The Politics of Drug Rehabilitation in the Philippines
Volume 24/1, June 2022, pp. 147-158 | PDF
Gideon Lasco and Lee Edson Yarcia
Abstract
The international consensus to end compulsory drug treatments and close forced rehabilitation facilities needs urgent transformation to country policies. In the Philippines, as with other countries in Asia, rehabilitation can be compulsory and is seen as the humane alternative to the “war on drugs.” In this paper, we present the landscape of rehabilitation and narrate the ways in which people who use drugs are forced to undergo treatment. We unpack the politics behind rehabilitation and explain the sociocultural foundations that support compulsory treatment. We argue that a transition to a human rights-based approach, including voluntary alternatives in community settings, is possible by capitalizing on the reforms that are, unwittingly, the result of the “war on drugs.”
This paper analyzes the Philippines as a case study of how politics and populism have framed the understanding and implementation of drug rehabilitation, particularly in an unstable democracy with a long history of authoritarianism and oligarchic patrimonialism.[1] The Philippines has taken global center stage since the Duterte administration’s launch of a “war on drugs” in 2016, with much attention and concern focused on extrajudicial killings—numbering at least several thousand—in connection with this campaign.[2]
Less critically examined, however, is how this period—during which drugs have been at the forefront of political and public discourse—has shaped compulsory drug interventions in the country. Compulsory treatment in the Philippines occurs inside spectacular “mega rehabilitation centers” and in the context of a growing number of public and private drug treatment facilities.[3] During the height of the “war on drugs,” the police conducted door-to-door searches in order to compel people who use drugs to “surrender”—effectively a form of forced apprehension—and undergo “voluntary” rehabilitation.[4] Philippine drug courts continued ordering people who use drugs to undergo rehabilitation in government centers or inside jails, with rehabilitation considered a penalty under the national drug law.[5] In recent years, promising community-based programs have operated in parallel with compulsory detention and involuntary treatment, but difficulties have arisen in implementing a fully autonomy-respecting system given the punitive legal environment for people whose lives include drugs.[6]
In this case study, we argue that long-standing perceptions on drugs in the Philippines have created an uncritical acceptance that people who use drugs require “rehab” and, consequently, a permissive political environment for compulsory detention and involuntary treatment. Moreover, we argue that the punitive drug regime has reinforced similarly pernicious attitudes by presenting forced “rehab” as the humane and acceptable alternative to extrajudicial killings. To support our findings, we present figurations of “rehab” in the country over the past six years, from the Duterte administration’s statements and programs to the policy pronouncements of those who are running to succeed him in the 2022 elections. We explain this fixation on treating people who use drugs as either criminals or patients—in both cases deemed as without full autonomy to make informed and moral personal decisions—as a product of exploited populism in a predominantly Catholic country. Drawing from international human rights obligations in relation to drug policy, we conclude by identifying critical leverage points and structural factors that drug policy reformists in unstable democracies can maneuver toward a public health-centered framework that respects full patient autonomy and human dignity.
The drug rehabilitation landscape in the Philippines
Duterte’s election to the highest post in the country was premised on a relentless and sustained fight against criminality, illegal drugs, and corruption.[7] On his first day in office, Duterte appointed his former city police chief Ronald dela Rosa to implement his “war on drugs” to fulfill his campaign promise of eliminating illegal drugs in three to six months.[8] As noted by the Office of the United Nations High Commissioner for Human Rights, between July 1, 2016, and November 27, 2017, there was a staggering average of nearly 40 deaths per day as a result of drug operations by the police and from homicides perpetrated by unidentified persons.[9] The prosecutor of the International Criminal Court subsequently requested authorization to open an investigation in the Philippines after finding reasonable basis to believe that the crime against humanity of murder was being committed in the context of the government’s “war on drugs.”[10]
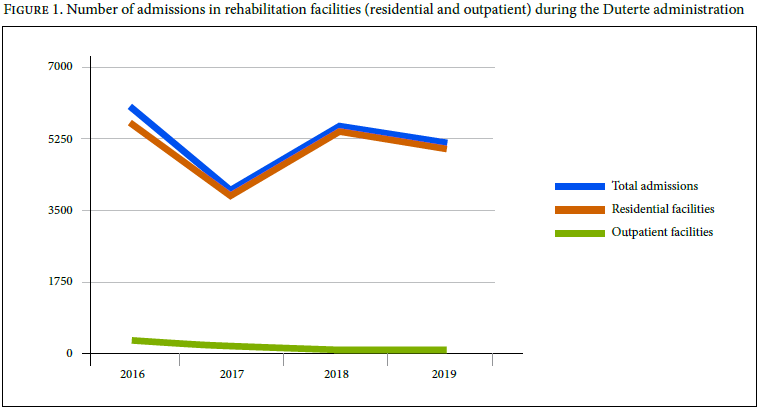
Against the backdrop of extrajudicial killings apparently perpetrated pursuant to an official state policy of the Philippines, the drug rehabilitation landscape in the Philippines was changing in light of the threat to life and liberty of people who use drugs.[11] The 2016 statistics of the Philippine Dangerous Drugs Board (DDB) showed that 6,079 individuals were admitted to residential and outpatient facilities nationwide for rehabilitation.[12] A year later, the data showed a decrease in admission to 4,045 individuals, equivalent to a 33% reduction.[13] This substantial drop in admissions is understandable in light of the threat to life and liberty of people who are identified to be using drugs. In 2018, a significant 34.55% increase in admission was reported, largely due to a court-directed policy that allowed for plea bargaining by persons charged with criminal cases, which made up 24.89% of the 5,447 admissions for the year.[14] The 2019 data showed increasing admissions due to plea bargaining agreements, but an overall slight decrease of 4.04% in total admissions was observed, attributed to individuals’ “voluntary submission” to community-based drug rehabilitation.[15] Figure 1 shows the number of persons who use drugs who were admitted to rehabilitation facilities from 2016 to 2019. Close to the end of Duterte’s term, a total of 55 treatment and rehabilitation facilities were operating, up from 31 centers before the start of his presidency.[16]
In November 2016, Duterte inaugurated a 10-hectare compound, dubbed a “mega rehab center,” designed to house as many as 10,000 persons who “surrendered” and would undergo treatment.[17] According to the compound’s chief medical officer, Nelson Dancel, a typical day in the center starts at 5:30 a.m., when residents are required to do a series of physical exercises similar to those required in the army, followed by activities meant to teach the concepts of self-acceptance, self-development, and self-formation.[18] For recreation, the mega rehab center boasts basketball and volleyball courts, chess boards, and musical instruments, with television reserved as a privilege for more senior residents.[19] Dancel explains that escapes are a natural occurrence since some residents feel homesick or worry about their families; individuals who attempt to escape but fail are segregated from other residents, but Dancel is quick to clarify that they are not in solitary confinement.[20] If violations are severe, residents receive extra physical work, such as exercises or additional chores.[21]
Nevertheless, the protocols in the mega rehab center reflect typical programs in drug treatment and rehabilitation centers nationwide. Guided by the Manual of Operations for Drug Abuse Treatment and Rehabilitation Centers, which sets the minimum standards for this type of facility, the Department of Health accredits rehabilitation centers—both government and nongovernment owned or operated—based on their compliance with these prescribed uniform standards.[24] Notably, the manual enumerates the prescribed services, which are replicated here for a fuller appreciation of the mandated programs in rehabilitation centers:
- Medical service provides comprehensive health care services ranging from routine physical examination and screening procedure for diagnosis, treatment and follow-up of illnesses and other medical problems.
- Psychiatric service provides therapy to drug abusers with behavioural and psychiatric disorders through, among others, chemotherapy, individual and group psychotherapy, family therapy and occupational therapy conducted by a psychiatric team. A psychiatric team shall include a psychiatrist, psychologist and social worker. This may include an occupational therapist and para-professional worker.
- Psychological service assists the team in the assessment, diagnosis and management of drug dependents through psychological testing and evaluation as well as in conducting therapy/counselling to patients and their families.
- Social service assists the drug dependents help themselves cope [with] their problems, facilitate and/or promote their interpersonal relationship and adjustment to the demands of a treatment program with the end view of helping the drug dependents’ physical, social, moral and spiritual development.
- Spiritual and religious services include the development of moral and spiritual values of the drug dependent. It has been noted that the spiritual foundation of patients has been very weak that this could not provide support to them to enable them to cope with their problems and conflicts. Strengthening the spiritual foundation would involve, among others, reorientation of moral values, spiritual renewal, bible study and other charismatic sessions. It aims to bring them closer to God and better relate to their fellowmen. Various religious and civic organizations can be contacted to provide services. Spiritual counselling shall be helpful in aiding and resolution of individual and family problems.
- Referral service involves the process of identifying accurately the problems of the patient and sending him to the agency that can provide the appropriate services.
- Sports and recreation services provide facilities for sports and recreation to offer patients the opportunity to engage in constructive activities and to establish peer relationship as an alternative to drug abuse. The emphasis in all activities should be on developing the discipline necessary to improve skills and on gaining respect for good physical health.
- Residential/house care service includes provision of basic foods, clothing and shelter.
- Aftercare and follow-up services provided to the patient after the primary rehabilitation program. Aftercare activities can be viewed as the first line of defence against relapse. The activities include attending self-help programs like Narcotics Anonymous (NA) / Alcoholic Anonymous (AA) meetings, regular follow-up at treatment Center, individual and group counsellings sponsor/sponsee meetings, alumni association meetings, etc. This is for a period not exceeding eighteen (18) months and should be undertaken by the appropriate Center personnel.[25]
The manual further provides optional additional services, which may include placement service for work opportunities, volunteer service opportunities to assist the rehabilitation center, and educational opportunities.[26] Centers are mandated to contribute effectively to the goals of the Comprehensive Dangerous Drugs Act of 2002, which expresses the state policy of pursuing “an intensive and unrelenting campaign against the trafficking and use of dangerous drugs and other similar substances [including provision of] effective mechanisms or measures to re-integrate into society individuals who have fallen victims to drug abuse or dangerous drugs through sustainable programs of treatment and rehabilitation.”[27]
Presently, people who use drugs undergo drug treatment and rehabilitation programs and services following the guidelines set under Board Regulation No. 7 of 2019 by the DDB. Under this regulation, a verified application must be filed to the DDB to access a treatment and rehabilitation program. The application may be made by the person who uses drugs or by parents, spouses, guardians, or relatives within the fourth degree of consanguinity.[28] Upon recommendation by an accredited physician, “taking into consideration his/her level of drug dependency and the potential danger he/she may pose to himself/herself, his/her family and the community,” the DDB shall file a petition to the appropriate court for the confinement of the person for treatment and rehabilitation.[29] The court shall then order the person to undergo a drug dependency examination by an accredited physician, and, if certified to be drug dependent, “he/she shall be ordered by the court to undergo treatment and rehabilitation in a center designated by the Board for a period of not less than six (6) months.” Notably, the examination is conducted by physicians accredited by the Department of Health, with reference to the clinical parameters of drug dependency under the International Classification of Diseases, 10th revision.[30]
Modes of compulsion in drug treatment and rehabilitation during Duterte’s administration
Under the Duterte administration, persons who use drugs may be compelled to undergo drug rehabilitation through three major modes: first, through a police and law enforcement-directed door-to-door search and “request to surrender” campaign known as Oplan Tokhang; second, through court-mandated rehabilitation of people arrested for drug use; and third, through family-initiated admission without the consent of the person who uses drugs. The second and third modes are not unique to the Duterte administration, but a significant increase in arrests have been noted in the past six years, leading to congestion in jails.[31]
On the day of his appointment as chief of the Philippine National Police, dela Rosa issued a circular entitled PNP Anti-Illegal Drugs Campaign Plan – Project “Double Barrel,” where he ordered the police “to clear all drug affected barangays across the country.”[32] The international community was shocked by this policy’s aftermath, with the Office of the United Nations High Commissioner for Human Rights reporting 5,601 killed based on information from the Philippine Drug Enforcement Agency; government data mentions 16,355 “homicide cases under investigation” as accomplishments in the fight against illegal drugs, while 20,322 deaths are reported from drug operations by police and homicides perpetrated by unidentified persons.[33] Less visible in the international public discourse is the plight of 223,780 persons arrested for drug-related cases, which led to massive congestion in jails—85% to 90% of those incarcerated are there for drug-related offenses.[34]
The police have also conducted house-to-house visitations, which do not require search or arrest warrants, to “encourage voluntary surrender” to the government for drug-related acts.[35] Refusal leads to an immediate case build-up and “negation,” a term appearing in the aforementioned circular that could be interpreted by the police as permission to kill.[36] The DDB has noted “unprecedented responses from both law enforcement and the public,” including “voluntary surrender of self-confessed drug personalities nationwide.”[37] Under Board Regulation No. 3 of 2016, a “surrenderer” shall subscribe to an affidavit of undertaking and waiver that authorizes a medical examination and drug test; and if the individual in question is not engaged in trafficking or sale and is just using drugs, they shall state in the affidavit that “he/she shall undergo voluntary treatment and rehabilitation.”[38]
According to the most recent data from the Bureau of Jail Management and Penology, there are now 80,162 persons deprived of liberty detained for violation of the national drug law.[39] On November 8, 2021, the bureau signed a memorandum of agreement with the DDB so that such persons who have signed a plea bargain and who are classified as “low risk” or “moderate risk” for drug dependence may undergo court-mandated treatment and rehabilitation while in jail.[40]
Long-standing perception on drug rehabilitation: “Save the user, jail the pusher”
The above policies and programs cannot be disentangled from the long-standing perception—characterized by some scholars as a “moral panic”—that people who use drugs are “addicts” and societal villains.[41] This prohibitionist paradigm, which is perhaps best summed up by the popular slogan “save the user, jail the pusher,” has been reflected in various institutions throughout past half century, from the Catholic Church to broadcast and print media.[42] Essentially, this part-moralistic, part-medicalized view forges divisions between “pushers” and “addicts” who are a menace to society and “users” (often depicted as young people) who need to be “saved.” As the Catholic Bishops’ Conference of the Philippines wrote in a pastoral letter that coincided with Ferdinand Marcos’ ascendancy:
A country whose youths are mental and physical wrecks will be hopelessly doomed to ignominy unredeemable until, if that is possible, a new and strong breed will rise up from the ruins. These are the worst saboteurs and are worthy of the highest punishments. For they destroy the youth, the hope of the land.[43]
Rehabilitation centers figure in this narrative as sites where this “salvation” and “healing” can take place. In the words of a Catholic leader touting the church’s rehabilitation program, “Everybody needs healing. These drug addicts, they’ve been wounded very much and what they need is someone who can help them.”[44] Indeed, many such programs are affiliated with religious organizations; those who are not nonetheless orient themselves around the same themes of healing, redemption, and salvation.[45]
Duterte’s punitive approach to drugs has arguably made rehabilitation an even more socially and politically viable position—an alternative to the extrajudicial killings that allows individuals and institutions to continue being seen as “tough” on drugs while also satisfying civil society’s clamor for human rights.
Notably, however, drug treatment and rehabilitation remains largely compulsory in the Philippines, with evidence-based initiatives in some communities seen as the exception to general forced treatments that often have little or no scientific basis. As reported by the United Nations Office on Drugs and Crime and UNAIDS, the Philippines continues to detain people who use drugs in closed settings, often against their will, without sufficient human rights safeguards and forces them to undergo rehabilitation for an average duration of ten months.[46] Government data show severe overcrowding and substandard compulsory facilities, as well as little evidence supporting the use of spiritual or religious interventions.[47] People who use drugs are coerced to undergo treatment in order to “cure” themselves of their addiction.
A number of episodes during the Duterte administration are illustrative. In response to the first few months of Duterte’s drug war, for instance, the Catholic bishops remonstrated in another pastoral letter:
Our hearts reach out in love and compassion to our sons and daughters suffering from drug dependence and addiction. Drug addicts are children of God equal in dignity with the sober ones. Drug addicts are sick brethren in need of healing deserving of new life. They are patients begging for recovery. They may have behaved as scum and rubbish but the saving love of Jesus Christ is first and foremost for them. No man or woman is ever so unworthy of God’s love.[48]
As criticism mounted, including from the political opposition, Duterte at one point appointed Vice President Leni Robredo—the highest-ranking member of the opposition—as chair of the Inter-Agency Committee on Anti-Illegal Drugs. Although her tenure was short-lived—17 days—her report, which she published months after, is reflective of her view.[49]
Finally, the campaign for Duterte’s successor in the May 2022 elections—still underway at the time of writing—is also reflective of the same view. Virtually all the major candidates have expressed support for an “intensified” anti-drug campaign while vowing to respect human rights and promote a “public health” approach. Invariably, however, their idea of what constitutes “public health” includes scaling up the same rehabilitation paradigm that dichotomizes between killing and “rehab.”
Tellingly, when the leading candidate—Ferdinand Marcos Jr.—was accused by Duterte as using cocaine, his opponents lost no time in calling out the contradictions in Duterte’s drug war—while also calling on Marcos to be punished, as expressed in this tweet by Leody de Guzman, standard-bearer of the progressive left:
Tiyak, kilalang kilala ni Duterte kung sino ang supplier ng kandidatong ‘yan na nagpapasok ng cocaine sa bansa. ‘Yan dapat ang pokusan para mahuli at matigil na. Kaysa itsismis lang, ipahuli na ang kandidatong ‘yan para ipa-rehab. [For sure, Duterte knows who the supplier is of that candidate who trafficks cocaine in the country. That should be the focus so that he can be arrested and stopped. Instead of rumor-mongering, the candidate should be arrested and placed in rehab.][50]
For her part, Robredo has hewed close to the same discourse she raised as chair of the Inter-Agency Committee on Anti-Illegal Drugs:
In my belief, once DDB sits as the chair of DDB, its plan will not be just “kill, kill, kill” but the plan will be more comprehensive—heavy on prevention, heavy on rehabilitation.[51]
These political discourses reflect and reinforce the moral panic on drugs that sees rehabilitation as the humane (and only) way to “save the user,” precluding other initiatives such as harm reduction and decriminalization, which—notably—none of the candidates have mentioned.
Drug rehabilitation and populism
What can explain the subscription to the “save the user” narrative that has led to uncritical support for “rehabilitation” as it is (mis)understood by the Philippine public?
As discussed above, previous scholars have used the literature on “moral panic” to explain the long-standing vilification of drugs in the country. Drawing on the literature on penal and medical populisms, more recent scholarship has implicated political actors in reflecting and reinforcing public attitudes about drugs, portraying these actors as “moral entrepreneurs” who simplify, spectularize, and forge divisions between “addicts” and the virtuous public.[52]
Missing in these accounts, however, is the nuance regarding what people view as the rightful solution to the “problem.” Survey after survey has shown that Filipinos favor a strong approach to drugs—even approving of the “drug war”—despite the fact that they disapprove of the killings, suggestive that far from a monolithic dichotomy between supporting or opposing a draconian approach to drugs, people are divided on what particular draconian approach to take: either drug addicts deserve to be killed or drug addicts should be sent to compulsory rehabilitation.
Less emphasized in the scholarship is how Philippine drug policy has followed global drug policy flows; most notably, as Christopher Hobson notes, “among all the possible wrongdoing and bad things that exist in the world, it is slightly counterintuitive that drugs are the only one to be labelled as ‘evil’ in international law.”[53] Indeed, the first drug war in the 1970s coincided with the Nixon-era war on drugs and global commitments to the “drug problem,” leading to the establishment of DDB in 1972 and inaugurating a trend of increasingly punitive drug laws. The parallels in high incarceration rates in the United States and the Philippines and similar institutional configurations (e.g., a Philippine Drug Enforcement Agency patterned after a similarly named agency in the United States) speak of how this international—and particularly American—influence continues to have an impact on drug policy in the country.[54]
However, it must be pointed out that even as “Western democracies” and even international organizations are moving away from this approach, the Philippines and other countries in the region have steadfastly adhered to it (with notable exceptions such as Malaysia), suggesting that such an approach has been indigenized, likely enabled by a cultural environment that emphasizes “Asian values” such as conformity and social control, as well as the enduring valance of drugs as a populist trope in the region.[55]
Because they do not specifically address the question of why a particular form of rehabilitation has gained uncritical popular and political acceptance, these explanations are at best partial and would require corroboration through cultural histories and contemporary ethnographic accounts of rehabilitation today. However, they suffice to furnish a historical context to the figurations of rehabilitation in today’s political discourse that in turn perpetuate popular perceptions.
Compulsory rehabilitation in the Philippines an urgent human rights issue
There is a dangerous tendency for reform advocates to condemn extrajudicial killings and due process rights violations as human rights concerns, while supporting rehabilitation as an acceptable alternative. As we have observed, the motivations behind gross human rights violations and forcing people to treatment are the same: the dehumanization of people who use drugs and the removal of their autonomy to decide on the treatment approaches that respond to their felt needs. Drug policies in the Philippines remain to be “substance-centric, moralistic, and medicalized.”[56] Present drug policy from the Department of Health does not recognize non-pathological use, as substance use is classified as mild, moderate, or severe and, in any case, as requiring medical or psychological interventions.[57] Because treatments are compulsory in nature, the right to health, which includes access to voluntary and evidence-based services, is breached.[58]
Relatedly, drug testing has been transformed into a diagnostic and prosecutorial tool for treating people who use drugs.[59] A positive random drug test is enough justification to remove students from school or to terminate employment of otherwise productive employees and to force them to undergo rehabilitation.[60] Notably, random drug testing in schools violate students’ right to privacy and is inconsistent with international guidelines on the rights of children in relation to obligations arising from the human rights of particular groups.[61]
As a result, in 2015, countries from Asia and the Pacific committed to facilitate the transition away from compulsory centers toward an “evidence-informed system of voluntary community-based treatment and services that are aligned with international guidelines and principles of drug dependence treatment, drug use and human rights.”[62] Seven years after, however, the transition has yet to happen.
Moving forward: Transitioning to voluntary alternatives
Despite the problematics of drug rehabilitation in the Philippines being strongly determined by political and popular approaches to drug issues, recent developments suggest that a changing paradigm is not beyond the range of possibilities.
In the first place, the DDB has recognized the failures of closed settings in its approach to rehabilitation. The public admission that the mega rehab center was a mistake because it uproots people who use drugs from their families and the policy shift toward more community-based interventions are important concessions made as the country transitions to a more public health-based framework. More citations on community-based approaches appear in the DDB’s recent issuances that provide guidance to local government units on general interventions and programs.[63] Prior to Duterte’s time, rehabilitation programs were effectively available only in closed settings. Notably, the country has not closed down compulsory rehabilitation facilities and appears to be far from doing so. Nevertheless, at the close of Duterte’s term, we note a promising dent in the number of admissions in closed settings in favor of community-based programs.
This palpable shift in policy can be attributed largely to the work of civil society organizations, human rights groups, and academic institutions that are more sensitized to drug issues and more critical of the political discourses employed in the wake of Duterte’s war on drugs. Many of these groups still embrace a decidedly “drug-free” paradigm, but they can nonetheless serve as entry points for interrogating rehabilitation as it is practiced and understood in the Philippines today. Policy officials, too, have learned important lessons from the drug war, leading them to revise the national guidelines on rehabilitation.
Similarly, as one of the authors notes in another work, “there has been a proliferation of drug war-related researches, from the documentation of its ‘lived experiences’ to policy analyses.”[64] The academic interest in drug issues has included narratives of rehabilitation and case studies on community rehabilitation, all of which can contribute to a local evidence base for alternative interventions. Academic networks have been formed, and publications that problematize the drug war have allowed for dialogues nudging policy makers toward reform.
Second, although, as mentioned above, presidential politics have largely embraced the killings-versus-rehabilitation binary, lawmakers have in fact filed harm reduction bills and similar initiatives.[65] These legislative initiatives—though still unlikely to prosper at this stage—nonetheless represent a sea change from previous times and may signal more openness in the future. This is an important step to challenge the binary framework and to introduce a genuine option that promotes autonomy, human dignity, and health.
Nevertheless, legislative change is necessary. We can no longer avoid and delay the conversation on decriminalization of drug use, as it is apparent that the courts—supposedly the champions of human dignity—have become agents for compulsory rehabilitation. In the Philippines, people are ordered to undergo rehabilitation or face imprisonment. People arrested for drug-related offenses bargain for a lesser penalty, which includes rehabilitation. Jails are now formally considered centers for rehabilitation, putting into question the capacity of these institutions to provide the standards necessary for genuine health programs.[66]
Third, despite the defiant tone that government officials have struck in terms of Duterte’s possible trial before the International Criminal Court, international pressure has been effective in forcing government officials to reform policies that address drug-related concerns. For example, the United Nations Joint Programme for Human Rights in the Philippines has become an important platform for introducing human rights-based approaches to drug control. Among other things, it calls for the improvement of prison conditions and development of community-based programs. If it is to make further progress in the country, however, the joint program must implement the international consensus on ending compulsory rehabilitation and invest in a transition toward voluntary services, following the consensus from the Third Regional Consultation on Compulsory Centres for Drug Users in Asia and the Pacific, and further accommodating the recommendations from the United Nations Office on Drugs and Crime and UNAIDS on adopting voluntary community-based services as the framework for drug-related programs and interventions.[67]
One caveat about international pressure, though, is that it might perpetuate policies that can be framed by populist politicians as “colonial interventions,” especially given the backdrop of how human rights and concerns over the drug war were cast by local politicians as “Western” or “colonial” impositions.[68] This goes to show that beyond “decolonizing drug policy,” drug reform must also move toward decolonizing harm reduction.[69] It is important that attempts to reshape rehabilitation be based on the perspectives of people who use drugs. Thus, international support must not be merely a transplantation of practices from abroad but a genuine privileging of the voices of the communities whose lives involve drugs. Crucial to this project is empowering local actors (e.g., academics and advocates) who can then provide local scholarship and offer localized, culturally sensitive communications efforts that can be more difficult to delegitimize.[70]
Finally, the long-standing support for forced rehabilitation ultimately rests on how people who use drugs are perceived by the public and leaders, both political and religious. Thus, any attempt to reform must involve careful thinking as to how public attitudes can be changed. The narratives that inform policies negatively portray people who use drugs, and moral leaders (predominantly Catholic) have provided the justifications for a draconian approach to drugs, including the removal of personal autonomy in decisions affecting one’s life and health. Admittedly, this sociocultural foundation that supports compulsory rehabilitation is the hardest to break. However, cultural values such as the importance of family can be important themes in counter-narratives that can support family- and community-based approaches. Similarly, amplifying narratives from people who use drugs themselves can illuminate the lived realities of drug rehabilitation for the general public. More fundamentally, however, we need to deepen our understanding of the paradigms that inform the rigid binary to be able to transition to a framework that fully embraces human rights and public health.
Conclusion
In the Philippines, owing to a long history of penal populism, moral panic around drugs, and long-standing moralistic views of people who use them, “drug rehabilitation” is seen as a humane and acceptable alternative to the “drug problem,” and this has been reflected in (and reinforced by) contemporary political discourse. However, as we have shown in this paper, there is very little difference between jails and rehabilitation centers in terms of both philosophy and practice; in fact, jails are now centers for compulsory treatment. Those who seek to reform this untenable status quo need to capitalize on recent policy reforms, informed by a vibrant civil society and supported by the international community, to end the era of forced rehabilitation, with local actors and stakeholders empowered to take the lead.
As the Philippines undertakes a change of leadership, advocates in the country and elsewhere must recognize the need to go beyond addressing killings and insist on a discussion about what kind of rehabilitation should exist—and for whom—and about how to genuinely expand our responses to drug-related issues in a way that goes beyond criminal and medical frameworks. Institutions that have been sensitized to what is at stake with drug policy in the country can be potential allies in this move, but it must be accompanied by international attention beyond the killings—as well as a recognition that “decolonizing drug policy” also entails decolonizing the ways we have sought to reform it.[71] Lessons learned from the Philippines are likely relevant for neighboring countries and thus for drug policy and human rights advocacy around the world.
Gideon Lasco, MD, PhD, is a senior lecturer in the Department of Anthropology, University of the Philippines Diliman, and a research fellow at the Ateneo de Manila University’s Development Studies Program, Quezon City, Philippines.
Lee Edson Yarcia, MD, JD, is a senior lecturer in medical jurisprudence and constitutional law at the College of Law, University of the Philippines Diliman, Manila, Philippines, and a drug policy expert at the United Nations Joint Programme for the Protection and Promotion of Human Rights in the Philippines.
Please address correspondence to Gideon Lasco. Email: pdlasco@up.edu.ph.
Competing interests: None declared.
Copyright © 2022 Lasco and Yarcia. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction.
References
[1] L. Escresa and N. Garoupa, “Judicial politics in unstable democracies: The case of the Philippine Supreme Court, an empirical analysis 1986–2010,” Asian Journal of Law and Economics 3/1 (2012), p. 1; R. Juan-Bautista, Readings in Philippine legal history (Quezon City: University of the Philippines College of Law, 2017), pp. 143–281; N. Quimpo, “Review: Oligarchic patrimonialism, bossism, electoral clientelism, and contested democracy in the Philippines,” Comparative Politics 37/2 (2005), pp. 229–250.
[2] Office of the United Nations High Commissioner on Human Rights, Situation of Human Rights in the Philippines, UN Doc. A/HRC/44/22 (2020).
[3] A. Abando, Mega rehab gives hope to lost souls (December 2017). Available at https://www.pna.gov.ph/articles/1013310.
[4] Office of the Prosecutor or the International Criminal Court, Situation in the Republic of the Philippines, ICC-01/21 (2021).
[5] Republic Act No. 9165 (2002).
[6] United Nations Office on Drugs and Crime and Joint United Nations Programme on HIV/AIDS, Compulsory drug treatment and rehabilitation in East and Southeast Asia (January 2022). Available at: https://unaidsapnew.files.wordpress.com/2022/01/booklet-3-12th-jan-2022.pdf.
[7] R. Duterte, Inaugural address of President Rodrigo Roa Duterte (June 2016). Available at https://www.officialgazette.gov.ph/2016/06/30/inaugural-address-of-president-rodrigo-roa-duterte-june-30-2016/.
[8] A. Tejada, Duterte vows to end criminality in 3 months (February 2016). Available at https://www.philstar.com/headlines/2016/02/20/1555349/duterte-vows-end-criminality-3-months.
[9] Office of the United Nations High Commissioner for Human Rights (see note 2).
[10] Office of the Prosecutor of the International Criminal Court (see note 4).
[11] Ibid.
[12] Dangerous Drugs Board, Reported cases by type of admission and sex (facility based) CY 2016 (June 2017). Available at https://www.ddb.gov.ph/research-statistics/statistics/45-research-and-statistics/329-2016-statistics.
[13] Dangerous Drugs Board, Reported cases by type of admission and sex (facility based) CY 2017 (February 2019). Available at https://www.ddb.gov.ph/research-statistics/statistics/45-research-and-statistics/396-2017-statistics.
[14] Dangerous Drugs Board, 2018 statistics (October 2019). Available at https://www.ddb.gov.ph/research-statistics/statistics/45-research-and-statistics/434-2018-statistics; Estipona v. People of the Philippines, Philippine Supreme Court, G.R. No. 226679, August 15, 2017.
[15] Dangerous Drugs Board, Statistical analysis CY 2019 (September 2020). Available at https://www.ddb.gov.ph/research-statistics/statistics/45-research-and-statistics/499-2019-statistics.
[16] Ibid.; compare with Dangerous Drugs Board, Reported cases by type of admission and sex (facility based) CY 2015 (August 2016). Available at https://www.ddb.gov.ph/research-statistics/statistics/45-research-and-statistics/287-2015-statistics.
[17] Abando (see note 3).
[18] Ibid.
[19] Ibid.
[20] Ibid.
[21] Ibid.
[22] A. Carbonell, Mega drug rehab center in Ecija a mistake—DDB (November 2, 2017). Available at https://www.manilatimes.net/2017/11/02/todays-headline-photos/top-stories/mega-drug-rehab-center-ecija-mistake-ddb/360157.
[23] Ibid.
[24] Dangerous Drugs Board, Manual of operations for drug abuse treatment and rehabilitation centers. Available at https://www.ddb.gov.ph/images/MANUAL%20OF%20OPERATIONS%20-%20DRUG%20REHAB.pdf.
[25] Ibid.
[26] Ibid.
[27] Republic Act No. 9165 (2002).
[28] Dangerous Drugs Board, Regulation no. 3 series of 2007.
[29] Ibid.
[30] Dangerous Drugs Board, Regulation no. 2 series of 2019.
[31] L. Yarcia and J. Bernandas, “Articulating key obligations of states to persons deprived of liberty under a right to health framework: The Philippine case study,” International Journal of Human Rights in Healthcare (2021).
[32] Philippine National Police, Command memorandum circular no. 16-2016. Available at https://didm.pnp.gov.ph/images/Command%20Memorandum%20Circulars/CMC%202016-16%20PNP%20ANTI-ILLEGAL%20DRUGS%20CAMPAIGN%20PLAN%20%20PROJECT%20DOUBLE%20BARREL.pdf.
[33] Office of the United Nations High Commissioner for Human Rights (see note 2).
[34] Ibid.
[35] Ibid.
[36] Ibid.
[37] Dangerous Drugs Board, Regulation no. 3 series of 2016.
[38] Ibid.
[39] Bureau of Jail Management and Penology, Data on number of PDL with drug cases (as of May 31, 2021). Available at https://www.bjmp.gov.ph/images/data_and_stats/Data_on_Number_of_PDL_with_Drug_Cases.jpg.
[40] Dangerous Drugs Board, Regulation no. 8 series of 2021.
[41] G. Lasco, “Drugs and drug wars as populist tropes in Asia: Illustrative examples and implications for drug policy,” International Journal of Drug Policy 77 (2020); M. Tan, “The construction of drug abuse in the Philippines,” in G. Lasco (ed), Drugs and Philippine society (Quezon City: Ateneo de Manila University Press, 2021), pp. 47–70.
[42] J. Cornelio and G. Lasco, “Morality politics: Drug use and the Catholic Church in the Philippines,” Open Theology 6/1 (2020), pp. 327–341; C. R. Soriano, C. C. David, and J. M. Atun, “Crystallising the official narrative: News discourses about the killings from the Philippine government’s campaign against illegal drugs,” Journalism 22/9 (2021), pp. 2386–2403.
[43] Catholic Bishops’ Conference of the Philippines, Statement on drug abuse. Available at https://cbcponline.net/statement-on-drug-abuse/.
[44] Catholic Bishops’ Conference of the Philippines, Church’s rehab program, a concrete response. Available at https://cbcpnews.net/cbcpnews/churchs-rehab-program-a-concrete-response/.
[45] See, for example, Bridges of Hope, Easter and addiction recovery: Redemption and renewal. Available at http://bridgesofhope.com.ph/index.php/easter-and-addiction-recovery-redemption-and-renewal/.
[46] United Nations Office on Drugs and Crime and UNAIDS (see note 6).
[47] Ibid.
[48] Sangguniang Laiko ng Pilipinas, I will turn their mourning into joy. Available at https://www.cbcplaiko.org/documents/i-will-turn-their-mourning-into-joy/; see also Cornelio and Lasco (see note 42).
[49] Office of the Vice President, Vice President Leni Robredo’s report as co-chairperson of the Inter-Agency Committee on Anti-Illegal Drugs (ICAD). Available at https://ovp.gov.ph/post/vice-president-leni-robredos-report-co-chairperson-inter-agency-committee-anti-illegal-drugs-icad.html.
[50] R. Noriega, “De Guzman: Put cocaine-using presidential bet in rehab,” GMA News (November 19, 2021). Available at https://www.gmanetwork.com/news/topstories/nation/811583/de-guzman-put-cocaine-using-presidential-bet-in-rehab/story/.
[51] J. E. Mendoza, “Robredo to set a ‘drug war’ that focuses on rehab and prevention than ‘kill, kill, kill,’” Inquirer.net (October 30, 2021). Available at https://newsinfo.inquirer.net/1508254/robredo-to-set-a-drug-war-thats-more-on-rehab-and-prevention-than-kill-kill-kill.
[52] G. Lasco and N. Curato, “Medical populism,” Social Science and Medicine 221 (2019), pp. 1–8; J. Pratt, Penal Populism (London: Routledge, 2007).
[53] C. Hobson, “Challenging ‘evil’: Continuity and change in the drug prohibition regime,” International Politics 51 (2014), pp. 525–542.
[54] G. Lasco, “Introduction: Redefining drugs and the people who use them,” in G. Lasco (ed), Drugs and Philippine society (Quezon City: Ateneo de Manila University Press, 2021), pp. 1–26.
[55] Lasco (2020, see note 41); see, for example, United Nations, Joint Statement: compulsory drug detention and rehabilitation centers (2012). Available at https://files.unaids.org/en/media/unaids/contentassets/documents/document/2012/JC2310_Joint%20Statement6March12FINAL_en.pdf; United Nations, Joint statement on compulsory drug detention and rehabilitation centres in Asia and the Pacific in the context of COVID-19 (2020). Available at https://unaidsapnew.files.wordpress.com/2020/05/unjointstatement1june2020.pdf; United Nations Office on Drugs and Crime, Guidance for community-based treatment and care services for people affected by drug use and dependence in Southeast Asia. Available at www.unodc.org/documents/drug-treatment/UNODC_cbtx_guidance_EN.pdf; United Nations Office on Drugs and Crime and World Health Organization, Principles of drug dependence treatment (2018). Available at www.unodc.org/documents/drug-treatment/UNODC-WHO-Principles-of-Drug-Dependence-Treatment-March08.pdf.
[56] L. Yarcia, “It’s time to decriminalize drug use: Insights from the legal history of prohibition in the Philippines,” in G. Lasco (ed), Drugs and Philippine society (Quezon City: Ateneo de Manila University Press, 2021), pp. 298–319.
[57] Dangerous Drugs Board, Regulation no. 7, series of 2019.
[58] International Centre on Human Rights and Drug Policy, UNAIDS, World Health Organization, and United Nations Development Programme, International guidelines on human rights and drug policy (2019).
[59] Yarcia (see note 56).
[60] Ibid.
[61] International Centre on Human Rights and Drug Policy et al. (see note 58).
[62] United Nations Office on Drugs and Crime, United Nations Economic and Social Commission for Asia and the Pacific, and UNAIDS, Report of the third regional consultation on compulsory centres for drug users in Asia and the Pacific (2015). Available at https://unaidsapnew.files.wordpress.com/2015/12/report-of-the-third-regional-consultation-on-ccdus-in-asia-and-the-pacific-21-23-september-2015.pdf.
[63] See, for example, Dangerous Drugs Board, Regulation no. 4 series of 2020.
[64] Lasco (2021, see note 54).
[65] See, for example, House Bill No. 5567, Harm Reduction Act of 2016, filed by Representative Jose Christopher Y. Belmonte.
[66] Dangerous Drugs Board, Regulation no. 8 series of 2021.
[67] United Nations Office on Drugs and Crime and UNAIDS (see note 6).
[68] Lasco (2020, see note 41).
[69] C. Daniels, A. Aluso, N. Burke-Shyne, et al, “Decolonizing drug policy,” Harm Reduction Journal 18 (2021); G. Lasco, “Decolonizing harm reduction,” Harm Reduction Journal 19 (2022).
[70] Lasco (2020, see note 41).
[71] Ibid.