From Apathy to Structural Competency and the Right to Health: An Institutional Ethnography of a Maternal and Child Wellness Center
Vol 25/1, 2023, pp. 23-38 PDF
Margaret Mary Downey and Ariana Thompson-Lastad
Abstract
Given the persistence of health inequities in the United States, scholars and health professionals alike have turned to the social determinants of health (SDH) framework to understand the overlapping factors that produce and shape these inequities. However, there is scant empirical literature on how frontline health and social service workers perceive and apply the SDH framework, or related movements such as the right to health, in their daily practice. Our study seeks to bridge this gap by applying constructs from the sociological imagination and structural competency (an emerging paradigm in health professions’ education) to understand the perspectives and experiences of social work case managers, community health workers, legal advocates, and mental health counselors at a maternal and child health center in a large US city. This frontline workforce displayed strong sociological imagination, elements of structural competency, and engagement with the principles of the right to health. Workers shared reflections on the SDH framework in ways that signaled promising opportunities for frontline workers to link with the global movement for the right to health. We offer a novel approach to understanding the relationships between frontline worker perspectives on and experiences with the SDH, sociological imagination, structural competency, and the right to health.
Introduction
Health inequities are avoidable and unjust differences in injury, disease, violence, and opportunities to experience optimal health. The social determinants of health (SDH) are a framework to understand the overlapping factors that produce these inequities. The World Health Organization defines the SDH as “the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.”[1] Frontline health and social service workers play a pivotal role in shaping what the SDH framework becomes in daily practice. However, most extant scholarship on SDH has undertheorized the role and experiences of the frontline workers who are tasked with bringing this framework to life.[2] Moreover, many of the SDH framework’s leading proponents have expressed concern over a narrow or reductive uptake of their original message around the conditions shaping health status, citing research and practice that emphasizes “lifestyle” factors such as exercise or diet at the expense of social and economic rights.[3] Understanding frontline workers’ perceptions of and experiences with the SDH framework is critical to addressing health inequities. Such understanding will inform the development of trainings, programs, policy, and organizing efforts toward the right to health. Frontline workers have a crucial role in the broader movement for the right to health because they witness, experience, and may be complicit in the embodiment of injustice.
Drawing from an institutional ethnography of frontline workers in a maternal and child wellness center in a large US city, the present study examines frontline workers’ perspectives on the etiology and origins of the interlocking health and social inequities within which they and their clients live. We seek to inform the development of structural competency (an emerging health education paradigm) and link to movements for a right to health. We first turn to C. Wright Mills’s concept of “sociological imagination” to understand workers’ perspectives on the SDH framework and its implementation.[4] This paper argues that sociological imagination is necessary for the development of structural competency and that structural competency and the right to health are complementary frameworks that should inform each other.
Finally, we examine how previous scholarship on social and economic rights and the right to health might inform frontline worker perspectives on health inequities. Those who fight against health inequities may vacillate between apathy, burnout, sociological imagination, and structural competency during their engagement with the right to health. We outline how health as a human right is an animating vision to guide the shift from apathy to structural competency. We also discuss how engaging with the framework of human rights offers workers opportunities for allyship and solidarity in a global project for the right to health.
Background
Maternal health inequities in the United States
Maternal health inequities are a persistent, devastating public health problem in the United States. Black and Indigenous people and low-income people face poorer outcomes across nearly every metric of pregnancy and postpartum health.[5] The United States has the highest maternal mortality rate among industrialized nations, with 23.8 deaths per 100,000 live births, most of which are classified as preventable.[6] Black and Native American women are three to four times more likely than white women to die due to pregnancy-related conditions.[7] Socioeconomic stratification alone cannot explain maternal health inequities.[8] Research shows that experiencing racism throughout the life course contributes to a “weathering” impact that produces physiological harms for women of color.[9] These inequities reflect the persistence of structural racism and other social and structural conditions that are often overlooked or obscured in health services.
Sociological imagination
Developed by Mills, sociological imagination is the capacity to step outside of one’s own routines, habits, and personal beliefs; understand individual experiences as part of a larger societal whole; and distinguish between “troubles” (personal dilemmas) and broader “issues.” Issues are public problems that may be experienced individually but are contingent on imbricated institutional, structural, and historical forces beyond the control of any one person. Mills argues that the absence of sociological imagination leads to individual and collective apathy, expressed as a dismissal of the social nature of crises and injustices. Apathy may mean pity or regret at the misfortune of others, yet failure to consider the social and structural causes of such misfortune. Individuals and whole societies may become accustomed to inequities even while agreeing that such inequities are objectionable.
We view Mills’s “apathy” as related to the concept of “burnout” so prominent in health and social service research.[10] Apathy and burnout are common challenges in the health professions and often surface in undervalued, under-resourced settings that serve populations most impacted by health inequities.[11] Expressed in part as a cynicism, detachment, and loss of commitment to improving patients’ lives, we understand burnout as potentially correlated with apathy as it emerges in health care settings. One may of course exist without the other. Burnout may persist among health care workers who are deeply invested in recognizing social determinants and detach because of their frustration when they feel they cannot solve social problems (i.e., burnout but no apathy). Other health care workers may be committed to and satisfied with individual patient care but be indifferent to inequities (i.e., apathy but no burnout). Recent scholarship on the sociological imagination suggests that approaching poor health outcomes as individually embodied and structurally determined may help prevent and address burnout among health care workers. Other research on burnout has identified the need for institutional and structural change to support the well-being of health care workers and their patients alike.[12]
Perspectives on the social determinants of health framework
A growing body of empirical literature examines the perspectives of physicians, nurses, and social workers on SDH.[13] This work suggests that knowledge of and support for engaging SDH in these professions is uneven, even for social workers (who ostensibly receive more training on social inequality than other health care workers).[14] There is little empirical research on other frontline worker perspectives (e.g., case managers, community health workers, health educators) on SDH. Our analysis attempts to fill these gaps in the literature.

Structural competency
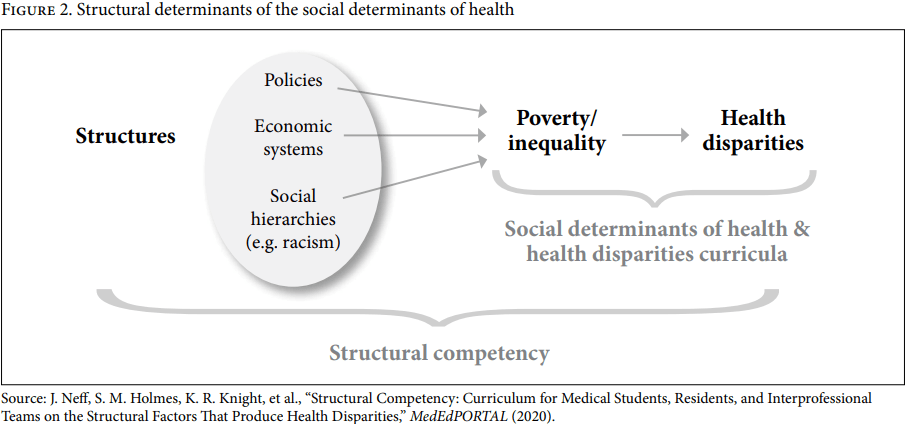
Despite decades of research on SDH, health care workers typically receive minimal training on upstream factors.[15] Physician-anthropologists Jonathan Metzl and Helena Hansen have developed structural competency as a medical education framework to train clinicians in understanding how social structures inequitably shape individual and community health, and in working to change these structures (for Metzl and Hansen, examples include zoning laws, economic systems, schools, and courts).[16] Structural competency includes five intersecting skill sets: (1) recognizing the structures that shape clinical interactions, (2) developing an extra-clinical language of structure, (3) rearticulating “cultural” presentations in structural terms, (4) observing and imagining structural intervention, and (5) developing structural humility.[17] As noted by Joshua Neff et al., structural competency emphasizes “the structural determinants of the social determinants of health.”[18] Thus, poverty (a well-documented social determinant of health) is determined by structures such as policies, economic systems, and social hierarchies (e.g., racism; see Figure 2). Since its inception, structural competency has been embraced by other professions, including nursing, social work, and psychology.[19]
Structural competency provides a framework to address health and health care inequities, as well as health care working conditions, by acting collectively—with colleagues, patients, and clients—to challenge unjust structures and institutions. Here, structural competency fills another important gap in the SDH framework. Though a powerful tool to describe patterns of inequity, the SDH framework does not define approaches to systems change or to combatting the “highly advanced knowledge of the biological impacts of lived environments alongside relatively undertheorized analyses of the environments themselves.”[20] A sociological imagination allows people to imagine systems, broadly speaking. Structural competency is about understanding inequity and actively working toward structural change. Structural competency rests on the foundation set by sociological imagination and SDH while moving health care into proactive, collaborative strategies at the sociopolitical level and providing more patient-centered care at the individual level.
The right to health
The right to health is among the basic social and economic rights and encompasses both the right to health and health care for individuals and the right to public health, broadly defined.[21] While other concepts discussed in this paper (sociological imagination, SDH, and structural competency) were developed primarily by scholars in the United States and Western Europe, leading advocates and scholars of the right to health are based in Africa, Latin America, and the Caribbean, among other regions.[22] Engaging in the right to health movement situates local work to eliminate health inequities amidst a broad, visionary, transnational project. It gives frontline workers something to work for as part of broader organizing with the right to health movement. In a US context, it also serves as a corrective to the imperialist nature of some human rights work, where the United States and Western Europe claim moral supremacy, police other societies, and ignore violations of social and economic rights in our own countries.[23] Moreover, the right to health is a legal term, codified in international law and United Nations conventions ratified by most countries. In this paper, we analyze data from an institutional ethnography using SDH, structural competency, and right to health frameworks together in order to illuminate the ways in which frontline workers enact these frameworks in their day-to-day practice. We argue that independently, each framework is necessary but insufficient to understand and further motivate frontline workers’ engagement with health inequities.
Methods
Institutional ethnography
This study employs institutional ethnography—a social science research method in which researchers embed with participants in their daily lives and routines.[24] Institutional ethnography investigates contested issues in the sociopolitical world through the experiences of participants whose lives are shaped by institutional forces (e.g., health policy, social welfare programs), such as frontline health and social service workers. Institutional ethnography was developed by sociologist Dorothy Smith to enhance social research’s capacity to deal with everyday problems, knowledge, and relationships that are mediated through institutions. It has been extensively used in health care settings to investigate how nurses, social workers, and other professionalized groups experience everyday life.[25] Compared to other ethnographic methods, institutional ethnography pays particular attention to the role of text, making it an ideal methodology to study health and social service settings that rely on written communication to create, share, and reinforce authoritative knowledge.
The field site
Family Center is a 30-year-old nonprofit maternal and child wellness center located in a large city on the US West Coast. Since its inception, it has addressed the social determinants of the region’s maternal and child health inequities. Family Center has approximately 100 full-time employees. More than half of its workers come from a community health worker program that recruits staff from former clients (primarily poor and working-class Latina and Black women). The current study began by focusing on the center’s Health Team, which frequently receives referrals from local biomedical institutions (e.g., hospitals and clinics) and addresses what are traditionally understood as biomedical issues, such as prenatal and postpartum health, contraceptive use, and breastfeeding initiation, as well as financial, housing, food, and educational needs for pregnant and postpartum clients.
Reflexivity
Both authors are facilitators with the Structural Competency Working Group, a network of health care workers, patients, and social scientists who provide workshops and consultation on structural competency to health care workers and trainees, policy makers, and health professions faculty. These roles enhance our ability to interpret the data in relation to structural competency’s core concepts. It also may lead us to overly rely on structural competency as an analytic frame. Our distinct professional backgrounds and shared personal backgrounds also influenced our analysis. In the tradition of critical, post-structuralist ethnographers, we harnessed our social positions as data.[26] We are both middle-class white women with experience working in safety-net health care institutions. The first author is a former birth and abortion doula, social worker, and social welfare scholar, while the second author has given birth to two children, has worked as a health educator in the US health care safety net for five years, and is a medical sociologist.
The first author, as the researcher in the field, negotiated several relationships with participants and the research questions. Her identity as a white, middle-class social worker who moved to the region during a wave of gentrification perpetuated by similarly situated professionals may have influenced the way participants spoke about the economic and racial inequities they observe and experience. Her identities may have positioned her as an outsider. On the other hand, her health and social service-related training may have positioned her as an insider, facilitating access within Family Center.
Data collection
The first author spent nine months (three days per week) conducting fieldwork at Family Center, primarily with the Health Team. Her activities included clerical work, escorting clients to appointments, and preparing tea and leading doula demonstrations for weekly prenatal education classes. She attended staff meetings and trainings weekly. She also attended activities outside of the agency, such as colloquia at the local teaching hospital where Family Center staff were invited to brainstorm strategies to address health inequities. Early on in participant observation, she noted that while text on the city’s Department of Public Health website and presentations used the SDH framework to describe Family Center’s work, no frontline workers ever used the framework to describe their work. In the case of the Department of Public Health, the Dahlgren and Whitehead model was cited to describe Family Center. Manuscripts in development from this ethnography report more specifically on findings from participant observation.
Participant observation assisted the researcher in identifying relevant participants for semi-structured interviews, specifically those who worked most closely with clients on health and health care needs. There were 21 interviewees in total, including social work case managers, health counselors, health educators, community health workers, and a member of Family Center’s executive team who supervised all frontline workers. All quotations are from semi-structured interviews. Throughout informal interviews during participant observation, all participants endorsed the relevance of social determinants in creating health and health care inequities, which motivated the interview protocol development. A purposive sampling approach was utilized. Interviews were conducted in person at a mutually agreed-on location within Family Center and averaged 67 minutes in length. Participants received a US$25 gift card. The semi-structured interview guide probed for daily routines and practices concerning client care, collaboration practices, and explanations for health inequities (e.g., “What makes it hard for some clients to be healthy?”). Perspectives on the SDH framework were elicited at the close of interviews, when participants were shown an image of Dahlgren and Whitehead’s model and asked to describe it. This model was chosen because the Department of Public Health uses it to describe Family Center’s work, because it is widely cited in public health literature generally, and because it balances breadth and depth with visual clarity.
Analysis
Data analyzed for this paper include field notes, interview transcripts, and agency documents. The first author repeatedly read all data to achieve immersion. She then combined a priori codes with codes derived inductively through a close reading of the transcripts.[27] She analyzed texts that were widely discussed within the center (e.g., annual reports) as well as those texts generated by authors or organizations outside of the center (e.g., Department of Housing policies). Next, directed and conventional content analysis were employed.[28]
For directed content analysis, terms from the Dahlgren and Whitehead model (e.g., “living and working conditions: housing”) served as a priori directed codes and were applied to interview transcripts, agency texts, and field notes. Conventional content analysis was applied to the same data to achieve inductive category development whereby data were read line by line to capture emergent codes and subcodes (e.g., “origin of health inequity”). Interview transcripts, agency documents, and field notes were then coded in Microsoft Word and subsequently organized into a matrix.[29] For subsequent analysis, both authors focused on data regarding work routines, reflections, and explanations for health inequities, alongside directed codes drawn from the Dahlgren and Whitehead model.
Results
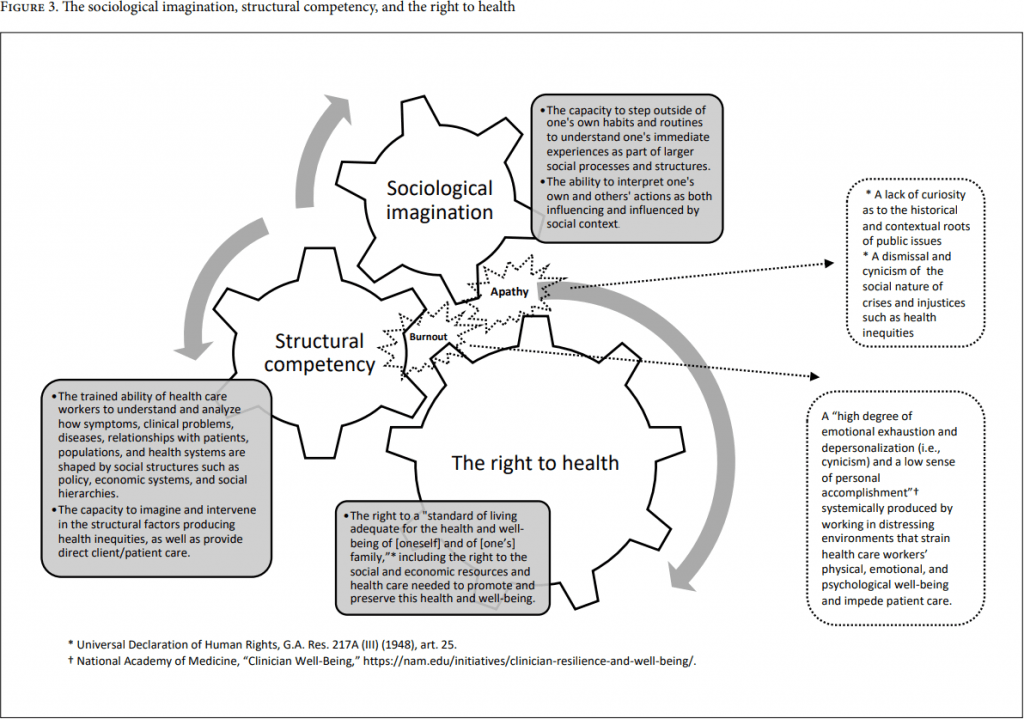
Below, we describe workers’ perspectives on health inequities and their reflections on applying the SDH framework. We outline how workers described their intervening in social factors beyond the individual level. Next, we describe a framework (Figure 3) to understand these results in terms of a relationship between possible frontline worker perspectives on apathy and burnout, SDH, sociological imagination, structural competency, and the right to health. Frontline workers articulate core tenets of the right to health movement, such as social and economic rights as necessary conditions for health equity, in ways that surface the complementary yet distinct aspects of structural competency and the right to health.
Figure 3 presents a novel approach to understanding the range of frontline worker responses to their own role vis-à-vis health inequities. Here, we seek to capture the dynamic, reinforcing, complementary nature of engaging with SDH via the sociological imagination, structural competency, and the right to health. We also seek to illustrate, based on frontline worker perspectives, how apathy and burnout can occur separately or together and can stall the positive momentum produced by developing sociological imagination, structural competency, and the movement for the right to health. In this approach, structural competency builds on the momentum of the sociological imagination, providing a guide for collective action and direct service provision that challenges narratives of blame, bias, and the individualization of social problems. The right to health, as a framework and movement, can motivate and guide engagement with structural competency, including structural interventions that are international, politically oriented, and based in global solidarity. Analyzing the right to health in structural competency trainings will enhance trainees’ ability to “observe and imagine structural interventions” (Metzl and Hansen’s fourth structural competency) at a global scale. For example, codifying the right to health in more and more international legal contexts could be an example of a structural intervention with implications beyond the United States. Understanding and acting on the right to health and being surrounded by other people who are motivated by the right to health may help prevent or mitigate individual burnout. As noted by participant Sam in her interview, working at Family Center helped her see (1) social forces as fundamental to individual and overall health and (2) her own and clients’ struggle as part of broad social processes rather than the result of their individual successes or failures. Given the identified connections between blame (self and client or patient), burnout, apathy, and health systems’ lack of engagement with SDH, Sam provides an example of how working in an environment that does engage with SDH can buffer against cynicism (present in both apathy and burnout).
Importantly, these are not fixed perspectives; structural competency is an ongoing process of development that should be approached with humility.[30] The approach outlined in Figure 3 offers several important considerations from frontline workers. First, frontline health care workers apply multiple lenses to the social world at once; therefore, frontline health and social services work requires consistent reflexivity. Second, these complementary concepts may be beneficial for the well-being of health care workers and patients/clients in the clinical encounter while also fostering engagement with broader social change.
Worker perspectives on SDH
All workers endorsed the social origins of health inequities. Workers differed in which aspects of the SDH framework they found most relevant to explaining health inequity. In this section, we describe how responses fall into three levels of SDH in the Dahlgren and Whitehead model: (1) social and community networks, (2) living and working conditions, and (3) general socioeconomic, cultural, and environmental conditions (see Figure 2). Workers also highlighted that these levels often overlap with or influence one another.
Social and community networks
Five workers endorsed social and community networks as the most relevant set of SDH. For example, Marilyn—a health educator and program coordinator—noted:
We know that [social and community networks are] the protective factor … to have parents who are supportive in social networks. There’s a limit to the amount that we are able to change in the overall social world and community that clients operate within, but, to the extent that we create new communities within our clients, there’s some level of an influence.
Similarly, Gabriella, a Health Team case manager, stated:
Healthy pregnancy is a lot of things. The first thing I think of is support and not being alone in the pregnancy. It’s nutrition. It is being housed. It is having the education to know how to take care of your body, access to prenatal care. I think the biggest part of having a healthy pregnancy is not being completely alone in that experience and being able to have a supportive community or at least supportive people.
These comments reflect and reinforce two fundamental dynamics observed during fieldwork. First, workers shift their practice focus and analysis between levels of SDH before landing on one. This suggests both helpful mutability in their understandings of SDH and opportunities for the agency to clarify its theory of change or approaches to the SDH framework. Second, social and community factors were more central to Family Center’s public-facing image than were other aspects of SDH endorsed by workers. Annual reports directed at funders, flyers advertising services directed at clients, and Family Center’s website all emphasize the agency’s health and social services as part of a mission to strengthen families and promote a positive experience of pregnancy and childbirth. In a context where overtly addressing the sociopolitical aspects of Family Center’s work—such as the provision of housing and health services for marginalized people—may be alienating to politicians, funders, partners, or clients, emphasizing social and community networks may be a strategy to ensure maximum public support.
Living and working conditions
Most workers interviewed (12 of 21) endorsed living and working conditions as the most important part of the SDH framework. Four of these defined housing as the most relevant aspect of this level. This may be due to the marked lack of affordable, safe housing in the city in which Family Center operates. Consider the response of Layla, a Health Team case manager. She connects housing access to income, linking this factor to the broader socioeconomic tier of the rainbow model (Figure 1) while focusing on housing as the most salient factor in Family Center’s work. She also connects housing, health, and human rights:
I think that it’s just really hard to stay healthy when you’re not housed. So, I think housing is a human right, and I think that really, if we want a healthy society, we need everyone inside. And so being able to be housed is the biggest barrier. And the barriers to being housed, a lot of times, is income. Where we live it is extremely difficult to find market-rate housing that a client or that any person can afford who is not making an upper-level salary.
Michael, another health case manager, also brought up housing. He immediately connected housing (and another living and working conditions factor, water and sanitation) to unemployment:
If you’re unemployed, you’re not going to have access necessarily to sanitation and water because you’re not going to have a house over you, a roof over you … so it’s almost like the unemployment leads you to this [points to water and sanitation], and the work environment leads you to this [points to housing].
Michael’s response is also an example of how workers understand the interaction of social determinants.
General socioeconomic, cultural, and environmental conditions
Three workers and the manager described the broadest level of the SDH framework—general socioeconomic, cultural, and environmental conditions—as the most relevant. This level includes a range of concepts, including economic systems and distributions of wealth and resources, norms and values, and governance structures.[31] Thus, some factors included in this level overlap with definitions of the “structural determinants of the social determinants of health.” Anne, a health educator, endorsed socioeconomic conditions as the main driver of health inequity while also aligning with structural competency’s “structural determinants of the social determinants of health” concept.
Well, we look at the government that we have now, and we know that we are a capitalist society, that we have a percent of the population tak[ing] 90% of the money, of what we make here, so when there’s that much of a disparity with income there’s always going to be people at the lower echelon, and the middle class is getting shrunk, so you get a few more richer but a lot more poorer. We could have a classless system, but we don’t.
Andrea, a housing case manager, noted policy as the most important aspect of the socioeconomic tier: “I’m just thinking of policy. That’s really going to make or break a community, I feel like, which is hard to explain. Just because of the people in power that have so much of a say for communities that they know nothing about.” Similarly, Mayra, the supervisor and manager, described policy as a specific expression of “general socioeconomic conditions” in action:
We continue to have practices in place or limiting resources in a way that automatically excludes certain populations … I think for the Department of Housing in particular, it’s very important that there be more individuals on their staff that reflect the population that they serve and or have lived experience with, having experienced homelessness or housing insecurity. That’s not currently the case, and so it makes for policy that sometimes can feel nonsensical to those that are experiencing homelessness or housing insecurity because the people who are making the policies don’t necessarily understand the realities of what it means to actually go through it.
Other workers described a broad social process of who is valued and who is not. For example, Sarah, a health case manager, connected wealth inequity to social norms as opposed to the presence or absence of income or access to employment:
It [the socioeconomic tier] is so important because, well, in the US, maternal mortality is … fairly high, and similarly with infant mortality. Being able to have a healthy pregnancy and a healthy birth is something that our society doesn’t throw all its resources at like some other societies, and it’s so segregated by wealth.
Here, wealth inequity is understood to be a driver of healthy pregnancy and birth. Distinct from individual-level income or employment status, which other workers described as part of living and working conditions, wealth segregation is understood to be a wider issue of socioeconomic, cultural, and environmental conditions. Notably, Sarah (who is white) does not mention racism, which is a main driver of maternal and infant mortality in the United States. This gap in Sarah’s response may demonstrate that some frontline workers apply their analysis of the broader level of the SDH framework unevenly.
Innovations on the SDH framework
Three respondents proposed, unprompted, changes to the Dahlgren and Whitehead model, suggesting that frontline workers have knowledge to contribute to the development of the SDH framework or that the SDH framework can be adapted as part of workforce development. They also prefigured a key aspect of structural competency—namely, that structures persist upstream of the top tier of the Dahlgren and Whitehead model’s “socioeconomic, cultural, and environmental conditions.” Jessica, a case manager, responded to the model in terms of its limitations. She found the framework useful but, as presented, too static to capture the complexity of social forces that she considered relevant to health inequity:
I think what stands out to me about this is that there is no active blame, it’s not calling out the actual structures. It’s just saying like “housing, health care, water, and sanitation.” Like “socioeconomic, cultural, and environmental conditions” are such a general blameless term as opposed to like oppressive structures that actively hold people down. What if those were, like, in this beautiful rainbow? I think a lot of social determinants models can remove blame and make it sound like it’s like this, yeah, it’s just listing things. I like how it moves inward toward the individuals, but there is no mention of racism or interpersonal violence or anything like that, capitalism, white supremacy … This is a great “101.”
Marilyn, a health educator, shared that she would add a level between the Dahlgren and Whitehead living and working conditions tier and its general socioeconomic tier to describe her clients’ experiences. She invoked core elements of the right to health by questioning the inevitability of health inequities and framing clients’ health issues in terms of social systems of valuation or devaluation of communities who live in poverty:
I think that a lot of the really big things that our clients are up against fit in between the outer and the second to outer category, in the intersection between how do we view poverty, how do we really think about that as a society, and how do we think about people in situations of poverty? How do we structure our society to take care of people or not? All of those things, it’s kind of right in between the systems level and the community philosophy level.
Finally, Eleanora, a community health worker, suggested a need for a more dynamic visual SDH framework—one that could capture relationships between factors. The following quote suggests similar themes in the work of Jaime Breilh, Nancy Krieger, and others who have attempted to advance a model of SDH that captures the direct impact of structural forces on people’s lives and survival:[32]
I think general socioeconomic, culture, environmental conditions, I would put that much closer [to the individual]. Because I think those conditions include racism, and what kind of services are being given to the people.
Sociological imagination at Family Center
Frontline workers also discussed how the absence of engaging with the social origins of health inequities is problematic both practically and ethically. These observations display engagement with some of structural competency’s core constructs. Sam, a housing case manager, stated in an interview, “Of course health is more than your genetics and your lifestyle choices, right? I mean, anyone with a lick of sense understands that, right? It’s just common sense,” demonstrating how, for her, possessing a sociological imagination was a practical, common-sense part of her approach to client services.
Sam went on to reflect, “I probably see things differently since I’ve worked here than I did before that because it does open your eyes to what people have to struggle with, which I might not have had that exact same kind of struggle, you know, within my own life.” By understanding her clients’ health as more than a personal struggle and her professional role in a broader social context, she demonstrated the uses of sociological imagination in a workplace where intervening upon health inequity is the goal. Her words suggest endorsement of a worldview in which health inequities are understood as reflective of and exacerbating social problems. Furthermore, she is aware of her own place in a social structure through frontline experience. This also links to structural competency’s notion of structural humility.
Like Sam, other Family Center workers spoke of professional apathy and burnout as a barrier to addressing health inequity, supporting Mills’s assertion that social apathy in the form of blaming those who are suffering from health inequities for their plight contributes to social problems. As noted by Eileen, a mental health clinician, “It’s much harder to make changes when you have lots and lots piled up on you. And when you’ve got a society that is also making you [a pregnant person] at fault.”
Another frontline worker discussed how lack of sociological imagination emerged in education. Ali worked in the Health Team, focusing on outreach and service initiation for pregnant and postpartum clients. Ali was also a medical student. During our interview, in response to a question about how her medical education impacted her daily work at Family Center, she threw up her hands and stated:
In the classroom, the material has historically been presented without any structural context on, like, why are people injecting drugs? Why might somebody experience homelessness? There just, like, isn’t really any context. It’s part of just like, in many cases, race-based medicine, like give African American patients this medicine, or like Asian populations are more likely to be subject to this disease. Instead of like, well, what an anti-racist care would look like, “Okay, let’s look at the structural reasons for why some of these things might be true. How are people ended up in more marginalized positions, and how does that affect their health? What can we do about it? How are we changing it?”
She went on to express frustration at health and social service providers outside of Family Center who she saw as content with a “race-based medicine” approach and consciously or unconsciously relied on racial, ethnic, or class stereotypes to make decisions. She described Family Center as a counterpoint to her medical education and a broader culture in which individuals are blamed for their poor health. Ali portrayed many clinicians she encountered outside Family Center as lacking a structural understanding of how populations come to be disproportionately impacted by poor health. She also signposted structural competency’s core concept of rearticulating cultural presentation in structural terms by questioning the use of “race” rather than racism to explain health inequities
Similarly, Anne, a health educator, reflected on the broader culture of health and social services present outside Family Center:
There are core elements [of health services] that sometimes get placed on a level of unimportance, when in fact they should be the primary. So, let’s say this person comes in, and they could be disregarded because, oh, they’re drunk. Or they’re really very poor. Let’s see this person here because they look like they’re dressed better, or something like that … Some people are there just to put in their eight hours, they only have four hours to go. Is that how you’re measuring your day, or are you measuring your day by how you can influence health in your clients or in the patients?
Here, Anne demonstrates an understanding that social forces (classism and stigma) shape clinical interactions, shifting blame from the patient and engaging with a core skill set of structural competency. Frontline workers like Anne may be well poised to develop this understanding and engage in structural competency curricula that link poor-quality care or clinician bias with structural conditions such as profit-based health care. Anne also demonstrates alignment with the right to health by endorsing the concept that economic stratification should not determine who lives or thrives and who does not. Overall, frontline workers displayed rejection of apathy and burnout, strong sociological imagination, and, when presented with the SDH framework, endorsement of the framework as necessary knowledge in their work to intervene upon health inequity. Some frontline workers innovated on the Dahlgren and Whitehead model, suggesting that frontline workers have potential contributions to this public health knowledge framework. They also displayed components of structural competency as outlined by Metzl and Hansen. Frontline workers at Family Center engage with social and economic injustices as inextricable from health inequities, signaling their potential allyship with the right to health movement and the contribution of human rights as an animating vision to their current work. Notably, workers did not, unprompted, connect their efforts to international contexts or struggles, despite the diasporic (e.g., Latin American, Central American, Caribbean) sociodemographic profiles of many of their clients. The international nature of their clients’ lives, their own work to intervene in social determinants that have international origins and implications, and this lack of international framing of their own work suggests an opportunity to research connections (current or potential) that frontline workers may have to the right to health.
Discussion
This research reveals insights into the relationships between the sociological imagination, structural competency, SDH, and the right to health, particularly the relationships between social and economic rights violations and maternal health inequities. The perspectives of frontline health and social service workers inform SDH frameworks at a key era in SDH research and practice. Scholars and policymakers in the United States are calling for action and increased attention to structural racism following police murders and subsequent political uprisings, while the global COVID-19 pandemic has led to increased advocacy for the right to health as global practice. In our fieldwork, social and community networks, living and working conditions, and general socioeconomic, cultural, and environmental conditions emerged as most salient to the production and organization of health inequities. Frontline workers also proposed innovations to the SDH framework, highlighting the need for knowledge and practice frameworks to capture the dynamic relations of power, social hierarchy, and oppression that contribute to health inequities, in line with contemporary SDH research.
It is our emic assertion that fieldwork demonstrates that frontline workers cultivate a sociological imagination regarding health inequities because they feel that understanding clients’ suffering in terms of social forces and historical context is a counterweight to apathy and burnout, which impede client services as well as staff members’ and clients’ well-being. Workers displayed the capacity to develop a general sociological imagination into an analysis of specific social forces such as racism and poverty that are causes of health inequities. Moreover, workers are engaged in several key elements of structural competency, including structural humility, developing extra-clinical language, and rearticulating “cultural” presentations in structural terms. Frontline workers’ thinking connects to existing frameworks of health as a basic right alongside social and economic rights as well as global social movements.
Limitations
The current study has several limitations. By excluding most managers and clients and focusing solely on frontline worker perspectives and experiences, our data are limited to certain Family Center roles. Including managers and clients could enrich the analysis of the perspectives on key issues at stake in this project: apathy, burnout, the SDH framework, sociological imagination, and the right to health. Participant observation with frontline workers at the agency itself inevitably limited our access to those workers whose duties occurred primarily outside of the agency, such as Family Center birth doulas, which may have limited our understanding of how frontline workers applied their perspectives in distinct but related contexts or settings. Future work could be comparative, transnational, or transregional. Additional research could also explore the perspectives of frontline workers in biomedical settings such as hospitals and clinics. For example, frontline workers in a hospital during the COVID-19 pandemic might have poorer working conditions (e.g., overwork, lack of personal protective equipment) and experience greater apathy and burnout, less capacity to engage in structural competency, and less alignment with the right to health. Conversely, the inequitable outcomes of the pandemic may create heightened sensitivity to SDH and more alignment with the right to health movement. Finally, choosing just one visual of SDH (i.e., the Dahlgren and Whitehead rainbow model) privileged this version of portraying SDH over others (e.g., those of the US Centers for Disease Control and Prevention or World Health Organization) and biased results toward endorsing the model presented. Here, the study methods offer a potential means of mitigating this limitation. The methods and principles of institutional ethnography, including participant observation, reflexivity, reciprocal relationships, and attunement to power dynamics meant that the first author spent significant time in the field building relationships (e.g., as fellow commuter, fellow social service provider, fellow trainee) in addition to playing the role of interviewer. While not erasing social and institutional hierarchies between researcher and participant, such relationships can facilitate more open and transparent discussion in interviews than conventional interview methods alone.
Conclusion
These findings indicate that frontline workers are engaging with many of the key elements and questions of structural competency, such as recognizing the structures that shape clinical interactions and developing an extra-clinical language of structures. For example, Family Center workers named the physiological impacts of racism on pregnant people as socially contingent and spoke of racism itself as a social and political force. Family Center workers also connected this with the ability to empathize with clients and destigmatize the need for social services. Some workers added innovations and interpretations to the SDH framework when the Dahlgren and Whitehead model was presented to them, indicating that frontline workers have valuable insights concerning this popular public health framework. Examining and understanding their perceptions and experiences will inform education, training, and the development of an expanding SDH workforce. Where much research on SDH and structural competency has focused on clinicians, movements for the right to health acknowledge the importance of laypeople and a range of frontline workers in achieving health for all. Frontline workers may see themselves better represented in a framework that includes the right to health.
The framework offered here represents the shifts and fluctuations in frontline worker perspectives. Addressing health inequities through collective action and the right to health requires continual, shared reflection on praxis and accountability to client and patient communities.[33]Cultivating a sociological imagination is a necessary but insufficient step toward structural competency and enfranchising the right to health. By cultivating the sociological imagination present in health and social services providers, we may foster empathy with clients, prevent or mitigate burnout, inform the implementation of structural competency curricula and practice, and motivate engagement with movements for human rights, including the right to health.[34] The sociological imagination may be an important precursor for frontline workers to understand and enact structural competency and take part in the right to health as a global social movement. Existing training and curricula on the social determinants of health would be well served by approaching the sociological imagination, structural competency, and the right to health as adjacent frameworks. By demonstrating that frontline workers may be poised to put structural competency into practice and unite with the right to health movement, research can motivate future developments of this promising framework. And by understanding structural competency in relation to apathy and burnout, sociological imagination, and the SDH framework, it is possible to develop insights into the perspectives of those with the most intimate knowledge of service delivery.[35] Moreover, understanding these concepts can enrich the participation of health care workers in the collective struggle for the right to health by fostering imagination in better futures. Extending beyond health care systems, this means working toward what James Baldwin calls the “perpetual achievement of the impossible.”[36]As Angela Davis reminds us, “You have to act as if it were possible to radically transform the world. And you have to do it all the time.”[37]
Margaret Mary Downey, MSW, PhD, is a member of the Structural Competency Working Group and an assistant professor at Tulane University’s School of Social Work, New Orleans, United States.
Ariana Thompson-Lastad, PhD, is a member of the Structural Competency Working Group’s leadership team, an assistant professor at the University of California San Francisco School of Medicine, and core faculty at the Osher Center for Integrative Medicine, San Francisco, United States.
Please address correspondence Margaret Mary Downey. Email: mdowney2@tulane.edu.
Competing interests: None declared.
Copyright © 2023 Downey and Thompson-Lastad. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] World Health Organization, “The Social Determinants of Health” (2022), https://www.who.int/health-topics/social-determinants-of-health.
[2] M. D. Fleming, J. K. Shim, I. H. Yen, et al., “Patient Engagement at the Margins: Health Care Providers’ Assessments of Engagement and the Structural Determinants of Health in the Safety-Net,” Social Science and Medicine (1982) 183 (2017); A. Schickedanz, C. Hamity, A. Rogers, et al., “Clinician Experiences and Attitudes Regarding Screening for Social Determinants of Health in a Large Integrated Health System,” Medical Care 57/Suppl 2 (2019); K. H. Chaiyachati, D. T. Grande, and J. Aysola, “Health Systems Tackling Social Determinants of Health: Promises, Pitfalls, and Opportunities of Current Policies,” American Journal of Managed Care 22/11 (2016).
[3] G. Dahlgren and M. Whitehead, “The Dahlgren-Whitehead Model of Health Determinants: 30 Years on and Still Chasing Rainbows,” Public Health 199 (2021); P. Farmer, “Challenging Orthodoxies: The Road Ahead for Health and Human Rights,” Health and Human Rights Journal 10/1 (2008).
[4] C. W. Mills, The Sociological Imagination, reprint (Harmondsworth: Penguin Books, 1959).
[5] D. Hoyert, “Maternal Mortality Rates in the United States, 2020,” National Center for Health Statistics (2022), https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2020/maternal-mortality-rates-2020.htm.
[6] Ibid.
[7] Ibid.
[8] E. E. Petersen, N. L. Davis, D. Goodman, et al., “Racial/Ethnic Disparities in Pregnancy-Related Deaths—United States, 2007–2016,” Morbidity and Mortality Weekly Report 68/35 (2019).
[9] A. T. Geronimus, “Black/White Differences in the Relationship of Maternal Age to Birthweight: A Population-Based Test of the Weathering Hypothesis,” Social Science and Medicine 42/4 (1996).
[10] M. P. Salyers, K. A. Bonfils, L. Luther, et al., “The Relationship between Professional Burnout and Quality and Safety in Healthcare: A Meta-Analysis,” Journal of General Internal Medicine 32/4 (2017).
[11] Ibid., p. 475.
[12] M. Balfe, “The Sociological Imagination for Mental Health Nursing: A Framework and Some Reflections,” Journal of Psychiatric and Mental Health Nursing 29/2 (2022); S. Kitto, “Strategies for Teaching the Sociological Imagination to Medical Students: The Role of Embodiment,” Health Sociology Review 13/1 (2004); B. A. Pescosolido, “Taking ‘The Promise’ Seriously: Medical Sociology’s Role in Health, Illness, and Healing in a Time of Social Change,” in B. A. Pescosolido, J. K. Martin, J. D. McLeod, and A. Rogers (eds), Handbook of the Sociology of Health, Illness, and Healing (New York: Springer New York, 2011).
[13] Advisory Committee on Training in Primary Care Medicine and Dentistry, Addressing the Social Determinants of Health: The Role of Health Professions Education (Washington, DC: Health Resources and Services Administration, 2016).
[14] Y. Park, R. Crath, and D. Jeffery, “Disciplining the Risky Subject: A Discourse Analysis of the Concept of Resilience in Social Work Literature,” Journal of Social Work 20/2 (2020); Fleming et al. (see note 2).
[15] S. M. Holmes, A. C. Jenks, and S. Stonington, “Clinical Subjectivation: Anthropologies of Contemporary Biomedical Training,” Culture, Medicine, and Psychiatry 35/2 (2011), pp. 105–112.
[16] J. M. Metzl and H. Hansen, “Structural Competency: Theorizing a New Medical Engagement with Stigma and Inequality,” Social Science and Medicine 103 (2014).
[17] Ibid., pp. 126–127.
[18] J. Neff, S. M. Holmes, K. R. Knight, et al., “Structural Competency: Curriculum for Medical Students, Residents, and Interprofessional Teams on the Structural Factors That Produce Health Disparities,” MedEdPORTAL (2020).
[19] A. Ali and C. E. Sichel, “Radicalizing Advocacy in Service Settings: Using Structural Competency to Address Tensions between Social Action and Psychological Practice,” Psychological Services 17/S1 (2020); M. M. Downey, J. Neff, and K. Dube, “Don’t ‘Just Call the Social Worker’: Training in Structural Competency to Enhance Collaboration between Healthcare Social Work and Medicine,”Journal of Sociology and Social Welfare 46/4 (2019); R. Waite and D. Hassouneh, “Structural Competency in Mental Health Nursing: Understanding and Applying Key Concepts,”Archives of Psychiatric Nursing 35/1 (2021).
[20] Metzl and Hansen (see note 16).
[21] E. Beracochea, C. Weinstein, and D. P. Evans (eds), Rights-Based Approaches to Public Health (New York: Springer, 2011).
[22] A. Hernández, A. L. Ruano, A.-K. Hurtig, et al., “Pathways to Accountability in Rural Guatemala: A Qualitative Comparative Analysis of Citizen-Led Initiatives for the Right to Health of Indigenous Populations,” World Development 113 (2019); Beracochea et al. (see note 21).
[23] Farmer (see note 3).
[24] D. E. Smith, Institutional Ethnography: A Sociology for People (Walnut Creek: AltaMira Press, 2005).
[25] E. Mykhalovskiy and L. McCoy, “Troubling Ruling Discourses of Health: Using Institutional Ethnography in Community-Based Research,” Critical Public Health 12/1 (2002).
[26] D. E. Foley, “Critical Ethnography: The Reflexive Turn,” International Journal of Qualitative Studies in Education 15/4 (2002).
[27] E. H. Bradley, L. A. Curry, and K. J. Devers, “Qualitative Data Analysis for Health Services Research: Developing Taxonomy, Themes, and Theory,” Health Services Research 42/4 (2007).
[28]. F. Hsieh and S. E. Shannon, “Three Approaches to Qualitative Content Analysis,” Qualitative Health Research 15/9 (2005).
[29] La Pelle, “Simplifying Qualitative Data Analysis Using General Purpose Software Tools,” Field Methods 16/1 (2004).
[30] Metzl and Hansen (see note 16);
[31] Dahlgren and Whitehead (see note 3).
[32] J. Breilh, “Latin American Critical (‘Social’) Epidemiology: New Settings for an Old Dream,” International Journal of Epidemiology 37/4 (2008); N. Krieger, “Proximal, Distal, and the Politics of Causation: What’s Level Got to Do With It?,” American Journal of Public Health 98/2 (2008).
[33]G. Merlo, “Developing Cultural Praxis,” in Principles of Medical Professionalism (Oxford: Oxford University Press, 2021).
[34]T. A. Ghebreyesus, “Health Is a Fundamental Human Right,” World Health Organization (2017), who.int/news-room/commentaries/detail/health-is-a-fundamental-human-right.
[35]Office of the Surgeon General, Addressing Health Worker Burnout: The U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce (Washington, DC: Department of Health and Human Services, 2022).
[36] J. Baldwin, The Fire Next Time (New York: Modern Library, 2021), p. 86.
[37] A. Davis, Lecture at Southern Illinois University Carbondale (February 13, 2014).