Quantifying the Ripple Effects of Civil War: How Armed Conflict Is Associated with More Severe Violence in the Home
Volume 23/1, June 2021, pp. 75-89
Jocelyn T. D. Kelly, Elizabeth Colantuoni, Courtland Robinson, and Michele R. Decker
Abstract
Both the fields of public health and that of human rights seek to improve human well-being, including through reducing and preventing all forms of violence, to help individuals attain the highest quality of life. In both fields, mathematical methods can help “visibilize” the hidden architecture of violence, bringing new methods to bear to understand the scope and nuance of how violence affects populations. An increasing number of studies have examined how residing in a conflict-affected place may impact one of the most pervasive forms of violence—intimate partner violence (IPV)—during and after conflict. This paper contributes to this effort by examining whether severe forms of IPV are associated with previous experience of political violence in one conflict-affected country: Liberia. Our findings indicate that living in a district with conflict fatalities increased the risk of IPV among women by roughly 60%. Additionally, living in a district with conflict fatalities increased the risk of a past-year injury from IPV by 50%. This analysis brings to light links between two of the most pervasive forms of violence—political violence and violence against women. The findings suggest that women residing in a district that is more highly affected by conflict, not only people experiencing direct trauma during conflict, may be at risk of increased violence long after peace is declared. These findings point to the need for targeted programs that address IPV postconflict.
Introduction
Violence, including political conflict and interpersonal violence, accounts for a significant burden of injury and death worldwide.[1] For the purposes of this paper, political violence is defined as “the use of force by a group with a political purpose or motivation.”[2] Interpersonal violence is defined as “the intentional use of physical force or power, threatened or actual, against another person, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation.”[3]
Both the fields of public health and that of human rights seek to improve human well-being, including through reducing and preventing all forms of violence, to help individuals attain the highest quality of life. The right to health and the right to live a life free from violence are enshrined in human rights law and promoted by the World Health Organization (WHO).[4] While addressing violence is core to both human rights and public health, each field leverages distinct approaches to understand the abuses that threaten human well-being.
One of the ways that human rights efforts have historically sought to mobilize action is through advocacy. In many cases, the images associated with atrocities—in media portrayals and through victim narratives—have played a key role in engaging global attention and action. Yet, feminist and postcolonial scholars have interrogated how “atrocity aesthetics” can distort our understanding, privileging certain forms victimization while dismissing others.[5] As noted by Randle DeFalco, “dominant socially shared understandings of what constitutes an atrocity are grounded in an aesthetic model of large-scale harm causation that is comprised of two key elements: spectacle and familiarity.”[6] Media accounts can both amplify and distort human rights advocacy, narrating and re-narrating stories that play into comfortable understandings of what atrocities look like—a practice that can occlude an accurate understanding of how and where abuses occur.[7]
To address this challenge, a number of human rights organizations have sought to ground advocacy narratives in systematic analyses of data, a practice that has become increasingly common in recent decades.[8] The field of public health is founded on a strong tradition of conducting large-scale systematic efforts to quantify morbidity and mortality through population-based surveys, clinical records, rapid needs assessments, and other approaches. As each field grapples with the ability to collect and analyze ever larger data sets with increasingly sophisticated analytical techniques, they can learn from and complement each other.
Mathematical methods in particular can help “visibilize” the hidden architecture of violence, bringing new methods to bear to understand the scope and nuance of how violence affects populations. By helping lay bare patterns of abuse that may not conform to our understanding of “typical” atrocities, these approaches can represent a powerful tool to advance the twin pursuits of public health and human rights to recognize and address grave harms. Perhaps nowhere is this leveraging of empirical methods more important than for a form of violence that is notoriously hidden—gender-based violence (GBV).
GBV refers to any harmful act that is perpetrated against a person’s will and that is based on socially ascribed gender differences between males and females; it is one of the most prevalent forms of interpersonal violence and has been called one of the most pervasive forms of human rights violations worldwide.[9] Globally, it is among the top 10 causes of disability-adjusted life years lost and disproportionately affects women.[10] GBV not only carries severe physical, psychological, and social consequences but also keeps women from fully engaging in political and economic systems.[11]
The past four decades have witnessed a belated recognition that addressing GBV is fundamental to protecting human rights. A succession of meetings and international commitments in the 1990s recognized the vital importance of violence prevention as a public health and human rights imperative.[12] One of the most common forms of GBV is intimate partner violence (IPV). WHO defines IPV as “behavior by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviours.” As governments turned their attention the prevention of GBV, including IPV, there was a call for rigorous, population-based research that could provide an empirical foundation for action.[13] This call mirrored a wider trajectory in the field of human rights to draw on epidemiological methods and population-based data to examine some of the most hidden forms of violence, particularly in conflict and crisis. Oskar Thoms and James Ron trace the influence of methods used to quantify the cost of conflict, noting that “epidemiologists are gradually demonstrating that most existing studies grievously underestimate war’s overall human cost by failing to capture its indirect and long-term impacts.”[14]
An increasing number of studies have begun examining how residing in a conflict-affected place may impact IPV during and after conflict.[15] This paper aims to contribute to this continued effort by examining whether severe forms of IPV are associated with previous experience of political violence in one conflict-affected country: Liberia. The conclusion will explore the long-term repercussions of conflict for individuals and communities, and the implications for public health and human rights.
Beyond battle deaths: Quantifying the ripple effects of war
Increasingly, studies have documented the detrimental impacts of conflict, looking not only at excess mortality but also at a range of other health outcomes, including injury, trauma, and disease.[16] A central conundrum, however, is that the chaotic nature of war has made the systematic examination of its human impact difficult or impossible. Christopher Murray et al. discuss how examining the health impact of conflict has fallen into a limbo between the fields of public health and political science and receives inadequate attention from both.[17] However, new techniques to measure physical and mental health are changing existing understandings of the impact of war. A number of efforts have taken the first steps to estimate the direct and indirect effects of political instability in new ways.
Population-based surveys that draw on family health history and verbal autopsy have proven effective in documenting the impact of conflict in a number of countries, as have nesting mortality assessments within other planned assessments.[18] These techniques have shown that indirect causes of death—such as inadequate access to water, sanitation, and health services—have accounted for most civilian deaths and have had a differentially large impact on children and early teens.[19]
Violence: From political conflict to interpersonal violence
One of the newest frontiers in understanding conflict involves quantifying how political violence may impact human aggression even after formal peace is declared. An increasingly rich body of literature documents the “contagion” of violence. Like diseases and many complex social phenomena, violence can be transmitted across individuals, groups, generations, and different levels of social organization.[20]
Together, political violence and GBV, including IPV, represent two of the most pressing affronts to human rights and well-being throughout the world; understanding how these abuses are linked will help advance an understanding of how cycles of violence can potentially be disrupted.[21] Globally, 35% of women globally have been victims of physical or sexual abuse during their lifetime.[22] In turn, war accounts for roughly one-fifth of deaths globally.[23]
IPV can be a major factor affecting the physical and mental health of individuals before, during, and after conflict.[24] Because it occurs in homes rather than in theaters of war and may be condoned or overlooked because of cultural norms, IPV is often far less visible than conflict-related sexual violence.[25] This form of abuse, however, may be more common than sexual violence perpetrated by armed actors during war.[26] Relatively few studies have examined how political violence at the community level may impact IPV, though this field is rapidly expanding to understand how residing in a conflict-affected place may impact IPV after peace has been declared.[27] However, previous research from Liberia has shown that residence in a fatality-affected district in Liberia was significantly associated with a 50% increase in IPV and increases in nonpartner physical violence.[28]
This paper aims to extend this body of work by examining whether severe forms of IPV are associated with previous experience of political violence. The multilevel analysis focuses on a single conflict-affected setting—Liberia—and leverages household-based survey data collected through Liberia’s Demographic and Health Survey (DHS) for IPV outcomes, and data gathered from the ACLED database for political violence exposures. Results are discussed in the context of the long-term impact of conflict on individuals and communities, and the implications for public health and human rights.
Liberia country profile
Situated in West Africa, Liberia is one of the continent’s smaller countries. In 1979, riots broke out in the country in reaction to rising prices of rice, economic stagnation, and increasing tension between the Americo-Liberian population and Indigenous groups.[29] The ensuing unrest launched the first Liberian war (1985–1996). From 1989 to 1997, according to national-level data, the countrywide conflict resulted in the deaths of over 150,000 Liberians.[30] In 1999, antigovernment fighting once again broke out. Rebel groups entered Liberia from neighboring countries and fighting became widespread in the following year.[31] The Second Liberian Civil War (1999–2003) ended after international intervention, when a peace agreement was signed and rebel troops were demobilized. In both wars, combatants were both victims and perpetrators of human rights abuses, including rape, torture, and murder.[32]
Study data and methods
Analytic sample
This study combines geo-coded information from two existing datasets: the Liberia DHS, which provides individual-level data on health and social outcomes in 2007—four years after the Liberian Civil War—and ACLED, which provides information on the number of conflict events and fatalities occurring during Liberia’s civil unrest from 1999 to 2003.[33] We chose the 2007 Liberia DHS because it provides the first population-based data in Liberia after the conflict. While other DHSs are more recent, they represent a longer lag between the conflict and the outcomes we are seeking to understand. In the 2007 DHS, 7,092 of 7,448 women sampled completed the survey. Of these, a total of 4,913 women were sampled for the domestic violence module. Roughly 400 individuals were not given a geographic identifier in the DHS dataset, representing 8.4% of the sample, leaving 4,502 women. Of these 4,502 women, just over 80% (n=3,648) were administered questions about intimate partner violence because they reported being currently or formerly in a union. Over 98% of the sample (n=3,596 women) responded to this question and are thus eligible for inclusion in the analysis.
Severe intimate partner violence in the past 12 months
Ever-partnered women were classified as having experienced partner physical violence or partner sexual violence within the last 12 months if they replied “yes” to at least one item from Table 1 and responded that the violence occurred “sometimes” or “often” within the last 12 months.
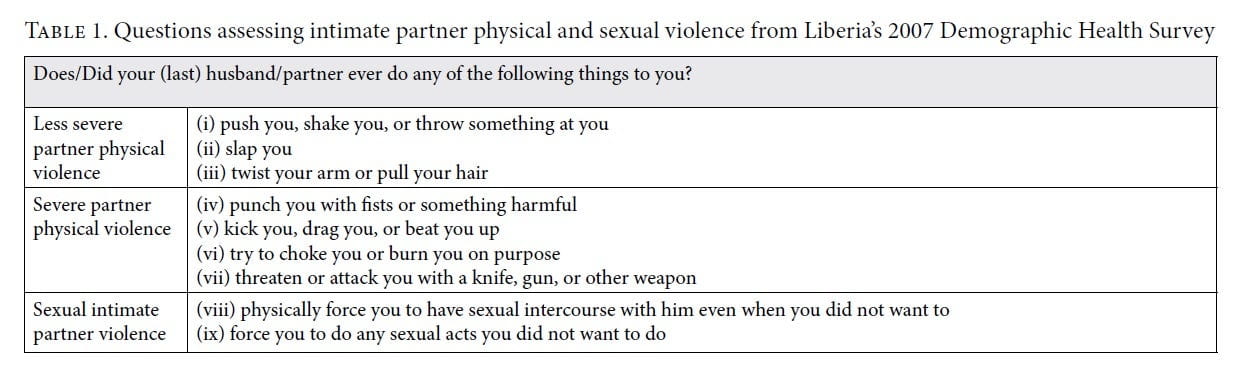
Severe IPV is defined by WHO “on the basis of the severity of the acts of physical violence: being beaten up, choked or burnt on purpose, and/or being threatened or having a weapon used against you is considered severe. Any sexual violence is also considered severe.”[34] Those women who reported any of the forms of violence from items iv–vii were defined as having experienced severe IPV. Those women who responded having experienced any of the forms of violence from items viii or ix were defined as having experienced sexual IPV. This approach is in keeping with other studies that have looked at the severity of IPV.[35]
Our project assessed IPV in the categories given in Table 1: no IPV, less severe IPV, severe IPV, and sexual IPV. WHO categorizes sexual IPV within the severe category; we assessed this form of violence separately from physical violence to determine whether there might be differences between sexual and physical IPV. This approach reflects the fact that IPV often escalates from less severe to more severe, either during the same altercation or over time. Looking at only one form of violence while excluding less severe forms of violence would result in untenably small sample sizes for the analysis. Women are classified according to the most severe form of violence they have experienced during the past year, with sexual IPV considered the most severe.
Injuries from intimate partner violence in the past 12 months
Of those women reporting having experienced IPV, women were given three questions that assessed three different sets of injuries: (1) cuts, bruises, or aches; (2) burns, eye injuries, sprains, or dislocations; and (3) deep wounds, broken bones, broken teeth, or any other serious injury. Women who responded “yes” to any of the three questions were classified as having experienced injuries from past-year IPV.
Primary predictor: Conflict exposure
ACLED defines a politically violent event as “a single altercation where often force is used by one or more groups for a political end, although some instances, including protests and non-violent activity, are included in the dataset to capture the potential pre- cursors or critical junctures of a conflict.”[36] The quantification of politically violent events in Liberia allows us to characterize conflict in the country through fatalities and events—the primary exposures for this analysis.[37] Events are any political incident, including clashes, protests, riots, and battles that occurred during the 1999–2003 civil war. If an event resulted in any deaths, then the number of fatalities were recorded. Thus, all fatalities occur as a result of a political event, but every event does not necessarily result in fatalities. The conflict measures were aggregated at the district level. There are 61 districts in Liberia, which are administrative areas defined by the national government. Districts were chosen because they are large enough areas to have large numbers of individuals and have heterogeneity across their levels of conflict exposure.
Potential confounding variables
Potential confounding variables measured for each woman were selected based on theory as well as by those variables that have been found to be significantly associated with interpersonal violence.[38]
Model specification
Multilevel regression models were used to quantify the associations between levels of IPV (multinomial model) and experience of IPV-related injury (logistic model) with district-level conflict. Models contained a random intercept defining the district. Separate models were constructed using the primary exposure and the two alternative conflict measures. All models included the potential confounding variables described above. To account for the complex survey design of the DHS, the survey weights for the DV module were included in all analyses.[39] Analyses were conducted with Stata/SE 14.0.
Results
Severe intimate partner violence
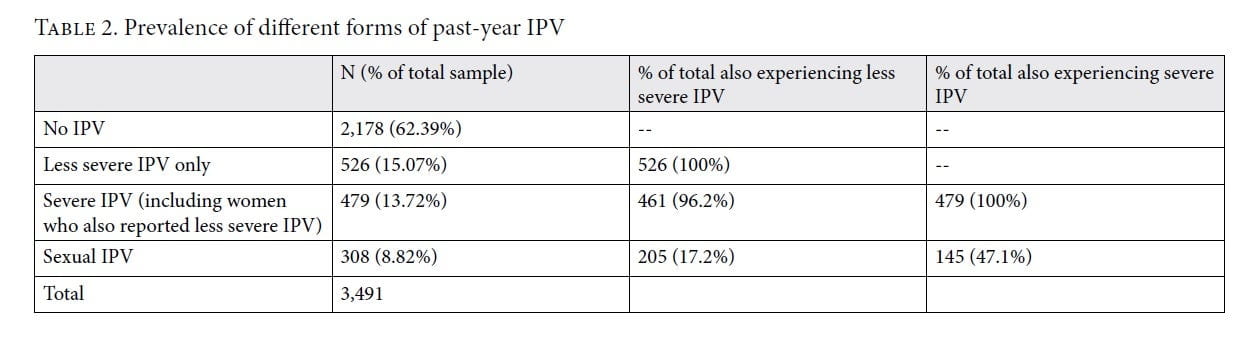
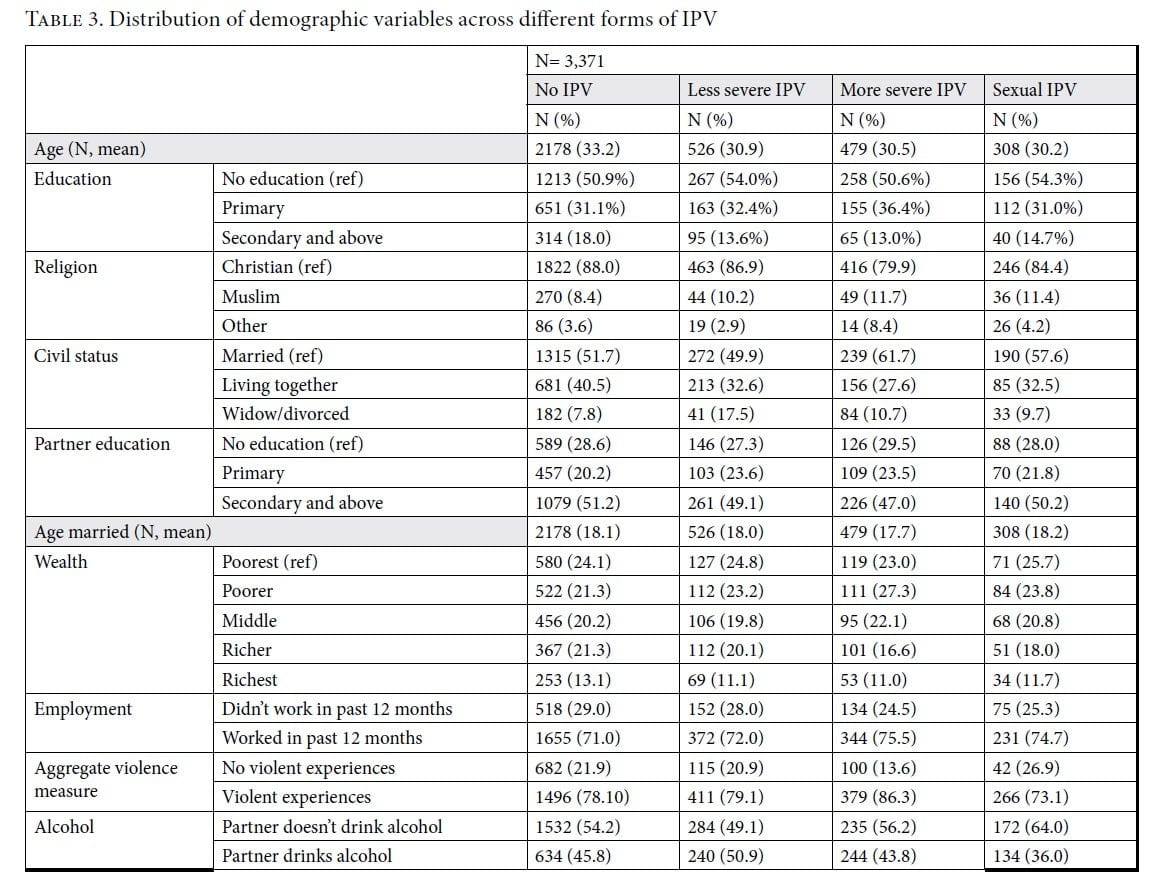
Of the 3,596 women asked about past-year IPV, 18.5% (n=665) stated they had experienced less severe IPV, 12.6% (n=454) reported severe IPV, and 8.3% (n=299) reported sexual IPV. As noted in the methods, violence often escalates from less to more severe forms of IPV. This is borne out by the data below: 96% of women who experience severe IPV also experience less severe IPV. While sexual IPV does occur without physical IPV, roughly half of women experiencing sexual IPV also experience severe IPV (Table 2). The distribution of demographic characteristics of women across the different levels of IPV is given in Table 3.
Analysis comparing districts with and without conflict fatalities
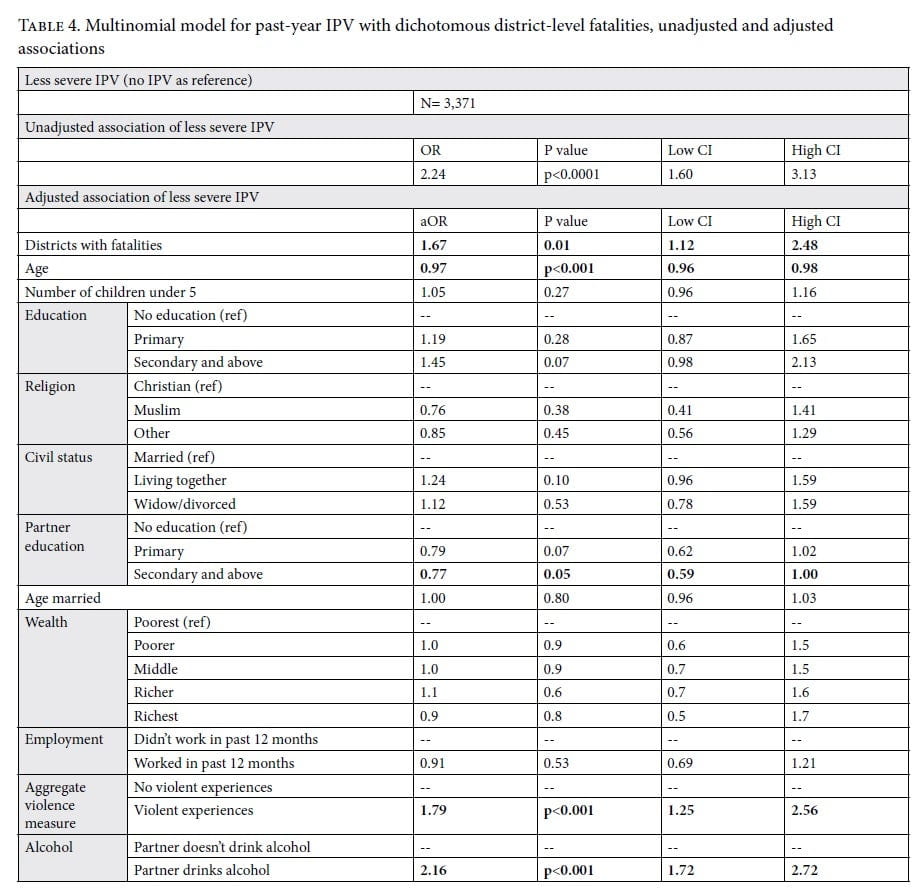
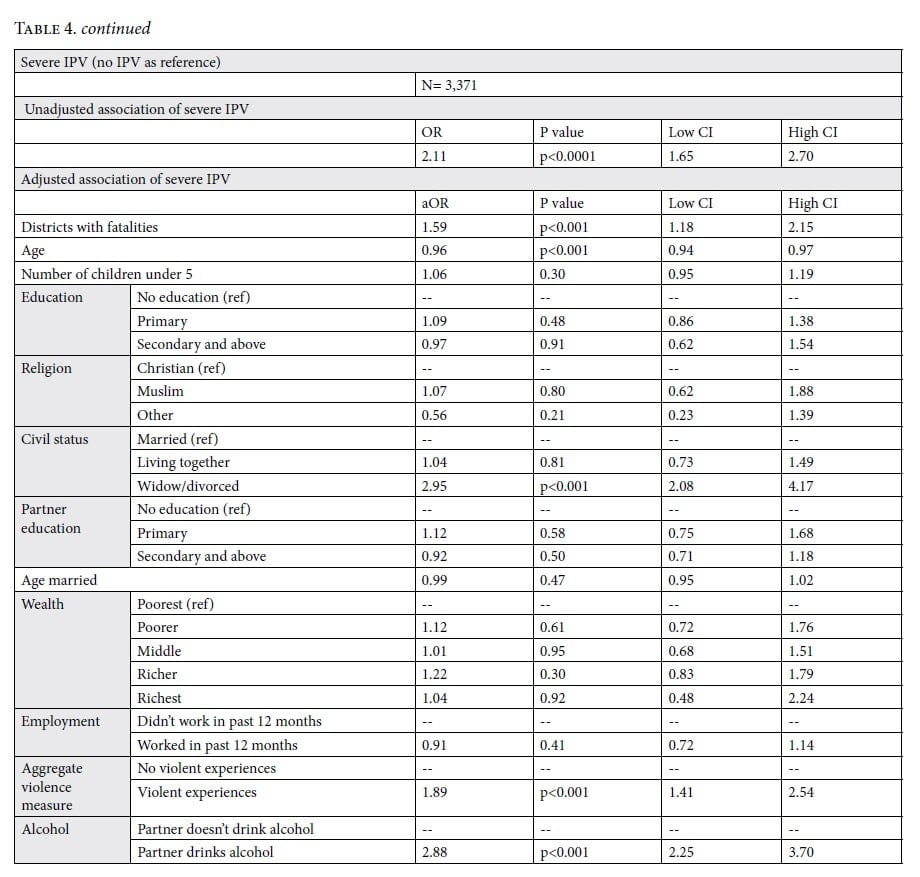
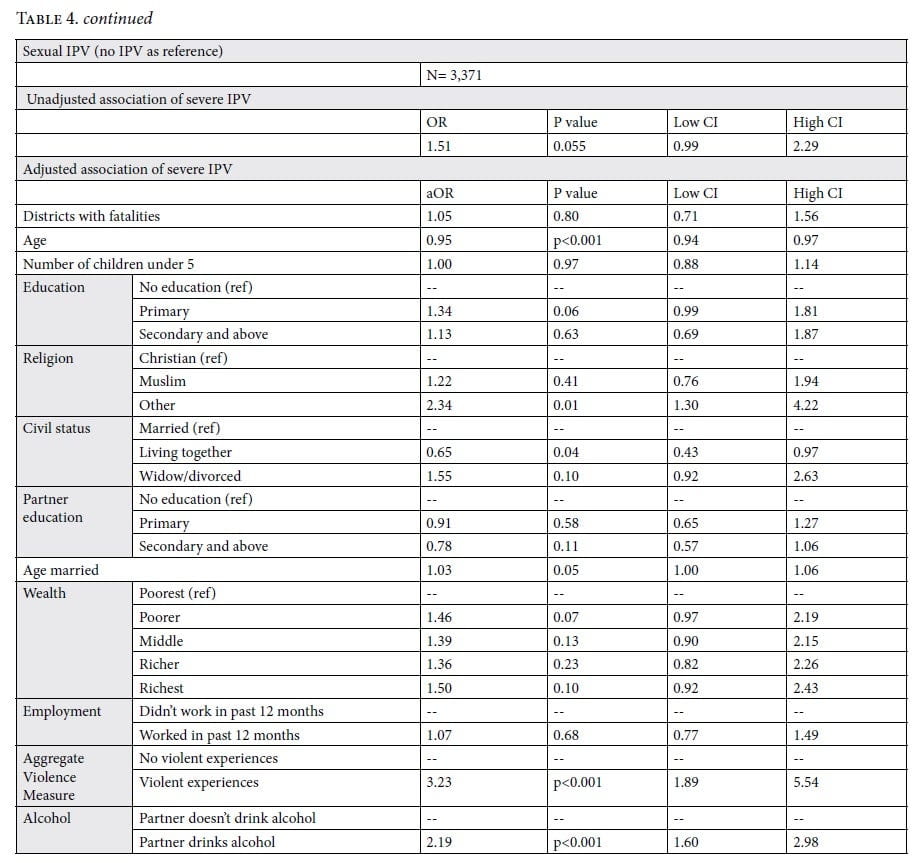
Compared to women living in a district with no conflict fatalities, the unadjusted relative odds of women reporting less severe IPV versus no IPV were 2.24 times greater among women living in a district with conflict fatalities (95% confidence interval (CI): 1.60–3.13). A similar association is seen with regard to severe IPV: women reporting severe IPV versus no IPV were roughly two times greater among women living in a district with conflict fatalities compared to no fatalities (odds ratio (OR) 2.11, p<0.0001). Sexual IPV has a more attenuated relationship than the other forms of IPV to the conflict predictor. For a district experiencing fatalities versus no fatalities, the odds of sexual IPV compared to no IPV are 1.5 times higher with marginal significance (OR 1.51, p=0.055).
The adjusted relative odds of experiencing less severe IPV versus no IPV among women living in a district with no fatalities compared to a district with any conflict fatalities were 67% higher for women living in fatality districts compared to their counterparts living in fatality-free districts (aOR 1.67, p=0.01).
Women living in a district with any fatalities were 59% more likely to experience severe IPV than their counterparts living in fatality-free districts compared to the referent group (aOR 1.59, p<0.001). Being widowed or divorced (aOR 2.95, p<0.001), having a partner who drinks alcohol (aOR 2.88, p<0.001), and having any past violent experiences (aOR 1.89, p<0.001) were also risk factors for this abuse. Each additional year of age (aOR 0.96, p<0.001) was a protective factor.
Compared to women living in a district with no conflict fatalities, the adjusted relative odds of women reporting sexual IPV versus no IPV were 5% higher for women living in a district with conflict fatalities. However, this result was not significant (aOR 1.05, p=0.80) (Table 4).
Because this analysis parses the outcome into four levels, the sample size was too small to run across cumulative conflict event years. However, the additional injury analysis below provides some insight into how cumulative levels of conflict may be related to IPV.
Injuries resulting from intimate partner violence
Of the 1,418 women who reported any form of past-year IPV, 1,397 answered questions about injuries resulting from that violence (97.8% response rate). From this sample, 30.2% (n=419) reported having an injury resulting from IPV.
Analysis comparing districts with and without conflict fatalities
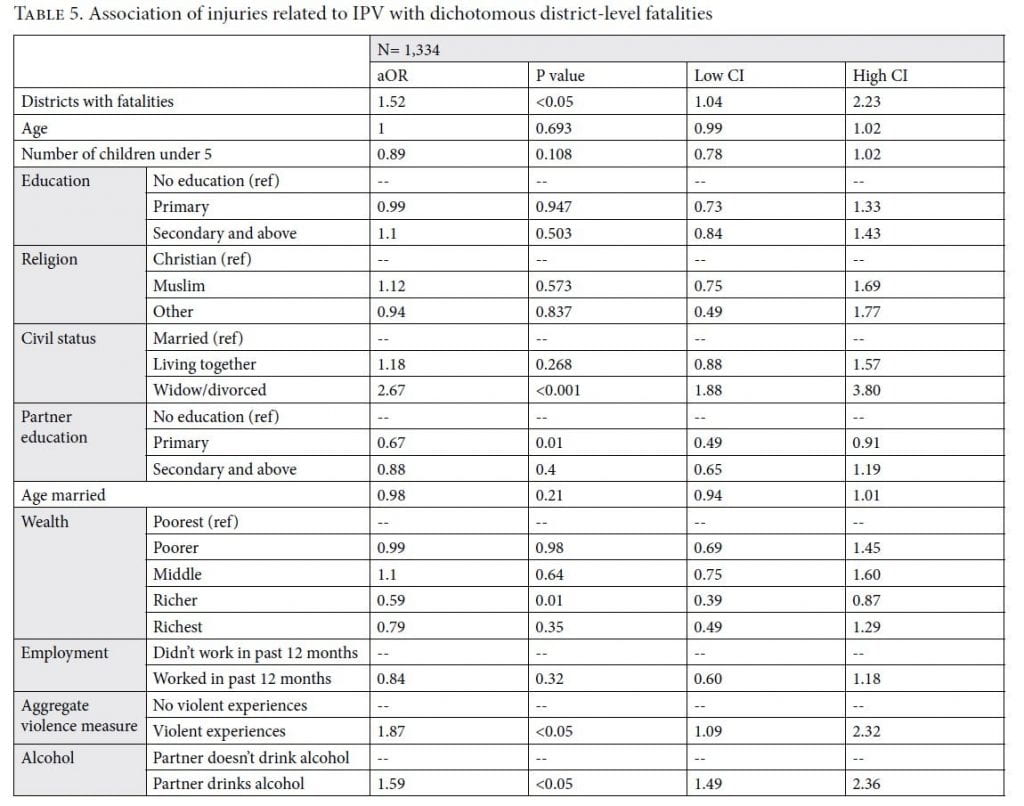
In the adjusted model, living in a district with conflict fatalities was associated with a 50% increase in IPV-related injuries (aOR 1.52, p<0.05; Table 5). Other variables significantly associated with increased risk of injury were being widowed or divorced compared to currently married (aOR 2.67, p<0.0001); having a partner who drinks alcohol (aOR 1.87, p<0.0001); and having any previous experiences with violence (aOR 1.59, p<0.05). Protective factors were having a partner with primary versus no education (aOR 0.67, p=0.01) and being in the second-richest wealth quintile versus the poorest (aOR 0.59, p<0.05).
Analysis of cumulative conflict event years
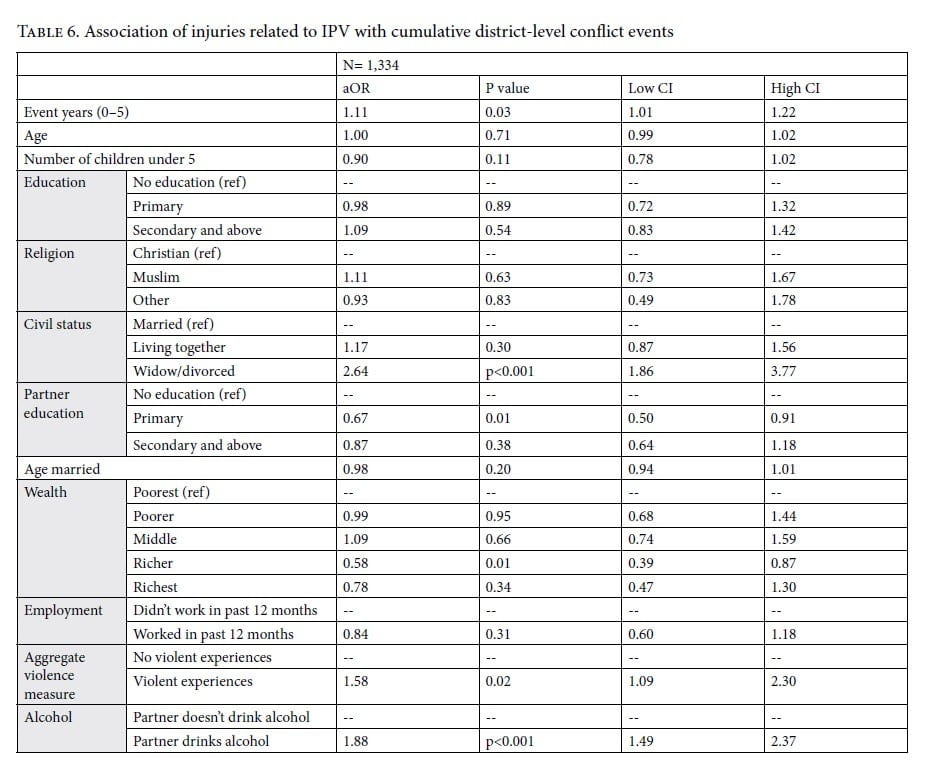
A similar pattern is seen when looking at the burden injury while using a different measure of conflict. After adjusting for all independent variables in the final model, each additional conflict year was associated with an 11% increase in injuries associated with IPV (aOR 1.11, p<0.05) (Table 6).
Limitations
The cross-sectional nature of the DHS limits the ability to draw causal conclusions about the impact of conflict on IPV. However, the fact that conflict events preceded the measurement of the outcomes helps establish a temporal, if not causal, relationship. Additional literature presented here supports the hypothesis that conflict may contribute to postconflict IPV; however, this paper does not make causal claims. Because our analysis draws on secondary data, we were not able to design a survey that elicits additional pertinent information for this analysis (for instance, personal exposure to political violence). The DHS approach to measuring IPV can also be problematic, for it asks only ever-partnered women about IPV even though women in informal or unstable relationships may also be at risk of IPV, and possibly at higher risk. Additionally, direct reporting to an interviewer may lead to systematic underreporting of this abuse.[40] Expanding this analysis to additional countries and undertaking qualitative work to better understand the dynamics and mechanisms at play in postconflict contexts would further our understanding of these issues.
Discussion
The pursuit of human rights is to allow all humans—regardless of age, sex, national or ethnic origin, or other status—to live a life of safety, dignity, and freedom.[41] Political violence and GBV represent some of the gravest threats to human rights globally.[42] In 1993, the United Nations Declaration on the Elimination of Violence against Women recognized violence against women and girls as a violation of human rights.[43] This global acknowledgement of women’s right to “equal enjoyment and protection of all human rights and fundamental freedoms” helped propel a recognition that GBV is unacceptable in all contexts.
For decades, scholars and advocates had challenged long-held beliefs that GBV was an inevitable and inherent by-product of war.[44] The declaration helped enshrine this belief in global doctrine. With an increased understanding of GBV during conflict came a recognition that some of the worst and most pervasive forms of violence during war included violence in the home.[45] Yet, we still have an incomplete understanding of how GBV changes during conflict, and how these changes persist after war has formally ended.
This paper represents a new contribution to the literature examining whether the most severe forms of IPV are associated with previous experience of political violence. Living in a district that experienced conflict fatalities during war can increase the risk of experiencing severe and less severe forms of physical IPV, and being injured from IPV, in the postconflict period. Living in a district with any versus no conflict fatalities increased the risk of both less and more severe forms of IPV by roughly 60% for each form of violence compared to the referent group (no IPV).
Additionally, injury from IPV may serve as a vital, but underreported, measure of the impact of violence in the home. Living in districts with any conflict fatalities increased the risk of a past-year injury from IPV by 50% (p<0.05). There was also an evident dose-response relationship: for each additional year that a district experienced at least one conflict event, the odds of a woman reporting an injury from IPV increased by 11% (OR 1.11, p<0.05).
Research from Uganda, Thailand, Peru, Burma, Cote D’Ivoire, and Liberia has found that women who have higher levels of conflict-related abuses also report higher levels of IPV victimization during and after conflict.[46] This study adds to the growing literature on the links between violence that has begun to make evident the connection between political violence and postconflict IPV—and draws out additional information on how the most severe forms of IPV might be exacerbated. The findings from this and previous studies clearly show the subtle “ripple effects” of conflict on one of the most hidden forms of violence: IPV. Recognizing that violence may endure in communities after political conflict officially ends has implications for postconflict policy decisions, humanitarian response, and public health efforts.[47]
The 2020 Global Peace Index describes a world emerging from the conflicts that have characterized the past decade, but moving toward continuing instability and uncertainty. Current conflicts are characterized by those same factors that are drivers of violence for women—not only during conflict but after: chronic poverty, a vacuum of state and civil institutions, poor access to health care and education, low levels of state accountability, and the risk of continuing instability. Without a better understanding of how two fundamental threats to human rights—war and GBV—are interlinked, we will be less prepared to address ongoing instability globally.
Conclusion
The past two decades have highlighted synergies between the fields of public health and human rights.[48] One vitally important area of convergence is in the understanding of how best to document, prevent, and address violence, particularly during conflict and its aftermath. Large population-based studies and increasingly sophisticated statistical techniques have allowed us to improve our understanding of risk factors and impacts of violence and have shaped policies and the deployment of resources around this issue.[49]
The current analysis show links between two of the most pervasive forms of violence—political violence and violence against women—and suggests that women residing in a district that is more highly affected by conflict, not only people experiencing direct trauma during conflict, may be at risk of increased violence long after peace is declared. These findings point to the need for targeted programs that address IPV after a conflict. This form of violence may become elevated and persist at higher levels for years after war, especially in highly war-affected areas.[50] Understanding the long-term impact of war is vital for effective and sustained recovery, yet there has been little scholarship on the enduring consequences of political violence. Assessing how violence may persist and morph after war is critical, since it may impact a country’s ability to achieve sustained peace.
Jocelyn T. D. Kelly is Director of the Program on Gender, Rights and Resilience at the Harvard Humanitarian Initiative, Cambridge, USA.
Elizabeth Colantuoni is a Senior Scientist in the Department of Biostatistics at the Johns Hopkins Bloomberg School of Public Health, Baltimore, USA.
Courtland Robinson is an Associate Professor in the Department of International Health and Center for Humanitarian Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA.
Michele R. Decker is an Associate Professor in the Department of Population, Family and Reproductive Health and Director of the Women’s Health and Rights Program at the Center for Public Health Human Rights, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA.
Please address correspondence to Jocelyn Kelly. Email: jkelly@hsph.harvard.edu.
Competing interests: None declared.
Copyright © 2021 Kelly, Colantuoni, Robinson, and Decker. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction.
References
[1] E. G. Krug, J. A. Mercy, L. A. Dahlberg, and A. B. Zwi, “The world report on violence and health,” Lancet 360/9339 (2002), pp. 1083–1088.
[2] C. Raleigh and C. Dowd, Armed conflict location and event data project (ACLED) codebook (2015).
[3] World Health Organization, Violence: A public health priority; WHO global consultation on violence and health (Geneva: World Health Organization, 1996).
[4] Ibid.; G. H. Brundtland, “Violence, health and human rights: Toward a shared agenda for prevention,” Health and Human Rights Journal 6/2 (2003), pp. 11–13; Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948); International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966); Office of the United Nations High Commissioner for Human Rights and World Health Organization, The right to health: Fact sheet no. 31 (June 2008).
[5] K. Cronin-Furman and R. Krystalli, “The things they carry: Victims’ documentation of forced disappearance in Colombia and Sri Lanka,” European Journal of International Relations 21 (2021), pp. 79–101; V. Das, Life and words: Violence and the descent into the ordinary (Berkeley: University of California Press, 2007); T. Kimberley, Intimate enemies: Violence and reconciliation in Peru (Philadelphia: University of Pennsylvania Press, 2012); K. Cronin-Furman and M. Lake, “Ethics abroad: Fieldwork in fragile and violent contexts,” PS: Political Science and Politics 51/3 (2018), pp. 607–614.
[6] R. C. DeFalco, International crimes as familiar spectacles: Socially constructed understandings of atrocity and the visibility politics of international criminal law (PhD dissertation, 2017), p. 52.
[7] A. A. Quijano and J. Kell, “A tale of two conflicts: An unexpected reading of sexual violence in conflict through the cases of Colombia and Democratic Republic of Congo,” in M. Bergsmo, A. Butenschon, and E. J. Wood (eds), Understanding and proving international sex crimes (Beijing: Torkel Opsahl, 2012).
[8] P. Ball and M. Price, “Using statistics to assess lethal violence in civil and inter-state war,” Annual Review of Statistics and Its Application 6 (2019), pp. 63–84.
[9] S. T. Fried, “Violence against women,” Health and Human Rights Journal 6/2 (2003), pp. 88–111.
[10] K. S. Chibber and S. Krishnan, “Confronting intimate partner violence: A global health priority,” Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine 78/3 (2011), pp. 449–457.
[11] J. C. Campbell, “Health consequences of intimate partner violence,” Lancet 359 (2002), pp. 1331–1336; M. R. Decker, S. Peitzmeier, A. Olumide, et al., “Prevalence and health impact of intimate partner violence and non-partner sexual violence among female adolescents aged 15–19 years in vulnerable urban environments: A multi-country study,” Journal of Adolescent Health 55/6 (2014), pp. 58–67; K. M. Devries, J. Y. T. Mak, C. García-Moreno, et al., “The global prevalence of intimate partner violence against women,” Science 340/6140 (2013), pp. 1527–1528; R. M. Tolman, “The impact of intimate partner violence on low-income women’s economic well-being,” Center for Financial Security Research Brief No. 5.1 (2011); M. Dekker, “Promoting gender equality and female empowerment: A systematic review of the evidence on property rights, labour markets, political participation and violence against women,” African Studies Center Working Paper 111 (2013).
[12] C. Garcia-Moreno, C. Watts, H. Jansen, et al., “Responding to violence against women: WHO’s multicounty study on women’s health and domestic violence,” Health and Human Rights Journal 6/2 (2003), pp. 112–127.
[13] World Health Organization (1996, see note 3).
[14] O. N. T Thoms and J. Ron, “Public health, conflict and human rights: Toward a collaborative research agenda,” Conflict and Health 1/1 (2007).
[15] G. Østby, “Violence begets violence: Armed conflict and domestic sexual violence in sub-Saharan Africa,” paper presented at SVAC (Sexual Violence and Armed Conflict) Workshop, Harvard University, 2016, pp. 2–3; J. V. Gallegos and I. A. Gutierrez, “The effect of civil conflict on domestic violence: The case of Peru,” SSRN Electronic Journal (2011); M. Janko, S. Bloom, and J. Spencer, Community exposure to violent conflict increases the risk of intimate partner violence in Rwanda (Boston: Population Association of America, 2014).
[16] M. J. Toole, S. Galson, and W. Brady, “Are war and public health compatible?,” International Journal of Gynecology and Obstetrics 44/2 (1994), p. 187; D. G. Sapir and V. T. Gomez, Angola: The human impact of war (Brussels: Université Catholique de Louvain, 2006); B. Coghlan, R. J. Brennan, P. Ngoy, et al., “Mortality in the Democratic Republic of Congo: A nationwide survey,” Lancet 367/9504 (2006), pp. 44–51; P. H. Wise, “The epidemiologic challenge to the conduct of just war: Confronting indirect civilian casualties of war,” Daedalus 146/1 (2017), pp. 139–154.
[17] C. J. L. Murray, G. King, A. D. Lopez, et al., “Armed conflict as a public health problem,” BMJ 324/7333 (2002), pp. 346–349.
[18] S. Doocy, G. Burnham, and W. C. Robinson, “Estimating demographic indicators in a conflict-affected population in Eastern Sudan,” Prehospital and Disaster Medicine 22/2 (2007), pp. 112–119.
[19] Toole et al. (see note 16); Sapir and Gomez (see note 16).
[20] O. W. Barnett, C. L. Miller-Perrin, and R. D. Perrin, Family violence across the lifespan: An introduction (Thousand Oaks: Sage Publications, 1997); S. M. Stith, A. L. Busch, K. Lundeberg, and R. P. Carlton, “The intergenerational transmission of spouse abuse: A meta-analysis,” Journal of Marriage and Family 62/3 (2000), pp. 640–654; K. M. Kitzmann, N. K. Gaylord, A. R. Holt, and E. D. Kenny, “Child witnesses to domestic violence,” Journal of Consulting and Clinical Psychology 71/2 (2003), pp. 339–352.
[21] World Health Organization, WHO report on violence and health (Geneva: World Health Organization, 2002).
[22] World Health Organization, Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence (Geneva: World Health Organization, 2013).
[23] Ibid.
[24] L. Stark, L. Roberts, W. Wheaton, et al., “Measuring violence against women amidst war and displacement in northern Uganda using the ‘neighborhood method,’” Journal of Epidemiology and Community Health 64/12 (2010), pp. 1056–1061.
[25] Ibid.; M. Hynes, K. Robertson, J. Ward, and C. Crouse, “A determination of the prevalence of gender‐based violence among conflict‐affected populations in East Timor,” Disasters 28/3 (2004), pp. 294–321; A. Peterman, T. Palermo, and C. Bredenkamp, “Estimates and determinants of sexual violence against women in the Democratic Republic of Congo,” American Journal of Public Health 101/6 (2011), pp. 1060–1067; P. Parmar, P. Agrawal, P. Gregg Greenough, et al., “Sexual violence among host and refugee population in djohong district, Eastern Cameroon,” Global Public Health 7/9 (2012), pp. 974–994.
[26] L. Stark and A. Ager, “A systematic review of prevalence studies of gender-based violence in complex emergencies,” Trauma, Violence and Abuse 12/3 (2011), pp. 127–134; Peterman et al. (see note 25); Parmar et al. (see note 25).
[27] Gallegos and Gutierrez (see note 15); Janko et al. (see note 15).
[28] J. Kelly, E. Colantuoni, C. Robinson, and M. R. Decker, “From the battlefield to the bedroom: A multilevel analysis of the links between political conflict and intimate partner violence in Liberia,” BMJ Global Health 3/2 (2018); Jocelyn Kelly, E. Colantuoni, C. Robinson, and M. R. Decker, “From political to personal violence: Links between conflict and non-partner physical violence in post-conflict Liberia,” Global Public Health 14/12 (2019), pp. 1639–1652.
[29] Peace Insight, Liberia: Conflict and peace (2014). Available at https://www.peaceinsight.org/conflicts/liberia/.
[30] “Security Council extends UN peace mission in Liberia for another year,” UN News (September 18, 2013). Available at http://www.un.org/apps/news/story.asp?NewsID=45888#.V-0vgvkrLIU.
[31] British Broadcasting Corporation News, Liberia country profile (2020). Available at https://www.bbc.com/news/world-africa-13729504; Central Intelligence Agency, World factbook Liberia country profile (2020). Available at https://www.cia.gov/library/publications/the-world-factbook/geos/li.html.
[32] K. Johnson, J. Asher, S. Kayden, and A. Raja, “Association of combatant status and sexual violence with health and mental health outcomes in post conflict Liberia,” JAMA : The Journal of the American Medical Association 300/6 (2008), pp. 676–690.
[33] C. Raleigh, A. Linke, H. Hegre, and J. Karlsen, et al., “Introducing ACLED: An armed conflict location and event dataset,” Journal of Peace Research 47/5 (2010), pp. 651–660.
[34] World Health Organization, Violence against women prevalence estimates, 2018: Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women (Geneva: World Health Organization, 2021), p. 6.
[35] B. Sabri, L. M. Renner, J. K. Stockman, et al., “Risk factors for severe intimate partner violence and violence-related injuries among women in India,” Women and Health 54/4 (2014), pp. 281–300.
[36] Raleigh and Dowd (see note 2).
[37] Ibid.
[38] Kelly et al. (2018, see note 28); Kelly et al. (2019, see note 28).
[39] S. Rabe-Hesketh, A. Pickles, and A. Skrondal, “GLLAMM: A general class of multilevel models and a STATA programme,” Multilevel Modelling Newsletter 13/1 (2001).
[40] C. Cullen, Method matters: Underreporting of intimate partner violence in Nigeria and Rwanda, Working Paper (Washington, DC: World Bank, 2020); N. Metheny and R. Stephenson, “Interviewer effects on the reporting of intimate partner violence in the 2015 Zimbabwe demographic and heath survey,” Journal of Gender-Based Violence 4/2 (2020), pp. 241–258.
[41] Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948).
[42] World Health Organization (2002, see note 21); World Health Organization (2013, see note 22).
[43] Declaration on the Elimination of Violence against Women, G.A. Res. 48/104 (1993).
[44] E. J. Wood, “Sexual violence during war: Variation and accountability,” in A. Smeulers (ed), Collective crimes and international criminal justice: An interdisciplinary approach (Antwerp: Intersentia, 2010); E. J. Wood, “Armed groups and sexual violence: When is wartime rape rare?,” Politics and Society 37/1 (2009), pp. 131–161.
[45] Stark et al. (see note 24); Hynes et al. (see note 25); Peterman (see note 25); Parmar et al. (see note 25).
[46] R. Saile, F. Neuner, V. Ertl, and C. Catani, “Prevalence and predictors of partner violence against women in the aftermath of war: A survey among couples in Northern Uganda,” Social Science and Medicine 86 (2013), pp. 17–25; K. L. Falb, M. C. McCormick, D. Hemenway, et al., “Violence against refugee women along the Thai–Burma border,” International Journal of Gynecology and Obstetrics 120/3 (2013), pp. 279–283; J. Gupta, E. Reed, J. Kelly, et al., “Men’s exposure to human rights violations and relations with perpetration of intimate partner violence in South Africa,” Journal of Epidemiology and Community Health 66/6 (2012); P. Vinck and P. N. Pham, “Association of exposure to intimate-partner physical violence and potentially traumatic war-related events with mental health in Liberia,” Social Science and Medicine 77 (2013), pp. 41–49.
[47] Thoms and Ron (see note 14).
[48] S. Gruskin, “Violence or health?,” American Journal of Public Health 93/7 (2003).
[49] Thoms and Ron (see note 14).
[50] Kelly et al. (2018, see note 28); Kelly et al. (2019, see note 28).