Leaving No One Behind: Human Rights and Gender as Critical Frameworks for U=U
Volume 24/2, December 2022, pp. 1-11 | PDF
Laura Ferguson, William Jardell, and Sofia Gruskin
Abstract
Experience has shown the need to explicitly address human rights and gender-related barriers in the rollout of HIV-related biomedical innovations, including “undetectable equals untransmittable” (U=U). This paper brings to light rights and gender considerations relevant to supporting U=U, recognizing a range of barriers that remain to be addressed for all people to benefit equally from U=U. We conducted a literature review to ascertain how human rights and gender were addressed in relevant publications, including peer-reviewed articles published between 2006 and 2020, relevant nongovernmental and global organizations’ publications, and abstracts presented at the 2019 International AIDS Conference, that explicitly addressed U=U or “treatment as prevention.” Despite evidence to illustrate the importance of attention to human rights and gender within U=U policies and interventions, there remains a lack of explicit attention to human rights and gender considerations in research and programming, particularly with regard to the rights principles of participation and accountability. Explicitly engaging all of these dimensions is key to informing interventions and improving people’s lives, health, and well-being.
Introduction
Decades of experience in the HIV response have shown that attention to realizing human rights and promoting gender equality in laws, policies, interventions, and services helps ensure that clinical efficacy is translated into real-world effectiveness.[1] This means, for example, drawing attention to and addressing non-clinical barriers to accessing services, adhering to treatment, and maintaining viral suppression as they affect different populations.
HIV treatment is known to lead to improved clinical outcomes while yielding the additional benefit of preventing onward transmission once viral suppression is achieved, sometimes referred to as “treatment as prevention” or “TasP.” In 2006, the Swiss Statement—an authoritative statement that people living with HIV who are in receipt of effective antiretroviral therapy (ART), and who do not have any sexually transmitted infections, cannot transmit HIV through sexual contact—explicitly called on courts to consider this information in criminal HIV transmission cases, noting that unprotected sex between a person with a positive HIV diagnosis and an HIV-negative partner “does not comply with the criteria for an attempt to spread a dangerous disease under section 231 of the Swiss Penal Code, nor for an attempt to cause serious bodily harm under section 122, 123 or 125 of the Swiss Penal Code.”[2]
Since then, several large studies have confirmed the accuracy of the science, setting the foundation for global scientific acceptance of the message that an undetectable viral load leads to negligible risk of HIV transmission.[3] Importantly, however, distinct from the Swiss Statement, there is no reference to legal implications, human rights principles, or gender considerations in the write-ups of these later studies. Yet, lived realities and decades of experience have shown the need to pay attention not just to the provision of new HIV-related technologies in the abstract but to the people who are their intended beneficiaries and, consequently, to legal, human rights, and gender considerations in the rollout of any HIV-related intervention.[4]
In 2019, the Prevention Access Campaign launched the “Undetectable Equals Untransmittable,” or “U=U,” initiative, now supported by more than 990 organizations from over 100 countries. More recently, the campaign added a third “U,” for “universal,” urging advocates to use U=U as a platform for demanding universal access to HIV diagnosis, treatment, and health care for all people living with HIV.[5] These initiatives have been explicit in recognizing barriers such as stigma, discrimination, criminalization, and inadequate health care infrastructure and calling for increased access to needed treatment by removing these barriers. U=U has been key in strengthening advocacy efforts for universal access to treatment, care, and diagnostics.[6]
For U=U to benefit everyone, and to avoid the potential of creating or exacerbating divisions between those who are virally suppressed and those who are not, addressing the structural factors that shape people’s ability to access and adhere to ART remains critical. Of relevance, the political declaration emanating from the United Nations High-Level Meeting on HIV/AIDS in 2021 calls on member states to address persistent inequalities in relation to HIV among gay men and other men who have sex with men, people who inject drugs, sex workers, people in prisons, and transgender populations, recognizing that they are more likely to face violence, stigma, discrimination, and laws that restrict access to services.[7] Although the U=U campaign has successfully united community and medical experts in a number of ways, attention to gender and rights has been inadequate.
In this paper, we seek to draw attention not only to the ways in which rights and gender dynamics are important in the context of U=U, but critically to the extent and reality of how these issues are being considered by key global actors. We favor the language of U=U but use TasP where authors have specifically chosen this terminology. We hope this analysis can help inform how attention to rights and gender can better support future U=U work at the global and national levels, deliver improved HIV-related outcomes, and ensure that everyone, including the most marginalized, can benefit from U=U.
Overview of human rights and gender considerations in HIV programming
Attention to rights considerations and gender equality have long been recognized as integral to an effective HIV response, even as this recognition may be more evident on paper than in practice. We take as our starting point that human rights and gender are synergistic frameworks, noting in particular the ways in which gender equality can effectively be promoted through human rights realization; if both are taken into account, this can help ensure that U=U works for all its intended beneficiaries.
The application of human rights principles to HIV research and programming brings a number of issues into play. In the first instance, the legal and policy environment is known to shape the availability of HIV-related services and programs and the degree to which they can be responsive to individual needs and aspirations.[8] With respect to U=U, consideration of human rights principles alongside efforts to strengthen the legal and policy environment can help identify and overcome challenges to increasing and sustaining access to treatment and services for all people, as well as promote accountability and transparency for what is done and how.[9]
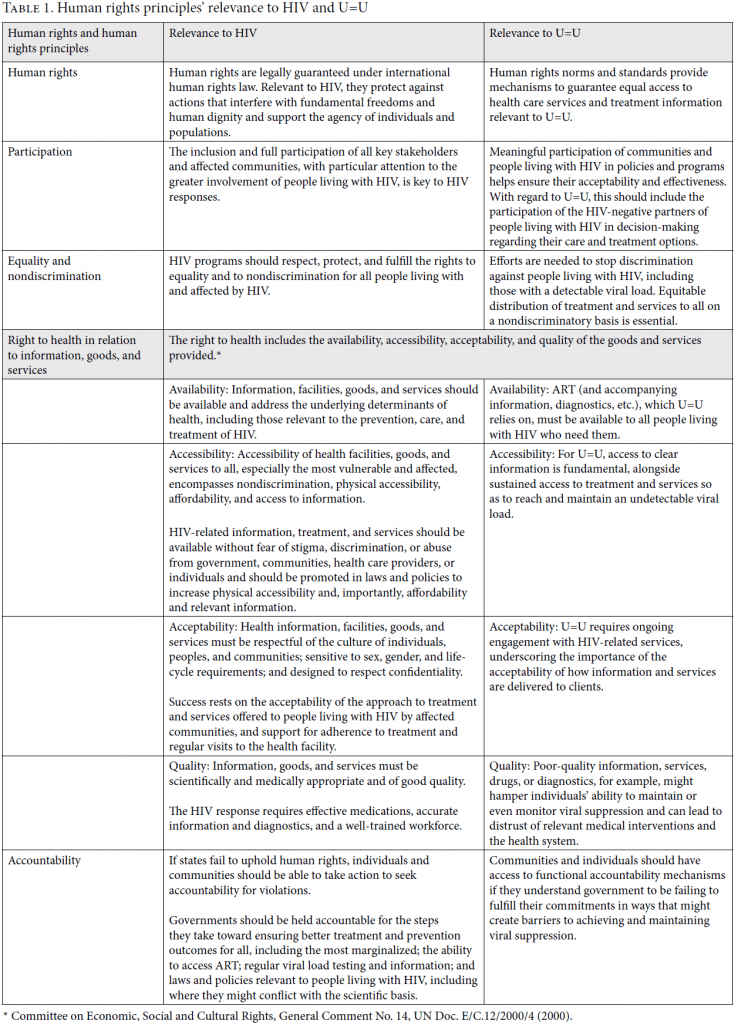
To clarify the ways in which human rights form the basis of our analysis, Table 1 identifies the range of human rights principles commonly considered relevant to HIV responses and provides a suggested overview of their relevance within the specific context of U=U. These rights then serve as subheadings for the grouping of information that follows in the findings section.
Gender equality is a long-recognized cornerstone of HIV responses, and there is wide recognition of the distinct barriers and challenges that women, men, transgender populations, and nonbinary populations face in relation to HIV prevention and treatment. Gender norms and dynamics are understood to affect access to resources and decision-making power, vulnerability to HIV infection, and people’s willingness and ability to access HIV-related services.[10] With respect to U=U, if gender norms and dynamics are ignored, many of the structural barriers that impede equitable access and use of HIV-related services are likely to remain in place, unchallenged, and unaddressed even if ART is available. On the flip side, systematic efforts to address gender-related barriers are a key step in ensuring that these strategies can work for everyone.[11]
Methods
Documents from global organizations that provide guidance and funds for ART provision were analyzed to determine their approach to U=U. The organizations and initiatives considered included the World Health Organization (WHO), UNAIDS, the Global Fund to Fight AIDS, Tuberculosis and Malaria (the Global Fund), and the US President’s Emergency Plan For AIDS Relief. Statements, guidelines, and other documents from leading nongovernmental organizations (NGOs) dealing with U=U policy and programming were also reviewed to examine how these organizations discuss U=U, with a focus on their approach to human rights and gender. The inclusion of global organizations and NGOs in this review was not exhaustive; rather, we included only those most widely used across the field as the basis for U=U and TasP recommendations.
In 2020, using PubMed, we conducted a literature review of articles published between 2006 and 2020. The search terms utilized included “U=U,” “TasP,” “treatment as prevention,” “gender,” “human rights,” and “rights.” Articles met inclusion criteria if they discussed TasP or U=U with attention to gender or rights and were published in English. Each piece was evaluated to assess if and how human rights and gender were addressed, and the ways in which recommendations included work to promote the realization of human rights and gender equality in future programming. Abstracts that explicitly discussed U=U and TasP presented at the 2019 International AIDS Conference were also reviewed to understand new and emerging research being done in the field. Data were extracted and analyzed to determine if and how this range of publications addressed gender and rights in order to understand the state of the field. No ethical review was required for this work.
Findings
Below, we provide an overview of how HIV-related guidance documents published by global institutions have considered human rights and gender equality. We then offer a more granular analysis of the extent to which and ways in which laws and policies, relevant human rights principles (see Table 1), and gender norms and dynamics are addressed in documented U=U efforts.
Global institutions’ general guidance
National HIV responses are shaped by a variety of factors, including not only national legal and policy environments and social constructs but guidance issued by global-level institutions. The approach taken in these guidance documents strongly impacts what is done and how it is done, including the degree of national-level governments’ understanding, and commitment to inclusion, of efforts to realize rights and promote gender equality in the HIV response. WHO, UNAIDS, the Global Fund, and the US President’s Emergency Plan For AIDS Relief each include, to varying degrees, attention to laws and human rights principles in their general HIV-related guidance, and, to some extent, there is also mention of rights within their individual discussions of U=U and TasP.[12] While these organizations’ documents recognize the importance of gender in terms of HIV, as well as the need to address gender dynamics in HIV programming, by 2020 only the Global Fund had noted the importance of addressing gender-related norms and dynamics in its U=U-specific guidance materials. The Global Fund notes that a biomedical approach to HIV is insufficient and that to promote U=U, it is critical to address the root causes of vulnerability for women and key populations, as well as the barriers to accessing health services faced by heterosexual men.[13]
Within its TasP guidance, WHO signals the importance of a rights framework to treat and eliminate HIV, highlighting rights-related barriers such as stigma and discrimination, inequity, lack of accessibility, and weak data and monitoring systems.[14] The Global Fund discusses rights—namely in relation to stigma and discrimination, accountability for data, and the need to address human-rights related barriers—in the design and delivery of products and programs.[15] The only one of these organizations to have issued guidance on human rights specifically in relation to U=U is UNAIDS. In its U=U Explainer, UNAIDS calls for the scale-up of comprehensive responses; awareness and knowledge of U=U; access to affordable, quality, stigma- and discrimination-free testing and treatment; and the need to address unjust criminalization that violates human rights and deters people living with HIV from accessing services.[16]
Laws and policies
Addressing the legal and policy barriers that inhibit the sustained access to treatment necessary for people living with HIV to achieve and maintain a suppressed viral load is key to U=U. Not only is the criminalization of HIV transmission detrimental to the overall HIV response, but it has been shown to be contrary to the science of U=U and to contribute to fear and anxiety among people living with HIV in ways that have a direct impact on implementation. U=U as a strategy can bring attention to the need for legal reform in the many contexts where HIV remains criminalized, and the promotion of U=U can be more systematically used to foster legal and policy changes, including the removal of HIV-specific criminalization laws. Other types of laws also create barriers to U=U, including laws that criminalize sex between men or the provision of harm-reduction programs for people who use drugs, because even if services are available these can result in people being afraid to access them.[17] Removing laws that criminalize people living with HIV and are otherwise vulnerable can also help shift public attitudes and reduce stigma, in turn helping support sustained access to treatment.[18]
In addition to the legal environment, a range of policies can impact the effectiveness of U=U. For example, national policies limiting comprehensive sexuality education restrict access to basic information about sex, sexuality, HIV, and HIV programs, which in turn can impact gender dynamics and result in limited awareness of U=U among young people and other key and vulnerable populations even when these services are available.[19]
Policies relating to U=U in and of themselves can be both barriers and facilitators. A range of HIV-specific government policies can make it impossible for people living with HIV to achieve an undetectable viral load. For example, in 2019, while 182 countries reported that ART can be initiated irrespective of CD4 count, seven countries reported not initiating ART until a client’s CD4 count dropped below 500 cells per cubic millimeter.[20] Thus, for some people living with HIV, U=U is unattainable simply because of how government shapes relevant policy. Additional policies that can either facilitate or hinder the accessibility of treatment include the frequency of required clinic visits, particularly when people live far from where services are available, due to the time and costs associated with multiple visits.[21]
Conversely, official government policies can improve accessibility of treatment and remove barriers to access. For example, the removal of upfront copayments for treatment or providing access to free ART to all people living with HIV can radically enhance access to the means of achieving an undetectable viral load.[22]
Participation
There is a noticeable lack of literature addressing participation specifically in the context of U=U. While the language of “nothing about us without us” and the concept of meaningful involvement of communities permeate HIV responses, how this is operationalized within the context of U=U appears to be under-explored within the literature.
Equality and nondiscrimination
Studies have long documented that stigma and discrimination create barriers to accessing relevant HIV information, treatment, and care. This has been found to be true specifically in the context of U=U.[23]
In line with its original intention, U=U can serve as a means to begin to dismantle both external and internalized stigma, as well as discrimination. Knowledge of U=U has been found to be associated with lower anxiety and depression and reductions in internalized stigma among, for example, Latin American men who have sex with men.[24] Highlighting the relevance of U=U to stigma reduction, a study in Vietnam identified key success factors that included government endorsement of the message, community leadership in campaigns at the national, provincial, and city levels, efforts to bring health workers on board, and having “champions” for the success of U=U.[25]
Of concern, the withholding of information about U=U has been found to occur among some health care providers, particularly with patients from marginalized populations. Documented factors include not only lack of provider knowledge but disbelief in U=U, and negative and discriminatory attitudes.[26] In some settings, the medical community has been accused of withholding messaging from patients both because of their fears that negligible risk of transmission is not zero risk and because of their judgment that patients cannot be trusted with this information.[27] In a 2013 study, fewer than half of the women surveyed were told by their providers that having an undetectable viral load was a form of prevention, even though most were engaged in care and on a successful treatment regimen; it goes without saying that this would have been useful information for them.[28] While it is certainly hoped that things have improved since that time, the study results provide an important cautionary tale. Research in the United States in 2020 found that while Black men who have sex with men expected their providers to initiate conversations around HIV transmission and U=U, the stigmatizing and discriminatory attitudes of some health providers made them less likely to share this information and decision-making power with their Black clients.[29]
The right to health: Availability, accessibility, acceptability, and quality of services
Within the health system, many different issues have been found to impact the success of U=U strategies. A human rights lens draws attention to the availability, accessibility, acceptability, and quality of the HIV treatment services delivered, as well as the access that people have to the information they need for informed decision-making, all with significant implications for the success of any U=U strategy. These issues are, of course, also gendered, with gender dynamics playing out and intersecting in relation to each. For example, some women may face challenges to accessing needed services if spousal permission is required, which might be further exacerbated if they are responsible for work or child care within limited facility opening hours. Transgender people may not find services acceptable if they are unable to present according to their gender identity, or if they are not allowed to access services if the gender marker on their identity document does not match how they live in the world.
Concerns have been raised about a potential disconnect between the dissemination of U=U messaging alongside the limited availability or accessibility of ART in some contexts: achieving an undetectable viral load is contingent on the sustained accessibility of ART, so any such mismatch must be addressed in U=U campaigns. There is a need, therefore, to consider U=U interventions not only on a country-by-country basis but at subnational levels, taking into account the health system and in particular the sustained availability of free or affordable treatment and viral load monitoring.[30] Where ART is available and accessible, the acceptability of TasP has been found to increase with people’s direct exposure to its success, such as with regular testing and exposure to positive testimonials disseminated in person or through mass media.[31]
Taking this one step further, there is a need to ensure the availability, accessibility, acceptability, and quality of a wide range of health information and services, including but not limited to HIV-specific services, to ensure the ultimate success of U=U. This could include not only pre-exposure prophylaxis but family planning, information and services related to sexually transmitted infections and sexual health (including in the context of condomless sex), and mental health services. The right to health reminds us that U=U cannot be implemented in isolation. While U=U offers opportunities for individuals to manage HIV and prevent onward transmission, these same individuals also need access to quality health services in a range of areas that can support their overall health and well-being, over and above the ability to reach and maintain viral suppression.[32]
Resource constraints impacting HIV responses are real, whether driven by decreases or limitations in donor funding, reluctance to fund services related to HIV or sexual and reproductive health, or the inability to ensure the sustainability of free treatment. Many settings have seen a move toward “AIDS fatigue” and decreases not only in funding but in political will, particularly in the context of COVID-19. Even if a U=U strategy is in place, funding shortfalls can negatively impact service availability and accessibility, resulting in drug stockouts, high costs, and a lack of consistent and reliable (or indeed any) viral load testing, with devastating impacts on clients even if appropriate policies are in place.[33]
The right to health: Availability, accessibility, acceptability, and quality of information
An analysis across 25 countries found that people living with HIV with adequate knowledge about U=U, not surprisingly, had more favorable health outcomes, including in relation to mental health, sexual health, treatment satisfaction, and viral suppression, than those who did not.[34] Yet, barriers exist in the ability to access updated, comprehensive, and culturally tailored information about U=U. The language used by researchers, NGOs, global institutions, public health officials, and health care providers matters and impacts both attitudes and access to care: clarity and non-judgmental messaging are always key.[35]
The science behind U=U tells us that negligible risk is zero risk in the context of sexual transmission. Since 2017, leading HIV scientists have promoted a semantic change and the use of phrasing such as “effectively zero,” “no risk,” or “cannot transmit” to resolve earlier incorrect or biased communications around U=U that may have prevented the medical community from delivering information about risk of transmission being effectively zero.[36] Even with these semantic shifts, however, messages still need to be tailored to individual contexts, communities, clients, and partners.
The provision of accurate information regarding U=U in health services is critical but so too is education and messaging at the community level. Widespread understanding of U=U can help reduce HIV-related stigma and discrimination within communities more generally, even as promoting such understanding often requires nuanced approaches. Millions of people living with HIV, as well as those at risk of infection, have yet to receive the facts and potential implications of U=U for their lives and those of their sexual partners. Of concern when messaging does take place, however, are the differences that have been found in the perception of accuracy of U=U messaging across various subgroups, including people who are HIV negative and gay and other men who have sex with men, depending on the source of the information. This is based on trust in the source, as well as how this intersects with such factors as socioeconomic status, race and ethnicity, geographic location, drug use, engagement in sex work, being on pre-exposure prophylaxis, and HIV status, highlighting the need for accurate targeted messaging campaigns to reach different groups.[37]
The issues described above call for nuanced, subgroup-specific health promotion messaging.[38] The involvement of NGOs and community members in government-led health programs even at the community level is critical, so that targeted and trusted messaging can shape prevention responses and allow for public participation.[39] Even within identified communities or population groups, none is monolithic or has uniform and predictable behaviors, underscoring the need for any community-level U=U messaging to be designed as an entry point for individual-level discussion.[40]
Accountability
Relatively little has been published about accountability in the context of U=U. One study was found in which providers acknowledged concern around providing information about U=U to patients for fear of being blamed if transmission nonetheless were to occur.[41] Issues of accountability of providers and other duty bearers for the provision of accurate U=U information and services to all who need them remain to be better addressed.
Gender
It seems that U=U research with women living with HIV, transgender populations, and nonbinary populations is only just beginning. Gay and other men who have sex with men appear to be the main populations studied in published U=U research to date.[42] Additionally, the intersection of gender with race and other factors is evident, but not often studied, creating additional layers of complexity to be tackled moving forward.
Widespread power inequalities have long been known to delay women’s access to viral load testing, which is necessary for U=U to be effective.[43] Fear of intimate partner violence and economic dependency have also been found to deter women from seeking treatment and care.[44] Two studies completed in 2017 with important implications for U=U included interviews with women, their male partners, and service providers in Kenya, South Africa, and Zimbabwe. In both cases, they found that providing HIV treatment to women was perceived by some as approving increased sexual freedom for women, a notion that is highly stigmatized, consequently leading to lower access and adherence to treatment.[45]
The exclusive focus of U=U messaging on sexual transmission of HIV, with little attention to its implications for transmission from parent to child, constitutes another real limitation from a gender perspective. In the absence of relevant information, women of reproductive age have struggled to understand the implications of U=U for the prevention of vertical transmission of HIV if their viral load is undetectable, suggesting once again that clearer messaging is required.[46]
Transgender and nonbinary people are well known to face great barriers in accessing ART, including because of the lack of knowledge and sensitivity among health care providers exacerbated by stigma, discrimination, and legal impediments more broadly. Issues of concern identified in one study include those associated with poor mental health, substance use, violence, lack of family support, homelessness, and unemployment, all of which can compromise the ability to achieve a suppressed viral load.[47]
Tackling the gender stereotypes and dynamics that disadvantage specific people is critical to the success of U=U, and critical to addressing the structural, health system, and community- and individual-level factors that influence the effectiveness of these interventions.
Conclusion
While much U=U research and many interventions have focused on the reductions in epidemiological risk of HIV transmission during different types of sexual intercourse, including condomless vaginal sex and condomless anal sex, far fewer efforts have been made to address the legal, rights-related, and gender-related factors that play key roles in influencing people’s ability to reach and maintain undetectable viral loads. As discussed above, examples of success in bringing in rights concerns and understanding gender dynamics as they relate to U=U exist but are limited. Most of the interventions found considered only one or two rights principles, and none attempted to systematically address all the legal, rights, and gender concerns noted above, even as each has, individually, been shown to bring benefits for U=U.[48] Notably, the human rights principles of participation and accountability have received very little explicit attention in documented U=U efforts to date.
This analysis has underscored how U=U interventions can incorporate efforts to understand and address local gender norms and dynamics, as well as benefit from explicit attention to the legal environment and realization of the human rights principles and standards outlined in Table 1. The findings from this work can provide signposts as to ways in which, with systematic attention to rights and gender, the legal and policy environment, health systems, and community environments can be strengthened to ensure that U=U works for all people. This is broader than the purely biomedical approach that is so often at the center of U=U efforts.
The success of U=U is contingent on the environment of structural and societal factors beyond the mere availability of ART, many of which are out of an individual’s explicit control. Increased focus on ensuring the availability and accessibility of functional mechanisms of accountability can help promote attention to the range of structural issues identified above, drawing attention to who is responsible for taking action, where programming is succeeding, and, importantly, where programming is falling short and what steps are needed to ensure that U=U achieves its potential for its intended beneficiaries. Far more attention is needed to the differences among and within national and local contexts, as programming will play out differently given the structural, cultural, legal, health system, and gender dynamics that exist. Community participation in accountability schemes is as key as it is to involvement in the planning and design of U=U interventions.
NGOs such as the International Community of Women Living with HIV, the International Council of AIDS Service Organisations, and the Prevention Access Campaign have been extremely vocal about many of these issues, but despite these efforts there remains a lack of explicit attention to gender dynamics and human rights considerations in research and programming efforts concerned with U=U. What does exist is limited largely to the need to address human rights-related barriers regarding accessibility, affordability, and stigma and discrimination.[49] This is necessary but not sufficient.
The COVID-19 pandemic has highlighted the inadequacies of health care systems around the world to tackle growing threats on top of their current responsibilities. The last few years have seen increasing declines in funding and attention to HIV programming, justified by the perceived urgency of addressing COVID-19, exacerbating preexisting reductions in HIV funding globally.[50] The 2021 Political Declaration on HIV and AIDS calls for an end to the inequalities that persist within both the COVID-19 and the HIV pandemics and pushes for the world to prioritize the right to health for all without discrimination.[51] This must be the approach taken to U=U in all respects, including financially and programmatically.
U=U is an incredible scientific advance: it can have the most impact where it is boldly embraced, clearly articulated, and tailored to reach those who need it most. A systematic approach to understanding and addressing the legal, human rights, and gender-related factors noted here can bolster the effectiveness of U=U messaging and programming and can be utilized across geographical contexts. There is sufficient evidence of what is needed to ensure that as U=U rolls out across the world, it creates benefits, and that these benefits accrue to all populations, not just those who are easiest to reach.
Laura Ferguson, PhD, SM, MA, is the research director at the USC Institute on Inequalities in Global Health, University of Southern California, Los Angeles, USA.
William Jardell, MPH, is a program specialist in the USC Institute on Inequalities in Global Health, University of Southern California, Los Angeles, USA.
Sofia Gruskin, JD, MIA, is the director of the USC Institute on Inequalities in Global Health, University of Southern California, Los Angeles, USA.
Please address correspondence Laura Ferguson. Email: laura.ferguson@med.usc.edu.
Competing interests: None declared.
Copyright © 2022 Ferguson, Jardell, and Gruskin. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Global Commission on HIV and the Law, Risks, Rights and Health (New York: Global Commission on HIV and the Law, 2012).
[2] P. Vernazza, B. Hirschel, E. Bernasconi, and M. Flepp, “Les personnes séropositives ne souffrant d’aucune autre MST et suivant un traitement antirétroviral efficace ne transmettent pas le VIH par voie sexuelle,” Bulletin des Médecins Suisses 89 (2008).
[3] A. J. Rodger, V. Cambiano, and T. Bruun, “Sexual Activity without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy,” JAMA 316/2 (2016); R. W. Eisinger, C. W. Dieffenbach, and A. S. Fauci, “HIV Viral Load and Transmissibility of HIV Infection: Undetectable Equals Untransmittable,” JAMA 321/5 (2019).
[4] UNAIDS, End Inequalities. End AIDS. Global AIDS Strategy 2021–2026 (Geneva: UNAIDS, 2021).
[5] Prevention Access Campaign, “Consensus Statement: Risk of Sexual Transmission of HIV from a Person Living with HIV Who Has an Undetectable Viral Load” (2019), https://www.preventionaccess.org/consensus.
[6] Ibid.
[7] UNAIDS, Political Declaration on HIV and AIDS: Ending Inequalities and Getting on Track to End AIDS by 2030 (Geneva: UN General Assembly, 2021).
[8] S. Gruskin, L. Ferguson, and J. O’Malley, “Ensuring Sexual and Reproductive Health for People Living with HIV: An Overview of Key Human Rights, Policy and Health Systems Issues,” Reproductive Health Matters 15/Suppl 29 (2007).
[9] S. Gruskin, E. J. Mills, and D. Tarantola, “History, Principles, and Practice of Health and Human Rights,” Lancet 370/9585 (2007).
[10] UNAIDS, UNAIDS Gender Assessment Tool: Towards a Gender-Transformative HIV Response (Geneva: UNAIDS, 2018).
[11] Global Fund to Fight AIDS, Tuberculosis and Malaria, “HIV and AIDS” (2020), https://www.theglobalfund.org/en/hivaids/.
[12] Ibid.; Global Fund to Fight AIDS, Tuberculosis and Malaria, HIV, Human Rights and Gender Equality (Geneva: Global Fund, 2019); World Health Organization, Programmatic Update: Antiretroviral Treatment as Prevention (TasP) of HIV and TB (Geneva: World Health Organization, 2012); Global Fund to Fight AIDS, Tuberculosis and Malaria, Step Up the Fight: Focus on Human Rights (2019), https://www.theglobalfund.org/media/8119/publication_humanrights_focuson_en.pdf; PEPFAR, Strategy for Accelerating HIV/AIDS epidemic Control (2017–2020) (Washington, DC: US Department of State, 2017).
[13] Global Fund to Fight AIDS, Tuberculosis and Malaria (2020, see note 11); Global Fund to Fight AIDS, Tuberculosis and Malaria, HIV, Human Rights and Gender Equality (see note 12).
[14] World Health Organization (2012, see note 12).
[15] Global Fund to Fight AIDS, Tuberculosis and Malaria, HIV, Human Rights and Gender Equality (see note 12).
[16] UNAIDS, Undetectable = Untransmittable: Public Health and HIV Viral Load Suppression (2018), https://www.unaids.org/sites/default/files/media_asset/undetectable-untransmittable_en.pdf.
[17] T. Bereczky, “U=U Is a Blessing: But Only for Patients with Access to HIV Treatment; An Essay by Tamás Bereczky,” BMJ 366 (2019).
[18] A. S. Breslow and M. E. Brewster, “HIV Is Not a Crime: Exploring Dual Roles of Criminalization and Discrimination in HIV/AIDS Minority Stress,” Stigma and Health 5/1 (2020); J. C. Phillips, A. Webel, C. D. Rose, et al., “Associations between the Legal Context of HIV, Perceived Social Capital, and HIV Antiretroviral Adherence in North America,” BMC Public Health 13 (2013).
[19] M. Muñoz, V. Zalazar, M. Vazquez, et al., “Knowledge of HIV, Access to HIV Testing and Awareness of PEP, PrEP and U=U among Adolescent Boys and Young Men Who Have Sex with Men in Argentina” (presentation at the International AIDS Conference, 2020).
[20] World Health Organization, “WHO Policy Data 2019: Recommended ART CD4 Initiation Threshold in Adults and Adolescents” (2019), http://lawsandpolicies.unaids.org/topicresult?i=38.
[21] Prevention Access Campaign, “Programs,” https://preventionaccess.org/programs.
[22] D. Callander, M. Stoové, A. Carr, et al., “A Longitudinal Cohort Study of HIV ‘Treatment as Prevention’ in Gay, Bisexual and Other Men Who Have Sex with Men: The Treatment with Antiretrovirals and their Impact on Positive and Negative men (TAIPAN) study protocol,” BMC Infectious Diseases 16/1 (2016).
[23] Prevention Access Campaign (see note 21); I. Prado Generoso, “The Relation of Internalized Homonegativity with HIV Prevention Strategies: Results from Latin-America MSM Internet Survey (LAMIS) in Brazil” (presentation at the International AIDS Conference, 2020).
[24] M. Reyes-Diaz, A. J. Schmidt, M. A. Veras, et al., “Undetectable=Untransmissible (U=U) Knowledge and Sexual Behavior during the Most Recent Sexual Encounter with Non-steady Partners among MSM in the Latin-American MSM Internet Survey (LAMIS)” (presentation at the International AIDS Conference, 2020).
[25] A. Nguyen, “Undetectable = Untransmittable (U=U) to Drive Stigma Reduction and Epidemic Control in Vietnam: A Global Model for Political and Program Innovation” (presentation at the International AIDS Conference, 2020).
[26] O. G. Ford, “Understanding Undetectable Equals Untransmittable: A Growing Global Community Builds a Movement,” POZ (February 18, 2019), https://www.poz.com/article/understanding-undetectable-untransmittable; S. K. Calabrese and K. H. Mayer, “Stigma Impedes HIV Prevention by Stifling Patient-Provider Communication about U = U,” Journal of the International AIDS Society 23/7 (2020).
[27] Ford (2019, see note 26).
[28] Ibid.
[29] Calabrese and Mayer (see note 26).
[30] UNAIDS (2018, see note 16).
[31] S. C. Kalichman, C. Cherry, M. O. Kalichman, et al., “Mobile Health Intervention to Reduce HIV Transmission: A Randomized Trial of Behaviorally Enhanced HIV Treatment as Prevention (B-TasP),” Journal of Acquired Immune Deficiency Syndromes 78/1 (2018); A. C. Mooney, A. Gottert, N. Khoza, et al., “Men’s Perceptions of Treatment as Prevention in South Africa: Implications for Engagement in HIV Care and Treatment,” AIDS Education and Prevention 29/3 (2017).
[32] M. E. Charurat, B. Emmanuel, C. Akolo, et al., “TRUST Study Group: Uptake of Treatment as Prevention for HIV and Continuum of Care among HIV-Positive Men Who Have Sex with Men in Nigeria,” Journal of Acquired Immune Deficiency Syndromes 68/Suppl 2 (2015).
[33] Bereczky (see note 17).
[34] C. Okoli, B. Richman, B. Allan, et al., “A Tale of Two ‘U’s and Their Use by Healthcare Providers: A Cross-Country Analysis of Information-Sharing about ‘Undetectable = Untransmittable’ (U=U)” (presentation at the International AIDS Conference, 2020).
[35] “HIV and Language,” POZ (2022), https://www.poz.com/basics/hiv-basics/hiv-language.
[36] “The Evidence for U=U (Undetectable = Untransmittable): Why Negligible Risk Is Zero Risk,” i-Base (October 1, 2017), https://i-base.info/htb/32308.
[37] H. J. Rendina and J. T. Parsons, “Factors Associated with Perceived Accuracy of the Undetectable = Untransmittable Slogan among Men Who Have Sex with Men: Implications for Messaging Scale-up and Implementation,” Journal of the International AIDS Society 21/1 (2018).
[38] Ibid.
[39] S. S. Monteiro, M. Brigeiro, W. V. Vilella, et al., “Desafios do tratamento como prevenção do HIV no Brasil: Uma análise a partir da literatura sobre testagem,” Ciencia e Saude Coletiva 24/5 (2019).
[40] J. Chikovore, N. Gillespie, N. McGrath, et al., “ANRS 12249 TasP Study Group: Men, Masculinity, and Engagement with Treatment as Prevention in KwaZulu-Natal, South Africa,” AIDS Care 28/Suppl 3 (2016).
[41] Calabrese and Mayer (see note 26).
[42] B. Jungwirth and M. Helfand, “This Week in HIV Research: Do You Believe in U=U?” TheBodyPro (February 27, 2020), https://www.thebodypro.com/slideshow/week-hiv-research-undetectable-equals-untransmittable-belief.
[43] ICASO, Understanding U=U for Women Living with HIV: ICASO Community Brief (Toronto: ICASO, 2018).
[44] Kalichman et al. (see note 31); Chikovore et al. (see note 40).
[45] A. M. Minnis, E. T. Montgomery, S. Napierala, et al., “Insights for Implementation Science from 2 Multiphased Studies with End-Users of Potential Multipurpose Prevention Technology and HIV Prevention Products,” Journal of Acquired Immune Deficiency Syndromes 82/Suppl 3 (2019).
[46] ICW, “U=U + Women: Minding the Gaps” (presentation at the International Community of Women Living with HIV, June 18, 2020), https://www.thewellproject.org/groups/hiv-eventsconferences/webinar-topic-uu-women-minding-gaps-june-18-2020.
[47] M. Teti, L. A. Bauerband, and C. Altman, “Adherence to Antiretroviral Therapy among Transgender and Gender Nonconforming People Living with HIV: Findings from the 2015 U.S. Trans Survey,” Transgender Health 4/1 (2019).
[48] See, for example, Muñoz et al. (see note 19); Charurat et al. (see note 32); ICW (see note 46).
[49] World Health Organization (2012, see note 12); PEPFAR (see note 12).
[50] G. Barrow and C. Barrow, “HIV Treatment as Prevention in Jamaica and Barbados: Magic Bullet or Sustainable Response?,” Journal of the International Association of Providers of AIDS Care 14/1 (2015).
[51] UNAIDS (2021, see note 7).