Food Security as a Social Determinant of Health: Tackling Inequalities in Primary Health Care in Spain
Vol 25/1, 2023, pp. 9-21 PDF
Mireia Campanera, Mercè Gasull, and Mabel Gracia-Arnaiz
Abstract
Food insecurity can be understood as a manifestation of health inequality and thus a deprivation of the right to health. This paper explores the strategies followed in primary health care centers in Spain to care for people struggling to regularly access healthy, safe, and sufficient food. Ethnographically based, our study analyzes, on the one hand, the resources available to primary health care teams to assess the social determinants of health and, on the other, the importance that professionals give to food in the diagnosis, treatment, and prevention of diseases related to inequality. Given that our study was carried out during the recent economic and health crises, the results show the difficulties faced by these centers in responding to constantly changing social needs. Budget cuts, a lack of specific or structural actions, and the invisibilization of particular expressions of inequality have proven challenging to the aim of providing integrated care capable of recognizing the environmental factors that condition patient health. In the case of food insecurity, our study found that there are no instruments in primary care centers to identify and therefore address this insecurity. We explore whether this is due mainly to the growing lack of means or more to the fact that the relationship between material living conditions, food, and health has been downplayed—and the responsibility of the health system in guaranteeing the right to food correspondingly diluted.
Introduction
Decades ago, the 1978 Declaration of Alma-Ata focused on the responsibility of governments to provide health care for the entire population, emphasizing the importance of primary health care and its potential to cover 70% of health needs during the life cycle.[1] Years later, the World Health Organization (WHO) recognized that social, political, and economic conditions can make it extremely difficult for people to access health care and, consequently, for the right to health to be fulfilled.[2] Recognizing the impact of structural and intermediate determinants on health, WHO established guidelines on the social determinants of health that were to guide states in combating social inequalities.[3]
Despite health equity having gained priority within the European political agenda, Spain confronts specific obstacles to addressing social inequality in its health care system. The Ministry of Health developed a roadmap for moving toward health equity in 2015, but its proposed policies and interventions to reduce social inequalities have been repeatedly altered.[4] These difficulties have been exacerbated as a result of the cuts in health care spending following the economic recession of 2008 and the impact of COVID-19.[5] The hospital-centered and primary health care policies before the 2008 meltdown tended not to include goals or resources aimed at reducing inequality.[6] There were few examples of interventions that took inequality into account, and even fewer that included identifying and addressing food insecurity and its associated comorbidities.[7] It is well established that not having regular access to enough safe, healthy, and culturally appropriate food is related to obesity, hypertension and hyperlipidemia, diabetes, hypoglycemia, chronic kidney disease, and frailty in the elderly.[8] Food insecurity is an expression of social inequality that compromises the physical and emotional health of marginalized people, and therefore their right to health.[9]
Despite the fact that food security is fundamental to human dignity and the full enjoyment of human rights—and that Spain is a party to the International Covenant on Economic, Social and Cultural Rights, which protects the right to adequate food—recent administrations have not taken sufficient measures to ensure this right. On the contrary, the increase in food insecurity in the last decade, coinciding with the recent economic and health crises, makes this evident.[10]
This paper explores the strategies followed in primary health care centers (PCCs) in Catalonia, Spain, to provide care to people struggling to regularly access healthy, safe, and sufficient food. Ethnographically based, the study analyzes, on the one hand, the resources available to primary health care teams to assess the social determinants of health and, on the other, the importance that professionals give to food in the diagnosis, treatment, and prevention of diseases related to inequality. Recognizing that equity depends in part on the implementation of public health actions and social policies, we focus particularly on the type of dietary prescriptions and recommendations proposed to patients visiting these centers, examining whether they are an effective means of addressing the determinants of social inequalities in health.[11]
Since the study was carried out during the recent economic and health crises, the results show the difficulties faced by these centers in responding to continuously evolving social needs. Budget cuts, the lack of specific or structural actions, and the invisibilization of particular expressions of inequality are proving challenging to the aim of providing integrated care capable of recognizing the environmental factors that condition patient health. In the case of food insecurity, no tools were found in the PCCs to identify and thus address it. We explore whether this is due mainly to the growing lack of resources or more to the fact that the relationship between material living conditions, food, and health has been downplayed—and the responsibility of the health system in guaranteeing the right to food correspondingly diluted. The ultimate purpose of this paper is to suggest conceptual and practical changes that could contribute to making health equity a priority for all.
Materials and methods
This paper presents the results of research carried out at the primary care level during two periods as part of different research projects, both focused on food security. The first studied the precarization of daily life due to the 2008 recession, and the second (which is ongoing) explores food insecurity among the elderly post-COVID-19.[12] We have selected primary health care as our focus because it is an essential sector that provides basic assets for the health of individuals and can monitor the extent of social determinants that are detrimental to a population’s health.
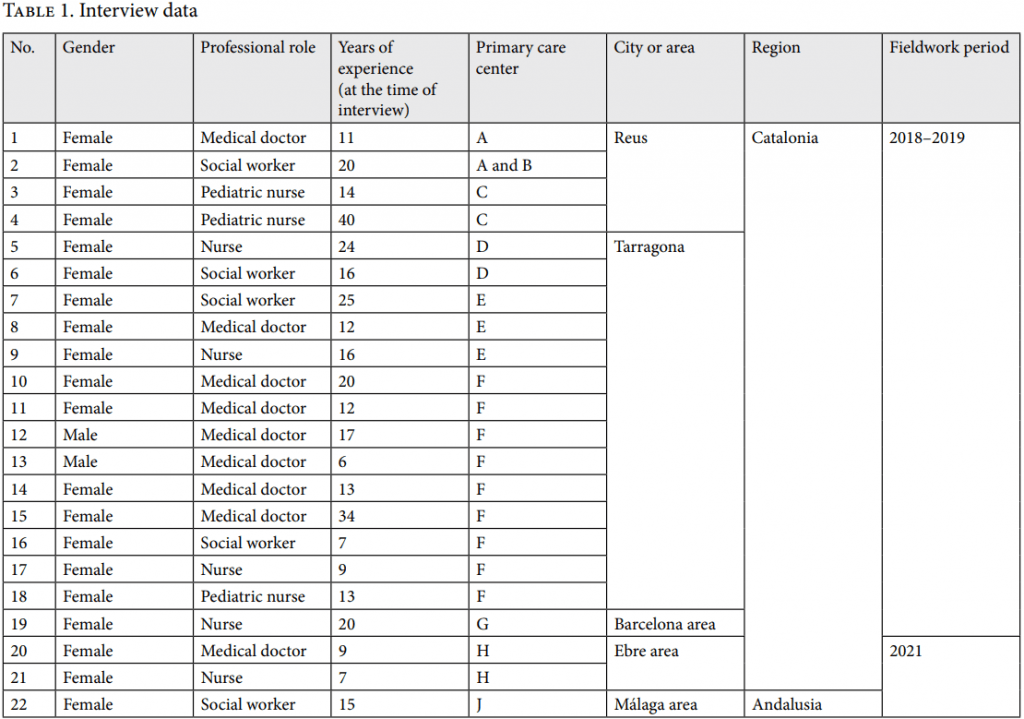
In Spain, the health system is decentralized, with health management and policies mainly the responsibility of the different autonomous communities, such as Catalonia and Andalusia. Each autonomous community is divided into “health regions” (regiones sanitarias), which are in turn subdivided into “basic health areas” (áreas básicas de salud). Each health region has multiple teams of primary health care practitioners who serve in PCCs that provide basic medical care to all citizens at the local level.[13] Catalonia is the Spanish region where most of our fieldwork took place—specifically, in the cities of Reus and Tarragona, and the Barcelona and Ebre areas. We also did research in the Málaga area, within the Andalusia region (see Table 1). In this work, our informants consisted of 22 professionals from nine PCCs who worked in the areas of nursing, family practice, and social work. We selected those centers due to their location in neighborhoods with high levels of socioeconomic deprivation.[14]
Since primary health care staff are one of the groups closest to citizens when it comes to health care, these practitioners are key actors in this research. The practitioner selection process was conducted using the snowball technique, following some contacts from the research team at two PCCs who, in turn, put us in contact with staff working in other highly deprived areas. One center that was especially accessible to our research team was selected for an in-depth study, with nine interviews and participant observation conducted over seven months.
Our research techniques consisted of participant observation and semi-structured interviews. Given their complementarity, these qualitative techniques are useful for collecting and analyzing health practitioners’ narratives and for looking at subjective and institutional contexts as well as daily practices in primary health care. The interviews allowed us to gain deeper insights into the perceptions of primary health care practitioners about social inequalities, the social and health status of their patients, and their own professional performance.
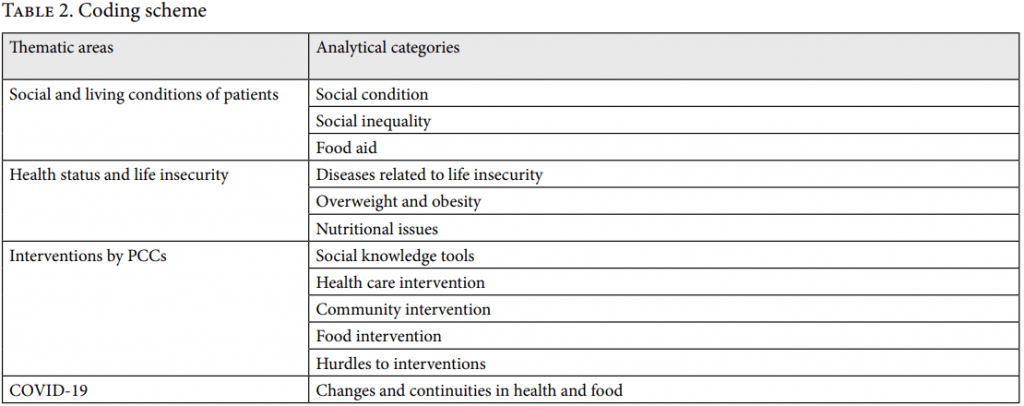
All interviews lasted 60–90 minutes and were conducted in the clinics where the health care and social workers were active. The same script was used by eight members of our research team. Staff from different areas were interviewed given their relevance and suitability to the study: eight nurses (general and pediatric), nine family doctors, and five social workers, all of them women except for two family doctors. Most professionals had begun working before 2008. In addition to interviews, we conducted participant observation in the nine selected PCCs. At each PCC, the researcher took center-specific notes and collected information on the activities of the center and the social context of the neighborhood. After recording and transcription, we coded and processed the interviews using the ATLAS.ti qualitative data analysis software. Sixteen codes were selected to identify the main variables of analysis, contributing to the systematic development of category organization and thematic analysis (see Table 2). The most relevant codes were defined though a consensus meeting among all the researchers.
Our methodology also gave consideration to the importance of contrasting and complementing the practitioners’ discourses with data from health surveys at the national and regional levels related to the 2006–2021 period—that is, going back to before the 2008 economic meltdown and including the COVID-19 pandemic. These surveys provide quantitative data on diseases broken down by gender, age, educational level, and social class. At the same time, we analyzed extensive documentation, including national and regional strategic health plans, reports and programs from the health care sector, and specific documentation for each center, as well as specific tools such as social scales.
Results
Patients’ social situation
When assessing the social and economic situation of patients, nurses and doctors use various methods. In the medical history of each patient, there is a section with a social-risk scale that allows health practitioners to describe those situations that they consider to be affecting their patient’s health. This section contains six items on economic vulnerability, family context, housing conditions, and dependency status, but none on food security. Practitioners also have recourse to “Z codes,” a list of labels that can be used to indicate social problems such as economic, job, or family insecurity, or gender violence.[15] Just two of the interviewees, who are family doctors, acknowledged using these codes occasionally, but they also stated that they have access to a complete social history of the patient, compiled by social workers.
The clinical interview is the most commonly used means in medical and social settings for understanding a patient’s context. According to practitioners, it is possible to gauge a patient’s social situation by means of direct or indirect questions: for example, what kind of work they do, whom they live with, what ailments they suffer from, whether they struggle to make ends meet, how many meals they have a day, and what they ate the day before or earlier that same day. Doctors and nurses alike pointed out that for patients in a precarious situation, their health problems are just one more issue on top of a set of difficulties that they consider to be of a more serious nature because of their urgency.
While almost half of the practitioners interviewed reported being clearly interested in their patients’ context and asking questions and listening to them, this does not necessarily mean that talking about these issues is a common practice or that informs practitioners’ interventions and prescriptions. Most nurses consulted reported feeling awkward when asking about these issues, not least because of the embarrassment that some patients experience when talking about “their hardship” during their clinical appointment. Patients often show reluctance to talk about their difficulties in accessing food and their loss of purchasing power, as well as their need for social assistance. Some practitioners try to compensate for the limited time available to them for individual visits by working toward a more lasting relationship and building trust over the long term. This allows them to learn more about the lives of those patients who are willing to share their experiences. However, the professionals interviewed explained that the COVID-19 pandemic significantly transformed patient-practitioner contact—which was reduced to phone calls during lockdown—and made it more difficult to detect situations of deprivation. With home visits, often made by nurses in very unique cases of dependence, it is easier to see if a person is struggling with their finances. At home, practitioners can directly observe what resources for hygiene and personal care are available to the patient, if they suffer mobility restrictions that keep them from doing their own shopping, whether they can cook, whether they live alone, and what they eat; practitioners can even detect cases of malnutrition that might otherwise remain unnoticed. Of all the professionals interviewed, only one nurse considered that the socioeconomic situation of patients has no impact on their health and that there is therefore no need to inquire about it.
Embodying uncertainty
Most practitioners said that the economic recession of 2008 led to a worsening health status among the most disadvantaged layers of society. Respondents were asked about the effects of growing uncertainties. “There are social problems that lead to health issues,” explained a 64-year-old nurse. Mental health problems were the most cited. They refer to an increase in despondency, anxiety, and depression, and also to the way in which unemployment, job insecurity, and economic instability all damage health. All professionals interviewed in 2021 pointed to an increase in solitude, isolation, fear, and emotional suffering in their older patients.
Health care professionals also associated various insecurities with obesity, cardiovascular risk, diabetes, smoking, and increased alcohol consumption. Although few reported examples of how social inequalities are reflected in the health of their patients, it was common for them to relate the emotional alterations that come with job instability to weight gain: “Anxiety always leads to excess weight, in the cases we see here. When anxiety subsides, they start to lose weight; they gain weight partly because of the medication and partly because they move less. Anxiety itself makes them increase the amounts they eat” (P27, Tarragona). Practitioners cannot easily separate mental health from other health issues, especially when “suffering people say that they eat as a way to find relief from anxiety and get immediate gratification” (P27, Tarragona). A doctor treating a family that had been hard hit by the economic meltdown saw a link between the continuum of employment and emotional setbacks experienced by family members and their mental health: work incapacitation and psychic dementia in the mother, job insecurity and suspected cancer in the father, and domestic violence by the mother on her daughter.
One family doctor explained that, in the peak years of the recession, she received work incapacity applications on a weekly basis. She associated this fact with worsening working and economic conditions; indeed, the Catalan Health Survey reported an increase in incapacity for work during that period of crisis, particularly among people with primary education only (complete or incomplete).[16]
Other health issues related to social inequality are chronic diseases and malnutrition. While just a few cases of undernourishment have been detected in primary health care appointments, obesity and overweight, as well as diabetes, are often seen as the result of precarious social situations. Health care workers explained that undernourishment occurs in elderly people who live alone, have few resources, and do not follow the recommended diet, especially in families who depend on food donations (with a very high incidence among non-European Union citizens) and in extended family households whose only income is a retirement pension. People over 75 are usually tested for undernourishment by health professionals, often with positive results. These are people who eat little meat, fish, and dairy products; many are care-dependent or else cook only with difficulty and go shopping irregularly. The practitioners we interviewed did not report applying these tests to people at risk of poverty.
Food practices in medical consultations: Recommendations, habits, and individual responsibility
Nursing professionals are the ones who intervene most in the food sphere, issuing recommendations based on each patient’s situation. They advise on food types, amounts, products to avoid or eat sparingly (e.g., sweetened or ultra-processed foods, pastries), mealtimes, and number of daily meals. One of the most commonly used techniques is the “dish method,” where patients are instructed that a meal needs to contain 50% vegetables, 25% carbohydrates, and 25% protein; this also entails an explanation about the different food groups. Nurses also suggest physical activity and modified shopping habits, and they perform checks on weight. When they detect diabetes, excess weight, or obesity, they also suggest specific diets. According to one nurse, it is a matter of “sorting out their diet a bit … so they know what to eat and what to say no to, what shouldn’t enter the house and what shouldn’t be bought” (P12, Tarragona). In general, they suggest eating five times a day, including five pieces of fruit and vegetables, and reducing the intake of hyper-caloric foods.
All of these are interventions focused on individual behavior. Many physicians and nurses pointed out the difficulty of effecting change in eating habits or of conducting follow-up due to the short visiting time they are accorded for each patient. Nurses noted that their advice usually falls on deaf ears because “people already know what they should do, but fail to do it” (P12, Tarragona). Those professionals with patients who try to introduce healthier eating habits say that barely 30% of their patients manage to do so. These are usually younger people or individuals with health problems that can be aggravated (e.g., diabetes and high blood pressure), and therefore they see the need for a change in habits. They tend to be people motivated to make changes, and people with sufficient economic and emotional resources for such a transformation, who also find support in their social environment.
About half of the professionals considered that community intervention is necessary to change the population’s eating practices, although they also pointed out that some colleagues refuse to implement a model that requires leaving their offices, citing a lack of time and incentives. One nurse participated in a “Health at School” program by conducting workshops on healthy eating in schools, where similar recommendations adapted for children were made. Another nurse collaborated with teachers in the community project Dynamis, involving 12- to 14-year-old students, their families, and the school, and promoting extracurricular physical activity and healthy eating. This program was endorsed by the Health Department, and a nurse considered it more effective than the “10-minute talk in consultation room” (P5, Tarragona). In most cases, practitioners’ assessment of the effects of these actions mentioned only short-term change; in other cases, there was no consistent monitoring or assessment of the program, and therefore its impact is not known.
In cases of patients with a diagnosis of obesity or diabetes, all practitioners acknowledged having treated people who cannot follow the recommended diet due to financial difficulty in accessing a varied and nutritionally adequate diet. After one doctor prescribed a proper diet to treat diabetes, her patient replied that he could hardly follow it because “he only ate what he was given at the Red Cross” (P1, Tarragona). The organization provides non-perishable food packages that only occasionally include fresh fruit, vegetables, meat, and fish. In cases where food insecurity is detected, practitioners refer the patient to charities (e.g., Red Cross, Caritas) or social services. Referral to social services and monitoring of the patient is done by the center’s social worker in coordination with doctors. There is no specific monitoring of food consumption, though practitioners acknowledged that their patients receive canned, ultra-processed, and ready-to-eat food. During the 2020 lockdown, two PCC professionals, in coordination with the local council, charities, and social movements, collaborated in a food security initiative that organized home deliveries of food to the elderly.
When asked whether they had detected changes in the types of food consumed by their patients and the possible causes, professionals pointed to a high intake of sugary, high-fat, and pre-cooked products because they are more affordable. They argued that “today, people cook less and eat badly due to an excess of certain ingredients or to their quality” (P6, Reus). They also observed a widespread and excessive use of low-nutrient ingredients. In fact, the Spanish Food Consumption Panel and the National Health Survey confirm a decline in fresh fruit, milk, meat, and fish consumption, and an increase in processed foods.[17] Both WHO and Spain’s Strategy for Nutrition, Physical Activity and the Prevention of Obesity state that the food industry has played a role in making “unhealthy” food more accessible, and they call for a reduction in the fat, sugar, and salt content in food and for the regulation of the advertising of such food.[18] Only two nurses identified the food industry and health authorities as responsible for this easy access to unhealthy food. Regarding the food practices of their patients, one doctor highlighted the importance that sweet foods (e.g., pastries, cakes, and candies) have in celebrations and hospitality practices in certain cultures. Another professional commented that the appreciation of the corpulent body as healthy and beautiful among Moroccan women hinders any medical intervention aimed at reducing overweight and obesity in this community.
In general, most professionals recognized their limitations in trying to reduce health inequalities. One way to tackle them, suggested some nurses, would be to increase community interventions. These practitioners noted that patients are often reluctant to follow medical-nutritional prescriptions because they see them as part of an outdated and repetitive monologue; the practitioners thus proposed increasing the actions carried out with and from the community through a participatory process that considers the particular needs of the community. But other practitioners were skeptical of the effectiveness of community interventions; they emphasized the individual responsibility of patients, judging their habits to be not so much a result of their living conditions but of inappropriate behavior, or unwillingness or lack of interest in following the rules: “It’s hard for them to diet, it’s hard for them to exercise, it’s hard for them to do anything … Aw! You have to lose weight. Can’t you see you’re too fat?” (P14, Reus). This divergence in practitioners’ views is then reflected in practitioners’ greater or lesser involvement in community actions.
Intervention in community health
Training in community intervention for health personnel can be an important tool for tackling social inequality, given that it involves a shift in intervention strategy and in the practitioner-patient relationship. According to a nurse who works in social diagnosis, “It’s not about what you think people need; what I have learnt from the community is that it is about being there and letting them express their demands … and finding out what it is they need the most” (P12, Tarragona). This training process can be seen as one of co-learning and adoption of diagnostic and social intervention tools that can produce results in the medium term.
One of these centers studied in our research has a multidisciplinary team that undertakes various community-based initiatives; one such initiative was the conducting of a social diagnosis of the neighborhood in collaboration with primary health care workers, the city council, the community center, and Catalonia’s Public Health Agency. The center shared the results in a video posted on YouTube.
Another center has been implementing the Catalan government’s COMSalut community program—which seeks to reduce social inequalities as they relate to health—since 2017. Every month, the entire primary health care team is provided with social resources to be prescribed to their patients, in the same way as prescription drugs. These resources include social, recreational, and sports activities or programs, as well as other services such as addiction care and services for women. Though the COMSalut project started in 2015, only 16 of the 434 PCCs in Catalonia are involved.
In a third center, the nursing area conducts workshops on nutrition in secondary schools within the framework of the Health at School program. Its objective is to improve adolescent health through health promotion actions, such as consulta oberta (literally “open consultation”) whereby nursing staff are regularly sent out to schools. One nurse explained that this action is sometimes seen as an imposition by some schools, hindering positive collaboration.
The Catalonia Health Department has implemented other community health programs. A prominent one was “Health in the Neighborhood,” created in 2005; however, the actions and programs that were in place at the time of our research mainly fall under the AUPA Network, formed by working groups providing support and training to primary health care and public health professionals in each health district. In the Tarragona area, only nine primary health care teams are part of this network. It is an initiative that originated from the Interdepartmental Plan for Public Health, in line with WHO’s recommendations to promote health in all areas and policies.[19]
Discussion
The current Spanish strategic framework and recent Catalan health plans recognize the impact of the 2008 recession on the living conditions of the most vulnerable. The latest health plan also points out the negative consequences of the COVID-19 pandemic.[20] While these policies are presented as being inclusive, the scarce resources available at PCCs allow for only a limited integration of the social determinants of health approach, which hinders progress in reducing inequalities.[21] The severe cuts in funding during the last decade, the failure to implement effective specific or structural measures, and the lack of recognition of the specific effects of social inequality—such as food insecurity—have reduced the overall system’s ability to respond to citizens’ health needs. The social determinants of health are recognized but not addressed in a systematic and community-based form, either within or outside the health sector. This inevitably hinders the exercise of the rights to health and to food. The COVID-19 pandemic has worsened this situation by forcing a sharp shift in the organization of primary care that focuses on the pandemic while neglecting other health services.[22] Moreover, these services, when provided, are approached from a merely biomedical stance. Although professionals have information about the social situation of their patients, this does not necessarily translate into a practice focused on mitigating the consequences of inequality.
Most of the primary health care professionals participating in this research are aware of the importance of the social determinants of health; however, their views on the effects of increasing life uncertainties in health are divergent. The majority recognize the lack of tools to improve health equity but believe that it is not in their hands to solve it. A minority signal the need to design strategies that would allow them to intervene in the social sphere, along with other non-health sectors, in order to deal with health problems. We found that those professionals who are motivated to carry out community activities do so more of their own volition than at the instigation of the health system. They consider the instruments available to them to address the social determinants of health to be clearly insufficient. As is the case in other countries, a lack of time, training, and incentives are added difficulties for overburdened professionals after decades of underfunding, further compounded by budget cuts after 2008, and especially after tackling the COVID-19 pandemic, which interrupted community intervention.[23] As WHO has pointed out, many health professionals have experienced burnout following the pandemic, resulting in their own physical and emotional health being compromised.[24]
However, the lack of training in social determinants of health and a structural competency approach explains this divergence in understanding and tackling health inequalities, specifically food insecurity. As Jonathan Meltz and Helena Hansen propose, training in structural competency requires gaining competences in recognizing the structures that shape medical interaction and understanding “socially structured patterns of disease across population groups and economies in ways that point to structural agendas for political and economic change.”[25] They also recommend considering how complex cultural structures produce inequalities and barriers to inclusion. Finally, such an approach would require practitioners to be trained in discerning how issues defined clinically as symptoms, attitudes, or diseases also represent the implications of social and political structures.[26]
The response from primary health care to health problems resulting from increasing insecurity in the population’s living conditions has been vague and feeble. The primary care model in Spain was and still is a disease-oriented model, rather than being person and community centered. This is due to practical and bureaucratic reasons: poor allocation of resources has always made it impossible for PCC practitioners to devote time to education, health promotion, or community health tasks, other than in pilot programs such as those described above. Our results reveal that the largest barrier seems to be the organization of primary care itself, as well as its coordination with other social and public services. This is a burden that some experts say comes directly from the split between health services and social services during the 1980s.[27]
The health system alone cannot remove health inequalities, but it must do its part to reduce them. A comprehensive approach to social inequalities in health is needed from the perspective of the social determinants of health. The health system is just one more determinant, so its contribution to equity is necessarily limited, if essential.[28] Before the COVID-19 pandemic, the social determinants of health approach in Catalonia was rare at the first level of health care, and the social and community perspective had not been widely assimilated into primary health care, except for a few pilots. In Spain more generally, the Ministry of Health’s plan to reduce inequalities has not been implemented to any significant extent. No substantial progress has been made in citizen participation or adequate service provision for the most vulnerable groups.[29] In this country, the COVID-19 pandemic stopped all community nutritional health programs for almost two years. However, other community initiatives emerged during lockdown to mitigate food access difficulties.[30] According to the Food and Agriculture Organization, the number of Spaniards in a situation of food insecurity rose from 600,000 in 2019 to 700,000 in 2020.[31] Although there are no official reports on food insecurity in Spain, some studies indicate that women experience greater forms of food insecurity, as they have to mobilize all the resources available in order to minimize the impact of precarization on their households.[32] At the global level, there is little implementation of the WHO proposal on the social determinants of health, and a lack of specific actions stemming from the Declaration of Astana or the human rights approach.[33]
One of the limitations reported by primary health care personnel is their limited capacity to have an impact on situations of social suffering, understood as the distress resulting from unemployment or precarious employment, and difficulties in accessing decent housing or healthy food, among other situations. In the case of food insecurity, what is surprising is that despite its being associated with poorer health outcomes in routinely managed conditions such as obesity and chronic diseases, PCCs do not use specific instruments to identify it.[34] Nor do they have any indicators to analyze and determine individual or household levels of food insecurity. In fact, food insecurity is not mentioned as a problem to be solved in any public health plan in Spain or Catalonia. The Catalan government designed a food safety plan in order to address the social determinants of health in 2021 but did not ensure regular access to adequate food in times of increasing poverty.[35] In fact, a WHO report pointed out that food security has been further compromised for marginalized communities worldwide due to COVID-19, and the new health policy did not tackle that.[36]
This is partly a consequence of using a conceptual framework that reduces food to mere individual behaviors. As far as food practices are concerned, health interventions are limited to providing healthy eating guidelines within a clinical-therapeutic framework. The activities proposed to patients are still focused on self-control and responsibility, as if the individuals’ food choices and practices were not determined partly by their social and family structures.[37] Food is thus decontextualized from the social environment, stripped of everything in a way that ultimately hinders regular access to nutritionally and culturally adequate eating practices. This reduces practitioners’ proposals to a set of generic recommendations on healthy eating and contributes to ignoring food insecurity both as a health and as a political issue.
Three specific findings from our research stand out in terms of increasing our understanding of food insecurity as a manifestation of health inequality and the way it is addressed in primary care.
First, we observed a difficulty among practitioners, due to a lack of specific or adequate tools, in detecting food insecurity. Long-term, trusting doctor-patient conversations and home visits have significant potential but are neither systematically nor widely developed. We wonder to what extent this lack of intervention is due to inadequate means and resources in the health care centers and to what extent it stems from a downplaying of the relationship between material living conditions, food, and health, leading to a dilution of the health system’s responsibility.
Second, Catalonia’s current and previous health plans recommend a “Mediterranean” diet—in other words, lots of vegetables—and this is the message that nurses transmit.[38] But in cases where food insecurity is detected—in Spain as in other countries—the patient is usually referred to charities or social services, which donate consignments of non-perishable, canned, processed, and ready-to-eat food.[39] Ultra-processed products are very common in the daily diet of people living in precarious situations, in part because these foods are often cheaper.[40] This makes the recommended healthy diet, based on the variety, quality, and quantity of certain ingredients, difficult to follow.[41] Moreover, with the COVID-19 crisis, the demand for food aid tripled in Spain in 2020, so the public sector response to this problem continues to revolve around emergency aid, or “discarded food for hungry people.”[42]
Third, public policies on health, food, and social welfare are failing to guarantee the right to food or to prove effective in enabling the most impoverished populations to feed themselves with autonomy and dignity in times of increasing poverty.[43] Health, social, and food policies must embrace coordinated actions to mitigate inequality and must be designed, systematized, and evaluated with the participation of vulnerable social groups, health professionals, and social agents.[44] In this area, the Spanish state has identified shortcomings that have not been resolved for more than a decade yet require urgent solutions.[45] Our research shows the importance of analyzing food insecurity in detail at the primary level of health care, given that it is not only an indicator of inequality in itself but also at the root of preventable health problems. If healthy, safe, and sufficient food is not assured, the right to health is compromised.
Ethics approval
The results discussed in this paper are part of a research project evaluated and funded by Spain’s Ministry of Science and Competitiveness in 2016 (reference number CSO2016-74941-P). The ministry did not request a specific evaluation by an ethical committee, so our research was not submitted for an ethical evaluation.
Mireia Campanera, PhD, is a postdoctoral researcher in the Department of Anthropology, Philosophy and Social Work at the University Rovira i Virgili, Tarragona, Spain.
Mercè Gasull, MsC, is a lecturer in the Department of Nursing at the University Rovira i Virgili, Tarragona, Spain.
Mabel Gracia-Arnaiz, PhD, is a professor in the Department of Anthropology, Philosophy and Social Work at the University Rovira i Virgili, Tarragona, Spain.
Please address correspondence to Mireia Campanera. Email: mircampa@ucm.es.
Competing interests: None declared.
Copyright © 2023 Campanera, Gasull, and Gracia-Arnaiz. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] World Health Organization, Report of the International Conference on Primary Health Care, Alma-Ata, USSR, Sep. 6–12 (September 12, 1978).
[2] World Health Organization, Social Determinants of Health: The Solid Facts (Geneva: World Health Organization, 2003); World Health Organization, Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health (Geneva: World Health Organization, 2008).
[3] A. Espelt, X. Continente, A. Domingo-Salvany, et al., “La vigilancia de los determinantes sociales de la salud,” Gaceta Sanitaria 30 (2016).
[4] G. Pérez, M. Rodríguez-Sanz, F. Domínguez-Berjón, et al., “Indicadores para monitorizar la evolución de la crisis económica y sus efectos en la salud y en las desigualdades en salud: Informe SESPAS 2014,” Gaceta Sanitaria 28/1 (2014); Ministerio de Sanidad, Servicios Sociales e Igualdad, Comisión para Reducir las Desigualdades Sociales en Salud en España, Avanzando hacia la equidad: Propuestas de políticas e intervenciones para reducir las desigualdades sociales en salud en España (Madrid: Ministerio de Sanidad, 2015).
[5] Amnesty International, La otra pandemia: Entre el abandono y el desmantelamiento; El derecho a la salud y la atención primaria en España (Madrid: Amnesty International, 2021).
[6] G. López i Casasnovas, “Crisis económica, gasto sanitario y desigualdades en salud: Reflexiones desde la economía de la salud,” Icade: Revista Facultad de Derecho 99/1 (2016).
[7] C. Borrell and L. Artazcoz, “Las políticas para disminuir las desigualdades en salud,” Gaceta Sanitaria 22/5 (2008); J. Pooler, V. Hoffman, and F. Karva, “Primary Care Providers’ Perspectives on Screening Older Adult Patients for Food Insecurity,” Journal of Aging and Social Policy 30/1 (2017).
[8] Food and Agriculture Organization, An Introduction to the Basic Concepts of Food Security (Rome: Food and Agriculture Organization, 2011).
[9] A. Kopparapu, G. Sketas, T. Swindle, et al., “Food Insecurity in Primary Care: Patient Perception and Preferences,” Family Medicine 52/3 (2020).
[10] Food and Agriculture Organization (see note 8).
[11] R. Baeten, S. Spasova, B. Vanhercke, et al., “Inequalities in Access to Healthcare: A Study of National Policies 2018,” European Social Policy Network (European Commission, 2018).
[12] First project: “The Precariousness of Daily Life: Food (In)security, Gender and Health,” reference CSO2016-74941-P, funded by Ministry of Economy and Competitiveness (2016–2019). Second project: “Eating Matters: The Challenges of Inclusive, Healthy and Sustainable Eating for a Better Ageing,” reference PID2019-104253RB-C21, funded by Ministry of Science and Innovation (2020–2024).
[13] Departament de Salut, Servei Català de la Salut (2020), https://catsalut.gencat.cat/ca/coneix-catsalut/.
[14] In order to guarantee the anonymity of the informants, we do not specify the names of the centers. M. F. Domínguez-Berjón, C. Borrell, G. Cano-Serral, et al., “Construcción de un índice de privación a partir de datos censales en grandes ciudades españolas (Proyecto MEDEA),” Gaceta Sanitaria 22/3 (2008); Agència de Qualitat i Avaluació Sanitàries de Catalunya, Revisió de la dimensió socioeconòmica de la fórmula d’assignació de recursos de l’atenció primària (2016), http://aquas.gencat.cat; Agència de Qualitat i Avaluació Sanitàries de Catalunya, Desigualtats socioeconòmiques en el nombre de casos i la mortalitat per COVID-19 a Catalunya (Barcelona: Departament de Salut, 2020).
[15] World Health Organization, International Statistical Classification of Diseases and Related Health Problems 2010 (Geneva: World Health Organization, 2010).
[16] Departament de Salut, Enquesta de salut de Catalunya (Barcelona: Generalitat de Catalunya, 2006–2022).
[17] Ministerio de Agricultura Pesca y Alimentación, Informe del consumo de alimentación en España (Madrid: Ministerio de Agricultura, Pesca y Alimentación, 2018).
[18] World Health Organization (2003, see note 2); World Health Organization (2008, see note 2); Ministerio de Sanidad, Consumo y Bienestar Social, Estrategia para la nutrición, actividad física y prevención de la obesidad (Madrid: Agencia Española de Seguridad Alimentaria, Ministerio de Sanidad, 2005); Ministerio de Sanidad, Consumo y Bienestar Social, Estrategia para la nutrición, actividad física y prevención de la obesidad: 10 años de estrategia NAOS (Madrid: Agencia Española de Seguridad Alimentaria, Ministerio de Sanidad, 2015).
[19] Departament de Salut, Salut comunitaria (Barcelona: Generalitat de Catalunya, 2022).
[20] Departament de Salut, Pla de salut Catalunya 2016–2020 (Barcelona: Generalitat de Catalunya, 2016); Departament de Salut, Pla de salut Catalunya 2021–2025 (Barcelona: Generalitat de Catalunya, 2022).
[21] J. Simó and J. Gérvas, “Gasto sanitario en atención primaria en España: Insuficiente para ofrecer servicios atrayentes para pacientes y profesionales; Informe SESPAS 2012,” Gaceta Sanitaria 26/1 (2012); Departament de Salut (2016, 2022, see note 20).
[22] M. Marí-Dell’Olmo, M. Gotsens, M. I. Pasarím, et al., “Desigualtats socials i covid-19 a Barcelona,” Barcelona Societat 1 (2020); Agència de Qualitat i Avaluació Sanitàries de Catalunya (2020, see note 14); Amnesty International (see note 5).
[23] Pooler et al. (see note 7); M. Knowles, S. Khan, D. Palakshappa, et al., “Successes, Challenges, and Considerations for Integrating Referral into Food Insecurity Screening in Pediatric Settings,” Journal of Health Care for the Poor and Underserved 29/1 (2018); J. Devoe, A. W. Bazemore, E. K. Cottrell, et al., “Perspectives in Primary Care: A Conceptual Framework,” Annals of Family Medicine 14 (2016); F. Douglas, K. Machray, and V. Entwistle, “Health Professionals’ Experiences and Perspectives on Food Insecurity and Long‐Term Conditions: A Qualitative Investigation,” Health Social Care Community 28 (2020); F. Cervero-Liceras, M. McKee, and H. Legido-Quigley, “The Effects of the Financial Crisis and Austerity Measures on the Spanish Health Care System: A Qualitative Analysis of Health Professionals’ Perceptions in the Region of Valencia,” Health Policy 119/1 (2015); Ministerio de Sanidad, Servicios Sociales e Igualdad, “Portal estadístico del Ministerio de Sanidad, Servicios Sociales e Igualdad, 2020,” http://inclasns.msssi.es/main.html; Amnesty International (see note 5).
[24] World Health Organization, COVID-19 and the Social Determinants of Health and Health Equity (Geneva: World Health Organization, 2021).
[25] J. M. Metz and H. Hansen, “Structural Competency: Theorizing a New Medical Engagement with Stigma and Inequality,” Social Science and Medicine 103 (2014); F. Beck, M. Curran, A. W. Henize, et al., “Is Poverty Making Me Sick? An Example of the Impact of Medical-Legal Partnership on Keeping Children Healthy,” H. Hansen and J. M. Metz (eds), Structural Competency in Mental Health and Medicine (New York: Springer, 2019).
[26] Metz and Hansen (see note 25).
[27] E. Perdiguero-Gil and J. M. Comelles, “The Roots of the Health Reform in Spain,” in: L. Abreu (ed), Health Care and Government Policy (Évora: Publicações do Cidehus, 2019).
[28] I. Hernández-Aguado, M. Santaolaya, and P. Campos, “Las desigualdades sociales en salud y la atención primaria: Informe SESPAS 2012,” Gaceta Sanitaria 26 (2012).
[29] Ministerio de Sanidad (2015, see note 4).
[30] J. L. Fernández, J. Fernández, and N. Ramírez, Solidaridades de proximidad: Ayuda mutua y cuidados ante la Covid19 (Madrid: Tangente, 2022).
[31] Food and Agriculture Organization, Pan American Health Organization, World Food Programme, and UNICEF, Regional Overview of Food Security and Nutrition in Latin America and the Caribbean (Santiago: Food and Agriculture Organization, 2019); Food and Agriculture Organization, International Fund for Agricultural Development, World Food Programme, et al., The State of Food Security and Nutrition in the World (Rome: Food and Agriculture Organization, 2020).
[32] M. Llobet, P. Durán, C. R. Magaña, et al., “Précarisation alimentaire, résistances individuelles et expériences pratiques: Regards locaux, régionaux, transnationaux,” Anthropology of Food 15 (2020); M. Gracia-Arnaiz, M. Garcia-Oliva, M. Campanera, “Food Itineraries in the Context of Crisis in Catalonia (Spain): Intersections between Precarization, Food Insecurity and Gender,” Social Sciences 10 (2021).
[33] K. Rasanathan, “10 Years after the Commission on Social Determinants of Health: Social Injustice Is Still Killing on a Grand Scale,” Lancet 392 (2018); G. Walraven, “The 2018 Astana Declaration on Primary Health Care: Is It Useful?,” Journal of Global Health 9/1 (2019).
[34] Kopparapu et al. (see note 8).
[35] Institut d’Estadística de Catalunya, Enquesta de condicions de vida 2021 (Barcelona: Institut d’Estadística de Catalunya, 2022).
[36] World Health Organization (2021, see note 24).
[37] M. Gracia-Arnaiz, “Learning to Eat: Establishing Dietetic Normality in the Treatment of Eating Disorders,” Food, Culture and Society 12/2 (2009).
[38] Departament de Salut 2016 (2016, see note 20); Departament de Salut (2022, see note 20).
[39] Kopparapu et al. (see note 8); Pooler et al. (see note 7).
[40] M. Gracia-Arnaiz, M. Garcia-Oliva, and M. Campanera, “Food Itineraries in the Context of Crisis in Catalonia (Spain): Intersections between Precarization, Food Insecurity and Gender,” Social Sciences 10 (2021); M. Chica, Aspectos nutricionales y socio-económicos de las familias con menores, incluídos los de 16 años, usuarias de la Red de Distribución de Alimentos de Reus, master’s thesis (Universitat Rovira i Virgili, 2015).
[41] J. Aranceta, V. Arija, E. Maíz, et al., “Guías alimentarias para la población española (SENC): La nueva pirámide de la alimentación saludable,” Nutrición Hospitalaria 33/8 (2016); V. Dapcich, G. Salvador, L. Ribas, et al., Guía de la alimentación saludable (Barcelona: Sociedad Española de Nutrición Comunitaria, 2004).
[42] J. Catà, “Cáritas multiplica por tres las ayudas para alimentos y alerta de una crisis sin precedentes,” El País (June 12, 2020); EFE Agencia, “El Banco de Alimentos de Zaragoza lanza un SOS para atender a los necesitados,” Heraldo (April 3, 2020); C. Pollard and S. Booth, “Food Insecurity and Hunger in Rich Countries—It Is Time for Action against Inequality,” International Journal of Environment Research and Public Health 16/10 (2019); K. Pérez de Armiño, “Los bancos de alimentos en España durante la crisis: Su papel y discurso en un contexto de erosión de los derechos sociales,” in L. Escajedo, E. Rebato, and A. López, Derecho a una alimentación adecuada y despilfarro alimentario (Valencia: Tirant lo Blanch, 2018); G. Riches, Food Bank Nations: Poverty, Corporate Charity and the Right to Food (London: Routledge, 2018).
[43] P. Farmer, “Challenging Orthodoxies: The Road Ahead for Health and Human Rights,” Health and Human Rights Journal 10/1 (2008); Riches (see note 42); M. E. Ibáñez-Zamacona, E. Rebato, and L. Escajedo San-Epifanio, “Los llamados puentes alimentarios: Solidaridad, lucha contra el despilfarro y derechos humanos,” Revista de Antropología Social 30/2 (2021); Ministerio de Derechos Sociales and Agenda 2030, Informe de progreso 2022 de la Estrategia de Desarrollo Sostenible 2030 (Madrid: Ministerio de Derechos Sociales, 2022); C. Golay and M. Büschi, The Right to Food and Global Strategic Frameworks: The Global Strategic Framework for Food Security and Nutrition (GSF) and the UN Comprehensive Framework for Action (CFA) (Rome: Food and Agriculture Organization, 2012), p. 35; Institut d’Estadística de Catalunya (see note 35).
[44] E. Marchis, J. M. Torres, T. Benesch, et al., “Interventions Addressing Food Insecurity in Health Care Settings: A Systematic Review,” Annals of Family Medicine 17/5 (2019).
[45] C. Borrell and L. Artazcoz, “Las políticas para disminuir las desigualdades en salud,” Gaceta Sanitaria 22/5 (2008); M. I. Vidal Sánchez, R. Magallón Botaya, C. B. Benedé Azagra, et al., “¿Qué hacemos y qué podríamos hacer desde el sistema sanitario en salud comunitaria? Informe SESPAS 2018,” Gaceta Sanitaria 32 (2018).