Developing Data Governance Agreements with Indigenous Communities in Canada: Toward Equitable Tuberculosis Programming, Research, and Reconciliation
Volume 24/1, June 2022, pp. 21-33 | PDF
Robin P. Love, Billie-Jo Hardy, Courtney Heffernan, Amber Heyd, Melissa Cardinal-Grant, Lori Sparling, Bonnie Healy, Janet Smylie, and Richard Long
Abstract
Indigenous rights to self-determination and data sovereignty support Indigenous-led data governance, which, when adequately resourced, can act as a catalyst for Indigenous-led strategic planning and decision-making in public health research and programming. Respecting Indigenous data sovereignty and governance requires time, resources, education, and planning. Here we share our experiences and lessons learned when developing and implementing data governance agreements with First Nations and Métis partnering communities in Canada in the context of tuberculosis prevention and care. We define the process undertaken to create a decision space, defined by data governance agreements, where researchers, program (government) stakeholders, and Indigenous community partners are equally and equitably informed to co-develop public health interventions. The decision space has implications for tackling all manner of public health concerns and can inform policy for nation-to-nation public health relationships and advance public health goals.
Introduction
Indigenous rights to self-determination and data sovereignty support Indigenous-led data governance, which, when adequately resourced, can act as a catalyst for Indigenous-led strategic planning and decision-making in public health research and programming. For Indigenous peoples, self-determination is central to reversing the impact of colonialism, an Indigenous-specific social inequity impeding their right to health. In the Canadian context, Indigenous refers to the first inhabitants of Canada—First Nations, Métis, and Inuit—each with their own distinct culture, history, language, and spiritual beliefs.1 The calls to action in the Truth and Reconciliation Commission of Canada’s (TRC) report summarize steps toward reconciliation with Indigenous peoples in Canada.2 The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP), recently ratified by the government of Canada, alongside research guidelines (e.g., Tri-Council Policy Statement 2) and First Nations ethical principles (e.g., ownership, control, access, and possession, or OCAP®), further outline rights and corresponding duties for the conduct of equitable and beneficial research and health programming with and for Indigenous peoples in Canada.3 Together, these authoritative statements have prompted many universities and public institutions in Canada to work toward meaningfully engaging with First Nations, Inuit, and Métis organizations and their respective communities. Key to meaningful engagement and equitable relationships with Indigenous peoples and communities in Canada is the recognition, by universities and public institutions, of Indigenous data sovereignty and the Indigenous right to self-determination in research and programming.
Indigenous sovereignty in Canada, albeit affirmed in the Indian Act, has been a long-standing area of neglect among government officials and other decision-makers.4 The Canadian government plays a paternalistic role in the health and welfare of Indigenous peoples, with jurisdictional disputes revealing reluctant responsibility (e.g., Jordan’s Principle).5 Acts to defend sovereignty, particularly land-based sovereignty, such as Oka in 1998 and more recently in Fairy Creek, highlight disconnects between those maintaining a colonial agenda and those who continue to experience ongoing colonization.6 Indigenous sovereignty broadly refers to the right to self-governance. Self-governance requires full and unfettered access to information relating to the state of one’s affairs. In Canada, health data are collected and disseminated according to relevant federal, provincial, and territorial legislation and policies. As with other areas of Indigenous sovereignty, these policies and laws do not always include Indigenous communities as equal partners in the process. As a result, Indigenous communities have limited input on how health data about their respective communities are collected and shared. The effect of these approaches is to reduce the ability of Indigenous communities to make informed and evidence-based decisions, thereby infringing on their rights. With respect to communicable diseases such as tuberculosis (TB), a community’s lack of access to health information is indirectly a lack of access to care.
Data sovereignty as a component of Indigenous sovereignty is not limited to data held by governments; it encompasses all Indigenous knowledges, whether health related or cultural. These may include history, stories, art, health knowledge, science, and practices. Indigenous knowledges and data are the subject of much interest within the research community and consequently form the basis of a number of studies. However, Indigenous knowledges and data, when taken out of context, can be abused, appropriated, and exploited in ways that fail to benefit Indigenous communities, most of whom continue to experience significant health inequities when compared to non-Indigenous people. As recently as 2004, the Havasupai Tribe filed a lawsuit against Arizona State University for allowing a researcher to use blood samples drawn from community members to describe genetic factors pertaining to diabetes. These samples were later used to study many other health-related issues without the donors’ consent.7
Indigenous data sovereignty and governance are essential rights protected by articles 18 and 23 of the UNDRIP.8 In most of Canada, however, public health research and programming are resourced and controlled primarily by non-Indigenous researchers and government agencies, even when Indigenous peoples are the subjects of those activities. As a result, Indigenous communities are often required to negotiate with researchers and government agencies to gain access to the resultant data or the resources necessary to collect or access their own data.9 Data governance agreements (DGAs), as legally binding documents, provide a mechanism to support community interests. Well-designed DGAs support equitable relationships by increasing both transparency and accountability toward Indigenous partners. In this way, a well-designed DGA can contribute to shifting the inherent imbalances of power that typically characterize the relationship between researchers and researched, or government agency and community. DGAs should therefore outline the purpose, roles, available resources, and time frames for interaction and accordingly demonstrate commitment by partners to the agreement. They may also include stipulations on the ownership, analysis, and interpretation of data, including the appropriate communication of findings. These stipulations should maximize beneficial community returns and lead to relevant and meaningful conclusions.
The Pathways TB Project
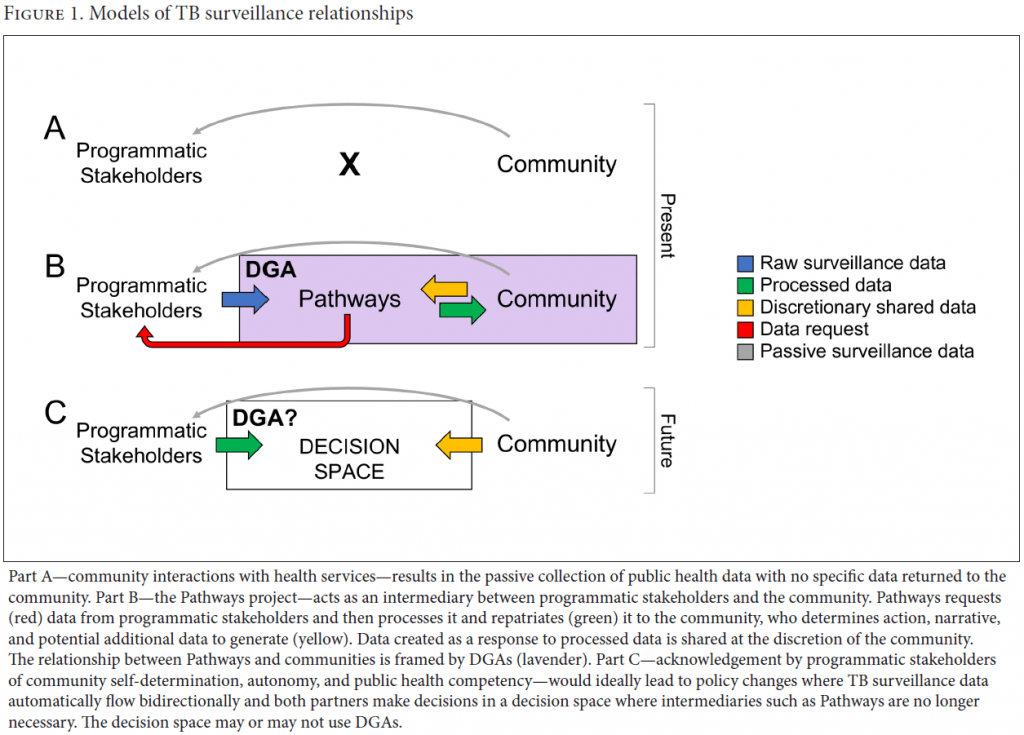
The Canadian Institutes of Health Research’s signature initiative, the Pathways to Health Equity for Aboriginal Peoples, funds projects aimed at addressing four priority areas: mental wellness; diabetes and obesity; oral health; and TB.10 The Pathways TB Project is one such funded project. This project partners with Indigenous community co-investigators who work together to develop interventions to close gaps in local TB surveillance and improve the provision of public health outreach.11 It also brings together practitioners and government agencies to meet and respond to community-identified priorities. In this now well-established network, where all input is considered to be equally significant, Indigenous community partners have direct input into the provision of TB prevention and care services adapted to their own realities. Progress toward more equitable and respectful public health surveillance relationships is modeled in Figure 1.12
Early on, community partners identified a lack of TB surveillance data describing their local TB epidemic. Government and programmatic stakeholders passively gather TB surveillance data, which is then stored in difficult-to-access forms for under-resourced communities (Figure 1A). At the behest of community partners, the Pathways team began repatriating TB surveillance data to communities (Figure 1B). Informed by the TB surveillance data, communities were able to contextualize local TB epidemics and define additional surveillance or action. As this environment of data flow and response developed, Pathways and community partners formalized the process through DGAs and thereby created a model for future government/programmatic stakeholder-community relations regarding public health data where an intermediary like Pathways would not be necessary (Figure 1C).
TB persists in many middle and far northern Indigenous communities across Canada.13 In general, the persistence of TB is multifactorial and includes geographic challenges, systemic neglect, ignorance, imposition of multiple forms of exclusion, and segregation.14 In Canada, the high burden of disease in Indigenous populations, relative to that in the non-Indigenous population, is long-standing (49-fold higher rates in Indigenous versus non-Indigenous Canadians in 2017), and to date, solutions identified or implemented by researchers and programmers have failed to advance the TB elimination agenda.15 To achieve TB elimination among Indigenous peoples in Canada—a target that is well within sight for non-Indigenous peoples—a new way forward, with solutions identified and implemented by and with First Nations, Inuit, and Métis communities, is required.16 TB is a notifiable disease of public health concern, meaning that public health TB surveillance data is collected at the provincial and national levels.17 However, these data, although public, are reported in aggregate and generally do not recognize the principles of Indigenous data sovereignty (e.g., ownership, control, access, and possession), limiting their utility to individual Indigenous communities.
The Pathways TB Project was designed to show that a community-centered, multijurisdictional collaboration is entirely possible and that this approach can help reduce regional TB incidence. It is expected that collaboration will lead to greater awareness, community-initiated and -led programs, and improved health outcomes for Indigenous peoples in the participating region.
The Indigenous communities and regional partners of the Pathways TB Project are in Treaty 8 territory across Alberta and Saskatchewan, two of the three prairie provinces of Canada. They include four communities: two First Nations, one small northern city, and a northern village inhabited predominantly by Métis people. The four communities are connected through culture, kinship, commerce, and employment. The continuity of TB patient care and any public health issue can be interrupted by extensive travel between communities and across multiple health jurisdictions. As colonial by-products, jurisdictional silos confound TB prevention and care programs wherever they overlap.
The Pathways TB Project comprises three sequential components spanning a teambuilding phase, an implementation science component, and a scale-up or ripple-out component.18 Initially, a set of shared values was developed in Component I to guide the partnership, focusing on trust building to foster strong relationships. A community co-investigator was recruited from each community. Component II identified specific interventions of the communities’ choosing and laid the groundwork for their implementation, which, in turn, revealed the need to develop a formal DGA. Finally, Component III, which is currently underway, sees expansion of the program to other regions among culturally distinct Indigenous groups, beyond Treaty 8 territory. This component will demonstrate the generalizability, feasibility, and portability of the Pathways concept.
Process of data governance agreement development
Phase 1: Introduction to data governance agreements
The Pathways TB Project developed a network of community co-investigators, academics, TB program nurses and physicians, medical officers, policymakers, and Indigenous research centers who shared the common goal of advancing TB elimination. Well Living House, an Indigenous-led action research center and Pathways affiliate, helped the network initiate research agreements with Indigenous community partners through presentations and the provision of templates and background materials. Discussion within the network began with a presentation on research, publication, and DGAs by Well Living House at an annual meeting of the Pathways TB Project in year one of Component II. These meetings include participation from all members and had been underway prior to the discussion of agreements. The purpose of the presentation was to highlight current wise practices in Indigenous health data governance and management, affirming the need to actively involve Indigenous governing agencies or organizations in the management and governance of their health data through collaborative research agreements. The nominated principal investigator from the University of Alberta proposed the following as a starting point for discussion:
The purpose of our eventual agreement will be to ensure that the project is respectful to the cultures, language, knowledge, values, and rights to self-determination for the peoples in [the four groups identified]. This agreement also provides a framework for the use of data collected during the Research Project. This agreement supports principles of Indigenous collective and self-determined data management and governance. These are not financial agreements. The agreement supports the information needs of the community partners, as well as acknowledging the desire of Dr. Richard Long and his research team to conduct this collaborative research. It defines the opportunity(ies) to develop research questions and responses alongside our community partners. Our community partners should anticipate this research project will assist in programming, service delivery, policy making, planning, and evaluation.
The above text was derived from conventional research agreements. It was concluded that a more broad definition of data was needed. The community co-investigators were requesting access to public health data—a task that Pathways could facilitate. Research data, if co-generated by the project and the community, would indeed be covered by the DGA; however, it was the flow of public health data that precipitated the DGA.
A number of different principles were proposed and discussed. These included maintaining mutual respect and accountability between the parties; recognizing the complementary and distinct expertise, responsibilities, mandates, and accountability structures of each party; ensuring the highest standards of research ethics, including the acknowledgement of community-partner-specific principles of self-determined data management; respecting the individual and collective privacy rights of community-partner personnel; recognizing the value and potential of research that is scientifically and culturally validated and programmatic data sharing that is mutually beneficial; data storage and stewardship; potential publications; disagreement resolution; who would be tasked with enforcing the agreement; and recognizing the value of supporting community-partner processes, including the analysis and dissemination of results and timing of any research activities.
Phase 2: Drafting the data governance agreements
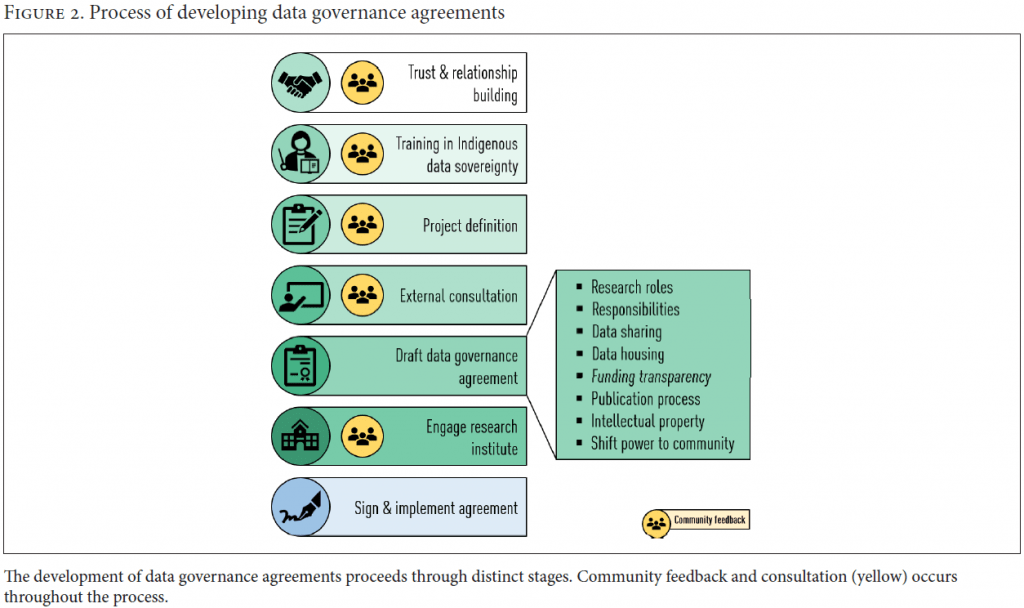
Several months later, the Pathways team reviewed the template agreements that had been provided by Well Living House and worked with the Indigenous community partners to prepare a draft DGA. This draft addressed roles, responsibilities, data-sharing protocols, funding transparency, the publication process, and intellectual property. Community partners raised the issues of storage and stewardship of data, information technology limitations, privacy, and human resource gaps within the community (e.g., students, volunteers, etc.) as significant concerns, and thus these considerations were included. Agreements were developed to explicitly address these community priorities, as well as community co-ownership of program surveillance data and co-authorship of research publications.
DGAs are legal agreements that identify the parties and outline how the data are collected and used, with the intention of shifting the balance of power back to community signatories. These agreements were central to achieving the goals of sustainability and scalability identified in Components I and II. Discussions with the home institution from which Pathways originated—in this case, the University of Alberta—regarding the nature of the agreements was also critical given the legal implications engendered by these agreements. The principles of UNDRIP and First Nations OCAP® were used to underpin the legal proceedings.
Phase 3: Definition of data
Community partners worked together to identify and define the data of interest at the local level. Co-investigators highlighted the need for routine access to relevant TB surveillance data that could be used to develop community-defined strategies to achieve elimination.
Public TB surveillance data are collected and held by provincial health authorities, but aggregation dilutes the relevance of these data to TB-affected communities. They are not research data per se but data that were requested as an “intervention” within the context of a research project. In response to this community-identified need, the Pathways team repatriated these surveillance data to the community and provided support by way of presentation, dissemination, and interpretation. Implicit in the entire exercise was the intention that routinely collected surveillance data (from high-incidence communities) could, in the future, be repatriated in such a manner, perhaps as policy, beyond the life of the Pathways TB Project, and with an agreement to respond to the data collaboratively.
These repatriated TB surveillance data further equip the community to ask their own questions and identify gaps in understanding and managing local epidemics. These questions could then develop, or not, into data-generating initiatives, with the Pathways team acting as facilitator. For example, some TB surveillance data not collected by the province but which community partners considered relevant include the experience and effects of trauma and grief; addictions and mental health; maternal and child health; available health services and programs and their perceived usefulness; and community-based strengths and resources. In the event that data are collected on any of these factors, they could, in turn, be shared with the Pathways network to the extent that members therein are well positioned to enhance and improve TB prevention and care services in response to this new knowledge. This final step—the sharing of community-collected data—is at the discretion of the community and defined as such in the DGA.
Phase 4: Site visits
Over the next several months, numerous site visits and teleconferences were undertaken with partner communities. Additional community data collection was identified in relation to kinship, cultural healing, and well-being to complement the TB surveillance data. These valuable considerations were realized following careful thought and rumination by community partners and would have been missed had the process been hastily undertaken.
It was proposed that discrete DGAs be established with each community to fit their unique needs. All four communities performed their own negotiation. It was established from the outset, at all-participant meetings, that all negotiations and drafts would be shared across the network to foster increased discussion and cross-learning. The research team had little experience initiating DGAs. Moreover, community research partners differed in negotiation experience with respect to DGAs. Openly discussing strengths and challenges pointed both directly to solutions and to the need to look outside the network for additional support. As an example of this, the First Nation partner community in Alberta requested support from the Alberta First Nations Information Governance Centre (AFNIGC), the regional satellite center of the National FNIGC, which then provided basic training and advice on the process.
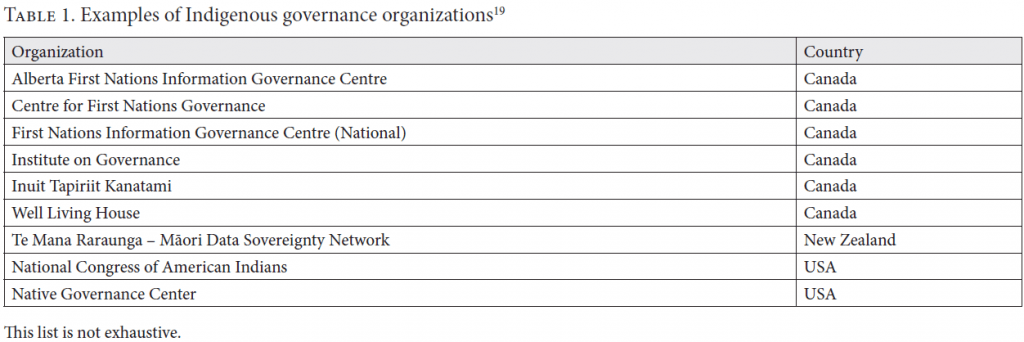
Indigenous governance organizations such as the AFNIGC offer support to communities and should be considered essential brokers in fair negotiations. First Nations and Métis are distinct and consist of many nations and regions, each of which may or may not have organizations that can be invited to perform this role. Indigenous governance organizations are found around the world in support of distinct communities (see Table 1 and Box 1).
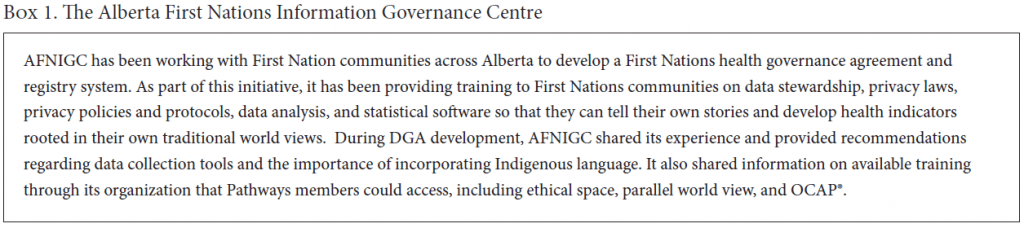
A teleconference was held with all community partners, the Pathways team, Well Living House, and the AFNIGC (see Box 1) to decide the role of each in the DGA development process.
Some of the research team and community research partners noted their unfamiliarity with OCAP® principles; as a result, it was agreed that investing in the training available through the AFNIGC would provide value to the ongoing negotiations. The AFNIGC thus provided a training session on ethical space and OCAP®. The fees for training were waived as an in-kind contribution by the AFNIGC to the researchers and Indigenous partners.
Following the training sessions, community co-investigators once again reflected on the type of research they would like to see conducted at the community level, as well as how any resultant data might be stewarded and stored. An adapted framework with key elements of the agreements was established with each community research partner and included the following: a definition of the parties; establishment of each party’s authority to share and receive the data; provisions regulating the use and restrictions of data disclosure; security and privacy requirements; policies and procedures and oversight committee; a determination of whether data are project or program specific; provisions for the publication of results; and provisions on how a party can terminate the agreement and how data will be destroyed or archived. The new agreements incorporated the AFNIGC framework and the principles of ownership, control, access, and possession relevant to each community. To the First Nation in Alberta, AFNIGC provided additional core support to the negotiations.
Phase 6: Data governance agreement negotiations
Nearly 18 months after initial the discussions of DGAs, negotiations began between the Pathways TB Team, the Board of Governors of the University of Alberta, and the AFNIGC. Concerns were raised by the university regarding publication rights given the equal authority provided to community co-investigators. While, initially, the terms put forth by each side were non-negotiable, the university eventually acquiesced to the DGAs co-developed by the Pathways team and community partners, and met its stated commitments to the TRC’s calls to action and related obligations to Indigenous partners. By so doing, a legal precedent was established by the team in which Indigenous partners were made equal participants in the full scope of the research project and co-authors on relevant outputs. The most significant takeaway from these negotiations was that in the face of opposition to this kind of relationship or agreement, there is a moral imperative to insist on the protection of the rights of Indigenous community partners, or else be complicit in the colonial agenda that has historically propped up institutions of exclusion—an antithetical proposition to reconciliation within the academe. This imperative has been affirmed and reaffirmed in UNDRIP, the TRC’s calls to action, and other rights-based documents.
One First Nations partner community was simultaneously negotiating three or four additional research agreements independent of Pathways. This community actively used what was learned in those negotiations when approaching the Pathways agreement. This active iteration increased the period necessary for negotiation but also both the confidence the community had with the final Pathways agreement and the quality of the document.
Finally, the two provincial communities (the northern city and the northern village) opted to pursue less formal DGAs. Each of these communities had multiple governing bodies and research interests, and they did not want to create the perception that one would have power or be prioritized over the others. Moreover, in both of these communities, the primary source of data for the surveillance component of our work is provincial governments—in other words, both communities reside within the jurisdictions of regional health authorities governed by provincial legislation and mandates for the provision of services. As a result, a formal DGA in these contexts would have been between the province and itself, with the university acting as shepherd through the bureaucracy. Letters of acknowledgement (LOAs) for the receipt and responsible use of data were agreed on by these parties instead.
Outcome
Discussions related to the development of DGAs began in May 2017, and negotiations were complete by 2019. Two DGAs were negotiated and signed with two First Nations, one in Alberta and one in Saskatchewan. LOAs for the receipt of data were signed by appropriate signatories (research partners and knowledge users) in the city and northern village (Métis).
Since signing the DGAs, the Pathways team has presented surveillance data to the communities on several occasions. The community has convened committees to respond to the data and pitch ideas for additional surveillance and action.
Discussion
In the creation of DGAs or LOAs with the four partnering communities, we set the stage for a decision space where stakeholders in health come together, equally informed, to devise interventions and action against TB (part C of Figure 1). This was possible because Pathways recognizes the sovereignty of Indigenous peoples and communities, respecting their right to self-determination in the development of partnerships. The decision space described here builds on the ethical space of engagement described by Willie Ermine.20 Indeed, Indigenous self-determination vis-à-vis public health will require the sharing and processing of surveillance data and respect for community decisions that result from their interpretation. The creation of decision-making spaces for other public health concerns may not require the explicit development of DGAs; however, the exercise undertaken with Pathways demonstrates the time and care required for all parties.
An ethical decision space framework can be applied to all public health concerns, as it reflects the spirit of nation-to-nation relationships inherent to questions of sovereignty and self-determination. A commitment to equitability and respect for others’ right to autonomy leads to better outcomes and greater efficiency. In the Canadian context, many well-intentioned public health programs aimed at tackling addiction, mental health, and communicable infectious diseases are created without the consideration of local priorities of Indigenous communities and, as a result, are not as effective or outright fail.21
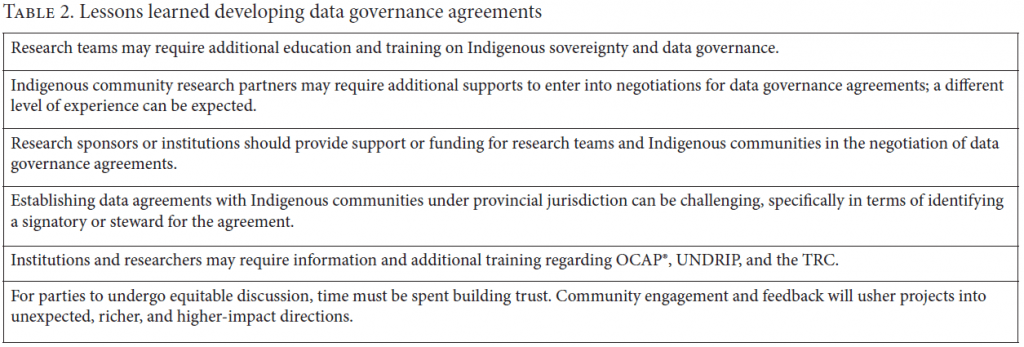
Several lessons were learned during the DGA process (Table 2). All members of the Pathways research team required training and education on Indigenous data sovereignty. Each community research partner came with a different level of experience, and some required additional support and resources to enter these negotiations. Additional funding support may be required to supply both research teams and partners with training.22 Fully informed negotiating parties can contribute to addressing power imbalances and lead to more equitable arrangements.
The work and agreements were between researchers representing a Canadian institution—the University of Alberta—and First Nations and Métis communities. Some of the process and developmental details reported herein may be specific to Canada, but colonized and post-colonized Indigenous peoples are found throughout the world. As a result, the act of DGAs is sound policy for respecting Indigenous rights to self-determination and data sovereignty worldwide.
The University of Alberta has only recently begun to implement the recommendations made by the TRC’s calls to action, hiring an Indigenous vice provost to develop and implement an Indigenous strategic initiative in 2019. As a result, establishing legally binding agreements with explicit intentions to share power and research (via co-authorship) with Indigenous communities was still relatively novel at the administration level. These novel asks posed a challenge with respect to the timeliness of negotiation and required some capacity-building to reach consensus on the requirements of UNDRIP, OCAP®, and the TRC. For instance, the contract office lacked a basic template and was mostly hands-off during the initial development of the agreements. These gaps in knowledge reflect similarities with past research that identified the need for practical instructions for financial administrators and researchers to better understand how to implement the Tri-Council Policy Statement 2 guidelines to improve the research interface with Indigenous communities.23 It is recommended that universities proactively address these gaps in knowledge through capacity-building and training of their staff and faculty and that researchers engage their institutions well in advance of agreement negotiations.
Establishing DGAs with non-First Nations Indigenous communities can be challenging, specifically in terms of identifying an agreed-upon, responsible, and interested signatory or steward for the agreement. In our project, non-First Nations communities were not able to identify a preferred signatory or steward and so, by consensus, opted for an LOA. An LOA does not provide the same legal supports as a DGA and, as a result, may not achieve the same goals (e.g., shifting power dynamics and reciprocity between researchers and community). An LOA is not an agreement between an academic research team and an Indigenous community; it simply provides unidirectional data accountability. However, given the underlying statement of values, co-generated by all signatories in the early stages of Component I, we do not believe this will negatively affect a mutually beneficial relationship. Furthermore, the shifting of power dynamics and encouragement of reciprocity between researchers and community should be prioritized when working in partnership with Indigenous communities, regardless of intention or presence of a DGA or LOA.
Indigenous peoples have been, at times, “researched to death.”24 A long history of disclosure abuse, privacy violations, misinterpretations, and misappropriation exists.25 Conversely, data collected by government bodies may be locked away, becoming inaccessible or uninterpretable. These fears also fuel worries about deductive disclosure since communities are small.26 Working together with communities to develop DGAs that describe expectations, timelines, and outcomes is an important step in addressing the aforementioned pitfalls.
Forming equitable partnerships and then negotiating formal DGAs relates to five important Indigenous data sovereignty considerations. First, the right questions are asked. Phenomena seen from outside communities may appear and feel very different to those with lived experience. The group knowledge and history of a problem will generate hypotheses and actions unavailable to an outsider.27 Additionally, Indigenous groups are best equipped to define their membership.28 Jurisdictional division and technical definitions of group membership are often the result of colonial rulings and, at times, fail to reflect real communities.
Second, privacy is respected. The community is the only party fit to interpret and disclose sensitive descriptive data about themselves. There are currently no laws in Canada recognizing community rights to self-descriptive data.29 Outside parties disclose data for singular goals; these goals may be well intentioned, but they are seldom permanent. The community must, then, “live” with disclosure decisions. The continuity of the community will vastly outrun the continuity of research teams. The community participating in collecting their own data are not impeded by deductive disclosure, though moratoria may be put in place to protect individuals.
Third, agreements ensure that data are converted to knowledge, ensuring their social value to Indigenous communities. Data exist that are unavailable to decision-makers in Indigenous communities because of barriers to access and interpretation. Data are often exported without a return of knowledge. Data analysis requires resources that are, at times, lacking in Indigenous communities.30 Further, data generation and analysis without community input should be deemed meaningless, potentially harmful, and likely to contribute to research hesistancy.31 Agreements should include stipulations on reporting actionable information.
Fourth, communities retain the publishing rights of data. Including Indigenous partners in writing and publishing efforts ensures open dialogue and prevents the reckless sensationalizing of negative aspects of study results. Community publishing rights ensure that the role of ongoing colonialization is squarely considered in the Indigenous experience.
Fifth, data are described as the sovereign property of the community. Harvesting and publishing data without community consent is theft.
Throughout the process of negotiating these DGAs, we have learned that it is critical to be flexible, to respond to context and the priorities and needs of community members, and to remember that their input guides the process (Figure 2). It requires conviction to create policy changes in institutions. The case we have outlined herein took time, but the process is key to fair dealings in research and reconciliation. Our own DGA is available upon request to the corresponding author as an example of the process described throughout this paper and as a potential template for other researchers and community teams.
Acknowledgments
We are grateful to all the members of the Pathways coalition, especially the community co-investigators, for their contributions to the success of this project. We also thank the Canadian Institutes of Health Research, Alberta Innovates, Saskatchewan Health Research Foundation, and Indigenous Services Canada Alberta and Saskatchewan Regions for their generous financial support.
Funding
Funding for this study was provided by the Canadian Institutes of Health Research, Saskatchewan Health Research Foundation, and Alberta Innovates.
Ethics statement
This work did not involve human subjects or data.
Robin P. Love, MSc, is a research study coordinator at the Tuberculosis Program Evaluation and Research Unit (TB PE & RU) in the Department of Medicine, Faculty of Medicine and Dentistry at the University of Alberta, Canada.
Billie-Jo Hardy, PhD, is a research scientist at Well Living House at St. Michael’s Hospital, Unity Health Toronto, Canada, and an assistant professor (status only) at the Dalla Lana School of Public Health at the University of Toronto, Canada.
Courtney Heffernan, PhD, is the manager of the TB PE & RU, University of Alberta, Canada.
Amber Heyd, RN, MSc, is a former research study coordinator at the TB PE & RU, University of Alberta, Canada.
Melissa Cardinal-Grant, BScN, MPH, is a former research study coordinator at the TB PE & RU, University of Alberta, Canada.
Lori Sparling, MNGD, is a director of health and social development for a First Nations community in Saskatchewan, Canada.
Bonnie Healy is a health director at the Blackfoot Confederacy Tribal Council, Calgary, Canada.
Janet Smylie, MD, FCFP, MPH, is the director of Well Living House Action Research Unit and a professor at the Dalla Lana School of Public Health at the University of Toronto, Canada.
Richard Long, MD, is the director of the TB PE & RU and a professor in the Department of Medicine, Faculty of Medicine and Dentistry at the University of Alberta, Canada.
Please address correspondence to Richard Long. Email: richard.long@ualberta.ca.
Competing interests: None declared.
Copyright © 2022 Love, Hardy, Heffernan, Heyd, Cardinal-Grant, Sparling, Healy, Smylie, and Long. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction.
1. See S. Abonyi, M. Mayan, J. Boffa, et al., “‘Finally when I started falling down’: Indigenous tuberculosis patient experiences of health and illness on the Canadian prairies,” International Journal of Indigenous Health 12/1 (2017), p. 3.
2. Truth and Reconciliation Commission of Canada, Truth and Reconciliation Commission of Canada: Calls to action (2015). Available at https://ehprnh2mwo3.exactdn.com/wp-content/uploads/2021/01/Calls_to_Action_English2.pdf; A. Gaudry and D. Lorenz, “Indigenization as inclusion, reconciliation, and decolonization: Navigating the different visions for indigenizing the Canadian Academy,” AlterNative International Journal of Indigenous Peoples 14/3 (2018), pp. 218–227.
3. Secretariat on Responsible Conduct of Research, Canada, Tri-council policy statement ethical conduct for research involving humans TCPS2 2018 (Ottawa: Canadian Institutes of Health Research et al., 2019), p. 231. Available at https://ethics.gc.ca/eng/documents/tcps2-2018-en-interactive-final.pdf; First Nations Information Governance Centre, OCAP®. (1998). Available at https://fnigc.ca/ocap.
4. The Indian Act, R.S.C. c. 1-5 (1985). Available at https://laws-lois.justice.gc.ca/eng/acts/i-5/.
5. Government of Canada, Jordan’s Principle (2021). Available at https://www.sac-isc.gc.ca/eng/1568396042341/1568396159824.
6. H. S. LaForme, “Indian sovereignty: What does it mean?,” Canadian Journal of Native Studies 11/2 (1991), pp. 253–266.
7. N. A. Garrison, “Genomic justice for Native Americans: Impact of the Havasupai Case on Genetic Research,” Science, Technology and Human Values 38/2 (2013), pp. 201–223.
8. United Nations Declaration on the Rights of Indigenous Peoples, G. A. Res. 61/295 (2007), arts. 18, 23.
9. I. Pool, “Colonialism’s and postcolonialism’s fellow traveller: The collection, use and misuse of data on Indigenous people,” in T. Kukutai and J. Taylor (eds), Indigenous data sovereignty: Toward an agenda (Acton: Australian National University Press, 2016); C. M. Snipp, “What does data sovereignty imply: What does it look like?” in T. Kukutai and J. Taylor (eds), Indigenous data sovereignty: Toward an agenda (Acton: Australian National University Press, 2016), pp. 39–55.
10. Canadian Institutes of Health Research, Pathways to health equity for Aboriginal peoples (2018). Available at https://cihr-irsc.gc.ca/e/43630.html.
11. R. Long, C. Heffernan, M. Cardinal-Grant, et al., “Two row wampum, human rights, and the elimination of tuberculosis from high-incidence Indigenous communities,” Health and Human Rights Journal 21/1 (2019), pp. 253–265.
12. Ibid.
13. M. LaFreniere, H. Hussain, N. He, and M. McGuire, “Tuberculosis in Canada: 2017,” Canada Communicable Disease Report 45/2–3 (2019), pp. 67–74.
14. P. E. Farmer, B. Nizeye, S. Stulac, and S. Keshavjee, “Structural violence and clinical medicine,” PLoS Medicine 3/20 (2006), p. e449; J. Galtung, “Violence, peace and peace research,” Journal of Peace Research 6/3 (1969), pp. 167–191; K. Lönnroth, E. Jaramillo, B. G. Williams, et al., “Drivers of tuberculosis epidemics: The role of risk factors and social determinants,” Social Science and Medicine 68/12 (2009), pp. 2240–2246; S. Patel, C. Paulsen, C. Heffernan, et al., “Tuberculosis transmission in the Indigenous peoples of the Canadian prairies,” PloS One 12/11 (2017), p. e0188189.
15. Long et al. (2019, see note 11); LaFreniere et al. (see note 13); R. Long, V. Hoeppner, P. Orr, et al., “Marked disparity in the epidemiology of tuberculosis among Aboriginal peoples on the Canadian prairies: The challenges and opportunities,” Canadian Respiratory Journal 20/4 (2013), pp. 223–230.
16. L. T. Smith, Decolonizing methodologies: Research and indigenous peoples, 2nd ed. (London: Zed Books, 2012); V. W. Simonds and S. Christopher, “Adapting Western research methods to Indigenous ways of knowing,” American Journal of Public Health 103/12 (2013), pp. 2185–2192; D. H. Martin, “Two-eyed seeing: A framework for understanding Indigenous and non-Indigenous approaches to Indigenous health research,” Canadian Journal of Nursing Research Archive 44/2 (2012), pp. 20–42.
17. Public Health Agency of Canada, Canadian tuberculosis standards, 7th ed. (2014). Available at https://www.canada.ca/en/public-health/services/infectious-diseases/canadian-tuberculosis-standards-7th-edition.html.
18. For a review of implementation science, see S. Theobald, N. Brandes, M. Gyapong, et al., “Implementation research: New imperatives and opportunities in global health,” Lancet 392/10160 (2018), pp. 2214–2228.
19. For more information on listed Indigenous governance groups, see Alberta First Nations Information Governance Centre. Available at http://www.afnigc.ca/main/index.php?id=home; Centre for First Nations Governance. Available at http://www.fngovernance.org/about/; First Nations Information Governance Centre. Available at https://fnigc.ca/splash/; Institute on Governance. Available at https://iog.ca/; Inuit Tapiriit Kanatami. Available at https://www.itk.ca/about-canadian-inuit/; Well Living House. Available at http://www.welllivinghouse.com/about-us/; Te Mana Raraunga – Maori Data Sovereignty Network. Available at https://www.temanararaunga.maori.nz/patai; National Congress of American Indians. Available at http://www.ncai.org/policy-issues/tribal-governance; Native Governance Center. Available at https://nativegov.org/.
20. W. Ermine, “The ethical space of engagement,” Indigenous Law Journal 6/1 (2007), pp. 193–203.
21. M. Lambert, J. Luke, B. Downey, et al., “Health literacy: Health professionals’ understandings and their perceptions of barriers that Indigenous patients encounter,” BMC Health Services Research 14 (2014), pp. 614–624; P. E. Farmer, N. Bruce, S. Stulac, and S. Keshavjee, “Structural violence and clinical medicine,” PLoS Medicine 3/10 (2006) p. e449; P. H. Mason, A. Roy, J. Spillane, and P. Singh, “Social, historical and cultural dimensions of tuberculosis,” Journal of Biosocial Science 48/2 (2016) pp. 206–232; E. Kilabuk, F. Momoli, R. Mallick, et al., “Social determinants of health among residential areas with high tuberculosis incidence in a remote Inuit community,” Journal of Epidemiology and Community Health 73/5 (2019) pp. 401–406; G. T. Kitching, M. Firestone, B. Schei, et al., “Unmet health needs and discrimination by healthcare providers among an Indigenous populations in Toronto, Canada,” Canadian Journal of Public Health 111/1 (2020) pp. 40–49.
22. K. F. King, P. Kolopack, M. W. Merritt, and J. V. Lavery, “Community engagement and the human infrastructure of global health research,” BMC Medical Ethics 13/15 (2014), p. 84; J. K. Riddell, A. Salamanca, D. J. Pepler, et al., “Laying the groundwork: A practical guide for ethical research with Indigenous communities,” International Indigenous Policy Journal 8/2 (2017).
23. Riddell et al. (see note 22); C. Moore, Implementing chapter 9 of the Tri-Council policy statement on the ethics of research involving Aboriginal peoples in Canada: How’s that going, MA thesis (Dalhousie University, 2015). Available at https://dalspace.library.dal.ca/bitstream/handle/10222/64699/Moore-Carla-MA-HP-November-2015.pdf?sequence=1&isAllowed=y.
24. A. Goodman, R. Morgan, R. Kuehlke, et al., “‘We’ve been researched to death’: Exploring the research experiences of urban Indigenous peoples in Vancouver, Canada,” International Indigenous Policy Journal 9/2 (2018).
25. Pool (see note 9); Snipp (see note 9); Smith (2012, see note 16).
26. Pool (see note 9); Snipp (see note 9).
27. D. E. Smith, “Governing data and data for governance: The everyday practice of Indigenous sovereignty,” in T. Kukutai and J. Taylor (eds), Indigenous data sovereignty: Toward an agenda (Acton: Australian National University Press, 2016); F. Morphy, “Indigenising demographic categories: A prolegomenon to Indigenous data sovereignty,” in T. Kukutai and J. Taylor (eds), Indigenous data sovereignty: Toward an agenda (Acton: Australian National University Press, 2016); Simonds and Christopher (see note 16); Martin (see note 16).
28. Smith (2016, see note 27).
29. First Nation Information Governance Centre, “Pathways to First Nations’ data and information sovereignty,” in T. Kukutai and J. Taylor (eds), Indigenous data sovereignty: Toward an agenda (Acton: Australian National University Press, 2016).
30. Snipp (see note 9), p. 45.
31. Smith (2012, see note 16); M. Saini, “A systematic review of Western and Aboriginal research designs: Assessing cross-validation to explore compatibility and convergence,” National Collaborating Centre for Aboriginal Health (2013). Available at https://www.ccnsa-nccah.ca/docs/context/RPT-ReviewResearchDesigns-Saini-EN.pdf; S. Hyett, S. Marjerrison, and C. Gabel, “Improving health research among Indigenous peoples in Canada,” Canadian Medical Association Journal 22/190(20) (2018), pp. e616–621; T. Mitchell, “Colonial trauma: Complex, continuous, collective, cumulative and compounding effects on the health of Indigenous peoples in Canada and beyond,” International Journal of Indigenous Health 14/2 (2019), pp. 74–94.