Establishing Good Practice for Human Rights-Based Approaches to Mental Health Care and Psychosocial Support in Kenya
Volume 22/2, December 2020, pp 139 – 154
Faraaz Mahomed, Jacqueline Bhabha, Michael Ashley Stein, and Dainius Pūras
Abstract
A human rights-based approach (HRBA) to health has long been seen as an important way in which to address public health needs in a manner that is equitable and conducive to social justice. Yet the actual content of an HRBA to health remains unspecific, and therefore implementation remains heterogeneous. This situation is even more challenging in the field of mental health, where human rights considerations are particularly complex and have emerged out of a history of myriad violations. Even when research has been conducted into mental health, it has focused predominantly on the Global North, raising questions of contextual and cultural relevance. Accordingly, this study examined the issue from the perspectives of stakeholders in Kenya who consider their work or the services they use to be rights based. It explored the key principles and interventions deemed to constitute an HRBA to mental health care and psychosocial support, the perceived benefits of such approaches, and the main barriers and supports relevant for implementation. The results produced seven key principles and corresponding interventions. Among other things, it highlighted the importance of economic well-being and self-efficacy, as well as the reduction of barriers to implementation, such as stigma and lack of adequate resourcing. Two key tensions were apparent—namely, the un/acceptability of coercion and the role of traditional and faith-based modalities in an HRBA to mental health care and psychosocial support.
Introduction
For over 60 years, the health rights community has advanced the idea of an HRBA to attain health outcomes. Article 12(1) of the International Covenant on Economic, Social and Cultural Rights, a treaty that has been ratified by 171 countries, asserts the right of all people to the highest attainable standard of physical and mental health.[1] Scholars have subsequently noted that
the public health community has come to a largely shared perspective that a human rights lens on health helps shape understandings of who is disadvantaged and who is not; who is included and who is ignored; and whether a given disparity is merely a difference or an actual injustice.[2]
Despite this “largely shared perspective,” a common and universally accepted definition of what constitutes an HRBA has not been articulated. General Comment 14 by the Committee on Economic, Social and Cultural Rights provides interpretive guidance on the content of the right and establishes a now commonly utilized “AAAQ” framework, referring to standards of availability, accessibility, acceptability, and quality.[3] Drawing on this and other instruments, the World Health Organization and the Office of the United Nations High Commissioner for Human Rights have adopted an HRBA consisting of the following elements: availability, accessibility, acceptability, quality, nondiscrimination, participation, and accountability.[4]
While these principles provide some guidance, it has been noted that such instruments adopt a “lowest common denominator approach, privileging consensus over specificity … [Their] general nature has made it difficult to operationalize.”[5] Content and specificity are required to actualize HRBAs via a focus on interventions as well as principles. Moreover, while HRBAs to health services have been a central preoccupation of public health approaches, it has been suggested that an HRBA to health may extend beyond the health system to broader questions of inequity, policy, and social exclusion:
Human rights-based approaches, by their nature, cut across sectors and draw from multiple strategies. They might require legal or policy reform to create “enabling” environments; the identification and capacity-building of “rights holders”; comprehensive programs for education, health, and human rights literacy, advocacy, and empowerment; or the elaboration of more participatory accountability and oversight mechanisms.[6]
Efforts to address health concerns from a rights perspective, therefore, may approach these challenges through avenues that address inequality, promote inclusion, and foster accountability, at times outside the realm of the health system. Officials in health and other associated systems should also pay due to attention to the right to benefit from scientific endeavor on an equal basis.[7] This is especially true in the present day, as the COVID-19 pandemic lays bare the many ways in which health rights are affected by issues of equity, inclusion, and accountability, and as activists, advocates, and scholars grapple with the question of how to imagine a more just world, including but not limited to the realm of health.
Mental health and human rights
Considerable human rights violations have been perpetrated within mental health systems.[8] These have ranged from widespread neglect of people with lived experience of mental health challenges (also referred to as psychosocial disabilities) to incarceration and coercive treatments, often without any clinical validity.[9] Problematic beliefs about mental health have been cited as some of the main drivers behind these erroneous and counterproductive ways of “caring” for people with psychosocial disabilities. These beliefs have ranged from supernatural attributions responsible for mental health conditions (that is, the belief that an individual is possessed or has been a victim of witchcraft) to conceptions of such conditions as manifestations of “feeble-mindedness.”[10] Our everyday mental health vernacular is largely derived from the Diagnostic and Statistical Manual of Mental Disorders, now in its fifth edition (DSM-5). It classifies the range of “mental disorders” and is utilized widely as a basis for providing services and for justifying insurance coverage.[11] These practices and tools have been criticized as overemphasizing the biomedical basis of mental health and offering little insight or support to address the psychological, social, cultural, spiritual, economic, and political determinants of mental health.[12]
Calls for a “human rights model” of mental health have become more vocal in recent years.[13] Against this backdrop, in 2006, the United Nations General Assembly adopted the Convention on the Rights of Persons with Disabilities (CRPD), the first comprehensive treaty on disability rights.[14] One hundred eighty-one states have ratified the CRPD, reflecting near-universal adoption.[15] In 2017, the United Nations Special Rapporteur on the rights of persons with disabilities reported that at least 32 countries were undertaking reforms to their mental health laws and policies to incorporate the paradigm advanced by the CRPD.[16]
Nevertheless, despite the emergence of rights-based mental health laws, compliance with them remains poor, particularly in low-income countries.[17] Hence “the paradigm shift to the human rights model has yet to be reflected in implementation.”[18] A review of the literature on the applied practice of HRBAs to mental health care and psychosocial support services (MHCPS) yielded just 10 studies in 2016, demonstrating the lack of a substantial body of research.[19] Strikingly, this paucity is even more glaring in low- and middle-income country contexts and contexts where sociocultural factors may be different from the Western developed world, with just two studies referring to HRBAs to mental health in these settings appearing in this review.[20] Ensuring the cultural and contextual relevance of MHCPS services can also be an issue of health quality and health acceptability in terms of the AAAQ framework referred to above. For this reason, any attempt at articulating an HRBA requires contextual specificity and sensitivity to cultural and social norms.
Bearing in mind the need for specificity of context and a clear focus on implementation, our study identified good practices in HRBAs to MHCPS services for people with psychosocial disabilities in Kenya. Recognizing that the HRBA is itself an amorphous, contextually bound concept subject to interpretation, the study’s aim was to elicit from respondents their own understanding of what an HRBA means. Using key informant interviews, we aimed to identify what, in the opinion of key stakeholders—and, prominently, people with psychosocial disabilities as mental health service users themselves—constituted the key features of rights-based MHCPS services. Similarly, we sought to identify key interventions of such an approach, along with practical barriers to and supports for implementing these interventions in the Kenyan context, where the mental health system is undergoing a transition to CRPD-aligned legislation but where mental health services remain underfunded despite their inclusion in universal health coverage provisions.[21]
Methodology
Study sites
We chose two organizations—the Kamili Mental Health Organization and the Home of Brains—as sites for this study based on their explicit orientation toward HRBAs to mental health in community-based settings. Due to space constraints, it is not possible to elaborate on the work of these organizations here, but more information is available on their respective websites and in the first author’s doctoral dissertation.[22]
Interviews
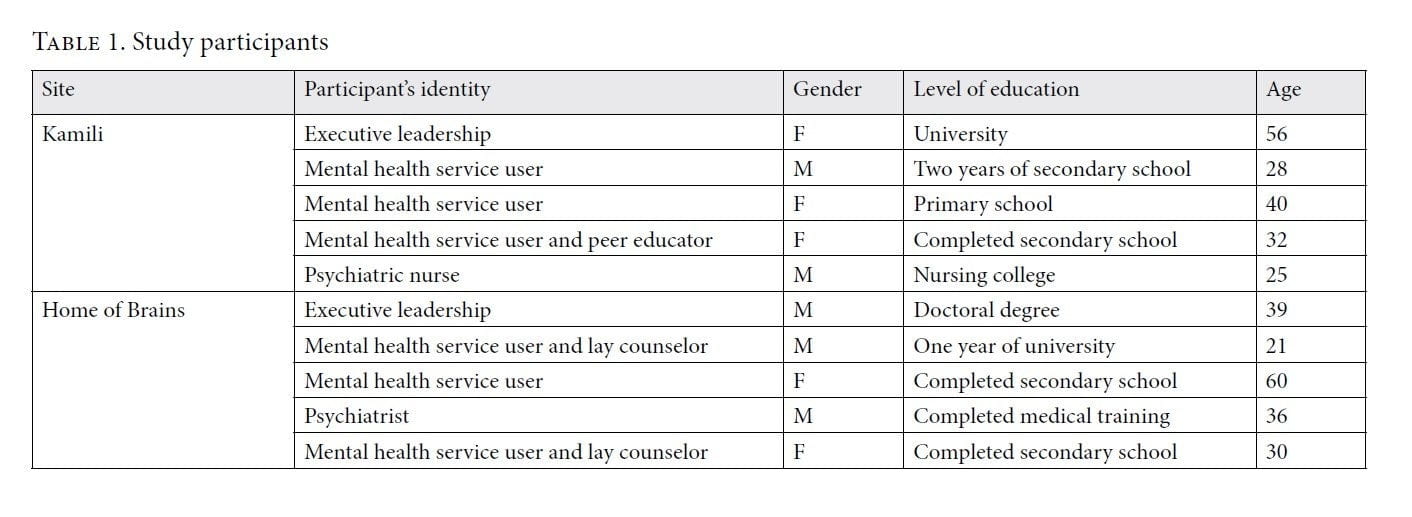
We conducted 10 interviews as part of this study. These interviews emphasized the participation of mental health service users while also considering the experiences of other key stakeholders, including implementers, clinicians, and advocates. Our sampling of key informants was purposive, utilizing the assistance of the organizations. Key informants were chosen based on three main criteria:
- Familiarity with the practices of the organization
- Diversity among interviewees (in terms of gender, educational attainment, and professional orientation or identity as a mental health service user or member of the organization’s executive leadership)
- Balance between sites (five interviews at each site)
When we approached participants, we provided them with an introduction to our study, indicating that it was an interpretivist study concerned with stakeholder perceptions of what constitutes an HRBA to mental health. We sought their verbal consent prior to the interview. Eight interviewees were fluent in English, meaning that an interpreter was not necessary. For two interviews (one at each site), the aid of an interpreter was employed, including for the consent process. We developed a semi-structured interview schedule (available from the authors) to examine the nature of interventions and the values included in an HRBA and the perceived benefits of such an approach, and we used this as a guide for the interviews. Additional probing questions included those related to issues such as the barriers faced by implementers and the resource and capacity needs for implementation of an HRBA to MHCPS services. Interviews were between 30 and 60 minutes in length and were recorded and transcribed for analysis. We then undertook a process of interpretive data analysis following Robert Elliot and Ladislav Timulak’s five-step method.[23]
The Harvard School of Public Health granted an Institutional Review Board exemption for this study (IRB18-0839).
Results
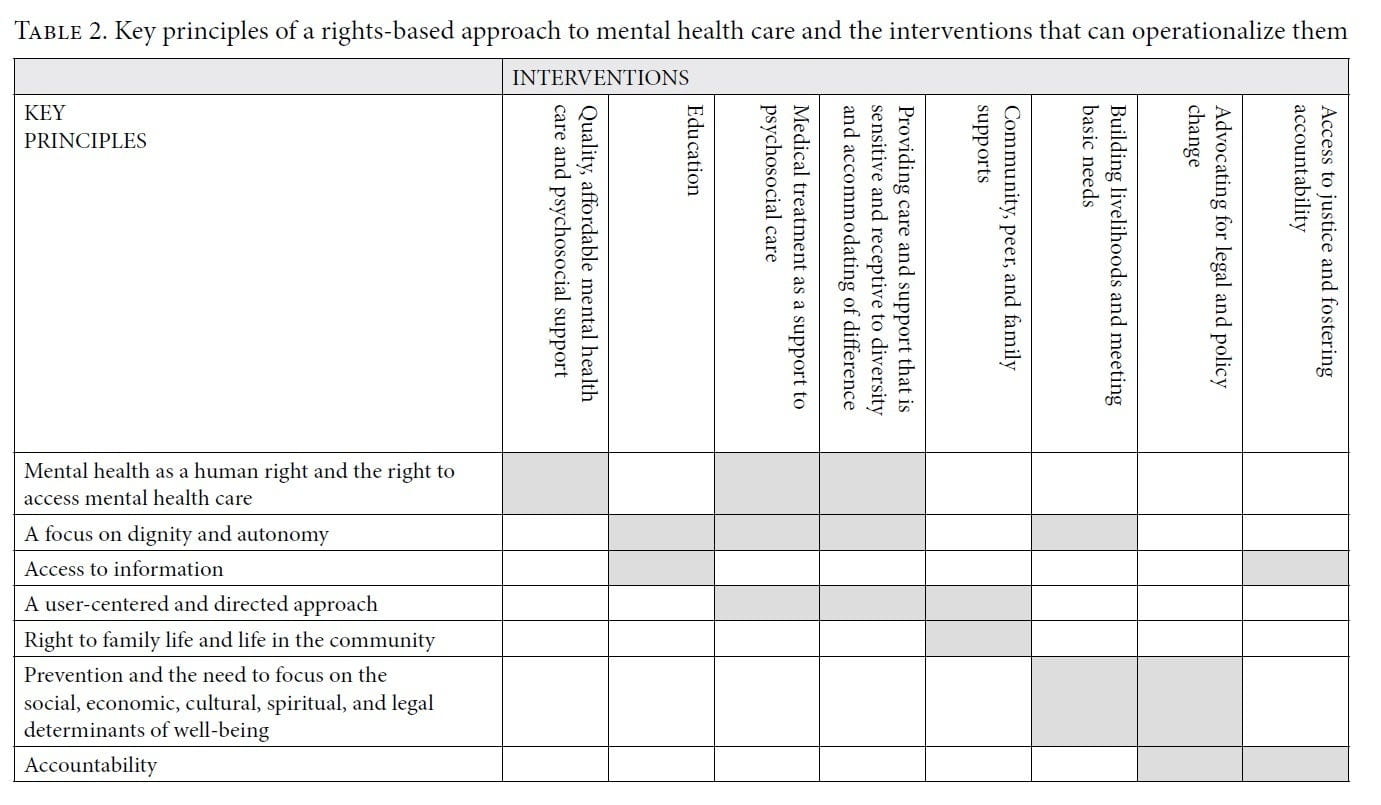
We organized the interview data into three main categories: stakeholder perspectives regarding key components of an HRBA to MHCPS (subcategorized into seven key principles and eight key interventions as outlined below); stakeholder opinions regarding the contribution and efficacy (that is, the impact) of an HRBA to MHCPS; and statements related to the barriers and supports to implementing such an approach (further subcategorized into supports and barriers).
Key principles
Mental health as a human right and the right to access mental health care. A common perception was that the experience of mental health and well-being is itself a fundamental human right (in other words, that no one, on any basis, should be faced with societal barriers to well-being). One participant noted:
The purpose is the guiding factor … we want to ensure that people are healthy and we want to meet public health goals, [but] we want also to fulfill the right to mental health itself.
An HRBA to mental health and well-being must begin from a position that mental health itself is a right and that barriers to this right (including discrimination, violence, poverty, and unemployment) must be seen as rights violations. Similarly, the factors that contribute to its realization or lack thereof are key determinants not only of well-being but also of rights realization, reflecting the importance of the indivisibility of rights.[24] One such factor mentioned several times was the cost of accessing mental health services in Kenya.
A focus on dignity and autonomy. Participants conceived of dignity in several ways, ranging from the ability to participate freely in society to the way in which an individual is perceived by others. Similarly, autonomy was a key theme in the interviews, with respondents highlighting the value of this principle for the realization of mental health and well-being and as an inalienable right.
Despite the CRPD’s assertion of equal recognition before the law (amounting to a prohibition of coercion), tensions remain in the realm of autonomy and decision making.[25] One respondent noted that she sometimes experiences difficulty in operationalizing autonomy as part of the organization’s model:
Of course autonomy and decision making are important. We are here because too many people have been locked up, but sometimes we have to … when someone is going to get hurt … we have to.
This is illustrative of the fact that tensions continue to play themselves out in the realm of autonomy and decision making. Evidently, even when organizations are purporting to implement an HRBA, they may qualify or limit a right when they feel they “have to” because of the potential risk to the mental health service user or others, despite provisions in international human rights law that prohibit limitation of the right.[26]
Access to information. Knowledge regarding human rights and mental health can significantly alter the way in which people with psychosocial disabilities are able to self-advocate or pursue their rights. This is in keeping with the principle of access to services and access to the benefits of scientific progress as part of the AAAQ framework.[27] One participant noted:
It starts with information. An [HRBA] requires that people know enough about their own rights and about their condition. Otherwise, they will not be able to make informed choices.
Another participant echoed this point:
I cannot [access] my rights if I do not know about them, and I cannot understand my mental health if I don’t know about it … The truth is that people do not know enough, and I think this is a problem, especially in the hospitals.
A user-centered and -directed approach. “User-centricity” and “user-directedness” are closely linked with the ideas of dignity and autonomy, but they also appear to manifest as a more personalized and individualized idea. As one respondent noted:
Our model is about asking the person where they are … and then finding ways to meet them there.
Another highlighted the following:
I am not getting all the same [support] that my friend is getting, and she is not getting some of the [support] that I am getting, because we need different things.
This illustrates that there is an emphasis on individualized support among respondents, aiming to “meet” mental health service users where they are and to recognize and accommodate difference. In essence, this is in keeping with the principle of acceptability as part of the AAAQ framework.[28]
Right to family life and life in the community. Speakers believed community-oriented care and support to be especially important philosophical elements of an HRBA to MHCPS. For example, one individual remarked:
Why should we be separate? We are not animals [to be kept] in a zoo … I want to be with others [in the community] … and I can take my treatment [at the organization] and still live [among them].
Respondents also noted the key role that families play in promoting, preserving, and restoring mental health. One individual noted that
the family is the first source of community. Without my family knowing and understanding my condition, I would be in a much worse position.
Prevention and the need to focus on social, economic, cultural, spiritual, and political determinants of well-being. According to participants, a focus on prevention is an important means through which to fulfill the right to mental health. When barriers to well-being are addressed, distress can be averted. One participant noted:
This is what makes a [HRBA] different … We aren’t only thinking about circumstances in treatment, we’re thinking about the right to be healthy so that treatment isn’t really necessitated.
An emphasis on the economic determinants of health in supportive interventions has, according to some respondents, a direct relationship with autonomy, as the following quotation suggests:
I am better because I have a way to feed myself and my family. I don’t have that stress anymore, it has made me feel like the person I used to be.
Similarly, another important component of an HRBA to MHCSP is the way in which societies respond to mental health conditions, with the problems of stigma and discrimination being a significant source of distress and a significant human rights violation.
Accountability. Respondents highlighted that over and above a need to ensure that laws and policies accurately reflect an HRBA, they must be implemented and invested in by officials, and the commitments made by these duty bearers must be fulfilled. Referring to impediments to accessing services because of failures in laws and policies, one participant stated:
How can we be well if there is no one that cares enough about this? [The government] doesn’t care.
In a similar vein, respondents noted that the health system, too, has a duty to be accountable to mental health service users, catering to their needs in ways that are respectful and transparent. One individual stated:
I am the beneficiary, but sometimes [doctors and nurses] don’t think they have any [duty] to me.
This is indicative of the apparent lack of accountability in traditional mental health systems, countered to some extent by more transparent approaches, expanded on as follows:
Our aim is to build the model and the care as a collective … We try to do this periodically through participatory means … It’s still a work in progress, but our aim is to be accountable and responsive.
Interventions embodying the rights-based approach to MHCSP
Quality, affordable MHCPS. In a context where financial resources are limited and the ability to access care and support is determined by economic factors, the right to health is significantly compromised. As one individual noted:
How can I pay ten thousand [Kenyan shillings] each time I come for counseling? I would not have money for food. Without [the organization], I would not be able to see a counselor.
Fundamentally, and in keeping with the principle of quality in the AAAQ framework, respondents noted that an HRBA means that service quality is not sacrificed for the sake of affordability, as demonstrated by this statement:
We appreciate the fact that we need to work within our resources, so we try to be creative and actively look for ways to be more efficient … but to change the level of attention a beneficiary receives or to deny them the same level of care that a [wealthier] person would get … that would be discrimination.
The act of being “creative” with resources in this instance means finding ways to use the facilities of the government or other agencies or to promote peer support activities that emphasize the participation and efficacy of mental health service users themselves as a viable and possibly even preferable alternative to over-reliance on specialist staff. Peer support activities can take multiple forms and reflect different models, but they share the same common factor of providing support from the perspective of someone with similar lived experience.[29] In terms of gauging the quality of services provided, one respondent stated the following:
We promote quality care in a number of ways, using our networks to continuously train staff, providing beneficiaries with the opportunity to change their treatment plans if they feel they are not effective.
A key part of the work is therefore continuous refinement of the HRBA to ensure quality service provision and democratic decision making concerning treatment and support options. This sentiment comports with the right to benefit from scientific endeavor, as noted above.[30]
Community, peer, and family supports. Community-based mental health models eschew the possibility that people with psychosocial disabilities might be institutionalized or otherwise removed from their communities. This, according to one respondent, is a direct manifestation of an HRBA:
We aren’t taking people away from [their communities]. We are coming to them because they have a right to live with their people.
Community-based interventions, however, are also about actually reaching the wider community, providing education that can help combat stigma, mobilizing resources to ensure service delivery, and addressing living conditions that might contribute to distress. Similarly, respondents spoke about the role of family supports, because often the family is the most direct determinant of an individual’s well-being, a sentiment that is also reflected in the literature.[31] As one participant said:
The family have a right to mental health too, and they can benefit from therapies or education. This has direct benefit to our beneficiary too. It’s a sort of virtuous cycle.
Peer support was also mentioned as a key intervention, because people living with psychosocial disabilities might utilize these activities to develop self-efficacy or might find that there are less paternalistic forms of support than traditional approaches. Peer support initiatives include group counseling, the formation of sports teams, and a collective to build autonomy and foster self-advocacy through the development of a user-led radio show produced and hosted by mental health service users. Additionally, a storytelling collaborative in the community was mentioned as one means through which mental health service users can build community. Peer supporters are volunteers in both organizations where the study was conducted.
Medical treatment as a support to psychosocial care. HRBAs, in the organizations visited, did not emphasize psychotropic medication as a preference over psychosocial supports. Instead, the organizations viewed medical treatment as one of several interrelated components of care and as a supportive mechanism for conducting other interventions. One participant noted:
We know that medicine can be an important thing … but we also know that it doesn’t really [achieve the objectives] of helping a person live a whole, happy, healthy life … For those things, there’s a lot more that needs to happen.
The assertion that “there’s a lot more that needs to happen” is also borne out in the following quote:
When you go to the clinic, they give you your tablets and they send you away. How is that going to help me [realize] my rights? I need [the medication] but I also need to be able to work.
Education. Initiatives to operationalize the right to access to information include educating people with psychosocial disabilities as well as educating communities. One participant described the nature and purpose of these interventions as follows:
Our organization sees the provision of education around mental health and the rights of service users as an avenue to foster dignity … We do this through publications, through radio shows and through direct engagement, sometimes even door-to-door engagement.
The use of peer educators is also a useful model because it ensures that people with psychosocial disabilities become self-advocates and agents of change in their communities. One peer educator stated:
As a peer educator, I can offer something that others can’t. I can speak about the experience from a perspective that a doctor can’t. The doctors don’t know how alone you feel.
Another key aspect is the incorporation of these models into formal mental health training. Supporting mental health training in universities and medical colleges can ensure that a human rights orientation is embedded in clinical practice.
Advocating for legal and policy change. Because Kenya’s mental health system is in the process of transition, there is significant interest among the organizations in question to mobilize beneficiaries to claim their rights and to develop advocacy strategies to support reforms. One respondent stated:
Our [HRBA] is a bit of a mishmash because we think that being involved in the political space is as important as being involved in service provision. Our goal is to support our clients to become involved in these processes themselves.
This suggests that mental health organizations providing care and support also naturally advocate for the incorporation of HRBAs into broader systems through, for example, advocacy to promote improved resourcing for mental health or to promote community-based services in the new mental health legislation in Kenya.
Building livelihoods and meeting basic needs. Respondents were unanimous that supporting mental health requires an emphasis on economic well-being. One individual noted:
You can’t claim that you care about rights and then not pay attention to people’s right to work, or their right to learn and become self-sufficient, or their right to food. How can anyone be mentally well if they have no source of income to feed themselves and their families?
Efforts to provide support for receiving an education, to provide work opportunities or other sources of income, and to promote food security can all be important and useful ways in which to promote well-being. Another speaker, applauding the cultivation of a community vegetable garden tended by mental health service users, noted:
The thing that I used to worry about the most, and that made me sick was how am I going to feed my children?
Access to justice and fostering accountability. Interventions to assist people denied access to their property and subjected to exploitation to seek redress are seen as part of an HRBA to MHCPS in the eyes of some of the interviewees. These interventions are closely aligned with objectives to educate people with psychosocial disabilities about their rights and to educate judicial officers and other officials about the rights of this population. In this sense, there is both a service provision and an advocacy component to an HRBA to MHCPS. A respondent noted:
Our mobilization is about participatory approaches to holding government to account … We use various means to do so … but our primary goal is to work with beneficiaries to claim their own rights.
Internally, efforts to foster accountability are equally relevant and require critical engagement with mental health service users and communities. As one respondent noted:
We actively seek out feedback and we use methods like informal and anonymous complaints-handling … it can be a challenge to implement because people aren’t really accustomed to participating in these kinds of mechanisms … we are trying to plant the seeds.
Providing care and support that is sensitive and receptive to diversity and accommodating of difference. The provision of gender-, culture-, and language-appropriate services is an important way in which MHCPS can be rights-based. Participants highlighted the specific needs of particular populations and the potential benefit that a more sensitive or diversity-inclusive approach can have. As one individual stated:
In the clinic, no one cares whether you are male or female, or whether you are Masai or Kikuyu. What if I need something [specific] because I am a woman or because I am Kikuyu? [The service provider] has to be [sensitive] to this.
The way in which organizations go about encouraging or implementing diversity-sensitive practices is multifaceted, focusing on training of staff to offer appropriate supports and to respond to varying needs, on building capacity in the organization that is diverse itself (including recruiting people with psychosocial disabilities), on ensuring access to interpreters, and on emphasizing the user-centered perspective as a means of individualizing the supports provided.
Some participants acknowledged the importance of culturally appropriate care and support but viewed traditional approaches to mental health with suspicion, arguing that these interventions may actually violate human rights. The following quote exemplifies this stance:
Sure, there are traditional services but they are problematic to be honest. You hear about people being chained and beaten or about their bodies being mutilated by these so-called healers.
Faith-based mental health interventions were the subject of some disagreement among respondents. One participant said:
It’s really difficult to say. I think that churches and mosques are essential sources of community, so we want to connect with them as much as possible, but some of the things you hear that come out of them about mental health are really chilling.
The fact that “churches and mosques are essential sources of community” is clearly an important point and an indication of the ways in which religious institutions might be partnered with when seeking to ensure a holistic approach to MHCPS provision. However, the “chilling” occurrences in some of these settings lead to the adoption of a cautious stance and, at times, to avoidance of faith-based models of MHCPS despite the need for sensitivity to diversity. This therefore represents a considerable dilemma for the implementation of HRBAs to MHCPS.
Stakeholder opinions regarding the contribution and efficacy of a rights-based approach to mental health
Dignity and self-esteem. Participants highlighted the effect of an HRBA on dignity and self-esteem. For example, one stated:
The primary purpose and idea behind an [HRBA] is this idea of dignity. I know it’s difficult to operationalize or quantify, but you see it in the way that people live their lives, going back to work or advocating in civic spaces or becoming part of the organization as peer educators or lay counselors. I think you have to apply a bit of a subjective lens and say “I know it when I see it.”
Another participant stated:
When I was just going to the clinic, I would get sent home with medication and left alone for another month. I don’t think they understand that I want to [participate in society]. They think that I can’t or maybe they think that I don’t want to.
Importantly, this individual is one of the participants who has since become a lay counselor and who views this as a testament to the validity of an HRBA.
The importance of a focus on social and economic determinants. Reducing stigma through community awareness-raising and education has been shown to contribute to improved mental health outcomes.[32] This is borne out by the statements of participants. One participant stated:
It used to be so depressing hearing people call me mad … I think that [itself] used to make me unhappy and then I used to isolate myself more, and that used to make me more depressed. Now [with the public education campaign], I don’t hear those names and I don’t feel so isolated.
Addressing social circumstances can therefore contribute substantially to well-being. The same is true, according to numerous interviewees, of initiatives to address the economic determinants of mental health and well-being. In the words of one respondent:
I can honestly say that it has changed everything … When we started doing these livelihoods programs, we found that people participated more and that they were becoming well faster and staying well longer … it makes sense, because it is actually a core [component] of social justice.
Preventive benefits and the benefits (and possible limits) of autonomy. Participants also raised the contribution of an HRBA as a preventive measure, stating that it has the capacity to produce better mental health outcomes. This is exemplified by the following quote:
I don’t use these five medications anymore. I don’t get sick all the time the way I used to. When I was going to the hospital, I would get sick all the time…Now, I know when I am getting sick, and I can [take the necessary steps] to stop it [from getting worse].
The effect of the HRBA in this case has therefore, been relapse prevention, but it was also highlighted that the provision of appropriate information and the practice of care in the community may have equally beneficial implications.
Participants noted the substantial benefit to users of an autonomous model, based on information sharing and self-monitored care, although a key unresolved question relates to the subject of coercion, as demonstrated by the following quote:
Sometimes you need it, unfortunately…sometimes it can’t be avoided…for people who are dangerous or who need protection, surely they have a right to be protected, and their health is better served that way.
The health effects of coercion are the subject of continuous debate, not unlike the situation described by researchers.[33] Even so, as the following quote suggests, the benefits of an HRBA can be realized even when these contentious questions remain without an axiomatic answer:
It’s absurd to say that a rights-based approach isn’t being operated because of some very real unanswered questions. We do what we know for sure, and the things we don’t know, we try to engage with.
This also reflects a need for further documentation and elaboration of the clinical effectiveness of HRBAs and for further engagement with some of the complexities of applying this approach in prevailing systems.
The benefits to mental health service users and their families of peer and family supports. HRBAs to MHCPS incorporating a peer and family support component can aid in the development of self-efficacy among participants. This is highlighted as follows:
Now I am healthy myself but I also can help others … I wouldn’t know how to help them if it were not for [the organization] … I would still be going to the hospital and getting told what to do like I am a child.
Peer education can be a meaningful way in which to foster self-esteem, while contributing to the mental health and well-being of others, as illustrated by the following quote:
[The peer groups] help me to share my feelings and make me think in a way that the clinic never did. I think that because of this my mind is more clear and I feel more supported.
Similarly, family support systems and services can have a direct impact on mental health service users while also contributing to more harmonized and supportive family systems. This can be a vital way to cater to family needs, using interventions such as family education, counseling, and caregiver training.
Empowering mental health service users to be self-advocates and to participate in society, including civic spaces. Respondents highlighted the fact that the ability to participate in society can be an indication of agency, which in turn contributes to well-being. The following quote illustrates this point:
It makes me feel better that I can use my own voice rather than asking the doctor or the nurse [to speak for me].
Beyond this direct benefit to users, speakers also highlighted that policies and laws benefit significantly from the input of the people most directly affected by them, in keeping with the right to participation in instruments such as the CRPD.[34] Therefore, the benefit of an HRBA is also its contribution to better lawmaking, in the process strengthening mental health systems.
Factors that impede the implementation of HRBAs to mental health care and support services
Stigma on the basis of psychosocial disability. Stigma on the basis of psychosocial disability continues to be a pervasive challenge, and it has the effect of causing mental health to be a neglected issue. One participant stated the following:
I don’t think [the government] cares about [mental health]. I don’t think it means anything to them because it’s seen as a condition of the feeble-minded or the bewitched. Even among government officials, you hear these beliefs being repeated.
This indicates that stigma contributes significantly to the under-prioritization of mental health. With respect to HRBAs specifically, these appear even more marginalized because there remain segments of society who do not believe people with mental health conditions should possess the same rights as others. This is exemplified by the following quote:
You are talking about human rights and the [HRBA], but what happens if my neighbor does not think of me as a human being? What happens if my doctor does not think of me as a human being?
Lack of resources. Mental health is clearly a neglected priority, suffering from low levels of investment and social and political barriers that can at times render it difficult to meet the needs of people with psychosocial disabilities. Participants highlighted this as a major impediment to the advancement of HRBAs to mental health, noting, for example, that
we are talking about decades, perhaps centuries of neglect, and about needs that go well beyond the rollout of drugs. I don’t think governments and funders are willing to admit that.
This speaker suggested that the biomedical approach was seen as a more cost-effective way to address mental health needs because it requires a more finite allocation of resources. An HRBA is, in the opinion of some, a more substantial ask because of the social supports that characterize it. This, however, was not a view shared by all participants, with one interviewee stating:
Actually I think these community-oriented models are actually cheaper to implement. They don’t require new investment in hospitals or a lot of salaries for highly specialized staff and they aren’t asking people to travel for miles and miles to access services.
It seems that further clarification is needed to consider what the actual resource allocation needs are for HRBAs to MHCPS, and whether allocating resources in this way is in fact more efficient than allocating for large-scale biomedical interventions that rely heavily on clinicians trained in models developed in the Global North, who may have a contribution to make but need not be the only human resource for health. This speaker also stated:
Even if they are more expensive, that is not the point … The point is what is the right thing to do? What will create more cohesive and healthier societies in the long term?
Lack of research to support HRBAs. Research to establish standards in HRBAs and to build an evidence base to support the implementation of these approaches is sorely needed. This is a considerable impediment to the rollout of HRBAs. As one interviewee noted, this problem is particularly acute in low- and middle-income countries:
There is very little [documented evidence] to show that HRBAs work in settings like Kenya … Even if you can show that [HRBAs] are effective, people will say it’s because they have all these resources in Sweden and Canada that we don’t have here.
Further research to support the implementation of HRBAs to MHCPS in the Global South is needed. On the subject of monitoring and evaluation specifically, another individual stated:
We want to monitor effectiveness, and we want also to improve delivery, but this is costly and technical … It’s something we know we need to work on.
Organizational challenges. A number of interrelated challenges within organizations can have the effect of making it difficult to implement and further develop HRBAs to MHCPS. These include lack of technical capacity and the short lifespans of some of these organizations due to funding constraints. Additionally, resistance within organizations to certain aspects of an HRBA might be an impediment, as illustrated by the following quote:
One of things we are talking about is supporting people with these so-called alternative lifestyles … transgender people and sex workers and so on … ideally we want to ensure that anyone who needs a service can get it … but we have to be aware that we are [operating] in a society that is conservative.
Factors that support the implementation of HRBAs to mental health care and support services
Coalition-building. Participants noted that they were able to make significant progress in building a community of practice to engage in HRBAs through building coalitions with like-minded organizations. For example:
There are some other organizations also working in this field, and this has had the effect of helping to create a coalition … It makes advocacy easier.
In this way, organizations that share an interest in HRBAs to mental health can act as partners. Even so, interviewees acknowledged that this was not always the case, particularly when competition for resources is acute.
Self-advocacy by mental health service users. Respondents noted that a significant supportive factor in developing and advocating for HRBAs to MHCPS services is the fact that these services are preferred and argued for by mental health service users themselves, as highlighted by the following quote:
I think there is no more powerful tool to advocate for HRBAs to mental health than having someone who has used such a service state unequivocally that it is the best way.
Ultimately, it seems that this enthusiasm for self-advocacy may also be somewhat tempered by doubts about the receptiveness of policy makers. Another participant stated:
When I share my story, I think sometimes they are surprised … It makes them notice, but I wonder what happens after they have noticed.
Discussion
This research project identified key principles of HRBAs to MHCPS based on the perspective of stakeholders themselves. These guiding principles form the basis for an ethos that underpins HRBAs. The results have also demonstrated that while the guiding principles of numerous definitions of an HRBA are indeed useful as overarching themes, there is a need to add particularized context to those principles and to engage with the actual interventions that might be said to operationalize them. In keeping with criticism of many definitions of HRBAs “privileging consensus over specificity” and their general nature that makes them “difficult to operationalize,” the results show that it is in the interventions described and the actual programming contemplated that HRBAs become more implementable, making standardization for good practice possible.[35]
This study also focused on the key contributions that an HRBA to MHCPS can make, including a clear orientation toward dignity and autonomy, toward prevention, and toward the self-efficacy of mental health service users. Impediments to implementation—such as the need for further research, stigmatization among policy makers, and the lack of sustainable financing—were also highlighted by participants. At the same time, there were some encouraging signs related to the strengthening of user voices, opportunities for coalition-building, and a sense that while it is not clear whether HRBAs might be considered more or less cost-effective, they are unequivocally the “right thing to do.”
The findings of this study offer useful insight into the potential challenges and opportunities in low-resource settings, but the small sample size and geographical limitation to Kenya mean that the transferability of these findings might be limited. Circumstances such as cultural norms, provisions in law and policy, and social attitudes toward mental health might be substantially different in other settings, despite their low-resource status. For this reason, multiple studies across contexts are needed. Tensions related to the role of coercion and the place of traditional and faith-based modalities in HRBAs have also been highlighted here, suggesting that further research would be warranted to capture nuances that were not possible in our study. A longitudinal study that seeks to establish the impact of HRBAs over time would also be an essential addition. Alongside an examination of the practice of HRBAs to MHCPS, there is arguably a need for an interrogation of the perception of these approaches among policy makers and funders to consider ways in which buy-in for them might be fostered.
What is made clear by our study is that an HRBA to MHCPS requires more than merely the elucidation of principles—it requires a clear sense of interventions to operationalize those principles and a strong understanding of local context. As more information is gathered and more practices are documented, the content of HRBAs to MHCPS will likely become more clear, and their contribution will be foregrounded. A necessary step will then also be the development of sound indicators, appropriate impact assessment, and refinement to ensure that mental health service users benefit from monitoring and evaluation.[36] As a field where human rights concerns have been so pervasive, this should be welcomed and supported. This is true now more than ever, as policy makers and practitioners around the world grapple with the ramifications of the COVID-19 pandemic and seek out ways to imagine healthier, more equitable, and, ultimately, more just societies.
Faraaz Mahomed is Program Officer for Mental Health and Rights at the Open Society Foundations, New York, USA; Research Associate at the Harvard Law School Project on Disability, Cambridge, USA; and Visiting Research Fellow at the Centre for Applied Legal Studies, University of the Witwatersrand, Johannesburg, South Africa.
Jacqueline Bhabha is Professor of the Practice of Health and Human Rights at the Harvard T.H. Chan School of Public Health, Director of Research at the François-Xavier Bagnoud Center for Health and Human Rights at Harvard University, and Jeremiah Smith Jr. Lecturer at Harvard Law School, Cambridge, USA.
Michael Ashley Stein is Executive Director of the Harvard Law School Project on Disability and Visiting Professor at Harvard Law School, Cambridge, USA; and Extraordinary Professor at the Centre for Human Rights, University of Pretoria, South Africa.
Dainius Pūras is Professor at the Clinic of Psychiatry, Vilnius University, Lithuania, and the former United Nations Special Rapporteur on the Right to Health.
Please address correspondence to Faraaz Mahomed. Email: faraazmahomed@gmail.com.
Competing interests: None declared.
Copyright © 2020 Mahomed, Bhabha, Stein, and Pūras. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A/21 (1966).
[2] S. Gruskin, D. Bogecho, and L. Ferguson, “‘Rights-based approaches’ to health policies and programs: Articulations, ambiguities, and assessment,” Journal of Public Health Policy 31/2, (2010) pp. 129–145.
[3] Committee on Economic, Social and Cultural Rights, General Comment 14: The Right to the Highest Attainable Standard of Health, UN Doc. E/C.12/2005/4 (2000).
[4] World Health Organization and Office of the United Nations High Commissioner for Human Rights, A human rights-based approach to health. Available at https://www.who.int/hhr/news/hrba_to_health2.pdf.
[5] Gruskin et al. (see note 2), p. 134.
[6] R. Thomas, S. Kuruvilla, R. Hinton, et al., “Assessing the impact of a human rights-based approach across a spectrum of change for women’s, children’s, and adolescents’ health,” Health and Human Rights Journal 17/2 (2015), pp. 11–20.
[7] S. Porsdam Mann and M. M. Schmid, “Health research priority setting: State obligations and the human right to science,” American Journal of Bioethics 18/11 (2018), pp. 33–35.
[8] N. Drew, M. Funk, S. Tang, et al., “Human rights violations of people with mental and psychosocial disabilities: An unresolved global crisis,” Lancet 378 (2011), pp. 1664–1675.
[9] N. Monteiro, Y. Ndiaye, D. Blanas, and I. Ba, “Policy perspectives and attitudes towards mental health treatment in rural Senegal,” International Journal of Mental Health Systems 8 (2014), p. 9.
[10] F. Mahomed, “Stigma on the basis of psychosocial disability: A structural human rights violation,” South African Journal on Human Rights 32/3 (2016), pp. 490–509.
[11] American Psychiatric Association, Diagnostic and statistical manual of mental disorders, 5th edition (Washington, DC: American Psychiatric Association, 2013).
[12] J. T. V. M. De Jong, Trauma, war, and violence: Public mental health in socio-cultural context (New York: Kluwer Academic, 2006).
[13] T. Degener and G. Quinn, “A survey of international, comparative and regional disability law reform,” in S. Yee and M. L. Breslin (eds), Disability rights law and policy: International and national perspectives (New York: Transnational, 2002), pp. 3–128.
[14] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006).
[15] Office of the United Nations High Commissioner for Human Rights, Status of ratification interactive dashboard. Available at https://indicators.ohchr.org.
[16] C. D. Aguilar, Report of the Special Rapporteur on the rights of persons with disabilities, UN Doc. A/HRC/37/56 (2017).
[17] J. Eaton, “Human rights-based approaches to mental health legislation and global mental health,” BJPsych International 16/2 (2019), pp. 37–40.
[18] T. Dejener, “A new human rights model of disability,” in V. Della Fina, R. Cera, and G. Palmisano, The United Nations Convention on the Rights of Persons with Disabilities: A commentary (Cham: Springer, 2017), pp. 41–59.
[19] S. Porsdam Mann, V. J. Bradley, and B. J. Sahakian, “Human rights-based approaches to mental health: A review of programs,” Health and Human Rights Journal 18 (2016), p. 1.
[20] Ibid.
[21] F. Mahomed, Establishing good practice in rights-based approaches to mental health in Kenya. Available at https://dash.harvard.edu/handle/1/40976814.
[22] Ibid.; Mental Health Innovation Network, Tinada Youth Organization. Available at https://www.mhinnovation.net/organisations/tinada-youth-organization-tiyo; Kamili Mental Health Organization, About us. Available at https://www.kamilimentalhealth.org/about_us.
[23] R. Elliott and L. Timulak, “Descriptive and interpretive approaches to qualitative research,” in J. Miles and P. Gilbert, A handbook of research methods for clinical and health psychology (Oxford: Oxford University Press, 2005), pp. 147–159.
[24] United Nations General Assembly, Resolution 60/251, UN Doc. A/RES/60/251 (2006).
[25] F. Mahomed, M. A. Stein, and V. Patel, “Involuntary mental health treatment in the era of the United Nations Convention on the Rights of Persons with Disabilities,” PLOS Medicine 15/10 (2018), e1002679.
[26] Ibid.
[27] Committee on Economic, Social and Cultural Rights (see note 3); Porsdam Mann and Schmid (see note 7).
[28] Committee on Economic, Social and Cultural Rights (see note 3).
[29] R. A. H. Shalaby and V. I. O. Agyapong, “Peer support in mental health: Literature review,” JMIR Mental Health 7/6 (2020), e15572.
[30] Porsdam Mann and Schmid (see note 7).
[31] F. Tramonti, A. Petrozzi, A. Burgalassi, et al. “Family functioning and psychological distress in a sample of mental health outpatients: Implications for routine examination and screening,” Journal of Evaluation in Clinical Practice 26 (2020), pp. 1042– 1047.
[32] P. W. Corrigan, S. B. Morris, P. J. Michaels, et al., “Challenging the public stigma of mental illness: A meta-analysis of outcome studies,” Psychiatric Services 63/10 (2012), pp. 963–973.
[33] P. Gooding, “Navigating the ‘flashing amber lights’ of the right to legal capacity in the United Nations Convention on the Rights of Persons with Disabilities: Responding to major concerns,” Human Rights Law Review 15/1 (2015), p. 45; Mahomed et al. (see note 25).
[34] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006).
[35] Gruskin et al. (see note 2), p. 134.
[36] Porsdam Mann and Schmid (see note 7).