Building the Evidence for a Rights-Based, People-Centered, Gender-Transformative Tuberculosis Response: An Analysis of the Stop TB Partnership Community, Rights, and Gender Tuberculosis Assessment
Volume 23/2, December 2021, pp. 253-267 | PDF
Brian Citro, Viorel Soltan, James Malar, Thandi Katlholo, Caoimhe Smyth, Ani Herna Sari, Olya Klymenko, and Maxime Lunga
Abstract
The global tuberculosis (TB) response has undergone a transformation in recent years. Calls for a paradigm shift have inspired a new focus on the importance of communities, human rights, and gender in the response. This focus has led to new approaches and innovative tools to fight an age-old disease that still affects millions each year. Notable among these tools is the Stop TB Partnership’s community, rights, and gender (CRG) assessment. TB civil society and community groups, in partnership with national TB programs and others, have conducted the CRG assessment in 20 countries across four regions. Using the normative right to health framework, this article analyzes the evidence base generated by this assessment to understand the communities, legal environments, and gender dynamics at the heart of the epidemic. It describes an array of issues revealed by the assessment findings, including limited access to health services, disease-based discrimination, lack of privacy protections, and the impact of patriarchal norms on women affected by TB. Finally, this article considers how to strengthen the CRG assessment and how countries affected by TB and their donors and technical partners can leverage its findings in line with the Sustainable Development Goals and the political declaration from the first-ever United Nations High-Level Meeting on Tuberculosis.
Introduction
The response to the global tuberculosis (TB) epidemic has undergone a transformation in recent years. Calls for a paradigm shift have inspired a new focus on the importance of communities, human rights, and gender in the response.[1] This focus has led to new approaches and innovative tools to fight an age-old disease. Notable among these is the community, rights, and gender (CRG) assessment developed by the Stop TB Partnership (STP), the United Nations (UN) global partnership to end TB.[2] Others include the Global Fund’s Breaking Down Barriers initiative and STP’s TB Stigma Assessment and OneImpact Community-Led Monitoring Framework.[3]
The CRG assessment is a qualitative research tool that prioritizes the experiences and participation of communities affected by TB, including TB key and vulnerable populations. TB key and vulnerable populations are groups at higher risk for TB or that lack access to health services due to biological, behavioral, social, or structural factors. The CRG assessment also interrogates and highlights the significance of human rights, law, and gender in the TB response. TB civil society and community groups, in partnership with national TB programs and others, have conducted the CRG assessment in 20 countries across four regions.
This article’s overall aim is to examine the evidence generated by the CRG assessment to better understand the communities, legal environments, and gender dynamics at the heart of the TB epidemic. The article first describes the context and background of the global TB epidemic and response, highlights the recent emergence of the community, human rights, and gender focus, and explains the CRG assessment tool. The article then sets forth the methodology for the analysis of the CRG assessments findings. Next, it uses the normative right to health framework to analyze the assessment findings from 20 countries, identifying and describing an array of issues and common challenges. Finally, this article considers how to strengthen the CRG assessment and how countries affected by TB and their donors and technical partners can leverage its findings to end TB by 2030 in line with the political declaration from the first-ever UN High-Level Meeting on Tuberculosis and other global plans.
Context and background
TB is both preventable and curable. Nevertheless, it is one of the leading causes of death worldwide.[4] In 2020, about 10 million people fell ill with TB and more than 1.5 million died—more than 4,000 people a day (1.3 million deaths were among HIV-negative people; 214,000 deaths were among HIV-positive people).[5] More than four million people who got sick with TB—more than 40% of the 2020 disease incidence—were “missed,” meaning national TB programs did not identify them.[6] Though some of these “missing millions” may obtain testing and treatment in the private sector, many are undiagnosed and untreated. People with active TB who go undiagnosed and untreated contribute to the further spread of the disease.
The global TB burden is distributed unevenly around the world. Almost 70% of all people who fell ill with TB in 2020 were in the World Health Organization (WHO) regions of South-East Asia (43%) and Africa (25%).[7] Within countries, including wealthy nations with low incidence rates, often the most vulnerable, such as the homeless, migrants, and racial and ethnic minorities, are at higher risk for TB than others.[8]
The COVID-19 pandemic has had a devastating impact on the TB response. In May 2020, a consortium of researchers led by STP estimated that COVID-19 lockdowns and their subsequent recoveries could lead to an additional 1.4 million TB deaths between 2020 and 2025.[9] In March 2021, STP reported that TB detection and treatment enrollment numbers in nine countries that account for 60% of the global TB burden had fallen during the pandemic in 2020 to levels not seen since 2008—a loss of 12 years of progress.[10] In its 2021 Global Tuberculosis Report, WHO reported that although the global disease incidence remained about the same as in 2019, there was an alarming drop in 2020 in the number of people who were newly diagnosed with TB and registered in their health systems—from 7.1 million in 2019 to 5.8 million in 2020.[11] This means that, compared with 2019, more than a million people who got sick with TB last year likely went undiagnosed, an 18% decline back eight years to the level in 2012.[12] WHO also reported an increase in TB deaths from 2019 to 2020 for the first time in 15 years, declining back four years to the level of deaths in 2017.[13]
Global plans and targets to end TB
The Sustainable Development Goals (SDGs), WHO’s End TB Strategy and Moscow Declaration to End TB, and the STP Global Plan to End TB establish global milestones, targets, and commitments to end the TB epidemic.[14] The Global Plan to End TB, for example, calls for a “paradigm shift” and sets three people-centered targets: reach at least 90% of all people who need TB treatment and prevention, reach at least 90% of people in TB key and vulnerable populations, and achieve at least 90% of treatment success among people diagnosed with TB or those eligible for preventive therapy.[15]
In 2018, the UN General Assembly held the first-ever high-level meeting on TB. The meeting produced a political declaration by which heads of UN member states committed to a set of ambitious targets to end TB by 2030.[16] In accordance with the SDGs, the political declaration from the UN High-Level Meeting on Tuberculosis sets a global target to successfully treat 40 million people with TB by 2022.[17] The declaration also commits countries to prioritize communities, human rights, and gender in their national disease responses. Among other things, countries pledged to protect and promote the right to health and access to affordable medicines, support an end to TB stigma and discrimination, enhance psychosocial support for people affected by TB, facilitate the meaningful participation of TB key and vulnerable populations, strengthen gender equality, and ensure multisectoral collaboration and accountability in their disease responses.[18]
Methodology
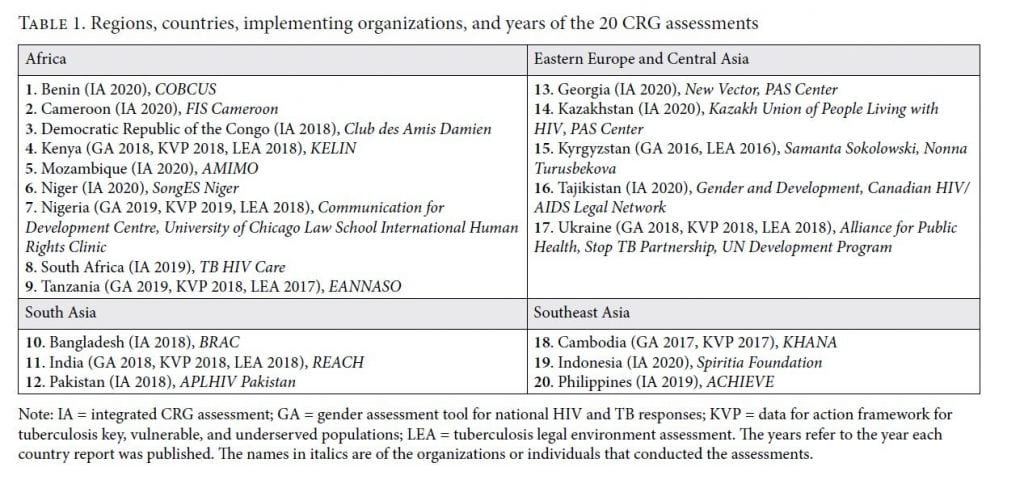
This article employs the normative right to health framework to analyze the findings of the 20 CRG assessments listed below in Table 1.
The CRG assessment
STP began developing the CRG assessment in 2015 through a series of global workshops involving people affected by TB, technical experts, and representatives of civil society groups and national TB programs. The CRG assessment is one component in a suite of initiatives at STP promoting community, human rights, and gender in the TB response. These include the OneImpact Community-Led Monitoring Framework, the OneImpact mobile application that collects real-time data on human rights violations and barriers to TB services, and the Challenge Facility for Civil Society, a small grants mechanism that supports TB civil society and community groups.[19]
The CRG assessment is a multistakeholder participatory process comprising four primary stages: (1) inception, adaptation of the assessment protocol, and secondary data collection; (2) training and primary data collection; (3) data analysis, validation, and report writing; and (4) dissemination and action planning.[20] Civil society and community groups lead the process with support from STP and technical experts. In each country, the CRG assessment is sanctioned and supported by the national TB program, and researchers obtain ethical clearances when necessary, according to national standards. The geographic scope of the assessment is typically national, with a further focus on important subnational jurisdictions, such as large cities or states or jurisdictions with high rates of TB.
Secondary data collection in the CRG assessment involves a desk review of public health and social science literature and legal and policy research. Primary data collection comprises qualitative research methods, including interviews, focus group discussions, and surveys.
The CRG assessment integrates three previously separate tools: the Data for Action Framework for Tuberculosis Key, Vulnerable and Underserved Populations; the Gender Assessment Tool for National HIV and TB Responses; and the Tuberculosis Legal Environment Assessment. Of the 20 countries considered in this article, 14 conducted the integrated CRG assessment and six employed the separate tools. Table 1 lists the countries, the tools that each country implemented, and the name of the implementing organizations. The United States Agency for International Development and the Global Fund provided financial support for the 20 assessments.
Right to health framework
The UN High Commissioner for Human Rights has emphasized the role of the right to health framework in “aligning law and policy with human rights, operationalizing the pledge to leave no one behind, [and promoting] accountability and participation” to achieve the health-related SDGs.[21] The content of the right to health framework derives from article 12 of the International Covenant on Economic, Social and Cultural Rights and General Comment 14 of the Committee on Economic, Social and Cultural Rights, the body that monitors states’ implementation of the covenant.[22] The mandate of the UN Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health also produces reports and other materials that contribute to the normative development of the right to health framework.[23]
Scholars, international institutions, and civil society and community groups have also contributed to the conceptual development of a human rights-based approach to TB, applying and extending the right to health framework established in international law. In 2000, STP, then hosted by WHO, identified “establish[ing] TB as a human rights issue” as the number one challenge for the following year and released a normative guidance on a rights-based approach to the disease.[24] In the years that followed, scholars and physicians further examined and debated human rights’ role in the TB response.[25] In 2016, this journal published a special section on TB and the right to health in which scholars considered access to new drugs for multidrug-resistant TB, the imprisonment of people with TB, and TB in vulnerable populations, among other issues.[26] In 2019, TBpeople, a global group of people affected by TB, released the Declaration of the Rights of People Affected by TB with support from STP.[27] In 2020, the Global Coalition of TB Activists, in partnership with the Northwestern Pritzker School of Law and STP, published a technical brief for policy makers and program implementers entitled Activating a Human Rights-Based Tuberculosis Response.[28]
This article relies on seven dimensions of the right to health framework: (1) availability, accessibility, acceptability, and quality (AAAQ); (2) nondiscrimination and equal treatment; (3) health-related freedoms; (4) gender perspective; (5) vulnerable and marginalized groups; (6) participation; and (7) remedies and accountability.
The rights enshrined in the International Covenant on Economic, Social and Cultural Rights, including the right to health, are generally subject to progressive realization due to states’ resource constraints.[29] This means that states are not legally bound to immediately realize the right to health in full. Instead, they must “take steps … to the maximum of [their] available resources” to progressively realize the right to health “by all appropriate means, including … the adoption of legislative measures.”[30] Notwithstanding the obligation of progressive realization, the right to health imposes certain obligations on states that are of immediate effect. These include the obligations to ensure that the right is enjoyed equally by all without discrimination of any kind and to take “deliberate, concrete and targeted” steps toward fully realizing the right.[31]
The AAAQ dimension of the right to health framework encompasses the right to physical and mental health facilities, goods, and services that are available, accessible, acceptable, and of good quality. Availability requires that these facilities, goods, and services be available in “sufficient quantity” in the country.[32] Accessibility includes nondiscrimination and physical, economic, and information accessibility.[33] Acceptability requires that health facilities, goods, and services be culturally appropriate, sensitive to gender and life-cycle requirements, and respectful of medical ethics, including confidentiality.[34] Quality requires that they be “scientifically and medically appropriate” and administered by skilled health workers.[35]
The nondiscrimination and equal treatment dimension comprises the prohibition against discrimination in health care and the underlying determinants of health, and a positive dimension requiring states “to provide those who do not have sufficient means with … health insurance and health-care facilities.”[36]
Health-related freedoms include the rights to privacy, to confidentiality, and to be free from nonconsensual medical treatment (i.e., the right to informed consent), as well as the freedoms of association, assembly, and movement.[37]
The gender perspective dimension of the right to health framework encompasses states’ obligation to “integrate a gender perspective in their health-related policies, planning, programmes and research,” including the disaggregation of health data according to sex.[38] This article also includes the health concerns of transgender persons within the ambit of the gender perspective.[39]
The vulnerable or marginalized groups dimension comprises states’ obligation to “give particular attention to all vulnerable or marginalized groups” in the process and content of their public health strategies and action plans and to ensure that health workers are “trained to recognize and respond to the specific needs of vulnerable or marginalized groups.”[40]
The participation dimension represents the right of affected communities to participate “in all health-related decision-making at the community [and] national … levels.”[41]
The remedies and accountability dimension of the right to health framework embodies the importance of accountability and effective remedies for health-related human rights violations, enabled by courts and nonjudicial mechanisms at the national and international levels.[42]
Analysis methodology
This article analyzes the CRG assessment country reports from the 20 countries listed in Table 1.[43] The country reports contain the CRG assessment research findings and recommendations. The civil society organizations, community groups, and technical experts that conduct the assessment write the country reports. National TB programs and other local stakeholders provide input and review and validate the findings and recommendations in each report before its publication. The authors of this article were involved in various stages of developing the CRG assessment, conducting the assessments, and drafting some of the country reports.
As detailed in Table 1, the country reports were published between 2018 to 2021 (except Kyrgyzstan, which was published in 2016). We note that some of the relevant circumstances in the countries involved may have changed since their publication. We also note that the organizations and individuals who conducted the CRG assessment took varying approaches in each country, focusing on a range of issues and concerns. The researchers’ capacities were also varied and developed over time, as later assessments benefitted from the knowledge and experience of earlier efforts.
To conduct our analysis of the CRG assessment findings, we first read each country report in full. We then focused on the sections containing the research findings to identify specific issues associated with the seven dimensions of the right to health framework. We then used various keyword searches for each dimension to find relevant information throughout the country reports.
We documented our findings with pinpoint citations to the country reports in 20 tables with seven columns for the right to health framework dimensions. We shared these tables with the implementing organizations that wrote the country reports for their review and validation. All 20 implementing organizations provided input, and we revised the tables as necessary. We then analyzed the tables one dimension at a time to identify common issues in the CRG assessment findings across the countries. Finally, we listed the common issues under the corresponding dimensions of the right to health framework and tallied the number of countries for which each issue appears in the assessment findings. The tables and lists of common issues are available upon request from the authors.
Limitations
This article’s analysis and the CRG assessment tool are both subject to limitations. Our analysis of the country reports produced by the CRG assessment was subject to two limitations. First, a degree of terminological inconsistency in the country reports weakened the effectiveness of keyword searches in identifying issues associated with the dimensions of the right to health framework. Second, four country reports are written in languages other than English: Benin (French), Cameroon (French), Niger (French), and Tajikistan (Russian). We employed a three-step process to address this limitation. First, we used Google Translate to translate the entire document, after which we performed our analysis in the English translation. Second, we conducted keyword searches in the original language and then used Google Translate to translate specific passages in which the keywords appeared. Third, we engaged the reports’ authors to discuss or request translations of specific passages in which keywords were located or that were of interest based on our analysis of the English translation.
The CRG assessment tool is subject to four main limitations. First, although the assessment generally employed a uniform set of qualitative research methodologies, as described above, there was some variance in the methodologies used among countries. Some assessments relied more heavily on interviews and focus groups than others, some conducted informal surveys of stakeholders, and others focused more heavily on desk research and analysis. Second, there was also meaningful variance in the nature of the disciplines and levels of expertise, training, and education among the individuals who conducted the assessments and drafted the country reports. For example, some researchers and authors were lawyers, while others were trained in the social sciences without legal education. Third, the 20 CRG assessments as a whole focused more on certain issues, conceptual frames, and dimensions of the right to health framework than others. Among these less considered issues are directly observed therapy (DOT) for TB, social protection and psychosocial support for people affected by TB, the participation of people affected by TB in the disease response, the availability and accessibility of remedies and accountability in the response, and the gender-transformative normative frame. Finally, while multisectoral engagement was a feature of the process in all 20 countries, there were nonetheless varying levels of engagement by certain stakeholders, such as national TB programs, TB doctors, and communities affected by TB.
CRG assessment analysis
This section analyzes the CRG assessment findings from the 20 countries in line with the seven dimensions of the right to health framework.
Availability, accessibility, acceptability, and quality
The CRG assessment revealed a variety of AAAQ challenges and concerns. The stigmatizing and discriminatory treatment of people affected by TB by health workers, an acceptability issue observed in 16 countries, is the most frequently identified issue. A lack of privacy and confidentiality in TB clinics and health services, another acceptability issue, is the second most common concern, found in 15 countries. Prohibitively long distances to TB clinics, a physical accessibility challenge, appears in the assessment findings in 12 countries. In 11 countries, the assessment discovered acceptability problems with the standard TB treatment, particularly the length of treatment, treatment side effects, and the nature of DOT, all of which are also quality concerns. A low awareness and lack of access to information about TB disease and TB health services are the leading information accessibility issues, highlighted in 11 and 10 countries, respectively. The CRG assessment further revealed the limited availability of trained TB health workers in TB centers, primary health care and other clinics, and prisons in 10 countries.
Additional availability issues include a lack or limited availability of TB treatment support services, particularly counseling and other mental health care, found in nine countries. In seven countries, the assessment highlighted the limited availability of rapid molecular diagnostics for TB that are faster and more accurate than traditional sputum smear microscopy and detect resistance to first-line TB drugs. The assessment findings in seven countries uncover first-line TB drug stock-outs. In four countries, the assessment identified a lack of integration of TB care with HIV and diabetes care and opioid-substitution therapy as a challenge at the primary health care level.
The key economic accessibility barriers observed in eight countries are out-of-pocket payments for TB tests and incidental expenses associated with TB treatment, most notably transportation costs to clinics for mandated facility-based DOT. The two principal discrimination accessibility challenges the CRG assessment identified are discriminatory treatment of TB key and vulnerable populations in health care in seven countries and discriminatory administrative barriers to health services in five countries in Eastern Europe and Central Asia. The latter includes residency and identification requirements to access TB health services, impacting mobile populations, internally displaced persons, and people with a history of incarceration. Finally, assessment findings in five countries highlight the lack of access to nutritional support during TB treatment as a major concern.
Ten countries identified additional acceptability challenges related to operational issues, including limited hours, long wait times, and overcrowding at TB clinics. These operational issues are also accessibility and quality concerns.
The primary quality issue identified in the CRG assessment findings is the limited availability of trained TB health workers in 10 countries (noted above as an availability concern). The findings in seven and six countries, respectively, also highlight the misdiagnosis or delayed diagnosis and inappropriate treatment of people with TB as major quality concerns.
Nondiscrimination and equal treatment
Discrimination and stigmatizing treatment of people affected by TB are pervasive in the CRG assessment findings. In 18 of 20 countries, the assessment revealed that people affected by TB experience discrimination in health care, including when they seek TB care but also in primary health care settings. The findings in 15 countries show that people affected by TB experience employment discrimination at the hands of both employers and coworkers. In 11 countries, the findings exhibit discriminatory and stigmatizing treatment of people affected by TB in families and communities. In the family context, the assessment findings indicate that women affected by TB are sometimes divorced or abandoned because of their experience with the disease. The findings in six countries draw attention to how children and young people affected by TB experience discrimination in education, in both schools and higher education.
Remarkably, despite the evidence of widespread discrimination against people affected by TB, the CRG assessment reveals that only one country explicitly prohibits TB-related discrimination in law. The other 19 countries lack legal prohibitions targeting discrimination against people affected by TB. The findings further highlight that the law and policies governing the TB response in two countries contain stigmatizing and discriminatory terminology. However, the assessment findings identify laws or executive decrees in some countries that address some aspects of discrimination against people with TB, including in employment. In one country, the assessment found that people affected by TB have used the courts to combat employment discrimination with some success using the constitution and other employment-related laws.
Health-related freedoms
The lack of protection for the privacy and confidentiality of people affected by TB in law, policy, and practice is the central challenge to health-related freedoms identified in the CRG assessment findings. Eighteen countries highlighted various kinds of privacy concerns. These include a lack of privacy and breaches of confidentiality in health care that deter the use of TB testing and treatment services and challenge treatment adherence. The assessment revealed that most countries do not have laws or policies that specifically recognize and protect the right to privacy of people affected by TB; however, some countries have laws protecting confidentiality in health care more generally. The findings in several countries highlight privacy concerns related to TB public health activities, including contact tracing and disease notification procedures. The assessment also discovered that TB clinics’ infrastructure and operational procedures impinge on privacy with exterior and interior signs and waiting room practices.
The CRG assessment findings in 13 countries also highlight concerns about the involuntary isolation and hospitalization of people with TB. The findings reveal that most of these countries do not have laws or policies that set forth the circumstances, procedures, or protections for the isolation of people with TB. By contrast, some have laws broadly authorizing the quarantine or compulsory hospitalization of people with TB and other infectious diseases, out of line with the WHO Ethics Guidance for the Implementation of the End TB Strategy.[44] In two countries in East Africa, the assessments discovered that the arbitrary arrest, detention, or imprisonment of people with TB or multidrug-resistant TB for stopping treatment or for posing a threat to public health was common.
The assessments in six countries revealed that law or policy permits the forced testing or treatment of people affected by TB. In four countries, the assessments highlighted the lack of protection of the right to informed consent for TB treatment and testing or during the collection of personal health data for public health purposes.
The CRG assessment in nine countries discovered that criminal laws erect barriers to health services for people affected by TB, including for TB key and vulnerable populations. These findings reveal that laws criminalizing personal drug use, commercial sex work, and same-sex sexual conduct discourage health-seeking behavior among people affected by TB. In two countries, the findings further highlight that national and subnational laws criminalize the transmission of TB.
Gender perspective
The CRG assessment findings shed new light on the role of gender in the TB epidemic and response. The primary issue emerging from 13 countries is the impact of patriarchal social and cultural norms, including around domestic gender roles and household finances. These findings indicate that patriarchal norms limit women’s health-related decision-making autonomy, impede their access to TB health services, and increase their vulnerability to TB infection and disease. The findings in 12 countries further reveal that women affected by TB experience more frequent or more intense stigma and discrimination than men in their families and communities, sometimes leading to abuse, gender-based violence, divorce, or abandonment. Three countries also found that women lack access to information and are less knowledgeable than men about TB disease and TB health services.
In 10 countries, the CRG assessment findings show that men affected by TB also face unique challenges. Men experience heightened risks of exposure to TB infection, reduced access to TB health services, and higher mortality rates from TB due to a host of factors, including employment insecurity, occupational exposure, labor migration, notions of masculinity, and social and behavioral factors such as smoking, excessive alcohol consumption, and problematic drug use.
In seven countries, the CRG assessment found that transgender persons and sex workers affected by TB and other members of TB key and vulnerable populations also face unique challenges using the health system because of their gender and other gender-related circumstances.
The CRG assessment discovered substantial gender-related programmatic, legal, and policy gaps in the national TB responses in 12 countries. These include the lack of a legal prohibition of gender-based discrimination in health care and the failure to consider the role of gender in TB programs, policies, guidelines, and monitoring and evaluation frameworks. The findings in eight countries further highlight the limited availability or lack of gender-sensitive TB health services, including for transgender persons, due to the lack of gender-sensitivity training for TB health workers, among other things. Eight countries also identified the lack of epidemiological and other data for TB disaggregated by gender, including for transgender persons, as a critical programmatic concern.
Vulnerable and marginalized groups
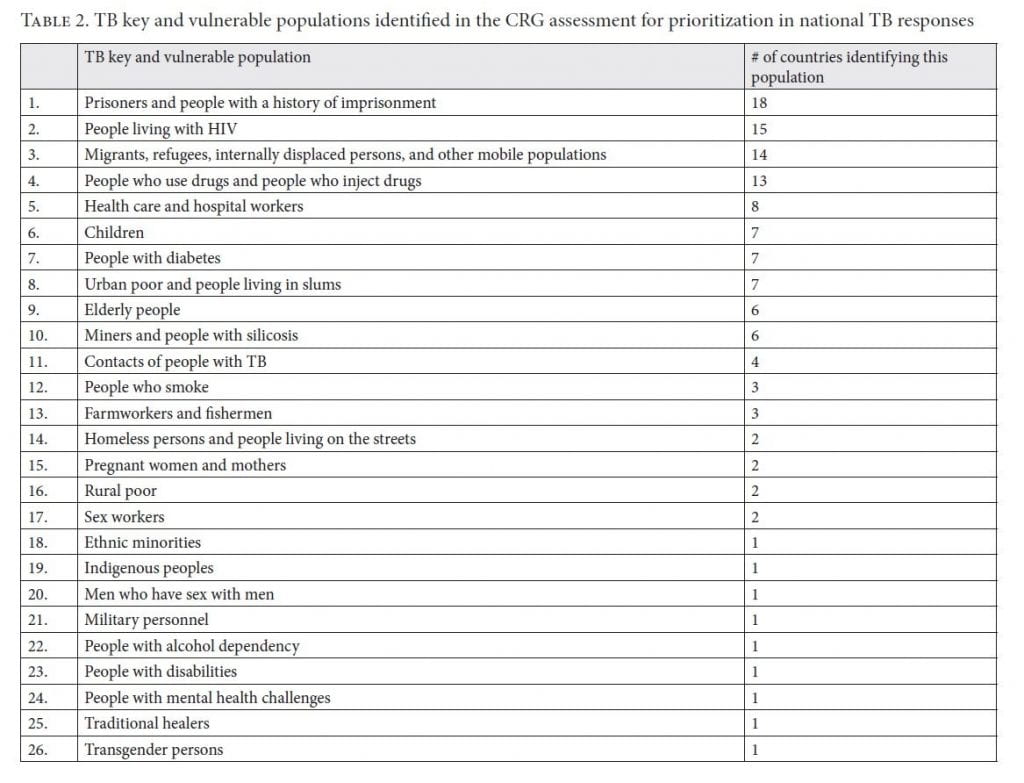
Identifying groups who are especially vulnerable to TB infection or disease or who experience barriers to accessing TB health services is a unique component of the CRG assessment. The assessment in each country identifies these groups through a combination of research and consensus among national stakeholders. In all 20 countries, the CRG assessment identified new TB key and vulnerable populations for prioritization that were not previously recognized by the national TB programs. Table 2 presents a tally of the 26 unique TB key and vulnerable populations identified during the CRG assessment in the 20 countries in this analysis.
The assessment findings in 16 countries also highlight various programmatic, legal, and policy gaps and barriers that negatively impact TB key and vulnerable populations. These include an absence of policies, programs, and dedicated resources in national TB programs recognizing and prioritizing these populations in national disease responses. Relatedly, the findings in seven countries reveal that national TB programs do not collect or effectively disaggregate data for TB key and vulnerable populations to understand their size, locations, and unique vulnerabilities. In 10 countries, the findings reveal that criminal or administrative laws and policies and the fear of law enforcement deter the use of TB health services among these populations, such as people who use drugs, sex workers, undocumented migrants, and people with a history of imprisonment. The assessment findings in six countries further highlight that a lack of health services integration for people affected by TB living with HIV, who use drugs, or who have diabetes deters their use of TB health services.
Participation
The CRG assessment findings expose a dearth of mobilization and meaningful engagement of people affected by TB and TB key and vulnerable populations in the national TB responses in most of the 20 countries in this analysis. The fact that reports from four countries do not discuss participation at all underscores this situation. The reports in the other 16 countries do not address participation to the same extent or in as much detail as the other issues examined in this section.
Nonetheless, the findings in 10 of the 16 countries that consider participation highlight the low number of civil society and community groups working on TB, the limited influence of such groups, and the limited financial and other support available to these groups to facilitate their meaningful participation in the TB response. The findings in eight countries further reveal that national TB programs fail to meaningfully engage people affected by TB in designing, implementing, monitoring, and evaluating TB policies and programs. The assessments in two countries discovered that gaps or barriers in law and policy hinder the meaningful participation of communities affected by TB. These gaps include the failure of legislation to recognize the right of people affected by TB to participate in health decision-making processes.
Remedies and accountability
The CRG assessment findings reveal that people affected by TB have limited access to justice and accountability mechanisms in the TB response. The fact that reports from three countries do not address concerns related to remedies and accountability highlights this problem. In 10 of the 17 countries that consider the issue, the assessments found that law and policy do not establish judicially enforceable legal rights or mechanisms for people affected by TB to seek remedies for rights violations and other legal matters. Reports from these countries noted a range of issues for which remedies and accountability were out of reach. These include discrimination in employment and health care, violations of the rights to privacy and confidentiality, denial of health services, and compensation for occupational exposure to TB, including for health workers.
The assessment in nine countries discovered that people affected by TB lack access to justice due to the absence or limited availability of legal aid services. The findings in eight countries highlight that the limited use of courts by people affected by TB is due to low levels of legal literacy and knowledge about legal rights. Two countries specifically mentioned the need for alternatives to litigation, such as alternative dispute resolution and mediation, so that people affected by TB may more easily, quickly, and affordably obtain remedies and promote accountability for rights violations.
The CRG assessment findings in two countries emphasize the lack of accountability for preventable TB deaths, inappropriate medical treatment of people with TB, and other issues of serious neglect of people affected by TB, including in prisons. The findings in three countries draw attention to criminal laws that act as inappropriate and ineffective deterrents or interfere with access to remedies for people affected by TB. The reports from two countries assert that the law should not criminalize the failure of doctors, chemists, or other health workers to notify TB cases. Instead, the reports recommend that national TB programs use incentives to promote disease notification among health workers, particularly in the private sector. The assessment findings in another country reveal that laws criminalizing drug use discourage people who use drugs from seeking legal services to obtain remedies for TB-related rights violations due to fear of law enforcement.
Discussion and way forward
The political declaration from the first-ever UN High-Level Meeting on Tuberculosis contains pioneering commitments by UN member states to prioritize communities, human rights, and gender in the TB response.[45] Framed by a pledge to “protect[] and fulfill[] the human rights and dignity of all people,” these commitments strengthen and expand upon preexisting human rights commitments in the WHO End TB Strategy, the WHO Moscow Declaration, and the STP Global Plan to End TB.[46] The CRG assessment findings constitute the most robust evidence available by which to reflect on these commitments, revisit strategic priorities, and scale up investments in communities, human rights, and gender.
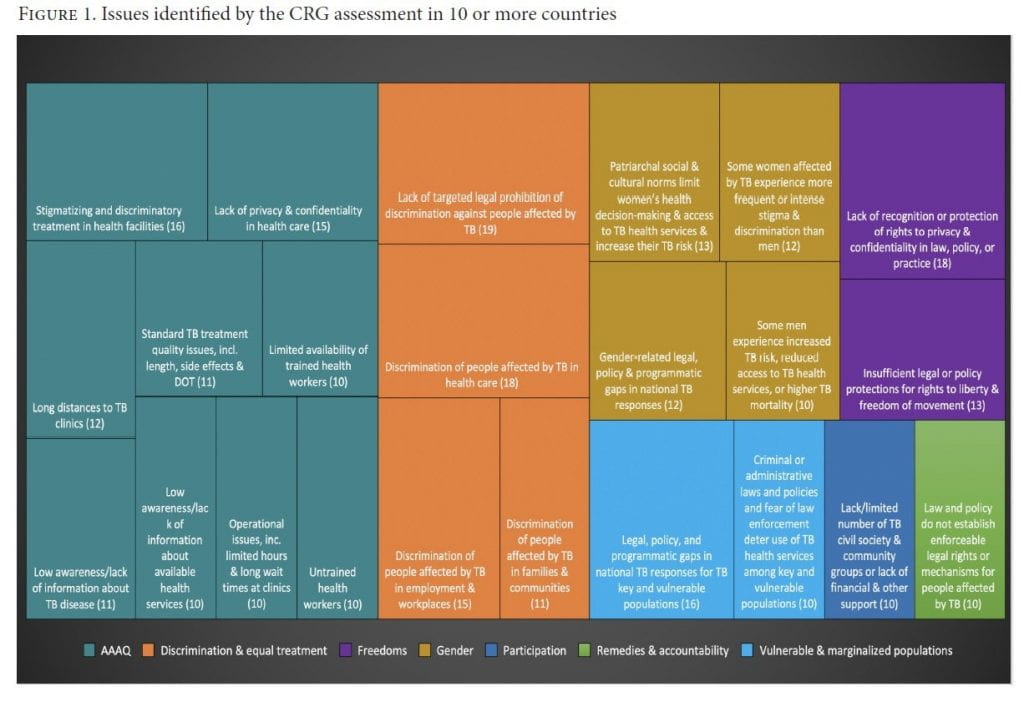
The CRG assessment findings examined in this article highlight a broad spectrum of challenges and opportunities. Despite considerable diversity among the issues, as Figure 1 demonstrates, there is a meaningful overlap of shared challenges across the 20 countries and four regions. For example, 90% of the assessments found that people affected by TB experience stigmatizing and discriminatory treatment in health care. Seventy-five percent of the assessments revealed that people affected by TB experience employment discrimination. Despite this, 95% of the countries in this article fail to explicitly prohibit discrimination against people affected by TB in law. The assessment findings in 90% of the countries highlight various privacy concerns, including breaches in confidentiality that deter the use of TB health services. In 65% of the countries, the assessment findings indicate that patriarchal norms negatively impact women’s access to TB health services and increase their vulnerability to TB infection and disease. These remarkable findings shed new light on often overlooked challenges that are critical to meeting global commitments to end TB by 2030.
This year, WHO released an updated list of countries with high burdens of TB, TB/HIV coinfection, or multidrug/rifampicin-resistant TB.[47] More than 30 of these high-burden countries have not yet conducted the CRG assessment. In 2020, the STP Affected Communities Delegation and the Developed and Developing Countries NGO Delegations called for all high-burden countries to conduct the CRG assessment and develop costed national action plans with detailed budgets and monitoring and evaluation frameworks for community, human rights, and gender by 2022.[48] They recommended that countries integrate the assessment findings into their TB national strategic plans to establish relevant targets and set national funding and intervention priorities. The STP delegations further recommended that a completed CRG assessment and corresponding national action plan be prerequisites for countries to obtain grants from the Global Fund and other donors.[49] In line with these recommendations, the CRG assessment has already led to costed national action plans for community, human rights, and gender in Bangladesh, the Democratic Republic of the Congo, India, Nigeria, and Tanzania, and similar processes are forthcoming in most of the other countries in this article.[50]
The CRG assessment findings represent a call to action for donors and technical partners to prioritize community, human rights, and gender in their programmatic and investment priorities for TB. These institutions include WHO, STP, the Global Fund, other multilateral donors, bilateral donors, international organizations, and philanthropic foundations. The WHO Global Tuberculosis Programme should incorporate the CRG assessment findings into World Health Assembly resolutions, its influential annual Global Tuberculosis Report and normative guidances, and the WHO Multisectoral Accountability Framework to Accelerate Progress to End TB by 2030.[51]
As the largest international donor for TB, the Global Fund should leverage the CRG assessment findings to increase its financial support for community, human rights, and gender interventions in TB through established funding mechanisms by promoting TB community-led monitoring and developing TB indicators for human rights and gender.[52] The latter could be enabled within the Global Fund’s 2021 Strategy Framework and operational guidance and incentivized as prerequisites for national TB grants building on the stigma indicator in the Global Fund’s Performance Framework.[53]
The UN-hosted STP should improve the CRG assessment tool in line with this article’s suggestions (see below) and seek increased donor support for its Challenge Facility for Civil Society grant program. Among other things, this program funds TB community and civil society groups to conduct the CRG assessment and implement and monitor the assessment’s recommendations.[54] STP should also include the CRG assessment findings in its upcoming Global Plan to End TB: 2023–2030 and the next iterations of the Governance of TB Programs and TB Commitments vs. TB Realities reports due ahead of the next UN High-Level Meeting on Tuberculosis in 2023.[55]
As more countries—including those on the new WHO high-burden lists—focus on community, human rights, and gender, STP and partners should strengthen the CRG assessment tool and promote greater consistency in the country reports it produces. Six concrete ideas for strengthening the CRG assessment tool emerged from this article’s analysis: (1) ensure that the assessment process is adaptable and capable of integrating emerging issues, such as COVID-19 and other health emergencies; (2) improve the quality and promote greater uniformity of the assessment’s methodologies through enhanced guidance, training, and technical support, including for quantitative methodologies that researchers may incorporate; (3) identify and prioritize critical issues neglected in the 20 completed assessments, such as TB community participation, health governance and systems, legal aid and remedies, and psychosocial support; (4) incorporate a critical analysis of DOT—the predominant but flawed TB treatment paradigm—in favor of community-based approaches; (5) employ a gender-transformative—rather than simply a gender-sensitive—lens in the assessment; and (6) explicitly position the assessment as the start of a dialogue and process to integrate communities, human rights, and gender into national TB responses, including through costed national action plans and dedicated funding for civil society and community groups.
Conclusion
A paradigm shift has begun in the global TB response. The emergent focus on communities, human rights, and gender has rejuvenated the fight against an age-old yet curable disease driven by social and economic disadvantage. The STP CRG assessment and its findings from the 20 countries in this article are both a product and a forceful example of these new ideas. We urge further research, discussion, and action by national TB programs, people affected by TB, scholars, and other global and national stakeholders to develop solutions to the challenges identified by the CRG assessment. Community, human rights, and gender-focused TB interventions are especially critical in light of the unprecedented challenges of the COVID-19 pandemic. As the world quickly moves toward the conclusion of the 2030 Sustainable Development Agenda, civil society and community groups, countries affected by TB, and donors and technical partners must leverage the CRG assessment and its findings in pursuit of the targets and commitments to end TB in the political declaration from the UN High-Level Meeting on Tuberculosis and other global plans.
Brian Citro, BM, JD, is a human rights lawyer and independent researcher, Chicago, USA.
Viorel Soltan, MPH, MBA, PhD, is head of country and community support for impact at the Stop TB Partnership, Geneva, Switzerland.
James Malar, LLB, BSocSC, LLM, is a community, rights, and gender program officer at the Stop TB Partnership, Geneva, Switzerland.
Thandi Katlholo, BSc (Hons), MPH, is a program officer at the Stop TB Partnership, Geneva, Switzerland.
Caoimhe Smyth, MA, MSc, is a community, rights, and gender program officer at the Stop TB Partnership, Geneva, Switzerland.
Ani Herna Sari, SIP, MMedKom, is a PhD candidate in social science at Airlangga University and a tuberculosis survivor, Surabaya, Indonesia.
Olya Klymenko, BSc, is the chairwoman of TBpeople Ukraine, a member of the Stop TB Partnership Community Delegation, and a tuberculosis survivor, Kyiv, Ukraine.
Maxime Lunga, BDD, is the chairman of Club des Amis Damien, a member of the Stop TB Partnership Community Delegation, and a tuberculosis survivor, Democratic Republic of the Congo.
Please address correspondence to Brian Citro. Email: bricitro@gmail.com.
Competing interests: None declared.
Copyright © 2021 Citro, Soltan, Malar, Katlholo, Smyth, Herna Sari, Klymenko, and Lunga. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Stop TB Partnership, Global plan to end TB 2018–2020: The paradigm shift (Geneva: STP, 2018).
[2] Stop TB Partnership, About Stop TB Partnership (2021). Available at https://www.stoptb.org/about-stop-tb-partnership.
[3] Global Fund, Questions and answers: Breaking down barriers to access; Scaling up programs to remove human rights-related barriers to health services in 20 countries and beyond (Geneva: Global Fund, 2020); Stop TB Partnership, TB stigma assessment implementation handbook (Geneva: STP, 2019); Stop TB Partnership, OneImpact community-led monitoring framework: Empowering communities to End TB (Geneva: STP, 2021).
[4] World Health Organization, Global tuberculosis report 2021 (Geneva: WHO, 2021), p. 8.
[5] Ibid., pp. 1, 7.
[6] Ibid.
[7] Ibid., p. 9.
[8] M. Deutsch-Feldman, R. Pratt, S. Price, et al., “Tuberculosis: United States, 2020,” Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report 70 (2021), pp. 409–414; J. Self, C. McDaniel, S. Bamrah Morris, et al., “Estimating and evaluating tuberculosis incidence rates among people experiencing homelessness, United States, 2007–2016,” Medical Care 59 (2021), pp. S175–S181; J. L. Potter, L. Inamdar, E. Okereke, et al., “Support of vulnerable patients throughout TB treatment in the UK,” Journal of Public Health 38 (2016), pp. 391–395.
[9] Stop TB Partnership, The potential impact of the COVID-19 response on tuberculosis in high-burden countries: A modelling analysis (Geneva: STP, 2020).
[10] Stop TB Partnership, One year on, new data show global impact of COVID-19 on TB epidemic is worse than expected (Geneva: STP, 2021).
[11] World Health Organization (2021, see note 4), pp. 1, 4.
[12] Ibid.
[13] Ibid., p. 7.
[14] United Nations General Assembly, Transforming Our World: The 2030 Agenda for Sustainable Development, UN Doc. A/RES/70/1 (2015); World Health Organization, The end TB strategy (Geneva: WHO, 2014); World Health Organization, Moscow declaration to end TB (Geneva: WHO, 2017); Stop TB Partnership (2018, see note 1).
[15] Ibid.
[16] United Nations General Assembly, Political Declaration of the High-Level Meeting of the General Assembly on the Fight against Tuberculosis, UN Doc. A/RES/73/3 (2018).
[17] Ibid., para. 24.
[18] Ibid., paras. 17, 19, 23, 33, 35, 37, 39, 48.
[19] Stop TB Partnership (2019, see note 3); Stop TB Partnership, Challenge facility for civil society. Available at https://www.stoptb.org/communities-rights-and-gender-crg/challenge-facility-civil-society.
[20] Stop TB Partnership, Communities, rights and gender (CRG). Available at https://www.stoptb.org/prioritising-people-human-rights-gender/communities-rights-and-gender-crg.
[21] Human Rights Council, Contributions of the Right to Health Framework to the Effective Implementation and Achievement of the Health-Related Sustainable Development Goals: Report of the United Nations High Commissioner for Human Rights, UN Doc. A/HRC/38/37 (2018).
[22] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI), art. 12 (1966); Committee on Economic, Social and Cultural Rights, General Comment No. 14, The Right to the Highest Attainable Standard of Health, UN Doc. E/C.12/2000/4 (2000); Office of the United Nations High Commissioner for Human Rights, Annual thematic reports of the Special Rapporteur on the right to physical and mental health (2021). Available at https://www.ohchr.org/EN/Issues/Health/Pages/AnnualReports.aspx.
[23] Office of the United Nations High Commissioner for Human Rights, Special Rapporteur on the right to physical and mental health (2021). Available at https://www.ohchr.org/EN/Issues/Health/Pages/SRRightHealthIndex.aspx.
[24] Stop TB Partnership Secretariat, Stop TB annual report 2000 (Geneva: WHO, 2001), p. 24; Stop TB Parntership Secretariat, A human rights approach to TB: Stop TB guidelines for social mobilization (Geneva: WHO, 2001).
[25] See, e.g., A. Boggio, M. Zignol, E. Jaramillo, et al., “Limitations on human rights: Are they justifiable to reduce the burden of TB in the era of MDR-and XDR-TB?,” Health and Human Rights Journal 10/2 (2008), pp. 121–126; J. J. Amon, F. Girard, and S. Keshavjee, “Limitations on human rights in the context of drug-resistant tuberculosis: A reply to Boggio et al.,” Health and Human Rights Journal 11/1 (2009); T. Slagle, M. Ben Youssef, G. Calonge, et al., “Lessons from Africa: Developing a global human rights framework for tuberculosis control and prevention,” BMC International Health and Human Rights 14 (2014).
[26] Health and Human Rights Journal 18/1 (2016).
[27] TBpeople and Stop TB Partnership, Declaration of the Rights of People Affected by Tuberculosis (2019).
[28] B. Citro, Activating a human rights-based tuberculosis response: A technical brief for policymakers and program implementers (Global Coalition of TB Activists, Stop TB Partnership, Northwestern Pritzker School of Law Center for International Human Rights, 2020).
[29] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 2.
[30] Ibid.
[31] Committee on Economic, Social and Cultural Rights (see note 22), para. 30.
[32] Ibid., para. 12(a).
[33] Ibid., para. 12(b).
[34] Ibid., para. 12(c).
[35] Ibid., para. 12(d).
[36] Ibid., paras. 18, 19.
[37] Ibid., paras. 3, 8.
[38] Ibid., para. 20.
[39] See Office of the United Nations High Commissioner for Human Rights, Special Rapporteur on the right to physical and mental health: Purpose of the mandate (2021). Available at https://www.ohchr.org/en/issues/health/pages/srrighthealthindex.aspx.
[40] Committee on Economic, Social and Cultural Rights (see note 22), para. 37.
[41] Ibid., para. 11.
[42] Ibid., paras. 59–62.
[43] Stop TB Partnership, Communities, rights and gender (CRG): TB CRG assessment country reports. Available at https://www.stoptb.org/prioritising-people-human-rights-gender/communities-rights-and-gender-crg.
[44] World Health Organization, Ethics guidance for the implementation of the end TB strategy (Geneva: WHO, 2017), ch. 15.
[45] United Nations General Assembly (2018, see note 16), paras. 17, 19, 23, 33, 35, 37, 39, 48.
[46] Ibid., preamble.
[47] World Health Organization, WHO global lists of high burden countries for tuberculosis (TB), TB/HIV and multidrug/rifampicin-resistant TB (MDR/RR-TB), 2021–2025: Background document (Geneva: WHO, 2021).
[48] Stop TB Partnership, Deadly divide: TB commitments vs. TB realities (Geneva: STP, 2020), p. 44.
[49] Ibid.
[50] Ibid., p. 22.
[51] World Health Organization, WHO multisectoral accountability framework to accelerate progress to end TB by 2030 (Geneva: WHO, 2019).
[52] Global Fund, Results Report 2021 (Geneva: Global Fund, 2021), p. 33.
[53] Global Fund, Strategy development. Available at https://www.theglobalfund.org/en/strategy-development/; Global Fund, Modular framework handbook (Geneva: Global Fund, 2019), p. 96.
[54] Stop TB Partnership, Challenge facility for civil society (see note 19).
[55] Stop TB Partnership and USAID, Governance of TB programs: An assessment of practices in 22 countries (Geneva: STP and USAID, 2021); Stop TB Partnership (2020, see note 48).