Promoting Patient-Centered Health Care and Health Equity through Health Professionals’ Education in Rural Chiapas
Vol 25/1, 2023, pp. 119-131 PDF
Fátima Rodríguez-Cuevas, Jimena Maza-Colli, Mariana Montaño-Sosa, Martha De Lourdes Arrieta-Canales, Patricia Aristizabal-Hoyos, Zeus Aranda, and Hugo Flores-Navarro
Abstract
Since 2011, the nongovernmental organization Compañeros En Salud, as Partners In Health is known in Mexico, has worked in collaboration with the Mexican Ministry of Health to strengthen the health care system in the Fraylesca and Sierra Mariscal regions of Chiapas, Mexico. In response to the high proportion of abandoned and understaffed clinics in the area, Compañeros En Salud has developed a program to entice medical students from some of the top medical schools in Mexico to spend their “social service year” in these facilities, where they receive financial support, on-site clinical mentoring, supplies, clinical support tools, and training in global health and social medicine using a structural competency framework. The idea is to provide high-quality health care to a historically underserved population through a lens of health as a human right. Although other structurally competent global health curricula have been implemented worldwide, primarily in the Global North, the Compañeros En Salud model is unique in that it combines (1) the facilitation of theoretical lectures based on the Social Medicine Consortium’s definition of social medicine, (2) global health case discussion and context-reflective experiential simulations, and (3) exposure to patients who suffer the burden of structural injustice. In this paper, we describe the motivations behind the training model, its holistic approach, and the impact of this initiative after a decade of implementation.
Background
Global health institutions and researchers are mostly based in high-income countries, whereas most global health interventions take place in low- and middle-income countries.1 Consistent with this, global health curricula are often developed and delivered by Global North institutions and faculty, with 95% of masters of global health programs located in high-income countries, and are mostly available to high-income country candidates who can afford the high fees of these programs and have more facilities to physically access classes.2 This dynamic often results in global health programs that lack the insights of practitioners working in the world’s most underserved and marginalized settings in which global health practice takes place.3 In addition, many students in global health programs from high-income countries will not end up facing the global health challenges addressed in their studies in their future practice.
To counter the disconnect between underserved settings and global health curricula and between global health students and their future practice settings, there is a need for global health education initiatives to emerge from the Global South for practitioners in the Global South. Instead of considering the Global South as a whole, it is important to develop context-specific curricula that consider the social determinants of health. This can help make global health education more fruitful and eliminate colonial remnants in the global health field, shifting power to local ownership.
On top of this, building global health education initiatives that move away from the public health and human rights orthodoxies prevalent in most US institutions presents a great opportunity to adopt an integrative human rights approach in which civil and political rights, as well as social and economic rights, are given the relevance they deserve.4 In order to achieve “the right to the enjoyment of the highest attainable standard of physical and mental health,” first articulated in the 1946 Constitution of the World Health Organization, more is needed than just health facilities, even if they provide health care services that are of good quality and medically and culturally acceptable. These facilities must be physically and financially accessible to the population in an equitable manner and combined with public health interventions for the prevention and control of diseases. And importantly, the population must participate in health-related decision-making. To achieve this, the right to health should not be seen as an independent human right but as a right that is interdependent with other economic and social rights, such as the rights to work, water, food, housing, education, and nondiscrimination.5
Pioneering this approach, Compañeros En Salud (CES)—the sister organization of Partners In Health in Mexico, a nongovernmental organization that receives funds from individuals, corporate donors, and private foundations to provide care to the rural populations of Chiapas—decided to develop a human rights-based global health and social medicine curriculum (GHSMC) adapted to the local setting of the rural region in 2011. The program is complementary to the work that the organization initiated to support rural outpatient clinics in the Fraylesca and Sierra Mariscal regions of the state in defending health care as a human right, with the premise that quality care must be accessible to all and consider structural factors. Specifically, the curriculum aims to improve the structural competency of pasantes, medical students in their mandatory “social service year.” In Mexico, as in other countries in Latin America, graduates from medical and nursing school are required to provide one year of “social services” to the government in order to obtain their licenses. This program started in 1936 and has been the main government strategy for staffing clinics in rural places. These professionals are called pasantes, as they “pass by” a community for a one-year period. In the case of medical pasantes, there has been a long debate over whether they are doctors or medical students (as they are technically considered now).6 Either way, they are often the only providers in rural communities, with little supervision and a lack of ongoing training. Although structural competency is a necessary skill for any health professional, it is especially relevant for those working with underserved and marginalized populations to better understand the social determinants of patients’ health.7 Structural competency has been defined as the ability of health care workers to acknowledge the influence or effects of social, political, and economic structures in people getting sick, as well as being able to respond to them.8 According to Michael Harvey et al., structurally competent global health education includes the following elements:
(1) … the role of social structures in producing and maintaining health inequities globally, (2) … the ways that structural inequalities are naturalized within the field of global health, (3) … the impact of structures on the practice of global health, (4) … structural interventions for addressing global health inequities, and (5) … the concept of structural humility in the context of global health.9
Chiapas is one of the most deprived states in Mexico in terms of structural and intermediary social determinants of health.10 At the structural level, the average degree of education is only 7.8 years (versus 9.7 years at the national level), and 84.2% of the working population lacks access to social security, as most work as farmers in the informal sector.11 Aligned to this, according to the National Institute of Statistics, in 2020, 35.3% of the Chiapas population did not have any form of health insurance or social security.12 This population has historically been covered by the health services provided directly by the Ministry of Health, which contributed 38.3% of total health expenditure in Mexico in 2020.13 In terms of intermediary social determinants of health, 49.1% of the population lives in houses without chimneys and uses firewood or charcoal for cooking, and only 47.8% of the population is food secure. All of this is reflected in the state’s high multidimensional poverty rate of 75.5%.11
These structural factors and precarious living conditions of the population are behind most of the top 10 causes of morbidity in the state: acute respiratory infections, perinatal complications, intestinal infections, urinary tract infections, gastritis, intestinal amebiasis, salmonellosis, otitis, periodontal diseases, and candidiasis. There is also a high burden of noncommunicable diseases, including mental health disorders, although due to the lack of training of health professionals to identify these conditions and of accurate electronic medical records, these diseases are largely under-diagnosed.14 Moreover, the lack of timely access to quality care is related to a high burden of preventable deaths from these conditions and also from complications during pregnancy, childbirth, and postpartum.15 Although the current Mexican public health model covers the entire population outside the formal labor market for all health needs at no cost, this is not the case in practice. Chiapas has the lowest number of health specialists in the country.1 Also, many outpatient clinics in the rural areas of Mexico, where 51% of the population of Chiapas resides, have access only to a pasante completing his or her social service year or are simply neglected.17 This forces users to travel long distances to seek care, which they often cannot afford or which sometimes takes too long if emergency care is needed, as only 22% of the state’s roads are paved.18
As mentioned above, the challenging living conditions of the Chiapas rural population make understanding structural competency key for health care providers in the region. However, there are scarce educational curricula in Mexico that train health personnel in becoming structurally competent.19 Hence, Compañeros En Salud has decided to address this issue through the GHSMC, a curriculum that combines knowledge acquisition, case discussion, and exposure to patients in an iterative process that aims to prepare competent and sensitized professionals.20 Unlike other global health programs worldwide, this one was created—and is delivered and taught—by professionals working in the same rural underserved settings in their own practices, thus ensuring that the program responds to the needs of local health professionals and patients while also considering the global factors that underlie local health inequities and understanding the right to health as interdependent with other social and economic rights. In this paper, we discuss the Compañeros En Salud approach, its learnings to date, and impact of this initiative after a decade of implementation.
Origins of the curriculum
Chiapas’s current burden of disease and socioeconomic indicators require personnel with capacities superior to providing mere clinical care. However, in Mexico, the training of health professionals remains largely clinically focused, centering on the diagnosis of diseases and pharmacological and interventional treatments and generally overlooking how health problems may derive from determinants and social structures that harm marginalized populations.21
As mentioned earlier, completing the “social service year” is a requirement for obtaining a medical or nursing degree in Mexico.22 This requirement entails being sent to a rural area to provide care and often means being responsible for an entire community. Such a responsibility carries the risk that the skills required to respond to the demands of the population and the system exceed those learned during one’s medical education. Clinical staff often remember this year as a difficult period without support. Compañeros En Salud seeks to transform the traditional social service year model by complementing this year with a diploma in global health and social medicine in order to allow practitioners to provide culturally competent and dignified clinical care that embraces a human rights-based global health and social medicine approach.
There are multiple reasons why structural competencies are considered fundamental in the curriculum: (1) because the understanding of structural and social determinants is directly linked to treatment success (for example, in the early days of Partners In Health’s work in Haiti, the organization realized that malnourished tuberculosis patients would not improve with medicines alone but also needed food); (2) because the reality of the communities served clearly expresses the origin of their health conditions; and (3) because these conditions frequently subject providers to situations of frustration that prevent them from making informed decisions, both for the population and for themselves. For Compañeros En Salud, it is equally as important to have well-trained personnel who can offer quality services as it is to have personnel with skills that allow them to respond to the challenges that the immediate reality requires.
When it was originally created, the GHSMC was geared toward medical providers. However, the curriculum has since extended to nursing, obstetric-nursing, and midwifery providers. This extension has involved restructuring the previous curriculum and incorporating interprofessional training, which has enriched learning and collaboration among the professions. Moreover, as mentioned above, the curriculum is taught by instructors who were former pasantes. This allows instructors to share real-life examples of how theoretical concepts, context, and practice intersect, which maximizes the educational experience.
Early curriculum structure
When it was first rolled out, the GHSMC included two main modules: (1) the social medicine and global health module and (2) a clinical module that responded to the local burden of disease that included an introduction to locally developed clinical algorithms that not only were evidence-based but also included an adaptation of the clinical decision-making points according to the availability of resources, including medications and logistical barriers.23
The first module included a three- to four-hour lecture that introduced global health and social medicine terms and offered a practical portion where pasantes engaged in case discussions, debates, experiential simulations, and reflective sharing. Proximity to the social problems from the field boosted a better introduction of the theoretical terms being learned. This module later incorporated the five points of social medicine as defined by the Social Medicine Consortium, a consortium that includes universities, organizations, and health and non-health professionals aiming to reach health equity:
- Understanding and applying the social determinants of health, social epidemiology, and social science approaches to patient care,
- An advocacy and equity agenda that treats health as a human right,
- An approach that is both interdisciplinary and multi-sectoral across the health system,
- A deep understanding of local and global contexts ensuring that the local context informs and leads the global movement, and vice versa,
- Voice and vote of patient, families, and communities.24
This definition served as the basis of the lecture topics presented to pasantes until 2020, when the need to restructure the curriculum arose due to the interdisciplinary professionalization of pasantes, the growing need to preserve the clinical topics that were most relevant to the context, and the need to improving pasantes’ skills to better communicate with the people they serve and with their colleagues.
Current curriculum structure
To restructure the curriculum, in 2020, the course was evaluated qualitatively to determine the extent to which it was aligned with the local burden of diseases and the extent to which its topics promoted the development of structural competency. This process was carried out in seven stages: curriculum needs diagnosis, definition of modules and themes, integration of modules and themes, profile of speakers, didactics, evaluations, and follow-up strategy. Throughout the restructuring period, the perspectives of pasantes, the administrative team, and the field implementation team were considered. These individuals’ recommendations were solicited in relation to the perceived needs of their communities—an approach that, though not ideal, was still valuable as a starting point.
The restructuring was focused on the selection of topics, didactics, health care strategies, clinical follow-up, and responses to health services. Theoretical, conceptual and didactic aspects were considered to offer a comprehensive adjustment to the curriculum.
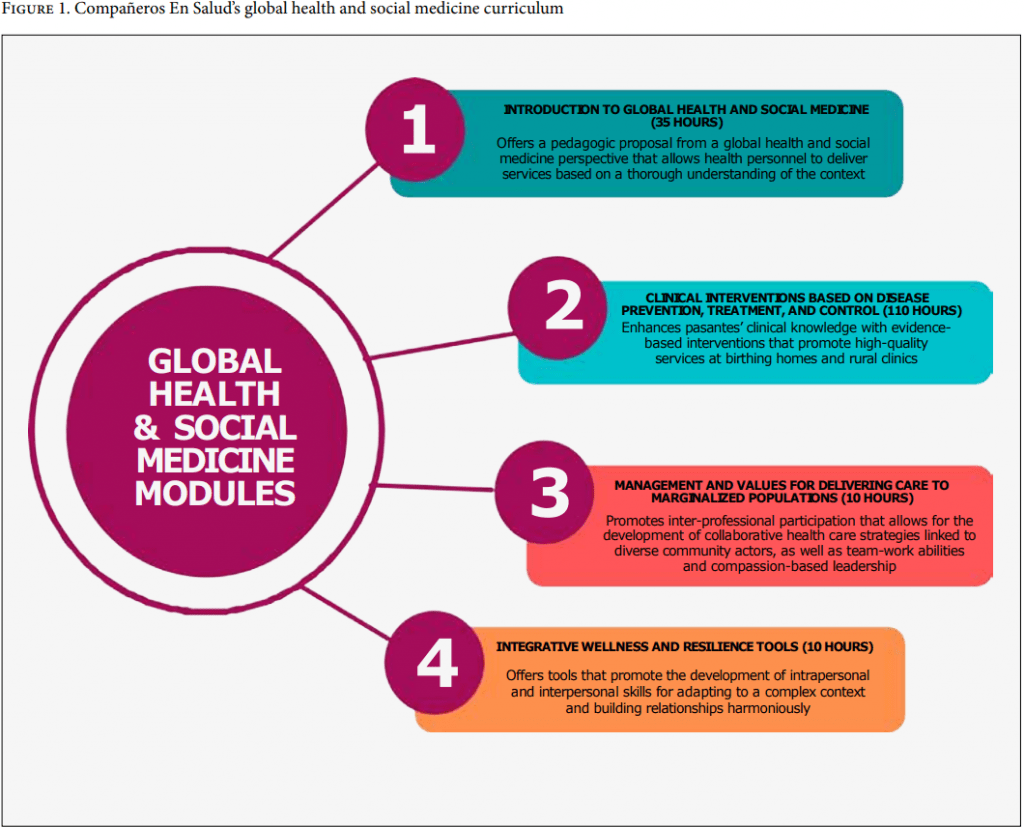
Finally, the curriculum was restructured to include four modules offered simultaneously, each with theoretical and practical components. The objective was to ensure the standardization of the clinical quality offered by pasantes, with a human rights-based global health approach and institutional values. The four modules are (1) introduction to global health and social medicine; (2) interventions focused on the prevention, treatment, and control of diseases, including sexual and reproductive health topics, ultrasound skills, and mental health topics; (3) management and values for the care of marginalized populations; and (4) tools for resilience and well-being (Figure 1). Before pasantes begin providing care in the community clinics, they are offered a 32-hour theoretical introduction that includes aspects of Compañeros En Salud’s context (values, protocols, and functions) and information on the organization’s alliances. Of particular interest are its alliances with the government, which allow pasantes to identify the regional and local response capacity.
The theoretical component consists of two monthly sessions of eight hours each day, which include content from the aforementioned modules. Among the topics of structural competence, the following stand out: relationship of global dynamics between countries and their impact on patients and on their local context, social approach to health and disease, social determinants of health, the human right to health, and the evolution of access to medicines.25 Moreover, in-person simulations such as the “poverty simulator” emulate the complex structural barriers in which people are embedded. The GHSMC also includes 480 practical hours in the field through community supervision and adaptation to the social context, which is expanded on later in this paper.
One of the key elements of the Compañeros En Salud curriculum is its emphasis on the daily practice of concepts from the four modules. For instance, for module 1, the practical training involves home visits, which allow students to understand the context in which people live, the challenges they face, and their family dynamics, and foster a closer bond between patients and providers. This module also encourages pasantes to follow up with patients who have been referred to specialized care in the capital city, which gives pasantes a better sense of what it means for a patient to miss a workday, make family arrangements, and navigate the health system in order to show up to a consultation in the city. For module 2, on-site clinical supervision promotes competency-based learning by allowing pasantes to model clinical skills such as ultrasound techniques and mental health consultations alongside a supervisor. For module 3, the use of interpersonal skills for communicating with the clinical team and with patients’ families offers pasantes the opportunity to engage in horizontal conversations among nurses, physicians, and community health workers and to learn how to allocate workloads or organize roles when attending to a patient’s emergency. For module 4, intrapersonal skills are taught for situations in which pasantes witness structural violence affecting their patients, which oftentimes may cause pasantes to experience feelings of helplessness, requiring them to strengthen their resiliency skills and structural competency for emotional processing. This process is often supported by pasantes’ supervisors in a genuine way, since they have experienced similar situations before.
Furthermore, the structural competencies are transversal in the modules; the proposed didactics include discussion spaces that allow pasantes to integrate knowledge from their own experiences and those of their peers. In addition to familiarity with concepts of structural competency, being an effective health care practitioner in culturally and ethnically diverse Mexico requires complementary skills such as cultural humility, clinical competency, active listening, and leadership. The GHSMC aims to develop these capacities as well and, by doing so, reduce barriers to accessing quality care.
Finally, as part of the curriculum’s evaluation of students, both qualitative and quantitative criteria are considered. The former are meant to assess the attitudes and soft skills expressed by trainees during care and teamwork. The latter are meant to assess students’ theoretical knowledge through written exams. Additionally, by the end of their service year, pasantes are invited to give a presentation that depicts their experiences, reflections, and learnings.
Complementary field supervision
The GHSMC learning process is complemented by field supervision in which pasantes are supported on site by a clinician who formerly worked as a pasante. This allows students to have a smoother immersion into the rural community and understanding of the social factors impacting them, as the supervisors have a thorough perspective of both the local burden of disease and the social issues affecting the community.
Generally, this supervision is performed by an obstetric-nurse or a medical supervisor who oversees all of the care delivery interventions and assures the quality of the delivery through feedback. The supervisors make improvements by observing and modeling during consultations with the pasantes, through systematic case discussion for collaborative clinical decision-making, and by offering evidence-based treatments that reconcile with the traditional-medicine remedies and that are appropriate to the patient’s particular reality. For example, supervisors teach obstetric-nursing students about childbirth care in the vertical position (squatting, sitting, or standing) and the use of the rebozo to facilitate labor, a “traditional midwifery practice of Aztec origin, which consists of using a scarf to perform different techniques in order to mobilize the pelvis and relax the muscles to favor the positioning of the fetus.”26 Obstetric-nursing pasantes also learn about the use of medicinal plants during pregnancy and labor and visit midwives in the region to exchange knowledge and ideas.
“Accompaniment” has been part of Partners In Health’s operative framework since the organization began working in Haiti and Peru. Currently, Compañeros En Salud has endeavored to incorporate the accompaniment model into many processes, such as accompanying patients to visit community health workers, accompanying the Ministry of Health in its efforts to strengthen the health system, and through the supportive supervision model. According to Paul Farmer, co-founder of Partners In Health, accompaniment is defined as follows:
To accompany someone is to go somewhere with him or her, to break bread together, to be present on a journey with a beginning and an end. There’s an element of mystery, of openness, of trust, in accompaniment. The companion, the accompagnateur, says: “I’ll go with you and support you on your journey wherever it leads; I’ll share your fate for a while. And by ‘a while,’ I don’t mean a little while.” Accompaniment is about sticking with a task until it’s deemed completed, not by the accompagnateur but by the person being accompanied.27
Pasantes receive oversight at the community rural clinics and at birthing centers, where their supervisors help them adapt to a new context, help them learn about the structural forces that make people get sick, and provide advice and manage expectations to allow pasantes to develop a structural competency lens of their own.
On-site supportive supervision for medical and nurse pasantes
At the community level, Compañeros En Salud provides comprehensive primary care for people living in or around any of the 10 communities with clinics that the organization supports along with the Ministry of Health. This care is provided through clinical teams that consist of a medical pasante, a nurse pasante, a graduated nurse, a health auxiliary, and community health workers. Each member of the team brings different skills to the table and provides distinct services so the clinics can deliver quality care to their users. A big part of the provision of quality services is an emphasis on training.
Such training is achieved by the continuous visits of clinical supervisors, registered nurses, and physicians with experience providing health services in rural areas, who spend a week every month in the communities in order to provide accompaniment, clinical mentorship, and management support to the clinical teams.
In some cases, supervisors also accompany pasantes during home visits to deliver medical care to where patients live. As mentioned earlier, this offers pasantes the opportunity to understand patients’ living conditions, their daily dynamics, and the social challenges they face. The supervisor role promotes understanding of the social medicine concepts that are studied in the theoretical lectures, emphasizing “proximity” to people’s context as a necessary element to convert the curriculum’s learnings into experiential practices, which ultimately leads to providing better health care.
Clinical supervisors also reinforce the topics from modules 1–3 by either intentionally talking about subjects reviewed that particular month or by seizing teaching opportunities when clinically or socially complicated cases arrive to the clinics. Having someone with more experience to guide the clinical teams through such occasions represents a valuable opportunity for meaningful learning and professional growth. “Bedside teaching” is essential for all health professionals, as it allows for real-time feedback and for the practice of clinical skills in a controlled environment. Therefore, it is essential to have both the theoretical sessions in the monthly training and the sessions of supportive supervision that help cement the acquired knowledge.
Supportive supervision for obstetric-nursing pasantes and midwifery pasantes
After a few years of working only with physicians, Compañeros En Salud expanded its operation to support a birthing center at the local hospital, Ángel Albino Corzo Hospital. This program was launched in collaboration with the National School of Obstetric Nursing and started receiving obstetric-nursing pasantes in 2016. The birthing center is one of the few places in Mexico where low-risk childbirth care is provided autonomously and independently by obstetric-nurses under the midwifery model. It is a place where midwifery and obstetric-nursing pasantes are trained in respectful, women-centered care. For instance, women’s preferences around birth delivery position and family accompaniment are prioritized, in contrast to the unjust status quo of most birthing experiences in Mexico, where birth delivery is centered not on the woman’s needs but on the needs of health personnel. Here, pasantes learn to guarantee the fulfillment of women’s sexual and reproductive rights. As direct care providers, the pasantes provide consultations, counseling on sexual and reproductive health issues, delivery care, postpartum care, and immediate newborn care.28
During the supervision, nursing pasantes are able to put into practice what they learn through the GHSMC since they are accompanied at all times by five obstetric-nurse supervisors and a professional midwife who graduated from the program in a previous cohort. For example, in the course they review the term “social construction of reality,” which shows that worldviews are built on ideas and practices determined by society, recognizing how people’s behavior may be determined by their subjective construction of reality.29 By recognizing that the woman, the traditional midwife, and they, as students, have a different but equally valid perspective of a particular situation, they learn to establish a respectful, collaborative, and harmonious plan for all parties. This stands in contrast to the usual practice whereby providers impose their perspectives without listening to the patient’s concerns or ideas.
Supervisors help nursing pasantes understand their patients’ context through clinical assessments that inquire about where patients live in order to know the distance they need to travel to reach the services, what their support network is like, and what particular concerns might help adapt management to their context. Moreover, nursing pasantes are encouraged to incorporate local words into their language to facilitate more effective communication.
Pasantes spend 10 months working at the birthing center. In order for them to understand firsthand the context of the vast majority of women who seek care there, they live for one month in a small rural community where medical pasantes are based, strengthening the care and counseling provided to pregnant women or women of reproductive age in that locality. During this time, they also make home visits to accompany women in coordination with the primary care clinic.
Pasantes also spend one month at the second-level referral hospital where women who cannot be attended at the birthing center are transferred to. This large hospital’s care is not centered on women’s preferences. The pasantes’ objectives at this site are to share the midwifery model of care and advocate for the rights of users.
Discussion
Since the 1970s, Latin American academics’ discussions have challenged the mainstream ideas emanating from renowned universities in the Global North on social medicine.30 For instance, by this decade, Argentinian physician César García had already started implementing community medicine, which would later evolve into social medicine.31 And from the 1980s onward, global health associations such as the Latin American Social Medicine Association and the Latin American Alliance for Global Health were created in order to disseminate social medicine work and combat the neoliberal health vision, among other things; further, global health modules were included in university curricula in Chile, Brazil, and Peru.32
In Mexico, Compañeros En Salud’s GHSMC is one of the few global health or social medicine programs in existence. What makes Compañeros En Salud’s approach unique is that it includes proximity to vulnerable populations and their social determinants of health.33 It offers direct experiences of care and relies on the teaching-learning process, which is loaded with daily experiences that the pasantes observe, actively participate in, and reflect on under the guidance of mentors. It stands out for its affordability, as it has no cost for enrolled students; its appropriateness, as it is designed by and for health practitioners in rural Chiapas; its focus on practice rather than research, policy, or diplomacy; its holistic approach, as it combines theoretical lectures, case solving, and field practice with supervision under an enabling environment; and its alignment with the human rights framework, considering health as an integral human right that includes the components of availability, accessibility, acceptability, and quality. At its core is the concept of human dignity, why every human being deserves the highest level of medical care available, and why anything less than that is essentially unethical, particularly in a society that systemically assigns lower standards of care to the poor.
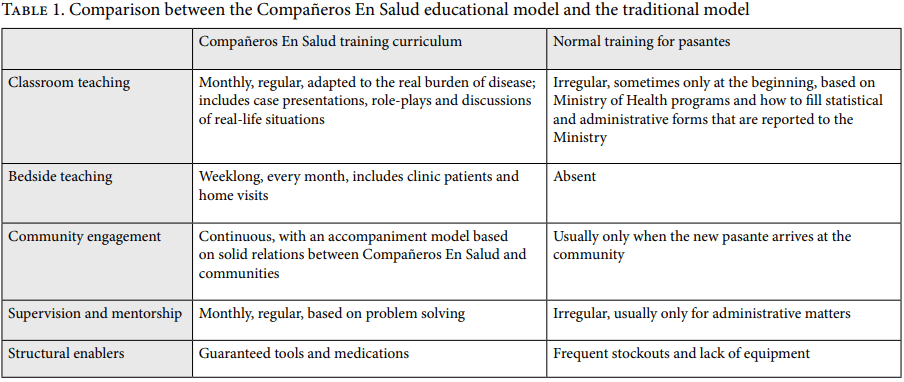
Therefore, the Compañeros En Salud curriculum not only teaches pasantes how to treat and follow up with patients but also provides the theoretical and practical tools to do so holistically. The approach would not be successful if pasantes were solely placed in remote clinics with thorough instruction and supportive supervision but without medicine or equipment to solve the health demands in front of them. Indeed, being the only provider in a remote village without access to medicine is one of the main reasons why pasantes in Mexico experience frustration during their social service year. Although ensuring supplies is not a formal part of the curriculum, it provides the environment that allows the instruction component to become a reality. All of these aspects of Compañeros En Salud’s educational model contrast with the traditional Mexican model, as summarized in Table 1.
The most outstanding outcome of this educational approach is that it can be transformational. Most of the current and past clinical management, nursing, obstetric-nursing, midwifery, and medical positions at Compañeros En Salud—including the organization’s current director—have been occupied by former pasantes. Ex-pasantes have also occupied positions such as director of Ángel Albino Corzo Hospital, home to the birthing center and the COVID-19 ward operated by Compañeros En Salud. This challenges the logic that the “best” pasantes will inevitably run away from rural communities and are interested only in prestigious hospitals in large cities. It shows that people respond to being able to see and create change around them and that instruction can be inspirational.
Many ex-pasantes have pursued higher education in global health and public health in renowned universities around the globe and have then come back to work at Compañeros En Salud. Others have pursued residency programs and worked in global health in Mexico and abroad, while others have continued to support the organization’s activities, such as its surgical campaigns. And yet others have started their own projects in their respective institutions. As of 2019, there were 114 graduates of the Compañeros En Salud program. By the time of their graduation, 60% had applied to work at Compañeros En Salud, 48% had worked or were working at Compañeros En Salud, 49% were working in a field related to global health, 33% had completed or were doing a medical residency, and 16% had completed or were pursuing a postgraduate degree related to humanitarian work.
Most importantly, these graduates continue to serve the poor and pursue a relentless battle against injustice in health delivery and outcomes. In the words of ex-pasante Miguel Hernández:
In the time I have spent at Partners In Health, I have begun to make the effort to listen before I speak. It is in the deepest silence that the voices of those we thought were silent begin to be heard. All that is needed is the will to pay attention to them and the courage to give them all that we can give.
Lessons learned
Providing a comprehensive curriculum designed to promote structural competency is not enough on its own. Theoretical knowledge without practical opportunities and support systems will always be insufficient to bring about real changes in care delivery. Accompanying the clinical teams has been crucial for applying the knowledge acquired in the classroom to daily practice. Adequate support systems and field supervision have been key to the success of this curriculum.
For professionals caring for rural and marginalized populations, structural competency in global health and social medicine should be integral to their training. We believe that the integration of such topics and the development of related skills should be an essential component of every program that instructs physicians and nurses. It is vital that such training be recognized and embraced by leading teaching institutions so it has the necessary validity and recognition in academic settings, which will allow this subject to grow and permeate all of the structures of care delivery. Well-grounded alliances with universities to obtain certificates and continuing medical education credits would help encourage health professionals to pursue further education in these areas.
The most important challenge has been to design an interdisciplinary curriculum that provides clinical knowledge specific to the needs of each cohort while also encouraging multidisciplinary collaborative work in the clinical environment. We have observed that in order to foster a collaborative teaching environment, we must actively promote nursing, obstetric nursing, and midwifery leadership in clinical teams, thereby breaking down traditional hierarchies in the medical field. Moreover, a remaining question is how to build a training curriculum and supervisory support that adapt to pasantes’ diverse needs and intra-and interpersonal skills.
In the future, Compañeros En Salud aspires to establish more proximity with the communities in order to understand their perspectives and, in turn, improve the services and care they receive. Last but not least, we have learned that the joint construction of a knowledge paradigm, agreed-upon intervention criteria, and the promotion of shared values between the medical team and the community generates the possibility of communicating through a language that helps unify the members of each cohort.
Conclusion
The impact of an education format that combines theory, practice, and the resources to link both falls into three domains. First, the social medicine approach is good for patients because it leads to better outcomes. Students are more aware of social barriers that influence patient behaviors such as missing an appointment or discontinuing a treatment course. They are able to understand the contexts and lived experiences of the patients, their working and housing conditions, their family and social dynamics, and so forth. This improves their diagnostic capabilities and provides them with tools to improve patients’ treatment completion, such as home visits.
Second, the model enables pasantes to do their job more effectively while reducing frustration originating from being alone and under-resourced in the face of difficult circumstances. It also creates spaces to promote community building with patients, colleagues, and supervisors.
Lastly, it is also good for organizations and society as a whole, as a comprehensive program such as this one can improve the retention of staff in rural areas, which is a problem even in high-income countries.
Compañeros En Salud is training multidisciplinary teams with the ability to understand and observe how health is not merely a biomedical issue but a complex social one that is specifically related to living conditions in the economic, environmental, cultural, and political spheres. This model expands the perspectives of students about what is possible regarding care provision in remote settings, which, in turn, helps these students become advocates to make health care a human rights reality.
Acknowledgments
We would like to thank Samuel M. DiChiara, research assistant at Compañeros En Salud Mexico, for proofreading this piece and for his valuable contributions, as well as Daniel Palazuelos, co-founder of Compañeros En Salud, for his input on the original global health and social medicine curriculum. Lastly, we are grateful to Paul Farmer, co-founder of Partners In Health, who left this world believing that every life is sustainable and who, through his teachings, fought relentlessly for health equity.
Fátima Rodríguez-Cuevas, MD, MSc, is the mental health coordinator at Compañeros En Salud/Partners In Health Mexico and an alumnus of the HEAL Initiative Fellowship, San Francisco, United States.
Jimena Maza-Colli, MD, is the clinical and teaching director at Compañeros En Salud/Partners In Health Mexico.
Mariana Montaño-Sosa, MD, is the sexual and reproductive health coordinator at Compañeros En Salud/Partners In Health Mexico and an alumnus of the HEAL Initiative Fellowship, San Francisco, United States.
Martha De Lourdes Arrieta-Canales, MD, MMSc-GHD, is the primary care coordinator at Compañeros En Salud/Partners In Health Mexico.
Patricia Aristizabal-Hoyos, RN, MA, PhD, is a professor at the Faculty of Higher Studies Iztacala at the National Autonomous University of Mexico, Mexico City, Mexico.
Zeus Aranda, MSc, MBA, is a research and impact intern at Compañeros En Salud/Partners In Health Mexico and a visiting scholar at El Colegio de la Frontera Sur, Chiapas, Mexico.
Hugo Flores-Navarro, MD, MGA, is a board member of Compañeros En Salud/Partners In Health Mexico and appointed faculty in the Division of Global Health Equity, Brigham and Women’s Hospital, Boston, United States.
Please address correspondence to Fátima Rodríguez-Cuevas. Email: fatimarodriguez@pih.org.
Competing interests: None declared.
Copyright © 2023 Rodríguez-Cuevas, Maza-Colli, Montaño-Sosa, De Lourdes Arrieta-Canales, Aristizabal-Hoyos, Aranda, and Flores-Navarro. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- O. F. Mogaka, J. Stewart, and E. Bukusi, “Why and for Whom Are We Decolonising Global Health?,” Lancet Global Health 9/10 (2021).
- A. Svadzian, N. Aguilera Vasquez, S. Abimbola, et al., “Global Health Degrees: At What Cost?,” BMJ Global Health 5/8 (2020).
- M. Mitra Chaudhuri, L. Mkumba, Y. Raveendran, et al., “Decolonising Global Health: Beyond ‘Reformative’ Roadmaps and towards Decolonial Thought,” BMJ Global Health 6/7 (2021).
- P. Farmer, “Challenging Orthodoxies: The Road ahead for Health and Human Rights,” Health and Human Rights Journal 10/1 (2013).
- World Health Organization, The Right to Health: Fact Sheet No. 32 (Geneva: World Health Organization, 2008).
- O. F. Ramírez de la Roche, A. Hamui Sutton, J. Reynaga Obregón, et al., “Condiciones de trabajo de los médicos pasantes mexicanos durante el servicio social,” Perfiles Educativos 34/138 (2012), p. 92.
- M. Harvey, J. Neff, K. R. Knight, et al., “Structural Competency and Global Health Education,” Global Public Health 17/3 (2022).
- J. Neff J, S. M. Holmes, K. R. Knight, et al., “Structural Competency: Curriculum for Medical Students, Residents, and Interprofessional Teams on the Structural Factors That Produce Health Disparities,” MedEdPORTAL 16 (2020).
- Harvey et al. (see note 7).
- O. Solar and A. Irwin, A Conceptual Framework for Action on the Social Determinants of Health, Social Determinants of Health Discussion Paper 2 (Geneva: World Health Organization, 2010).
- Consejo Nacional de Evaluación de la Política de Desarrollo Social, Informe de pobreza y evaluación Chiapas (Mexico City: Consejo Nacional de Evaluación de la Política de Desarrollo Social, 2020).
- Instituto Nacional de Estadística y Geografía, “Derechohabiencia” (2020), https://www.inegi.org.mx/temas/derechohabiencia/.
- Instituto Nacional de Estadística y Geografía, Cuenta satélite del sector salud México 2020 (Mexico City: Instituto Nacional de Estadística y Geografía, 2021).
- P. M. Newman, M. F. Franke, J. Arrieta, et al., “Community Health Workers Improve Disease Control and Medication Adherence among Patients with Diabetes and/or Hypertension in Chiapas, Mexico: An Observational Stepped-Wedge Study,” BMJ Global Health 3 (2018).
- C. E. Ruíz Hernández, Afectaciones en salud en poblaciones vulnerables (Mexico City: Consejo Nacional de Evaluación de la Política de Desarrollo Social, 2010).
- Instituto de Salud para el Bienestar, Modelo de salud para el bienestar dirigido a las personas sin seguridad social, basado en la atención primaria de salud, 2nd edition (Mexico City: Secretaría de Salud, 2020).
- Instituto Nacional de Estadística y Geografía, Censo de población y vivienda 2020 (Mexico City: Instituto Nacional de Estadística y Geografía, 2021); G. Nigenda, “Servicio social en medicina en México: Una reforma urgente y posible,” Salud Pública de México 55/5 (2013).
- S. Hernández García, M. Lelis Zaragoza, V. Islas Rivera, et al., Movilidad regional en Chiapas: Información básica para la planeación del transporte (Mexico City: Secretaría de Comunicaciones y Transportes Instituto Mexicano del Transporte, 2009).
- A. Van Wieren, L. Palazuelos, P. F. Elliott, et al., “Service, Training, Mentorship: First Report of an Innovative Education-Support Program to Revitalize Primary Care Social Service in Chiapas, Mexico,” Global Health Action 7/1 (2014).
- N. Beyeler, E. González-Pier, G. Alleyne, et al., “Salud global 2035: Implicaciones para México,” Salud Pública de México 57/5 (2015).
- J. L. Akaki Blancas and J. López Bárcena, “Formación de médicos especialistas en México,” Educación Médica 19/Suppl 1 (2018).
- R. León Bórquez, V. M. Lara Vélez, and L. F. Abreu Hernández, “Educación médica en México,” SciELO Analytics 21/3 (2021); G. E. Fajardo Dolci, J. Santacruz Varela, E. Lara Padilla, et al., “Características generales de la educación médica en México: Una mirada desde las escuelas de medicina,” Salud Pública de México 61/5 (2019); V. Smith Oka and M. K. Marshalla, “Crossing Bodily, Social, and Intimate Boundaries: How Class, Ethnic, and Gender Differences Are Reproduced in Medical Training in Mexico,” American Anthropologist 121/1 (2019).
- R. A. Borracci, A. I. Salazar, and E. B. Arribalzaga, “El futuro de la feminización de la medicina en Argentina,” SciELO España 21/3 (2018).
- Van Wieren et al. (see note 19).
- Social Medicine Consortium, “Program Details” (2022), http://www.socialmedicineconsortium.org; Consortium of Universities for Global Health, “Global Health Education Competencies Toolkit” (2022), https://www.cugh.org/online-tools/competencies-toolkit/.
- P. C. Rodríguez, P. B. Rollan, T. A. Alonso, et al., “Uso de la técnica de rebozo en el parto en la actualidad: Una revisión sistemática,” Revista Sanitaria de Investigación (2022), https://revistasanitariadeinvestigacion.com/uso-de-la-tecnica-de-rebozo-en-el-parto-en-la-actualidad-una-revision-sistematica/.
- P. Farmer, “Partners in Help: Assisting the Poor Over the Long Term,” Foreign Affairs (July 29, 2011), https://www.foreignaffairs.com/articles/haiti/2011-07-29/partners-help.
- M. Montaño, V. Maías, R. L. Molina, et al., “The Experience of Obstetric Nursing Students in an Innovative Maternal Care Programme in Chiapas, Mexico: A Qualitative Study,” Sexual and Reproductive Health Matters 30/1 (2022).
- University of Minnesota, Introduction to Sociology: Understanding and Changing the Social World (Minneapolis: University of Minnesota, 2016); A. Kleinman, “Four Social Theories for Global Health,” Lancet (2010).
- G. Solimano and L. Valdivia, “Global Health in Latin-American Academic Institutions: Towards a Distinctive Development and Identity,” Saúde e Sociedade 23/2 (2014).
- E. D. Nunes and J. C. García, “Social Medicine as Project and Endeavor,” Ciência e Saúde Coletiva 20/1 (2015).
- Solimano and Valdivia (see note 30); Asociación Latinoamericana de Medicina Social, “Estatutos” (October 8, 2015), https://www.alames.org/redes-tematicas-5/estatutos; Alianza Latinoamericana de Salud Global, “Nuestra Historia” (2022), http://alasag.org/historia/.
- Escuela de Salud Pública, “Programa Salud Global” (2022), http://saludpublica.uchile.cl/escuela/programas-academicos/salud-global; Instituto Tecnológico de Monterrey, “Diplomado Salud Global para Líderes” (2022), https://maestriasydiplomados.tec.mx/programas/salud-global-para-lideres-virtual; Universidad Peruana Cayetano Heredia, “Master of Public Health and Global Health” (2022), https://www.posgradoupch.pe/programa/maestria-en-salud-publica-y-salud-global/; Universidad Autónoma Metropolitana Unidad Xochimilco, “XXV Curso Monográfico de Medicina Social” (2022), https://www.xoc.uam.mx/evento-cursoMonografico.