Right-to-Medicines Litigation and Universal Health Coverage: Institutional Determinants of the Judicialization of Health in Brazil
Volume 22/1, June 2020, pp 221 – 236
Mariana P. Socal, Joseph J. Amon, and João Biehl
Abstract
Over the past three decades, Brazil has developed a decentralized universal health system and achieved significant advances in key health indicators. At the same time, Brazil’s health system has struggled to ensure equitable and quality health services. One response to the broad promises and notable shortcomings has been a sharp rise in right-to-health litigation, most often seeking access to medicines. While much has been written about the characteristics of patient-plaintiffs and the requested medicines in right-to-health litigation in Brazil, little research has examined potential community-level and institutional drivers of judicialization and their role as mechanisms of accountability. To explore these dimensions, we used a mixed-effects analytical model to examine a representative sample of lawsuits for access to medicines filed against the state of Rio Grande do Sul in 2008. We found that the presence of a Public Defender’s Office was associated with a sevenfold increase in the likelihood of a municipality having a medicine-requesting lawsuit. This effect was maintained after controlling for a series of municipality characteristics. As low- and middle-income countries seek to achieve universal health coverage within the framework of the Sustainable Development Goals, Brazil’s experience may be illustrative of the challenges that health systems will face and the institutional mechanisms that will emerge, advancing accountability and individual patients’ interests in response.
Introduction
Universal health coverage (UHC) has become a rallying cry and pillar of the Sustainable Development Goals. Operationally, it can mean both focused reforms and sweeping health system changes. In its simplest formulation, UHC is understood as access to affordable, quality health services for all.[1]
Over the last three decades, among low- and middle-income countries, Brazil has been at the forefront in creating a universal health system (Sistema Único de Saúde, or SUS) grounded in the recognition of a right to health for all.[2] With significant investment, Brazil has increased life expectancy (from 65 to 75 years), reduced infant mortality (from 53 to 14 per 1,000), and pioneered pharmaceutical access initiatives.[3] In recent measures of UHC, Brazil received a 77 out of 100 in its UHC service coverage index, with scores for different services including 88 (family planning), 90 (antenatal care), and 96 (child immunization).[4]
Alongside these achievements, the country has faced major challenges: sustaining funding, building robust institutions and regulatory mechanisms, and ensuring equitable quality of care. The decentralization of care delivery has often occurred without adequate technical capacity, and the growing privatization of services has jeopardized efficiency and entrenched inequalities around the axes of race, gender, and region.[5] These trends are especially evident around pharmaceutical access: many Brazilian patients go to public pharmacies only to find that the medicines they were prescribed are out of stock or are not included in governmental drug formularies.[6]
One mechanism that emerged to address some of these challenges has been the phenomenon of right-to-health litigation (often referred to as the “judicialization of health”).[7] Highly contested and methodologically constrained, the debates over the whys, the hows, and the effects of this ever-expanding phenomenon have been marked by polarized arguments about equity, bureaucratic autonomy, resource allocation, and efficiency.[8] Many scholars and government officials have advocated for the containment and management of right-to-health litigation.[9] In contrast, our previous work has advanced an understanding of such litigation as a heterogeneous phenomenon and as a critical dimension of the country’s democratic life, enabling legal empowerment, fostering social mobilization, and working as a mechanism (albeit precarious) of accountability.[10] From this perspective, judicialization contributes to the struggle to define the contours and components of the country’s constitutionally mandated right to health alongside subsequent laws, Ministry of Health policies, and Supreme Court rulings that have advanced an expansive right to access to treatments.
While past studies of judicialization in Brazil have emphasized individual characteristics of patient-litigants and the types and costs of the medicines requested, in the present study we seek to identify how community-level and institutional determinants might influence right-to-health-litigation. As low- and middle-income countries invest in and develop stronger health systems, more attention should be paid to understanding Brazil’s experience in developing a universal health system and to the governmental and civil society mechanisms that arose to address its shortcomings and constraints. With hundreds of thousands of lawsuits seeking access to medicines annually, judicialization has played a central role in Brazil by mediating individuals’ access to health care. As low- and middle-income countries expand their efforts to establish UHC, and their populations face an increasing burden from non-communicable diseases, the potential role (and limits) of judicialization as a mechanism of accountability deserves close scrutiny, especially in light of current trends in pharmaceutical globalization and the privatization of health care.[11]
Neoliberal reforms, access to medicines, and judicialization in Brazil’s national health system
Two concurrent and paradoxical trends informed the structure of Brazil’s universal health care system in the early 1990s. On one hand, there was a trend toward a greater recognition of the government’s role in the fulfilment of social rights in democratizing Brazil. On the other hand, a neoliberal theory of government emphasized decentralization and the outsourcing of state functions to the private sector.[12] Nowhere was this conflicting direction more evident than in the question of pharmaceutical access.
From its inception, access to medicines was an integral part of Brazil’s national health system, SUS. Over time, with the introduction of drug-specific programs and policies and patient activism, access to medicines became an even larger component.[13] In the 1990s, community health boards (Conselhos de Saúde) were created at local, regional, and national levels to ensure accountability within SUS. They were designed to set priorities and to monitor the implementation of health policies.[14] These participatory mechanisms, however, have not alleviated major problems related to the lack of infrastructural investments (with public services outsourced to private providers) and the effective regulation of public and private health care actors. Thus, the country still sees large regional disparities in health care delivery and in health outcomes, with poorer regions and lower socioeconomic population groups disadvantaged the most.[15]
Even outside SUS, access to medicines has remained a core responsibility of the state. Private health insurance plans were introduced in the country in the late 1980s to complement SUS and to provide specialized and expedited care for higher-income segments. However, privately insured individuals (who now constitute about 24% of the population) have continued to benefit from SUS through access to state-subsidized medicines, since private insurance plans do not cover outpatient drugs.[16] This benefit, combined with the tax deductibility of health insurance premiums, puts a strain on state health expenditures while also lowering tax revenues. Of particular demand are increasingly high-priced specialty drugs such as treatments for diabetes, hepatitis C, and cancer.
In the mid-1990s, after Brazil signed the TRIPS agreement and began to see a successful response to HIV/AIDS with expanded access to antiretroviral drugs, an understanding of a right to medicines emerged. With exponentially increasing drug costs (due to tightening intellectual property laws for medicines and Brazil becoming a major market for global medicines), judicialization expanded to new patient populations, with people using the courts to seek access to medicines they were unable to find in public pharmacies. The arguments advanced in lawsuits drew on those used by HIV/AIDS activists, and the phenomenon grew especially quickly in the southern and southeastern regions.[17] Recognition of a right to medicines was endorsed by a ruling by the Supreme Court in 2000 concerning a patient’s access to a new antiretroviral drug and describing the HIV/AIDS pharmaceutical assistance program as the actualization of the government’s duty to implement programmatic norms that secure the health of the population.[18] With such programs, as Justice Celso de Melo argued, the right to health ceases to be “an inconsequential constitutional promise.”[19]
Patient-plaintiffs in Brazil obtain legal representation from private lawyers or public legal services, such as the independent Public Prosecutor’s Office (Ministério Público) and local branches of the Public Defender’s Office (Defensoria Pública). The Public Prosecutor’s Office operates at both the federal and state levels and is charged with defending the rights of minorities and civil society more broadly. The Public Defender’s Office promotes individual rights and provides free legal representation to individuals who earn below a certain income threshold (three times the minimum wage). Public Defenders’ Offices are present in all Brazilian states and in most large cities and are meant to guarantee the constitutional promise of a right to access to justice. Historically, lawsuits for access to medicines have been filed against the state, even when the drug has not been part of SUS’s formularies or when the plaintiff had a private health insurance plan. Since the early 2000s, courts have continued to consistently rule in favor of patient-plaintiffs, based on the interpretation that the right to state-provided medicines is part of the constitutional right to health.[20]
The state of Rio Grande do Sul, where we have been carrying out research for the past decade, has the highest number of right-to-medicines cases in the country.[21] In 2016, for example, this state of over 11 million inhabitants had 61,000 legal cases for access to medicines, costing 4% of the state’s entire health budget that year.[22]
Case study: Institutional determinants of judicialization in southern Brazil
Numerous investigations have described the characteristics of right-to-medicines litigation in Brazil. While some studies have found that judicialization is driven primarily by better-off individuals seeking expensive off-formulary treatments, others have found that judicialization serves mainly low-income individuals who are seeking inexpensive medicines that should have been available in SUS pharmacies.[23] When examining the legal and medical services most frequently involved, some scholars have suggested that judicialization is driven largely by physicians seeking to promote high-cost treatments and private lawyers specializing in health-related lawsuits, while other scholars have highlighted the important role played by SUS doctors and public defenders in encouraging patients to file lawsuits.[24]
Less closely examined has been the influence of community-level characteristics (such as socioeconomic development) and institutional factors (such as the presence of health and legal systems).[25] For example, some studies have suggested that regional differences in health budgets and in SUS’s administrative capacity might be drivers of judicialization.[26] From this perspective, judicialization could be seen as a response to a population’s health needs being insufficiently or inadequately fulfilled by state services at the local level.[27] Alternatively, the characteristics and accessibility of the legal system at the local level may influence individuals’ ability to “enter justice” (entrar na justiça, as plaintiffs generally call it—that is, to have their health claims addressed by the judiciary).[28]
In the context of what has been at times a polarized and overly narrow debate, broadening the understanding of judicialization beyond individual cases, types of medicines requested, and their immediate costs is timely and analytically significant.
Methods
To assess the possible influence of community-level and institutional factors on judicialization, we re-examined lawsuits for access to medicines filed against the state of Rio Grande do Sul in each of the state’s 496 municipalities in 2008. This representative sample was collected through a systematic survey of lawsuits on which we have previously reported. Methods from our research are described in detail elsewhere.[29] Briefly, the survey collected data from the State Health Secretariat’s electronic registry, a database that records all medicine-related lawsuits filed against the state and includes information on plaintiffs’ municipality of residence. In this analysis, we used plaintiffs’ municipalities of residence as the unit of analysis and considered municipalities with at least one medicine-requesting lawsuit to be positive cases. The research was reviewed and approved by the Institutional Review Board of Princeton University and by the Health Secretariat and the General Attorney’s Office of the state of Rio Grande do Sul.
Our analysis focused on the availability of health services and the presence of a Public Defender’s Office at the level of the municipality and health administrative region (HAR, or Coordenadorias Regionais de Saúde). Each HAR is responsible for managing and implementing state-sponsored health service delivery, including medicines, in the municipalities it covers.[30] The location of Public Defender’s Offices was obtained from the Rio Grande do Sul Public Defender’s Office website.[31] Availability of health services, defined as the number of facilities providing health services per 1,000 inhabitants, was obtained from a national health services survey known as the Pesquisa Assistência Médico-Sanitária.[32] We also examined several demographic, socioeconomic, and health characteristics of the municipalities, which we obtained from the Brazilian Census and the Ministry of Health’s epidemiologic surveillance system.[33] All 496 municipalities had full information, and there were no missing data.
Although the decision to submit lawsuits is made by patients and their sponsors (such as physicians and legal representatives), a patient’s likelihood of filing a lawsuit depends on the availability of such services in their community. Higher availability of health services in a given locale, for example, could be associated with a greater demand for pharmaceuticals and the increased likelihood of judicialization. Lower availability of health services could also be associated with a greater likelihood of judicialization as a means to fulfill the unmet health needs of a local population. In turn, higher availability of legal services could be associated with a higher likelihood of judicialization through increased access to legal representation.
In this study, we focused our analysis on outcomes and determinants at the community (municipality) level. Our analysis assumes that patients with the same individual characteristics would have different likelihoods of filing a medicine-requesting lawsuit, depending on the community level determinants and the characteristics of the health services and legal system of the municipality where they live.
Figure 1 displays the conceptual framework that guided our analysis. This theoretical scheme was adapted from Ronal Andersen and John F. Newman’s framework entitled “Societal and Individual Determinants of Medical Care Utilization” and is used here to represent the “claims formation stage” of the litigation process.[34]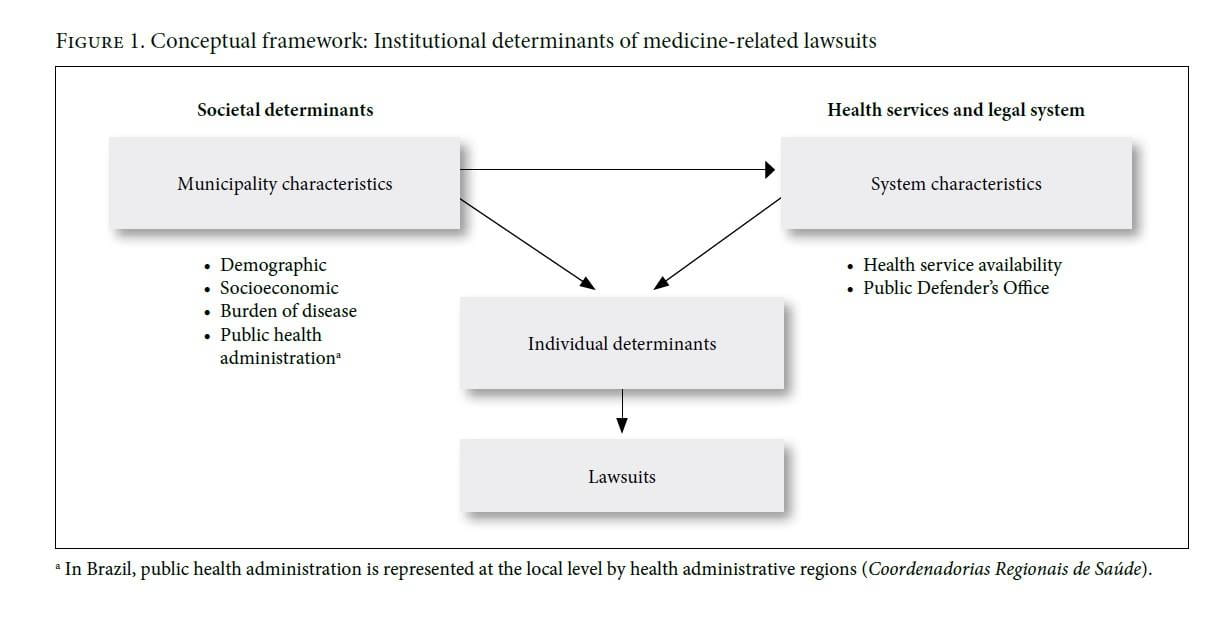
Controlling for demographic and socioeconomic characteristics, we implemented multi-level random effects logistic regression analyses grouped at the HAR level. The adjustment for municipality characteristics was implemented because these characteristics may simultaneously influence the likelihood of a municipality having a medicine-related lawsuit and the municipality having greater availability of health services or a Public Defender’s Office. There is also the possibility that the administrative capacity of the health system at the municipality level may play an independent role, as indicated by the municipality’s membership in a given HAR.
We tested the robustness of our results with sensitivity analyses using fixed-effects models for HAR and by repeating all models without the capital city of Porto Alegre (population of about 1.4 million), the only municipality with more than one Public Defender’s Office. All statistical analyses were implemented using Stata statistical package release 12 (StataCorp, College Station, TX).
Results
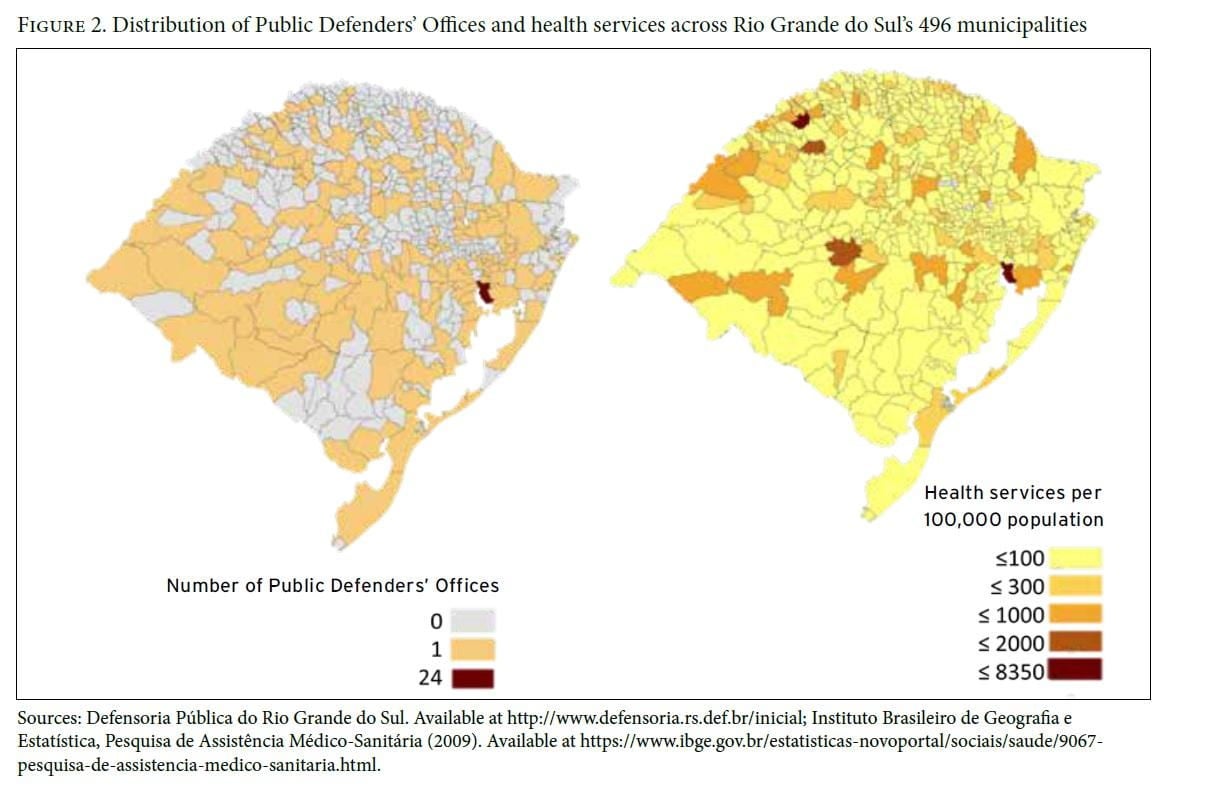
In 2008, over half of Rio Grande do Sul’s 496 municipalities were classified as urban (N=275, 55.5%), with an average of 21,000 inhabitants per municipality (range: 1,200–1.4 million) (Table 1). The state had a higher level of socioeconomic development than most states in Brazil, with an illiteracy rate among adults of 6.8% (range: 1–20% among municipalities) and monthly income of R$742.83 (US$462.50) (representing 1.8 times the national monthly minimum wage of R$415.00, or US$ 258.39, at the time).[35] The state had a crude mortality rate of 703.2 per 100,000, which varied between 120 and 1,200 deaths per 100,000 population among municipalities. Overall, 153 Public Defender’s Offices were present in the state, with at least one Office present in 31% (N=153) of the municipalities. There were, on average, 59 health services per 100,000 inhabitants (Figure 2).
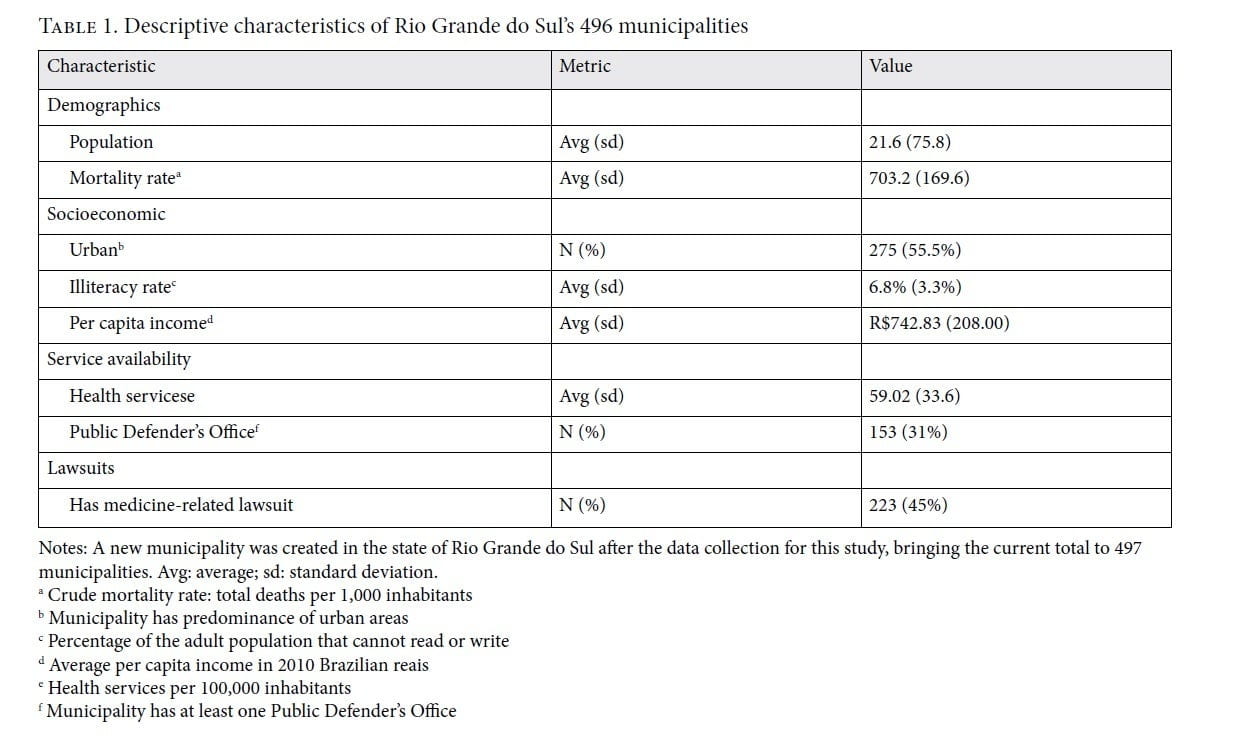
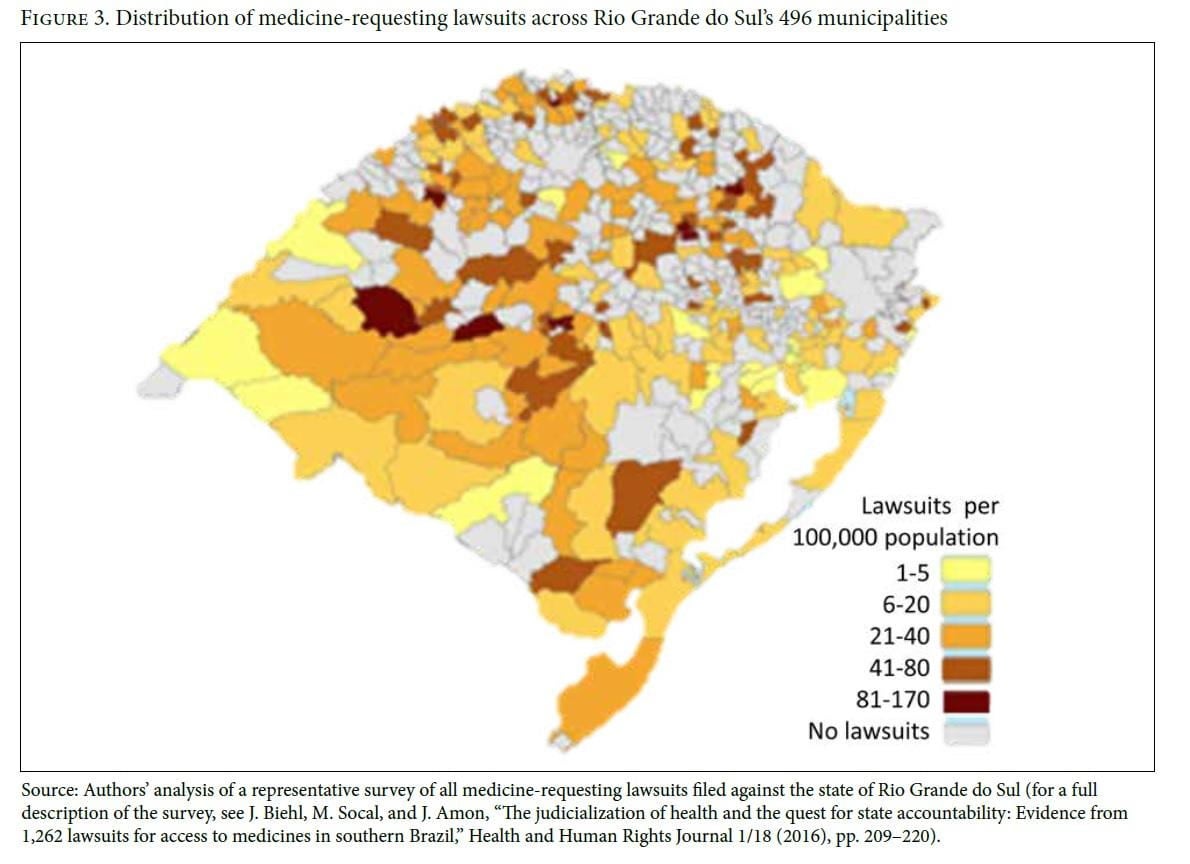
Ninety-two percent of lawsuits were found outside the capital city of Porto Alegre. About 45% (N=223) of municipalities had at least one lawsuit for access to medicines (Figure 3). Municipalities with lawsuits had an average of 28.5 lawsuits per 100,000 inhabitants (range: 1.5–168.6). Although the state capital had the highest number of lawsuits, when adjusted for population size it ranked 20th in lawsuits per 100,000 people. The municipalities with the highest density of medicine-requesting lawsuits were smaller municipalities, geographically scattered across the state.
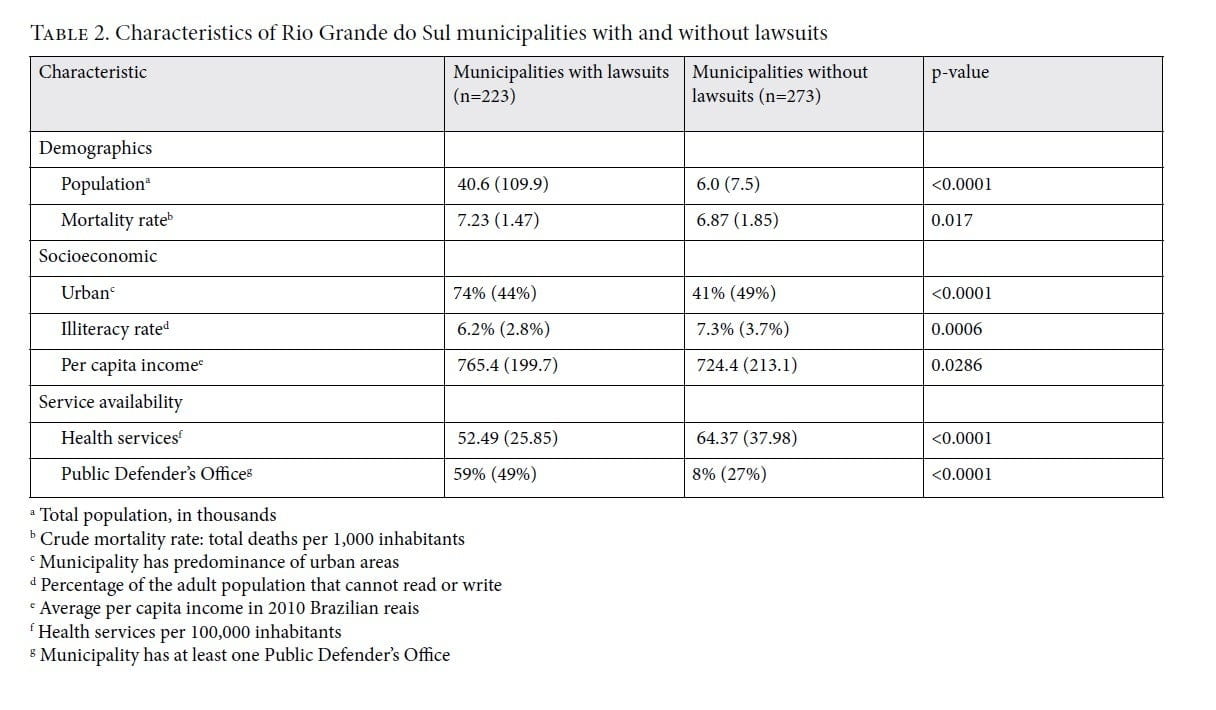
In a bivariate analysis, municipalities with medicine-requesting lawsuits had higher populations (40.9 ± 109.9 vs. 6.0 ± 7.5 thousand inhabitants, p<0.0001) and higher mortality rates (7.23 ± 1.47 vs. 6.87 ± 1.85 deaths per thousand, p=0.014) than municipalities without lawsuits (Table 2). Municipalities with lawsuits were more likely to be urban (26% vs. 59%, p<0.0001) and had lower illiteracy rates (6.2% vs. 7.3%, p=0.0006) and higher income levels (R$765.4 ± 199.7 vs. 724.4 ± 213.1, p=0.028) than those without lawsuits. Municipalities with lawsuits were more likely to have a Public Defender’s Office (59% vs. 8%, p<0.0001) and had lower availability of health services (0.52 ± 0.26 vs. 0.64 ± 0.38 services per 1,000 inhabitants, p<0.0001) than those without lawsuits.
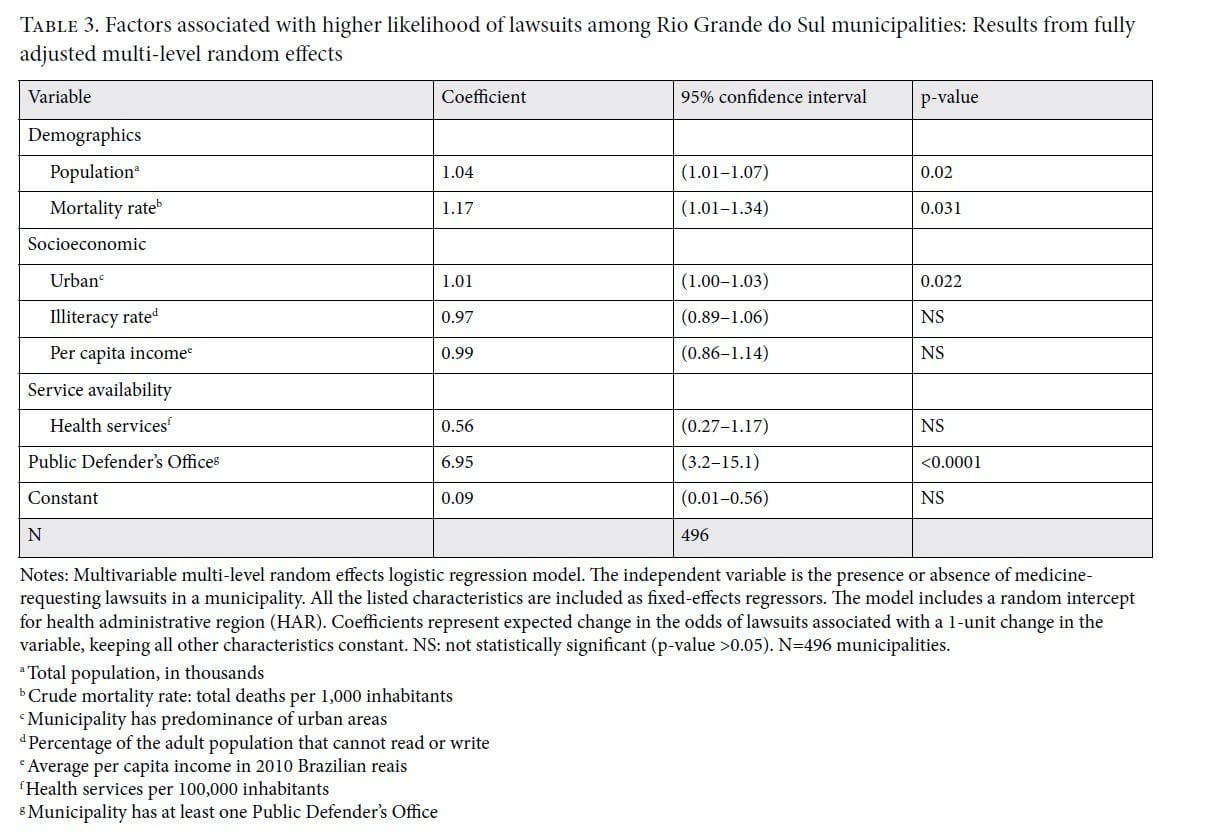
When controlling for all other characteristics in a multi-level random effects logistic regression model, municipalities with at least one Public Defender’s Office were about seven times more likely to have a medicine-requesting lawsuit than municipalities without it (odds ratio: 6.95, 95% CI: 3.2–15.1) (Table 3). Municipalities with greater availability of health services were less likely to have a lawsuit, yet this association was not shown to be statistically significant (odds ratio: 0.56, 95% CI: 0.27–1.17). Population size (odds ratio: 1.04, 95% CI: 1.01–1.07 per 1,000 population), mortality rate (odds ratio: 1.17, 95% CI: 1.01–1.34 per 1,000 individuals), and urban characteristics (odds ratio: 1.01, 95% CI:1.00–1.03 as compared to rural) continued to be associated with a greater likelihood of lawsuits. Neither of the variables associated with socioeconomic status, illiteracy, or per capita income was significantly associated with the presence of a lawsuit in the municipality. After adjusting for all characteristics, belonging to the same public health administration region explained 15% of the municipality’s likelihood of having a lawsuit (intraclass correlation coefficient: 0.15, 95% CI: 0.06–0.33). The different models implemented in the sensitivity analysis did not significantly change the results.
Analysis
Amidst global efforts to implement universal health care systems, the Brazilian experience of the last three decades is emblematic of the challenges that governments face in ensuring equitable and efficient health systems, while addressing an expansive, constitutionally mandated right to health and dealing with an accelerated political economy of pharmaceuticals.[36] In our previously reported work, we found that judicialization was geographically widespread in southern Brazil and that the majority of litigants were poor and older individuals with chronic diseases, seeking access to medicines that were already on governmental formularies and should have been available in local public pharmacies. Overwhelmingly, local judges ruled in favor of patient-plaintiffs, deeming their demands constitutionally legitimate.[37]
Our empirical findings here suggest that the presence of a Public Defender’s Office in a municipality is a major determinant of the likelihood of judicialization. Although this study implemented a cross-sectional analysis—which does not allow for the establishment of causative relationships between the institutional factors that we examined and the occurrence of judicialization—two main findings suggest that it is likely that the presence of Public Defenders’ Offices helped enable judicialization, and not the other way around. First, our fully adjusted models indicated that two municipalities with the same characteristics—same population size, mortality rates, and urban/rural characteristics—have significantly different likelihoods of having a medicine-related lawsuit, depending on the presence or not of a Public Defender’s Office. Even if the presence of a Public Defender’s Office in the municipality was initially a response to population needs, it still plays an important role in enabling patient-plaintiffs to file lawsuits. Second, the Public Defender’s Office is not the only form of legal representation available for low-income individuals in Rio Grande do Sul. When filing a lawsuit for access to medicines, low-income individuals may also be represented by a private lawyer and have their legal fees reimbursed by the state, as long as they request it as part of their lawsuit, present proof of need, and the judge approves it.
Judicialization as a mechanism of universal health coverage accountability
Charged with a mandate to represent vulnerable individuals and uphold justice, public defenders have accepted health-related lawsuits as part of their commitment to institutionally sustaining advancements in socioeconomic rights and promoting state accountability.[38] This accountability is manifest in two ways: first, it provides a measure of whether the state is fulfilling its constitutional obligations and administrative functions; and second, it pressures the state to respond to the rapidly changing landscape of population health needs and transparently and effectively address the incorporation of new technologies in the health system. In focusing on accountability within existing political and economic systems and sustaining hard-fought basic rights, the Public Defender’s Office thus elicits a vision of justice and political engagement at a local scale that includes the urgent need for health systems reform.[39]
If universal health coverage goes beyond access to minimum public health services and essential medicines and seeks to address the chronic, non-communicable diseases that are increasingly the cause of morbidity and mortality in low- and middle-income countries, then the increasing “pharmaceuticalization of health” must be anticipated.[40] Innovative treatments are available in the global market at ever-increasing speeds and heftier price tags. Incorporating these technologies into what can be offered to populations is a particular policy challenge for countries such as Brazil, which has become the world’s fifth most profitable and rapidly growing pharmaceutical market.[41] In this context, some scholars have argued that judicialization fails to act at the scale needed to combat neoliberally inflected policies.[42] That is, judicialization should focus more on court cases that seek structural changes to the political economy of medicines or on lobbying legislative bodies to take such steps as reforming patent laws and imposing regulations on price.
While judicialization might have the indirect effect of temporarily improving health care delivery, medicines granted by courts are often not fulfilled by the government, leaving patients with a legal victory but no treatment.[43] Or courts are slow to act, while patients suffer waiting for a resolution.[44] In a previous study we documented some responsiveness by the government to litigation, with several of the most sought-after medicines that were initially not on drug formularies later officially included, thus increasing the likelihood of availability.[45] While this is not a direct consequence of judicialization, it is a consequence of the expansion in the services and products provided by the public system that has occurred because of judicialization. Moreover, the lack of private insurance coverage for outpatient drugs in Brazil has left a gap that further challenges public policy and strains government budgets. Small steps have been taken in recent years by advancing regulations requiring private insurers to expand their benefits packages and include some high-cost drugs in their covered services.[46] Having private insurers cover drugs helps expand opportunities for Brazilians to finance the drugs they need, helps open new markets, and helps develop new opportunities for price negotiations with pharmaceutical companies.
It is easier to sue for medicines than for the improvement of public health services, and although massive individual right-to-health litigation may not represent sustainable structural change, it nonetheless helps strengthen the right to health and human rights more broadly, as seen in the institutional work of Public Defender’s Offices in southern Brazil. This work recognizes the fundamental importance of the State and its right-to-health obligations. Without establishing these obligations and institutionally sustaining advancements (albeit limited) in socioeconomic rights, pressing for governments to recognize their duty to challenge drug patents and negotiate pricing seems fanciful at best.[47]
There is indeed a sentiment across many sectors in Brazil that there should be a more effective way to address government malfunction and the privatization of SUS other than the judicialization route, but the answer from officials and scholars has often been that the better way is limiting access to justice and hoping that pharmaceutical delivery systems improve, either with expert advisory panels or on their own.[48] While better prioritization (that is, rationing) might be necessary, empowering expert advisory panels to determine what medicines should be provided by the state would not directly change the current dynamic in which courts judge that the state’s constitutional obligation to fund UHC at 15% of GDP is not being met and that individuals’ right to health includes medicines not on government formularies. If the recommendations of such panels were to constrain access to medicines, this might be considered a failure to progressively realize the right to health and in violation of Brazil’s treaty obligations under the International Covenant on Economic, Social and Cultural Rights. Expert panels might alternatively be charged with assessing the efficiency of the government’s pharmaceutical supply chain system, the influence of the pharmaceutical industry, the government’s use of (or failure to use) TRIPS flexibilities, or potential legislative policies and legal reforms around the coverage of medicines by private insurance. Local accountability efforts such as judicialization may not be the most efficient or all-encompassing political mechanism, but it is a critical element of a progressive rights movement and conduit of legal empowerment and a broader democratization of society.
Lawyers and legal services have played a role in Brazil in defining access to medicines in landmark cases going back to rulings on the free provision of antiretroviral therapy as a component of the right to health. In recent years, the legal pathway for access to medicines has allowed patients with hypertension to receive the basic drugs that were missing in their local public pharmacies, as well as patients with rare genetic disorders to receive the newest treatments in the field before their conditions become irreversible.[49] Although our data is from 2008, the mechanism of judicialization for accountability remains ever more relevant.
Legal empowerment as a grassroots strategy to expand health care has been documented globally, with, for example, defensores de saúde, or health advocates, in Mozambique supporting clients at the village level to resolve specific grievances with respect to health services, and “street lawyers” (Gadejuristen) in Copenhagen who provide legal education and sterile injecting equipment to drug users.[50] In Brazil, lawyers have also represented patients seeking broader protections such as access to information, transportation, specialized care, and family planning for those affected by the Zika virus.[51] In addition, legal empowerment demonstrates that the assumption that social rights litigation “benefits those in the ‘middle’ of the social spectrum because the poor have less access to courts” is fundamentally a product of the lack of options for access to legal representation.[52] Such lack can be successfully mitigated by institutions such as the Public Defender’s Office, which reinforce the “right to remedies” of individuals left out and left behind as policy makers (and often, international experts and norm-setting organizations) define what is, and what is not, included in universal health coverage.
As mentioned above, the role of public defenders and lawsuits as mechanisms of accountability for a functioning health system have limits—and inefficiencies. In order to effectively improve and expand Brazilians’ access to medicines, other accountability mechanisms ought to be engaged as well: the Public Prosecutor’s Office (Ministério Público), which represents vulnerable communities (including children, the elderly, and traditional populations); the community health boards (Conselhos de Saúde) that are SUS’s main accountability channel by design; state legislators and government health administrators who have the power to set up stronger mechanisms for prioritization and resource allocation; and civil society organizations, such as those representing Zika-affected families.[53] These mechanisms may target different shortcomings of universal health care systems, such as improving quality of care, transparency of decision-making, responsiveness, and resource allocation. They may also help expand the range of benefits offered from low-cost, low-complexity technologies toward increased access to high-cost and high-complexity ones.
Conclusion
Within global discussions of universal health coverage, the scant attention given to law has focused mostly on enabling legal environments and progressive health laws.[54] There has been little consideration of accountability mechanisms in general or access to legal services in particular. Our study demonstrates that the Public Defender’s Office plays an important role in right-to-health litigation, expanding it to geographically and socioeconomically diverse environments.
The volume of court cases is itself pressure on both the judiciary and the legislature to adopt structural reforms. Until now, this pressure has been insufficient to match the power of lobbyists and special interests who oppose such reforms, but it may not always be so. While it may be more strategic in the long term to fight for patent law reforms and hope for timely and effective implementation, those putting forward individual lawsuits seeking medicines actually embody structural vulnerabilities. They speak to the urgent need to strengthen public health systems and guard them against private cooptation.[55] The immediate need for human rights advocacy and legal access for multitudes of individual patients is clear.
The role of judicialization and of the Public Defender’s Office in improving accountability in access to medicines and overall health care delivery in Brazil should be further investigated. We contend that a combination of “real-time, comprehensive data collection multi-disciplinary academic research, robust public debate and media attention are needed in order to identify and strengthen these emergent accountability mechanisms aimed at both public and private health care institutions.”[56] In addition, policy makers aiming to improve access to care and pharmaceuticals in Brazil should consider the impact of judicialization and improve policy design and regulatory oversight based on the information generated by this process, with the normative ambition of achieving transparent, accountable, and participatory priority setting that promotes substantive human rights.
Acknowledgments
We want to thank Tiago Canelas Ferreira for his assistance with the figures in this article. We are also grateful to the Princeton Open Access Publication Fund Program for financial support for open-access publication fees.
Mariana P. Socal is Assistant Scientist at the Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA.
Joseph J. Amon is Director of Global Health and Clinical Professor at the Office of Global Health, Dornsife School of Public Health, Drexel University, Philadelphia, USA.
João Biehl is Susan Dod Brown Professor of Anthropology and Director of the Brazil LAB at Princeton University, Princeton, USA.
Please address correspondence to João Biehl. Email: jbiehl@princeton.edu.
Competing interests: None declared.
Copyright © 2020 Socal, Amon, and Biehl. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] United Nations General Assembly, G.A. Res 67/81, UN Doc. A/RES/67/81 (2012).
[2] Constituição da República Federativa do Brasil (Constitution of the Federative Republic of Brazil) (1988), art. 196. Available at https://www.senado.leg.br/atividade/const/con1988/con1988_06.06.2017/art_196_.asp; M. Castro, A. Massuda, G. Almeida, et al., “Brazil’s unified health system: The first 30 years and prospects for the future,” Lancet 394/10195 (2019), pp. 345–356.
[3] Castro et al. (see note 2).
[4] World Bank, Tracking universal health coverage: 2017 global monitoring report (Geneva: World Bank, 2017). Available at https://apps.who.int/iris/bitstream/handle/10665/259817/9789241513555-eng.pdf?sequence=1.
[5] C. Collins, J. Araujo, and J. Barbosa, “Decentralising the health sector: Issues in Brazil,” Health Policy 2/52 (2000), p. 113127; E. Pinafo, B. Carvalho, and E. Nunes, “Descentralização da gestão: Caminho percorrido, nós críticos e perspectivas,” Ciência e Saúde Coletiva 5/21 (2016), pp. 1511–1524.
[6] S. Mendis, K. Fukino, A. Cameron, et al., “The availability and affordability of selected essential medicines for chronic diseases in six low- and middle-income countries,” Bulletin of the World Health Organization 85/4 (2007), pp. 270–288; J. Watts, “Brazil’s health system woes worsen in economic crisis,” Lancet 387/10028, (2016), pp. 1603–1604.
[7] A. Messeder, C. Osorio-de-Castro, and V. Luiza, “Can court injunctions guarantee access to medicines in the public sector? The experience in the State of Rio de Janeiro, Brazil,” Cadernos de Saúde Publica 2/21 (2005), pp. 525–534; J. Biehl, A. Petryna, and A. Gertner “Judicialisation of the right to health in Brazil,” Lancet 373/9682, (2009), pp. 2182–2184; J. Biehl, M. Socal, V. Gauri, et al., “Judicialization 2.0: Understanding right-to-health litigation in real time,” Global Public Health (2018), pp. 1–10.
[8] L. Lopes, F. Acurcio, S. Diniz, et al., “(Un)Equitable distribution of health resources and the judicialization of healthcare: 10 years of experience in Brazil,” International Journal for Equity in Health 18 (2019), p. 10.
[9] D. Borges and M. A. Uga, “Conflitos e impasses da judicialização na obtenção de medicamentos: As decisões de 1a instância nas ações individuais contra o Estado do Rio de Janeiro, Brasil, em 2005,” Cadernos de Saúde Pública 26/1 (2010), pp. 59–69; O. H. Campos Neto, F. de A. Acurcio, M. A. Machado, et al., “Médicos, advogados e indústria farmacêutica na judicialização da saúde em Minas Gerais, Brasil,” Revista de Saúde Pública 46/5 (2012), pp. 784–790; A. Chieffi and C. Barata, “Legal suits: Pharmaceutical industry strategies to introduce new drugs in the Brazilian public healthcare system,” Revista de Saúde Publica 3/44 (2010), pp. 421–428; V. Da Silva and F. Terrazas, “Claiming the right to health in Brazilian courts: The exclusion of the already excluded,” Social Sciences Research Network (2008); O. Ferraz, “Harming the poor through social rights litigation: Lessons from Brazil,” Texas Law Review 7/89 (2011), pp. 1643–1668; F. Vieira and P. Zucchi, “Distorions to national drug policy caused by lawsuits in Brazil,” Revista de Saúde Publica 2/41 (2007), pp. 214–222.
[10] J. Biehl, M. Socal, and J. Amon, “The judicialization of health and the quest for state accountability: Evidence from 1,262 lawsuits for access to medicines in southern Brazil,” Health and Human Rights Journal 1/18 (2016), pp. 209–220; O. Ferraz “Moving the debate forward in right to health litigation,” Health and Human Rights Journal 2/18 (2016); J. Biehl, M. Socal, and J. Amon, “On the heterogeneity and politics of the judicialization of health in Brazil,” Health and Human Rights Journal 2/18 (2016), pp. 269–271.
[11] J. Biehl, Will to live: AIDS therapies and the politics of survival (Princeton, NJ: Princeton University Press, 2007); J. Biehl, “The judicialization of biopolitics: Claiming the rights to pharmaceuticals in Brazilian courts,” American Ethnologist 3/40 (2013), pp. 419–436; J. Biehl, “The postneoliberal fabulation of power: On statecraft, precarious infrastructures, and public mobilization in Brazil,” American Ethnologist 3/40 (2016), pp. 437–450; J. Biehl and J. Amon, “The right to remedies: On human rights critiques and peoples’ resources,” Humanity Journal (2019). Available at http://humanityjournal.org/blog/the-right-to-remedies-on-human-rights-critiques-and-peoples-recourses/; A Kapczynski, “The right to medicines in an age of neoliberalism,” Humanity Journal (2019). Available at http://humanityjournal.org/issue10-1/the-right-to-medicines-in-an-age-of-neoliberalism/.
[12] W. Brown, Undoing the Demos: Neoliberalism’s stealth revolution (Cambridge, MA: MIT Press, 2015); M. Goodale and N. Postero, Neoliberalism, interrupted: Social change and contested governance in contemporary Latin America (Stanford, CA: Stanford University Press, 2013); Biehl (2016, see note 11).
[13] Ministério da Saúde (Brazilian Ministry of Health), Portaria Nº 3.916, de 30 de Outubro de 1998 (1998). Available at http://bvsms.Saúde.gov.br/bvs/Saúdelegis/gm/1998/prt3916_30_10_1998.html; Ministério da Saúde (Brazilian Ministry of Health), Farmácia popular: Sobre o programa (2004). Available at http://portalms.Saúde.gov.br/acoes-e-programas/farmacia-popular/sobre-o-programa; Ministério da Saúde (Brazilian Ministry of Health), “Campanha Saúde não tem preço,” Portaria nº 184, de 03 de fevereiro de 2011 (2011). Available at http://portalarquivos.Saúde.gov.br/images/pdf/2014/junho/18/portaria184.pdf; Ministério da Saúde (Brazilian Ministry of Health), “Programa Aqui tem Farmácia Popular,” Portaria nº 111 de 28 de janeiro de 2016 (2016). Available at http://bvsms.Saúde.gov.br/bvs/Saúdelegis/gm/2016/prt0111_28_01_2016.html; J. Biehl, “The activist state,” Social Text 3/22 (2004), pp. 105–132; Biehl (2007, see note 11).
[14] N. Santos, “A Organização da Saúde no Rio Grande do Sul,” Revista Gestão & Saúde 3/1 (2010), pp. 1–10; Ministério da Saúde (Brazilian Ministry of Health), Estrutura do SUS. Available at http://portalms.Saúde.gov.br/sistema-unico-de-Saúde/estrutura-do-sus; Ministério da Saúde (Brazilian Ministry of Health), Conselhos de saúde: A responsabilidade do controle social democrático do SUS, 2nd edition (2013); R. Garcia, “Expanding the debate: Citizen implementation of the right to health in Brazil,” Health and Human Rights Journal 1/20 (2018), pp. 163–172.
[15] The current COVID-19 pandemic has exposed these regional inequalities, particularly in the Amazonian region. See M. Socal. “A Peça-Chave” (“The Key Piece”). Revista Piauí 164 (2020) pp.50-53. Available at https://piaui.folha.uol.com.br/materia/a-peca-chave/. See also C. Van Stralen, A. de Lima, D. Sobrinho, et al., “Conselhos de Saúde: Efetividade do controle social em municípios de Goiás e Mato Grosso do Sul,” Ciência e Saúde Coletiva 3/11 (2006), pp. 621–632; A. Massuda, T. Hone, F. Leles, et al., “The Brazilian health system at crossroads: Progress, crisis and resilience,” BMJ Global Health 3/4 (2018).
[16] Agência Nacional de Saúde Suplementar (Brazilian National Supplementary Health Agency), Taxa de cobertura (%) por planos privados de saúde (Brasil 2009–2019), (2019). Available at https://www.ans.gov.br/perfil-do-setor/dados-gerais; Agência Nacional de Saúde Suplementar (Brazilian National Supplementary Health Agency), Os medicamentos receitados pelo meu médico e que podem ser comprados em farmácia estão cobertos? (2019). Available at http://www.ans.gov.br/aans/index.php?option=com_centraldeatendimento&view=pergunta&resposta=487&historico=20587865.
[17] Messeder et al. (see note 7); Biehl (2004, see note 12); Kapczynski (see note 11); Biehl (2016, see note 11); J. Biehl, J. Amon, M. Socal, and A. Petryna, “Between the court and the clinic: Lawsuits for medicines and the right to health in Brazil,” Health and Human Rights Journal 1/14 (2012), pp. E36–E52; Brazilian National Justice Council, Judicialização da Saúde no Brasil: Dados e Experiências (2015). Available at https://www.cnj.jus.br/wp-content/uploads/2011/02/6781486daef02bc6ec8c1e491a565006.pdf; Conselho Nacional de Justiça (Brazilian National Justice Council), Judicialização da Saúde no Brasil: Perfil das Demandas, Causas e Propostas de Solução (2019). Available at https://www.cnj.jus.br/wp-content/uploads/2011/02/95da70941b7cd226f9835d56017d08f4.pdf.
[18] Biehl (2013, see note 11).
[19] Supremo Tribunal Federal (Brazilian Federal Supreme Court), Acórdão RE 271286 AgR/RS, Agravo Regimental no Recurso Extraordinário, Diário da Justiça Eletrônico (November 24, 2000).
[20] Biehl et al. (2012, see note 16); Biehl et al. (2016, see note 10); Biehl (2013, see note 11); Conselho Nacional de Justiça (2019, see note 17).
[21] F. Bassette, “RS Reúne Metade das Ações Judiciais em Saúde,” O Estado de São Paulo (April 29, 2011). Available at https://www.estadao.com.br/noticias/geral,rs-reune-metade-das-acoes-judiciais-de-saude-imp-,712418; Biehl et al. (2012, see note 17); Biehl (2016, see note 11).
[22] Conselho Nacional de Justiça (2019, see note 17).
[23] Chieffi and Barata (see note 9); J. Pereira, R. Santos, J. Nascimento Jr., and E. Schenkel, “Situation of lawsuits concerning the access to medical products by the health department of Santa Catarina State, Brazil, during the years 2003 and 2004,” Ciência e Saúde Coletiva 15/suppl. 3 (2007), pp. 3551–3560; Da Silva and Terrazas (see note 9); Vieira and Zucchi (see note 9); Biehl et al. (2012, see note 16); Biehl et al. (2016, see note 10); Messeder et al. (see note 7); M. Machado, F. Acurcio, C. Brandão, et al., “Judicialização do acesso a medicamentos no Estado de Minas Gerais, Brasil,” Revista de Saúde Pública 3/45 (2011); Ferraz (2011, see note 9).
[24] Da Silva and Terrazas (see note 9); Chieffi and Barata (see note 9); Ferraz (2011, see note 9); Biehl et al. (2012, see note 17); Biehl et al. (2016, see note 10); L. Romero, “Judicialização das políticas de assistência farmacêutica: O caso do distrito federal,” Consultoria Legislativa do Senado Federal (CONLEG): Textos Para Discussão 41 (2008), pp. 1–48.
[25] S. Gloppen, “Litigation as a strategy to hold governments accountable for implementing the right to health,” Health and Human Rights Journal 2/10 (2008), pp. 21–36.
[26] M. Prado, “The debatable role of courts in Brazil’s health care system: Does litigation harm or help?” Journal of Law, Medicine and Ethics 41 (2013), pp. 124–137.
[27] D. Borges, “Individual health care litigation in Brazil through a different lens: Strengthening health technology assessment and new models of health care governance,” Health and Human Rights Journal 1/20 (2018), pp. 147–162.
[28] Biehl (2013, see note 11); Biehl et al. (2012, see note 17).
[29] Biehl et al. (2016, see note 10).
[30] Estado do Rio Grande do Sul, População estimada por Município – RS, 2010 (2010). Available at http://www.saude.rs.gov.br/upload/arquivos/carga20181235/12113556-planilha-municipios-por-crs.pdf; Santos (see note 13).
[31] Defensoria Pública do Estado do Rio Grande do Sul, Plantões e Locais de Atendimento. Available at http://www.defensoria.rs.def.br/lista/411/plantoes-e-locais-de-atendimento.
[32] Instituto Brasileiro de Geografia e Estatística (Brazilian Institute of Geography and Statistics), Pesquisa de Assistência Médico-Sanitária (2009). Available at https://www.ibge.gov.br/estatisticas-novoportal/sociais/saude/9067-pesquisa-de-assistencia-medico-sanitaria.html.
[33] Instituto Brasileiro de Geografia e Estatística (Brazilian Institute of Geography and Statistics), Censo 2010 (2010). Available at https://censo2010.ibge.gov.br; Datasus: Ministério da Saúde (Brazilian Ministry of Health), Informações de Saúde (Tabnet). Available at http://www2.datasus.gov.br/DATASUS/index.php?area=0205.
[34] R. Andersen and J. F. Newman, “Societal and individual determinants of medical care utilization in the United States,” Milbank Quarterly 4/83 (2005) pp. 1–28; Gloppen (2008, see note 26).
[35] Brazil, Lei Nº 11.709, de 19 de junho de 2008 DOU 20.06.2008 (2008). Available at http://www.portalbrasil.net/salariominimo_2008.htm.Banco; Central do Brasil, Conversor de Moedas (January 30, 2020). Available at https://www.bcb.gov.br/conversao.
[36] Biehl (2016a, see note 11); Biehl and Amon (see note 11).
[37] Biehl et al. (2012, see note 16); Biehl et al. (2016, see note 10).
[38] Biehl (2013, see note 11).
[39] Biehl and Amon (see note 11).
[40] Biehl (2013, see note 11).
[41] IQVIA Institute for Human Data Science, The global use of medicines in 2019 and outlook to 2023 (January 2019). Available at https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/the-global-use-of-medicine-in-2019-and-outlook-to-2023.pdf?_=1580501725523.
[42] Kapczynski (see note 11).
[43] Biehl (2013, see note 11).
[44] Biehl (2016, see note 11).
[45] Biehl et al. (2016, see note 10).
[46] Portal G1, “Planos de saúde passam a cobrir 37 medicamentos contra o cancer,” Bem Estar (October 31, 2013). Available at http://g1.globo.com/bemestar/noticia/2013/10/planos-de-saude-terao-de-cobrir-mais-37-medicamentos-para-cancer.html; Agência Nacional de Saúde Suplementar (Brazilian National Supplementary Health Agency), Planos de saúde vão oferecer 18 novos procedimentos em 2018 (2018). Available at http://www.ans.gov.br/aans/noticias-ans/sobre-a-ans/4192-planos-de-saude-vao-oferecer-18-novos-procedimentos-a-partir-de-2018.
[47] Biehl and Amon (see note 11).
[48] Ferraz (2016, see note 10); Biehl et al. (2016b, see note 10).
[49] J. Biehl and A. Petryna, “Legal remedies: Therapeutic markets and judicialization of the right to health,” in J. Biehl and A. Petryna (eds), When people come first: Critical studies in global health (Princeton, NJ: Princeton University Press, 2013), pp. 325–346; M. Medeiros, D. Diniz, I. Schwartz, and V. Doederlein, “A tese da judicialização da saúde pelas elites: Os medicamentos para mucopolissacaridose,” Ciência e Saú
de Coletiva 4/18 (2013), pp. 1089–1098.
[50] A. Joshi, “Legal empowerment and social accountability: Complementary strategies toward rights-based development in health?” World Development 99 (2017), pp. 160–172; E. Feinglass, N. Gomes, and V. Maru, “Transforming policy into justice: the role of health advocates in Mozambique,” Health and Human Rights Journal 2/18 (2016), pp. 233; T. Ezer, R. McKenna, and M. Schaaf, “Expert meeting on social accountability and legal empowerment: Allied approached in struggle for health rights” (New York: Open Society Foundation, 2015). Available at https://pdfs.semanticscholar.org/43e2/9608669f533c74625f546b3839360b7847b4.pdf; T. Ezer, N. Burke-Shyne, and K. Hepford, “Legal support for palliative care patients,” Journal of Pain and Symptom Management 2/55 (2018), pp. S157–S162.
[51] D. Diniz, Zika: From the Brazilian backlands to global threat (London: Zed Books, 2017); Biehl et al. (2018, see note 7).
[52] D. Brinks and V. Gauri, “A new policy landscape: Legalizing social and economic rights in the developing world,” in D. Brinks and V. Gauri (eds), Courting social justice: Judicial enforcement of social and economic rights in the developing world (Cambridge: Cambridge University Press, 2008), pp. 303–337.
[53] N. Daniels, Just health: Meeting health needs fairly (Cambridge: Cambridge University Press, 2008); E. Yamin, A. Pichon-Riviere, and P. Bergallo, “Unique challenges for health equity in Latin America: Situation the roles of priority-setting and judicial enforcement,” International Journal for Equity in Health 1/18 (2019), p. 106; Diniz (see note 49); Biehl et al. (2018, see note 7).
[54] World Health Organization, Health laws and universal health coverage. Available at https://www.who.int/health-laws/universal-health-coverage/en/.
[55] Kapczynski (see note 11).
[56] Biehl et al. (2018, see note 7); W. Sobrinho, “Processos contra planos de saúde aumentam 431% em 5 anos no Brasil,” UOL (November 13, 2018). Available at https://noticias.uol.com.br/saude/ultimas-noticias/redacao/2018/11/13/processos-contra-planos-de-saude-aumentam-531-em-5-anos-no-brasil.htm; D. Alves, L. Bahia, and A. Barroso, “O papel da Justiça nos planos e seguros de saúde no Brasil,” Cadernos de Saúde Pública 2/25 (2009).