Police Discrimination, Misconduct, and Stigmatization of Female Sex Workers in Kenya: Associations with Delayed and Avoided Health Care Utilization and Lower Consistent Condom Use
Volume 22/2, December 2020, pp. 199 – 212
David Kuria Mbote, Laura Nyblade, Caroline Kemunto, Kayla Giger, Joshua Kimani, Pia Mingkwan, Stella Njuguna, Emmanuel Oga, and John D. Kraemer
Abstract
Discrimination and violence against sex workers by police are common in many populations and is associated with negative health outcomes, as well as being per se violations of human rights laws and norms. There is a close and mutually reinforcing nexus between legally actionable rights violations and stigma, and reducing human rights violations against sex workers likely requires both legal and societal interventions that address both. In this paper, we first aim to estimate levels of discrimination, violence, and stigma against women sex workers by police in Kenya. Second, we aim to estimate the association between manifestations of discrimination and stigma, on the one hand, and general health care utilization and consistent condom use, on the other. Using data from a survey of Kenyan sex workers, we document widespread discrimination and stigma. Through regression analyses, participants with the highest levels of all three categories of manifestations of discrimination and stigma reported significant lower consistent condom use. Those with the highest levels of witnessed/heard manifestations were significantly more likely to delay or avoid needed health care, and the highest level of experienced manifestations were associated with a marginally significant increase in delay or avoidance. Our findings document a plethora of violations of human rights obligations under Kenyan and international law.
Background
There is a close nexus between discrimination, violence, and other abuses that are actionable under international and national human rights regimes, on the one hand, and stigma as a social process, on the other. Discrimination, the remediation of which is an obligation of immediate effect in international human rights law, essentially occurs when members of groups that are situated similarly are instead treated differently. For discrimination to be legally actionable, disparate treatment must burden a protected group or be on prohibited grounds that are defined in international law and domestic constitutions and law.[1]
Stigma, meanwhile, is seen by social scientists as a process that distinguishes and labels differences, causes those differences to be associated with socially disfavored traits, and separates outgroups from ingroups. This, in turn, allows power to be exercised in such a way that further diminishes the power and social status of those who are stigmatized.[2] Discrimination is thus a cause of the process by which stigmatization occurs. Once marking and treating individuals as “the other” is authorized by governments—either directly or indirectly, such as by failing to redress discrimination by private actors—stigma is exacerbated.[3]
Simultaneously, the process of stigmatizing a group is an important mechanism by which discrimination comes into being. Once groups are stigmatized in a society, it is harder for them to make claims to being equally situated in the eyes of the law. Policies concerning such groups become increasingly likely to be based in animus or stereotype because those who make and enforce policies wrongly believe the distinctions to be material, and diminished power precludes effective protection against animus or contestation of stereotypes.[4] Thus, while legal measures to prevent and remedy discrimination and other acts that harm marginalized groups are necessary to reduce stigma, steps to reduce stigmatization are often also required to create the political space in which anti-discrimination law can be effectuated.[5]
In the usual social science framework, then, discrimination and stigma are mutual causes with a partial conceptual overlap.[6] Though stigma is commonly thought of as a mental state, social scientists think of it as a social process with measurable manifestations. Stigma can be measured in its various manifestations: the experience of discriminatory and othering acts (experienced stigma), the observation (witnessed or heard stigma) or secondhand perception of their likelihood, the anticipation of such acts (anticipated stigma), and internalization toward oneself (internalized stigma). Usually, multiple and layered manifestations act on the same person.[7] Acts of discrimination are measured within the concept of experienced stigma and are often actionable under the law. Other manifestations of stigma are often not legally actionable but cause meaningful harm to both individuals and groups, and failing to address them undermines the effective protection of human rights.
Around the world, sex workers encounter high levels of discrimination, violence, and stigma by police. While the problem is ubiquitous, levels are highest in settings where sex work is criminalized, granting police the opportunity to exploit power differentials over sex workers, and exacerbated where legal systems and policing culture do not provide accountability for misconduct.[8] Abuses committed by police include verbal and physical abuse, arrest, refusal to protect, and confiscation of condoms. This conduct violates state duties to respect a variety of human rights protected under international law and most countries’ domestic law. These rights include the right to be free from discrimination; freedom from cruel, inhuman, and degrading treatment; the right to the security of one’s person; the right to be treated with dignity; the right to privacy; the right to personal autonomy; and the right to equality before the law.[9] When conduct directly impedes access to public health or health care—either because sex workers experience wrongful acts or because of anticipated, witnessed or heard, or internalized manifestations of stigma created by police—violations of the right to the highest attainable standard of health also exist.[10]
Links between discrimination, violence, and stigma against sex workers, greater exposure to health risks, and reduced health care access and utilization are well documented across a variety of contexts.[11] Existing research framed through the lens of stigma against sex workers by police and health outcomes has focused primarily on experienced stigma. It has focused principally on outcomes related to HIV and other sexually transmitted infections, finding strong evidence that experiencing negative police interactions is associated with reduced condom carrying and use, as well as increased risk of HIV and other sexually transmitted infections.[12] UNAIDS has recognized the criminalization of sex work as a driver of HIV risk among sex workers, who bear disproportionate levels of HIV risk.[13] Additionally, violent injury at the hands of police is well documented, and research also indicates that stigma manifesting as police refusal to protect increases the likelihood of injury by private actors.[14]
Only a few studies have examined linkages between police conduct and health care utilization outside of HIV services, and research is lacking from sub-Saharan Africa.[15] Additionally, while a few studies have found aspects of anticipated and witnessed or heard stigma by police to be extensive, little work has examined the association between anticipated and witnessed or heard manifestations of police stigma and health outcomes. Anticipated and witnessed or heard stigma against sex workers by other actors is associated with a variety of adverse health outcomes.[16] While the interconnectedness of the right to health and violations of other human rights is central to the modern conception of health and human rights, achieving a more nuanced understanding of this relationship is important for both effective human rights advocacy and public health programming.[17]
Kenya is a particularly important country in which to understand linkages between human rights violations or manifestations of stigma against sex workers by police and health care outcomes. Though Kenya has made substantial progress in reducing HIV incidence and increasing access to treatment nationwide, the prevalence of HIV remains very high among sex workers—with estimates in Nairobi of about 30%.[18] While accurate estimates of the number of people engaged in sex work are difficult to acquire, a recent study estimates that about 5% of urban women aged 15 to 49 engage in sex work.[19] Simultaneously, Kenya has progressive constitutional provisions that should limit police misconduct and impunity for it; however, it also has a long legal tradition—reaching back to the colonial era—of failing to respect and protect the rights of sex workers.[20] As a result, recent studies suggest that violence against sex workers, including by police, increased in Kenya between 2013 and 2017.[21]
This study aims to answer the following questions. First, how often are manifestations of stigma—including those rooted in discrimination and expressed as various rights violations—by police reported by a sample of female sex workers in Kenya? Second, are these manifestations associated with reductions in general health care utilization and consistent condom use among Kenyan female sex workers—and if so, to what extent?
Methods
Participants and procedures. Survey data on which this analysis is based have been more fully described by Laura Nyblade et al. and are briefly summarized here.[22]
We drew a sample of 497 female sex workers in January 2015 with a modified respondent driven sampling (RDS) approach, stratified by four locations in Kenya to capture rural, urban, and transit corridor settings. Participants were eligible for inclusion if they were at least 18 years old, had lived in a study location for at least six months, and reported earning a significant portion of their income from sex work during the past three months. Partner sex worker organizations recruited 96 initial participants, who recruited up to four additional participants apiece. Those participants could then recruit up to four additional participants, and so forth. Because participation was greater than anticipated, the survey’s target sample was achieved within two waves, precluding full RDS analysis. (A companion sample of 232 male sex workers was also drawn but not included in this analysis due to insufficient sample size.)
Trained third-party interviewers collected information through face-to-face interviews conducted in private spaces at partner organizations’ offices. We selected interviewers through a competitive process to enhance surveying quality. All interviewers were trained on stigma, research ethics, and the survey instrument. We obtained ethics approval from the institutional review boards at the Kenya Medical Research Institute and Health Media Labs. All participants gave written informed consent prior to participating, and we complied fully with the Declaration of Helsinki.
Measures
Outcomes. We examined two principal outcomes, both self-reported: (1) avoidance or delay of general health (non-HIV) services perceived to be needed and (2) consistent condom use. To construct the health care avoidance or delay variables, we first asked respondents if they or their children had needed any services in the last 12 months and, among those who had needed health care services, whether they had ever not sought or delayed the service. Respondents were then separately asked to classify what health services they had used, avoided, or delayed up to the three most recent services (for example, maternal health, treatment for injury, etc.). Respondents were classified as avoiding or delaying a service if it was reported at least once. Condom use was assessed by asking respondents, “Of all the times you had sex in the last 12 months, how often was a condom used?” Response options were never, almost never, sometimes, often, and always. We dichotomized the variable into always or any other response.
Discriminatory and othering acts by police. The development of the discrimination and stigma items has been previously described.[23] We focused on three types of manifestations of police-related discrimination and stigma in this analysis: anticipated stigma, discriminatory and othering acts (experienced stigma), and witnessed or heard discrimination and othering acts.
Anticipated stigma and discrimination—the fear that stigma and discrimination will happen—was assessed by six items. They included fear of insult, harassment, or threat and fear of physical harm by police. Additionally, respondents indicated whether they feared carrying condoms because of trouble with police or askaris (as two separate items, the former referring to national government law enforcement officers and the latter referring to officers under the jurisdiction of county government) and whether they feared taking condoms from outreach workers because of possible trouble with police or askaris (again, two separate items). Fear about police and askaris were collapsed because responses were highly correlated, leaving four variables. Respondents were asked to report frequency and could respond never or not in the last 12 months (collapsed into one category), once, a few times, or often. For ease of interpretation, we assigned these responses values from 0 to 3 and summed respondents’ responses. We then categorized respondents as reporting none (a summed score of 0) or into tertiles of those who had anticipated police stigma and discrimination. We assessed the anticipated items’ internal consistency using ordinal alpha, and it met generally accepted criteria (0.87).[24]
The experience of discrimination and othering acts (experienced stigma) was constructed from respondents’ report of police engaging in five types of conduct toward them: verbal assault or harassment, physical harm, confiscation or destruction of condoms, arrest, or refusal to protect or take a statement. Witnessed and heard stigma was constructed from respondents’ report seeing or hearing of the same types of conduct toward other female sex workers. We constructed scores and categorized respondents’ experiences of discrimination and othering acts and witnessed/heard stigma the same way as for anticipated stigma. Both scales demonstrated good internal consistency using ordinal alpha (discrimination and othering acts=0.92; witnessed/heard=0.92).
For inclusion in secondary analyses, we also constructed variables specifically measuring manifestations related to condom possession. For discrimination and experienced stigma, responses to the item about how often police had confiscated or destroyed the respondent’s condoms in the last 12 months were categorized as never, once or a few times, and often. A single item asking how often respondents have witnessed or heard about police destroying or confiscating sex workers’ condoms was categorized the same way. Four anticipated stigma and discrimination questions, how often the respondent was fearful of either carrying or taking condoms because she might get into trouble with either police or askaris, were collapsed and then categorized into a comparable three-level variable.
Control variables. We included anticipated stigma and discrimination from health care workers as a control variable because we expected it to reduce health care utilization based on previous research, and it may correlate with manifestations of stigma and discrimination from police.[25] We measured this using two items—how often the respondent reported being fearful of gossip and how often the respondent reported being fearful of verbal harassment, insult, or threat from health care workers (never to often in the last 12 months). Because the items were strongly correlated, we constructed an ordinal variable for whether the respondent reported never, once or only a few times, or often anticipating at least one of these fears.
Other control variables included the site from which the respondent was recruited, the frequency with which she reported needing health services in the last 12 months (once, a few times, or often), quintiles of age, education (primary or less, secondary, or tertiary), marital status (never versus ever married or partnered), quintiles of time as a sex worker, and quintiles of income from sex work. All items can be found in the survey instrument, provided in the link to supplement 1.
Statistical methods
We described the sample using standard approaches: means, standard deviations, frequencies, and percentages. We then examined the association between discrimination and othering acts (experienced stigma), anticipated stigma, and witnessed or heard stigma by separately fitting logistic regression models. For avoidance or delay of general health care services, the base model also included the variable for how frequently the respondent had needed services in the last 12 months, and it was restricted to those respondents reporting that they needed services at least once. The base model for condom use included only stigma and discrimination and recruitment site. Fully adjusted models additionally included control variables for age, education, marital status, length of time as a sex worker, income from sex work, HIV status, and anticipated stigma from health care workers (in models of health care utilization only). Because odds ratios are often misinterpreted, we estimated and graphed adjusted probabilities of our outcomes of interest at various stigma and discrimination levels using marginal effects with other covariates held at their observed levels.
As a robustness check, we constructed tertiles of discrimination and othering acts, anticipated stigma, and witnessed or heard stigma in an alternative manner that has fewer assumptions about the survey items. Supplement 2 presents results from regression models substituting these discrimination and stigma variables, as well as the concordance between scores from this and our main approach. Finally, we used structural equation modeling to construct path models to test a hypothesis that lower consistent condom use was directly associated with the highest level of discrimination and othering acts (experienced stigma) and anticipated stigma, that experienced discrimination and othering acts transmitted an association through anticipated stigma, and that witnessed or heard stigma transmitted an association only through anticipated stigma. Supplement 2 provides fuller details of the approach we used.
All analyses used Stata, version 15.1.
Results
Participant characteristics
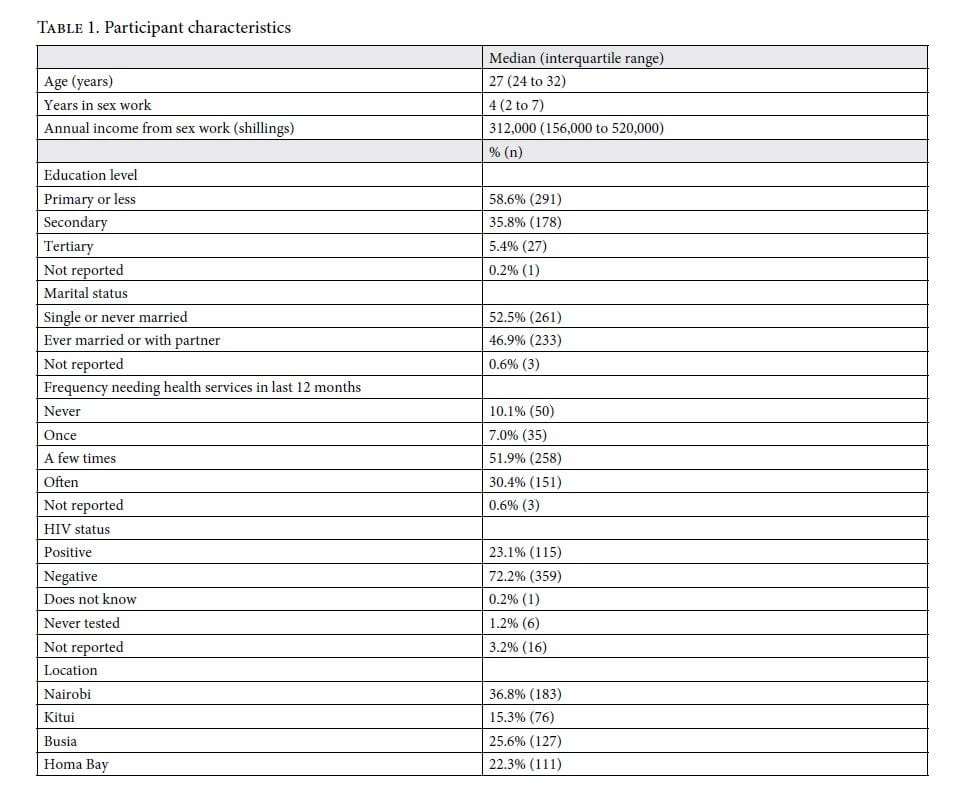
Participant characteristics are provided in table 1. Of note, most participants had primary schooling or less (58.6%), reported needing health care services for themselves or their children at least once in the last year (89.9%), and were not living with HIV (72.2%). Participants had been engaged in sex work for a median of four years and earned a median of 312,000 Kenyan shillings from sex work (approximately US$3,000) annually. Missing data were rare, with choice not to report HIV status the most common (3.2%).
Prevalence of manifestations of discrimination, othering acts, and stigma
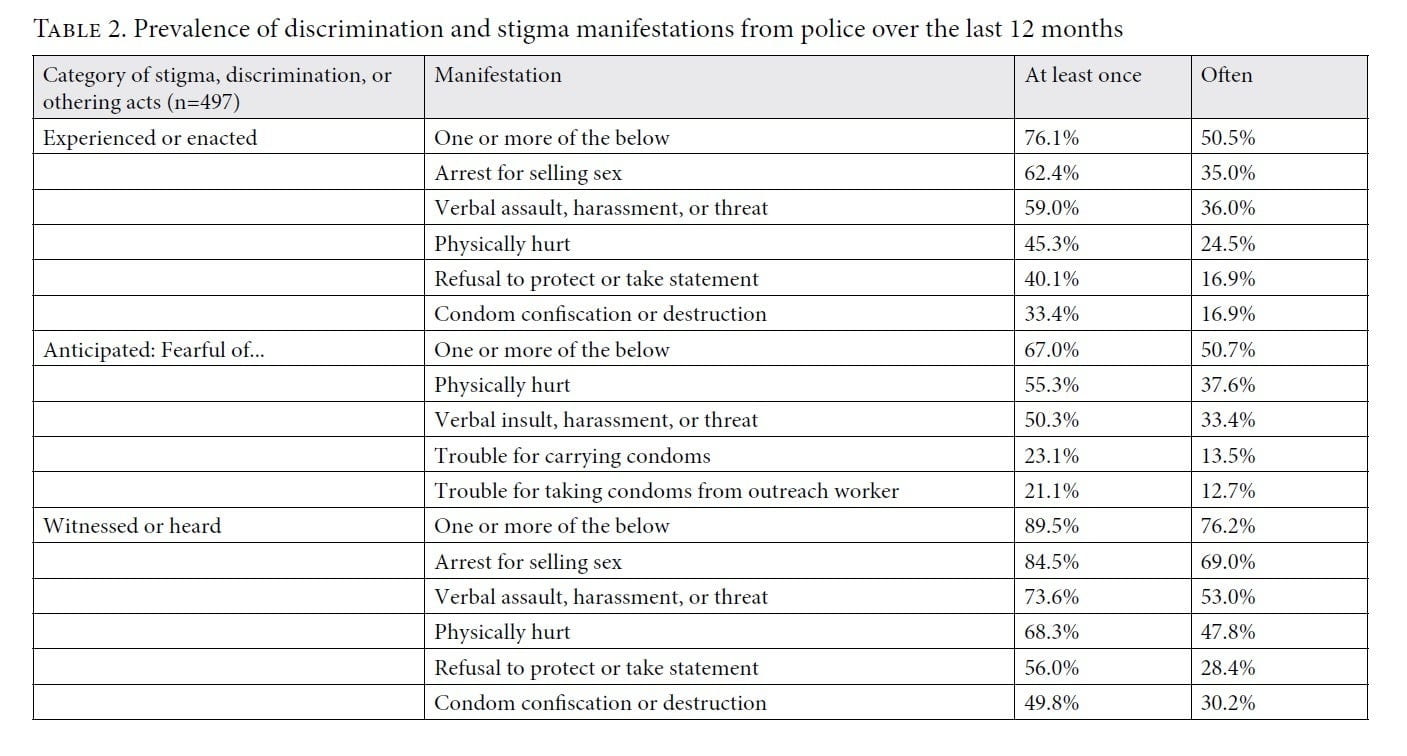
Three-quarters of respondents experienced one or more manifestations of discriminatory and othering acts (experienced stigma) by police in the past year, with 50% reporting often experiencing at least one manifestation in the past 12 months (table 2). The most common manifestations were arrest (62.4% at least once; 35.0% often), verbal abuse (59.0% at least once; 36.0% often), and physical abuse (45.3% at least once; 24.5% often). Forty percent reported at least one instance of police refusal to take the respondent’s statement or render protection. Two-thirds of respondents were fearful of one or more manifestation in the prior year. The most common anticipated manifestations were physical abuse (55.3% at least once; 37.6% often), verbal abuse (50.3% at least once; 33.4% often), and fearing trouble with police or askaris for carrying condoms (23.1% at least once; 13.5% often). Ninety percent of respondents reported witnessing or hearing about one or more manifestation, including, most frequently, arrest (84.5% at least once; 69.0% often), verbal abuse (73.6% at least once; 53.0% often), and physical abuse (68.3% at least once; 47.8% often).
Associations with avoidance and delay of health services
As respondents reported increased witnessed or heard manifestations, avoidance or delay of general healthcare services monotonically increased. Those reporting the highest level had 2.7 times the odds of delay or avoidance (95% CI 1.1–6.6) in the fully adjusted model (supplement 2). This corresponds to a 20.0 percentage point (95% CI 0.7–39.3) increase in avoidance or delay compared to those reporting no witnessed or heard manifestations (figure 1). Respondents reporting the highest level of discrimination and othering acts (experienced stigma) had 2.2 times the odds (95% CI 1.0–4.7) of avoiding or delaying general health services in the fully adjusted model, but the association was only marginally significant (p=0.055).
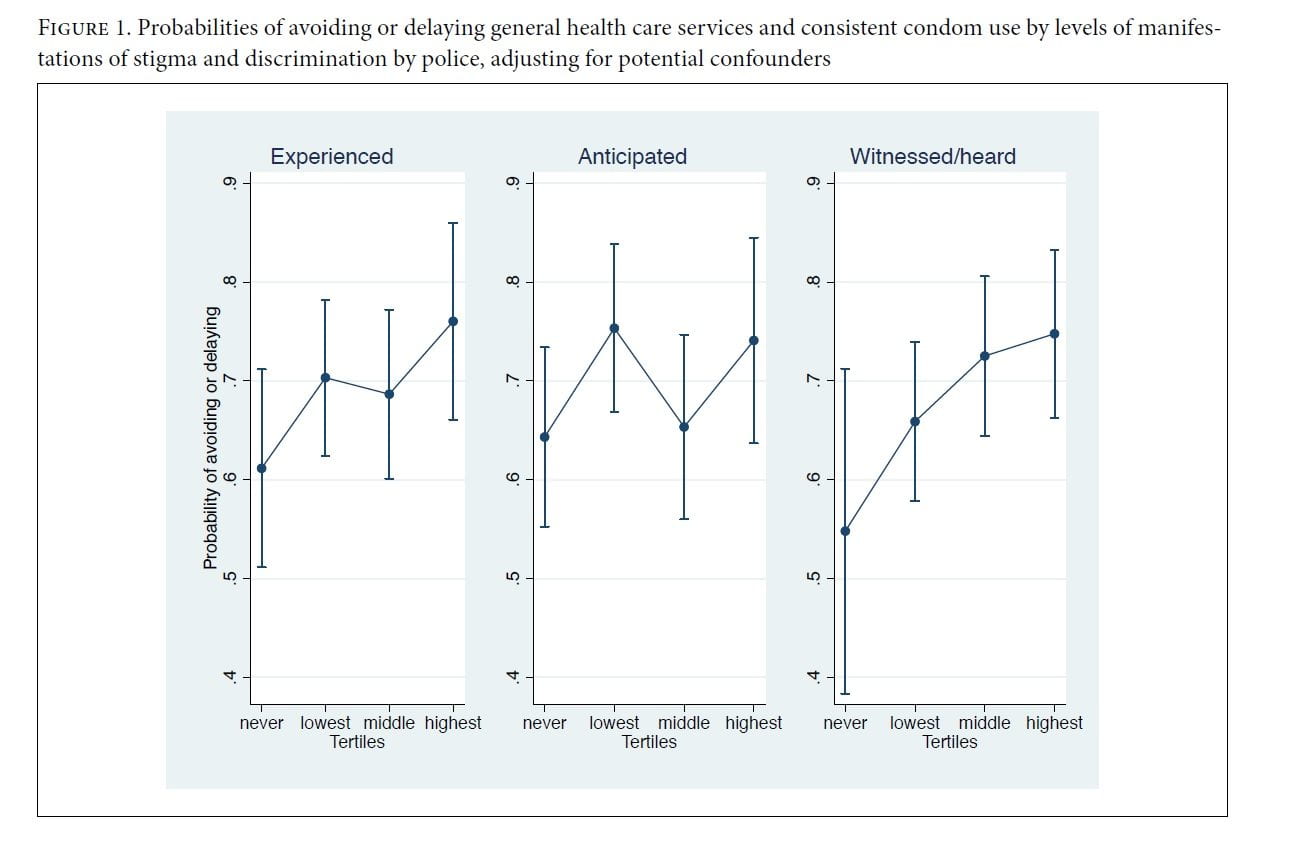
Though overall levels of experienced and witnessed/heard manifestations were associated with greater avoidance or delay of services, the only specific conduct that was by itself associated with delay or avoidance of health care services was police refusal to protect or take a statement from sex workers. In the fully adjusted model, those often experiencing this form of conduct had 2.6 times the odds (95% CI 1.3–5.4) of avoidance or delay than those who had never experienced it, which corresponds to an increase of 17.8 percentage points (95% CI 6.0–29.6). Those who often witnessed or heard about refusals to protect or take statements had 1.8 times the odds (95% CI 1.0–3.4) of avoidance or delay, corresponding to a 11.7 percentage point (95% CI 0.3–23.2) increase.
Associations with condom usage
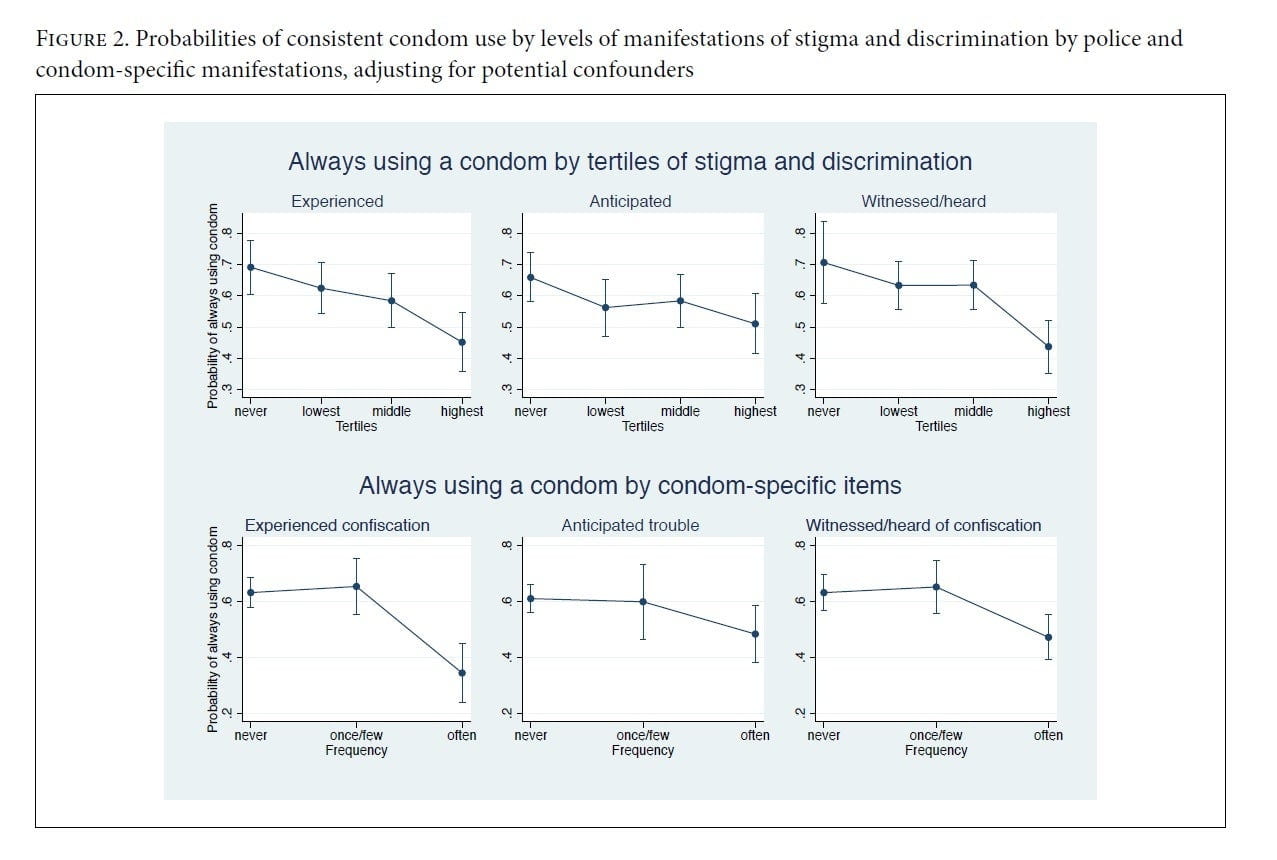
Adjusting for confounders, women in the highest category of experienced acts of discrimination or other othering acts from police had one-third the odds (OR=0.32, 95% CI 0.17–0.62) of always using a condom over the previous 12 months, which corresponds to a reduction of 24.0 percentage points (95% CI 10.6–37.3) (figure 2). The highest category of witnessed or heard manifestations was associated with a similar reduction (OR=0.28, 95% CI 0.12–0.64), corresponding to a reduction of 26.9 percentage points (95% CI 10.8–43.0); for anticipated manifestations, the odds ratio was 0.50 (95% CI 0.27–0.92), corresponding to a reduction of 14.8 percentage points (95% CI 1.8–27.8).
Women who experienced police confiscation of condoms “often” in the last 12 months had about one-quarter the odds of always using condoms than those who never experienced confiscation in the fully adjusted model (OR=0.26, 95% CI 0.15–0.47) (supplement 2). This corresponds to a reduction of 28.8 percentage points (95% CI 16.6–40.9) (figure 2). Among those who often witnessed or heard about police confiscating condoms, the odds of use were about half (OR=0.48, 95% CI 0.29–0.79), corresponding to a reduction of 16.0 percentage points (95% CI 5.1–26.9). Among those often anticipating trouble, the odds ratio of always using a condom was 0.56 (95% CI 0.33–0.95), corresponding to a reduction of 12.7 percentage points (95% CI 1.1–24.3).
Path analysis for condom usage met generally accepted guidelines for model fit (supplement 2). Often experiencing condom confiscation was directly associated with being 28.1 percentage points (95% CI 16.3–39.9) less likely to always use condoms and 15.1 percentage points (95% CI 2.5–27.7) more likely to often anticipate trouble with police. Similarly, those who often heard about or witnessed confiscation were 15.0 percentage points (95% CI 5.1–24.9) more likely to often anticipate trouble. However, there was no independent direct association between anticipated trouble with police and reduced condom use.
In all models, unadjusted results were similar to the fully adjusted results. There was a high degree of concordance between scores based on summing items and factor scores based on polychoric correlations. Estimates did not change meaningfully in a robustness check when categories were based on the factor scores (supplement 2).
Discussion
This study documents that Kenyan female sex workers encounter widespread acts by Kenyan police that constitute discrimination, abuse, and othering acts that are manifestations of stigma. Most respondents reported experiencing at least one manifestation, and virtually all had witnessed or heard of such acts from others. Those who had experienced, witnessed, or heard the highest levels of manifestations were markedly more likely to avoid or delay general health care services that they reported needing. Adjusting for confounders, respondents who often experienced police confiscation of condoms were 25 percentage points less likely to consistently use condoms.
Our findings are broadly consistent with existing research. Prior studies have documented that discriminatory and othering acts by police is a common experience for sex workers in sub-Saharan Africa.[26] A few studies find that negative interactions with police are associated with more inconsistent condom use.[27] In particular, studies from sub-Saharan Africa provide evidence that police harassment leads to hurried condom negotiation and sex workers being less likely to carry condoms.[28] There is relatively little research on the links between such manifestations by police and general health care utilization, a gap this study helps fill. Further, few studies examine anticipated or witnessed/heard stigma and discrimination among sex workers, especially regarding police, though several existing studies have found anticipated and witnessed/heard manifestations from police to be extensive across contexts.[29]
Much of the conduct reported by respondents in this study are per se violations of Kenyan constitutional law and international human rights law. At minimum, we document acts against sex workers that are violations of the following Kenyan constitutional provisions:
- Article 29(c)’s guarantee of the “right not to be subjected to any form of violence from either public or private sources” is violated by physical violence perpetrated by police. In a case decided under Kenya’s pre-2010 Constitution—but which made clear that comparable rights exist under the revised Constitution—the Kenyan state is liable for “acts … directly perpetrated against [victims] by the police.”[30]
- Article 29(f)’s protection from being “treated or punished in a cruel, inhuman, or degrading manner” is violated by both acts of physical violence and severe verbal abuse.[31]
- Article 31(b)’s guarantee of a “right to privacy, which includes the not to have their person … searched [and] possessions seized,” is likely violated by the unwarranted confiscation of condoms and predicate harassment.[32]
- Article 28’s guarantee that “every person has inherent dignity and the right to have that dignity respected and protected” is likely violated by all of the above acts, as well as police refusal to take statements from and render protection to female sex workers.[33] While this right is not fully defined in Kenyan law, there is precedent that both humiliation and the refusal to provide “care and attention” by those with a duty of care violates article 28.[34] Further, while government liability for failure to protect from third parties’ misconduct is limited in Kenyan case law, “where a report is made … and the police without any justifiable reason refuse to act … they have abdicated their duty to protect.”[35]
Sections 153 and 154 of the Kenyan Penal Code—part of its provisions on “offenses against morality”—make living on the earnings of sex work a felony.[36] The criminalization of sex work has repeatedly been identified by UNAIDS as a driver of HIV risk among sex workers, as well as giving police cover to engage in abuse.[37] It is an actionable form of discrimination that both results from and causes further stigma and discrimination. As we identify in this paper, manifestations of stigma and discrimination by police are associated both with decreased health care utilization and decreased consistent condom use. As evidenced by the finding that police refusal to take statements from or render protection to sex workers was individually predictive of delayed and avoided health services, it is likely that police refusal to protect magnifies the effect of discrimination and stigma by private actors.[38] The nexus between criminalization, police misconduct, and increased health risk renders criminalization inconsistent with Kenya’s constitutional article 43(1), which enshrines the “right to the highest attainable standard of health.”[39] While this study is cross-sectional and therefore cannot directly establish a causal relationship between police conduct and health outcomes, there are empirical and theoretical grounds for inferring causality.[40]
Additionally, while our analysis focuses on the protection of rights that are actionable under the Kenyan Constitution, police conduct violates comparable proportions of international agreements to which Kenya is a state party and which Kenya automatically gives effect in its domestic law, including the International Covenant on Civil and Political Rights, the Convention on the Elimination of All Forms of Discrimination against Women, the African Charter on Human and Peoples’ Rights, and the International Covenant on Economic, Social, and Cultural Rights.[41] More specifically, we note that verbal and physical harassment and violence by police targeted to sex workers violate the rights to security, dignity, freedom from inhuman and degrading treatment, and nondiscrimination.[42] To the extent that police misconduct against sex workers occurs without redress, it also violates rights to equal justice. Refusal by police to take statements and to protect sex workers violates the rights to personal security and to dignity.[43] The criminalization of sex work, which leads to sex workers being arrested, criminalizes voluntary and consensual sexual activity and further violates the rights to privacy and to personal autonomy, and, as noted above, the confiscation of condoms violates the right to health.[44]
Reducing discrimination against sex workers and those manifestations of stigma identified in this and other studies will require multifaceted interventions focusing on law reform, economic and social empowerment, and norm changes within police agencies. We note that discrimination and other human rights violations are a cause of further societal stigma, and the effective enforcement of international and domestic human rights law is critical. Similarly, we note that the types of conduct documented in this study are endpoints of the processes by which sex workers are marked and othered by society, so addressing stigma as a root cause of rights violations is also important. Strong evidence suggests that the decriminalization of sex work would reduce rights violations by police by reducing opportunities for abuse and improving the ability of sex workers to organize for their own protection.[45] Indeed, limited evidence from Senegal suggests that the legalization of sex work there has improved access to health services and reduced rights violations.[46]
Several studies suggest that partnerships between police and sex worker organizations can reduce harm, but creating such partnerships likely requires policy change and buy-in from police leadership.[47] Successful interventions in India have included advocacy with senior police officials as a critical component.[48] In particular, interventions should be multilevel, including components such as changing policy and law, training police, providing awareness to media (which can increase police accountability), and empowering sex workers.[49] Though not focused on police, we note that successful interventions to reduce stigma in health care settings in sub-Saharan Africa have been successful when employing a similar whole-of-institution approach.[50] The mobilization of sex workers as advocates for their own right has been particularly successful in India, though criminalization often poses a substantial barrier to mobilization.[51] Collectivization has been found to reduce rights violations and improve agency and resilience in African settings where sex work remains criminalized.[52] There is a vital need for more research on interventions to reduce discrimination and stigma and its manifestations by police, particularly in sub-Saharan Africa.
This study has a number of limitations. First, our data are cross-sectional, so the time-order between explanatory and outcome variables cannot be conclusively established and reverse causation cannot be excluded. However, existing literature and theoretical expectations make it more likely that police misconduct leads to less health care utilization and condom use than vice versa. Longitudinal studies to elucidate these relationships more deeply would be valuable. Second, respondents were recruited through sex worker support organizations, so our participants may have better-than-average access to health and social services than sex workers who are not linked to support organizations. Because we likely failed to equivalently sample sex workers most vulnerable to discrimination and manifestations of stigma, we likely underestimate their prevalence and may also underestimate the strength of its association with health care and condom use outcomes. Third, our sample of respondents living with HIV was too small to examine HIV treatment outcomes or investigate whether HIV status is an effect modifier, and there is likely some degree of misclassification of HIV status in our data because it is both self-reported and sensitive. Finally, all data are self-reported, so there is a risk of response biases. We aimed to reduce this risk through the use of carefully screened and trained interviewers and through procedures and study locations that underscored respondents’ privacy.
As identified in this study, police conduct that constitutes human rights violations against sex workers is widespread in Kenya. Such misconduct is associated with worse health outcomes. It violates rights protected by Kenya’s constitution and international agreements to which Kenya is a party. The government of Kenya has a duty to protect sex workers from discrimination and stigma and its manifestations by police, to educate the public on the need to reduce stigma and its manifestations against sex workers, and to investigate allegations of legally actionable discrimination and other rights violations and hold police accountable.
Appendices
Supplement 1: Survey Instrument. Available at https://perma.cc/W6V6-2SLJ.
Supplement 2: Supplemental analyses, data tables, and figures. Available at https://perma.cc/9K4Z-LHZ2.
David Kuria Mbote is an independent researcher and Director at the Kuria Foundation for Social Enterprise, Nairobi, Kenya.
Laura Nyblade is a fellow and Senior Technical Advisor, Stigma and Discrimination, RTI International, Washington, DC, USA.
Caroline Kemunto is Programs Manager for Survivors Organisation, Busia, Kenya.
Kayla Giger is a Public Health Analyst at RTI International, Washington, DC, USA.
Joshua Kimani is Clinical Director at Partners for Health and Development in Africa and Lecturer at the Institute of Tropical and Infectious Diseases, University of Nairobi, Nairobi, Kenya.
Pia Mingkwan is a Research Associate at RTI International, Washington, DC, USA.
Stella Njuguna is a Research Officer at the Kenya Medical Research Institute, Nairobi, Kenya.
Emmanuel Oga is a Senior Epidemiologist at RTI International, Rockville, MD, USA.
John D. Kraemer is an Associate Professor in the Department of Health Systems Administration at Georgetown University and Visiting Scholar at RTI International, Washington, DC, USA.
Please address correspondence to John Kraemer. Email: jdk32@georgetown.edu.
Competing interests: None declared.
Copyright © 2020 Mbote, Nyblade, Kemunto, Giger, Kimani, Mingkwan, Njuguna, Oga, and Kraemer. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Committee on Economic, Social and Cultural Rights, General Comment No. 20, Non-discrimination in Economic, Social and Cultural Rights, UN Doc. E/C.12/GC/20 (2009).
[2] B. G. Link and J. C. Phelan, “Conceptualizing stigma,” Annual Review of Sociology 27/1 (2001), pp. 363–385; J. C. Phelan, J. W. Lucas, C. L. Ridgeway, and C. J. Taylor, “Stigma, status, and population health,” Social Science and Medicine 103 (2014), pp. 15–23.
[3] See, e.g., Brown v. Board of Education of Topeka, 347 U.S. 483 (1954); A. F. Halaby and S. R. McAllister, “An analysis of the Supreme Court’s reliance on racial ‘stigma’ as a constitutional concept in affirmative action cases,” Michigan Journal of Race and Law 2 (1997), pp. 235–282.
[4] J. H. Ely, Democracy and distrust: A theory of judicial review (Cambridge, MA: Harvard University Press, 1980).
[5] D. K. Mbote, T. G. M. Sandfort, E. Waweru, and A. Zapfel, “Kenyan religious leaders’ views on same-sex sexuality and gender nonconformity: Religious freedom versus constitutional rights,” Journal of Sex Research 55 (2018), pp. 630–641; K. R. Eyer, “That’s not discrimination: American belief and the limits of anti-discrimination law,” Minnesota Law Review 96 (2012), pp. 1275–1362.
[6] E. Goffman, Stigma: Notes on the management of a spoiled identity (Englewood Cliffs: Prentice-Hall, 1963).
[7] J. C. Kane, M. A. Elafros, S. M. Murray, et al., “A scoping review of health-related stigma outcomes for high-burden diseases in low- and middle-income countries,” BMC Medicine 17/1 (2019), p. 17.
[8] M. R. Decker, A.-L. Crago, S. K. H. Chu, et al., “Human rights violations against sex workers: Burden and effect on HIV,” Lancet 385/9963 (2015), pp. 186–199; UNAIDS, Judging the epidemic: A judicial handbook on HIV, human rights and the law (2013); J. Okal, M. F. Chersich, S. Tsui, et al., “Sexual and physical violence against female sex workers in Kenya: A qualitative enquiry,” AIDS Care 23/5 (2011), pp. 612–618.
[9] Decker et al. (2015, see note 8); International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966).
[10] M. L. Hatzenbuehler, J. C. Phelan, and B. G. Link, “Stigma as a fundamental cause of population health inequalities,” American Journal of Public Health 103/5 (2013), pp. 813–821.
[11] G. L. Birbeck, V. Bond, V. Earnshaw, et al., “Advancing health equity through cross-cutting approaches to health-related stigma,” BMC Medicine 17/1 (2019), p. 40.
[12] L. Platt, P. Grenfell, R. Meiksin, et al., “Associations between sex work laws and sex workers’ health: A systematic review and meta-analysis of quantitative and qualitative studies,” PLOS Medicine 15/12 (2018), p. e1002680; J. T. Erausquin, E. Reed, and K. M. Blankenship, “Change over time in police interactions and HIV risk behavior among female sex workers in Andhra Pradesh, India,” AIDS and Behavior 19/6 (2015), pp. 1108–1115; M. R. Decker, A. L. Wirtz, S. D. Baral, et al., “Injection drug use, sexual risk, violence and STI/HIV among Moscow female sex workers,” Sexually Transmitted Infections 88/4 (2012), pp. 278–283.
[13] UNAIDS (2013, see note 8); UNAIDS, UNAIDS guidance note on HIV and sex work (2012).
[14] F. Scorgie, K. Vasey, E. Harper, et al., “Human rights abuses and collective resilience among sex workers in four African countries: A qualitative study,” Globalization and Health 9/1 (2013), p. 33.
[15] Platt et al. (see note 12).
[16] S. Stahlman, J. R. Hargreaves, L. Sprague, et al., “Measuring sexual behavior stigma to inform effective HIV prevention and treatment programs for key populations,” JMIR Public Health and Surveillance 3/2 (2017), p. e23; A. L. Grosso, S. C. Ketende, S. Stahlman, et al., “Development and reliability of metrics to characterize types and sources of stigma among men who have sex with men and female sex workers in Togo and Burkina Faso,” BMC Infectious Diseases 19/1 (2019), p. 208; S. Lim, S. Peitzmeier, C. Cange, et al., “Violence against female sex workers in Cameroon: Accounts of violence, harm reduction, and potential solutions,” Journal of Acquired Immune Deficiency Syndromes 68/Suppl. 2 (2015), pp. S241–S247; C. E. Oldenburg, K. B. Biello, D. Colby, et al., “Stigma related to sex work among men who engage in transactional sex with men in Ho Chi Minh City, Vietnam,” International Journal of Public Health 59/5 (2014), pp. 833–840; Decker et al. (2015, see note 8); L. Nyblade, A. Reddy, D. Mbote, et al., “The relationship between health worker stigma and uptake of HIV counseling and testing and utilization of non-HIV health services: The experience of male and female sex workers in Kenya,” AIDS Care 29/11 (2017), pp. 1364–1372.
[17] J. M. Mann, L. Gostin, S. Gruskin, et al., “Health and human rights,” Health and Human Rights 1/1 (1994), pp. 6–23.
[18] Kenya National AIDS Control Council, Kenya HIV estimates report 2018 (2018); H. Musyoki, T. A. Kellogg, S. Geibel, et al., “Prevalence of HIV, sexually transmitted infections, and risk behaviours among female sex workers in Nairobi, Kenya: Results of a respondent driven sampling study,” AIDS and Behavior 19 Suppl. 1 (2015), pp. S46–S58.
[19] W. O. Odek, G. N. Githuka, L. Avery, et al., “Estimating the size of the female sex worker population in Kenya to inform HIV prevention programming,” PLOS ONE 9/3 (2014), p. 89180.
[20] L. White, The comforts of home: Prostitution in colonial Nairobi (Chicago: University of Chicago Press, 1990).
[21] National AIDS and STI Control Programme, Third national behavioural assessment of key populations in Kenya: Polling booth survey report (2018); P. Bhattacharjee, G. J. Morales, T. M. Kilonzo, et al., “Can a national government implement a violence prevention and response strategy for key populations in a criminalized setting? A case study from Kenya,” Journal of the International AIDS Society 21/ Suppl. 5 (2018), p. e25122.
[22] Nyblade et al. (see note 16); L. Nyblade, D. Mbote, C. Barker, et al., Impact of stigma on utilization of health services among sex workers in Kenya (Washington, DC: Futures Group, Health Policy Project, 2015).
[23] Nyblade et al. (see note 16).
[24] A. M. Gadermann, M. Guhn, and B. D. Zumbo, “Estimating ordinal reliability for Likert-type and ordinal item response data: A conceptual, empirical, and practical guide,” Practical Assessment, Research and Evaluation 17/3 (2012), p. 13.
[25] Nyblade et al. (see note 16).
[26] K. A. Muldoon, M. Akello, G. Muzaaya, et al., “Policing the epidemic: High burden of workplace violence among female sex workers in conflict-affected northern Uganda,” Global Public Health 12/1 (2017), pp. 84–97; J. Coetzee, G. E. Gray, and R. Jewkes, “Prevalence and patterns of victimization and polyvictimization among female sex workers in Soweto, a South African township: A cross-sectional, respondent-driven sampling study,” Global Health Action 10/1 (2017), p. 1403815; M. Richter, M. F. Chersich, J. Vearey, et al., “Migration status, work conditions and health utilization of female sex workers in three South African cities,” Journal of Immigrant and Minority Health 16/1 (2014), pp. 7–17; K. A. Muldoon, “A systematic review of the clinical and social epidemiological research among sex workers in Uganda,” BMC Public Health 15 (2015), p. 1226.
[27] Erausquin et al. (see note 12).
[28] Muldoon et al. (see note 26); M. Erickson, S. M. Goldenberg, M. Ajok, et al., “Structural determinants of dual contraceptive use among female sex workers in Gulu, northern Uganda,” International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics 131/1 (2015), pp. 91–95.
[29] Stahlman et al. (see note 16); Grosso et al. (see note 16); Lim et al. (see note 16); Oldenburg et al. (see note 16).
[30] Constitution of Kenya (2010); Charles Murigu Murithii and 2 Others v. Attorney General (2015 eKLR).
[31] Constitution of Kenya (2010); J O O (also known as J M) v. Attorney General and 6 Others (2018 eKLR).
[32] Constitution of Kenya (2010); Standard Newspapers Limited and Another v. Attorney General and 4 Others (2013 eKLR).
[33] Constitution of Kenya (2010).
[34] R. Ebert, and R. M. J. Oduor, “The concept of human dignity in German and Kenyan constitutional law,” Thought and Practice 4/1 (2012), pp. 43–73; J O O (also known as J M) v. Attorney General and 6 Others (2018 eKLR); M A O and Another v. Attorney General and 4 Others (2015 eKLR).
[35] Florence Amunga Omukanda and Another v. Attorney General and 2 Others (2016); Charles Murigu Murithii and 2 Others v. Attorney General (2015 eKLR).
[36] Penal Code of Kenya (2012), ch. 63.
[37] UNAIDS (2013, see note 8).
[38] K. H. A. Footer, J. N. Park, S. T. Allen, et al., “Police-related correlates of client-perpetrated violence among female sex workers in Baltimore City, Maryland,” American Journal of Public Health 109/2 (2018), pp. 289–295.
[39] Constitution of Kenya (2010).
[40] UNAIDS (2012, see note 13); K. Shannon, A.-L. Crago, S. D. Baral, et al., “The global response and unmet actions for HIV and sex workers,” Lancet 392/10148 (2018), pp. 698–710; M. F. Chersich, S. Luchters, I. Ntaganira, et al., “Priority interventions to reduce HIV transmission in sex work settings in sub-Saharan Africa and delivery of these services,” Journal of the International AIDS Society 16/1 (2013), p. 17980; E. Albright and K. D’Adamo, “Decreasing human trafficking through sex work decriminalization,” AMA Journal of Ethics 19/1 (2017), pp. 122–126; K. Shannon and J. Csete, “Violence, condom negotiation, and HIV/STI risk among sex workers,” JAMA 304/5 (2010), pp. 573–574; K. N. Deering, A. Amin, J. Shoveller, et al., “A systematic review of the correlates of violence against sex workers,” American Journal of Public Health 104/5 (2014), pp. e42–e54; Z. Lazzarini, S. Bray, and S. Burris, “Evaluating the impact of criminal laws on HIV risk behavior,” Journal of Law, Medicine and Ethics: A Journal of the American Society of Law, Medicine and Ethics 30/2 (2002), pp. 239–253.
[41] M A O and Another v. Attorney General and 4 Others (2015 eKLR); N. W. Orago, “The 2010 Kenyan Constitution and the hierarchical place of international law in the Kenyan domestic legal system: A comparative perspective,” African Human Rights Law Journal 13 (2013), pp. 415–440; Decker et al. (2015, see note 8); Shannon et al. (see note 40); D. Kerrigan, C. E. Kennedy, R. Morgan-Thomas, et al., “A community empowerment approach to the HIV response among sex workers: Effectiveness, challenges, and considerations for implementation and scale-up,” Lancet 385/9963 (2015), pp. 172–185.
[42] Human Rights Watch, Off the streets: Arbitrary detention and other abuses against sex workers in Cambodia (New York: Human Rights Watch, 2010).
[43] Human Rights Watch, Capitol offense: Police mishandling of sexual assault cases in the District of Columbia (New York: Human Rights Watch, 2013).
[44] M. H. Wurth, R. Schleifer, M. McLemore, et al., “Condoms as evidence of prostitution in the United States and the criminalization of sex work,” Journal of the International AIDS Society 16 (2013), p. 18626.
[45] Platt et al. (see note 12).
[46] C. Mgbako and L. A. Smith, “Sex work and human rights in Africa,” Fordham International Law Journal 33/4 (2010), pp. 1178–1220.
[47] B. Tenni, J. Carpenter, and N. Thomson, “Arresting HIV: Fostering partnerships between sex workers and police to reduce HIV risk and promote professionalization within policing institutions; A realist review,” PLOS ONE 10/10 (2015), p. e0134900.
[48] P. Bhattacharjee, S. Isac, L. M. McClarty, et al., “Strategies for reducing police arrest in the context of an HIV prevention programme for female sex workers: Evidence from structural interventions in Karnataka, South India,” Journal of the International AIDS Society 19/4 Suppl. 3 (2016), p. 20856.
[49] T. S. Beattie, P. Bhattacharjee, S. Isac, et al., “Declines in violence and police arrest among female sex workers in Karnataka state, south India, following a comprehensive HIV prevention programme,” Journal of the International AIDS Society 18 (2015), p. 20079; E. Argento, S. Reza-Paul, R. Lorway, et al., “Confronting structural violence in sex work: Lessons from a community-led HIV prevention project in Mysore, India,” AIDS Care 23/1 (2011), pp. 69–74.
[50] L. Nyblade, N. A. Addo, K. Atuahene, et al., “Results from a difference-in-differences evaluation of health facility HIV and key population stigma-reduction interventions in Ghana,” Journal of the International AIDS Society 23 (2020).
[51] M. R. Biradavolu, S. Burris, A. George, et al., “Can sex workers regulate police? Learning from an HIV prevention project for sex workers in southern India,” Social Science and Medicine (1982) 68/8 (2009), pp. 1541–1547; Kerrigan et al. (see note 41).
[52] Scorgie et al. (see note 14).