Is Mandatory Vaccination for COVID-19 Constitutional under Brazilian Law?
Volume 23/1, June 2021, pp. 163-174
Daniel Wei Liang Wang, Gabriela Moribe, and Ana Luiza Gajardoni de M. Arruda
Abstract
Mandatory vaccination for COVID-19 has been the object of heated debate in Brazil. This article discusses the legality and constitutionality of such a policy. First, it analyzes the laws, regulations, and Supreme Court decisions that provide for the possibility of mandatory COVID-19 vaccination. Subsequently, it analyzes the constitutionality of a mandatory vaccination policy through the proportionality method to address the conflict between, on one side, the right to individual autonomy, which includes the right to refuse a medical intervention, and, on the other, health policies that interfere with individual autonomy to protect the rights to life and health. The application of this method allows for the identification of key questions that need to be answered to determine the constitutionality of a mandatory vaccination program. These questions cannot be answered a priori and in the abstract because they depend on the concrete circumstances of the pandemic, on the characteristics of the vaccine(s) against COVID-19, and on how a mandatory vaccination policy might be designed and implemented by authorities.
Introduction
The devastating effects of COVID-19 on public health are well known, especially when the necessary social distancing measures are not taken to avoid contagion. It is also clear that strict social distancing measures have significant impacts on the economy, people’s freedom, the education of children and adolescents, and the physical and mental health of the population.
The development of effective vaccines for COVID-19 offers the main route out of the present tragic bind. Effective vaccines can help reduce COVID-19-related mortality and hospitalization. It is also hoped that mass vaccination will help achieve herd immunity (also called “community protection” or “population immunity”), which is defined as the immunization of a sufficiently large portion of the population, either by infection or vaccination, to control the epidemic in a given location to the point of preventing major outbreaks.1
Vaccines pose dilemmas and difficult choices of their own. The first is related to the distribution of vaccines at the global level. Production capacity is still insufficient to meet global demand and—because the existing vaccines are mainly distributed through market mechanisms—access has been mostly restricted to the countries with the greatest purchasing power. This economic disparity can be mitigated by global aid and initiatives such as COVAX, led by the World Health Organization, which brings together most of the world’s countries to facilitate the development of vaccines and their equitable distribution among participants.2
The challenges of global justice are followed by others at the national level in terms of whom to prioritize for vaccination: health professionals, other essential workers, people in high-risk groups, or those living in areas with high degrees of contagion?3
Prioritization guidelines have already been proposed to address scenarios of scarcity.4
If the issues of access and distribution are solved, the next debate may well concern vaccine mandates. Mandatory COVID-19 vaccination has been discussed in the specialist literature and is being considered for specific groups, such as workers in older adult care homes in England, and determined for others, such as health care workers in Italy.5 To our knowledge, mandatory COVID-19 vaccination for the general population has not been implemented anywhere. Yet, in Brazil, compulsory COVID-19 vaccination for the general population is expressly authorized by the federal legislation that entered into force in March 2020, which was upheld by the Supreme Court in December 2020.
Brazil has a history of successful immunization policies, having served as a benchmark for other countries during many years. The universal access to vaccines from the 1970s onwards led to the eradication of polio and to the reduction in cases of measles, whooping cough, tetanus, and tuberculosis.6 However, the drop in vaccine coverage in recent years, coupled with declarations by President Bolsonaro that promote vaccine hesitancy, have raised concerns that voluntary vaccine uptake for COVID-19 may be low.7 It is against this backdrop that debates about mandatory COVID-19 vaccination gained momentum in October 2020, when the governor of São Paulo, João Dória, declared that vaccination would be mandatory in his state and President Jair Bolsonaro immediately took a contrary stance to it.8 Mandatory vaccination is by no means a new debate in Brazil, and it is worth recalling the historical and symbolic importance of the Brazilian “vaccine riots” (revolta da vacina) that broke out in response to mandatory smallpox vaccine legislation at the beginning of the 20th century.9
Compulsory vaccination raises difficult issues due to the direct clash between, on one side, the autonomy of individuals to decide about their own bodies, which includes the right to refuse medical interventions, and, on the other, the imperative to protect public health, which may require restricting individual liberties to avoid disease and protect life in the population. There is a vast literature on this topic, but, for reasons of scope, this paper will not engage with it in depth. We will simply start from the proposition that freedom cannot be absolute when an individual’s choices make him or her a potential vector of illness and death to others, and that any restriction on individual freedom needs to be justified and proportional to the desired public health gains.10
The tension between individual freedom and public health has been recognized in international human rights law documents—for example, the European Convention on Human Rights, the American Convention on Human Rights, and the Siracusa Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights—that accept restrictions on some civil rights if necessary to protect health. This tension has certainly been accentuated by the COVID-19 pandemic and the public measures to contain it.
This article offers a legal analysis of the possibility of the state making vaccination against COVID-19 mandatory. Although no legal analysis can ever be completely dissociated from ethical and political considerations, legal norms and problem-solving methods should be known and analyzed since, ultimately, they will determine whether vaccination against COVID-19 can be mandated. Rather than proposing a definitive position on the topic, this article argues that it is impossible to give an a priori and abstract legal response to the conflict between the claims of individual autonomy and public health. An adequate response will depend on the concrete circumstances of the pandemic, the characteristics of the COVID-19 vaccine(s), and how any mandatory vaccination policy might be designed and implemented by authorities. Although the paper focuses on the case of Brazil, our analysis should contribute to debates in other jurisdictions where mandatory vaccination is being or will be considered to tackle the COVID-19 pandemic.
Mandatory vaccination under Brazilian law
In this paper, mandatory vaccination is understood as the legal obligation to receive a vaccine or to take minors under one’s care to receive a vaccine. There may be legal sanctions for non-compliers, but, as will be discussed below, mandatory vaccination does not necessarily imply that people will be forced to vaccinate. By way of comparison, mandatory voting does not allow the state to drag people to a ballot box.
Mandatory vaccination exists in several countries, although it varies widely in terms of scope (in other words, which vaccines are mandated), reach (it may be general or targeted at children, risk groups, or health professionals), the types and intensity of sanctions (including fines, the loss of social benefits, and criminal sanctions), and the possibility of opting out (whether for religious, philosophical, or medical reasons).11
Mandatory vaccination has been provided for in Brazilian law. The first instance was Federal Law 1.261/1904, which made the smallpox immunization mandatory at the beginning of the 20th century and led to the famous vaccine riots. Regarding the legislation currently in force, an important part of it dates from the 1970s, when the National Immunization Program was created. Federal Law 6.259/1975 establishes the following:
Art. 3. The Ministry of Health is responsible for creating the National Immunization Program, which will define vaccinations, including mandatory ones.
Sole paragraph. Mandatory vaccinations will be provided systematically and free of charge by public bodies and entities, as well as by private entities subsidized by the Federal, State and Municipal Governments, throughout the national territory …
Art. 6. The state governments, subsequent to consultation with the Ministry of Health, may propose complementary legislative measures aiming at the provision of compulsory vaccinations to parts of the population, within the scope of their territories.
Federal Decree 78.231/1976, which regulates Federal Law 6.259/1975, sets forth the obligation of the Ministry of Health to draw up the National Immunization Program listing mandatory vaccines; allocates responsibilities for the execution of the vaccination program; and affirms the “duty of every citizen to submit himself and the minors under his custody or responsibility for mandatory vaccination.” The decree provides for cases in which there is an explicit medical contraindication proven by a medical certificate as the only allowed exemption from the vaccine mandate. Federal Law 6.347/1977 lists as a sanitary infraction “hindering or opposing the execution of sanitary measures aimed at the prevention of contagious diseases and their dissemination, and at the preservation and maintenance of [public] health.”
The list of vaccines that make up the National Immunization Program is updated periodically through ordinances issued by the Ministry of Health. The first list was established by Ministry of Health Ordinance 452/1977, mandating immunization against tuberculosis, polio, measles, diphtheria, tetanus, and whooping cough for infants under one year of age.
In 2004, Ordinance 597/2004 determined that all vaccines listed in the National Immunization Program were mandatory. In terms of enforcement, the presentation of a certificate proving that a person received all the vaccines became mandatory for receiving social benefits; for nursery, school, and university enrollment; for military conscription (military service is compulsory for 18-year-old men); and for signing work contracts in the public or private sector. These provisions were revoked by Ordinance 1.602/2006, which updated the list of vaccines but excluded any explicit mention of mandatory vaccination. Subsequent ordinances have not made vaccination mandatory for the general population either.
Vaccination is currently mandatory in Brazil for specific groups only. Ministry of Defense Ordinance 94/2020, which creates a specific list of vaccines for military personnel, determines that immunization is mandatory for this group. The obligation to vaccinate children was established by Federal Law 8.069/1990, which, in article 14(1), states that “vaccination of children is mandatory in the cases recommended by the health authorities.” Federal Law 8.069 of 1990 defines children as those under the age of 12, and establishes that the vaccines recommended for children would be defined by Ministry of Health ordinances. Mandatory vaccination with respect to minors also appears in other laws that create mechanisms to enforce it. For example, Federal Law 10.836/2004, which created the “Bolsa Família” Program (a cash transfer program for low-income families), established “health monitoring” as a condition for receiving this social benefit. According to Federal Decree 5.209/2004, this includes vaccination. São Paulo State Law 17.252/2020 makes it compulsory to present an up-to-date vaccination certificate for all students aged up to 18 years upon enrollment at any of the schools in the state. Other municipalities and states across the country also provide for this obligation.
Finally, and more specifically related to COVID-19, Federal Law 13.979/2020 establishes:
Art. 3. To respond to the public health emergency of international importance referred to in this Law, the authorities may adopt, within the scope of their competencies, among others, the following measures: …
III – determination of the compulsory undertaking of: …
- d) vaccination and other prophylactic measures; …
- 1. The measures provided for in this article can only be determined on the basis of scientific evidence and the analysis of strategic health information and must be limited in time and space to the minimum necessary for the promotion and preservation of public health.
Therefore, there are legal provisions in force, including primary legislation, allowing mandatory vaccination in Brazil, but this has mostly been implemented for specific groups only. In the case of COVID-19, although further regulation may establish more strict conditions, the current law gives the state quite broad powers to compel the population to vaccinate while the pandemic lasts by not specifying any specific target groups.
However, the mere legal provision for a vaccine mandate does not completely resolve the legal issue. Clarification is needed as to whether a mandatory vaccination program for COVID-19 is constitutional—in other words, whether it is compatible with the Brazilian Federal Constitution, the highest law in Brazil.
Mandatory vaccination according to Supreme Court case law
The nonconsensual administration of medical treatment raises difficult legal issues, as it is a serious interference with human rights such as the right to bodily autonomy. When, or if, it is legally permissible will normally depend on the group for which it is proposed.
Under Brazilian law, children under the age of 12 are not considered to be fully competent to make autonomous decisions, although their wishes and preferences should be considered. Decisions may therefore be imposed on them when in their best interests, even if a decision is contrary to the manifest wishes of the person herself or of her parents or guardians. There may be disputes as to what is best for the child, but, with regard to vaccination, the choice has already been made by the law insofar as vaccination is mandated.
There are instances of legal proceedings against parents who refuse to vaccinate their children, and one of them reached the Supreme Court (Supremo Tribunal Federal, or STF), the highest court in Brazil, through Extraordinary Appeal 1267879. This case involved parents who claimed the right not to vaccinate their children on the basis of their philosophical convictions and the alleged risks involved in vaccination. The STF issued a ruling in December 2020 concluding that mandatory immunization for children is constitutional if (i) it is prescribed by law, (ii) the vaccine has been approved by the national drug regulatory agency, and (iii) the vaccine is listed in the National Immunization Program or local-level immunization programs. According to the STF, if these conditions are met, then mandatory vaccination for children will not breach the freedom of thought and conscience of parents or those with parental responsibility.
The STF ratified what the law establishes in relation to children, whose best interests prevail over contrary wishes (even if expressed by parents or guardians). The court’s judgment is also in line with precedents of the Brazilian judiciary, which tends to reject the idea that parents’ philosophical or religious convictions can justify health care-related decisions that can harm their children, as shown by judgments authorizing the administration of treatments involving blood transfusions for children despite opposition from their Jehovah’s Witness parents.
However, the question of the constitutionality of mandatory vaccination for the general population, which includes adults with the capacity to consent, is more difficult because there is a direct clash with the individual autonomy of those who refuse to be vaccinated. Legislation and the Brazilian Federal Medical Council’s Code of Ethics recognize, with few exceptions (such as when the person lacks the capacity to decide for herself), that medical treatment can be given only if the person consents to it.12
Not acquiescing to an individual’s choice in order to protect her from harm raises concerns about paternalism. This is not the focus of this article because even though vaccination protects the individual, the dilemma that arises goes beyond the individual. Vaccination offers a benefit not only to the person who is immunized but also to the community. There is evidence that an immunized person is much less likely to spread COVID-19.13 In this sense, making a vaccination mandatory is a way of increasing its coverage and protecting those who for some reason cannot be immunized.14 The focus of this article is thus exclusively on the conflict between the individual autonomy to refuse a COVID-19 vaccine and the moral and legal imperative of protecting the most people possible from a highly contagious disease.
The constitutionality of provisions that allow mandatory vaccination for the general population had never been decided by the STF before December 2020. There is a decision—Habeas Corpus 71373-4, issued in 1994—in which several STF justices cited mandatory vaccination as an example of a situation in which the public interest may prevail over that of the individual. However, these comments were only obiter dicta, as mandatory vaccination was not the central issue in the case and was mentioned for mere illustrative purposes.
In 2020, this issue reached the STF through legal challenges against Law 13.9797/20, which, as mentioned above, allows authorities to require immunization for COVID-19. In December 2020, the STF ruled on cases ADI 6586 and ADI 6587 and concluded that the provisions in Law 13.979 are constitutional in principle. The court accepted that individual autonomy cannot be used as a trump against public health measures that promote the constitutionally protected right to health. The court also confirmed that local authorities at the state and municipal level can require COVID-19 if the federal government refuses to do so.
However, the STF clarified that a concrete policy mandating COVID-19 immunization needs to satisfy certain requirements. Non-compliers may be sanctioned, but in no circumstance may they be forcefully vaccinated, as this would breach their individual autonomy, bodily integrity, and human dignity; the decision to make vaccination mandatory must be informed by scientific evidence regarding the vaccines’ safety and efficacy and by strategic health information (such as epidemiological data and the existing policies to control the disease); there must be free and universal access to the COVID-19 vaccines; and the policy must respect human rights and satisfy the reasonableness and proportionality tests.
In sum, mandatory vaccination for COVID-19 is constitutional in principle, but the issue is far from settled since an actual mandate may still be unconstitutional depending on the concrete elements of such a policy. It is therefore necessary to further analyze the elements that should be considered when determining the constitutionality of a mandatory COVID-19 vaccine policy.
Mandatory vaccination and the proportionality test
The proportionality test is a commonly used method in law to resolve conflicts in which a fundamental right (such as the individual right to make decisions in relation to one’s own body) must be restricted in order to protect another (such as the right to life and health of others). This test aims to guarantee the greatest protection of a right with the least restriction on another.
The proportionality test was required by the aforementioned STF judgment. The STF also mentioned the reasonableness test, but, putting aside the details of the distinction between the reasonableness and the proportionality tests, it is generally agreed that the latter is more intensive in scrutinizing the merits of a policy than the former.15 Therefore, a policy that is proportionate is almost certain to be reasonable, but the opposite is not necessarily true. As shown below, the structure of the proportionality test also allows the analysis of the other requirements mentioned by the STF. Moreover, because the proportionality test is widely used by constitutional and international courts, focusing on this method will allow this paper to offer a direct contribution to debates in other jurisdictions where mandatory vaccination for COVID-19 may be considered.16
There are variations in the application of the proportionality test, but the structure and rationale are recognizable across different jurisdictions. This paper adopts the original and one of the most widespread versions of this method (which is also the one adopted by Brazilian courts), which consists of three subtests: suitability, necessity, and proportionality in the strict sense.17 A measure can be proportional and, consequently, constitutional, only if it satisfies all three subtests.
Suitability
The suitability test requires that a measure that restricts a fundamental right contribute to promoting another right—in other words, it requires that there be a rational connection between means and ends. In the case under analysis, is mandatory vaccination (which is a direct restriction on the autonomy of individuals to refuse a medical intervention) suitable to promote health protection (which promotes mainly the rights to health and life)? The answer for the suitability test here is apparently easy given that vaccination is an effective measure for containing the pandemic and there is solid evidence that mandates may increase vaccine uptake.18
However, the specific case of vaccination against COVID-19 presents peculiarities that make the analysis more complex when compared to immunization with vaccines that have been long used for diseases that are better understood. There is, of course, a great deal of haste to develop a vaccine, and the international scientific community has already expressed concern about the risk of losing scientific rigor due to the premature administration of vaccines.19 In Russia, for example, vaccines began to be applied before phase III clinical trials were concluded.20 The results of phase III trials, in which the vaccine is tested on a large number of volunteers, are normally required to obtain registration before health authorities. Other countries have started their campaigns with vaccines that have gone through phase III trials but that were approved for emergency use only—that is, before full marketing approval.
There are good reasons for allowing and encouraging people to voluntarily receive vaccines for which there is still some uncertainty about efficacy and safety. However, without robust evidence that a vaccine is effective and safe, the argument for restricting individual autonomy by making vaccination mandatory is weaker. The data for the COVID-19 vaccines currently in use in high-income countries are very encouraging, despite concerns about rare adverse events. However, many of the vaccines that are being or will be administered in middle- and low-income countries have not yet been approved by “stringent regulatory authorities,” as defined by the World Health Organization.21
One must also consider whether conditions exist for universal vaccination coverage.22 Mandatory vaccination without enough doses or infrastructure to reach the entirety of the population can generate distrust and controversy and can distort the priorities for the vaccine’s distribution. If universal coverage is not feasible, it makes more sense to prioritize based on clear and transparent criteria rather than to impose mandatory vaccination.
Finally, one must consider the risk that the mandate will end up fomenting resistance to the vaccine. Empirically, there is little evidence that this has occurred where mandatory vaccination has been implemented.23 On the contrary, as discussed, vaccination coverage tends to increase with mandates. Since the vaccine riots, Brazil has had no record of popular resistance to vaccination.24 In any case, this is a risk that needs to be considered.
Necessity
If mandatory vaccination passes the suitability test—that is, if there is evidence that it promotes the protection of public health—the next test is that of necessity. A measure is necessary when it is not possible to promote the same aim, to the same degree, by another less right-restrictive means. In other words, is it possible to achieve the public health result that is sought with mandatory vaccination, with the same intensity, through a means that is less restrictive of individual autonomy? The answer will depend fundamentally on the stage of the disease, the willingness of the population to be vaccinated voluntarily, and the alternatives to vaccination for preventing contagion.
Vaccine hesitancy is a serious challenge that may hamper COVID-19 vaccine uptake. There is huge variation in COVID-19 vaccine hesitancy across the world; in Brazil, the percentage of people who do not intend to get vaccinated is low when compared to other countries.25 This probably reflects the “culture of immunization” in Brazil, in which society accepts the need for and the importance of vaccination.26
To determine whether voluntary vaccination is sufficient (thus making mandatory vaccination unnecessary), it is important to consider the emerging evidence demonstrating that those who have already recovered from COVID-19 infection will acquire some form of durable immunity.27 If this is confirmed by further studies, then it is possible that the two groups combined—those who have already been infected and recovered and those who are willing to vaccinate voluntarily—will allow for the achievement of a sufficient level of community protection. This, of course, would depend on the analysis of other factors such as the rate of contagion of the disease and the effectiveness of the vaccine. The rate of contagion is affected by factors such as the profile of the population (age, co-morbidities, etc.) and their habits and their living conditions (housing, hygiene, etc.).28 Although the data suggest high or very high efficacy for many of the vaccines that have been tested, their efficacy will certainly not be 100%, and, therefore, not all those vaccinated will acquire immunity. As a rule, the higher the rate of contagion and the less effective the vaccine, the more people need to be vaccinated for herd immunity to be achieved. However, the lower the effectiveness, the lower the incentives for individuals to vaccinate voluntarily. This creates a problem of collective action that can make a vaccine mandate necessary.
It is also necessary to consider alternatives to vaccine mandates. For example, information campaigns, awareness-raising, and the removal of barriers to access (such as cost, location, and opening hours of vaccination sites) could avoid the three main obstacles to people getting vaccinated: distrust of the vaccine and of the purposes of the vaccination campaign; complacency regarding the risks of non-vaccination; and difficulty in accessing vaccination services.29
Nudge mechanisms should also be considered in order to change the choice architecture and increase the likelihood that people will choose to be vaccinated.30 Examples may include “immunization passports” so that others can identify people who have already been immunized, the creation of a mechanism that sends periodic alerts to individuals who have not yet been vaccinated, and cash prizes or other incentives for those who get vaccinated.31 These measures do not necessarily have to be alternatives to mandatory vaccination—they may coexist with it. The question, however, is whether it is possible to show with any degree of plausibility that a vaccine mandate will still be necessary if some or all of these measures are implemented.
Even if we come to the conclusion that a mandate is necessary, we must consider whether targeting certain groups (for example, those at high risk of contagion, of infecting others, or of dying in the case of contagion) could be an alternative to a general mandate. This is an option to be assessed in light of the concrete circumstances of the epidemic and of the characteristics of the vaccine(s) when (or if) the time comes to make such a policy.
Finally, it will be necessary to assess whether it is possible to achieve the aim of containing the pandemic through alternative measures to vaccination, such as mass tests, contact tracing, quarantine measures, social distancing, and so on. Even if this set of measures is equally capable of promoting this aim, we must consider whether such measures would be more or less restrictive of rights than mandatory vaccination. This leads us to the third test, discussed below.
Proportionality in the strict sense
Even where a mandate is suitable and necessary, it must also be proportional in the strict sense, which is to say that there must be a balance between the intensity of the restriction of a right and the gains made for the other right(s) with which it collides. Therefore, mandatory COVID-19 vaccination will be proportional in the strict sense only if the interference with the individual autonomy to refuse treatment is justified by the gains in the protection of the rights to health and life.
We must then consider what is lost in individual autonomy due to the obligation to be vaccinated against what is lost due to the pandemic or social distancing measures when these are imposed. The pandemic causes enormous losses in terms of mortality and morbidity, in addition to the massive financial and opportunity costs to the health system. This diverts financial and human resources that could be used to care for other diseases and patients.32 In other words, the absence (or insufficiency) of state intervention to promote public health and thus reduce the risk of harm to individuals also interferes with rights.33
The pandemic can be, to a certain extent, controlled through social distancing measures. However, such measures on their intensity and duration, may be even more limiting to a series of individual rights (such as the freedom of movement, freedom of association, and economic freedom) than the obligation to get a vaccine. In addition, social distancing measures have serious deleterious effects, such as on people’s physical and mental health, the right to education of children and young people, and the economy.34
Let us consider three scenarios. In the first, there is mandatory vaccination, which restricts the individual autonomy to refuse treatment, but which controls the pandemic and makes harsh social distancing measures unnecessary. In the second, there is no mandatory vaccination, but the pandemic is contained by strict social distancing measures (such as long lockdowns), which protects the rights to health and life but imposes severe limits on individual liberties. In the third, there is neither mandatory vaccination nor social distancing measures, which needlessly aggravates the COVID-19 health crisis, causing excess morbidity and mortality. A careful analysis of the three scenarios, considering the concrete facts and the nature and intensity of the interference with the different rights involved, may lead to the conclusion that, overall, the first scenario is the one with the least restriction of fundamental rights.
If this is indeed the case, then mandatory vaccination will be proportional in the strict sense. What is lost by this restriction on individual autonomy to refuse treatment is offset by what is gained in rights terms when pandemic control is achieved without the need for harsh social distancing measures.35
Sanctions and exceptions
The result of the proportionality test will depend on the scope and severity of a given policy. Therefore, when applying the three subtests to a concrete COVID-19 vaccine mandate, one must pay attention to the sanctions that are provided for in cases of noncompliance and the provision (or lack thereof) of exceptions to the vaccine mandate.
Mandatory vaccination means that a person can be subject to sanctions if she does not fulfill this duty. Sanctions can vary widely in their type and intensity. Examples include warnings, fines (as applied in some Brazilian cities to people who do not use face masks in public spaces), the loss of benefits (for example, a government benefit such as the “Bolsa Família” program), restrictions on freedom of movement or association (for example, an obligation to be monitored or restricted access to places), and even criminal sanctions. It is possible that, in certain contexts, the mandatory vaccination itself is constitutional, but, in light of the proportionality method, some of the sanctions are not. The Brazilian Supreme Court has already ruled that non-compliers cannot be forcefully vaccinated and, in the same judgment, some justices mentioned in obiter that criminal sanctions are likely to be disproportionate.
Another question to be considered is whether the law should tolerate exceptions and allow some people to opt out of the vaccine mandate. Exceptions could be for medical reasons for those to whom the risk of side effects (for example, due to allergy) is much greater than for the rest of the population. This exception is already provided for in article 29 of Federal Decree 78.231/1976: “Only persons who present a medical certificate explicitly informing a contraindication to the vaccine will be exempted from mandatory vaccination.” For these people, measures that promote herd immunity are highly protective of their lives and their freedom. On the other hand, forcing them to get vaccinated is probably disproportionate given the risk it presents to them.
Exceptions for nonmedical reasons are more controversial. Exceptions to the mandatory vaccination of children due to philosophical or religious views held by their parents are contemplated in places as Canada, Indonesia, Australia, and several US states.36 In Brazil, as previously mentioned, the STF has held that parents who are philosophically opposed to vaccines are still obliged to have their children vaccinated. The question of whether an adult can reject treatment for religious reasons was also referred to the STF in two cases dealing with blood transfusions refused by Jehovah’s Witnesses, but these cases have not been decided yet.37 These cases, however, are distinct from the question of vaccination because the balance therein is between the individual’s autonomy to refuse treatment and his or her right to life. In the case of vaccination, the conflict is between the individual’s autonomy and the rights of others.
For some people, a vaccine mandate may be an intense restriction on their freedom, including their freedom of religion and thought. However, following the logic of the proportionality method, the constitutionality of a vaccine mandate with very limited or no nonmedical exemptions will depend on the concrete circumstances, particularly the impact on the rights of others that may result from these exemptions.
It is important to note that there is evidence that people who oppose vaccination for religious or personal reasons tend to be concentrated in certain locations, meaning that such exceptions can generate localized epidemic outbreaks.38 In the case of diseases as contagious as COVID-19, this could have serious widespread implications. If this phenomenon is observed or expected, there is even greater justification for limiting or excluding nonmedical exceptions.
Conclusion
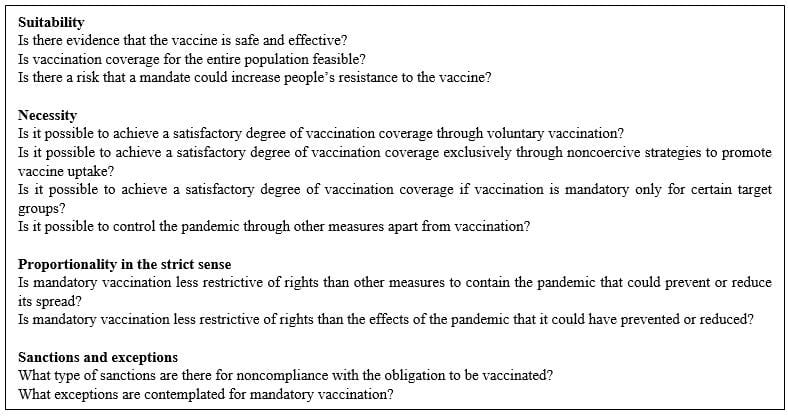
Whether a mandatory vaccination policy is constitutional will depend on the answers to some key questions in the application of the proportionality method (see Table 1). These questions can guide constitutionality reviews undertaken by the judiciary and help the executive and legislative branches formulate policies in a more transparent, informed, and balanced way, giving due weight to fundamental rights. The analysis in this text reinforces the view that the constitutionality of mandatory vaccination cannot be answered a priori and in the abstract. Any answer depends on the assessment of the actual facts when (and if) such a decision is made. This means that constitutionality can vary over time. An unconstitutional policy can become constitutional and return to being unconstitutional in light of new information or a change in context.
Table 1. Key questions for assessing the proportionality of mandatory vaccination
This paper has focused mainly on substantive issues related to the constitutionality of mandatory vaccination. Yet there are also institutional questions that are key to a court decision on this topic. Should the judiciary, in reviewing a mandatory requirement, have a more activist role in scrutinizing facts and policy considerations to impose what it considers the correct answer to these key questions, or, alternatively, should it grant the executive or the legislative branches a wider margin of discretion on these issues? An in-depth analysis of this question is beyond the scope of this article, but courts will have to engage with concerns about the limits of their institutional capacity to decide on issues that require the assessment of complex social facts and scientific information. This is all the more important considering that there will likely be reasonable disagreements over the answer to many of the key questions and that the evidence needed to decide on some matters may be inconclusive.
Acknowledgments
We thank Virgilio Afonso da Silva and the three anonymous reviewers for their insightful comments and suggestions on earlier versions of this paper. This research was supported by the São Paulo Research Foundation (grant no. 2019/15565-0). Gabriela Moribe and Ana Luiza Arruda are recipients of the Mário Henrique Simonsen scholarship. Ana Luiza Arruda is also supported by the São Paulo Research Foundation (grant no. 2020/00463-4).
Daniel Wei Liang Wang, LLM, MSc, PhD, is an Associate Professor at Fundação Getúlio Vargas Law School, São Paulo, Brazil.
Gabriela Moribe is a master in law and development candidate at Fundação Getúlio Vargas Law School, São Paulo, Brazil.
Ana Luiza Gajardoni de M. Arruda is a master in law and development candidate at Fundação Getúlio Vargas Law School, São Paulo, Brazil.
Please address correspondence to Daniel Wei Liang Wang. Email: daniel.wang@fgv.br.
Competing interests: None declared.
Copyright © 2021 Wang, Moribe, and Arruda. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction.
References
1. A. Fontanet and S. Cauchemez, “COVID-19 herd immunity: Where are we?,”Nature Reviews Immunology20/10 (2020), pp. 583–584.
2. GAVI The Vaccine Alliance, COVAX explained (September 2020). Available at https://www.gavi.org/vaccineswork/covax-explained.
3. E. J. Emanuel, G. Persad, R. Upshur, et al., “Fair allocation of scarce medical resources in the time of Covid-19,” New England Journal of Medicine 382/21 (2020), pp. 2049–2055; A. Giubilini, J. Savulescu, and D. Wilkinson, “COVID-19 vaccine: Vaccinate the young to protect the old?,” Journal of Law and the Biosciences (2020).
4. World Health Organization, WHO SAGE roadmap for prioritizing uses of COVID-19 vaccines in the context of limited supply (November 2020). Available at https://www.who.int/docs/default-source/immunization/sage/covid/sage-prioritization-roadmap-covid19 vaccines.pdf?Status=Temp&sfvrsn=bf227443_2%20;%20https://www.cdc.gov/vaccines/imz-managers/downloads/COVID-19-Vaccination-Program-Interim_Playbook.pdf.
5. L. O. Gostin, D. A. Salmon, and H. J. Larson, “Mandating COVID-19 vaccines,” JAMA 325/6 (2021), pp. 532–533; J. Savulescu, “Good reasons to vaccinate: Mandatory or payment for risk?,” Journal of Medical Ethics 47/2 (2021), p. 78; D. R. Reiss and A. L. Caplan, “Considerations in mandating a new Covid-19 vaccine in the USA for children and adults,” Journal of Law and the Biosciences 7/l (2020); UK Department of Health and Social Care, Open consultation making vaccination a condition of deployment in older adult care homes (April 14, 2021). Available at https://www.gov.uk/government/consultations/making-vaccination-a-condition-of-deployment-in-older-adult-care-homes/making-vaccination-a-condition-of-deployment-in-older-adult-care-homes; M. Paterlini, “Covid-19: Italy makes vaccination mandatory for healthcare workers,” BMJ 373 (2021), p. 905.
6. Brazilian Ministry of Health, Programa Nacional de Imunizações 30 anos (2003). Available at https://bvsms.saude.gov.br/bvs/publicacoes/livro_30_anos_pni.pdf.
7. C. M. A. S. Domingues, A. G. K. Maranhão, A. M. Teixeira, et al., “The Brazilian National Immunization Program: 46 years of achievements and challenges,” Cadernos de Saúde Pública (2020).
8. “Bolsonaro já disse que não tomaria vacina contra Covid e ‘ponto final’,” G1 (March 23, 2021). Available at https://g1.globo.com/politica/noticia/2021/03/26/bolsonaro-ja-disse-que-nao-tomaria-vacina-contra-covid-e-ponto-final-video.ghtml; “Bolsonaro: ‘Vacina não será obrigatória e ponto final’,” CNN (October 19, 2020). Available at https://www.cnnbrasil.com.br/saude/2020/10/19/bolsonaro-vacina-nao-sera-obrigatoria-e-ponto-final.
9. G. Hochman, “Vacinação, varíola e uma cultura da imunização no Brasil,” Ciência & Saúde Coletiva 16/2 (2011), pp. 375–386.
10. J. Brennan, “A libertarian case for mandatory vaccination,” Journal of Medical Ethics 44/1 (2018), p. 37; J. Wilson, “The right to public health,” Journal of Medical Ethics 42/6 (2016), p. 367.
11. S. H. E. Harmon, D. E. Faour, N. E. MacDonald, et al., “Immunization governance: Mandatory immunization in 28 Global NITAG Network countries,” Vaccine 38/46 (2020), pp. 7258–7267; E. Cave, “Voluntary vaccination: The pandemic effect,” Legal Studies (Society of Legal Scholars) 37/2 (2017), pp. 279–304; N. E. MacDonald, S. Harmon, E. Dube, et al., “Mandatory infant and childhood immunization: Rationales, issues and knowledge gaps,” Vaccine 36/39 (2018), pp. 5811–5818; K. Attwell and M. C Navin, “Childhood vaccination mandates: Scope, sanctions, severity, selectivity, and salience,” Milbank Quarterly (2019).
12. For an in-depth discussion on COVID-19 vaccination for people who lack the capacity to consent, see the England and Wales Court of Protection decisions in E v. London Borough of Hammersmith and Fulham [2021] EWCOP 7; SD v. Royal Borough of Kensington And Chelsea [2021] EWCOP 14; CR v. NHS Tameside & Glossop CCG [2021] EWCOP 19.
13. M. Voysey, S. A. C. Clemens, S. A. Madhi, et al., “Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: A pooled analysis of four randomised trials,” Lancet 397/10277 (2021), pp. 881–891.
14. Macdonald et al. (see note 11); S. Arora, J. Morris, and A. J. Jacobs, “Refusal of vaccination: A Test To Balance Societal And Individual Interests,” Journal of Clinical Ethics 29/3 (2018), pp. 206–216.
15. J. Mathews, “Reasonableness and proportionality,” The Oxford Handbook of Comparative Administrative Law (2020). Available at https://www.oxfordhandbooks.com/view/10.1093/oxfordhb/9780198799986.001.0001/oxfordhb-9780198799986-e-51.
16. K. Möller, “Proportionality: Challenging the critics,” International Journal of Constitutional Law 10/3 (2012), pp. 709–731.
17. V. A. da Silva, “How global is global constitutionalism? Comments on Kai Moller’s The Global Model of Constitutional Rights,” Jerusalem Review of Legal Studies 10/1 (2014), pp. 175–186.
18. C. Lee and J. L. Robinson, “Systematic review of the effect of immunization mandates on uptake of routine childhood immunizations,” Journal of Infection 72/6 (2016), pp. 659–666; E. Galanakis, A. Jansen, P. L. Lopalco, and J. Giesecke, “Ethics of mandatory vaccination for healthcare workers,” Eurosurveillance 18/45 (2013), p. 20627; O. M. Vaz, M. K. Ellingson, P. Weiss, et al., “Mandatory vaccination in Europe,” Pediatrics 145/2 (2020), p. e20190620; F. D’Ancona, C. D’Amario, F. Maraglino, et al., “The law on compulsory vaccination in Italy: An update 2 years after the introduction,” Eurosurveillance 24/26 (2019), p. 1900371.
19. S. Jiang, “Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees,” Nature 579/7799 (2020), pp. 321–321.
20. E. Callaway, “Russia’s fast-track coronavirus vaccine draws outrage over safety,” Nature 584/7821 (2020), pp. 334–335.
21. O. J. Wouters, K. C. Shadlen, M. Salcher-Konrad, et al., “Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment,” Lancet 397/10278 (2021), pp. 1023–1034.
22. M. M. Mello, R. D. Silverman, and S. B. Omer, “Ensuring uptake of vaccines against SARS-CoV-2,” New England Journal of Medicine 383/14 (2020), pp. 1296–1299.
23. Macdonald et al. (see note 11); D’Ancona et al. (see note 18).
24. R. Zorzetto, “As razões da queda na vacinação,” Revista Pesquisa FAPESP 270 (August 2018). Available at https://revistapesquisa.fapesp.br/as-razoes-da-queda-na-vacinacao/.
25. Wouters et al. (see note 21).
26. Domingues et al. (see note 7).
27. J. M. Dan, J. Mateus, Y. Kato, et al., “Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection,” Science 371/6529 (2021), p. eabf4063.
28. H. E. Randolph and L. B. Barreiro, “Herd immunity: Understanding COVID-19,” Immunity 52/5 (2020), pp. 737–741; T. Britton, F. Ball, and P. Trapman, “A mathematical model reveals the influence of population heterogeneity on herd immunity to SARS-CoV-2,” Science 369/6505 (2020), p. 846.
29. N. T. Brewer, G. B. Chapman, A. J. Rothman, et al., “Increasing vaccination: Putting psychological science into action,” Psychological Science in the Public Interest 18/3 (2017), pp. 149–207.
30. S. Neumann-Böhme, N. E. Varghese, I. Sabat, et al., “Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19,” European Journal of Health Economics 21/7 (2020), pp. 977–982.
31. A. Dubov and C. Phung, “Nudges or mandates? The ethics of mandatory flu vaccination,” Vaccine 33/22 (2015), pp. 2530–2535; N. G. Mankiw, “Pay people to get vaccinated,” New York Times (September 2020). Available at https://www.nytimes.com/2020/09/09/business/pay-people-vaccine-coronavirus.html.
32. M. Douglas, S. V. Katikireddi, M. Taulbut, et al., “Mitigating the wider health effects of covid-19 pandemic response,” BMJ 369 (2020), p. m1557.
33. J. Wilson, “The right to public health,” Journal of Medical Ethics 42/6 (2016), p. 367.
34. T. Douglas, L. Forsberg, and J. Pugh, “Compulsory medical intervention versus external constraint in pandemic control,” Journal of Medical Ethics (2020), p. medethics-2020-106435.
35. For an ethical argument on why compulsory treatment and vaccination for COVID-19 that interferes with body integrity is not more problematic than external constraints on liberty, see Douglas et al. (see note 32).
36. S. B. Omer, D. A. Salmon, W. A. Orenstein, et al., “Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases,” New England Journal of Medicine 360/19 (2009), pp. 1981–1988; Attwell and Navin (see note 11); Harmon et al. (see note 11).
37. Supremo Tribunal Federal, Arguição de Descumprimento de Preceito Fundamental: ADF 618 (2020). Available at http://portal.stf.jus.br/processos/detalhe.asp?incidente=5769402; Superior Tribunal de Justiça, Recurso Especial: RE 1.212.272 RS (2011). Available at https://processo.stj.jus.br/processo/revista/documento/mediado/?componente=MON&sequencial=14962545&tipo_documento=documento&num_registro=201001751868&data=20110425&formato=PDF.
38. National Conference of State Legislatures, States with religious and philosophical exemptions from school immunization requirements (January 2021). Available at https://www.ncsl.org/research/health/school-immunization-exemption-state-laws.aspx; Omer et al. (see note 36).