Are Development Finance Institutions Meeting Their Human Rights Obligations in Health?
Vol 25/2, 2023, pp. 141-153 PDF
Anna Marriott, Anjela Taneja, and Linda Oduor-Noah
Abstract
The right to the highest attainable standard of health is a fundamental right of every human being without distinction as to race, religion, political belief, or economic or social condition.[1] Spent wisely, aid and other forms of government spending are essential for attaining this right, as well as driving development. However, taxpayer funds from high-income governments such as the UK, France, and Germany are increasingly being funneled through development finance institutions (DFIs) toward multi-million-dollar investments in for-profit health care corporations in low- and middle-income countries. This contributes to the corporatization and financialization of health care in these contexts and is implicated in profiteering and exploitation, the denial of treatment to those who cannot afford it, and a range of human rights abuses—all with little or no accountability. This paper examines the human rights obligations of a sample of European DFIs and the International Finance Corporation, drawing on the “availability, accessibility, acceptability, and quality” right to health framework. We find that this investment approach is not only limiting the realization of the fundamental right to health for all but also placing significant barriers to accessing quality, affordable health services.[2]
Introduction
The COVID-19 pandemic has increased economic inequality worldwide, with the poorest people hit hardest. As a result of the pandemic, poverty has increased for the first time in 25 years. The pandemic saw a new billionaire created every 30 hours, with their wealth rising more in the first 24 months of the crisis than in the preceding 23 years combined. Oxfam’s 2022 Commitment to Reducing Inequality Index shows that the world’s governments failed to mitigate this dangerous rise in inequality.[3] Concurrently, the health care market is projected to grow at an annual growth rate of 10.4% and is anticipated to reach a market volume of US$85.95 billion by 2027.[4] However, half the world’s population continues to be denied access to essential health care largely due to health care costs, and every second 60 people suffer catastrophic and impoverishing costs by having to pay out of pocket for health care.[5] According to the World Bank and World Health Organization, catastrophic health expenditure occurs when an individual spends more than 10% of their income on health-related expenses.[6]
Ensuring that everyone everywhere can realize their fundamental right to the highest attainable standard of health requires enabling people to access quality, affordable health services without financial hardship.[7] A substantial body of evidence exists showing that this cause is hampered by the growth of for-profit private health care providers, which exacerbates inequitable access to health care services, including by increasing the life-expectancy gap between rich and poor people.[8]
This paper examines the body of health care investments made by European development finance institutions (DFIs) and the World Bank Group’s private sector development arm, the International Finance Corporation (IFC). DFIs are wholly or majority government-owned institutions and, with the exception of the European Investment Bank, support only private sector development. They do so in health through grants, loans, guarantees, equity investment, lending through financial intermediaries, and blended instruments such as public-private partnerships.[9] Our analysis focuses on DFIs’ support to private health care providers (and not the entire health portfolio, which includes investments in the pharmaceutical and other sectors). We seek to understand the extent to which the realization of article 12 of the International Covenant on Economic, Social and Cultural Rights is compromised by this support.[10] This analysis is important given the growing focus of international development institutions, including the World Bank Group, on private sector solutions, especially the mobilization of private capital, to address development challenges, including in the delivery of public services.[11]
Methodology
This paper examines whether IFC and a sample of European DFIs are meeting their obligations regarding the realization of the right to health. We use the availability, accessibility, acceptability, and quality (AAAQ) framework to interrogate the human rights impact of their investments. To make this assessment, we draw on the findings of two Oxfam reports that were also written by us, the authors of this paper—namely, Sick Development and First, Do No Harm.[12] The following methodologies were used in the development of the two reports: For the Sick Development report, a comprehensive portfolio analysis of health investments into for-profit health companies across all low- and middle-income countries was compiled for four European DFIs from 2010 to 2022 using DFI websites, the websites of financial intermediaries, and broader online searches. The DFIs in question included the UK’s British International Investment (formerly Commonwealth Development Corporation); Germany’s Deutsche Investigations- und Entwicklungsgesellschaft; France’s Proparco; the European Investment Bank; and the World Bank Group’s IFC, where its financing for health overlapped with the others.
Data were cross-checked against IFC’s project portal to identify where IFC co-invests alongside the European DFIs in health care. Health care provider companies were further investigated for their affordability, accessibility, and any information related to patients’ rights via desk-based research (including company websites, academic literature, and media searches) and direct inquiries. The authors of the report also utilized Oxfam’s global network of staff, partners, and contacts to seek further information about health care providers where possible.[13] Primary research involving individual and focus group interviews with key stakeholders (including patients, carers, and community health workers) was also conducted in two states in India, the country with the highest concentration of DFI investments in health care. Second, for the First, Do No Harm report, data were collected from IFC’s project portals for all IFC health care advisory and investment (direct and indirect) projects in India between 1997 and 2022. This was followed up with desk-based research and interviews with key stakeholders.[14]
DFIs in health care: Human rights law
The ultimate obligation to protect and fulfill the right to health lies with the state.[15] However, the International Covenant on Economic, Social and Cultural Rights and the United Nations Guiding Principles on Business and Human Rights place clear expectations on businesses to abide by international treaties and covenants. For instance, the United Nations Guiding Principles on Business and Human Rights note that businesses should “avoid causing or contributing to adverse human rights consequences and addressing their impact when they occur” and should ensure access to remedy for human rights abuses.[16] Principles 11 to 17 set forth several expectations in this regard, requiring that businesses establish appropriate policies and processes to communicate their commitments and human rights expectations of entities that they engage with. Businesses also have ongoing obligations to undertake human rights due diligence “in order to identify, prevent, mitigate and account for how they address their adverse human rights impacts.”[17] Due diligence should be an ongoing exercise as a business evolves. DFIs have, however, previously been criticized for categorizing human rights only as part of a compliance or risk management agenda, as opposed to part of broader efforts to improve their positive impact, including the realization of human rights.[18] We view the spirit of the law as meaning that their obligations are much broader than mere risk assessment.
The obligations of private actors can be further understood in light of General Comment 14 of the United Nations Committee on Economic, Social and Cultural Rights, which states that “private business all have responsibilities regarding the realization of the right to health” and outlines the AAAQ framework, which provides a summary of essential elements of the right to health and is a useful basis for assessing actions toward the fulfillment of the right.[19] General Comment 14 also warns that “financing towards private actors can be a retrogressive step if it leads to negative outcomes, either in terms of substantive health outcomes or in terms of procedural obligations, such as transparency, participation, and accountability,” and that retrogressive measures are broadly impermissible.[20]
Similarly, General Comment 24 of the Committee on Economic, Social and Cultural Rights states that all business activities and entities, “whether they operate transnationally, or their activities are purely domestic, whether they are fully privately owned or State-owned, and regardless of their size, sector, location, ownership and structure” are also required to respect covenant rights.[21] Moreover, the general comment states that “private health-care providers should be prohibited from denying access to affordable and adequate services, treatments or information.”[22] General Comment 24 also grants states the latitude to impose regulations that ensure that private actors assume “public service obligations.” States may therefore adopt legislation or measures to ensure that private actors deliver on “equal access to health care and health-related services provided by third parties.”[23]
The onus is on the state to regulate private actors in order to ensure that these provisions are upheld, including ensuring that the provision of services by non-state actors is reviewed and aligned or adapted to prevailing needs. Private actors should also make efforts to assess their contributions to health inequality and social segregation more broadly. Given the vast sums of money that governments are channeling through DFIs into private health care provision, it is clear that DFIs have a responsibility to ensure that these companies abide by the AAAQ framework and, at a minimum, do no harm.
Other applicable principles are found in the United Nations Guiding Principles on Human Rights Impact Assessments of Trade and Investment Agreements, which outline the obligation of states—and, by extension, DFIs—to ensure that the necessary safeguard clauses are inserted into investment agreements to enable states and business entities to abide by their human rights obligations.[24] The principles further note that “business enterprises may be perceived as being ‘complicit’ in the acts of another party where, for example, they are seen to benefit from an abuse committed by that party.”[25] The principles set forth the expectation that businesses will undertake due diligence actions, including ex ante and ex post human rights impact assessments to assess “the potential impacts of the trade and investment agreement on human rights outcomes and on the capacity of States (and non-State actors, where relevant) to meet their human rights obligations, as well as on the capacity of individuals to enjoy their rights.”[26]
Sick development: Examining DFI investments in health care
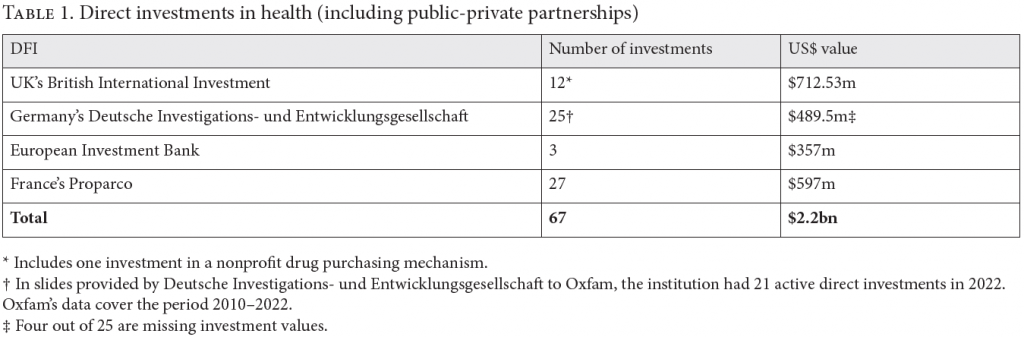
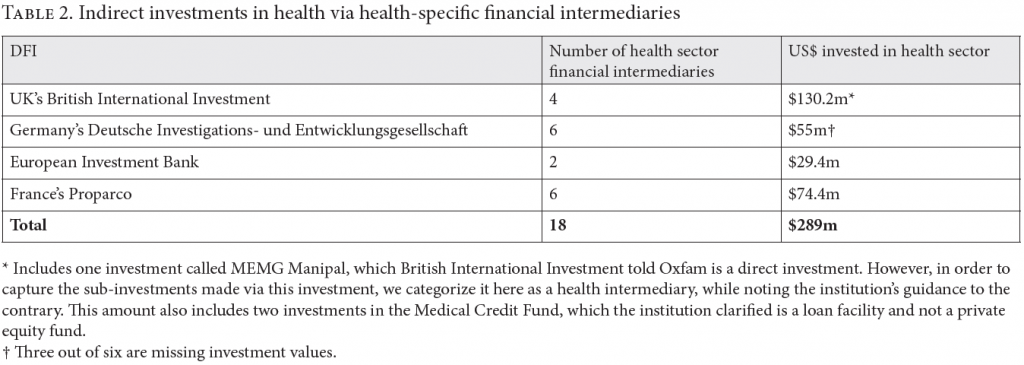
The authors of the two reports referenced in this paper found that 358 direct and indirect investments in private health companies in low- and middle-income countries were made by the four European DFIs between 2010 and 2022.[27] Together, these four DFIs invested at least US$2.4 billion directly in health and indirectly via health-specific financial intermediaries (see Tables 1 and 2). Eighty-one percent of their health investments were made via financial intermediaries, but the total value of these investments is impossible to calculate from the data available. Of the total investments, 56% were in for-profit hospitals or other private health care provider companies. Similarly, IFC has directly invested US$523 million in private health care companies in India since it began funding the sector in 1997.[28] A full review of IFC’s health portfolio was beyond the scope of the reports in question; however, widescale co-investment was identified by IFC (both directly and indirectly) in at least 42 of the same financial intermediaries and 112 of the same private health care company beneficiaries that are supported by the four European DFIs.
Do DFI investments violate the right to access health care services?
Accessibility to health has four overlapping dimensions: nondiscrimination, physical accessibility, economic accessibility, and information accessibility. Human rights law emphasizes protection for vulnerable groups, with conventions stating that “health facilities, goods and services must be accessible to all, especially the most vulnerable or marginalized sections of the population … without discrimination on any of the prohibited grounds.”[29] States are encouraged to adopt regulations that will address any discriminatory risk or actions, including by non-state entities, and to adopt “relatively low-cost targeted programmes and strategies to target and eliminate health-related discrimination, even in times of severe resource constraints.”[30] There is also an expectation that “health facilities, goods and services must be within safe physical reach for all sections of the population, especially vulnerable or marginalized groups … including in rural areas.”[31] A recent report by the Office of the United Nations High Commissioner for Human Rights, however, notes that while DFIs’ environmental and social safeguard policies have improved, insufficient attention is paid to the human rights of service users, including access to or affordability of services and the failure to address the limits of consumer protection policies in particular contexts.[32]
Given the above, we sought to understand the extent to which DFIs’ investments and support to private health care facilities enhance the availability and accessibility of health care.
Failure to improve access and availability of health care facilities in areas with the biggest health care gaps
While all but one of the five DFIs reviewed state that they aim to reach disadvantaged populations and to improve the affordability and quality of health care, the private health care facilities they fund are predominantly located in cities where private health care provision is available in greater volume than rural areas. In India, for example, IFC is investing in high-end urban hospitals and clinics concentrated in highly populated urban areas where profits can be generated. This is despite poor rural populations suffering the greatest access gaps. Only 4.2% of IFC direct-investee hospitals are in smaller habitations (known as Tier III cities), and of the 144 hospitals listed on the corporate websites of these chains, only one describes itself as being in a rural area.[33] Only 13.9% of the hospitals are in the 10 states ranked lowest in terms of the overall performance of the health system based on the Annual Health Index 2021.[34] One partial exception is the IFC investee Apollo, which expanded its operations to Tier III cities through its Apollo Clinics and Reach Hospitals. However, as evidenced by a report by the German development agency GIZ, high consultation fees mean its services remain unaffordable to average patients visiting these clinics.[35]
Health care services that are inaccessible and unaffordable
According to General Comment 14, economic accessibility requires that
health facilities, goods and services must be affordable for all. Payment for health-care services, as well as services related to the underlying determinants of health, has to be based on the principle of equity … Equity demands that poorer households should not be disproportionately burdened with health expenses as compared to richer households.[36]
Emphasis is also given to health care services not becoming less affordable or of lower quality in a bid to enhance profits. An increase in provision by private actors should not make health care services “conditional on the ability to pay.”[37] Additionally, emergency or life-saving treatment cannot be denied on the grounds of one’s inability to pay.
The evidence suggests that DFIs are falling short across all these requirements by directing development resources to hospitals that are unaffordable to patients on low incomes and that deny services, including emergency care, to those unable to pay. As one example, countries have committed to reducing maternal mortality as part of the Sustainable Development Goals, but so far there has been little improvement.[38] Research into the fees charged for maternity services by all of the European DFI-funded private hospitals, where these were available (in 49% of the 224 private health care facilities identified ), showed that the average starting cost of an uncomplicated vaginal birth amounts to over one year’s income for an average earner in the bottom 40%, and the cost of a cesarean birth amounts to over two years’ income for the same person. For an average earner in the bottom 10%, the starting cost for an uncomplicated vaginal birth at a DFI-funded private hospital rises to over nine years’ income, and over 16 years’ income for a cesarean birth.[39]
Data from Nigeria illustrate this further: Nigeria has the fourth-worst maternal mortality rate in the world, with approximately 90% of the poorest women giving birth on their own without a midwife or other medical professional.[40] Hygeia, a Nigerian-based health care company, has received at least 11 direct and indirect investments from Germany’s and France’s DFIs, the European Investment Bank, and IFC since 1999.[41] The company’s website states that it provides health care at “affordable rates,” but its hospitals are located in exclusive districts where childbirth costs start at the equivalent of nine months’ income for the poorest 50% of Nigerians.
Elsewhere, but similarly, at the height of the pandemic, when the need for accessible and affordable hospital care was most acute, several DFI-funded private hospitals either refused emergency treatment to COVID-19 patients or exploited the crisis by escalating charges. For example, the DFI-funded Maputo private hospital charged an upfront deposit of US$10,000 for COVID-19 treatment and care. In Uganda, Nakasero Hospital in Kampala reportedly charged US$1,900 per day for a COVID-19 bed in intensive care.[42] Lastly, in India, national legislation dictates that patients have a right to receive emergency medical care even if they cannot pay for it. The authors in First, Do No Harm, however, documented at least eight emergency cases where patients were reportedly turned away by DFI-funded CARE Hospitals and Narayana Health.[43]
False faith in health insurance mitigating gaps in access
DFIs often point to the potential role of health insurance in equalizing access to the private health care they fund. The World Bank Group, for example, argues that health insurance expands “affordable, quality health care and creates a mass market for lower-income populations” specifically.[44] The new strategy of the British DFI, British International Investment, also states that for all of the new private hospital investments it makes, it will ensure that a significant proportion of users are on government payment schemes.[45] This theory assumes that these schemes currently work for people living in poverty. In most low- and middle-income countries, however, these assumptions do not hold.[46] In India, for example, 80% of people lack government or private health insurance to cover regular and emergency medical spending.[47] Furthermore, merely having insurance does not guarantee the ability to benefit from it. Narayana Health and CARE Hospitals have both been DFI funded and are officially registered providers in the Chhattisgarh and Odisha government-funded health insurance schemes that aim to reduce the financial burden of accessing health care for poor and vulnerable groups.[48] Both hospitals are required to provide free health care to eligible members and their families, but patients interviewed in Sick Development were blocked from using their cards at both of these hospitals without justification. The patients suffered catastrophic financial consequences as a result.
For example, 73-year-old Hammond stated, “The staff told us not to bring the card because it was of no use here. They told me it was for survey purposes and was not used for treatment.” This led to Hammond spending 30% of his total pension income at CARE Hospitals—which is above the threshold deemed catastrophic by the World Health Organization.[49] A different patient, Robert, had to mortgage his family’s plot of land and take out three private loans to pay for tests and treatments associated with his heart surgery at CARE Hospitals that should have been covered by his government insurance card but was rejected. After repayments, Robert was left with just 1,300 rupees (US$16) per month to support himself and his family. Stakeholder and focus group interviews revealed that the denial and selective use of government insurance cards was commonplace at these DFI-funded hospitals, especially for tribal people and patients on low incomes.[50]
Inability to demonstrate improved access, especially for marginalized populations
DFIs claim that their health investments improve access to health services for patients.[51] However, they provide no supportive impact evidence. For example, after over 25 years of advisory and investment projects on health care in India, IFC has still not disclosed any evaluation or published development results or outcomes, nor has it shared any baseline data or anticipated impact frameworks.[52] As a result, it is not possible to carry out any objective assessment of whether or how women or marginalized communities benefit from or are impacted by its investment projects. In its own evaluations, the World Bank Group’s Independent Evaluation Group has highlighted the systemic challenges and issues with IFC’s health portfolio, stating that IFC does not adequately prioritize quality and equity when investing and monitoring impact.[53] Similarly, there was no disclosed evidence from the European DFIs of any comprehensive impact evaluation or any meaningful and substantiated impact data in relation to health care access for people on low incomes, or for women and girls.[54]
Are DFIs helping improve the acceptability and quality of health care?
The drive to maximize income and profit can increase the risk of unethical, exploitative, extractive, and, in some cases, dangerous and harmful behavior on the part of hospitals that lower both the acceptability and quality of care.[55] We therefore set out to assess the extent to which patients’ rights were being upheld in DFI-supported hospitals, especially given the weak regulatory contexts in which such investments are made.
Patients’ rights are rooted in the United Nations Universal Declaration of Human Rights and often find local expression through patients’ rights charters, laws, regulations, and other instruments that doctors and hospitals are bound by. Some DFIs have further domesticated these principles—for example, IFC provides a set of voluntary guidelines that investees can opt into in order to promote quality, patient safety, and ethics in service delivery known as the Ethical Principles in Health Care.[56] Despite these laws and guidelines, we find significant gaps in how these principles are enforced. For instance, in IFC’s case, the authors in First, Do No Harm could not identify a single project information window on the IFC portal that addresses the status of patients’ rights at its investee hospitals in India. There is also no information available to the public about IFC’s outreach to patients’ rights groups, health worker unions, or the public health movement.[57]
Our evidence shows that abuses within the DFI-funded private hospitals are widespread and that DFIs appear largely unresponsive to them, even in contexts where such practices frequently occur or receive widespread media attention. A large number of these alleged and confirmed abuses violate both international conventions and national laws. For example, in India, we found over 70 reported patients’ rights violations that have been adjudicated and whose convictions have been upheld by national regulators against IFC-supported corporate hospitals. The violations include overcharging, denial of health care, price rigging, fraud and financial conflict of interest, medical negligence, and refusal to provide free health care to patients living in poverty despite this being a condition under which free or subsidized land was allotted to these hospitals.[58] Some more detailed examples of the alleged and confirmed patients’ rights violations perpetrated by the DFI-funded private hospitals in question included the following:
- Refusal to treat patients or offer emergency treatment. In India, national legislation dictates that patients have a right to receive emergency medical care even if they cannot pay for it. However, the author in Sick Development documented at least eight emergency cases where patients were reportedly turned away by CARE Hospitals and Narayana Health.[59]
- Patient detentions and retention of the bodies of deceased patients due to unpaid hospital bills. We identified up to 37 cases of alleged and confirmed patient detentions (including babies and a secondary school student) at the DFI-funded Nairobi Women’s Hospital in Kenya. Many of the DFI investments in this hospital came a year after the hospital director had made public the hospital’s policy of detaining patients who could not pay.[60]
- Failure to obtain consent while undertaking medical procedures.[61]
- From a patients’ rights perspective, unrealistically high frequency of billing, unnecessary treatments, and unreasonable charges for basic items such as protective gloves and hand sanitizer.[62] In India, it was found that fees charged to patients who sought care at DFI-funded hospitals in our sample ranged from between three and a half months to 14 years’ worth of wages for an average earner. The authors in First, Do No Harm questioned the high cost of accessing treatment and medicines at DFI-funded hospitals in India: one medical and sales representative stated in response that the average markup on medicines at private hospitals was around 50% but could be more than five times the purchase cost. The Competition Commission of India is undertaking an inquiry into inflated drug pricing in three of the biggest corporate hospital chains in the country, including several that are financed by IFC. The commission’s four-year investigation has so far concluded that the hospital chains have been abusing their dominance in the market by overcharging patients for both services and medical products.[63]
Additionally and according to human rights law, including the Guiding Principles on Business and Human Rights, businesses are required to undertake human rights due diligence to “identify, prevent and mitigate the risks of violations of Covenant rights, to avoid such rights being abused, and to account for the negative impacts caused or contributed to by their decisions and operations and those of entities they control.”[64] In response, IFC has established performance standards and an environmental and social risk mitigation system.[65] This system requires IFC-supported hospitals to follow applicable standards. Compared to other DFIs, IFC’s environmental, social, and corporate governance frameworks are relatively mature, with the environmental and social risk assessment system having undergone several reviews.[66] It is therefore considered to be a benchmark or industry standard.
Yet, the above evidence shows that there are significant weaknesses therein that need to be tackled. For instance, all IFC investments in hospitals and clinics have an “environment and social review summary” information page in which environmental and social action plans should be listed. However, review of these pages for health care investments showed no updates on action plans, or information on levels of compliance. The actual risks identified and any “progress in practice” also remained largely undisclosed. Further, we were unable to ascertain whether appropriate actions had been taken by IFC to resolve any identified risks.[67] Lastly, in First, Do No Harm, the authors found that environmental and social risk assessments inadequately capture the potential negative impacts of profit-driven health care actors on the larger health care system, including the potential to undermine government health care capacity via brain drain or to drive up health care access inequality.
The evidence collected, together with the absence of disclosed data, is a clear indication of gaps in environmental and social risk systems, which highlights the dangerous inadequacy of due diligence, oversight, and monitoring mechanisms for DFI investments.
Does absence of effective remedy make DFIs party to ongoing rights abuses?
The right to redress and effective remedy for harm where violations have occurred is a core tenet of international human rights law.[68] It holds that business enterprises have a responsibility to ensure that individuals and communities who have experienced human rights violations as a result of their activities have access to remedy by providing for or cooperating in remedial action.[69] DFIs share this same responsibility and should not exit a project before remedy has been provided.[70]
The evidence strongly indicates inadequate DFI oversight and governance of their health care portfolios, which has increased the risk of harm, as well as a remedy gap, which has been observed by way of the following: Some of the DFIs in question, such as the UK’s British International Investment, lack independent grievance mechanisms; none of the interviewees who had experienced harm were aware of the DFI investments in the private hospitals concerned or of the grievance or accountability mechanisms available to them; and some DFIs, such as IFC, stand accused of failing to act even where non-compliance has been identified by their accountability mechanisms.[71] Human rights abuses and violations at DFI-funded hospitals are well documented, including in the press. However, none of the DFIs have publicly acknowledged these abuses and deficits prior to the outlined investigations, even in cases where their investee hospitals have been publicly held to account by a court of law. There is nothing that gives confidence that concrete and systematic scrutiny of investments is in place.
These shortcomings in accountability are discernible in relation to direct health care investments, but are further amplified for the majority of DFI health care investments because they are made indirectly via financial intermediaries.[72] Respondents—including patients, duty bearers, and community members—were found to be unaware of the role, responsibilities, and impact of financial intermediaries in the provision of their health care services and were also uninformed of any grievance or accountability mechanisms available to them and how to engage them.[73]
Conclusion
Our collective experience with the COVID-19 pandemic provided unfortunate truths and a stark reminder of the injustices and impacts of global health inequity on the right to health. In order to strengthen health systems, efforts must be ramped up to reduce these gaps. To do so, clear and substantive action will be needed to stem trends toward investments in for-profit health care that worsens health disparities, particularly in low-income countries. Governments are responsible for deploying development funds in a manner that will ensure that their investments enhance the accessibility, affordability, and quality of health care services, including via their development finance institutions. We find, however, that DFIs are failing to anticipate, prevent, or respond to the risks to health care equity and to patients’ rights presented by their investments in profit-seeking health care providers. The DFI model of investing in health care, especially via financial intermediaries, has proven dangerously flawed in upholding human rights in health care and incapable of delivering safe investments in contexts of inadequate government health care regulation.
On the basis of the evidence collected, we recommend that high-income governments and the World Bank Group not fund any future for-profit health care programs, projects, or providers, directly or indirectly, through DFIs unless and until the following steps are taken:
- Urgently commission an independent evaluation of existing and historic DFI health care funding, with a priority focus on the impact of DFIs on advancing universal health coverage, and the protection and promotion of patients’ rights.
- Require that DFIs provide demonstrable evidence of positive impact on advancing health equity and the protection of human rights.
- Ensure full transparency for all existing investments and advisory services, including all investments made through financial intermediaries, and fully monitor and disclose evidence on impact.
- Strengthen DFIs’ approach to human rights due diligence and ensure that independent accountability and grievance mechanisms are appropriately implemented.
- Take action to remedy any harms resulting from their investments, including violations of human and patients’ rights.
Human rights bodies, including the Human Rights Council, must be more cognizant of the risks described above and explicitly examine the impact that DFIs have on the realization of the right to health. They should:
- Strengthen the integration of patients’ rights within human rights frameworks, ensure adherence to these frameworks by multilateral and bilateral organizations, and develop guiding principles for corporate businesses active in direct patient services to protect against any human rights abuse.
- Review DFI operations in health and make recommendations to strengthen the impact of their investments on the right to health.
Acknowledgments
We thank Harry Bignell and Abha Jeurkar for their contributions to this paper.
Anna Marriott is public services policy manager for Oxfam GB and health policy lead for Oxfam International, Oxford, UK.
Anjela Taneja is public services and inequality lead for Oxfam International, Delhi, India.
Linda Oduor-Noah is health policy and advocacy advisor for the IFIs team at Oxfam International, Nairobi, Kenya.
Please address correspondence to Anna Marriott. Email: amarriott@oxfam.org.uk.
Competing interests: None declared.
Copyright © 2023 Marriott, Taneja, and Oduor-Noah. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Constitution of the World Health Organization (1946).
[2] World Health Organization, “Human Rights” (December 10, 2022), https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health.
[3] J. Walker, M. Martin, E. Seery, et al., The Commitment to Reducing Inequality Index 2022 (Oxfam and Development Finance International, 2022).
[4] Statista, “OTC Pharmaceuticals – Worldwide,” https://www.statista.com/outlook/emo/otc-pharmaceuticals/worldwide?currency=usd.
[5] A. Marriott, “Sick Development,” Oxfam Briefing Paper (June 2023); World Health Organization, Primary Health Care on the Road to Universal Health Coverage: 2019 Monitoring Report (Geneva: World Health Organization, 2019).
[6] M. G. Shrime, “Catastrophic Expenditure for Health: From Antiquity to Today,” World Bank Blogs (February 19, 2021), https://blogs.worldbank.org/opendata/catastrophic-expenditure-health-antiquity-today.
[7] Ibid.; World Health Organization (2022, see note 2).
[8] Marriott (2023, see note 5).
[9] Ibid.
[10] Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000).
[11] OECD, Private Finance Mobilised by Official Development Finance Interventions: Opportunities and Challenges to Increase Its Contribution towards the SDGs in Developing Countries (Paris: OECD Publishing, 2023); World Bank, “Ending Poverty on a Liveable Planet: Report to Governors on World Bank Evolution,” Development Committee (September 28, 2023), https://www.devcommittee.org/content/dam/sites/devcommittee/doc/documents/2023/Final%20Updated%20Evolution%20Paper%20DC2023-0003.pdf.
[12] Marriott (2023, see note 5); A. Taneja and A. Sarkar, First, Do No Harm (Delhi: Oxfam India, 2023).
[13] A. Marriott, Sick Development: Methodology Note (Oxford: Oxfam International, 2023).
[14] Taneja and Sarkar (see note 12).
[15] Committee on Economic, Social and Cultural Rights, General Comment No. 24, UN Doc. E/C.12/GC/24 (2017); Committee on Economic, Social and Cultural Rights (2000, see note 10).
[16] Office of the United Nations High Commissioner for Human Rights, Guiding Principles on Business and Human Rights (Geneva: Office of the United Nations High Commissioner for Human Rights, 2011), principles 29–31.
[17] Ibid., principle 17.
[18] Marriott (2023, see note 5).
[19] Committee on Economic, Social and Cultural Rights (2000, see note 10), para. 42.
[20] Ibid., paras. 32, 48.
[21] Committee on Economic, Social and Cultural Rights (2017, see note 15), para. 3.
[22] Ibid., para. 11.
[23] Ibid., para. 21.
[24] Human Rights Council, Report of the Special Rapporteur on the Right to Food, Olivier De Schutter: Guiding Principles on Human Rights Impact Assessments of Trade and Investment Agreements, UN Doc. A/HRC/19/59/Add.5 (2011); Committee on Economic, Social and Cultural Rights (2017, see note 15), paras. 15–17.
[25] Office of the United Nations High Commissioner for Human Rights (2011, see note 16).
[26] Human Rights Council (see note 24).
[27] Marriott (2023, see note 5).
[28] Ibid.; Taneja and Sarkar (see note 12).
[29] Committee on Economic, Social and Cultural Rights (2000, see note 10), para. 12(b).
[30] Ibid., para. 18; Committee on Economic, Social and Cultural Rights (2017, see note 15).
[31] Committee on Economic, Social and Cultural Rights (2000, see note 10).
[32] Office of the United Nations High Commissioner for Human Rights, Benchmarking Study of Development Finance Institutions’ Safeguard Policies (Geneva: Office of the United Nations High Commissioner for Human Rights, 2023).
[33] Taneja and Sarkar (see note 12).
[34] Ibid.
[35] R. Sengupta, Sustainable and Inclusive Innovations in Health Care Delivery: A Business Model Perspective (GIZ India and CII-ITC Centre of Excellence for Sustainable Development, 2013); Taneja and Sarkar (see note 12).
[36] Committee on Economic, Social and Cultural Rights (2000, see note 10).
[37] Committee on Economic, Social and Cultural Rights (2017, see note 15), para. 22.
[38] E. Suzuki, C. Kouame, and S. Mills, “Progress in Reducing Maternal Mortality Has Stagnated and We Are Not on Track to Achieve the SDG Target: New UN Report,” World Bank Blogs (February 22, 2023), https://blogs.worldbank.org/opendata/progress-reducing-maternal-mortality-has-stagnated-and-we-are-not-track-achieve-sdg-target.
[39] Marriott (2023, see note 5).
[40] Concern USA, “The 10 Worst Countries to Be a Mother” (May 4, 2022), https://concernusa.org/news/worst-countries-to-be-a-mother/; World Health Organization, “Health Equity Assessment Toolkit (HEAT),” https://whoequity.shinyapps.io/heat/.
[41] Marriott (2023, see note 5).
[42] E. Kiggundu, “20 Days Spent in ICU at IHK, Nakasero, Victoria, Case Hospitals Will Cost You Money Worth a House in Gayaza, Kira,” Nile Post (June 18, 2021), https://nilepost.co.ug/2021/06/18/20-days-spent-in-icu-at-ihk-nakasero-victoria-case-hospitals-will-cost-you-money-worth-a-house-in-gayaza-kira/; M. Afonso, “COVID-19: A Glance at Prices in Maputo Private Hospitals – Carta,” Club of Mozambique (February 1, 2021), https://clubofmozambique.com/news/covid-19-a-glance-at-prices-in-maputo-private-hospitals-carta-183402/.
[43] Marriott (2023, see note 5); Taneja and Sarkar (see note 12).
[44] World Bank, UHC in Africa: A Framework for Action (Washington, DC: World Bank, 2016); C. Averill and A. Marriott, “Universal Health Coverage: Why Health Insurance Schemes Are Leaving the Poor Behind,” Oxfam Briefing Paper (October 2013); Taneja and Sarkar (see note 12).
[45] British Investment International, Productive, Sustainable and Inclusive Investment: 2022–26 Technical Strategy (London: British Investment International, 2022).
[46] International Finance Corporation, “Public-Private Partnership Stories: India; Meghalaya Health Insurance” (2013), https://documents1.worldbank.org/curated/en/423401542223247768/pdf/132050-bri-public-pppstories-meghalaya-unversal.pdf; B. Khawaja and R. Riddell, “Stealth Privatization: Kenya’s Approach to Universal Health Coverage Is a Private Sector Giveaway,” Open Global Rights (May 20, 2022), https://www.openglobalrights.org/stealth-privatization-kenyas-approach-to-universal-health-coverage-is-a-private-sector-giveaway/?lang=English; Averill and Marriott (see note 44); Taneja and Sarkar (see note 12).
[47] “The Fortis Case Is No Exception—These Charts Show How Healthcare Costs Are Soaring in India,” Scroll (November 22, 2017), https://scroll.in/pulse/858849/the-fortis-case-is-no-exception-these-charts-show-how-healthcare-costs-are-soaring-in-india.
[48] Taneja and Sarkar (see note 12); Marriott (2023, see note 5).
[49] Shrime (see note 6).
[50] Marriott (2023, see note 5).
[51] Ibid.; Proparco. “Investments Driven by Their Contribution to Development in Southern Countries,” https://www.proparco.fr/en/investments-driven-their-contributiondevelopment-southern-countries; International Finance Corporation, “The Role of the Private Sector in Expanding Health Access to the Base of the Pyramid,” https://documents1.worldbank.org/curated/en/442501492766874363/pdf/114449-WP-IFC-HealthReport-PUBLIC.pdf; H. Wadge, R. Roy, A. Sripathy, et al., Evaluating the Impact of Private Providers on Health and Health Systems (London: Imperial College London, 2017); Investors for Health, https://www.investorsforhealth.com/.
[52] Taneja and Sarkar (see note 12).
[53] Ibid.; World Bank, World Bank Group Support to Health Services: Achievements and Challenges, Independent Evaluation Group (Washington, DC: World Bank, 2018).
[54] Marriott (2023, see note 5).
[55] S. Marathe, D. Kakade, S. Bhalerao, and K. Pawar, “Perils of the Commercialised Private Health Care Sector for Patients: Analysis of Patients’ Experiences from COVID-19 Pandemic in Maharashtra, India,” Journal of Health Management (2023); J. Ward, “Failed Market Approaches to Long-Term Care,” Social Europe Research Essay (May 2023); M. Duggan, A. Gupta, E. Jackson, and Z. S. Templeton, “The Impact of Privatization: Evidence from the Hospital Sector,” National Bureau of Economic Research, Working Paper 30824 (2023).
[56] Ethical Principles in Health Care, “About EPiHC,” https://www.epihc.org/about.
[57] Taneja and Sarkar (see note 12).
[58] Ibid.
[59] Marriott (2023, see note 5); Taneja and Sarkar (see note 12).
[60] Marriott (2023, see note 5).
[61] Ibid.; Taneja and Sarkar (see note 12).
[62] Taneja and Sarkar (see note 12).
[63] Marriott (2023, see note 5).
[64] Committee on Economic, Social and Cultural Rights (2017, see note 15), para. 16; Office of the United Nations High Commissioner for Human Rights (2011, see note 16), principle 22; Office of the United Nations High Commissioner for Human Rights, Remedy in Development Finance: Guidance and Practice (New York: Office of the United Nations High Commissioner for Human Rights, 2022).
[65] International Finance Corporation, “IFC’s Performance Standards on Environmental and Social Sustainability,” https://www.ifc.org/en/insights-reports/2012/ifc-performance-standards.
[66] Review Team, External Review of IFC/MIGA E&S Accountability, including CAO’s Role and Effectiveness Report and Recommendations (World Bank, June 2020); Compliance Advisor Ombudsman, Review of IFC’s Policy and Performance Standards on Social and Environmental Sustainability and Policy on Disclosure of Information (Washington, DC: Compliance Advisor/Ombudsman, 2010).
[67] Taneja and Sarkar (see note 12); B. Natkin, “Concerns over IFC’s Upcoming Performance Standards Review,” Bretton Woods Project (September 22, 2009), https://www.brettonwoodsproject.org/2009/09/art-565337/.
[68] United Nations General Assembly, Basic Principles and Guidelines on the Right to a Remedy and Reparation for Victims of Gross Violations of International Human Rights Law and Serious Violations of International Humanitarian Law, UN Doc. A/RES/60/147 (2006); Office of the United Nations High Commissioner for Human Rights (2022, see note 64).
[69] Office of the United Nations High Commissioner for Human Rights (2011, see note 16), principle 22; Office of the United Nations High Commissioner for Human Rights (2022, see note 64), principles 11, 28–31.
[70] Office of the United Nations High Commissioner for Human Rights (2011, see note 16), principle 22; Office of the United Nations High Commissioner for Human Rights (2022, see note 64).
[71] Marriott (2023, see note 5); Compliance Advisory Ombudsman, Insights on Remedy: The Remedy Gap; Lessons from CAO Compliance and Beyond (Washington, DC: Compliance Advisor Ombudsman, 2023).
[72] Marriott (2023, see note 5).
[73] Ibid.