Crisis Response as a Human Rights Flashpoint: Critical Elements of Community Support for Individuals Experiencing Significant Emotional Distress
Volume 22/1, June 2020, pp 105 – 120
Peter Stastny, Anne M. Lovell, Julie Hannah, Daniel Goulart, Alberto Vasquez, Seana O’Callaghan, and Dainius Pūras
Abstract
This paper proposes a set of nine critical elements underpinned by human rights principles to support individuals experiencing a serious crisis related to mental health problems or psychosocial disabilities. These elements are distilled from a range of viable alternatives to traditional community mental health approaches and are linked to a normative human rights framework. We argue that crisis response is one of the areas of mental health care where there is a heightened risk that the rights of service recipients may be infringed. We further make the case that the nine critical elements found in advanced mental health care models should be used as building blocks for designing services and systems that promote effective rights-based care and supports.
Introduction
Over the last two decades, the United Nations and other organizations have released a number of groundbreaking reports documenting widespread, systemic human rights abuses within mental health systems worldwide.[1] Overall, these documents emphasize the need to seek better health and social outcomes through sustainable means, using a human rights-based approach in keeping with the 2006 United Nations Convention on the Rights of Persons with Disabilities (CRPD) and the right to health framework. These normative standards, along with persistent calls by service users and advocates, have brought attention to the rights of persons with psychosocial disabilities, particularly the right to freedom from coercion in mental health services. They provide the impetus to find suitable practices to transform and modernize mental health care in communities everywhere.
However, the form and substance of rights-based interventions through which mental health service providers, family members, and other engaged citizens might offer support, without resorting to coercive and dehumanizing interventions, remain unclear. While promising non-coercive interventions for persons experiencing serious emotional crises have been piloted in several countries, usually as alternatives to involuntary hospitalization, better evaluation and research is needed to increase their potential for widespread implementation.[2] And although recent publications argue for such rights-based approaches, how to operationalize this evolving framework has yet to be described.[3]
The present paper fills this important gap by identifying a set of elements that are likely critical to rights-based support for individuals experiencing serious emotional crises, whether or not they use mental health services. The aim of this paper is to help ensure that a rights-based approach to crisis response becomes a distinct and crucial operational component of mental health care. Crisis response is a human rights flashpoint where coercive structures and practices dominate and the human rights threat to individuals is consistently manifest.
The critical elements presented in this paper are grounded in the rights-based approach and the right to health. Specifically, they correspond to principles underlying the key normative frameworks enshrined in the CRPD and to the principle of the right to the enjoyment of the highest attainable standard of mental and physical health, which are incorporated into article 12(1) of the International Covenant on Economic, Social and Cultural Rights (ICESCR).[4] We follow the 1946 Constitution of the World Health Organization in defining health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”[5]
A quest for rights-based mental health systems
Practices with the potential to transform or replace community-based mental health care have been in existence, and many shown to be effective, since the advent of modern community psychiatry in the mid-1960s. Some, such as the Italian and Brazilian experiences, involve large-scale mental health reforms driven by deinstitutionalization and the development of sectorized community mental health services.[6] However, they also include highly innovative, small-scale efforts that have eluded larger systems.[7] These have been spearheaded by former patients or by visionary psychiatrists; many focus on people experiencing psychosis.[8] Most began as alternatives to coercive treatment and enhance personal liberties. Although these initiatives preceded the contemporary human and disability rights discourse by years, they contain critical elements which align with these rights.
A first type of innovation, beginning in the 1970s, involves small, community-based support structures. For example, the Soteria model provides a safe community home, largely non-professional staffing, and minimal medication use as a substantive, non-coercive alternative to acute hospitalization for people experiencing early psychosis.[9] Consumer/survivor/ex-patient groups have established other alternatives to mainstream mental health services for people in crisis.[10] The strongest outgrowth—peer-run respite facilities—provides peer support and non-coercive safe spaces where individuals in crisis can stay for varying periods of time.[11] Some such solidly established initiatives include the Berlin Runaway House (Germany), the Bapu Trust (India), and Western Massachusetts Recovery Learning Community (United States).
A later crisis response paradigm is embodied in the now widespread Open Dialogue model, created in Finland in the 1980s. Instead of an alternative residential setting, Open Dialogue uses systemic network approaches to support individuals in crisis in their homes and communities.[12] Structured conversations between a treatment team, the person in crisis, and members of her social network give equal weight to all viewpoints on the crisis, even those that would elsewhere be dismissed as “psychotic.” By engaging persons in crisis with their network members, Open Dialogue attempts to transform the experience of “psychosis” and to destigmatize and empower the person in crisis.[13]
Alternative and “radical” models often show better social and clinical outcomes than “standard care”; others, according to Piers Gooding et al., may contribute to lowering coercive hospitalization.[14] Yet they have failed to spur rights-based, voluntary mental health systems. Instead, involuntary hospitalization, mandatory community treatment, and other coercive measures have risen significantly in Europe and North America, despite consistently poor outcomes.[15] Meanwhile, in the Global South, where mental health care is either lacking or depends almost exclusively on hospitalization, powerful global health actors working to close the “treatment gap” promote interventions focused primarily on medication use, rather than strategies to reduce coercion and safeguard human rights.[16] While advocates critique these neoliberal development strategies, global health proponents argue that only evidence-based practices merit replication.[17] This criterion excludes many rights-based alternatives which are difficult to test through traditional experimental designs. Yet usual crisis responses (such as police intervention and involuntary hospitalization) are taken for granted without being submitted to the same research standard.
This contradictory situation calls for a wide range of localized innovations that adhere to human rights law while offering workable alternatives to the dominant mental health system.
This paper contributes critical elements as guideposts for such efforts. Rather than proposing one paradigm, a competing technology, or total system reform at once, it offers rights-based building blocks that, when endorsed by local stakeholders, can contribute to system reconfiguration of responses to serious mental health crises.
Methodology: Linking abstract principles and practical responses
To identify critical elements of a rights-based approach to crisis response, we modified Paul Hunt’s three-step process for developing a normative framework of human rights principles and values and translating them into practical elements.[18] Whereas Hunt’s model moves from the abstract to the practical, we chose to identify already existing practices and confirm their human rights underpinnings.
First, we located the human rights laws and standards that should underpin elements of a rights-based approach (normative framework). Second, we specified a core set of human rights principles and values expressed in this framework. Third, we identified elements of crisis response practices that research shows or that our clinical and advocacy practice suggests are anchored in human rights. Most research to date focuses on whether entire programs, but not specific components, contribute to avoiding hospitalization, and its results are mostly inconclusive. Most studies focus on avoidance of coercion as the outcome, but some studies examine the association of these practices with a subjective sense of empowerment.[19]
The critical elements identified through clinical and advocacy experience are described in the second part of the paper. Our practice employs experience-based phenomenological processes to discern what persons in crisis might experience as coercive—a dimension that conventional, positivist evidence-based research may not pick up.[20] Rather than relying on normative criteria based on objective behavioral response, we focus on understanding the singular subjective processes involved in a situation of crisis. This approach better suits the perspective of human rights, especially if social, cultural, and individual differences are to be taken seriously. We selected those elements that seemed aligned with specific human rights principles in the normative framework. The result is a set of nine critical elements that can be operationalized, subjected to research, and embraced as components of rights-based approaches to mental health crises.
Normative framework
There is no universal definition of a “rights-based approach to health” in general or specific to the mental health context.[21] This paper takes a rights-based approach to crisis response to include the full spectrum of civil, political, social, economic, and cultural rights: the rights of the child; the rights to privacy, life, participation, association, non-discrimination, equality, and family; and the prohibition of torture and cruel, inhuman, or degrading treatment or punishment. Health policies, strategies, and programs are to be guided by all these human rights standards and principles and should aim at empowering rights holders and strengthening the capacity of duty bearers. The proposed critical elements emanate from these core normative standards, but they importantly and explicitly foreground the right to the enjoyment of the highest attainable standard of physical and mental health (the right to health) and the specific rights enshrined by the ICESCR, adopted in 1966.
The right to health is recognized in various international and regional human rights treaties and enshrined in the Constitution of the World Health Organization. All states have ratified one or more of these instruments. While the right to health includes both freedoms and entitlements and has been interpreted to encompass both health care and the underlying social and psychosocial determinants of mental and physical health, operationally it has been understood to possess unique elements essential for the effective implementation of a rights-based approach to crisis response.[22]
According to Sofia Gruskin, Dina Bogecho, and Laura Ferguson, a minimal set of operational elements of the right to health includes availability, accessibility, acceptability, and quality (the AAAQ framework), as well as participation, transparency, and accountability.[23] The AAAQ framework finds its legal basis in General Comment 14 of the Committee on Economic, Social and Cultural Rights and is a unique and essential feature of the right to health. How these operational elements of the right to health have been articulated over time both through the CRPD and through the work of authoritative sources, such as the Committee on the Rights of Persons with Disabilities and reports of the United Nations Special Rapporteurs on the right to health and on the rights of persons with disabilities, informs our proposed framework.
The CRPD represents the highest standard of protection for the rights of persons with disabilities. It calls for the full realization of all human rights and fundamental freedoms for all persons with disabilities (actual or perceived), and it outlines specific steps to be taken by state parties to ensure the full and equal enjoyment of these rights.
Emphasizing the universality, indivisibility, and interdependence of human rights, the CRPD effectively contributes to a rights-based approach to crisis response by stressing the principle of non-discrimination and the notion of support in the exercise of rights. Article 12 of the CRPD affirms the legal capacity of all persons with disabilities in all areas of life and acknowledges the role of supported decision-making in exercising legal capacity. Article 14 of the CRPD clarifies that “the existence of a disability shall in no case justify a deprivation of liberty,” which the Committee on the Rights of Persons with Disabilities and other bodies and experts have interpreted as an “absolute ban” to involuntary commitment to a mental health facility, including in crisis situations.[24] Furthermore, as underscored by Catalina Devandas, article 25 of the convention reaffirms the right of all persons with disabilities to the enjoyment of the highest attainable standard of health without discrimination, including the right to free and informed consent.[25]
In sum, under the CRPD framework, impairments—whether actual or perceived, or temporary or long standing—cannot be a legitimate ground for the denial or restriction of human rights, particularly in the context of crisis response, which often has been considered as exempted from those very safeguards. The support paradigm of the CRPD calls for non-coercive support responses within and outside the health sector.[26] In doing so, the CRPD questions previous international and regional standards that allow for exceptional circumstances in which the rights of persons with psychosocial disabilities could be restricted in the context of mental health provision.[27] While some CRPD detractors claim that a ban on coercive practices may endanger the right to health of persons with psychosocial disabilities, there is an increasing consensus that the CRPD represents an opportunity to realize a rights-based approach to mental health care.[28]
Key underlying principles
The core set of human rights principles and values that underpin the critical elements spring from the need to mitigate the losses of rights described in the ICESCR and CRPD that can occur when individuals experiencing a mental health crisis interact with emergency services and other systems of care. To be diagnosed with a mental illness can be stigmatizing and can result in a loss of social capital for individuals within their communities. In many legal contexts around the world, a diagnosis amounts to being labeled non compos mentis and means a loss of the enjoyment of a range of rights under international law. Once this occurs, substitute decision-making takes the place of self-determination. Emergency responders—police, medics, and others—are often empowered to apply force, to medicate without consent, to restrain, and to detain an individual for observation. In the worst such circumstances, individuals experiencing what appears to be a mental health crisis lose not only their rights but also their lives. Most survive the ordeal but, in many countries, they may be detained indefinitely, ostensibly for the safety of the larger community and without the provision of adequate care. In more progressive countries, where deinstitutionalization has advanced, substitute decision-making can remain in force for years, and legally mandated treatment with psychiatric medications as a condition for release from institutional detention or regaining other rights and freedoms is widespread and growing.[29]
The key principles that guide the identification of the critical elements for rights-based mental health care are selected here because they can eliminate substitute decision-making and promote self-determination for individuals within crisis response and systems of mental health support. Without these assurances, crisis situations, whether gradually or rapidly evolving, are likely to result in the immediate and sustained infringement of human rights. Crisis is defined but not limited to a broad range of experiences: sudden or frightening levels of agitation or turmoil; long-term withdrawal and isolation without attention to basic needs, physical health, or safety; suicidal intent; intense interpersonal animosity; expression of extreme fear or beliefs at odds with those of others; elevated mood or behavior; loss of awareness of surroundings; and struggling to plan and use foresight in their actions.
Participation and empowerment
Empowered participation has proved critical in improving care through preserving and bolstering the rights of persons with psychosocial disabilities in countries that have undergone deinstitutionalization, such as the United States, Italy, Portugal, and Brazil, to name some of the best-documented instances. In the United States, empowerment became the central organizing principle among the consumer/survivor/ex-patient movement that emerged from the era of deinstitutionalization and that has improved care for those with the most severe diagnoses, reducing inhumane practices and excessive use of seclusion and restraint. Empowerment and inclusion are proposed by consumer/survivor groups as measures of mental well-being. In our view, empowerment establishes a virtuous cycle of increased freedoms and well-being for those who are diagnosed with mental illnesses. Ideally, all critical elements should either promote or not restrict participation and empowerment.
Equality and non-discrimination
Article 5 of the CRPD upholds a complex substantive model of equality that addresses structural and indirect discrimination, values different layers of identity, and acknowledges intersectional discrimination.[30] Consistent with this strong definition of non-discrimination, the critical elements of mental health programs and systems should “recognize that all persons are equal …, prohibit all discrimination on the basis of disability …, and take all appropriate steps to ensure that reasonable accommodation is provided.” Persons with psychosocial disabilities must be supported in exercising rights and should not be restricted in their exercise.
Quality and diversity of care
If the quality of mental health care is deficient, then the right to mental health care is effectively curtailed. Consistent with the principles of non-discrimination and equality, the critical elements should require that programs and systems of mental health care and psychosocial support be of high quality, be at least on par with quality standards for general health care, and demonstrate a record of, or hold reasonable promise of, promoting improved well-being and recovery. The effectiveness of supports should be measurable in ways that are meaningful to the individuals receiving care, and supports should be provided within an organized and accountable network. Because there is no singular recognized cure for any mental health problem, and because both personal and cultural diversity have strong and largely unpredictable effects on mental well-being, a multiplicity of options for care and models of care is essential.
Social inclusion
Social exclusion often lies at the heart of mental health problems and crises and limits the achievability of empowerment while interfering with the basic human need for social connectedness. Therefore, the critical elements must not inhibit and, when applicable, should actively promote social inclusion for and destigmatization of individuals with psychosocial disabilities.
Autonomy and dignity
The principle of autonomy means that individuals can make their own decisions about their lives, with adequate support if required, avoiding substitute decision-making. Respect for autonomy bolsters individuals’ rights to choose the types and elements of the care and support they receive and to make decisions about their lives as independently as possible. It must be accounted for within the critical elements of crisis response. Each person should be respected as an individual with the right to autonomy and with the inherent dignity of a free person with equal rights to all others. People with psychosocial disabilities have the right to make decisions that others feel are unwise or with which they disagree.
Critical rights-based elements for crisis response
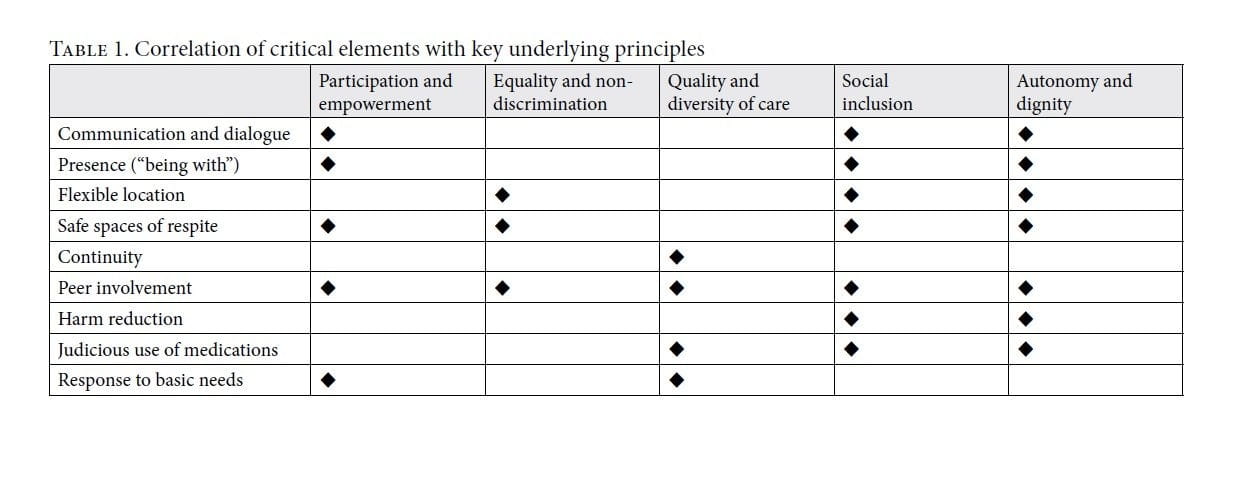
The critical elements of rights-based services for individuals in psychiatric crisis should be underpinned by the five key principles described above. Each of the following nine rights-based critical elements for response to mental health crisis incorporates up to five of these principles (Table 1). While no single critical element encompasses all five principles, a human rights-based crisis response integrating more than one element would likely translate all five into concrete practices.
 1. Communication and dialogue
1. Communication and dialogue
The reality or the belief that it is impossible to be heard and understood is often central to an individual’s mental health crisis. Connection to a trusted professional, friend, or “person with experience” can help resolve the immediate situation and avoid coercive consequences. Supportive communication underlies programs ranging from the widely disseminated Friendship Bench, developed in Zimbabwe, to free-standing peer-support techniques.[31] Dialogical encounters, the communication paradigm underlying Open Dialogue and other programs, foster unexpected viewpoints, contradictions, and change. Both paradigms may broaden social capital by reinforcing already available relationships or building new networks around the crisis. The range of dialogical communication can extend from simple one-on-one exchanges to complex engagements in group-formats (“network meetings”).
Communication and structured dialogue correspond to three key rights principles. Both facilitate empowerment, autonomy, and social inclusion through listening, gauging the distressed person’s tolerance for others present, and involving him or her in deconstructing the situation of crisis. Social inclusion is preserved through acceptance of coexisting differences and conflicts, which in turn avoids a collapse of interpersonal relationships. Interventions based on immediate, frequent, and sustained dialogue with people experiencing psychosis have been shown to have better clinical outcomes than usual treatment and to circumvent coercion and overmedication.[32]
2. Presence (“being with”)
Alongside communication, presence—the idea of simply “being with”—responds to the basic human need for authentic human companionship, especially in crisis situations. As a result, it reinforces three rights principles: participation, social inclusion, and the autonomy and dignity of the person in crisis. The art of spending time with a person, without a predetermined objective, has been a key element in pioneering programs for persons experiencing acute psychosis (“altered states”), such as Windhorse, Soteria, Diabasis, and Emanon.[33] Time spent together may occur in a scheduled manner, such as during three-hour “basic attendance” sessions (Windhorse, a crisis support program based on contemplative principles) or 24–78 hour shifts (Soteria) or more spontaneously. Autonomy is preserved through continual renegotiation of the degree of physical closeness and active engagement in a space that protects the safety of the person in crisis. The mere fact of sharing space with someone in extreme distress communicates trust and has been shown to have a sustained calming effect.[34]
3. Flexible location
Ideally, mental health workers should encounter someone in extreme distress in flexible locations, especially wherever that person happens to be or to feel most comfortable. Equality, non-discrimination, and social inclusion are preserved through flexibility as opposed to transporting the person to a “special” or stigmatizing place (such as a psychiatric service or institution). Autonomy and dignity are assured if the person in crisis invites the worker into his or her home or “personal territory” on the street, or if his or her personal space is safeguarded in shared living spaces.[35]
Mobility, outreach and home visits recognizing flexible location are key components of many community mental health services, including crisis intervention.[36] Ethnographic research has shown that respecting or being welcomed into the spaces occupied by homeless persons in crisis can be conducive to a better understanding and resolution of the situation.[37]
4. Safe spaces of respite
Persons in distress may seek safe spaces of “respite” from harmful or traumatizing environments, which may have provoked or could sustain the mental health crisis.[38] Respite spaces can provide around-the-clock support for individuals in crisis, through several-day to two-week stays.[39] Such spaces meet key rights principles of empowerment, equality and non-discrimination, social inclusion, and autonomy and dignity, as long as decisions to use them are made by the person in crisis or collaboratively.
Respite services involve peer workers, make pantry and cooking facilities continuously accessible, organize group meetings, and allow residents to come and go and pursue outside activities. Overtly illegal acts are not tolerated and can lead to being asked to leave.[40] Trained lay families or friends can also provide relief outside the home. Both types of respite have been shown to have better outcomes than hospitalization and to safeguard human rights.[41] Such rights-based respite approaches must be differentiated from those affiliated with locked or otherwise coercive mental health services.[42]
5. Continuity
Continuity of care remains an elusive goal of mental health services, in spite of widespread consensus regarding its essential role.[43] Continuity of personnel beyond the moment of crisis is almost nonexistent in current systems of care.[44] Critical Time Intervention, peer-bridgers, and Open Dialogue provide continuity by at least one person from the initial encounter through crisis resolution, but they are exceptions to this rule.[45] Such ongoing connection empowers the person and assures quality and diversity. In contrast, such typical practices during crisis assessments as “assessment and referral,” triage, and other means of handing the person over to another service emphasize technical and managerial solutions rather than the development of emotional bonds. While some respond well to a one-time intervention, the offer of an ongoing relationship provides a powerful tool for persons in crisis to reconstitute their lives, even in the face of fractured connections. Continuity may be especially crucial when the person in crisis is suicidal.
6. Meaningful peer involvement
“Experts by experience,” also known as peer workers or peer specialists, are trained to use their personal mental health and psychosocial disability experiences to help persons in crisis. While the personal life experiences of anyone who seeks to help others can be used in powerful ways, interventions based on the unique personal experience of extreme mental states and with various treatment responses have been widely embraced. Meaningful peer involvement in crisis situations, alone or with other mental health providers, ideally meets all five key rights principles in our framework.
When peer workers engage and judiciously disclose their personal experiences as they apply to the crisis situation at hand, they support and empower the person in crisis in a non-discriminating manner that preserves dignity and promotes social inclusion.[46] To ensure the standard for quality that the right to health assumes, peers should be well trained in the subtle and often tacitly acquired skill (for example, Intentional Peer Support). Peer collaboration has been used by some non peer respites and Open Dialogue teams to generate innovative types of support.[47]
Peer-led services appear to contribute to reducing coercive interventions and the cost of services.[48] In this regard, the extent to which crisis responses require professionalization or can be directly provided by lay or peer practitioners outside medicalized frameworks is an essential question that requires greater attention.[49] To be successful, peer involvement must be meaningful and not be implemented in a tokenistic fashion. In too many instances, peer involvement is encumbered by power imbalances, where peer workers are involved in a superficial manner and have little or no control over crisis responses.[50]
7. Harm reduction
Harm reduction approaches prioritize access to care by reducing or eliminating behavioral thresholds linked to disturbing, taboo, or even illegal behaviors. This model was pioneered in the domain of substance use services but can be applied to mental health, including for those without substance-related problems. Within the harm reduction paradigm, people are supported in their efforts to eliminate, avoid, or lessen risks associated with mental health problems, such as cutting or other forms of self-harm, unsafe sex, radical isolation, and illicit drug use. In this way, harm reduction assures the principle of diversity in health care, through social inclusion that respects the dignity and autonomy of the person. One can assume that reconceptualizing risk assessment into harm reduction will increase the quality of care and its outcomes.
Harm reduction focuses on providing care in a non-stigmatizing manner while tolerating the engagement in risky behavior. Such care is achieved by maintaining a collaborative stance with the person, who may be ashamed and fearful of losing rights due to such behavior, when seeking help. Importantly, harm reduction considerations are different from risk-benefit calculations, since no external assessment of risks or benefits concerning the situation or behavior is involved.[51] In other words, engaging with a broad range of risks in mental health supports is taken as a given, rather than a separate “administrative” layer of concern, which inherently interferes with a host of human rights principles.[52]
Responses to mental health crises that incorporate harm reduction principles may be more acceptable to distressed persons because they destigmatize harmful acts and reduce shame. For example, a person who engages in physical self-harm can be supported by considering less harmful ways instead of provoking categorical interdiction. Still, some situations will require the ongoing presence of another alert human being who may step in to engage the person in a conversation, or even, with permission, to gently prevent them from self-harm by physical contact (for example, through touch, not wrestling).[53]
However, violence against another person should be considered not a psychiatric problem but a likely violation of criminal law. A person in crisis who engages in interpersonal violence may be warned; in addition, the threatened individuals may be protected, and non-discriminatory police intervention may be called on to avert potential harm. Judicial guarantees and safeguards protecting the rights of those accused of a crime should apply in such cases, including the presumption of innocence, the right to a fair trial, and the provision of procedural accommodations.[54]
8. Judicious use or avoidance of psychotropic medications
Because the distinctions among prescribed psychiatric drugs, over-the-counter remedies, and licit (for example, alcohol) and illicit substances is relatively arbitrary, a harm-reduction approach is applicable to all of them. Meta-analyses suggest that less psychotropic medication is superior to more and that cautious gradual introduction is preferable to an immediate and high-dose prescription. Intermittent use under the person’s control is likely less harmful over the short and long term than ongoing “maintenance” administration.[55] However, intermittent use may also increase the risk of harm due to inconsistent effects on receptor sites, an issue beyond the scope of this paper.[56]
Judicious psychotropic use enhances the quality and diversity of health care and ensures the autonomy and dignity of the person in crisis. How the person in distress views medication can help determine the most beneficial alternative.[57] Providing medication at the request of the person in crisis—for example, for quick relief of insomnia or intense anxiety—can be an important step in crisis resolution that also protects the person’s rights.[58] On the contrary, the forced administration of psychotropic drugs is considered by many to be equivalent to torture and physical abuse.[59] Indiscriminate use of medication can undermine trust; it interferes with optimal, dignified care and frequently ignores the person’s preference.
9. Response to basic needs
Many, if not most, crises manifested in emotional distress originate in interpersonal problems or environmental stressors (such as poor nutrition; lack of clothing, funds, or access to transportation; housing conditions; and legal problems). Such adversities can push someone from a state of adequate functioning to severe distress.[60] Empowerment of the person in distress and quality and diversity of health care are promoted when basic needs are addressed immediately. This may involve mobilizing a person’s natural support system, collaborating with him or her on problem-solving, and even providing material resources, such as food, clothing, or money, which will yield desired results quickly. Bureaucratic obstacles also often trigger crises, and a competent guide through such mazes (for example, concerning health coverage, financial benefits, or access to essential services) can go a long way. The worldwide Housing First movement advocates for housing without requiring that the person in crisis be in a stable condition.[61]
Practical application of critical rights-based elements
Peer-run organizations such as the Western Massachusetts Learning and Recovery Center and Bapu Trust in India incorporate all nine critical elements.[62] Although current mental health systems would be unlikely to accomplish this, it is possible to demonstrate how crisis response can engage the nine critical elements as safeguards of the five key rights principles.
The following example from our work illustrates this possibility in real life. It involves a woman in her forties who was first encountered in the streets when she appeared to be wandering into traffic without paying much attention. When an outreach team pair (peer specialist and social worker) approached her, she seemed intoxicated from alcohol and spoke about scary people who were following her. By listening, without encroaching on her space, the team was able to conclude that the women’s fears were outside consensual reality but that she recognized the need to be more careful with street traffic (communication and dialogue, presence, flexible location, and meaningful peer involvement).
The same team re-contacted the woman several times on the street and brought her food and warm bedding, which she had requested. She eventually accepted going to a respite space instead of being taken to a psychiatric emergency room (continuity, respite, and basic needs).
At the respite center, her drinking bothered residents who were trying to stay sober. The respite workers successfully sought a “wet house,” which allowed her to drink and supported her in limiting the amount and frequency (harm reduction). The outreach team pair continued to spend time with her and support her with nutrition, personal hygiene, and forward planning (presence and continuity). When the woman complained about medications she had taken in the past, a consultant psychiatrist involved her in a collaborative plan to use medication only as needed which was the least adversely interactive with alcohol (judicious use of medication). The team pair helped her apply for long-term supported housing and reconnect with her children.
Accountability
Accountability, one of the most powerful aspects of a rights-based approach, should tie all nine critical elements to a rights-based culture. Accountability is necessary for ensuring that the rights of individuals within a system of care are upheld and that quality of care is preserved.
It is also an essential aspect of how rights-based critical elements can be “rightly” implemented. As such, it requires a system or organization that can embed what is to be accounted for, to assure not only that rights are respected but also that a full range of critical elements, perhaps even beyond those mentioned above, are validly and reliably put into practice as proposed.[63]
In order to succeed in creating a rights-based alternative to coercive standard care, a robust accountability framework should take into account the above critical elements and local law. It should provide means of pressuring existing mental health systems and programs to operationalize alternatives through a plurality of appropriate choices. The adoption of such measures, as well as an effective but not overly onerous approach to ensuring quality of care, must be acceptable to relevant stakeholders, particularly users of mental health services and supports. One example of a tool that can monitor such a process is the World Health Organization’s Quality Rights Initiative.[64] Evaluation of crisis response is a crucial component of this accountability framework, and the promotion and upholding of the CRPD standards should be incorporated as outcome measures. Finally, the meaningful and routine inclusion of service users within teams that evaluate, monitor, and report on service implementation and outcomes is an important part of ensuring accountability.
Risks and limitations
The greatest limitations to establishing supports that uphold human rights for individuals in mental health crisis lie with the vested interests that hold most power within existing mental health systems.[65] The two most prominent are the pharmaceutical industry and the mainstream medical establishment, which is still largely centered around hospital-based services.[66] Half a century ago, antipsychotic medications were heralded by policy makers as miracle cures that would enable those deemed in need of being separated from society to leave psychiatric institutions. The ensuing deinstitutionalization failed largely from lack of adequate community-based alternatives. In the meantime, the efficacy of psychotropic medications has been shown to be equivocal, adverse, even lethal, outcomes (such as dependency, metabolic disease, and suicidality) are not uncommon. Despite this, the pharmaceutical industry and its lobbyists have shaped public policy for decades.[67] Psychiatrists and other mental health professionals are key players in this status quo, and their incentives are skewed toward a focus on short-term evidence of medication effectiveness and away from long-term well-being, recovery, and human rights.[68]
Mainstream critics largely dismiss psychosocial interventions on the grounds that they lack an adequate evidence base. They also argue that implementing such alternatives would put people in crisis and the community around them at risk. Psychosocial interventions, which we argue can preserve rights and improve well-being, are much more complex and difficult to study. Yet their study receives vastly less funding than medication-related research. Researchers should advocate for more funding and develop the evidence base for such alternatives, and civil rights advocates should join forces with them in this effort.
As we have noted, several international developments and reports uniformly decry present conditions and call for a complete revamping of the current mental health system. However, countries, guilds, and mental health systems have yet to take these challenges seriously. Exceptional local efforts to redesign mental health services remain insular and rely on limited funding and practical experience, while broadcasting excellent values and beliefs.
Another important tool that has not been addressed in this paper is the availability and promotion of psychiatric advance directives that can be used by persons with psychosocial disabilities in an attempt to influence crisis response in the future.[69] While important to the advocacy movement and to many persons with psychosocial disabilities, of advance directives’ the widespread impact on system transformation is still doubtful.[70]
Where do we go from here?
The trajectory within international law clearly bends toward greater freedom and autonomy for people with psychosocial disabilities, although significant barriers to upholding those freedoms and autonomy remain, particularly at a point of crisis when state authorities may intervene. However, since the 1960s, when the era of deinstitutionalization began, a range of alternatives to coercive treatment, especially for those in crisis, have been developed that can show the way toward the realization of rights-based crisis mental health care.
In countries where health systems are less funded and medical professions less powerful than in the Global North, the status quo may resemble the pre-deinstitutionalization era and may be replicating some of the least promising practices in post-colonial settings.[71] Global South nations must rely on cheaper and hence older generic medications, which have high-risk profiles, especially in the short term. As a result, seclusion and restraint, including the chaining of individuals, are frequently used.[72] Implementing the nine critical elements that preserve human rights, for example as part of a comprehensive Open Dialogue approach, requires considerable human interaction by paid staff, and certainly costs more than medication-centered practices.[73] In resource-poor environments, providing training to non-professional lay providers from the community and mental health peers that allows them to assist in preventing coercion and restraint and in implementing basic interventions may help overcome cost barriers.
Based on the characteristics of some of the more promising and prominent alternative models in the literature, we have distilled nine critical elements that incorporate key principles of the right to health. These can provide valuable guideposts for those who are either reforming or developing community mental health supports in an effort to adopt international humanitarian standards of care.
Peter Stastny, MD, is Consulting Psychiatrist at Community Access and the Pratt Institute, New York, USA, and founding member of the International Network towards Alternatives and Recovery.
Julie Hannah is Co-Director of the International Centre on Human Rights and Drug Policy and a member of the Human Rights Centre, University of Essex, UK.
Anne M. Lovell, PhD, is Senior Research Scientist Emerita at INSERM (Institut de Santé et de la Recherche Medicale) at CERMES 3, Villejuif and Paris, France.
Daniel Magalhães Goulart, PhD, is Associate Professor of the Faculty of Education and Health Sciences, University Center of Brasilia, Brazil.
Alberto Vasquez Encalada is Research Coordinator, Office of the United Nations Special Rapporteur on the Rights of Persons with Disabilities, Geneva, Switzerland, and Chair of Sociedad y Discapacidad – SODIS, Lima, Peru.
Seana O’Callaghan is a consultant research scientist in New York, USA.
Dainius Pūras, MD, Clinic of Psychiatry, Vilnius University, Lithuania, is the United Nations Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of health.
Please address correspondence to Peter Stastny. Email: pestastny@yahoo.com.
Competing interests: None declared.
Copyright © 2020 Stastny, Lovell, Hannah, Goulart, Vasquez, O’Callaghan, and Pūras. This is an open access article distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] N. Drew, M. Funk, S. Tang, et al., “Human rights violations of people with mental health and psychosocial disabilities: An unresolved global crisis,” Lancet 378/9803 (2011), pp. 1664–1675; European Network of (Ex-) Users and Survivors of Psychiatry, Submission of the European Network of (Ex-) Users and Survivors of Psychiatry (ENUSP) for the day of general discussion (DGD) on the right of persons with disabilities to live independently and be included in the community, to be held on 19 April 2016 in Geneva. Available at https://www.ohchr.org/Documents/HRBodies/CRPD/DGD/2016/EuropeanNetworkof_Ex-_Users_and_Survivors_Psychiatry-ENUSP.doc; World Health Organization, Quality rights, promoting human rights in mental health. Available at https://www.who.int/mental_health/policy/quality_rights/en/; United Nations Working Group on Arbitrary Detention, United Nations basic principles and guidelines on remedies and procedures on the right of anyone deprived of their liberty to bring proceedings before a court, UN Doc. WGAD/CRP.1/2015 (2015); United Nations, Report of the eighth session of the Conference of States Parties to the Convention on the Rights of Persons with Disabilities, UN Doc. CRPD/CSP/2015/5 (2015); C. Devandas, Report of the Special Rapporteur on the rights of persons with disabilities, UN Doc. A/HRC/40/54 (2019).
[2] P. Gooding, B. McSherry, C. Roper, and F. Grey, “Alternatives to coercion in mental health settings: A literature review” (Melbourne Social Equity Institute, University of Melbourne, 2018). Available at https://socialequity.unimelb.edu.au/__data/assets/pdf_file/0012/2898525/Alternatives-to-Coercion-Literature-Review-Melbourne-Social-Equity-Institute.pdf; S. P. Mann, V. J. Bradley, and B. J. Sahakian, “Human rights-based approaches to mental health: A review of programs,” Health and Human Rights 18/1 (2016), pp. 263–275.
[4] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006); International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 12.
[5] Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006); International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 12; Constitution of the World Health Organization (1946).
[7] L. Mosher and L. Burti, Community mental health: Principles and practice (New York: W. W. Norton, 1981).
[8] M. W. Cornwall, “Merciful love can relieve the emotional suffering of extreme states,” Journal of Humanistic Psychology 59/5 (2019).
[9] L. Mosher, “Soteria and other alternatives to acute psychiatric hospitalization: A personal and professional review,” Journal of Nervous and Mental Disorders 187/3 (1999), pp. 142–149.
[10] P. Stastny and P. Lehmann (eds), Alternatives beyond psychiatry (Berlin: Peter Lehmann Publishing, 2007).
[11] L. Ostrow and B. Croft, “Peer respites: A research and practice agenda,” Psychiatric Services 66/6 (2015), pp. 638–40.
[12] J. Seikkula and M. E. Olson, “The Open Dialogue approach to acute psychosis: Its poetics and micropolitics,” Family Process 42/3 (2003), pp. 403–418.
[13] M. Olson, J. Seikkula, and D. Ziedonis, The key elements of dialogic practice in Open Dialogue (Worcester: University of Massachusetts Medical School, 2014); L. P. Kantorski and M. Cardano, “Open Dialogue and the challenges for its implementation: An analysis based on a review of the literature,” Ciência e Saúde Coletiva 24/1 (2019), pp. 229–246.
[14] Gooding et al. (see note 2).
[15] A. Turnpenny, G. Petri, A Finn, et al., Mapping and understanding exclusion: Institutional, coercive and community-based services and practices across Europe: Project report (Brussels: Mental Health Europe, 2018); E. Fabris, Tranquil prisons: Chemical incarceration under community treatment orders (Toronto: University of Toronto Press, 2011).
[16] D. Pūras D and J. Hannah, “Prioritizing rights-based mental health care in the 2030 Agenda,” in L. Davidson (ed), The Routledge handbook of international development, mental health and wellbeing (New York: Routledge, 2019); V. Patel, S. Saxena, C. Lund, et al., “The Lancet Commission on Global Mental Health and Sustainable Development,” Lancet 392/10157 (2018), p. 6; Lancet, Global mental health 2007. Available at https://www.thelancet.com/series/global-mental-health; Lancet, Global mental health 2011. Available at https://www.thelancet.com/series/global-mental-health-2011; S. J. Hoffman, L. Sritharan, and A. Tejpar, “Is the UN Convention on the Rights of Persons with Disabilities impacting mental health laws and policies in high-income countries? A case study of implementation in Canada,” BMC International Health Human Rights 16/28 (2016).
[17] C. Mills, Decolonizing global mental health: The psychiatrization of the majority world (London: Routledge, 2014).
[18] P. Hunt, “Interpreting the international right to health in a human-rights based approach to health,” Health and Human Rights Journal 18/2 (2016), pp. 109–126.
[19] Gooding et al. (see note 2); Olson (see note 13); Kantorski and Cardano (see note 13); Turnpenny et al. (see note 15).
[20] N. K. Denzin and Y. S. Lincoln, The Sage handbook of qualitative research, 5th edition (London: Sage, 2018); Tarabochia (see note 6).
[21] Hunt (see note 16).
[23] S. Gruskin, D. Bogecho, and D. Ferguson, “‘Rights-based approaches’ to health policies and programs: Articulations, ambiguities and assessment,” Journal of Public Health Policy 31/2 (2010), pp. 138–140.
[24] Devandas (2019, see note 1).
[25] C. Devandas, Report of the Special Rapporteur on the rights of persons with disabilities, UN Doc. A/73/161 (2018), paras. 14–15.
[26] Devandas (2019, see note 1), para. 56.
[27] Ibid.
[29] S. R. Kinsley, L. A. Campbell, and R. O’Reilly, “Compulsory community and involuntary outpatient treatment for people with severe mental disorders,” Cochrane Database of Systematic Reviews 3 (2017), pp. 1–63.
[30] T. Degener, “Disability in a human rights context,” Laws 5/3 (2016).
[31] D. Chibanda, H. A. Weiss, R. Verhey, et al., “Effect of a primary-care based psychological intervention on symptoms of common mental disorders in Zimbabwe: A randomized clinical trial,” JAMA 316/24 (2016), pp. 2618–2626; R. K. Schutt and E. S. Rogers, “Empowerment and peer support: Structure and process of self‐help in a consumer-run center for individuals with mental illness,” Journal of Community Psychology 37/6 (2009), pp. 697–710.
[32] Olson et al. (see note 13).
[33] J. Fortuna, “Therapeutic households,” Journal of Contemplative Psychotherapy 4 (1987), pp. 49–76; Mosher (see note 9); R. Bennett, “The Crisis Home Program of Dane County,” in R. Warner (ed), Alternatives to hospital for acute psychiatric treatment (Washington, DC: American Psychiatric Press, 1995), pp. 227–236; J. Fortuna, “The Windhorse Program for Recovery,” Journal of Contemplative Psychotherapy 9 (1994), pp. 73–96.
[34] S. Mead and D. Hilton, “Crisis and connection, speaking out,” Psychiatric Rehabilitation Journal 27/1 (2003), pp. 87–94.
[35] E. Goffman, “The interaction order,” American Sociological Review 48/1 (1983), pp. 1–17.
[36] S. M. Murphy, C. B. Irving, C. E. Adams, and M. Waqar, “Crisis intervention for people with severe mental illnesses,” Cochrane Database of Systematic Reviews 12/5 (2015), pp. 1–89.
[37] M. Rowe, Crossing the border (Berkeley: University of California Press, 1999).
[38] J. Cullberg, S. Levander, R. Holmqvist, et. al., “One-year outcome in first episode psychosis patients in the Swedish Parachute project,” Acta Psychiatrica Scandinavica 106 (2002), pp. 276–285.
[39] B. A. Stroul, “Residential crisis services: A review,” Hospital and Community Psychiatry 39/10 (1988), pp. 1095–1099; Ostrow and Croft (see note 11).
[40] E. E. Bouchery, M. Barna, E. Babalola, et al., “The effectiveness of a peer-staffed crisis respite program as an alternative to hospitalization,” Psychiatric Services 69/10 (2018), pp. 1069–1074.
[41] P. R. Polak and M. W. Kirby, “A model to replace psychiatric hospitals,” Journal of Nervous and Mental Disorders 162/1 (1976), pp. 13–22; Bennett (see note 33); R. Bellion, “How we invented the Soteria principle,” in P. Stastny and P. Lehmann (eds), Alternatives beyond psychiatry (Berlin: Peter Lehmann Publishing, 2007); K. Lötscher, H. H. Stassen, et al. “[Community-based crisis home programme: Cost-efficient alternative to psychiatric hospitalization],” Nervenarzt 80/7 (2009), pp. 818–826 [in German].
[42] M. Heyland, C. Emery, and M. Shatell, “The Living Room, a community crisis respite program offering people in crisis an alternative to emergency departments,” Global Journal of Community Psychology Practice 4/3 (2013), pp. 1–10.
[43] E. F. Torrey, “Continuous treatment teams in the care of the chronic mentally ill,” Hospital and Community Psychiatry 37/12 (1986), pp. 1243–1247.
[44] New York Association of Psychiatric Rehabilitation Services, Peer Bridger project. Available at https://www.nyaprs.org/peer-bridger.
[45] D. Herman, L. Opler, A. Felix, et al., “A critical time intervention with mentally ill homeless men: Impact on psychiatric symptoms,” Journal of Nervous and Mental Disorders 188/3 (2000) pp. 135–140.
[46] N. Hunter, Trauma and madness in mental health services (London: Palgrave and MacMillan, 2018), pp. 201–219.
[47] C. Wusinich, D. Lindy, D. Russell, et al., “Experiences of Parachute NYC: An integration of Open Dialogue and Intentional Peer Support,” Community Mental Health Journal (2020).
[49] Ibid.; M. Chinman, P. George, R. H. Dougherty, et al., “Peer support services for individuals with serious mental illnesses: Assessing the evidence,” Psychiatric Services 65/4 (2014), pp. 429–441.
[51] R. M. Krausz, G. R. Werker, V. Strehlau, and K. Jang, “Applying addictions harm reduction lessons to mental healthcare,” Advances in Dual Diagnosis 7/2 (2014), pp. 73–79.
[52] D. Ougrin, T. Tranah, D. Stahl et al., “Therapeutic interventions for suicide attempts and self-harm in adolescents: Systematic review and meta-analysis,” Journal of the American Academy of Child and Adolescent Psychiatry 54/2 (2015), pp. 97–107; K. James, I. Samuels, P. Moran, and D. Stewart, “Harm reduction as a strategy for supporting people who self-harm on mental health wards: The views and experiences of practitioners,” Journal of Affective Disorders 214 (2017), pp. 67–73.
[53] Bellion (see note 41).
[54] Devandas (2019, see note 1), para. 50.
[55] M. I. Herz, W. M. Glazer, M. A. Mostert, et al., “Intermittent vs maintenance medication in schizophernia: Two-year results,” Archives of General Psychiatry 48/4 (1991), pp. 333–339; P. Stastny, “Taking charge of psychotropic drugs,” Disability Studies Quarterly 3/2 (1993).
[56] V. Aderhold and P. Stastny, “A guide to minimal use of neuroleptics,” Mad in America (October 2, 2016). Available at https://www.madinamerica.com/2016/10/a-guide-to-minimal-use-of-neuroleptics/.
[57] T. Van Putten, P. R. May, S. R. Marder, and L. A. Wittmann, “Subjective response to antipsychotic drugs,” Archives of General Psychiatry 38/2 (1981), pp. 187–190.
[58] K. T. Mueser, P. W. Corrigan, D. W. Hilton, et al., “Illness management and recovery: A review of the research,” Psychiatric Services 53/10 (2002), pp. 1272–1284; Herz et al. (see note 56); J. A. Baker, K. Lovell, and N. Harris, “A best-evidence synthesis review of the administration of psychotropic pro re nata (PRN) medication in in-patient mental health settings,” Journal of Clinical Nursing 17/9 (2008), pp. 1122–1231; Aderhold and Stastny (see note 56).
[59] Office of the United Nations High Commissioner for Human Rights, UN reports. Available at https://www.ohchr.org/EN/Issues/Disability/Pages/UNStudiesAndReports.aspx.
[60] M. Rotenberg, A. Tuck, and K. McKenzie, “Psychosocial stressors contributing to emergency psychiatric service utilization in a sample of ethno-culturally diverse clients with psychosis in Toronto,” BMC Psychiatry 17/234 (2017), pp. 1–7.
[61] T. Aubry, G. Nelson, and S. Tsemberis, “Housing First for people with severe mental illness who are homeless: A review of the research and findings from the At Home-Chez Soi Demonstration Project,” Canadian Journal of Psychiatry 60/11 (2015), pp. 467–474.
[62] Western Massachusetts Recovery Learning Community, RLC articles. Available at https://www.westernmassrlc.org/rlc-articles; C. Mills and B. Davar, “A local critique of global mental health,” in S. Grech and K. Soldatic (eds), Disability in the Global South: The critical handbook (Cham: Springer, 2016), pp. 437–451.
[63] United Nations, Rights of persons with disabilities (New York: United Nations, August 2016), paras. 67–69; Devandas (2019, see note 1), paras. 73–75.
[64] World Health Organization, Quality Rights Initiative (2019). Available at https://www.who.int/mental_health/policy/quality_rights/en/.
[65] Mills (see note 17).
[66] D. Ingleby, “How ‘evidence-based’ is the movement for global mental health?,” Disability and the Global South 1/2 (2014), pp. 203–226.
[67] G. Contino, “The medicalization of health and shared responsibility,” New Bioethics 22/1 (2016), pp. 45–55.
[68] Mills (see note 17).
[69] Y. Khazaal, R. Manghi, M. Delahaye, et al., “Psychiatric advance directives, a possible way to overcome coercion and promote empowerment,” Frontiers in Public Health 2/37 (2014).
[70] S. Philip, S. K. Rangarajan, S. Moirangthem, et al., “Advance directives and nominated representatives: A critique,” Indian Journal of Psychiatry 61/Suppl. 4 (2019), pp. S680–S685.
[71] Patel et al. (see note 16); Mills (see note 17).
[72] Human Rights Watch, “Like a death sentence”: Abuses against persons with mental disabilities in Ghana (New York: Human Rights Watch, 2012).
[73] S. von Peter, V. Aderhold, L. Cubellis, et. al. “Open Dialogue as a human rights-aligned approach.” Frontiers in Psychiatry 10 (2019), article 387.