Community Mobilization to Promote and Protect the Sexual and Reproductive Rights of Women Living with HIV in Latin America
Volume 22/2, December 2020, pp. 213 – 226
Tamil Kendall, Jimena Avalos Capin, Nazneen Damji, and Eugenia Lopez Uribe
Abstract
Between 2009 and 2014, the International Community of Women Living with HIV in Latin America and the Mexican feminist civil society organization Balance coordinated a five-country community-led intervention that brought together women living with HIV (WLHIV), trans women, sex workers, and feminist lawyers to document and respond to sexual and reproductive health and rights (SRHR) violations of WLHIV and advocate for legal, policy, and programmatic changes to fulfill SRHR. The experiences of involved community leaders (n=26) indicate that knowledge of national, regional, and international human rights commitments and up-to-date medical information positively influenced personal health behaviors, empowered WLHIV as subject matter experts, and emboldened them to hold duty-bearers to account. The research evidence generated through collective action was critical for legitimating SRHR violations of WLHIV with decision-makers and for positioning the issue in the advocacy agendas of national and regional HIV and women’s movements. Collective action contributed to social cohesion among diverse groups of women living with and affected by HIV and increased available technical, financial, and organizational resources and political opportunities by linking organizations and networks. Collectively, community leaders mobilized to influence policy, legal frameworks, and service delivery to promote and protect the SRHR of WLHIV.
Introduction
UNAIDS recently stated that the Sustainable Development Goals—including ending the HIV and AIDS pandemic—will not be achieved without advancing women’s full enjoyment of their human rights, particularly to bodily autonomy and sexual and reproductive health and rights (SRHR).1 This recognition coincides with resurgent interest in community-led responses in HIV among international organizations and donors.2 There is also a growing body of evidence on the contributions of community mobilization to HIV prevention, treatment, and care among diverse groups of women.3 Approaches grounded in human rights and the meaningful involvement of people living with HIV have been identified as critical for responding to HIV and AIDS for more than 30 years and strongly advocated for by women living with HIV (WLHIV) as necessary to improve quality of life and well-being, and specifically to realize SRHR.4 Nevertheless, documentation and analysis of human rights-based, community-led initiatives to advance the SRHR of WLHIV is limited in the grey and peer-reviewed literature.5
From 2009 to 2014, the International Community of Women Living with HIV in Latin America (ICW-Latina) and the Mexican feminist nongovernmental organization Balance implemented community-led research, advocacy, and coalition-building to promote and protect the SRHR of WLHIV in five countries (El Salvador, Guatemala, Honduras, Mexico, and Nicaragua). The first section of this paper draws on interviews with participants, participant observation, and project documents to describe the development and evolution of this participatory community mobilization intervention and the collective action taken by participants to promote and protect the SRHR of WLHIV.
In the second section, we draw on concepts from the community mobilization literature to analyze interviews with participating community leaders about the individual and institutional effects of engaging in collective activities to promote and protect the SRHR of WLHIV. We analyze how gaining knowledge about SRHR and local, national, and regional human rights mechanisms and generating their own evidence about SRHR violations affected community leaders’ critical consciousness about SRHR, sense of agency, and internalization and ownership of human rights discourses.3 We also analyze the role of collective action for strengthening social cohesion (bonding social capital) and organizational networks and structures (linking and bridging social capital), as well as its consequences for advocacy efforts to promote and protect the SRHR of WLHIV.6
Methods
We conducted in-depth semi-structured interviews (n=26) with community leaders to explore the personal, professional, and organizational effects of participating in the community mobilization intervention to promote the SRHR of WLHIV. All community leaders who participated in the community mobilization and the interviews were women. In each country, interviewees included at least one feminist lawyer or leader of the national women’s movement, one sex worker, one trans woman, and one WLHIV affiliated with ICW-Latina (El Salvador n=4, Guatemala n=4, Honduras n=5, Mexico n=8, Nicaragua n=5). These categories can and do overlap, but for sampling purposes we treated them as discrete to ensure the inclusion of perspectives and experiences from the different subpopulations. Interviews were conducted between May 2014 and February 2015 by a research assistant who had not been involved in the intervention; they were conducted in Spanish over the telephone or by Skype, were recorded, and were then transcribed verbatim. We thematically coded the interviews using a combination of a priori codes (such as impact_personal, impact_professional, impact_funding, and coalitionbuilding) and inductive codes (such as appropriating SRHR and legal tools). Overt participant observation was conducted by Tamil Kendall during meetings and trainings (November 2009–December 2012). We also analyzed related project documents such as reports and meeting minutes. We managed data using the qualitative analysis package Atlas-ti 7.0. Ethics approval was granted by the Institutional Review Board of Harvard University (IRB14-1132) and the University of British Columbia Okanagan Behavioural Research Board (H09-00738).
The intervention: Taking collective action to promote and protect the SRHR of WLHIV
Background
In 2008, the International Community of Women Living with HIV (ICW) identified fulfilling SRHR as a global priority.7 At this time, in Latin America, the SRHR of WLHIV were not well integrated into national HIV plans and were not an advocacy priority for either the broader HIV or women’s movements. Moreover, despite the existence of ICW-Latina, WLHIV leaders at the national level were isolated and institutionally weak, with limited political and social capital to advance their priorities.8
From 2009 to 2014, ICW-Latina and Balance implemented a community-led intervention focused on promoting and protecting the SRHR of WLHIV. The initial phase of this community-led intervention (2009–2010) involved participatory prioritization, which is described in the community mobilization literature as the process of problem identification (or issue framing) and the development of critical consciousness.9 The second phase (2011–2014) refined the collective action frame—that is, the “action-oriented sets of beliefs and meanings that inspire and legitimate the activities and campaigns” of a social movement to focus on documenting SRHR violations experienced by WLHIV and responding using human rights mechanisms and legal strategies.10
The “what” and the “how” of collective action was developed collaboratively and evolved over time in response to the goals and aspirations of participants. The importance of a truly participatory process was expressed clearly by a participant who explained that what they most liked about the process of documenting SRHR violations was that “it wasn’t imposed. We validated [the data collection tool], we readapted it, and we reached consensus … because we were a bit fed up with everything coming from other countries and just being used” (interviewee 14).
The section below describes the implementation and evolution of the community mobilization intervention and shares the results of collective action identified by the participants.
Phase one of the intervention: Analyzing SRHR commitments and articulating gaps and priorities (2009–2010)
In 2009 and 2010, ICW-Latina and Balance convened week-long participatory workshops in El Salvador, Honduras, Guatemala, Mexico, and Nicaragua to build the capacity of WLHIV community leaders in the area of SRHR, identify advocacy priorities, and begin to work collaboratively on these priorities with national women’s organizations. International and regional guidelines and commitments relevant to the sexual and reproductive health of WLHIV were presented, and a content analysis of national HIV, reproductive health, and violence against women plans was discussed.11 The analysis identified that HIV was not well integrated into national reproductive health or violence plans and that national HIV plans did not consider comprehensive services to promote and protect the sexual and reproductive health of WLHIV, specifically the prevention and treatment of sexually transmitted infections (including human papillomavirus and cervical cancer), contraception, and information and services for safer conception; all plans identified the provision of antiretrovirals for the prevention of vertical (mother-to-child) transmission.12 When national plans included actions to promote sexual and reproductive health, ICW members identified gaps in service delivery. For instance, even if the HIV plan mentioned contraception, WLHIV reported that if they disclosed their HIV status, the only contraceptive options available to them in public services were male condoms or sterilization.
The content analysis of national plans focused on service delivery, but during strategy sessions to prioritize advocacy issues and actions, WLHIV shared experiences of HIV-related discrimination that violated SRHR. Such experiences included providers’ refusal to provide or unwarranted delays in the provision of caesarean sections and pap smears; providers making discriminatory comments to women who expressed that they wanted to become pregnant; discriminatory treatment by medical staff during pregnancy and childbirth; and sterilization without informed consent.13 WLHIV identified advocacy priorities and shared these with women’s organizations at the conclusion of each workshop in order to identify opportunities for collaboration. Representatives of government and United Nations agencies also participated. Sharing the policy analysis and advocacy priorities was useful to begin conversations with policymakers; however, the SRHR violations described by WLHIV during the meetings were minimized by decision-makers as “anecdotal evidence.” Further, while this initial engagement with women’s organizations on SRHR did result in some cross training and joint advocacy—for example, highlighting the links between violence and HIV as part of the 16 days of activism against violence—it did not result in ongoing collective action.14
Phase two of the intervention: Documenting SRHR violations and using human rights mechanisms, including strategic litigation (2011–2014)
Strategic or impact litigation involves taking on a legal case as part of a strategy to achieve broad structural change. It can be a key tool in changing law, policy, or practice by setting legal precedent, as well as by placing an issue in the public eye and raising awareness.15 The potential of strategic litigation to compel states to progressively realize the right to health and respond to reproductive rights violations, in part by dedicating the maximum available resources, was perceived as an attractive antidote to WLHIV’s frustration that national policymakers deflected or rejected demands for greater attention to SRHR in the HIV response by saying that resources were limited.16 Also, ICW-Latina and Balance were strongly motivated to generate more evidence about SRHR violations to overcome the dismissal of WLHIV’s accounts of serious rights violations as “anecdotal” and for broader advocacy purposes. In early 2011, ICW-Mexico began to work with Balance and FUNDAR, an organization specializing in public interest legal strategies, to develop a questionnaire to identify SRHR violations for the purposes of strategic litigation. In the spring, ICW chapters in El Salvador, Guatemala, Honduras, and Mexico decided to document SRHR violations among WLHIV and pursue strategic litigation.17
In June 2012, 47 leaders from 35 different networks and civil society organizations from El Salvador, Guatemala, Honduras, Mexico, and Nicaragua gathered in Mexico City for a week-long workshop that provided in-depth training on frameworks that guarantee SRHR (with a focus on the Convention on the Elimination of Discrimination against Women and the Inter-American Convention on the Prevention, Punishment, and Eradication of Violence against Women) and detailed discussions of supportive strategies and practical considerations for strategic litigation.18 Country representatives from ICW, the regional transgender network RedLacTrans, the sex worker network RedTraSex, feminist lawyers, WLHIV affiliated with other organizations, and lesbian activists from Latin America participated in the training workshop. Selection criteria for participation included experience documenting rights violations, geographic location, and representation of or experience working with different populations, including indigenous women and women of African descent. This phase of the intervention explicitly sought to increase personal and professional contact and common objectives to strengthen trust and social cohesion among different groups of WLHIV, including those belonging to key populations. Social cohesion, or bonding social capital, is the strength or level of trust in social bonds, which influences a community’s willingness and ability to take collective action.19 The intervention also sought to increase relationships with feminist lawyers and other leaders of national women’s movements (bridging and linking social capital) to position the issues of WLHIV, particularly those related to SRHR, more firmly and prominently in the agenda of national women’s movements and mobilize additional political priority and resources from outside the HIV movement.20
During the workshop, each country team adapted the questionnaire based on a comprehensive SRHR framework that included the principles of nondiscrimination, availability, accessibility, acceptability, and quality previously piloted in Mexico to reflect their country contexts. Consensus on the final questionnaire was reached by all meeting participants. Country teams also created an action plan and signed a memorandum of understanding that defined the processes to implement the questionnaire and to refer WLHIV who wanted to pursue an SRHR human rights complaint to the feminist lawyer who would provide legal advice and, if appropriate, litigate on behalf of the complainant. The memorandum represented a commitment on behalf of the organizations to participate in the collaborative research and advocacy strategy and was intended to clarify roles and responsibilities to support the community leaders in working together.
From July 2012 to February 2013, 60 peer researchers completed interviewer-applied questionnaires to assess SRHR violations with 347 WLHIV from 42 political districts (departments or states) in El Salvador (n=69), Guatemala (n=10), Honduras (n=100), Mexico (n=91), and Nicaragua (n=77). Participants then presented the results collaboratively at face-to-face meetings with national policymakers and at press conferences held in each country. The participants also implemented a referral system to link WLHIV who wanted to use judicial or quasi-judicial mechanisms to allied feminist lawyers.
Intervention results: Collective action to promote and protect the SRHR of WLHIV
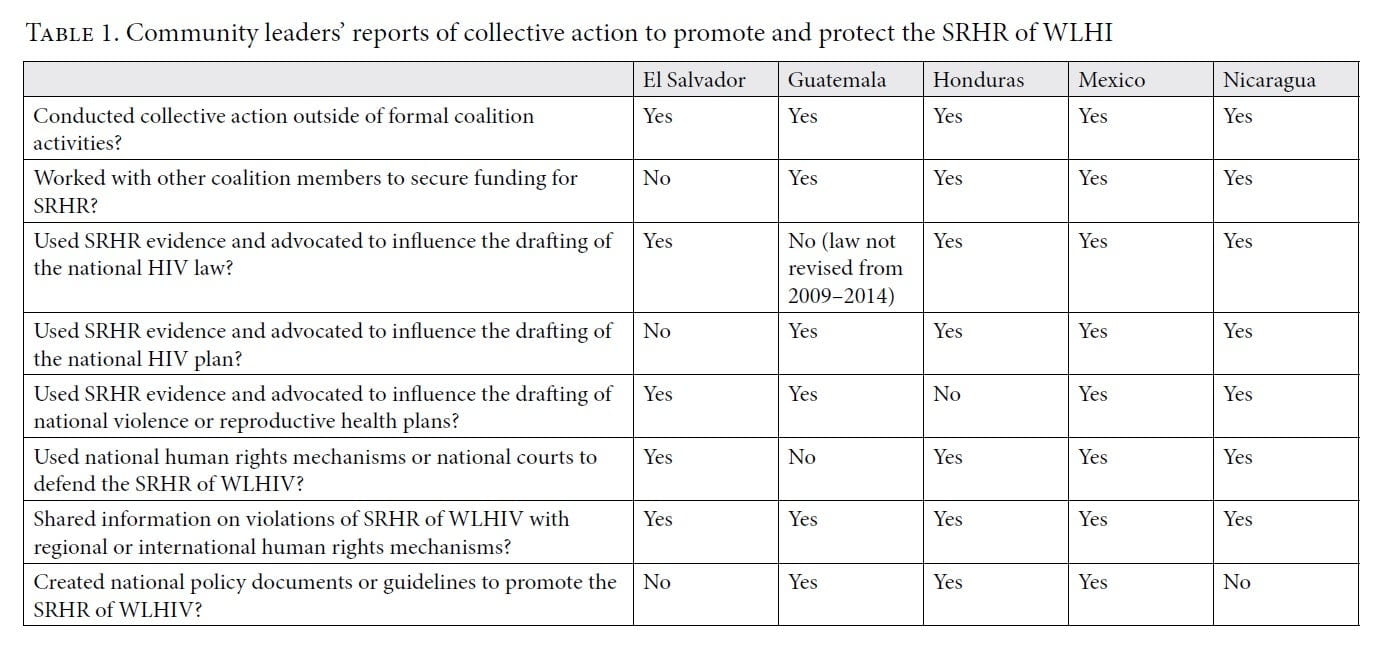
Participants in this community mobilization process used courts and national human rights mechanisms to protect SRHR by getting access to prevention and treatment services, sought redress for SRHR violations, and undertook joint advocacy to improve the promotion of SRHR in HIV laws, policies, and programs (Table 1). For example, in El Salvador, one of the participating human rights organizations brought a case alleging the forced sterilization of a 17-year-old WLHIV to the country’s Constitutional Court. The WLHIV was admitted to hospital at 9:45 in the morning for a planned cesarean section. To increase the probability of preventing vertical HIV transmission, cesarean delivery should take place before the rupture of membranes; she was seeking a cesarean section because of her gestational age. However, she was not taken to surgery until 9:45 at night. Despite her testimony that health care providers refused to take her to the operating theater until she signed a consent form for sterilization and that she did so under duress during active labor, the court did not find that the sterilization was coerced or an act of discrimination on account of her HIV status. However, it did find that because the complainant was a minor and had not received comprehensive counseling on contraceptive methods during her prenatal care, her fundamental rights to reproductive health, reproductive autonomy, and personal integrity had been violated. The hospital was ordered to provide ongoing psychological treatment for the complainant, and the Ministry of Health was directed to update technical guidance and training for health care providers to align with national and international human rights law.21
Participants also promoted respect for the SRHR of WLHIV by influencing legal reforms and public policy. To illustrate, in Mexico, coalition members introduced language explicitly recognizing the reproductive rights of WLHIV into the HIV law and achieved recognition of the need for coordinated action and co-responsibility between the national HIV and reproductive health programs to address perinatal HIV transmission.22 In Nicaragua, coalition members negotiated the removal of draft language making partner notification obligatory from the HIV law, preserving the status quo that people living with HIV could not be forced or coerced to disclose their HIV status.23 Coalition members also worked with national governments and international organizations to develop and disseminate position papers and guidance to promote the SRHR of WLHIV. For example, in Guatemala, the Ministry of Health, UNFPA, and ICW-Guatemala published specific medical guidance on the SRHR of WLHIV.24
Coalition members also took joint action to hold duty-bearers to account to deliver SRHR services to individual WLHIV in line with existing national standards. Examples included mobilizing to force local decision-makers to program cesarean sections and provide breast milk substitutes to WLHIV and, in one case, to provide antiretrovirals to a pregnant WLHIV who faced additional discrimination because she was a sex worker. Additionally, in four out of five countries, participating organizations raised additional funds to work on SRHR with other coalition members (Table 1).
These illustrative examples suggest the power of community-led collective action to advance SRHR by holding duty-bearers to account for service delivery, as well as by influencing laws and public policy. Below, we consider in greater depth how the intervention processes enabled effective collective action by changing knowledge and perceptions, promoting common goals, and developing relationships that strengthened bonding and bridging social capital.
How did the community mobilization process affect SRHR knowledge, evidence, and advocacy?
Increased knowledge, critical consciousness, and agency
The intervention created opportunities for community leaders to deepen their knowledge of SRHR and engage in dialogue and critical reflection. This process resulted in common understanding, identification of solutions, and eventually individual and collective action. Developing a common understanding of injustice and strategies to respond has been denominated “critical consciousness” and “issues framing.”25 During phase one, WLHIV identified SRHR violations as a problem because of gross and clearly discriminatory abuses that they or their peers had experienced. Through the intervention, community leaders acquired up-to-date information about WLHIV’s sexual and reproductive health options, including medical guidance on a range of contraceptive options and the fact that having an undetectable viral load allowed WLHIV to consider vaginal delivery and breastfeeding. Leaders deepened their analysis of the SRHR violations being committed and increased their ability and confidence to respond. One WLHIV leader explained:
Now I have foundational elements … First, that if they have a viral load below 1,000 they can have a vaginal birth, two that there are options for assisted reproduction that should be offered, that there are family planning methods [appropriate for WLHIV], all of these [are] issues that I couldn’t deal with before because I didn’t have what we would call the scientific information. (interviewee 7)
WLHIV reported that the knowledge they gained improved their education and counseling efforts with their peers and their own health behaviors. As a consequence of participating in the coalition, WLHIV described changed health behaviors that ranged from seeking routine sexual and reproductive health exams (such as pap smears, mammograms, and tests for sexually transmitted infections) to beginning to contemplate becoming sexually active again post-diagnosis, to overcoming guilt about sexual pleasure and masturbation, to exercising increased autonomy in sexual decision-making with partners. Participants also described feeling more empowered and exercising greater decision-making autonomy in their relationships with health care providers. An illustrative testimony came from a relatively new WLHIV leader who explained that her engagement with the coalition introduced her to the idea of bodily autonomy and informed her about sexual and reproductive options. She said:
Our partner can even be the one who is violating our right to decide about our body … Now, I can say when, how and where [I want to have sex], and I can exercise my right if I want to get pregnant, [and know] what the guidelines are for my care. (interviewee 12)
WLHIV linked their individual health-seeking behaviors to engagement in community monitoring of services and advocacy on behalf of themselves and other WLHIV. For example, one interviewee said:
Now I go and get a pap, and my mammography … as a network [of WLHIV] we make our presence felt, we go to the clinics and we ask that they do this or that, if we feel mistreated, we tell them. (interviewee 8)
Coalition participants who were not living with HIV also described changes in their health behavior and perceptions, with feminist lawyers frequently expressing increased awareness of vulnerability to HIV transmission:
I don’t assume that because I’m in a monogamous relationship, I’m not vulnerable … I am trying to get pregnant again and my gynecologist didn’t order the HIV test, saying “you did it a year ago” and I said “yes, but that was a year ago, and you don’t know and neither do I.” (interviewee 22)
Participants made it clear that, overall, women in their countries lacked knowledge about SRHR, regardless of their HIV status. One WLHIV described the situation poignantly, saying, “I ask myself: Why is it necessary to have a diagnosis to discover so many things? Why didn’t we learn before it happened?” (interviewee 4). In all five countries, participants identified the development of a “culture of rights” as a result of the intervention. For example:
Something that is really important is when you realize that a woman doesn’t think that her rights have been violated, rather that it was the work of the Holy Spirit. Now there is a culture that talks about rights—there were many women who didn’t know what their rights are, that that they have to fight for them, that they have to speak up—and that has changed. (interviewee 21)
Community leaders also described how their sense of agency increased upon learning that states have obligations to promote and protect human rights and that there are national, regional, and international mechanisms to hold duty-bearers to account. One theme that emerged was that applying the questionnaire, which was grounded in international human rights law, was important for community leaders’ adoption of a rights-based perspective. For example, one trans leader living with HIV explained that, for her, the turning point for being able to communicate a rights-based perspective with her peers and talk about SRHR was the process of repeatedly asking other WLHIV the questions in the questionnaire and internalizing the knowledge that “every point, every question in that survey is from a treaty that Mexico has with national and international organisms, and that Mexico signed and that isn’t being fulfilled” (interviewee 17).
Reflecting on the process of documenting SRHR violations, a feminist ally said:
When you hear [community leaders] say how useful what they learned is, it is really motivating. At one point, I thought that it was going to be a really academic exercise, very intellectual, but no. They really grasped the key issue of knowing the women that they work with better, recognizing rights violations that they hadn’t believed were violations, rights that they hadn’t believed were rights. (interviewee 20)
Community leaders also noted that their increased knowledge of administrative mechanisms to pursue human rights complaints gave them new tools and an increased sense of agency. This was exemplified by a WLHIV leader who said:
Before, they [WLHIV] didn’t really recognize what we call sexual and reproductive rights, how to respond, how to make a complaint if our rights are violated. So, in the process the women have become more empowered. (interviewee 26)
Participants described their new knowledge about the regional and international accountability mechanisms as hopeful and motivating. For example, one interviewee said:
There is a process, there is an administrative machine in my country, and if they don’t respond, I can go to the international level so that my voice is heard—maybe it won’t resolve anything for me, but it can help other women in the future. (interviewee 23)
According to community leaders, the process of gaining knowledge about SRHR and the national, regional, and international mechanisms that exist to protect human rights contributed to their development of critical consciousness about SRHR and resulted in the appropriation and dissemination of human rights discourses. It also resulted in increased agency, which allowed them to enact behaviors to promote and protect their SRHR and the SRHR of WLHIV as a group.
Focused advocacy: Positioning WLHIV as SRHR experts
The identification of SRHR as an institutional priority from 2009 to 2014 by the country and regional chapters of ICW, coupled with capacity building and the generation of evidence, provided coherence and substance for advocacy. The collective action frame strengthened community leaders’ advocacy efforts, as illustrated by one WLHIV leader who said that having
a political agenda gave the [WLHIV leaders] a tool, to be able to make the same argument at all of the tables … [when modifications to the HIV law were discussed in each locality] the need for a chapter on sexual and reproductive health was always mentioned—that was the women’s position. (interviewee 26)
In each of the four countries where the HIV law was modified between 2009 and 2014, coalition members influenced outcomes in favor of SRHR (Table 1). Further, their increased knowledge and focus on SRHR allowed WLHIV, sex workers, and trans women community leaders to position themselves as experts, which in turn increased their standing with other civil society organizations, government representatives, and the United Nations:
These alliances have allowed us to do advocacy at a different level, and it has also allowed us to empower ourselves. Having knowledge gives you power and positions you politically. As the Guatemalan [chapter of ICW], we are the main reference point on the sexual and reproductive health of women living with HIV in Guatemala. They call us, they tell us—knowledge gives you strength, learning gives you power and legitimacy and arguments. (interviewee 9)
In some instances, at the very local level, increased knowledge of SRHR among community leaders and access to intellectual resources created through the coalition allowed them to quickly resolve SRHR violations by sharing information with local authorities:
She is HIV positive, and they raped her, and she got pregnant. She went to the hospital, but they refused to give her an abortion [even though abortion is legal in cases of rape] and they didn’t give her any information so that she could go to Mexico City [where abortion is available on demand up to 12 weeks]. They didn’t give her any options. So that girl had a home abortion, and then they arrested her. So, we gave the information sheet on sexual and reproductive rights to the state prosecutor, and based on that, they let her free. (interviewee 25)
Using evidence about SRHR violations for advocacy: “These aren’t urban legends”
During phase one of the process, when WLHIV shared examples of SHRH violations with policymakers, the examples were dismissed as “anecdotes.” The evidence generated through participatory research with 347 WLHIV from five countries undertaken during phase two of the intervention was perceived by WLHIV and their allies as legitimating the importance of SRHR violations. The survey found that 41% of respondents had experienced discrimination when seeking reproductive health services, only 22% had received female condoms, only 34% had been tested for human papillomavirus, and almost a quarter reported coercion to sterilize or forced sterilization.26 One WLHIV leader summed up the effects of having evidence when advocating before national decision-makers, saying that the research results prove that the SRHR violations experienced by WLHIV “aren’t urban legends” (interviewee 7). That the evidence was quantitative and conceptually grounded in international human rights law was perceived by participants as increasing impact:
We have generated evidence that we didn’t have before, systematized, that allowed us to use nonlegal mechanisms, but from a much stronger position … We have percentages, and we have gotten press coverage because of the percentages that we have. So, we are still using nonlegal mechanisms, but starting to work within a legal framework strengthened our work a great deal. (interviewee 20)
In all countries, community leaders brought forward evidence from the community-led participatory research to influence the development of national plans on HIV, sexual and reproductive health, and gender-based violence (Table 1). The generation and presentation of evidence was perceived to favorably affect policy advocacy efforts. For example, a Mexican feminist attributed the integration of sexual and reproductive health with HIV in the HIV and reproductive health national sectoral plans to coalition members
insisting for years—with evidence—that HIV needs to be incorporated into the reproductive health response. And generating the evidence and being willing to work with decision-makers, and providing evidence to decision-makers. (interviewee 18)
The evidence generated was also incorporated into documents developed with the United Nations system and presented to regional and international human rights bodies, including the Special Rapporteur on torture (in the case of Mexico) and the Universal Periodic Review (in the case of Honduras).27 A significant example for all countries was reporting the results to the United Nations Commission on the Status of Women via the confidential communications procedure. In addition to the commission providing the information to national governments and requesting a response, it highlighted the SRHR of WLHIV as an issue of concern in its conclusions.28
Finally, sharing evidence about SRHR violations experienced by WLHIV was identified as important for helping community leaders position the issue on the agenda of the broader HIV and women’s movements. A WLHIV leader explained that
we have used the evidence to convince other organizations, like [the network of people living with HIV] to fully embrace issues of sexual and reproductive health. (interviewee 16)
Similarly, research results were used to raise the visibility of the issue within the women’s movement. For example, at the “national feminist summit, it was made visible and recognized that [the SRHR of WLHIV] is also a feminist fight” (interviewee 24).
How did the community mobilization process contribute to building bonding and bridging social capital?
Strengthening social cohesion and bonding social capital
Working jointly to identify violations and to promote and defend SRHR contributed to a sense of common purpose and identity among diverse community leaders who are active in the HIV movement. In the words of one trans woman leader:
We have issues in common, a common fight, because it hurts us to see the suffering that our populations experience in Mexico and Central America because of their rights being denied. (interviewee 3)
Participation in the coalition didn’t overcome all discrimination based on professional and gender identity or completely erase political tensions between different groups of WLHIV, sex workers, and trans women. However, in general, respondents reported that working together on SRHR reduced stigma and discrimination and improved personal and working relationships. To illustrate, a sex worker explained that the initiative
brought us together, because there had always been a distancing with the network [of WLHIV] because they blamed us for their husbands infecting them with HIV and because the men came to us rather than bringing home the bacon, so these things got smoothed out, and now we take joint actions. (interviewee 11)
For their part, WLHIV leaders reported that collective action helped them overcome prejudices toward trans women and sex workers and created relationships that increased the scope of their advocacy and programmatic work:
Now I don’t only work specifically with women living with HIV, I also work with sex workers, and women who use drugs and trans women living with HIV. So, this joint collaboration totally expanded my work because we can talk about the same issues and have a common goal. (interviewee 21)
Protecting and promoting the SRHR of WLHIV through bridging social capital
Feminist lawyers reported that working with WLHIV convinced them that the specific challenges faced by WLHIV were worthy of attention from the broader women’s movement:
The violations of human rights of all women are so severe in our countries that the specificities can become invisible. For me, the main change is that I can’t stop making [HIV] visible, I have to make the specific forms of discrimination that are experienced and the vulnerabilities with respect to accessing specific rights visible. (interviewee 24)
Beyond their focused technical support in filing human rights complaints and their formal and informal mentorship of WLHIV leaders in feminist analysis, the influential roles that the majority of the feminist lawyers held in national and regional women’s organizations—for example, as leaders of prominent sexual and reproductive health organizations or as founders of networks dedicated to addressing violence against women—increased the policy advocacy spaces available to WLHIV. For example, in El Salvador, relationships forged through the coalition resulted in ICW being invited to participate in the national working group for the Violence against Women and Gender Equality Law. Similarly, in Nicaragua, a coalition member stated that
the effort over the past years has been to try to bring feminist organizations together with organizations that work in HIV, particularly with women. They did come closer together which enabled [WLHIV] to provide feedback and experiences on violence, health care (interviewee 24)
Further, the relationships and evidence generated through the coalition were fed directly into policy and legislative processes through the intervention of feminist allies. For example, a participating feminist lawyer said, “I had the report [on SRHR violations] in my hand” (interviewee 6) as she drafted the revised HIV law.
New relationships also allowed community leaders who lived outside of national capitals to inform national decision-makers about SRHR violations through coalition members located in the capitals. For example, a local Mexican HIV organization identified a pregnant WLHIV who had been discriminated against at a public hospital and who had not had her viral load or CD4 count evaluated or a caesarean section performed at 39 weeks’ gestation, even though national guidelines stated that a caesarean delivery should have been programmed at 38 weeks. The organization informed coalition colleagues in Mexico City, who immediately notified senior officials at the National AIDS Program and National Human Rights Commission; these officials, in turn, communicated to the State AIDS Program and hospital the urgency of providing health services in line with national medical guidelines, resulting in the prompt provision of a caesarean delivery.
The value added of relationships built through the coalition were frequently reciprocal and went beyond advocacy around the SRHR of WLHIV. For example, speaking about efforts to lobby for a law on gender identity, a trans leader explained that
we decided to bring it forward with other [coalition] organizations, because with strategic and organizational allies, it gives us more back up, it makes us stronger in the struggle. (interviewee 14)
In agreement with the community mobilization literature about the importance of bridging and linking social capital and organizational structures, bringing together feminist lawyers from women’s and human rights organizations with leaders from three HIV networks in the region (namely ICW-Latina, RedLacTrans, and RedTraSex) provided additional access to and support in political spaces, as well as technical resources.
Conclusion
This analysis of participant perspectives on the effects of a five-year community-led intervention indicates that sustained capacity-building and creation of network structures contributed to the development of a “culture of rights,” the increased agency of community leaders, and collective action that effectively promoted and protected the SRHR of WLHIV. The development of critical consciousness and the collective action frame of promoting and protecting the SRHR of WLHIV strengthened bonding and bridging social capital among diverse groups of WLHIV, women affected by HIV, and feminist allies. These relationships mobilized technical, financial, and organizational resources to defend the SRHR of individual WLHIV and to influence the legislative and policy environment. Flexible and renewed funding over the five-year period allowed the initiative to be truly community-led and participatory by adapting to evolving priorities and supporting collective processes.
The participatory generation of evidence through community-led research deepened community leaders’ understanding of and motivation to defend the SRHR of WLHIV and was described as central for internalizing, adapting, and adopting human rights concepts. Community leaders reported changes in their health behavior and thinking about SRHR, which suggests that knowledge and skills development benefited them personally and started to permeate through their social networks. WLHIV also reported that the intervention began to create a “culture of rights” in which the normalization of SRHR violations and taken-for-granted discrimination based on HIV status began to be questioned. As a consequence, both individuals and networks of WLHIV began to raise their voices in protest. Having credible evidence about SRHR violations and scientific knowledge was perceived by participants as critical for positioning themselves as experts, engaging in dialogue and policy advocacy with decision-makers, and using national, regional, and international human rights mechanisms. In agreement with community leaders’ reports about their increased capacity and collective action to defend SRHR because of this intervention, a 2016 survey of 343 WLHIV and 101 external stakeholders identified SRHR and other human rights of WLHIV as the thematic areas in which ICW-Latina has had the greatest influence and advocacy success.29
Actions by participating community leaders improved immediate access to SRHR for individual WLHIV and resulted in legal decisions, guidelines, policies, and legislation that promoted the SRHR of WLHIV in alignment with international human rights law. This analysis indicates that community mobilization interventions that foster critical consciousness, social cohesion, and organizational linkages increase the capacity of community leaders to hold governments to account for meeting national, regional, and international human rights standards and can make broad contributions to the health and well-being of society by supporting health policy and systems improvements.
Acknowledgments
We would like to acknowledge Monica Paulina Hernández Leyva for her assistance with data collection and Arely Cano Meza, regional secretary of ICW-Latina, for her leadership and commitment to advancing the SRHR of WLHIV. During her postdoctoral research fellowship, Tamil Kendall was supported by the Canadian Institutes of Health Research, the Pierre Elliot Trudeau Foundation, the Women and Health Initiative, and the Takemi Program in International Health of the Harvard School of Public Health.
Tamil Kendall, PhD, is an Adjunct Professor at the School of Population and Public Health, University of British Columbia, Vancouver, Canada.
Jimena Avalos Capin, JD, LLM, MPP, is Head of the Prevention and Combat against Sexual Harassment Unit of the Federal Judiciary Council of Mexico, Mexico City, Mexico.
Nazneen Damji, MSc, is Policy Advisor for Gender Equality, HIV and Health at the United Nations Entity for Gender Equality and the Empowerment of Women, New York, USA.
Eugenia Lopez Uribe, MA, is Head of Engagement for Latin America and the Caribbean at Girls Not Brides, Mexico City, Mexico.
Please address correspondence to Tamil Kendall. Email: tamil.kendall@ubc.ca.
Competing interests: Tamil Kendall, Jimena Avalos Capin, and Eugenia Lopez Uribe participated in the design and delivery of the community mobilization intervention in their past roles with Balance Promoción para el Desarrollo y Juventud, Mexico City, Mexico. The Ford Foundation’s Office for Mexico and Central America provided financial support for the activities described but did not have any role in the preparation of this manuscript. Tamil Kendall received personal fees from UN Women during the preparation of this manuscript.
Copyright © 2020 Kendall, Avalos Capin, Damji, and Lopez Uribe. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction.
All Spanish language material was translated into English by Tamil Kendall.
References
1. Joint United Nations Programme on HIV/AIDS, Power to the people (Geneva: Joint United Nations Programme on HIV/AIDS, 2019), p. 21.
2. Joint United Nations Programme on HIV/AIDS, What is a community-led organization? (Geneva: Joint United Nations Programme on HIV/AIDS, 2019); Global Fund to Fight AIDS, Tuberculosis and Malaria, Technical brief: Community systems strengthening (Geneva: Global Fund, 2019).
3. T. J. Coates, M. Kulich, D. D. Celentano, et al., “Effect of community-based voluntary counselling and testing on HIV incidence and social and behavioural outcomes (NIMH Project Accept; HPTN 043): A cluster-randomised trial,” Lancet Global Health 2/5 (2014), pp. e267–277; D. Kerrigan, J. Mbwambo, S. Likindikoki, et al., “Project Shikamana: Community empowerment-based combination HIV prevention significantly impacts HIV incidence and care continuum outcomes among female sex workers in Iringa, Tanzania,” Journal of Acquired Immune Deficiency Syndromes 82/2 (2019), pp. 141–148; S. A. Lippman, A. M. Leddy, T. B. Neilands, et al., “Village community mobilization is associated with reduced HIV incidence in young South African women participating in the HPTN 068 study cohort,” Journal of the International AIDS Society 21/Suppl 7 (2018), p. e25182.
4. F. Anam, C. Chung, S. Dilmitis, et al., “Time to realise our sexual and reproductive health and rights,” Lancet Global Health 6/10 (2018), pp. e1064–1065; L. Orza, E. Bass, E. Bell, et al., “In women’s eyes: Key barriers to women’s access to HIV treatment and a rights-based approach to their sustained well-being,” Health and Human Rights Journal 19/2 (2017), pp. 155–168.
5. S. Kumar, S. Gruskin, R. Khosla, and M. Narasimhan, “Human rights and the sexual and reproductive health of women living with HIV: A literature review,” Journal of the International AIDS Society 18/Suppl 5 (2015), p. e20290; S. Van Belle, V. Boydell, A. S. George, et al., “Broadening understanding of accountability ecosystems in sexual and reproductive health and rights: A systematic review,” PLoS One 13/5 (2018), p. e0196788.
6. P. R. Payne and K. R. Williams, “Building social capital through neighborhood mobilization: Challenges and lessons learned,” American Journal of Preventive Medicine 34/Suppl 3 (2008), pp. 42–47.
7. See ICW Global International Community of Women Living with HIV/AIDS, International Strategic Plan 2009–2014 (2009).
8. T. Kendall and E. Lopez Uribe, “Improving the HIV response for women in Latin America: Barriers to integrated advocacy for sexual and reproductive health and rights,” Global Health Governance 4/1 (2010), pp. 1–8.
9. Lippman et al. (see note 3).
10. R. D. Benford and D. A. Snow, “Framing processes and social movements: An overview and assessment,” Annual Review of Sociology 26 (2000), p. 614.
11. International Convention on the Elimination of All Forms of Discrimination against Women,
G.A. Res. 34/180 (1979); Inter-American Convention on the Prevention, Punishment and Eradication of Violence against Women (Convention of Belém do Pará) (1994); United Nations, Fourth World Conference on Women, Beijing Declaration and Platform for Action, UN Doc. A/CONF.177/20 (1995); United Nations Population Fund, Programme of Action Adopted at the International Conference on Population and Development, Cairo, 5–13 September 1994 (New York: United Nations Population Fund, 2014); United Nations Statistics Division, Millennium Development Goals indicators. Available at http://mdgs.un.org/unsd/mdg/Default.aspx; United Nations General Assembly, G.A. Res. 60/262, UN Doc. A/RES/60/262 (2006), paras. 27, 29, 30, 31, 34.
12. Kendall and Lopez Uribe (see note 8).
13. Fieldnotes from Tuxtla Gutierrez, Mexico, November 27, 2009; Guatemala City, Guatemala, April 11, 2010; Managua, Nicaragua, April 19, 2010; San Pedro Sula, Honduras, March 15, 2010.
14. Fieldnotes from Mexico City, Mexico, December 15, 2010; Report to Ford Foundation, December 17, 2010.
15. M. W. McCann, Law and social movements (Burlington: Aldershot, 2006).
16. Fieldnotes,from Tuxtla Gutierrez, Mexico, November 27, 2009.
17. Fieldnotes from Mexico City, Mexico, April 27, 2011.
18. Fieldnotes from Mexico City, June 23–25, 2012.
19. Payne and Williams (see note 6).
20. Ibid.
21. GM v. Hospital Nacional de Maternidad, Amparo 749-2014 GM, Supreme Court, San Salvador, El Salvador (March 11, 2015). Available at http://www.csj.gob.sv/Comunicaciones/2015/MAR_15/COMUINICADOS/Amp%20749-2014%20Sentencia%20Esterilizaciones%20Forzadas.pdf.
22. Mexican Ministry of Health, Norma Oficial Mexicana NOM-010-SSA2-2010, Para la prevención y el control de la infección por Virus de la Inmunodeficiencia Humana, art. 5.6.5; Mexican Ministry of Health, Respuesta al VIH, SIDA e ITS: Programa sectorial de salud 2013–2018 (2014); Mexican Ministry of Health, Salud materna y perinatal: Programa sectorial de salud 2013–2018 (2014).
23. Government of Nicaragua, Ley No. 238. Ley de Promoción, Protección y Defensa de los Derechos Humanos ante el SIDA (1996, modified December 2012), art. 27.
24. Guatemalan Ministry of Public Health and Social Assistance, UNFPA, and ICW-Guatemala, Manual para la atención de la salud sexual y reproductiva de mujeres que viven con VIH y VIH avanzado (sida) (Guatemala: United Nations Population Fund, 2012).
25. S. A. Lippman, T. B. Neilands, H. H. Leslie, et al., “Development, validation, and performance of a scale to measure community mobilization,” Social Science and Medicine 157 (2016), p. 129.
26. Mesoamerican Coalition for the Reproductive Rights of Women with HIV, Political statement about reproductive rights violations experienced by women living with HIV in Mesoamerica. Available at https://www.balancemx.org/sites/default/files/recursos/StatementMesoCoalition.pdf; T. Kendall and C. Albert, “Experiences of coercion to sterilize and forced sterilization among women living with HIV in Latin America,” Journal of the International AIDS Society 18/19462 (2015).
27. Human Rights Council, Informe de seguimiento del Relator Especial sobre la tortura y otros tratos o penas crueles, inhumanos o degradantes: Mexico, UN Doc. A/HRC/34/54/Add.4 (2017), para. 89; Asociadas por lo Justo, Centro de Derechos de Mujeres, Centro de Estudios de la Mujer Honduras, et al., Informe conjunto presentando por las organizaciones feministas de Honduras para el Examen Periódico Universal (September 2014), para. 24.
28. United Nations Commission on the Status of Women, Report on the Fifty-Seventh Session (4–15 March 2013), UN Doc. E/2013/27 (2013), para. 103(7)(i).
29. See L. Sanchez Calvo, Consultoria para la construccion de la linea de base del proyecto de ICW Latina subvencionado por el Fondo Mundial de Lucha Contra el Sida, la Tuberculosis y la Malaria (2016), pp. 75, 121.