts of health care commercialization on human rights across the world, including notably in countries such as India, Italy, Kenya, Lesotho, Nigeria, South Africa, Uganda, and the United States.[12] In part, this focus reflects the key role that international human rights law can play in addressing commercialization, economic inequality, and the right to health. In fact, under international human rights law, even when private actors are involved in health care, states retain a primary obligation to ensure the realization of the right to the highest attainable standard of physical and mental health (the right to health), which is enshrined in article 12 of the International Covenant on Economic, Social and Cultural Rights (ICESCR).[13]
In its General Comment 14, the Committee on Economic, Social and Cultural Rights (CESCR) further clarifies that this right includes “the provision of equal and timely access to basic preventive, curative, rehabilitative health services and health education.”[14] According to a report by former Special Rapporteur on the right to health Paul Hunt, the entitlement to universal health care services encompasses states’ duty to ensure that “disadvantaged individuals and communities enjoy, in practice, the same access as those who are more advantaged.”[15] Importantly, the United Nations Guiding Principles on Business and Human Rights detail states’ duty to respect, protect, and fulfill human rights, including when third parties are involved in health care, as well as the corporate responsibility to respect human rights.[16] While the framework on protecting human rights from third-party abuses is more developed than that which governs private health care provision’s involvement in fulfilling the right to health, the latter requires urgent scrutiny.[17] In fact, private actors’ involvement in health care is increasingly part of long-term development strategies, particularly in several low- and middle-income countries.[18]
Beyond the ICESCR, which had been ratified or acceded to by 171 states at the time of writing, many other human rights treaties, as well as more than 100 constitutions around the world, contain right to health provisions.[19] Nonetheless, there remains little human rights-based research and scholarship on the right to health and private health care actors, especially in comparison to fields such as education and water.[20] However, there are the following important exceptions:
- Former Special Rapporteur on the right to health Anand Grover has noted that “privatization of health care often results in … increased inequity in the accessibility of health care and greater out-of-pocket expenditures.”[21]
- In the context of access to vaccines, the current Special Rapporteur on the right to health, Tlaleng Mofokeng, has indicated that “the benefit of industry and private companies cannot be prioritized over the rights to life and health of billions” and has more generally noted that she is considering “an examination of the role played by the privatization of health-care services—including public-private partnerships, financial aid and philanthropy—in attaining universal health coverage.”[22]
- Scholar Audrey Chapman states that the private provision of health care, in which she includes private health insurance, can have negative impacts on the right to health because it makes accountability more complex, burdens underfunded public entities with regulatory and monitoring responsibilities, negatively impacts equality and discrimination, and undermines social solidarity.[23]
- Scholar Eduardo Arenas Catalán, in a more recent and dynamic analysis of the right to health, focuses on the inherent incompatibility of “solidarity” with the commercialization of health care, arguing that widespread understandings of the right to health presently reflect “acquiescence of the commercial logic around which healthcare services have been organized under the influx of neoliberalism.”[24]
- Scholars Antenor Halo De Wolf and Brigit Toebes conceptualize a human rights impact assessment framework for health care privatization, or commercialization, plans.[25] Toebes further applies such framework to the case study of the Netherlands.[26]
- Scholar Sarah Hawkes and others have investigated the little attention to human rights in the context of public-private partnerships in health.[27]
- Human rights mechanisms and scholars have explored how the private interests of pharmaceutical companies impinge on access to medicines.[28]
- Recently developed expert principles on “Human Rights and Public Health Emergencies” strongly stress the need for the effective regulation of private health care actors at all stages in the preparation for, prevention of, response to, and recovery from health emergencies such as pandemics.[29]
In this paper, we aim to make a modest contribution to this body of human rights-based scholarship on the right to health, private health care actors, and economic inequality in accessing health care services. After defining private actors in health care, we analyze normative trends at the international level relating to states’ obligation to realize the right to health where private actors are involved in financing, providing, or supplying health care goods and services. We focus on health-related statements of United Nations human rights treaty bodies, which are the institutions mandated to authoritatively interpret and monitor the implementation of human rights treaties. Results compare the recent work of treaty bodies with recent jurisprudence of the African Commission on Human and Peoples’ Rights on the provision of public services and social rights. Drawing from this survey of health-related statements, our conclusions raise a series of questions that should be addressed through further normative development.
Methodology
This paper is based on a systematic review of treaty bodies’ statements on private actors’ involvement in health care produced between 1990 and 2023. First, we analyze general comments issued by treaty bodies to review their normative interpretations of the right to health, including how they evolved over time. Second, we analyze crosscutting normative trends in treaty bodies’ concluding observations, which are recommendations issued after their periodic review of states’ efforts to implement human rights treaties.[30] Such concluding observations were qualitatively coded based on normative indicators related to the right to health and private actors. Each extract could be associated to multiple codes due to the interconnectedness of the right to health framework. From this comparative analysis, we draw empirical conclusions on how treaty bodies interpret the right to health when private health care actors are involved, with a special focus on economic inequality within countries.
Data for this analysis were retrieved from a publicly available database collecting treaty bodies’ statements on private actors in health care, which is compiled and routinely updated by the nongovernmental organization Global Initiative for Economic Social and Cultural Rights (GI-ESCR).[31] As of June 2023, this database included 55 extracts from the concluding observations of the following treaty bodies:
- Committee on Economic, Social and Cultural Rights (CESCR)
- Committee on the Rights of the Child (CRC)
- Committee on the Rights of Persons with Disabilities (CRPD)
- Committee on the Elimination of Discrimination against Women (CEDAW)
- Committee against Torture (CAT)
- Committee on the Elimination of Racial Discrimination (CERD)
To complement this analysis, we also reviewed treaty bodies’ general comments, recommendations, and open statements, which we retrieved through complementary search. Likewise, we reviewed relevant reports of United Nations Special Rapporteurs on the right to health. At the regional level, we reviewed recent relevant developments at the African Commission.
Defining private health care actors’ involvement in health care
While there is no universal definition of private health care actors, previous human rights scholarship on this topic provides a useful guide.[32] In this paper, we understand private actors as nonstate entities that might be either individuals or institutions, whether formal or informal. Private actors in health care include “faith-based and other nongovernmental non-profit organizations and individual health-care entrepreneurs, both formal and informal, to private for-profit firms and corporations.”[33]
Health care actors can perform three functions: financing health care; providing health care; and supplying medical goods, such as pharmaceuticals, equipment, and technologies.
- We define health care financing as the act of providing funds for health care, which can happen through general taxation, insurance contributions, out-of-pocket payments, or forms of donation, including international assistance. Private actors involved in health care financing are frequently private insurers, which might be for-profit companies as well as nonprofit sickness funds.[34]
- We define health care provision as the act of delivering health care services, from prevention to treatment and rehabilitation. Private health care providers may encompass a range of health professionals (e.g., individual doctors, nurses, or psychologists) and health facilities (e.g., hospitals, clinics, nurseries, and pharmacies).
- Finally, we understand private health care suppliers as entities that are involved in researching, developing, and manufacturing therapeutics, vaccines, and other drugs, as well as medical devices, equipment, and technology. Examples of such private actors are pharmaceutical and medical devices companies.
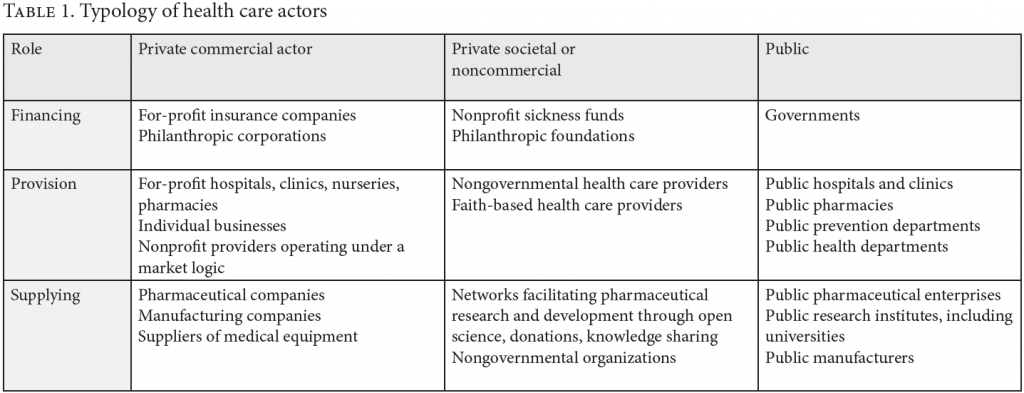
These private actors participate in the financing, provision, and supply of health care in different ways. They also have different reasons for participating in health care, including commercial and noncommercial goals.[35] These different motives have fundamental implications for the organization of health systems, and health policy scholars normally distinguish health care systems based on the relative role played by the state, the market, and societal or nongovernmental actors in health care.[36] Following this reasoning, Table 1 summarizes a typology of these health care actors, of which an earlier version was published by GI-ESCR.[37]
Treaty body statements on private actors and the right to health
Overview of relevant general comments and recommendations
Treaty bodies’ general comments have consistently regarded the role of private actors as, at the very least, nominally compatible with the right to health. CESCR’s General Comment 3, published in 1990, notes that ICESCR “neither requires nor precludes any particular form of government or economic system … provided only that it is democratic and that all human rights are thereby respected.”[38]
In General Comment 14, published in 2000, CESCR echoes this economic agnosticism, explaining that ICESCR places a duty on state parties to fulfill the right to health through “the provision of a public, private or mixed health insurance system which is affordable for all.”[39] However, in this same general comment, the committee also highlights the special risks posed by private entities involved in health care, noting that states’ obligation to protect the right to health under ICESCR requires that “the privatization of the health sector does not constitute a threat to the availability, accessibility, acceptability and quality of health facilities, goods and services.”[40]
More recently, in its 2017 General Comment 24, CESCR stresses, along similar lines, that “privatization is not per se prohibited by the Covenant,” but simultaneously notes that private actors involved in sectors such as health should be “subject to strict regulations that impose on them so-called ‘public service obligations’.”[41] In the specific context of health care, General Comment 24 further adds that “private health-care providers should be prohibited from denying access to affordable and adequate services, treatments or information.”[42]
As a result, while CESCR has consistently reiterated an agnostic position toward private entities’ involvement in health care, it has appeared to grow increasingly skeptical of market mechanisms to deliver the right to health. For example, later in General Comment 24, CESCR expresses concern that
goods and services that are necessary for the enjoyment of basic economic, social and cultural rights may become less affordable as a result of such goods and services being provided by the private sector, or that quality may be sacrificed for the sake of increasing profits.[43]
Other treaty bodies have similarly had to grapple with the role of the private sector in the realization of the right to health, as expressed within their mandates. For example, CRC’s 2013 General Comment 16 on state obligations regarding the impact of the business sector on children’s rights, which is grounded in a recognition “that the business sector’s impact on children’s rights has grown in past decades because of factors such as … outsourcing and privatizing of State functions that affect the enjoyment of human rights,” provides a comprehensive framework for state parties to ensure “that the activities and operations of business enterprises do not adversely impact on children’s rights,” including the right to health.[44]
Consistent with this trend toward greater skepticism of market actors, in May 2023, CERD released the first draft of its General Recommendation 37 on racial discrimination in the enjoyment of the right to health, which lists “privatisation and commercialisation” as potential causes of racial discrimination and includes a dedicated section on “private actors.”[45] While subject to change, this draft language endorses “mandatory human rights due diligence regimes” and more overtly recommends that
States should adopt regulation[s] ensuring that private business enterprises, private health-care facilities, insurance and pharmaceutical companies, manufacturers of health-related goods and equipment and other relevant organizations comply with the principle of equality and non-discrimination in the right to health.[46]
It is noteworthy that the report of the Special Rapporteur on the right to health on “Racism and the Right to Health” alludes to similar concerns.[47] Similarly, in its General Comment 22 on the right to sexual and reproductive health, CESCR emphasizes that states should refrain from retrogressive measures, including “legal and policy changes that reduce oversight by States of the obligation of private actors to respect the right of individuals to access sexual and reproductive health services.”[48]
This skepticism of private entities’ involvement in health care has been further cemented in treaty bodies’ general comments and recommendations over the past two decades. Their concluding observations during this period, presented in the following sections, provide additional context about the drivers of this concern and evince emerging normative trends with respect to private health care actors’ position within the right to health framework.
Concluding observations and the absence of a per se prohibition against privatization: A changing position?
While privatization may not be per se prohibited under ICESCR, concluding observations from the CESCR and other treaty bodies suggest that, at least insofar as individuals lack access to public health care options and depending on circumstances, private actors may largely be ill-suited to deliver the goods and services essential to the right to health.
For example, in 2013, CESCR noted with concern that the decline in public health spending in Egypt had resulted in a “fragmented and increasingly privatized health-care system” that had resulted in “a large percentage of the population, particularly those in vulnerable situations, being excluded from health insurance and deprived of access to health facilities, goods and services.”[49] Voicing concerns relating to economic equality, CESCR suggested in a 2023 concluding observation on El Salvador that the country’s shrinking public health care sector had increased economic segregation:
Access to health services is limited owing to the lack of financial means allocated by the State party to the public sector, and by the preference for a private-sector approach to the management, financing and provision of services, to the detriment of those who are unable to pay for such services.[50]
Recent concluding observations from other treaty bodies similarly reflect what may be a stricter scrutiny of private actors’ involvement in health care where individuals lack robust public health care. For example, in a 2022 concluding observation to Cyprus, CRC stated that it is “seriously concerned” about the “lack of access to public health care, including early detection and rehabilitation, forcing parents to cover the costs of private healthcare services.”[51] Concerning Bahrain, CRC also emphasized its concern about “the increasing trends towards the privatization” of the health and education sectors, and “the potentially negative consequences this may have on the enjoyment of economic, social and cultural rights by all children.”[52] For its part, CEDAW noted in its 2022 concluding observation on Türkiye that the lack of public options for safe abortion “compels many women to resort to expensive private clinics or unsafe abortion.”[53]
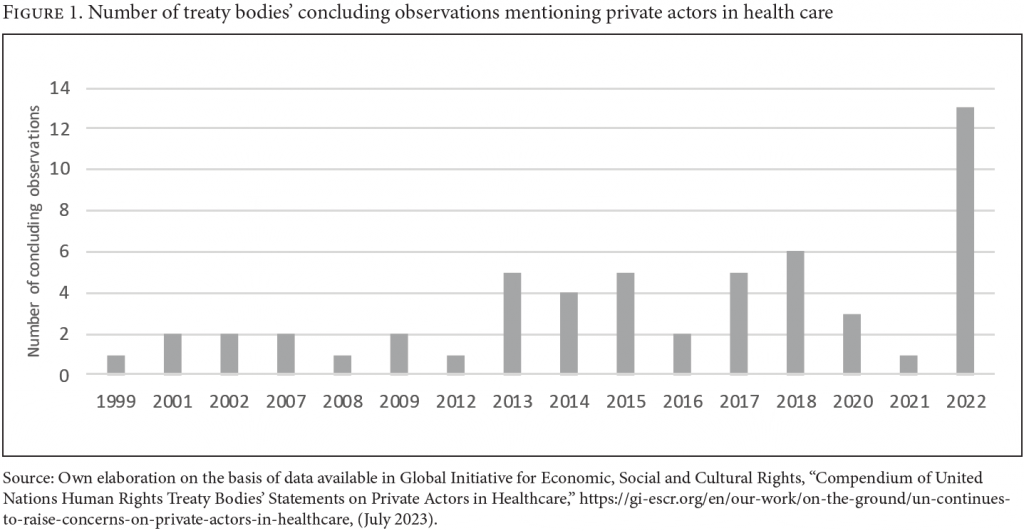
Overall, the number of concluding observations including language on private actors in health care has grown over time, as shown in Figure 1. In 2022, for example, there were 13 concluding observations that mention private actors in health care, which is more than the total number of mentions between 1999 and 2012.
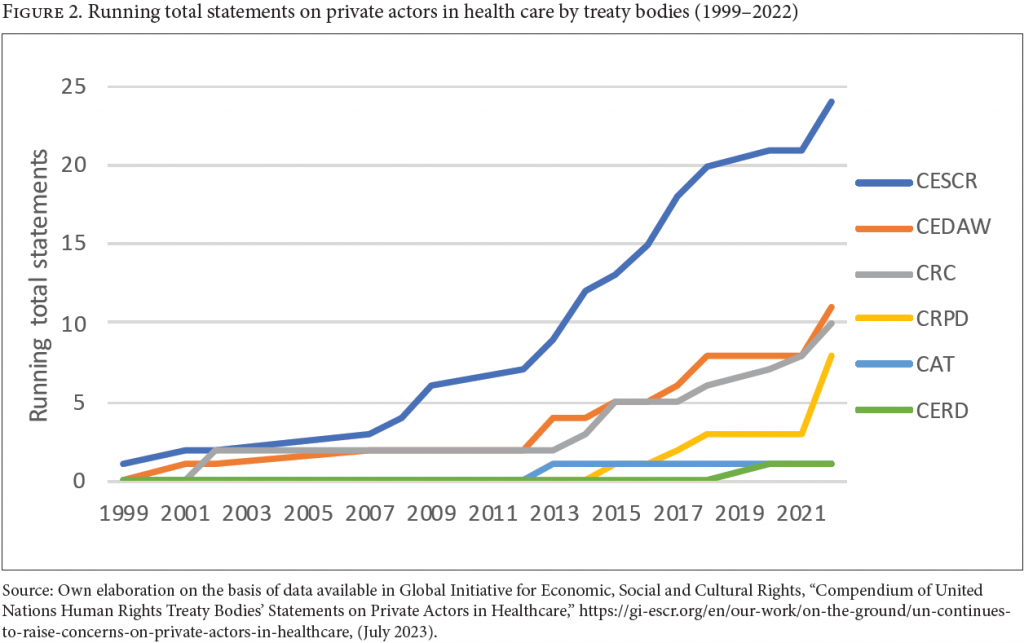
As shown in Figure 2, CESCR published the plurality of the concluding observations touching on private health care actors during 1999–2022, accounting for 24 of the 55 identified. However, other treaty bodies also increased their work on private health care actors between 2013 and 2022.
The concluding observations analyzed often refer to health care services in general, focusing on access to such services for the whole population or a specific group (e.g., women, persons with disabilities, children, or migrants). Only four focus on mental health care specifically, and nine on sexual and reproductive rights.
Concluding observations on nondiscrimination and equality
Of the 55 concluding observations in our sample, only 5 focus on vertical inequalities due to differences in wealth or income, while 29 mention inequality between groups on grounds such as gender, poverty, citizenship status, disability, and age.
With regard to such vertical inequalities, the CRC commented in a few cases that expensive private medical services might increase vertical inequalities among children, including recommending that Sri Lanka “combat … expensive private medical care, with a view to ensuring that each child has equal access to quality public health care.”[54] Likewise, it stated that it was “deeply concerned that children do not enjoy equal access to quality health care owing to the high cost of health care … , and in part to the domination of the health sector by the private sector” in the case of Lebanon.[55] In Vietnam, the CESCR expressed concern to the government about “the health protection divide in the society and … the adverse impact of privatization on the affordability of health care.”[56] These observations are linked to concerns regarding “economic and social status” as a basis for discrimination, which CESCR specifies in General Comment 20 on nondiscrimination in economic, social, and cultural rights.[57]
Treaty bodies also discussed differences between public and private health sectors as problematic per se. In 2015, CRC noted with concern “the difference in quality between public and private health-care services” in Chile.[58] Similarly, CESCR recommended that Ireland introduce “a common waiting list for treatment in publicly funded hospitals for privately and publicly insured patients.”[59] This resonates with Gillian MacNaughton’s definition of one-to-one equality, or positive equality, regardless of status, which can have positive impacts on reducing economic inequalities in accessing health care.[60]
Treaty bodies’ statements addressing horizontal inequality and private health care are more specific and frequent than those addressing vertical inequality. For instance, CESCR recommended that Croatia “carefully review the probable effects of its plans to privatize portions of the national health-care system on the most disadvantaged and marginalized sectors of society, including … those living in poverty.”[61]
Concluding observations on the availability, accessibility, acceptability, and quality of health care
Treaty bodies have frequently raised concerns regarding the effects that private health care actors have on the availability, accessibility, acceptability, and quality of health care—a series of standards commonly referred to as the AAAQ framework.[62] We found that 22 out of 55 statements apply the AAAQ framework’s language to analyze privatization of health care, either as a stand-alone challenge or as part of a broader range of concerns.
Among these observations, a few raise an economic inequality dimension. CESCR, for example, stated that “the Committee is also concerned that the gradual privatization of health care risks making it less accessible and affordable” in Poland and expressed concerns about “the adverse impact of privatization on the affordability of health care” in Vietnam, without referring to a specific marginalized group.[63] More commonly and directly, treaty bodies look at how privatization impacts the AAAQ framework in the context of specific groups. For instance, CEDAW raised concerns to Cyprus regarding “the insufficient availability of abortion services in public hospitals and the high cost of such services in private clinics.”[64]
Concluding observations on monitoring and regulating
Treaty bodies frequently emphasize states’ obligations to monitor and regulate private providers, with 21 out of 55 statements in our sample focusing entirely on this or otherwise including this aspect.
The practice of these treaty bodies is in line with the Guiding Principles on Business and Human Rights, which highlight states’ duty to protect human rights, including states’ obligations to provide remedies to victims of corporate abuse and adopt a “legal framework requiring business entities to exercise human rights due diligence,” so as to “identify, prevent and mitigate the risks of violations” of the right to health.[65]
In its 2008 concluding observations on India, for example, the CESCR recommended that the government “provide information on the measures to regulate the private health-care sector.”[66] CRC, for its part, recommended in 2015 that Brazil “establish a systematic monitoring mechanism for private care institutions, with a view to ensuring compliance with minimum quality standards.”[67] That same year, CEDAW noted with concern the “insufficient monitoring of private health-care providers” in Lebanon.[68]
Importantly, treaty bodies’ statements suggest that one way that states can monitor privatization plans is to conduct preemptive impact assessments.[69] For example, in 2009, CESCR recommended to Tajikistan that it “ensure that any public-private partnership has no negative impact on the affordability of medical services, particularly for the most disadvantaged persons.”[70]
Concluding observations on public budgets
In nine statements, treaty bodies address the linkage between available resources and private actors in health care, also addressing whether including private actors in health care is an appropriate way to fulfill the right to health. [71] For example, in 2014, CESCR recommended to Lebanon that the government “review whether the practice of contracting out the delivery of basic services to private actors constitutes an optimal use of available resources” and noted that it “finds it regrettable that the health budget is insufficient to provide adequate coverage for the entire population, thereby favoring the private provision of health-care services” in Guatemala.[72]
Treaty bodies have also started to analyze the balance between public and private health care from a budget perspective. For example, CEDAW recommended to India that it take measures to “balance the roles of public and private health providers in order to maximize resources and the reach of health services.”[73] However, treaty bodies have missed opportunities to unpack the economic inequality implications of such observations. A partial exception is when the CESCR noted that, in Korea, “disadvantaged and marginalized individuals do not have adequate access to medical services in privately run hospitals, which constitute 90 per cent of all hospitals,” and urged the state party to “increase expenditure for health care and to take all appropriate measures to ensure universal access to health care, at prices that are affordable to everyone.”[74]
Recent innovations from the African Commission on Human and Peoples’ Rights
The African Commission has recently made statements that both affirm a right to public health care services and go further than treaty bodies with respect to calling for more limited private actor involvement in health care.
In 2019, the African Commission issued a resolution affirming that African states are “the duty bearers for the protection and fulfillment of economic, social and cultural rights, in particular the rights to health and education without discrimination, for which quality public services are essential.”[75] Building on this resolution, in 2022, the commission issued its General Comment 7, acknowledging that “many commercial actors have pursued profit-seeking strategies that make services [like health care] more inaccessible to large segments of the population” and that “increasingly commercial interests in Africa are transforming social services into private commodities.”[76] The commission called on states to ensure “equal and democratic involvement of all members of the community or society in their design, organization, governance, financing, delivery and monitoring of social services, in the exclusive pursuit of the public interest.”[77] Moreover, the commission indicated that when “private social service providers are unable or unwilling to comply with standards and regulations,” states should require them to “cease their operations.”[78]
Conclusions and recommendations
The commercialization of health care systems still does not appear to have reached its zenith. The right to health framework under international law provides a powerful tool to address the adverse impacts that private health care actors, especially commercial ones, have on economic inequality and access to health care.
However, while this paper has highlighted several important normative developments, including a growing skepticism of the compatibility and compliance of private actors with the right to health framework and concrete guidelines, such as preemptive human rights impact assessments, there remain significant opportunities for these bodies to advance, formalize, and regularize inequality-reducing interpretations of states’ right to health obligations relating to the private sector. Below, we specify the gaps in treaty bodies’ analyses and suggest some potential ways to address them.
First, human rights institutions should use a more consistent typology when discussing private actors in health care, going beyond the binary public-private divide. Building on previous work, this paper presents a potential typology that could be used in this context, including by paying attention to whether the actor is financing, providing, or supplying medical goods for health care, and whether the actor is a commercial or noncommercial entity.
Second, treaty bodies should examine more comprehensively the ways through which commercial mechanisms lead to an inefficient allocation of resources within health systems. For example, they might promote over-investment in more-profitable medical services, such as expensive curative care, to the detriment of, and underinvestment in, preventative and other less-profitable services that benefit a larger population, such as prevention, family medicine, and urgent care.[79]
Third, treaty bodies should expand their work on public budgets, private actors, and economic inequality. For instance, while the CESCR recently expressed concerns “about reports that referrals from public health-care providers to private health-care providers increase the health-care costs borne by the State party” and recommended that the state of Palestine “strengthen its public health-care system with a view to lowering expenses linked to referrals to private health-care providers,” it missed an opportunity to elaborate on the economic inequality implications of this predicament.[80] It is also worth questioning why the state obligation to realize the right to health within the “maximum of its available resources” often focuses exclusively on financial resources instead of considering the full range of available or potentially available resources (human, financial, technological, infrastructural, etc.). Arguably, the resources available should also include those under the control of private actors who typically control access to a range of key infrastructural, human, technological, and financial resources at the direct expense of the availability of such resources in the public sector.
Finally, treaty bodies should expand their work on the link between private sector involvement in health care and vertical inequality. Most treaty body recommendations to states are still concentrated on the traditional human rights concern of horizontal inequalities, including discrimination on the basis of poverty. Very little consideration is undertaken of the dynamics between public and private health care provision as potentially problematic from an economic inequality point of view. Treaty bodies have an opportunity to investigate the systemic impacts of health care commercialization on a range of issues, including social solidarity; spatial and other inequalities; and the quality, price, and availability of health services and products. This could be analyzed in the context of highly unequal societies to produce findings on the impact of different health systems on such inequality.[81] This would assist in answering the central question about to what degree, if at all, economic segmentation in health care access, often associated with commercialization, is consistent with international human rights law.
Rossella De Falco, PhD, is program officer on the right to health at the Global Initiative for Economic, Social and Cultural Rights, Naples, Italy.
Timothy Fish Hodgson, LLM, is a senior legal adviser at the International Commission of Jurists, Johannesburg, South Africa.
Matt McConnell, JD, is a researcher at Human Rights Watch, San Francisco, United States.
A. Kayum Ahmed, PhD, is a special advisor on the right to health at Human Rights Watch, New York, United States.
Please address correspondence to Rossella De Falco. Email: rossella.defalco@phd.unipd.it.
Competing interests: None declared.
Copyright © 2023 De Falco, Hodgson, McConnell, and Ahmed. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] See, for example, World Health Organization, The World Health Report: Health Systems Financing, the Path to Universal Coverage (Geneva: World Health Organization, 2010); Human Rights Council, Report of the Special Rapporteur on Extreme Poverty and Human Rights, UN Doc. A/73/396 (2018), para. 12.
[2] See F. Toth, “Healthcare Policies over the Last 20 Years: Reforms and Counter-Reforms,” Health Policy 95/1 (2010); J. Ferris and E. Graddy, “A Contractual Framework for New Public Management Theory,” International Public Management Journal 1/2 (1998).
[3] S. Berkeley, World Development Report: Investing in Health (Washington, DC: World Bank Group, 1993).
[4] Global Initiative for Economic, Social and Cultural Rights, Healthcare Systems and the Commercialisation of Healthcare: A Glossary (Global Initiative for Economic, Social and Cultural Rights, 2023).
[5] R. Horton and S. Clark, “The Perils and Possibilities of the Private Health Sector,” Lancet 388 (2016); D. Montagu and C. Goodman, “Prohibit, Constrain, Encourage, or Purchase: How Should We Engage with the Private Health-Care Sector?,” Lancet 388 (2016).
[6] For instance, see International Finance Corporation, The Business of Health in Africa: Partnering with the Private Sector to Improve People’s Lives (Washington, DC: World Bank Group, 2006); K. Mignano, Creating an Inclusive Market for Eye Care (Washington, DC: World Bank Group, 2006); A. Maresso, R. Waitzberg, F. Tille, et al., “Engaging the Private Sector in Delivering Health Care and Goods: Governance Lessons from the COVID-19 Pandemic,” World Health Organization Policy Brief 56 (2023); S. Nwaka, “Drug Discovery and Beyond: The Role of Public-Private Partnerships in Improving Access to New Malaria Medicines,” Transactions of the Royal Society of Tropical Medicine and Hygiene 99 (2005).
[7] E. Rotarou and S. Dikaios, “Neoliberal Reforms in Health Systems and the Construction of Long-Lasting Inequalities in Health Care: A Case Study from Chile,” Health Policy 121/5 (2017); N. Gottlieb and. N. Davidovitch, “The Role of Public-Private Partnerships in Extending Public Healthcare Provision to Irregular Migrants: Stopgap or Foot in the Door?,” Israel Journal of Health Policy Research 9 (2020); O. D. Williams, K. C. Yung, and K. A. Grépin, “The Failure of Private Health Services: COVID-19 Induced Crises in Low- and Middle-Income Country (LMIC) Health Systems,” Global Public Health 16 (2021); S. Basu, J. Andrews, S. Kishore, et al., “Comparative Performance of Private and Public Healthcare Systems in Low- and Middle-Income Countries: A Systematic Review,” PLoS Medicine 9/6 (2012).
[8] M. Duggan, A. Gupta, E. Jackson, and Z. S. Templeton, “The Impact of Privatization: Evidence from the Hospital Sector,” NBER Working Papers Series (2023), https://www.nber.org/papers/w30824.
[9] C. E. Boone, P. J. Gertler, G. M. Barasa, et al., “Can a Private Sector Engagement Intervention That Prioritizes Pro-poor Strategies Improve Healthcare Access and Quality? A Randomized Field Experiment in Kenya,” Health Policy and Planning 38 (2023).
[10] J. Dorjdagva, E. Batbaatar, B. Dorjsuren, and J. Kauhanen, “Income-Related Inequalities in Health Care Utilization in Mongolia, 2007/2008–2012,” International Journal for Equity in Health 14 (2015); E. Saito, S. Gilmour, D. Yoneoka, et al., “Inequality and Inequity in Healthcare Utilization in Urban Nepal: A Cross-Sectional Observational Study,” Health Policy and Planning 31/7 (2016); B. Walsh, M. Silles, and C. O’Neill, “The Role of Private Medical Insurance in Socio-Economic Inequalities in Cancer Screening Uptake in Ireland,” Health Economics 21/10 (2012); T. Gordon, F. Booysen, and J. Mbonigaba, “Socio-economic Inequalities in the Multiple Dimensions of Access to Healthcare: The Case of South Africa,” BMC Public Health 20/289 (2020).
[11] See Lancet, “The Commercial Determinants of Health,” https://www.thelancet.com/series/commercial-determinants-health; see also World Health Organization, “Commercial Determinants of Health,” https://www.who.int/news-room/fact-sheets/detail/commercial-determinants-of-health.
[12] Center for Human Rights and Global Justice and Hakijami, Wrong Prescription: The Impact of Privatizing Healthcare in Kenya (New York: NYU, 2021); Global Initiative for Economic, Social and Cultural Rights and Justice Empowerment Initiative, The Failure of Commercialized Healthcare in Nigeria during the COVID-19 Pandemic: Discrimination and Inequality in the Enjoyment of the Right to Health (Global Initiative for Economic, Social and Cultural Rights, 2021); Human Rights Watch, In Sheep’s Clothing: United States’ Poorly Regulated Nonprofit Hospitals Undermine Health Care Access (New York: Human Rights Watch, 2023); Human Rights Watch, “If I’m Out of Insulin, I’m Going to Die” (New York: Human Rights Watch, 2022); SECTION27, The Heart of Private Healthcare (Johannesburg: SECTION27, 2017); SECTION27, Submission on the National Health Insurance Bill (Johannesburg: SECTION27, 2019); Initiative for Social and Economic Rights, Profiteering in a Pandemic (Initiative for Social and Economic Rights, 2022).
[13] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 12.
[14] CESCR, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000), para. 17.
[15] Human Rights Council, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN Doc. A/HRC/7/11 (2008), para. 42.
[16] Human Rights Council, Protect, Respect and Remedy: A Framework for Business and Human Rights; Report of the Special Representative of the Secretary-General on the Issue of Human Rights and Transnational Corporations and Other Business Enterprises, John Ruggie, UN Doc. A/HRC/8/5 (2008), paras. 15, 16.
[17] A. Nolan, “Privatization and Economic and Social Rights,” Human Rights Quarterly 40/4 (2018).
[18] Ibid.
[19] Office of the United Nations High Commissioner for Human Rights, “OHCHR Dashboard, Status of Ratification,” https://indicators.ohchr.org/; other health-related provisions include Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006), art. 25; Convention on the Rights of the Child, G.A. Res. 44/25 (1989), art. 24; International Convention on the Elimination of All Forms of Racial Discrimination, G.A. Res. 2106A (XX) (1965), art. 5; International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966), art. 6; P. Hunt, “The Human Right to the Highest Attainable Standard of Health: New Opportunities and Challenges,” Transactions of the Royal Society of Tropical Medicine and Hygiene 100/7 (2006).
[20] Human Rights Council, Report of the Special Rapporteur on Extreme Poverty and Human Rights, UN Doc. A/73/396 (2018), para. 4; see, for instance, on the rights to education and water, S. Aubry and D. Dorsi, “Towards a Human Rights Framework to Advance the Debate on the Role of Private Actors in Education,” Oxford Review of Education 42/5 (2016); K. Beiter, “Why Neoliberal Ideology, Privatisation, and Other Challenges Make a Reframing of the Right to Education in International Law Necessary,” International Journal of Human Rights (2022); B. M. Meier, G. L. Kayser, U. Q. Amjad, and J. Bartram, “Implementing an Evolving Human Right through Water and Sanitation Policy,” Water Policy 15/1 (2013).
[21] Human Rights Council, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, Anand Grover: Addendum, Mission to Viet Nam, UN Doc. A/HRC/20/15/Add.2 (2012), para. 12.
[22] Human Rights Council, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, Tlaleng Mofokeng, UN Doc. A/HRC/47/28 (2021), para. 109.
[23] A. Chapman, “The Impact of Reliance on Private Sector Health Services on the Right to Health,” Health and Human Rights Journal 16/1 (2014).
[24] E. Arenas Catalán, The Human Right to Health: Solidarity in the Era of Healthcare Commercialization (Cheltenham: Edward Elgar Publishing, 2021).
[25] A. Hallo de Wolf and B. Toebes, “Assessing Private Sector Involvement in Health Care and Universal Health Coverage in Light of the Right to Health,” Health and Human Rights Journal 18/2 (2016).
[26] B. Toebes, “The Right to Health and the Privatization of National Health Systems: A Case Study of the Netherlands,” Health and Human Rights Journal 9/1 (2006).
[27] S. Hawkes, J. Kreienkamp, and K. Buse, “The Future of Inter-Governmental Organization Partnerships for Health and Human Rights,” in B. M. Meier and L. O. Gostin (eds), Human Rights in Global Health: Rights-Based Governance for a Globalizing World (Oxford: Oxford Academic, 2018).
[28] See, for instance, A. Chapman, Global Health, Human Rights, and the Challenge of Neoliberal Policies (Cambridge: Cambridge University Press, 2016), ch. 6; United Nations General Assembly, Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, UN Doc. A/63/263 (2008); S. Gruskin and Z. Raad, “Are Drug Companies Living Up to Their Human Rights Responsibilities? Moving Toward Assessment,” PLoS Medicine 7/9 (2010).
[29] Global Health Law Consortium and International Commission of Jurists, Principles and Guidelines on Human Rights and Public Health Emergencies (2023), https://www.icj.org/wp-content/uploads/2023/05/PGs-on-Human-Rights-and-Public-Health-Emergencies-21-May-2023.pdf; see also R. De Falco, “Non-State Actors and Public Health Emergencies,” Harvard Bill of Health (November 2, 2023), https://blog.petrieflom.law.harvard.edu/2023/11/02/non-state-actors-and-public-health-emergencies/.
[30] For a similar methodology, although on a much larger dataset and with a wider scope, see B. M. Meier and Y. Kim, “Human Rights Accountability through Treaty Bodies: Examining Human Rights Treaty Monitoring for Water and Sanitation,” Duke Journal of Comparative and International Law 26 (2016).
[31] Global Initiative for Economic, Social and Cultural Rights, Compendium on United Nations Human Rights Treaty Bodies’ Statements on Private Actors in Healthcare (Global Initiative for Economic, Social and Cultural Rights, 2023).
[32] See J. Tobin and B. Damon, “The Right to Health and Health-Related Human Rights,” in L. O. Gostin and B. M. Meier (eds), Foundations of Global Health and Human Rights (New York: Oxford Academic, 2020); Tobes (2006, see note 26).
[33] World Health Organization, “Strengthening the Capacity of Governments to Constructively Engage the Private Sector in Providing Essential Health-Care Services,” WHA 63.27, Agenda Item 11.22 (2010), https://apps.who.int/iris/bitstream/handle/10665/3101/A63_R27-en.pdf?sequence=1&isAllowed=y.
[34] OECD, Eurostat, and World Health Organization, A System of Health Accounts: Revised Edition (Paris: OECD Publishing, 2017), p. 121.
[35] For an overview, see S. Languille, “Public-Private Partnerships in Education and Health in the Global South: A Literature Review,” Journal of International and Comparative Social Policy 33/2 (2017), p. 144.
[36] For other examples of classifications of health care systems, see K. Böhm, A. Schmid, R. Götze, et al., “Classifying OECD Healthcare Systems: A Deductive Approach,” TranState Working Papers 165 (2012); C. Bambra, “Health Status and the Worlds of Welfare,” Social Policy and Society 5/1 (2006).
[37] Global Initiative for Economic, Social and Cultural Rights (2023, see note 4).
[38] CESCR, General Comment No. 3, UN Doc. E/1991/23 (1990).
[39] CESCR (2000, see note 14), para. 36.
[40] Ibid.
[41] CESCR, General Comment No. 24, UN Doc. E/C.12/GC/24 (2017), para. 21.
[42] Ibid.
[43] Ibid., para. 22.
[44] Committee on the Rights of the Child (CRC), General Comment No. 16, UN Doc. CRC/C/GC/16 (2013).
[45] Committee on the Elimination of Racial Discrimination, General Recommendation No. 37 (First Draft), UN Doc. CERD/C/GC/37 (2023), para. 2(b)(v).
[46] Ibid., para. 53.
[47] United Nations General Assembly, Report by the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health: Racism and the Right to Health, UN Doc. A/77/197 (2022), para. 66.
[48] CESCR, General Comment No. 22, UN Doc. E/C.12/GC/22 (2016), para. 38.
[49] CESCR, Concluding Observations: Egypt, UN Doc. E/C.12/EGY/CO/2-4 (2013), para. 21.
[50] CESCR, Concluding Observations: El Salvador, UN Doc. E/C.12/SLV/CO/2 (2007), para. 24.
[51] CRC, Concluding Observations: Cyprus, UN Doc. CRC/C/CYP/CO/5-6 (2022), para. 30.
[52] CRC, Concluding Observations: Republic of Bahrain, UN Doc. CRC/C/15/Add.175 (2002), para. 13.
[53] Committee on the Elimination of Discrimination against Women (CEDAW), Concluding Observations: Türkiye, UN Doc. CEDAW/C/TUR/CO/8 (2022), para. 47.
[54] CRC, Concluding Observations: Sri Lanka, UN Doc. CRC/C/LKA/CO/5-6 (2018), para. 30(b).
[55] CRC, Concluding Observations: Lebanon, UN Doc. CRC/C/15/Add.169 (2002), para. 42.
[56] CESCR, Concluding Observations: Viet Nam, UN Doc. E/C.12/VNM/CO/2-4 (2014), para. 22.
[57] CESCR, General Comment No. 20, UN Doc. E/C.12/GC/20 (2009), para. 24.
[58] CRC, Concluding Observations: Chile, UN Doc. CRC/C/CHL/CO/4-5 (2015), para. 58.
[59] CESCR, Concluding Observations: Ireland, UN Doc. E/C.12/IRL/CO/3 (2015), para. 28.
[60] G. MacNaughton, “Untangling Equality and Non-Discrimination to Promote the Right to Health Care for All,” Health and Human Rights Journal 11/2 (2009), p. 54.
[61] CESCR, Concluding Observations: Croatia, UN Doc. E/C.12/1/Add.73 (2001), para. 34.
[62] CESCR (2000, see note 14), para. 12.
[63] CESCR, Concluding observations: Poland, E/C.12/POL/CO/5 (2009), para. 29; CESCR, Concluding Observations: Vietnam, UN Doc. E/C.12/VNM/CO/2-4 (2014), para. 22.
[64] CEDAW, Concluding Observations: Cyprus, UN Doc. CEDAW/C/CYP/CO/8 (2018), paras. 40–41.
[65] Human Rights Council, Protect, Respect and Remedy (2008, see note 16).
[66] CESCR, Concluding Observations: India, UN Doc. E/C.12/IND/CO/5 (2008), para. 78.
[67] CRC, Concluding Observations: Brazil, UN Doc. CRC/C/BRA/CO/2-4 (2015), para. 46.
[68] CEDAW, Concluding Observations: Lebanon, UN Doc. CEDAW/C/LBN/CO/4-5 (2015), paras. 41–42.
[69] See also CESCR, Concluding Observations: Croatia, UN Doc. E/C.12/1/Add.73 (2001), para. 34.
[70] CESCR, Concluding Observations: Tajikistan, UN Doc. E/C.12/TJK/CO/4 (2022), para. 52.
[71] CESCR (2000, see note 14).
[72] CESCR, Concluding Observations: Lebanon, UN Doc. E/C.12/LBN/CO/2 (2016), para. 11; CESCR, Concluding Observations: Guatemala, UN Doc. E/C.12/GTM/CO/3 (2014), para. 22.
[73] CEDAW, Concluding Observations: India, UN Doc. CEDAW/C/IND/CO/2-3 (2007), paras. 40–41.
[74] CESCR, Concluding Observations: Republic of Korea, UN Doc. E/C.12/KOR/CO/3 (2009), paras. 22–30.
[75] African Commission on Human and Peoples’ Rights, Resolution on States’ Obligation to Regulate Private Actors Involved in the Provision of Health and Education Services, Res. 420 (LXIV) (2019).
[76] African Commission on Human and People’s Rights, General Comment 7 State Obligations under the African Charter on Human and Peoples’ Rights in the Context of Private Provision of Social Services (2022); see also African Commission on Human and People’s Rights, Resolution on the Need to Develop Norms on States’ Obligations to Regulate Private Actors Involved in the Provision of Social Services, Res. 434, EXT.OS/XXVl1 (2020).
[77] African Commission on Human and Peoples’ Rights (2022, see note 76), para. 14.
[78] Ibid, para. 50.
[79] For example, see Global Initiative for Economic, Social and Cultural Rights, Italy’s Experience during COVID-19: The Limits of Privatisation in Healthcare (Global Initiative for Economic, Social and Cultural Rights, 2021).
[80] CESCR, Concluding Observations: Palestine, UN Doc. E/C.12/PSE/CO/1 (2023), paras. 63–64. Note that this concluding observation was found by the researchers, as it is not included in the GI-ESCR’s database, which was last updated in July 2023.
[81] CESCR (2009, see note 57).