Menstruation, Myopia, and Marginalization: Advancing Menstrual Policies to “Keep Girls in School” at the Risk of Exacerbating Inequalities
Volume 24/2, December 2022, pp. 13-28 | PDF
Nay Alhelou, Purvaja S. Kavattur, Mary M. Olson, Lillian Rountree, and Inga T. Winkler
Abstract
As countries across the world adopt policies addressing menstruation, it is imperative to identify who benefits from such policies and to understand the dynamics of inclusion and exclusion. We examine such policies through the lens of human rights, as a framework that demands addressing marginalization, ensuring substantive equality, and guaranteeing inclusive participation to ensure that the menstrual needs of everyone, everywhere are met. Our review is focused on four countries (India, Kenya, Senegal, and the United States) and is based on data from 34 policy documents and interviews with 85 participants. We show that girls, particularly school-going girls, are the main target group of policies. Due to this myopic view of menstrual needs, policies risk leaving the needs of adult menstruators, including those experiencing (peri)menopause, unaddressed. Moreover, the intersection between menstrual status and markers of identity such as disability and gender identity produces further policy gaps. These gaps can be attributed to the exclusion of marginalized menstruators from decision-making processes by creating barriers and failing to ensure meaningful inclusive participation. To address inequalities, policy makers need to make a concerted effort to understand and accommodate the needs of menstruators in all their diversity.
Introduction
As countries across the world increasingly adopt policies addressing menstruation, it is imperative to identify who benefits from such policies and to understand dynamics of inclusion and exclusion. We examine such policies through the lens of human rights, as a framework that demands addressing marginalization, ensuring substantive equality, and guaranteeing inclusive participation to ensure that the menstrual needs of everyone, everywhere are met. For example, the Kenyan Menstrual Hygiene Management policy commits to making it the “responsibility of the state to employ the best and equitable measures to enable the widest possible enjoyment of these rights [related to menstruation].”[1]
Such policy developments in Kenya and elsewhere stem from a greater global awareness of menstrual needs.[2] Menstruators require access to accurate information about the menstrual cycle, the means to care for their bodies, access to health care services, and stigma-free environments.[3] Failing to address these needs can negatively impact their lives. Menstruators may experience ill health, anxiety, and stigma and be unable to participate—or be prevented from participating—in social, cultural, or religious activities.[4] These unmet needs have profound effects on the human rights to health, bodily integrity, education, work, and participation in social, cultural, and public life.[5] With recent policy developments, menstruation has been moving from a nonissue to a key component of public health efforts.[6] Several authors have begun to examine these policy efforts, including some insiders involved in policy development, in particular in India and the United States.[7] Only few of these studies emphasize notions of nondiscrimination, substantive equality, and justice.[8] Moreover, most of the existing studies rely on desk reviews and legal analysis. To date, there is no empirical cross-country inquiry that provides a comprehensive analysis of policy developments.
Against this background, our project sought to review menstrual health and hygiene policy initiatives in four countries: India, Kenya, Senegal, and the United States.[9] Our process-oriented review was informed by the human rights principles of nondiscrimination, participation, and accountability. We were particularly interested in whose interests, needs, and voices were centered—and whose were marginalized—in the policies and processes leading to their adoption, and how this focus helped determine who benefitted from policymaking. Following the presentation of our research design and methodology, we discuss how policy initiatives overwhelmingly focused on adolescent girls and failed to meet menstruators’ needs across the life-course and across different identities and intersecting forms of marginalization. We identify the reasons for these gaps: compounded stigma, power relationships, and structural inequalities that are perpetuated through consultation processes that privilege established stakeholders. While policy advocates (and researchers) have begun to acknowledge the compounded stigma and discrimination that many menstruators face, we identify a disconnect between awareness and practice: most policies continued to neglect the menstrual needs of those facing marginalization, failing to meet the commitment to reduce inequalities and address discrimination.
Research design and methodology
Our project consists of a desk review of policy documents alongside in-depth interviews with government officials, civil society actors, academics, United Nations (UN) staff, and other experts on menstrual policy. We chose the countries by considering geographic diversity and identifying leading countries in several regions. South Asia, Eastern Africa, West Africa, and North America have emerged as hubs for menstrual hygiene and health.[10] We conducted the analysis at the national level and, depending on the governance structure, in selected regions, states, counties, and municipalities. We selected early adopters, including Maharashtra in India, Kwale County in Kenya, the Louga and Djourbel regions in Senegal, and New York State and New York City in the United States.
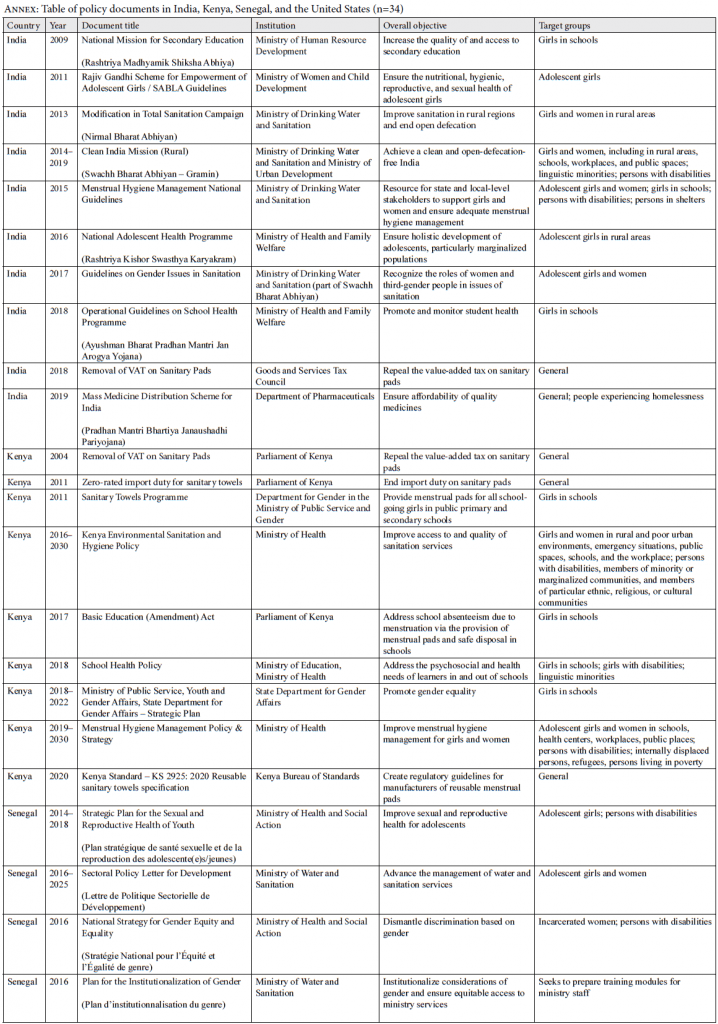
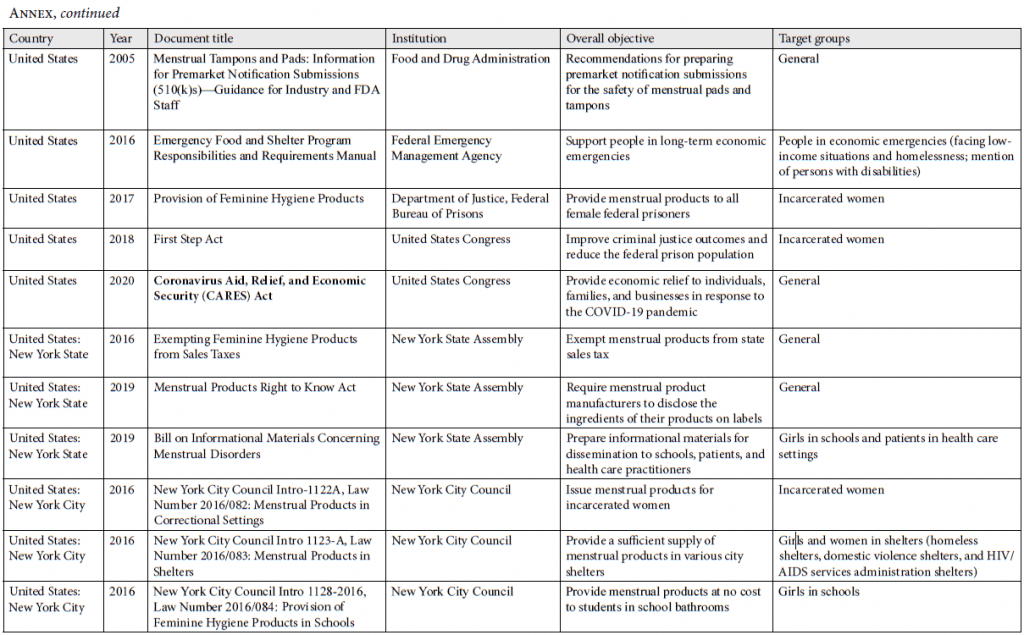
We identified 34 policy documents in India (n=10), Kenya (n=9), Senegal (n=4), and the United States (including New York State and New York City) (n=11). A complete list is available in the annex. We included all documents that (1) cover a topic related to menstruation, (2) were adopted between 2000 and 2020, and (3) were published and enacted by a governmental entity. This includes legislation and government-approved guidelines or mandates.
We (PSK and NA) interviewed 85 participants in India (n=19), Kenya (n=19), Senegal (n=23), and the United States (n=24), all of whom were active in policymaking or advocacy. We identified them by (1) reviewing relevant literature and documents; (2) connecting with initial contacts in the menstrual hygiene and health space and those in adjacent fields such as human rights, labor, gender, education, and sexual and reproductive health and rights; and (3) snowballing. We searched for participants who could contribute a range of perspectives, including advocates with disabilities, trans advocates, and people working in informal settlements and in the context of prisons. To the extent possible, we sought advocates who could speak from personal experience. Our interviews were semi-structured, focusing on processes, stakeholders, target populations, and policy priorities: What are the policy objectives? Which organizations, stakeholders, and individuals were involved in policy development? Who was consulted? Whose menstrual needs were addressed and whose were left unaddressed? All interviews were remote, using the video-conferencing software Zoom; most were conducted individually, while some participants were more comfortable in a group. In Senegal, most interviews were in French, some with the support of a French-to-English interpreter. Interviews in other countries were in English. The interviews lasted on average an hour, but varied from 30 minutes to two hours. All participants provided written informed consent. We transcribed the interviews to prepare them for data analysis and translated direct quotes from French into English.
We conducted a qualitative thematic analysis of the policy documents and interview transcripts.[11] Our approach was deductive, informed by human rights principles and prohibited grounds of discrimination.[12] Our codebook covered 34 populations, including school-going girls; incarcerated populations; Indigenous people; trans, non-binary, and gender-nonconforming menstruators; menstruators experiencing homelessness; and menstruators with disabilities. We used NVivo 12 for the analysis with a team of five coders (PSK, NA, LR, MMO, and a research assistant). Multiple coders double-coded a sample of transcripts to ensure the internal validity of coding and theme synthesis.
We received ethical clearance from the Institutional Review Board at Columbia University (protocol number AAAS8659) for the entire study. In India, only biomedical and clinical studies require ethical clearance. In Kenya, we received ethical clearance through Amref Health Africa’s Ethics and Scientific Review Committee (protocol number P775 2020) and a research permit from the National Commission for Science, Technology and Innovation (license number NACOSTI/P/20/5059). In Senegal, we were granted ethical clearance through the Comité National d’Ethique pour la Recherche en Santé (protocol number SEN20/40).
Interests, needs, and voices at the center and at the margins of policymaking
Policies addressed a range of target populations but were skewed toward the needs of adolescent girls, especially those in schools. More than half of the documents (19) explicitly targeted girls. Other policies (8) were universal in scope, indicating that “everyone” should have information and menstrual materials.
Despite beginning to recognize that menstruation is an experience lived by different people with different needs, policies did not address these needs comprehensively. An interviewee in Kenya encapsulated these challenges: “Not only did we not address the needs of all the menstruators, we didn’t address the needs even of the menstruators we provided for across the entire life cycle” (KEN03). In the following, we show how policies centered girls but ignored menstrual needs across the life-course. They also ignored the needs of menstruators facing marginalization due to compounded stigma, unequal power relationships, and structural inequalities. These very inequalities were manifest in the processes that led to the adoption of policies: marginalized menstruators were often excluded from decision-making processes, creating barriers and influencing policy priorities.
Centering girls
The overarching refrain motivating policy interventions during our interviews was to “keep girls in school” by addressing their menstrual hygiene needs. Many policies targeted girls in schools, including the Basic Education (Amendment) Act in Kenya, a municipal law in New York City, New York State’s Informational Materials Concerning Menstrual Disorders Act, the School Health Programme and National Health Mission in India, and a pad distribution program in Louga, Senegal (SEN06). While policies, in particular in the United States, also targeted other populations and settings, the focus remained primarily on adolescents and schools (e.g., IND16). Three-quarters of our interviewees referred to school-going girls. Even in the United States, interviewees discussed the needs of school-going girls far more often than any other population group. Even references to “women” were fewer, while they captured often generic policy initiatives.
These priorities align with the field more broadly. Schools are the most discussed, most targeted, and most studied setting for menstrual hygiene and health efforts, often linked to the WASH in Schools agenda.[13] A recent systematic review and meta-synthesis of menstrual experiences confirms that “studies focused on the experiences of adolescent girls were most strongly represented … Reflecting the focus of menstrual health research globally, there was an absence of studies focused on adult women.”[14]
Adolescence is a key phase of development, as the biosocial changes that pubescent youths go through impact their physical and social experiences.[15] Youths learn sociocultural norms and attitudes about themselves, their body, and the world around them.[16] Menarche influences how they experience their daily lives and communities.[17] Having long ignored the needs of girls—leading to significant disparities—global policy and development efforts focused on girls have become central with the adoption of the Millennium Development Goals, specifically the target on eliminating disparities in education, and initiatives such as the Girl Effect.[18] While policies to address girls’ needs are important—indeed, policy must be sensitive to barriers such as stigma and a lack of information—we see risks of placing an undue burden on girls as “changemakers” and overly centering them to the point of leaving others behind.
Policy makers and advocates viewed adolescents as vehicles of change, which may reinforce the idea that girls’ socioeconomic and political progress will trickle up to other populations.[19] Interviewees used the language of “change agents” (IND05), being “instrumental” (KEN08), and having a “ripple effect” (KEN08, SEN04). They explained that it was because of the impact on the “national economy … that … we must then make sure that our young girls are educated, that there are interventions accessible to them, and it’s affordable” (KEN08). Another interviewee stressed that “these are future mothers who will one day manage children and the family. Finally, it will be the entire future of society that will be impacted” (SEN04). Such narratives not only disregard reproductive autonomy but also place the expectation of social change on girls’ shoulders, making them responsible for lifting their communities out of poverty through individual consumption and investment regardless of the complex, generational history of privilege and oppression.[20] This falls within the context of the “girling” or even “girl-powering” of development.[21] Portraying girls’ empowerment as a lever for socioeconomic development can overshadow the goal of empowering girls in the first place and may overemphasize material menstrual needs.[22] As a result, policy makers place the burden on individual adolescent girls, while they shirk their own responsibility to bring about structural change.
Apart from their instrumentalization, focusing on girls in school produces two gaps: adult menstruators (discussed below) and out-of-school youth. Even before the pandemic, global estimates for 2018 indicated that 17% of children were out of school, which includes more girls than boys.[23] Initiatives that focus almost exclusively on school settings risk further marginalizing out-of-school children, compromising not only their right to education but also menstrual health rights. One interviewee in India stressed, “While … enrollment for girls has increased over the years, we still have adolescent girls who are dropping out after primary school … or girls who have never been to school … How do we reach them? … that has been a big question mark” (IND02). Based on global estimates for countries classified as low income, 36% of primary-school-age children in the lowest wealth quintile are out of school, compared to 10% in the highest quintile.[24] Such patterns persist across markers of identity, such as race, ethnicity, caste, and geography. In excluding girls who are unable to attend school, menstrual policies risk exacerbating inequalities.
Neglecting changing needs over the life-course
As soon as menstruators reach adulthood, they no longer receive the same attention in policies. Girls were contrasted with older women, who policy makers claimed “have been accustomed to live that way” (IND16). Interviewees in the United States explained the challenges in addressing “women’s issues”; societal discrimination against women resulted in menstrual health not being considered a “serious” legislative issue (USA19). When legislators began to mobilize around menstrual health, they were faced with backlash, which disincentivized more holistic action (USA18).
Some policies in India, Kenya, and Senegal did provide for community-level programming beyond schools. Senegalese sensitization trainings targeted all community members (SEN07, SEN14). Similarly, the Kenyan Menstrual Hygiene Management policy sought to make information widely accessible via the media, public health officers, nongovernmental organizations (NGOs), and the private sector. Women benefitted from community distribution and free menstrual products in public buildings. In India, community health and rural childcare centers also provided “mothers” with menstrual pads and information on menstruation (IND13). Trainings targeted community members, teachers, parents, government officials, and other decision makers. One interviewee explained that “every stakeholder is touched upon because the fact is if it’s a behavior change program, [you cannot] only target the girl. You have to create an enabling environment” (IND05). Despite such recognition, the community-level initiatives barely scratched the surface, and the focus remained on the needs of school-going girls.
As a result, we identified a lack of attention to changing needs over the life-course. This was most obvious in relation to menopause; we identified one brief reference to menopause in the Indian SABLA guidelines as a topic to be taught at schools. Merely one-sixth of participants—none of whom were government interviewees—referred to menopause or perimenopause. Those who did mention it did so exclusively to point out gaps in research, in data, and in understanding (e.g., SEN08). An interviewee in India shared her frustration: “We don’t have enough [research and data] on menopause, … people don’t pay attention because it’s an end of reproductive history” (IND12). Another interviewee added, “Menopausal women: that’s a group that we just never talk about. We only talk about adolescents” (IND08). In response, interviewees called for a life-course approach. One interviewee elaborated, “We need to move beyond adolescents to actually look at adult women. I think we need to look at postpartum bleeding … but also other types of vaginal bleeding” (IND01). While a life-course approach is gaining more attention in scholarship, this is yet to be reflected in policy.[25]
The settings that policies addressed clearly prioritized schools over the workplace. The Menstrual Hygiene Management policy in Kenya briefly calling for the provision of WASH facilities in workplaces was one of very few exceptions.[26] Only one interviewee briefly mentioned menstruators’ needs in the workplace (SEN15). In academic literature, menstruation and menopause at the workplace is beginning to receive attention.[27] Research notes that workers are preoccupied with managing their menstrual experience, hiding their menstrual status, managing pain, and anticipating stigma.[28] Some countries beyond the scope of our study have adopted menstrual leave policies, which have given rise to some debate.[29] While they accommodate menstrual needs and provide flexibility to take time off in case of discomfort, this may lead to overmedicalizing menstruation and perpetuating sexist beliefs and gender stereotypes.[30] Policy needs are more complex than merely providing leave. Overall, older menstruators still require policies that accommodate their needs.
Menstruation and marginalization
If gender and age lead to a disregard for menstruators’ needs, the intersection with other markers of identity such as disability exacerbates marginalization. Many identities affect how individuals experience menstruation and determine their menstrual needs, yet these are largely ignored in policymaking. We used the human rights framework to assess whether policies take into account prohibited grounds of discrimination to address the needs of all menstruators.[31] Article 2(2) of the International Covenant on Economic, Social and Cultural Rights guarantees that rights “will be exercised without discrimination of any kind as to race, colour, sex, language, religion, political or other opinion, national or social origin, property, birth or other status.”[32] These “other” grounds include disability, age, sexual orientation, gender identity, health status, place of residence, indigeneity, and socioeconomic situation.[33] Disability, homelessness, incarceration, and gender identity have begun to receive attention in policymaking or (more often) advocacy. For instance, some policies in the United States address the needs of menstruators facing homelessness and incarceration. Yet, even with increasing awareness, they remain significantly underaddressed in practice. The annex lists the policies we reviewed and the populations they target.
During our interviews, participants demonstrated awareness of the needs of specific population groups. About one-fourth recognized the needs of persons with disabilities, in particular pertaining to access to facilities and health services.[34] About one-fourth (in particular in the United States) mentioned incarceration. A government interviewee in Kenya referenced awareness trainings and explained, “We understand that even when they are behind bars, that they still menstruate” (KEN13). Similarly, about one-fifth of interviewees, mostly in the United States, discussed homelessness. Trans and non-binary menstruators were almost entirely absent from policies and largely excluded from advocacy platforms. A few interviewees noted the compounded menstrual and gender discrimination that trans and non-binary menstruators face (e.g., IND12). One interviewee in Kenya acknowledged, “What about trans menstruators? This is still a very, very difficult conversation to have in the African context, but all the same, these are people who exist here” (KEN12).
Additional populations and their menstrual needs were merely mentioned in passing, usually to identify gaps. Recognizing the needs of linguistic minorities, two policies, in Kenya and India, required that information be provided in a language that the target group understands. Some policies briefly referred to race, religion, and caste (in India), yet without any explicit acknowledgment of disparities or specific menstrual needs. Several interviewees mentioned race (mostly in the United States), ethnicity, indigeneity, migration status, caste (in India), language, and religion. Interviewees pointed to specific menstrual needs, to health disparities (USA01), and to the sociocultural context (IND17).[35] Some briefly mentioned the needs of menstruators in informal settlements, which often lack WASH and disposal infrastructure (KEN18). A few mentioned the needs of people living with HIV/AIDS and other health conditions (KEN10), as well as those of sex workers: “What happens to the sex workers? What happens to their menstrual hygiene? So we have no idea.” (IND12).
While these interviews demonstrate an emerging awareness of the intersections of menstrual injustice with various forms of marginalization, policy efforts remain very limited. States do not meet their obligation to achieve substantive equality by acting to dismantle discrimination and to accommodate the needs of different individuals.[36] Below, we examine some contributing factors: compounded stigma, power relationships, and structural inequalities.
Compounded stigma. Menstrual stigma is often compounded by other stigma. Systems of oppression, disadvantage, and stigmatization related to menstruation intersect with those based on race, caste, class, disability, gender identity, and others perpetuated through “patriarchy, white supremacy, classism, and ableism.”[37] Stigma is embedded in and contributes to social power dynamics that are intertwined with discrimination. For instance, the UN Committee on Economic, Social and Cultural Rights has recognized that “living in poverty or being homeless may result in pervasive discrimination, stigmatization and negative stereotyping” that impact the enjoyment of human rights.[38] Many menstruators experience the double stigma of menstruation and homelessness; they feel exposed in public while seeking privacy, warmth, and comfort.[39] Policy efforts such as the one in New York City to address these unique challenges have been very limited. Even then, interviewees voiced concern that menstrual products are not replenished due to “general disdain” (USA04) for people experiencing homelessness. As a result, even with mandates in place to provide menstrual products, material needs will not be met without changing attitudes toward people experiencing homelessness.
We observed similar dynamics in the context of disability. A few policies in Kenya, India, and Senegal addressed the needs of persons with disabilities but were limited to physical disabilities (e.g., related to toilet design). Many interviewees demonstrated awareness of the physical challenges that menstruators with disabilities may face and have worked to make WASH infrastructure inclusive. Some materials and trainings were tailored specifically to visually and hearing-impaired menstruators (IND02, KEN13). However, there continued to be “a lot of ableism in the marketing of the different menstrual materials” (KEN02). Most notably, psychosocial and cognitive disabilities, which carry much greater stigma than physical disabilities, remained largely unaddressed, even during interviews with advocates.[40] One interviewee noted that trainings included information on “how to accompany a woman with mental disabilities … to manage her menstruation” (SEN15). Another interviewee mentioned people on the autism spectrum and those with cognitive disabilities, which may make “some elements of caring for yourself during menstruation more difficult” (USA02). Because of menstrual stigma, menstrual materials often use euphemisms such as “feminine hygiene,” which can be difficult to comprehend for people who prefer literal terms.[41] Menstrual stigma and ableism compound to leave menstruators on the spectrum and those with disabilities further behind. Yet, few interviewees acknowledged this, and the needs are not (yet) reflected in policies. Without understanding how compounded stigma impacts menstrual needs, these needs will continue to be invisible and neglected.
Power relationships. As we have shown elsewhere, stigma is inextricably linked to power—the power to define what is considered “normal” and what is abject.[42] These power relationships manifest in many ways: the power of employers to terminate a woman in perimenopause because her heavy bleeding “soiled” the carpet; the power of judges to authorize forced sterilizations of women with disabilities because it makes it easier to “manage” menstruation; the power of staff in homeless shelters to decide whether to replenish supplies.[43] These power structures have implications for bodily autonomy, health, nondiscrimination, and other human rights. They warrant recognition in policies—for example, via procedural safeguards and trainings—but are hardly addressed.
Power relations are particularly visible in the context of detention, where menstruators face significant barriers, including unaffordability of products and lack of private facilities.[44] Interviewees in the United States noted that conditions have improved in terms of access to menstrual products (USA13); however, policies were not universal—local jails and migrant detention centers were not covered. In fact, in “the immigration detention system … isolation, power dynamics, and lack of control exacerbate menstrual injustices.”[45] In practice, access to menstrual products continued to be determined largely by power relations. One interviewee recalled:
As a formerly incarcerated woman … I went through devastating and dehumanizing experiences … To be issued additional pads, … I had to quantify my cycles, which meant I had to put the used pads in a brown paper bag, share it with the officer who was on duty, likely 95 percent of the time was male, for them to look in the bag to see that I actually used these five pads to issue me five more (USA25).
Legislators acknowledged dynamics of coercion, dependence, and manipulation; they considered them “outrageous. You don’t lose your right to deal with your health … when you’re incarcerated” (USA04). In India, women in prisons also faced violence. “There are cases of women who have exchanged sexual favors for sanitary napkins” (IND04). Advocates therefore cautioned against tokenism:
When their personhood is not respected, when their dignity is not respected, there’s a short hop and skip to violence and coercion … You see the denial of pads and tampons as a means of controlling women … It’s part of degrading people in order to groom them for sexual favors … When we see this happening, we know that it’s part of a larger narrative in the institution where women’s rights are being denied (USA03).
Without acknowledging—and addressing—this broader context, policy mandates on product provision risk being meaningless. The deep-rooted perceptions and ensuing power dynamics need to be tackled to improve the lives of menstruators in detention.
Structural inequalities. Ultimately, policies fail to address structural inequalities. As we have shown elsewhere, policies prioritize menstrual hygiene initiatives over menstrual health, infrastructure over education, and tangible solutions over sociocultural change.[46] These priorities mean that the needs of menstruators who face marginalization remain ignored.
Interviewees stressed that the challenges menstruators in detention faced extended far beyond the lack of access to menstrual products; medical care was often limited. One formerly incarcerated woman recalled, “I had uterine fibroids, I was actually encouraged to get a hysterectomy … I fought against that because I knew I didn’t need a full hysterectomy” (USA25). Another interviewee talked about needs during (peri)menopause, such as “gynecological appointments to deal with the various symptoms and side effects of menopause” (USA03). Despite this recognition, existing initiatives were focused primarily on product provision. Menstrual health was largely ignored, particularly as menstruators get older.
Similarly, the needs of menstruators experiencing homelessness went largely unmet. They may need pain relief and safe, comfortable, and warm places to manage both physical and emotional aspects of menstruation, in addition to access to menstrual products. But the very structural issues that render people homeless, such as lack of affordable housing, persist. This is reflected in the often-used term “period poverty” (e.g., KEN08, USA13), which isolates material menstrual needs rather than addressing systemic poverty.
When the needs of trans and non-binary menstruators were addressed at all, they focused on access to sanitation facilities, as bathroom politics have emerged as a galvanizing point.[47] While gender-segregated bathrooms have been suggested for meeting the privacy needs of menstruating cis women and girls, a trans advocate argued that gender-sensitive WASH infrastructure needs to be reimagined, with one option being all-gender bathrooms in public spaces (USA02). Interviewees also highlighted safety risks for trans and non-binary menstruators, including the risk of maltreatment in the health care context.[48] Interviewees in India pointed out that “a lot of trans people, even when they go on testosterone, they still menstruate, [and] trans men … have such horrible experiences with doctors” (IND04). The need for menstrual care goes beyond the question of hormone therapy and medical transition. “Folks … remain fixated on … a medical gender transition and lose sight of all the other parts of primary care” (USA02), one interviewee argued. This requires gender-inclusive curricula and protocols for standards of care (USA02), all of which remained unaddressed in the policies we analyzed.
Overall, the menstrual needs of all who menstruate must be addressed more comprehensively. Gaps in policymaking are particularly pronounced as they relate to markers of identity that are perceived as “political” or that are deeply stigmatized, such as race, caste, psychosocial and cognitive disabilities, and gender identity. These gaps reflect general patterns in failing to addressing marginalization in the context of the Sustainable Development Goals.[49] Comprehensive assessments of barriers to the realization of human rights that menstruators face—whether physical, geographic, economic, linguistic, cultural, attitudinal, or other—are needed. Such assessments must go beyond menstrual products and facilities and consider comprehensive information, menstrual health needs, and the impacts of sociocultural norms and attitudes.
Stakeholder participation: An NGO echo chamber at risk of excluding marginalized menstruators
Human rights guarantee people the “right to participate in and access information relating to the decision-making processes that affect their lives and well-being.”[50] Meaningful participation requires that all those concerned have a reasonable opportunity to influence decision-making.[51] Consultations and participatory processes are key for understanding menstrual needs, and addressing power imbalances between marginalized and privileged groups is key to meaningful participatory processes.[52] All four governments engaged, to varying degrees, with civil society organizations, NGOs, advocacy groups, and menstruators themselves. However, our findings show that various consultations repeatedly engaged the same stakeholders, while creating barriers for marginalized populations and failing to ensure inclusiveness. This may explain the gaps in policymaking that we identified.
In Kenya, the Hygiene Promotion Technical Working Group served as a “coordination platform through which … the Ministry of Health would rally in stakeholders” (KEN03). It involved NGOs, UN agencies, academic institutions, faith-based organizations, social enterprises, and, to some extent, grassroots organizations (KEN02). In India, government agencies held consultations while developing several policies. For the Swachh Bharat Mission, the Ministry of Drinking Water and Sanitation worked with the UN Water Supply and Sanitation Collaborative Council to present policy makers with testimonials from the ground (IND08) and solicited feedback once guidelines were drafted (IND11). In New York City, policy makers hosted roundtables when developing bills on product provision in schools, shelters, and prisons. One advocate recalled:
We put together … the menstrual equity roundtable and invited everyone we perceived as stakeholders to come to the table … everyone from the Women’s Prison Association to the YWCA, to afterschool programs to reproductive health providers to shelters … And then kind of worked from there to make sure all the right voices were at the table (USA17).
Not all consultations included a wide range of stakeholders, however. For example, when consulting stakeholders to update standards on disposable menstrual pads in India, a civil society advocate pointed out, “Ideally, it should be a very distributed stakeholder list with the manufacturers, researchers, academicians … But when we reached the table, it was basically manufacturers. So the interests [are] likely to get misrepresented” (IND15).
Interviewees identified several barriers. In Kenya, they stressed that a lack of resources put smaller organizations at a disadvantage (KEN03). Multiple interviewees noted that personal government contacts secured them a seat at the table. For instance, UNICEF staff had developed a close relationship with government officials in India, resulting in constant interaction (IND05) and access to budgetary data unavailable to others (IND01). Advocates recognized the power of UN organizations to influence governments (KEN02), and those with direct connections benefitted from them. However, such associations can perpetuate patterns of privilege and result in the marginalization of those without direct contacts. In India, interviewees repeatedly referenced the same stakeholders: UNICEF, UNFPA, the Aga Khan Foundation, WaterAid, Jhpiego, the World Bank, and the Gates Foundation. Often, consultations included those who were perceived as stakeholders and the “right voices” (USA17). Even with the best intentions, this raises concerns about gatekeeping and unequal weight given to the agendas of better-known organizations, to the detriment of grassroot organizations.
Stakeholder engagement does not necessarily mean public participation. One interviewee noted, “People make assumptions … they don’t ask. People assume that all the girls use reusable pads, but they don’t” (KEN09). Another interviewee stressed, “I still feel like it’s very much NGOs talking to other NGOs … I would love to see a town hall, where we can weigh in and just say, ‘This town hall is strictly about periods and policy, and what do you think we need to do?’” (KEN12). By excluding grassroot organizations and marginalized menstruators, stakeholder meetings risk turning into an NGO echo chamber. When the same organizations get together, the policies they advance tend to reflect their priorities. For example, since the raison-d’être of UNICEF is the protection of children, its influence may partially explain the emphasis on girls in the existing policies.
Financial, logistical, and attitudinal barriers to participation particularly impact the rights of people facing marginalization. In the United States, much policy advocacy is dominated by legal professionals, most of whom are white. Interviewees pointed out that racial and ethnic minorities, trans and non-binary menstruators, and people living in poverty have often been excluded from policy advocacy spaces (USA05). Even though power and privilege are allocated along different lines, similar patterns emerge in India. Advocacy is largely driven by “upper” caste women, thus centering their voices and leaving others, including Dalits, marginalized. Menstruation “has caste implication[s] that nobody wants to talk about” (IND03). One interviewee recalled an incident where event organizers initially objected to Dalit advocates sharing the stage with ministers (IND08), demonstrating deeply ingrained societal hierarchies even when people were invited to share their perspectives.
Several interviewees with disabilities spoke of the difficulties and lack of accommodations when engaging in consultative processes. A deaf participant explained the multiple challenges she faced in participating in government-run processes: stigma and no budgeting for sign language interpreters. She experienced it as being told, “‘You’re disabled, your level of education is low, and so we’re not going to hear you. We’re going to listen to the normal ones’” (KEN14). Similarly, an interviewee in the United States living with a disability shared her frustration: “‘Oh, you can’t make that meeting…? Sorry. It must not be that important to you.’ It’s an ableist society, and ableism has to come out of policy, especially for the policy makers that say they do social justice” (USA24).
While some steps were taken to understand the menstrual needs of persons with disabilities (SEN08) and to ensure representation during government convenings (IND08), overall, participatory processes need improvement to allow for different ways of participating, to open up spaces, and to accommodate the diverse needs of menstruators. The gaps in inclusive participation and the overreliance on the same stakeholders seem to have resulted in a myopic view of menstrual needs that center girls, while ignoring needs across the life-course and leaving behind many menstruators. Marginalization at the procedural level has led to continued neglect and exclusion in substantive policy priorities. Procedural rights to participation and substantive rights are deeply intertwined, and neglecting the participation of people facing marginalization has led to further entrenching structural inequalities.
Conclusion
Menstruation has become an issue of public policy. While some initiatives are promising, policies largely fail to live up to the commitment to address discrimination and marginalization and to achieve substantive equality. People with diverse backgrounds, characteristics, and identities experience menstruation, and it spans many decades of life. Yet the predominant policy focus is on adolescent girls in schools, which risks neglecting or dismissing the needs of adults, in particular related to perimenopause and menopause. By examining the intersections of menstrual status with other identities, policy makers have begun to address the needs of menstruators with disabilities, incarcerated menstruators, and menstruators experiencing homelessness. However, these efforts largely fail to address the causes rooted in compounded stigma, power relationships, and structural inequalities. Moreover, forms of discrimination that are perceived as “too political” remain almost entirely unaddressed, ignoring disparities based on race, caste and ethnicity, the menstrual needs of sex workers, and many others. By tracing policy processes from consultation to implementation, we demonstrate that inclusion and representation matter. All too often, consultations resulted in an NGO echo chamber that privileged powerful stakeholders and failed to include marginalized voices.
The human rights framework, through its emphasis on addressing marginalization, ensuring substantive equality, and guaranteeing inclusive participation, provides an opportunity to identify gaps in policymaking and reorient current efforts toward ensuring substantive equality for all people who menstruate. Some authors have found that the (global) discourse of human rights and human dignity has been instrumentalized and tokenized in menstrual advocacy to advance narrow perceptions of menstrual needs.[53] These perceptions reduce dignity to menstrual management, privacy, and cleanliness.[54] However, human rights—understood as a comprehensive framework—emphasize notions of agency, autonomy, and substantive equality that engage with the emancipatory promise to advance gender justice. As a relatively new policy and advocacy space, menstrual health provides a unique opportunity to change entrenched patterns of marginalization. Understanding and addressing menstrual needs in all their diversity and across the entire life-course is essential for achieving substantive equality. If not reduced to tokenism, human rights indeed hold the promise of bringing about transformative social change for all people who menstruate.
Acknowledgments
We would like to thank the project’s advisory group, which supported us throughout the research process in four countries and provided feedback on preliminary results. Neville Okwaro, Caroline Kabiru, Alex Manyasi, Arundati Muralidharan, Vinod Mishra, Santosh Mehrotra, and Mbarou Gassama Mbaye were instrumental in connecting us with interviewees. Rockaya Aidara (formerly with the UN Water Supply and Sanitation Collaborative Council) set the spark for this project and provided guidance throughout the process. We are also grateful to the Working Group on Menstrual Health and Gender Justice at the Center for the Study of Social Difference at Columbia University for the opportunity to discuss work in progress; to Chris Bobel and Margaret Johnson for their thoughtful comments on earlier drafts; to Elina Govil for her research assistance; and to Perri Schenker for her excellent editing.
Nay Alhelou, MA, is a research coordinator at the Population Council and former research fellow at the Institute for the Study of Human Rights at Columbia University, New York, USA.
Purvaja S. Kavattur, MSc, is a researcher with the National Advocates for Pregnant Women, and former staff associate at the Institute for the Study of Human Rights at Columbia University, New York, USA.
Mary M. Olson is a researcher at Columbia University, New York, USA, specializing in economics and its intersections with human rights and gender.
Lillian Rountree, an undergraduate at Columbia University, New York, USA, studies statistics and French with a research focus on menstrual health and contraception.
Inga T. Winkler, PhD, is an associate professor in human rights in the Legal Studies Department at the Central European University in Vienna, Austria, and former lecturer in human rights at Columbia University, New York, USA.
Please address correspondence to Inga T. Winkler. Email: winkleri@ceu.edu.
Competing interests: None declared.
Copyright © 2022 Alhelou, Kavattur, Olson, Rountree, and Winkler. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original authors and source are credited.
References
[1] Government of Kenya, Menstrual Hygiene Management Policy 2019–2030 (Nairobi: Ministry of Health, 2019).
[2] M. Sommer, J. S. Hirsch, C. Nathanson, et al., “Comfortably, Safely, and without Shame: Defining Menstrual Hygiene Management as a Public Health Issue,” American Journal of Public Health 105/7 (2015).
[3] J. Hennegan, I. Winkler, C. Bobel, et al., “Menstrual Health: A Definition for Policy, Practice, and Research,” Sexual and Reproductive Health Matters 29/1 (2021).
[4] I. T. Winkler and V. Roaf, “Taking the Bloody Linen Out of the Closet: Menstrual Hygiene as a Priority for Achieving Gender Equality,” Cardozo Journal of Law and Gender 21/1 (2014); J. Hennegan, A. K. Shannon, J. Rubli, et al., “Women’s and Girls’ Experiences of Menstruation in Low- and Middle-Income Countries: A Systematic Review and Qualitative Metasynthesis,” PLoS Medicine 16/5 (2019).
[5] Office of the United Nations High Commissioner for Human Rights, “International Women’s Day—8 March 2019: Women’s Menstrual Health Should No Longer Be a Taboo,” UN Special Procedures, press release (March 5, 2019), https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=24258&LangID=E.
[6] L. Amaya, J. Marcatili, and N. Bhavaraju, “Advancing Gender Equity by Improving Menstrual Health,” Bill and Melinda Gates Foundation and FSG (April 2020), https://www.fsg.org/publications/advancing-gender-equity-improving-menstrual-health.
[7] B. J. Crawford and E. G. Waldman, Menstruation Matters (New York: New York University Press, 2022); A. Patkar, “Policy and Practice Pathways to Addressing Menstrual Stigma and Discrimination,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020); A. Muralidharan, H. Patil, and S. Patnaik, “Unpacking the Policy Landscape for Menstrual Hygiene Management: Implications for School WASH Programmes in India,” Waterlines 34 (2015); J. Weiss-Wolf, “U.S. Policymaking to Address Menstruation: Advancing an Equity Agenda,” in Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[8] M. E. Johnson, “Menstrual Justice,” UC Davis Law Review 53 (2019); B. Goldblatt and L. Steele, “Bloody Unfair: Inequality related to Menstruation; Considering the Role of Discrimination Law,” Sydney Law Review 41/3 (2019).
[9] For different aspects of the project, see also N. Alhelou, P. S. Kavattur, L. Rountree, et al., “‘We Like Things Tangible’: A Critical Analysis of Menstrual Hygiene and Health Policy-Making in India, Kenya, Senegal and the United States,” Global Public Heath (2021); M. M. Olson, N. Alhelou, P. S. Kavattur, et al., “The Persistent Power of Stigma: A Critical Review of Policy Initiatives to Break the Menstrual Silence and Advance Menstrual Literacy,” PLOS Global Public Health 2/7 (2022).
[10] Patkar (see note 7); C. Bobel, The Managed Body: Developing Girls and Menstrual Health in the Global South (Cham: Springer International Publishing, 2019), p. 80.
[11] V. Braun and V. Clarke, “Using Thematic Analysis in Psychology,” Qualitative Research in Psychology 3/2 (2006).
[12] See Committee on Economic, Social and Cultural Rights, General Comment No. 20, UN Doc. E/C.12/GC/20 (2009).
[13] WinS4girls Compendium, “WASH in Schools for Girls,” http://www.wins4girls.org/.
[14] Hennegan et al. (see note 4), p. 12.
[15] L. Houghton, R. Troisi, M. Sommer, et al., “‘I’m Not a Freshi’: Culture Shock, Puberty and Growing up as British-Bangladeshi Girls,” Social Science and Medicine 258 (2020).
[16] Ibid., p. 9.
[17] Ibid.
[18] E. Unterhalter, “Mobilization, Meanings and Measures: Reflections on Girls’ Education,” Development 48/1 (2005); C. M. Caron and S. A. Margolin, “Rescuing Girls, Investing in Girls: A Critique of Development Fantasies,” Journal of International Development 27/7 (2015).
[19] See O. Koffman and R. Gill, “‘The Revolution Will Be Led by a 12-Year-Old Girl’: Girl Power and Global Biopolitics,” Feminist Review 105/1 (2013); Bobel (see note 10), pp. 47–48.
[20] Bobel (see note 10), pp. 50–53; Caron and Margolin (see note 18).
[21] Koffman and Gill (see note 19), p. 86.
[22] Ibid.
[23] United Nations, The Sustainable Development Goals Report 2020 (New York: United Nations, 2020), p. 34.
[24] UNESCO, “World Inequality Database on Education: Out-of-School Children” (2015), https://www.education-inequalities.org/indicators/eduout_prim#?sort=mean&dimension=wealth_quintile&group=all&age_group=eduout_prim&countries=all.
[25] V. Beck, J. Brewis, and A. Davies, “Women’s Experiences of Menopause at Work and Performance Management,” Organization 28/3 (2021); M. Sommer, P. Phillips-Howard, T. Mahon, et al., “Beyond Menstrual Hygiene: Addressing Vaginal Bleeding throughout the Life Course in Low and Middle-Income Countries,” BMJ Global Health 2/2 (2017).
[26] Government of Kenya (see note 1), p. 15.
[27] M. Sommer, S. Chadraratna, S. Cavill, et al, “Managing Menstruation in the Workplace: An Overlooked Issue in Low- and Middle-Income Countries,” International Journal for Equity in Health 15/86 (2016).
[28] K. Sang, J. Remnant, T. Calvard, et al., “Blood Work: Managing Menstruation, Menopause and Gynaecological Health Conditions in the Workplace,” International Journal of Environmental Research and Public Health 18/4 (2021); J. Hennegan, S. Kibira, N. Exum, et al., “‘I Do What a Woman Should Do’: A Grounded Theory Study of Women’s Menstrual Experiences at Work in Mukono District, Uganda,” BMJ Global Health 5/11 (2020).
[29] R. Levitt and J. Barnack-Tavlaris, “Addressing Menstruation in the Workplace: The Menstrual Leave Debate,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[30] S. King, “Menstrual Leave: Good Intention, Poor Solution,” in J. Hassard and L. Torres (eds), Aligning Perspectives in Gender Mainstreaming (Cham: Springer International Publishing, 2021).
[31] Committee on Economic, Social and Cultural Rights (see note 12).
[32] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 2.
[33] Committee on Economic, Social and Cultural Rights (see note 12).
[34] See also J. Wilbur, B. Torondel, S. Hameed, et al., “Systematic Review of Menstrual Hygiene Management Requirements, Its Barriers and Strategies for Disabled People,” PLoS ONE 14/2 (2019).
[35] See further E. Krusz, N. Hall, D. J. Barrington, et al., “Menstrual Health and Hygiene among Indigenous Australian Girls and Women: Barriers and Opportunities,” BMC Women’s Health 19/1 (2019); D. Sukumar, “Personal Narrative: Caste Is My Period,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[36] Committee on Economic, Social and Cultural Rights (see note 12).
[37] Johnson (see note 8), p. 23; see also K. Crenshaw, “Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color,” Stanford Law Review 43/6 (1991); P. H. Collins, “Intersectionality’s Definitional Dilemmas,” Annual Review of Sociology 41/1 (2015).
[38] Committee on Economic, Social and Cultural Rights (see note 12).
[39] S. Vora, “The Realities of Period Poverty: How Homelessness Shapes Women’s Lived Experiences of Menstruation,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020); M. Sommer, C. Gruer, R. Smith, et al, “Menstruation and Homelessness: Challenges Faced Living in Shelters and on the Street in New York City,” Health and Place 66 (2020).
[40] See M. O. Husain, S. S. Zehra, M. Umer, et al., “Stigma toward Mental and Physical Illness: Attitudes of Healthcare Professionals, Healthcare Students and the General Public in Pakistan,” BJPsych Open 6/5 (2020).
[41] R. Steward, L. Crane, E. Roy, et al., “‘Life Is Much More Difficult to Manage during Periods’: Autistic Experiences of Menstruation,” Journal of Autism and Developmental Disorders 48/12 (2018); I. Johnston-Robledo and J. C. Chrisler, “The Menstrual Mark: Menstruation as Social Stigma,” Sex Roles 68/1 (2013).
[42] Olson et al. (see note 9).
[43] Johnson (see note 8), pp. 30–31; L. Steele and B. Goldblatt, “The Human Rights of Women and Girls with Disabilities: Sterilization and Other Coercive Responses to Menstruation,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[44] T. A. Roberts, “Bleeding in Jail: Objectification, Self-Objectification, and Menstrual Injustice,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[45] V. Gomez and M. L. Karin, “Menstrual Justice in Immigration Detention,” Columbia Journal of Gender and Law 41/1 (2021).
[46] Alhelou et al. (see note 9).
[47] See A. Davis, “Regulating Restrooms,” in Bathroom Battlegrounds: How Public Restrooms Shape the Gender Order (Oakland: University of California Press, 2020); J. Sumerau and E. Grollman, Black Lives and Bathrooms: Racial and Gendered Reactions to Minority Rights Movements (Lanham: Lexington Books, 2020).
[48] See also B. Lane, A. Perez-Brumer, R. Parker, et al., “Improving Menstrual Equity in the USA: Perspectives from Trans and Non-binary People Assigned Female at Birth and Health Care Providers,” Culture, Health and Sexuality (2021) K. Rydström, “Degendering Menstruation: Making Trans Menstruators Matter,” in C. Bobel, I. T. Winkler, B. Fahs, et al. (eds), The Palgrave Handbook of Critical Menstruation Studies (Singapore: Palgrave Macmillan, 2020).
[49] I. T. Winkler and M. L. Satterthwaite, “Leaving No One Behind? Persistent Inequalities in the SDGs,” International Journal of Human Rights 21/8 (2017).
[50] UNFPA, “Human Rights Principles” (2005), https://www.unfpa.org/resources/human-rights-principles.
[51] United Nations General Assembly, Human Right to Safe Drinking Water and Sanitation, UN Doc. A/69/213 (2014).
[52] A. Yamin, Power, Suffering, and the Struggle for Dignity: Human Rights Frameworks for Health and Why They Matter (Philadelphia: University of Pennsylvania Press, 2016), pp. 165–173.
[53] K. Zivi, “Hiding in Public or Going with the Flow: Human Rights, Human Dignity, and the Movement for Menstrual Equity,” Human Rights Quarterly 42 (2020); I. T. Winkler, “Menstruation and Human Rights: Can We Move beyond Instrumentalization, Tokenism and Reductionism?,” Columbia Journal of Gender and Law 41 (2021).
[54] C. Bobel, “Beyond Dignity: A Case Study of the Mis/Use of Human Rights Discourse in Development Campaigns,” in R. Srikanth and E. H. Chowdhury (eds), Interdisciplinary Approaches to Human Rights (Milton Park: Routledge, 2018).