Gender-Based Violence Is a Human Rights Violation: Are Donors Responding Adequately? What a Decade of Donor Interventions in Colombia, Kenya, and Uganda Reveals
Volume 24/2, December 2022, pp. 29-45 | PDF
Clarisa Bencomo, Emily Battistini, and Terry McGovern
Abstract
Gender-based violence (GBV) is a violation of human rights and must be addressed as such. This paper examines whether donor practices align with a rights-based approach, using data from our comprehensive study of foreign funding flows related to GBV in Colombia, Kenya, and Uganda from 2010 to 2020. By analyzing data from 1,180 grants—and providing parallel analyses of the state of GBV, and GBV reporting and interventions in each country—we demonstrate donors’ role in shaping GBV outcomes and their consequent duty to address policies and practices that violate rights. Accordingly, we propose changes in donor practices to promote realization of the right to freedom from violence.
Introduction
Gender-based violence (GBV) is violence directed against a person because of their gender or violence that affects persons of a particular gender disproportionately.[1] It includes sexual, physical, psychological, and economic violence, and is a human rights violation that overwhelmingly affects women, girls, and gender-diverse people, with devasting impacts. Rates of GBV increased starkly during the COVID-19 pandemic as governments offered confused and inadequate responses to predictable shifts in vulnerability. Interventions aimed at reducing GBV prevalence and improving care for survivors remain grossly under-resourced.[2] Calls for increased GBV funding—and for “what works” to prevent and respond to GBV—are common, even as new commitments to eliminate GBV gradually emerge.[3] In many low- and middle-income countries, foreign donors are and will be a major source of funding for these initiatives, making it critical to understand who and what they fund and whether it aligns with human rights principles.
Currently, there are no comprehensive assessments of how much money donors direct to GBV, what interventions they support, how those interventions are evaluated, or whether they take a rights-based approach. International human rights law still does not reflect a clear definition of GBV in all its forms, despite growing recognition that a narrow focus on certain forms of violence against women fails to capture the myriad and intersecting ways women experience violence and contributes to protection gaps for gender-diverse people.[4] Donor states must be held accountable for aid policies that fail to address GBV or are complicit in sustaining domestic laws, policies, and norms that violate international human rights principles. While human rights advocates are increasingly aware of transnational threats to the right to health, especially those driven by multinational nonstate actors or multilateral institutions, research on international donors’ impact on GBV remains limited.[5]
This study—which focuses on the GBV funding and intervention landscapes in Colombia, Kenya, and Uganda from 2010 to 2020—seeks to fill this gap. We argue that donor states have transnational obligations to address GBV and contextualize these obligations by assessing their funding practices, highlighting how they often fail to prioritize human rights principles of nondiscrimination, transparency, participation, and accountability. We conclude with recommendations to improve donor practices.
Methodology
We selected Colombia, Kenya, and Uganda as examples of regionally significant countries with high rates of GBV and histories of humanitarian and development aid for GBV interventions. We reviewed human rights principles relating to GBV and transnational duties; GBV statistics and tracking systems in Colombia, Kenya, and Uganda; peer-reviewed and gray literature on the state of GBV, GBV funding, and GBV interventions; and all publicly available data on bilateral, multilateral, and foreign private foundation GBV funding streams relevant to the three countries of interest from 2010 to 2020, including development and humanitarian funding.
We constructed and analyzed a comprehensive database of 2010–2020 foreign GBV funding in the three countries using multiple databases, including those sponsored by Candid, Human Rights Funders Network, the European Union, the European Civil Protection and Humanitarian Aid Operation, the United Nations (UN) Office for the Coordination of Human Affairs, and the Organisation for Economic Co-operation and Development.
Where possible, we restricted searches to our targeted geographical area, time period, and populations of interest, and then used the following search terms: GBV or violence or gender-based or FGM or genital or FGC or marriage or IPV or trafficking. Where the database did not allow for this type of term entry, we either restricted our search to the relevant category (e.g., “ending violence against women and girls”) or did manual searches of all grants in the relevant geographical areas and time periods. This approach was as comprehensive and inclusive as possible, but still had unavoidable limitations: often, donors shifted their category descriptions over time, making search restrictions more relevant in some time periods than in others.
To fill any resultant gaps, we conducted parallel searches of supplementary materials from multilateral, bilateral, and foundation donors. The donors that yielded viable information include the UN Trust Fund to End Violence against Women, the UN Development Programme, the UN Population Fund, the World Bank, regional development banks, the United States Agency for International Development (USAID), Global Affairs Canada, the United Kingdom, the Ford Foundation, and the Global Fund for Women.
We reviewed the resulting funding descriptions to ensure they were inclusive of specific sub-categories of GBV—including domestic violence, intimate partner violence (IPV), non-partner sexual violence, physical abuse, sexual abuse, forced or coerced sex, genital trauma, female genital mutilation/cutting (FGM/C), trafficking, and child abuse and targeted violence against women, girls, adolescent girls/young women, and LGBTQI+ people—and removed funds that did not specifically address GBV, such as humanitarian funding for general violence or child protection programs.
This approach identified 1,180 grants relevant to GBV: 393 in Colombia, 400 in Kenya, and 387 in Uganda. One author then reviewed and coded each grant according to donor type, recipient type, funding period, target audience, type of intervention, type of evaluation, and focus on prevention or response. The same author used available project information to determine which grants took GBV as their central focus; these grants were coded as “GBV primary” and used to develop a restricted database that we compared to the above totals.
Some databases or donors listed discrete funding years, whereas others provided a time range: in the latter cases, we privileged disbursement year; otherwise, the first grant year was taken as default. Where disbursement and commitment numbers differed, disbursements were privileged. All currencies were converted into US dollars, according to the average conversion rate in the year of disbursement.
Situating GBV in international law
Women’s right to be free from gendered violence is well recognized in international law upholding the right to health and prohibiting torture and discrimination, and is an essential condition for the enjoyment of other human rights and fundamental freedoms.[6] The Committee on the Elimination of Discrimination against Women’s General Recommendation 35 cites opinio juris and state practice as suggesting that the prohibition of GBV against women has evolved into a principle of customary international law.[7] Regional human rights conventions ratified by Colombia, Kenya, Uganda, and most donor states (the United States being a notable exception) further clarify state responsibilities.[8]
This international legal framework is bolstered by decades of political commitments stressing integrated, evidence-informed GBV prevention. The 1994 International Conference on Population and Development affirmed the elimination of all forms of violence against women as a cornerstone of population and development programs.[9] The 1995 Platform for Action adopted at the Fourth World Conference on Women in Beijing then outlined detailed strategic objectives for integrated measures to end violence, including conducting and disseminating research on its causes, its consequences, and the effectiveness of preventive measures.[10] More recently, Sustainable Development Goal 5.2 set indicators for progress eliminating intimate partner and sexual violence against women and girls.[11]
States and international actors have immediate and progressive responsibilities to ensure these rights, including duties of international assistance and cooperation; to not “reinforce or condone legal, procedural, practical or social barriers … in the recipient countries”; and to avoid retrogressive measures.[12] Emerging norms also favor foreign states acting when a national government is unable or unwilling to prevent violations, and when those violations are widespread or severe, although the exact edges of responsibility are debated.[13]
International cooperation should be informed by three interrelated human rights and health governance concepts: conducting and disseminating research relevant to health priorities; maintaining transparency via access to information about government program performance; and sharing the benefits of scientific progress. Article 15 of the International Covenant on Economic, Social and Cultural Rights affirms “the right of everyone … to enjoy the benefits of scientific progress and its applications,” and the duty of states to take “steps … necessary for the conservation, the development and the diffusion of science.”[14] This right, based on principles of participation and transparency, is an essential tool for realization of the right to health and creates extraterritorial obligations on states negotiating multilateral and bilateral cooperation agreements.[15] Participation in the planning and implementation of health care is both a right and a duty of individuals alone and collectively.[16]
The state of GBV in Colombia, Kenya, and Uganda
Globally, GBV is its own pandemic: the World Health Organization estimates that 736 million women had been victimized by IPV at least once in their lives as of 2018. The burden is unequally shared: GBV disproportionately affects low- and middle-income countries such as Colombia, Kenya, and Uganda.[17] The number of GBV survivors is likely much higher; this statistic is pre-COVID-19 pandemic, excludes other forms of GBV such as femicide and sexual harassment, and undercounts at-risk populations such as women with disabilities and migrant, Indigenous, older, and transgender women. Stigma and risks around reporting violence where legal systems are weak or discriminatory further reduce our understanding of GBV’s scale and scope. Together, these limitations reduce our ability to assess the impact of specific GBV policies and interventions and their suitability for particular populations. This undermines progressive realization of the right to health by depriving policy makers and affected populations of meaningful baselines and analyses of the most effective local interventions and by hindering effective transnational cooperation.
A hidden toll of GBV in Colombia, Kenya, and Uganda
The best and most recent estimates suggest that GBV prevalence is highest in Uganda, where 50% of women experience IPV in their lifetimes and 30% of women have experienced IPV in the past 12 months. Rates are only marginally better in Kenya, where 40.7% of women experience IPV in their lifetimes and 25.5% have experienced IPV in the past 12 months. Colombia has the highest gender equality index of the three, but even there the numbers are 33.3% and 18.3%, respectively.[18] While IPV against women is the most prevalent form of GBV, a narrow focus on it excludes many other GBV components and often discriminates based on gender, age, disability, religion, ethnicity, and status. Undercounted human rights violations include physical and sexual non-partner violence; economic and psychological violence; harmful traditional practices such as early marriage and FGM/C; and all GBV experienced by LGBTQI+ people, as well as other at-risk and undercounted populations (e.g., migrants and refugees, people with disabilities, sex workers, domestic workers, and women and gender-diverse communities living with HIV). Moreover, the “most recent” data date from 2014 to 2016—meaning these estimates fail to capture COVID-19-related spikes in GBV.
Gaps in legal frameworks and implementation
Both Kenya and Uganda recently passed seminal pieces of GBV legislation. In Kenya, the 2006 Sexual Offences Act makes extramarital rape punishable by a minimum of 10 years in prison; in Uganda, the 2010 Domestic Violence Act recognizes domestic violence in multiple forms and categorically states that there can be no “consent” to such acts.[19] Both acts have significant limitations. Under Kenya’s Sexual Offences Act, only penetration by the genital organ counts as rape, with other penetration classified as sexual assault; the act also excludes marital rape, which is considered a civil offense under separate legislation.[20] Similarly, neither Uganda’s Domestic Violence Act nor its Penal Code address marital rape, and the Domestic Violence Act ignores violence committed by others on behalf of the spouse.[21] Ugandan law also allows traditional practices such as child marriage, bride price, and widow inheritance—even as both Kenya and Uganda continue to criminalize same-sex relationships.[22] Furthermore, both countries have plural legal systems whereby tribal and customary authorities retain jurisdiction over GBV cases.[23] The problem is exacerbated by over-taxed, under-resourced, and often corrupt judicial systems—which remain difficult to navigate and access. Uganda has no specialized courts for domestic violence, resulting in mishandling and backlogs, and its police and judicial personnel often lack awareness of or refuse to adhere to existing laws.[24] Kenya is similarly plagued by high court costs, long waits, and a perceived culture of impunity—even as organizations that offer complementary services remain under-resourced and “gender desks” designed to increase reporting fail to offer privacy or security for survivors.[25] These are clear violations of the prohibition on discrimination and the duty to ensure equal access to justice.
Colombia is progressing toward a legal and policy framework that addresses GBV. It criminalizes rape, marital rape, and domestic violence and, in 2008, adopted legislation establishing a women’s right to live free from violence and requiring the provision of health and social services to survivors.[26] Colombia is also the only country of the three to decriminalize same-sex relationships. However, implementation gaps in Colombia are severe, particularly in areas most affected by armed conflict and forced displacement. State institutions are often weak, absent, or implicated in rights violations—meaning that government capacity to deliver on legal frameworks for equality is low, especially where the most marginalized communities live.[27] This denies women, girls, and gender non-conforming people their right to effective protection against discrimination.
Gaps in health sector coverage
The availability of medical and psychosocial services in all three countries remains inadequate, especially in rural and conflict-affected areas. While all three have committed to providing timely GBV health services—including emergency contraception, post-exposure prophylaxis, treatment of sexually transmitted infections, and trauma counseling as part of broader sexual and reproductive health (SRH) care—these services are limited and unequally distributed. Kenya’s one-stop center (OSC) model of service provision, with OSCs run within hospital systems or by nongovernmental organizations (NGOs), affords minimal health and counseling services for GBV beyond hospital-based OSCs in Nairobi and Kisumu. This leaves rural areas heavily dependent on weak referral pathways that are difficult to navigate.[28] Uganda relies primarily on referral networks, but services are sporadic in rural areas and cross-sector coordination is poor. Facilities lack necessary infrastructure, including private spaces to examine women; victims are often asked to pay for forensic examinations; and rape kits and emergency contraception are limited by stockouts.[29] In Colombia, challenges remain in accessing universal health insurance, with most donor resources currently funneled to humanitarian response and low support for incorporating GBV into other health services.[30]
Flawed and inadequate GBV data monitoring systems
Colombia, Kenya, and Uganda have all committed to monitoring GBV and strengthening existing GBV data management systems.[31] But current systems are limited and discriminatory, and progress in implementation has been uneven.
Currently, only Uganda has established a national GBV database. It collates information from a domestic violence module of the Demographic and Health Surveys, last implemented in 2016; studies conducted by the Bureau of Statistics; and GBV incident reports filled out by survivors at service provision points such as police stations and shelters.[32] The database has been in operation since 2014, but only a fraction of district governments use the database, which requires internet access and often fails to integrate relevant data streams.[33] The database also privileges IPV over less visible forms of GBV and discriminates by excluding LGBTQI+ individuals and other vulnerable subpopulations.[34]
Kenya recently committed to the development of a centralized GBV data management system.[35] Kenya’s 2014 National Policy for Prevention and Response to Gender-Based Violence highlights multiple data sources, including quarterly reports of different ministries, departments, and agencies; population-based health surveys; and other large-scale surveys such as the Demographic and Health Survey. Coordinating these data sources remains difficult.[36] Despite recognizing GBV as a constellation of behaviors that includes physical, sexual, emotional/psychological, and socioeconomic violence, Kenya privileges sexual violence and IPV in practice. Its Demographic and Health Survey relies on a domestic violence module last implemented in 2014 and scheduled for inclusion in 2022, and its prevention and response framework emphasizes sexual violence as the starting point for a more integrated GBV monitoring system.[37] Kenya also discriminates by excluding LGBTQI+ individuals and other vulnerable subpopulations from its reporting.[38]
Colombia represents a different data collection model: it relies heavily on the legal and judicial system, and on bilateral donors such as USAID, rather than on its Demographic and Health Survey module, which was last implemented in 2015. Prevalence of sexual violence is typically estimated from the number of forensic exams conducted in legal cases, as well as from preliminary data on IPV, femicide, and sexual violence published by the National Institute of Legal Medicine and Forensic Sciences.[39] This presents difficulties related to under-reporting and lack of centralized, governmental coordination. While USAID-sponsored efforts and country-level surveys run through the National Administrative Department of Statistics are inclusive of less visible forms of GBV and LGBTQI+ individuals, no baseline or target numbers have been set in these categories. USAID has outlined indicators to address GBV, but it is unclear how much in-country participation and ownership there is over this process.
In all three countries, deprioritization of non-partner and less visible forms of GBV and delays in data collection and reporting limit understanding of the interrelationships between various components of GBV.[40] It also results in a substantial underestimation of the problem—which the field can scarcely afford, given that IPV, while privileged, is often inadequately measured.[41] The discriminatory neglect and exclusion of vulnerable populations such as LGBTQI+ individuals and people with disabilities is retrogressive and further undermines their right to participate in and benefit from scientific progress, while hindering accountability for serious human rights violations.
These problems are not unique to Colombia, Kenya, and Uganda. Recent studies in other countries emphasize the need for improved GBV monitoring—often favoring centralized national databases that frequently, regularly, and systematically collate data from diverse multisectoral sources—while assessing vulnerability to all forms of GBV within all at-risk populations.[42] At a minimum, progressive realization requires governments to identify baselines and conduct timely measurements to assess the availability, accessibility, acceptability, and quality of its strategies and interventions. Such data are an essential prerequisite to ensuring that development aid is efficiently, effectively allocated in accordance with human rights principles.[43]
The GBV funding landscape in Colombia, Kenya, and Uganda
Our analysis of 2010–2020 donor disbursements highlights five aid-related factors undermining efforts to ensure the right to freedom from gendered violence.
An opaque funding landscape
The majority of GBV donors reviewed fell short of human rights transparency principles, creating barriers to affected people’s participation in planning, implementing, and benefiting from these interventions. Even the most comprehensive databases provide limited and often conflicting information. Neither GBV nor violence against women are consistently included as searchable categories, and GBV-related search terms capture only a subset of the phenomenon. Other crucial information—including basic information on recipients or project terms—is not consistently available. The proliferation of relevant but non-overlapping search locations adds to the confusion and opacity of the landscape—even as the usefulness of available data is compromised by the difficulty of ascertaining what percentage of large multisectoral and multi-issue grants actually goes to GBV. As a result, analyses that draw data from all grants with a GBV component vastly overstate the amount of GBV funding actually available, as many larger grants include only small flows to GBV. Similarly, our restricted database of “GBV-primary” grants necessarily understates the amount of GBV funding in the system.
Few grant databases or project descriptions provide information about the evaluation methods or indicators that donors and recipient organizations use to assess impact. These data can sometimes be found in longer project documents, but these documents are inconsistently available—making across-the-board conclusions difficult to draw. This dearth of accessible, rigorous data on the impact of GBV funding flows and interventions stifles progress in developing and refining evidence-based policies, promoting meaningful participation, and sustaining effective transnational cooperation. The problem is exacerbated by the dearth of funding for GBV research generally.
Limited and uncertain funding
Overall, the amount of GBV funding flowing into Colombia, Kenya, and Uganda is small, especially in comparison to total aid to each country. Disbursements to Colombia significantly outpace those to Kenya and Uganda in both absolute and relative terms, despite Colombia’s lower GBV prevalence rates.
Between 2010 and 2020, Colombia received US$561,783,792 in total external GBV funding, of which US$142,960,617 was GBV-primary funding; Kenya received US$275,981,335 in total GBV funding, including US$92,003,048 in GBV-primary funding; and Uganda received US$134,238,870 in total GBV funding, including US$124,515,244 in GBV-primary funding. GBV-primary grants account for less than 1.5% of aid to Colombia, 0.5% of aid to Kenya, and 1% of aid to Uganda; when total GBV grants are considered, the figures rise to 5.9%, 1.6%, and 1.1%, respectively.[44]
An examination of individual grants and trends over time (Figure 1) reveals this to be due primarily to high levels of funding that Colombia received in support of its peace-building initiatives and the Venezuelan crisis. Kenya received similar influxes of humanitarian aid for management of internal conflicts, election processes, and the refugee crisis; this funding accounts for Kenya’s higher total GBV funding relative to Uganda despite its lower prevalence rate, as well as for the spikes in Kenya’s trendline.
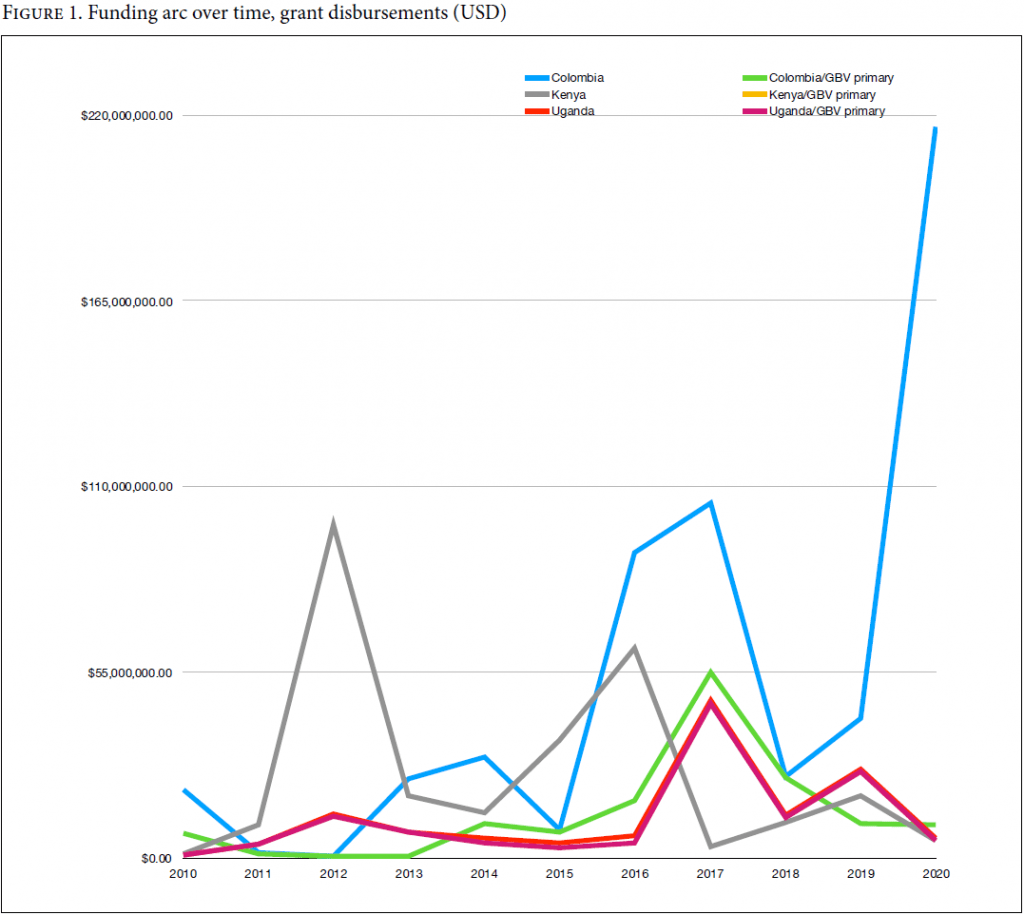
GBV’s secondary status relative to other priorities explains why cross-country differences in total GBV funding are more extreme than GBV-primary differences—while also suggesting that GBV-primary funding is a closer approximation of the actual amount of money for GBV flowing into all three countries. This is reinforced by examining Uganda, which experienced fewer fluctuations in humanitarian aid and more consistent levels of total GBV and GBV-primary funding. The modest echoes in GBV-primary funding accompanying the spikes in total GBV funding in Colombia and to a lesser extent Kenya suggest that inclusion of GBV in funding packages related to humanitarian or other emergencies does boost GBV efforts in-country—even if this boost is temporary and followed by a return to a relatively modest baseline.
A narrow donor ecosystem
In all three countries, bilateral and multilateral donors exert a dominant influence on the GBV funding landscape. In Colombia, these donors are responsible for the overwhelming majority of both total GBV and GBV-primary grant disbursements; this also holds true in Kenya and Uganda, though funding flows from foundations are more significant in those two countries (Figure 2). This suggests that Colombia’s decades-long civil war had a chilling effect on foundation investments, which were slow to rebound post-2016. In Uganda, where we see fewer fluctuations in humanitarian aid, foundation funding claims a greater share of the whole but is still outpaced by bilateral and multilateral aid. Our residual “others” category, consisting largely of international NGO and funding collaborative disbursements, accounts for a vanishingly small share of aid.
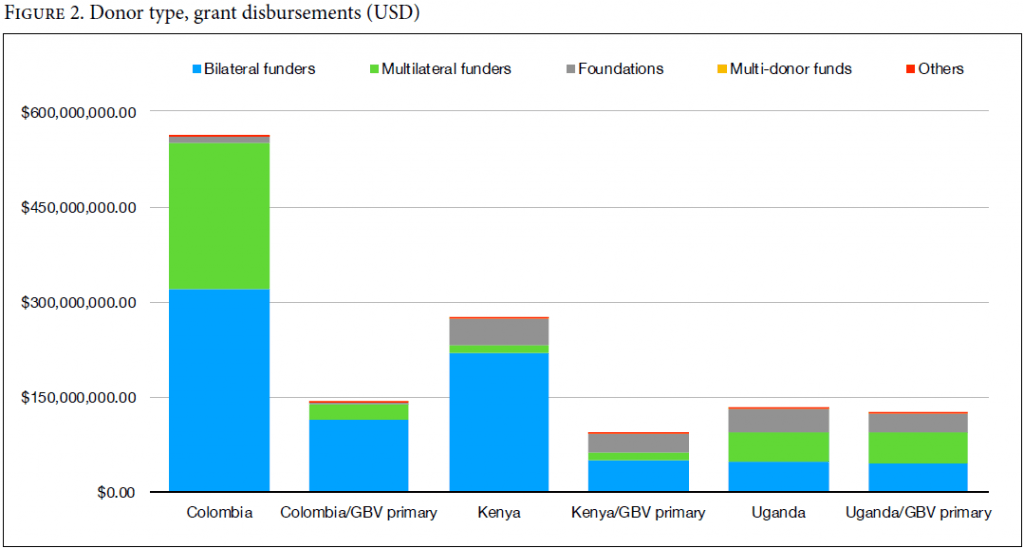
Foundations dominate when we look at the number of grants awarded rather than grant disbursements in US dollars—despite a relative deficit in Colombia (Figure 3). This suggests that foundations and other categories of donors—including multi-donor funds, funding collaboratives, and international NGOs—are giving larger numbers of small grants, whereas bilateral and multilateral donors are giving smaller numbers of large grants.
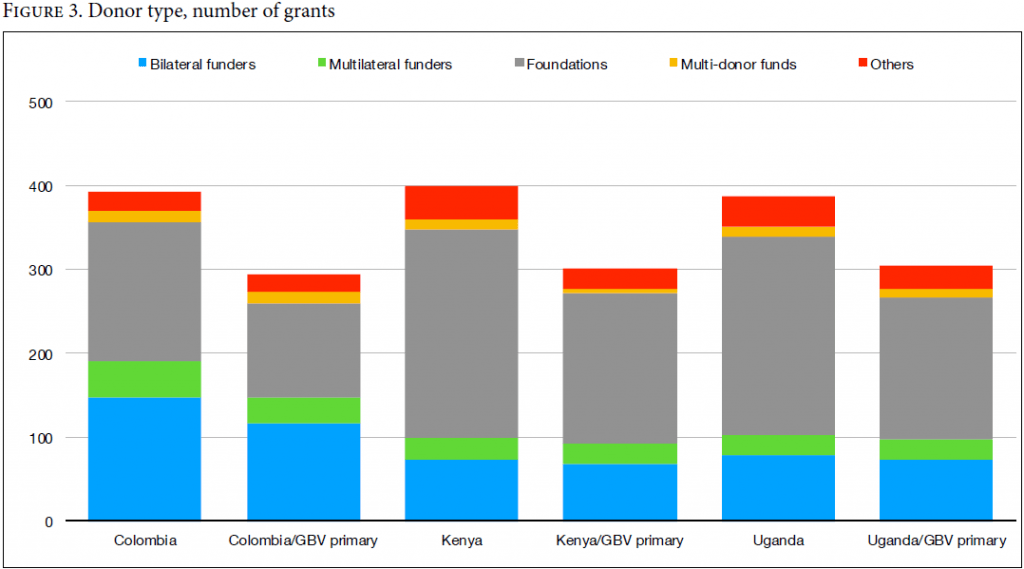
An analysis of disbursements under US$25,000 supports this point. Foundation funding dominates this category across all three countries, accounting for 63.6% of total GBV and 55.1% of GBV-primary funding in Colombia, 73.9% and 72.3% in Kenya, and 66.6% and 60.6% in Uganda. This implies a funding landscape with a multiplicity of actors, even if the relative influence of those actors is dwarfed by bilaterals and multilaterals.
This dominance of bilateral and multilateral donors creates risks to program sustainability, with potentially retrogressive impacts when a large donor sharply reduces aid. In the absence of other flexible funding for local organizations, a proliferation of small-foundation grants to discrete organizations, projects, and priorities can increase competition within country-level systems, undermining impact and making coordination more difficult. Failure to anticipate and mitigate such risks undermines progress toward eliminating GBV and can create greater harms.
A predominance of international recipients
A look at the organizations that receive aid reveals a predominance of groups headquartered outside these countries and, to a lesser extent, national governments (Figure 4). In Colombia, total GBV funding is flowing primarily to the Colombian government and UN agencies or bilaterals—though GBV-primary funding is much more concentrated on international and regional NGOs and other categories of recipients (notably, national and regional networks). This is consistent with what we know about the post-2016 spikes in Colombia’s humanitarian aid and confirms that much of the “primary” GBV funding is going to international and regional NGOs and networks with an active presence in the region. The picture is similar in Kenya: total GBV funding is split between international/regional NGOs and multilaterals/bilaterals, with international/regional organizations looking more dominant when the analysis is restricted to GBV-primary grants. In Uganda, the recipients are more evenly split from the outset, with particularly large shares of both total GBV and GBV-primary funding going to international and regional NGOs and the Ugandan government. In all three countries, funding is also flowing to many unspecified recipients, another marker of limited donor transparency and accountability.
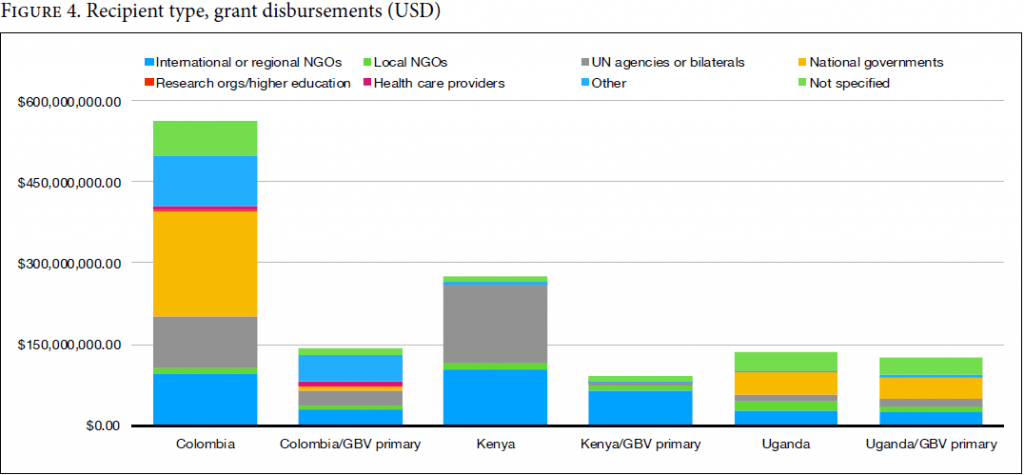
Across all three countries, we see a dearth of funding awarded directly to local organizations, a likely outcome of the predominance of multilateral and bilateral donors with complex application requirements. Limited donor transparency prevents us from determining what percentage of these awards are project versus flexible support or include sub-awards to local NGOs; both project support and sub-awards often have restrictive deliverables, application requirements, and reporting requirements. Limited support for local organizations has implications for the extent to which GBV interventions are accessible to marginalized populations, provide meaningful opportunities for participation, and benefit from and reflect their knowledge and perspectives.
(Under)privileged populations and interventions
In all three countries, the majority of donor-released project descriptions reference multiple components, sectors, types of interventions, and populations. Relatively few projects demonstrate significant engagement across sectors and components. Thus, a humanitarian project that includes both health and water components and encompasses basic health care; water and sanitation; nutritional supplements; and medical and legal services for GBV survivors is unlikely to integrate its GBV interventions into all activities.
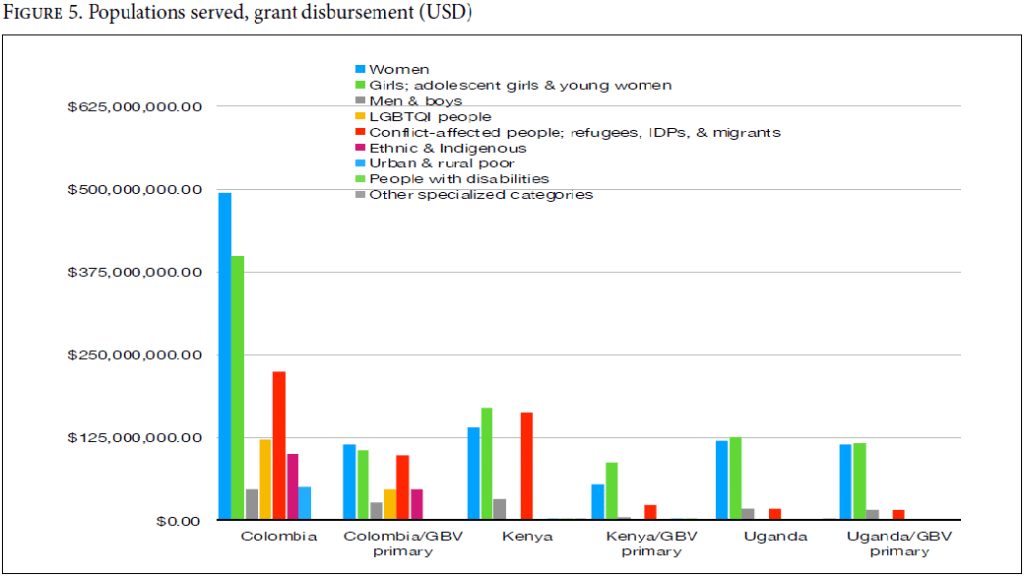
Similarly, even where project documents are available, they rarely provide details on how much funding is going to any specific population or intervention type. For example, in a grant that serves both women and adolescent girls, it is impossible to differentiate how much money is allocated to each. We can, however, give a fairly clear picture of where money is not flowing.
Populations served. A significant portion of GBV funding is directed toward women, girls, and adolescent girls/young women in all three countries (Figure 5). We also see an emphasis on conflict-affected people and refugees, internally displaced people, and migrants in overall GBV funding to Colombia and Kenya. More striking are the groups that are receiving far less attention—notably, LGBTQI+ people and those with disabilities. Both populations experience systemic discrimination that creates a duty of special protection.[45]
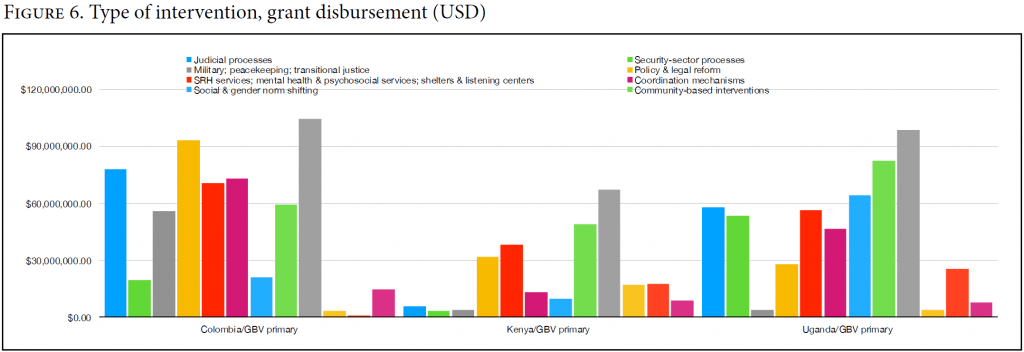
Types of interventions. When we focus on GBV-primary disbursements, we see that some categories of intervention—such as policy and legal reform, SRH and psychosocial services and shelters, community-based interventions, and civil society organization (CSO) capacity-building—are more likely to attract funding (Figure 6). There are also areas of relative neglect, such as social and gender norm shifting and research.
In Colombia, major funding streams are directed toward judicial processes; military, peacekeeping, and transitional justice; policy and legal reform; SRH services, mental health and psychosocial services, and shelters and listening centers; coordination mechanisms; community-based interventions; and CSO capacity-building.
In Kenya, the concentrations are in policy and legal reform; SRH and psychosocial services and shelters; community-based interventions; and CSO capacity-building.
In Uganda, the influxes are toward judicial processes; security-sector processes; policy and legal reform; SRH and psychosocial services and shelters; coordination mechanisms; social and gender norm shifting; community-based interventions; and CSO capacity-building.
These broad clusters reflect variations on OECD aid codes, but reveal nothing about how efficiently or effectively funding is allocated within those groupings. This raises questions about the availability, accessibility, acceptability, and quality of actual interventions, as we highlight in our discussion below.
Consequences for GBV interventions
Just as GBV is a complex problem, the GBV intervention landscapes in Colombia, Kenya, and Uganda are complex and multifaceted. Unlike the integrated approach envisioned in the Beijing Platform for Action, these efforts are often poorly coordinated and heavily reliant on external funding and governance; this frequently results in a chaotic mix of short-term projects rather than the advancement of sustainable, long-term goals. The vacuum left by national governments also overburdens CSOs, which are poorly supported relative to need.
Legal frameworks and judicial systems
States have an immediate obligation to end discrimination in legal and judicial systems, and all three countries have adopted legal frameworks that reflect some global standards related to gender equality—often as a result of local feminist advocacy.[46] Further legislative action is urgently needed in Kenya and Uganda to meet basic human rights standards, and the gap between policy and implementation in all three countries remains tremendous, restricting real progress toward eliminating GBV.
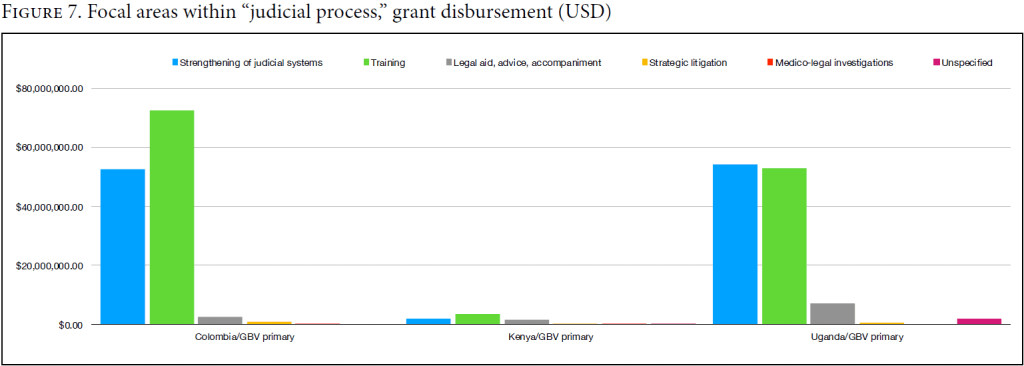
Given the hard-to-navigate systems previously discussed, one would expect GBV interventions in all three countries to emphasize legal aid and accompaniment for victims. However, when we restrict our analysis to GBV-primary grants that include funding for judicial processes, we find that most large grants emphasize training programs for police, prosecutors, judges, or other institutional actors along with an amorphous vision of “systems strengthening.” Litigation and legal accompaniment is more typically funded through small-foundation grants (Figure 7). This is problematic given that training in the absence of other enabling interventions is unlikely to have a material impact on these countries’ legal systems.
Access to safe housing
High levels of health sector dependence on donor funding—76% in Uganda and 23% in Kenya (current data not available for Colombia)—underscore the critical role of donors’ funding decisions and policies and the duties this creates.[47] Our analysis finds that although the broad category of SRH, mental, and psychosocial services and shelters is relatively well funded, only five grants provide resources for shelters, despite their pivotal role in providing safety and facilitating GBV reporting and access to justice and care. Shelters are notably missing or under-resourced in Kenya, and serve primarily as a temporary stop-gap for conflict-affected survivors in Colombia. There are only 13 GBV shelters serving all 134 districts of Uganda.[48]
Program design and infrastructure
The governments of Colombia, Kenya, and Uganda do not adequately coordinate or commit to gender-transformative GBV interventions, effectively ceding the field to donors, international NGOs, and under-resourced community-based organizations. This creates immense challenges for truly integrated multisectoral approaches to GBV; effective evaluation and learning; and long-term social and gender norm shifting.
Coordination and evaluation. Coordination within and across sectors is a major challenge in all three GBV intervention landscapes. While there is clear recognition of the need for comprehensive, multi-component, and multisectoral GBV interventions, these interventions rarely exist in practice. Instead, projects superficially engage many sectors without offering an integrated multisectoral approach. Lack of donor coordination and strategy setting contributes to the confusion, with foundation donors rarely included in multilateral and bilateral coordination discussions.[49]
Country-level frameworks to assess both progress toward the elimination of GBV and the effectiveness of GBV interventions are weak. Donors contribute to this weakness through under-investment in research and a limited vision of monitoring and evaluation. This is reflected in multiple evaluation frameworks that compete and overlap; rely on narrow output indicators, such as the number of people trained, rather than broader outcome or impact measures; and privilege evidence from large-scale randomized controlled trials. (One recent report, funded by the United Kingdom, included data exclusively from randomized controlled trials and quasi-experimental studies.[50]) This approach provides one type of information, but not the only one—and places significant burdens on local, grassroots organizations that often have the most innovative programming.
Reliance on the UN and international NGOs over local CSOs. Multilateral and bilateral donor preferences for funding UN agencies, international NGOs, and themselves steer money away from groups with direct knowledge of their communities and promising opportunities to influence change. While many agencies and international NGOs subcontract some portion of their work to local groups, subcontracting reinforces the trend toward short-term, project-based work and fosters the proliferation of competing projects, organizations, and priorities. It also limits local participation in program design, filtering out insights from frontline groups that are often working in multiple sectors and doing the preventive work of awareness-raising, capacity-building, empowerment, and norm shifting.
Limited support for long-term change. GBV prevention efforts such as social and gender norm shifting tend to be under-resourced relative to other GBV interventions. This is true generally (Figure 6)—but it is also an artifact of some flagship programs providing short-term project support, and their potential reluctance to adopt gender-transformative strategies. The US-funded DREAMS Initiative, which ran in both Kenya and Uganda and aims to reduce the prevalence of HIV and AIDS in adolescent girls, has not publicly supported legal and policy reforms and programs to decriminalize LGBTQI+ populations and prioritize gender-diverse adolescents, who face high risk of GBV and HIV.[51] It also drops recipients who fail to meet rigid annual performance targets.
Even well-tested gender-transformative interventions like SASA!, a GBV prevention program developed by the Ugandan NGO Raising Voices, can fail during adaptation and scale-up when donors modify core aspects to meet shortened timelines.[52] Large power differentials also plague relationships between local and international actors. Community-based programs are often dependent on underfunded national governments and face pushback if they disrupt existing power relations. Lack of local buy-in is also a significant and recurring issue in systems dominated by international NGOs. This is exacerbated in conflict-affected countries like Colombia, where instability has a chilling effect on both foundation investments and international NGO programming (Figure 2).
Conclusion
This analysis highlights critical ways that donor decisions can influence and reinforce systems and processes that limit progress toward fulfillment of the right to health in Colombia, Kenya, and Uganda. It points to the need for greater donor transparency and accountability surrounding the direct and indirect human rights impacts of aid policies. This is especially urgent as GBV rates rise and economic crises fuel pressures to adopt retrogressive health and aid policies.
Donors should act urgently to revise policies that promote or are complicit in discrimination and to ensure the transparency and participation required for scientific progress and human rights accountability. This will necessitate greater transparency about their own funding flows and programmatic interventions, as well as a fundamental shift in how they approach transnational cooperation. This includes committing to the following:
- Increase transparency about their own funding strategies and disbursements, providing timely information on what and who is funded, how interventions are selected for funding, and what outcomes and learnings those investments produced.
- Ensure that shifts in funding strategies do not result in retrogressive outcomes.
- Invest in true participatory research on GBV intervention adaptation and scale, and in strengthening national GBV data monitoring systems; both are crucial to inform national GBV laws and policies and intervention selection and adaptation. Data monitoring systems should provide timely, disaggregated information that is inclusive of all forms of GBV and allows for analysis of intersectional drivers of GBV, especially as they affect stigmatized and marginalized populations.
- Localize GBV programming and strengthen the GBV prevention ecosystem by directing more funding to community-based organizations and networks doing gender-transformative work and increasing their participation in program design, implementation, and evaluation. This will require revising funding processes to be more accessible, investing in recipient organizational capacities, and prioritizing longer-term, flexible funding.
- Support inclusive, transparent coordination processes and structures that facilitate timely information sharing and participatory design of GBV strategies, interventions, and measurement, evaluation, research, and learning frameworks. Sustaining the coordinated, comprehensive, multisectoral, and multi-component programming necessary to eliminate GBV requires equitable participation of all types of donors and recipients.
- Support urgently needed national legal and policy reforms and address implementation gaps through funding, advocacy, and technical assistance. Increased support for legal accompaniment and safe shelter are crucial to addressing implementation gaps.
Truly committing to the elimination of GBV means committing to a field-wide paradigm shift in which greater transparency, coordination, and accountability are privileged by all actors. Multilateral and bilateral donors have an outsized impact here—often in discriminatory directions—giving them a corresponding duty to act.
Acknowledgments
We thank the Ford Foundation for its support of our research, and Malia Maier and Mahnoor Nasir for their research assistance.
Clarisa Bencomo, MA, is associate director of the Global Health Justice and Governance Program, Department of Population and Family Health, Mailman School of Public Health, Columbia University, New York, United States.
Emily Battistini, MD, MPH, MA, is an independent research affiliate of the Global Health Justice and Governance Program, Department of Population and Family Health, Mailman School of Public Health, Columbia University, New York, United States.
Terry McGovern, JD, is Harriet and Robert H. Heilbrunn Professor and Chair, Department of Population and Family Health, and director, Global Health Justice and Governance Program, Mailman School of Public Health, Columbia University, New York, United States.
Please address correspondence to Terry McGovern. Email: tm457@cumc.columbia.edu.
Competing interests: None declared.
Copyright © 2022 Bencomo, Battistini, and McGovern. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction.
References
[1] United Nations High Commission for Refugees, “Gender-Based Violence,” https://www.unhcr.org/en-us/gender-based-violence.html; European Commision, “What Is Gender-Based Violence,” https://ec.europa.eu/info/policies/justice-and-fundamental-rights/gender-equality/gender-based-violence/what-gender-based-violence_en.
[2] Columbia University Global Health Justice and Governance Program, Missing in Action: COVID-19 Response Funding for GBV and SRH in Five Countries (2020), https://www.publichealth.columbia.edu/sites/default/files/multi-country_funding_2-pager_9_april_2021.pdf; N. John, T. McGovern, M. Mwangi, et al., “COVID-19 and GBV: Hard-to-Reach Women and Girls, Services, and Programmes in Kenya,” Gender and Development Journal (2021).
[3] L. Michau, J. Horn, A. Bank, et al., “Prevention of Violence against Women and Girls: Lessons from Practice,” Lancet 385/9978 (2015); UN Women, “Trailblazing Leaders Commit to End GBV, Drive Equality in Technology and Innovation, and Ensure Economic Justice and Rights for Women and Girls at the Generation Equality Forum,” (2021), https://www.unwomen.org/en/news/stories/2021/7/news-gef-paris-leaders-commit-to-end-gbv-drive-equality-in-tech-and-ensure-economic-justice.
[4] T. Ziniakova, “Gender-Based Violence in International Human Rights Law: Evolution
towards a Binding Post-binary Framework,” William and Mary Journal of Women and the Law 27/3 (2021).
[5] K. M. Gopakumar, “SDG 3: Corporate Influence on the Global Health Agenda,” in B. Adams, R. Bissio, D. Cibrario, et al. (eds), Justice beyond Rhetoric: Time to Overcome Contradictions and Hypocrisy in the COVID-19 Crisis (Beirut: Civil Society Reflection Group, 2021).
[6] Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948), arts. 5, 7, 25; Human Rights Council, Violence against Women, its Causes and Consequences: Report of the Special Rapporteur on Violence against Women, Its Causes and Consequences, UN Doc. A/HRC/41/42 (2019) paras. 26–57; Committee on the Elimination of Discrimination against Women, General Recommendation No. 19, UN Doc. A/47/38 (1993), paras. 6–7.
[7] Committee on the Elimination of Discrimination against Women, General Recommendation No. 35, UN Doc. CEDAW/C/GC/35 (2017), para. 2.
[8] Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa (Maputo
Protocol), OAU Doc. CAB/LEG/66.6 (2003); Organization of American States, Inter-American Convention on the Prevention, Punishment, and Eradication of Violence against Women (Convention of Belém do Pará) (1994); Convention on Preventing and Combating Violence against Women and Domestic Violence (Istanbul Convention), CETS No. 210 (2011).
[9] International Conference on Population and Development, Programme of Action, UN Doc. A/CONF.171/13 (1994).
[10] Fourth World Conference on Women, Beijing Declaration and Platform for Action, UN Doc. A/CONF.177/20 (1995).
[11] United Nations Department of Economic and Social Affairs, “SDG Indicators,” https://unstats.un.org/sdgs/metadata/.
[12] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 2(1); Committee on Economic, Social and Cultural Rights, General Comment No. 14, UN Doc. E/C.12/2000/4 (2000), paras. 30–33, 38–42, 63–65; Committee on Economic, Social and Cultural Rights, General Comment No. 22, UN Doc. E/C.12/GC/22 (2016), para. 52; Committee on Economic, Social and Cultural Rights, General Comment No. 25, UN Doc. E/C.12/GC/25 (2020), para. 24.
[13] International Council on Human Rights Policy, Duties sans Frontières: Human Rights and Global Social Justice (Geneva: ICHRP, 2003).
[14] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 15.
[15] Committee on Economic, Social and Cultural Rights (2020, see note 12), paras. 53–55, 67–71, 77–84.
[16] International Conference on Primary Health Care, Declaration of Alma-Ata (1978), art. 4.
[17] M. R. Decker, A. D. Latimore, S. Yasutake, et al., “GBV against Adolescent and Young Adult Women in Low- and Middle-income Countries,” Journal of Adolescent Health 56/2 (2015).
[18] World Health Organization, Violence against Women Prevalence Estimate, 2018: Global, Regional, and National Prevalence Estimates for IPV against Women and Global and Regional Prevalence Estimates for Non Partner Sexual Violence against Women (Geneva: World Health Organization, 2021).
[19] Republic of Kenya, Sexual Offences Act (2006); J. Mujuzi, “The Ugandan Domestic Violence Act: The Drafting History and Challenges to Its Implementation,” International Journal of Law, Policy, and the Family 28/3 (2014).
[20] Republic of Kenya (2006, see note 19).
[21] Republic of Uganda, Penal Code (Amendment) Act (2007); Mujuzi (see note 19).
[22] Human Rights Watch, The Issue Is Violence (September 2015), http://www.hrw.org/report/2015/09/28/issue-violence/attacks-lgbt-people-kenyas-coast; Constitution of Republic of Uganda (1995).
[23] L. McLean and P. Bukuluki, Uganda GBV Diagnostic: Report for the World Bank (Washington, DC: World Bank, 2016); Republic of Kenya (2006, see note 19).
[24] McLean and Bukuluki (see note 23); FIDH, Women’s Rights in Uganda: Gaps Between Policy and Practice (2012), https://www.fidh.org/IMG/pdf/uganda582afinal.pdf.
[25] P. Kameri-Mbote, “Violence against Women in Kenya: An Analysis of Law, Policy, and Institutions,” International Environmental Law Research Center Working Paper (2000), https://www.ielrc.org/content/w0001.pdf.
[26] Republic of Colombia, Law 1257 (2008).
[27] USAID, USAID/Colombia Gender Analysis and Assessment Final Report (Washington, DC: USAID, 2019); Instituto Nacional de Medicina Legal y Ciencias Forenses y Grupo Centro de Referencia Nacional sobre Violencia GCRNV, Boletín epidemiológico: Violencia de género en Colombia, análisis comparativo de las cifras de los años 2014, 2015, 2016 (2016), https://www.medicinalegal.gov.co/documents/20143/57985/Violencia+de+Género+en+Colombia.+Análisis+comparativo+de+las+cifras+de+los+años+2014%2C+2015+y+2016.pdf.
[28] J. Keesbury, W. Onyango-Ouma, C. Undie, et al., A Review and Evaluation of Multisectoral Response Services for GBV in Kenya and Zambia (New York: Population Council, 2012).
[29] McLean and Bukuluki (see note 23); Ugandan Ministry of Gender, Labour, and Social Development, National Action Plan on Elimination of GBV (Kampala: Ministry of Gender, Labour, and Social Development, 2014).
[30] USAID (2019, see note 27).
[31] Ministry of Gender, Labour, and Social Development (Uganda), National Policy on Elimination of GBV in Uganda, revised ed. (2019); Republic of Kenya, National Policy for Prevention and Response to GBV (2014); USAID (2019, see note 27).
[32] Bureau of Statistics (Uganda), Quality Assessment of Existing GBV/HP Management Information Systems in Uganda (2019).
[33] Ibid., p. 15.
[34] Ministry of Gender, Labour, and Social Development (Uganda) (2019, see note 31).
[35] Republic of Kenya, Generation Equality Forum: Kenya’s Roadmap for Advancing Gender Equality and Ending All Forms of GBV and FGM by 2026 (2021).
[36] National Gender and Equality Commission (Kenya), National Monitoring and Evaluation Framework towards the Prevention and Response to Sexual and Gender-Based Violence in Kenya (2014); National Gender and Equality Commission (Kenya), Annual Report 2018–2019 (2020).
[37] Bureau of Statistics (Kenya), Kenya Demographic and Health Survey, 2014 (2015).
[38] National Gender and Equality Commission (Kenya) (2014, see note 36).
[39] USAID (2019, see note 27).
[40] A. Peterman, J. Bleck, and T. Palermo, “Age and IPV: An Analysis of Global Trends among Women Experiencing Victimization in 30 Developing Countries,” Journal of Adolescent Health 57/6 (2015); L. McDougal, J. Klugman, N. Dehingia, et al., “Financial Inclusion and IPV: What Does the Evidence Suggest?” PLoS ONE 14/10 (2019).
[41] Y. D. Wado, M. K. Mutua, A. Mohiddin, et al., “IPV against Adolescent Young Women in Sub-Saharan Africa: Who Is Most Vulnerable?,” Reproductive Health 18/Suppl 1 (2021); T. Elghossain, S. Bott, C. Akik, and C. Makhlouf Obermeyer, “Prevalence of IPV against Women in the Arab World: A Systematic Review,” BMC International Health and Human Rights 19/1 (2019).
[42] M. V. Gattegno, J. D. Wilkins, and D. P. Evans, “The Relationship between the Maria da Penha Law and IPV in Two Brazilian States,” International Journal for Equity in Health 15 (2016); S. Suffla and M. Seedat, “The Epidemiology of Homicidal Strangulation in the City of Johannesburg, South Africa,” Journal of Forensic and Legal Medicine 37 (2016); N. Suryavanshi, S. Naik, S. Waghmare, et al., “GBV Screening Methods Preferred by Women Visiting a Public Hospital in Pune, India,” BMC Women’s Health 18/1 (2018), p. 19.
[43] S. Seims and R. Khadduri, “Measuring Improvements in SRHR in Sub-Saharan Africa,” Reproductive Health Matters 20/40 (2012).
[44] Organisation for Economic Co-operation and Development, “Aid (ODA) Disbursements to Countries and Regions [DAC2a],” https://stats.oecd.org/.
[45] Committee on Economic, Social and Cultural Rights (2020, see note 12), paras. 28, 34–35.
[46] Ministry of Gender, Labour, and Social Development (Uganda) (2019, see note 31); Republic of Kenya (2014, see note 31); USAID (2019, see note 27); USAID, GBV and Family Planning: An Implementation Assessment of Uganda’s Policy Framework (Washington, DC: USAID, 2018); Constitution of the Republic of Kenya (2010); FIDH (2012, see note 24).
[47] Economic Policy Research Center, “Investing in Health: The National Budget Framework FY 2021/22 Budget Brief,” https://www.unicef.org/esa/media/5961/file/UNICEF-Uganda-2020-2021-Health-Budget-Brief.pdf; K. K. McDade, K. Munge, G. Kokwaro, and O. Ogbuoji, “Reducing Kenya’s Health System Dependence on Donors,” Brookings (March 2, 2021), https://www.brookings.edu/blog/future-development/2021/03/02/reducing-kenyas-health-system-dependence-on-donors/.
[48] Ministry of Gender, Labour, and Social Development (Uganda), Uganda Management of Social Risk and GBV Prevention and Response Project (2017).
[49] Ministry of Finance Planning and Economic Development (Uganda), Uganda’s Development Partnership Review: A Country Pilot of the Global Partnership for Effective Development Cooperation (2020).
[50] A. Kerr-Wilson, A. Gibbs, E. McAslan Fraser, et al., A Rigorous Global Evidence Review of Interventions to Prevent Violence against Women and Girls (Pretoria: What Works to Prevent Violence Against Women and Girls Global Programme, 2020).
[52] L. Michau, E. Letiyo, T. Musuya, and L. Goldmann, “Social Norms Change at Scale: Insights from SASA!,” CUSP 2018 Case Study Collection, Case No. 3, Community for Understanding Scale Up (2018); L. Goldmann, R. Lundgren, A. Welbourn, et al., “On the CUSP: The Politics and Prospects of Scaling Social Norm Change Programming,” Sexual and Reproductive Health Matters 27/2 (2019).