Understanding US Immigration Detention: Reaffirming Rights and Addressing Social-Structural Determinants of Health
Volume 22/1, June 2020, pp 187 – 198
Altaf Saadi, Maria-Elena De Trinidad Young, Caitlin Patler, Jeremias Leonel Estrada, and Homer Venters
Abstract
A crisis of mass immigration detention exists in the United States, which is home to the world’s largest immigration detention system. The immigration detention system is legally classified as civil, rather than criminal, and therefore non-punitive. Yet it mimics the criminal incarceration system and holds detained individuals in punitive, prison-like conditions. Within immigration detention centers, there are increasing reports and recognition of civil and human rights abuses, including preventable in-custody deaths. In this paper, we propose understanding the health impacts of detention as an accumulation of mental and physical trauma that take place during the entirety of a detained immigrant’s experience, from migration to potential deportation and removal. Further, we explore the social-structural determinants of health as they relate to immigration detention, contextualize these determinants within a human rights framework, and draw parallels to the larger context of US mass incarceration. Realizing the right to health requires addressing these social-structural determinants of health. For the care of immigrant patients to be effective, clinicians and public health professionals must incorporate an awareness of the health risks of the immigration detention system into trauma- and human rights-informed models of care during and after detention.
Background
Approximately 7% of the US population, or 22.8 million people, are non-citizens.[1] In 2017, nearly 260,000 people sought asylum, or protection from persecution, within the United States.[2] These immigrant populations experience unique risks to health, including pre-migratory trauma, unsafe and stressful migration experiences, and post-migration discrimination.[3] Human rights abuses can occur across this spectrum of the immigrant experience. Once in the United States, immigrants may experience fears of deportation or mistrust of health services, dissuading care-seeking behavior.[4] Health outcomes associated with increased immigration enforcement and fear of deportation include increased cardiovascular risk factors, lower birth weights, and worsened mental health.[5] In addition, these health behaviors and outcomes ripple throughout the communities to which immigrants belong.[6] Twenty million children living in the United States have at least one immigrant parent, and more than 16.7 million people have at least one undocumented family member living with them, among whom nearly 50% are US born or naturalized citizens.[7]
Medical and public health research and practice has increasingly addressed the negative health impacts of anti-immigrant policies.[8] However, the health impacts of immigration detention beyond preventable deaths have received comparatively little attention, even though immigration detention has become increasingly prevalent and increasingly in violation of human rights standards.[9] In 2018, the US government detained nearly 400,000 people in the 200 immigration jails across the country, with a total average daily population of 42,000.[10] In 2019, this reached a total daily population of 55,000, the largest in American history, reflecting a steady and steep rise in the immigration detention population over the past few years.[11] At least one in four Latino/as say they personally know someone who has been detained or deported for immigration reasons in the last 12 months.[12] Knowing a deported person is associated with adverse mental health outcomes, irrespective of one’s own legal status.[13]
For the care of immigrant patients to be effective and their right to health realized, clinicians and public health professionals need a working understanding of the immigration detention system and the various ways it may affect a person or family unit’s health and well-being. This article uses a framework based on the social-structural determinants of health to offer an orientation to the detention system and calls for incorporating this awareness into trauma- and human rights-informed models of care for immigrant patients. The social determinants of health, as defined by the World Health Organization, are “the conditions in which people are born, grow, work, live and age, and the wider set of forces and systems shaping the conditions of daily life.”[14] Underpinning this framework is recognition of health as a right for all individuals, irrespective of immigration status, alleged criminality, or detention, as laid down in international human rights treaties such as the International Covenant on Economic, Social and Cultural Rights and other human rights conventions specific to refugees, migrants, and asylum-seekers.[15]
Understanding the US immigration detention system
Federal immigration enforcement policy changes paved the way for an expansive rise in detention rates over the past several decades.[16] In 1973, the US government detained a daily average of 2,370 migrants; this number rose to 5,532 by 1994, surged to 34,000 by 2009, and as of 2019 had risen to a record 55,000.[17] These numbers are dramatically out of proportion to the rate of unauthorized immigration during these same time periods; for example, from 2007 to 2017, there was actually a drop in national estimates of unauthorized immigrants.[18]
Federal policies that were central to this expansion were the 1996 Antiterrorism and Effective Death Penalty Act and the Illegal Immigration and Immigrant Responsibility Act, which established minimum daily detention numbers and lowered the bar for deportable offenses; many crimes categorized as “aggravated felonies” in the immigration context are considered neither aggravated nor felonies in the criminal context.[19] Notably, both undocumented and legal permanent residents are subject to detention.
The immigration detention system, unlike criminal jails or prisons, operates under civil law. Consequently, many constitutional protections available under criminal law do not exist in the detention system. For example, immigrants can be detained indefinitely; there is no federal right to legal representation for detainees; and most immigrants are not entitled to government-appointment lawyers, greatly reducing their chances of winning their case.[20]
Yet detention conditions are often similar to those of prisons or jails.[21] Detained individuals are held in secured facilities, wear prison uniforms, and subjected to strict control of time and movement. Indeed, many local jails contract bed space to Immigration and Customs Enforcement (ICE), and for-profit, stand-alone immigration detention facilities use corporate prison models.[22]
Further, there is significant fragmentation of responsibility and accountability among the agencies managing the immigration detention system. The Office of Refugee Resettlement, housed in the Department of Health and Human Services, oversees the detention of children and unaccompanied children, whereas Customs and Border Protection (CBP) and ICE, within the Department of Homeland Security, administer adult detention. The structure and quality of health services in detention settings is similarly fragmented. Approximately 25% of detainees receive care from the ICE Health Service Corps (staff detailed from US Public Health Service), while others are cared for by direct employees of for-profit health staffing vendors. The policies and procedures that govern health care in ICE and CBP detention settings—the ICE Performance Based National Detention Standards and the CBP National Standards on Transport, Escort, Detention, and Search—are unevenly applied across the various detention settings, and quality assurance is often subcontracted to for-profit vendors. For health professionals working in detention centers, law enforcement security may dictate the scope of care, unlike hospitals and ambulatory settings, where medical experts inform those decisions.[23] Analyses of documented preventable deaths reveal gross deficiencies in access to care, quality of care, and transparency in death review.[24] This fragmented system of care operates without clear or transparent oversight, falling short of both human rights and other legal standards.[25]
Human rights and the social-structural determinants of health in the US immigration detention system
The social determinants of health in immigration detention include direct physical and mental health outcomes from neglect, abuse, poor conditions of confinement, and challenges to economic stability and social networks—adverse effects that continue long after detention ends and that reach beyond the individual. Experiences of discrimination, racialization, and criminalization are structural determinants of health that further shape immigrant patients and exacerbate health inequities. Realizing the human rights and inherent dignity of migrants, including their right to health, requires addressing these social-structural determinants of health.[26]
Multiple forms of abuse
Recent reports indicate that physical abuse and sexual assault in detention centers are frequently ignored. For example, the Department of Homeland Security received 33,126 complaints of sexual and physical abuse from January 2010 to July 2016 but investigated only 570.[27] Rape and sexual assault are often underreported in immigration detention due to fears of retaliation, social isolation, language barriers, and knowledge that allegations are not seriously investigated.[28] Many detention facilities use solitary confinement as punishment or to monitor individuals who experienced victimization or are mentally ill, despite its detrimental impact on physical and psychological well-being.[29] Because some security personnel and private prison officials are responsible for developing and managing health services, there is often a punitive instead of therapeutic approach to mental health care.[30]
Conditions of confinement
Detention center medical systems have limited health care services, are frequently under-staffed, and are focused on managing acute care needs rather than chronic medical problems, resulting in medical neglect, delayed diagnoses and care, and severe negative consequences, especially among trauma-exposed individuals.[31] As the daily population of detained adults and children has increased, overcrowding has become a risk to the health of detained individuals. Epidemiologic investigations by local and state health departments and the Centers for Disease Control and Prevention have documented outbreaks of mumps and measles, pneumonia, influenza, and other respiratory disease in several detention facilities.[32] Other conditions of confinement that affect health include facility practices such as continuous lighting and sleep deprivation, lack of privacy, sanitation deficiencies, restricted recreation time, dirty or inadequate clothing (particularly for weather changes), inadequate meals, deprivation of autonomy and security, and verbal harassment and physical mistreatment by detention officers.[33] In one review of more than 7,000 asylum cases, one-third of detained asylum-seekers reported poor conditions, treatment, or medical issues. Among them, 61.8% reported issues related to food and water, 34.5% reported issues related to hygiene, and 45.6% reported issues related to the inability to sleep, overcrowded conditions, confinement, and the temperature being too cold.[34]
Economic and social stressors
Immigration detention compounds preexisting social determinants of health, such as language barriers, economic inequalities, and disrupted social networks. For example, lost wages, steep prices for phone calls, having to purchase necessary items from commissary (such as toiletries), legal fees, and exorbitant bond prices all exacerbate the economic burden on immigrants and their families, who may already be from low socioeconomic backgrounds.[35] The absence of appropriate interpretation services to meet the diverse language needs of immigrants in detention centers also contributes to poor and devastating health outcomes, as does the disruption of social networks and social ties due to distance from immigration detention centers and separation from family and support systems in the United States and native countries.[36] Legal noncitizen residents—who are the most likely to have work and family ties—are likely to be detained longer than other noncitizens and may therefore be especially vulnerable.[37] Undocumented family members lack additional freedoms of mobility relative to other immigrants. Due to fears of “entering the belly of the beast,” many undocumented immigrants do not visit detained family members, weakening family and social cohesion.[38] Lastly, the social determinants of health are compounded by the legal context of immigration detention centers—for example, the absence of a lawyer and the reality of indefinite detention with lengthy backlogs and unclear timelines—adding uncertainty to the immigration detention process, which itself is associated with anticipatory stress detrimental to health.[39]
Racialization and criminalization
These social determinants of health are reinforced by structural determinants of health—conditions further “upstream”—such as systemic racism. In the immigration detention context, racism and the dual racialization-criminalization of immigrants are particularly poignant forces. Male Latino immigrants have been especially subjected to criminal stereotypes and scapegoating; nearly 90% of detained individuals are men, and more than 97% are Latin American or Caribbean.[40]
Black immigrants are also disproportionately affected due to the immigration enforcement system’s reliance on police and courts to funnel immigrants who have committed crimes into immigration detention.[41] Racial discrimination in law enforcement and criminal sentencing leads Black immigrants to be more likely than any other population to interact with law enforcement and to be arrested, convicted, and imprisoned.[42] As a result, although only 7% of non-citizens in the United States are Black, they make up 20% of those facing deportation on criminal grounds.[43] Further, Black immigrants are more likely than other immigrants to be detained for criminal convictions and to be deported due to a criminal conviction.[44]
Like police officers in criminal law enforcement, immigration enforcement agents may also use racial profiling as an enforcement strategy. This can lead to the arrest and detention of US citizen Latino/as in addition to those who are undocumented, serving as a significant psychosocial stressor with consequent health impacts among both immigrants and citizen communities of color perceived to be immigrants.[45]
Immigration intercept model: A conceptual framework
Given the impact of immigration detention on the health outcomes of detainees, their families, and communities, health care professionals outside the immigration detention system must be prepared to approach patients’ history of immigration detention as an important health risk factor.[46] Further, the health impacts of detention must be understood as embedded within the accumulation of mental and physical trauma that take place over the spectrum of the immigration experience, often in violation of human rights standards. The range of experiences prior to and following detention include adjusting to life as an immigrant in US communities, coping with preexisting trauma, dealing with the pain of family separation immediately following apprehension, and adapting to new social and economic circumstances after detention. Understanding these factors allows health care professionals to intervene at different stages of an immigrant person’s or family’s immigration journey. We propose the Immigration Intercept Model (Figure 1), adapted from the Justice Intercept Model used to identify community interventions for individuals with substance use and mental health disorders as they move through the criminal justice system.[47]
Figure 1. Immigration Intercept Model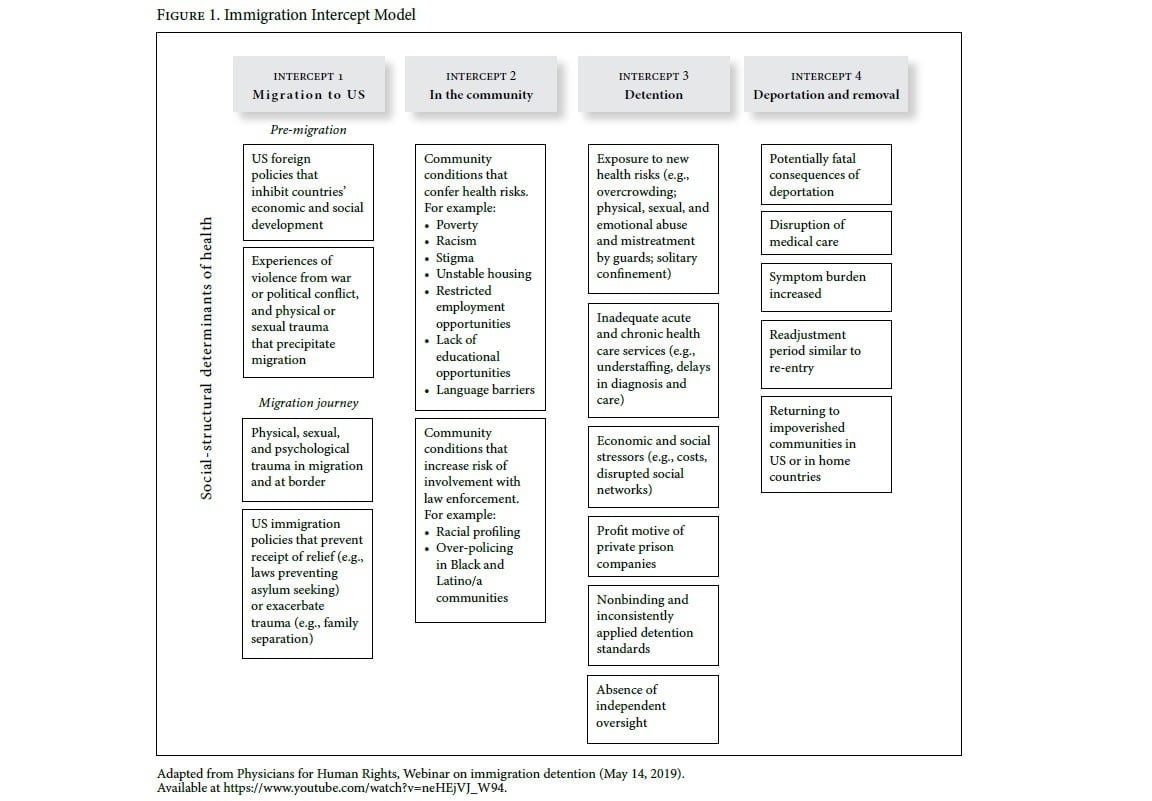
Adapted from Physicians for Human Rights, Webinar on immigration detention (May 14, 2019). Click on image for full size view.
The Immigration Intercept Model identifies points, or intercepts, at which social-structural determinants of health play a role and where health care professionals could advocate for interventions. Some immigrants (such as asylum-seekers) are immediately detained after crossing the border and do not experience life in the United States; some experience deportation or removal while others do not. As a result, it is critical to consider these intercepts and how a social-structural determinants of health framework, based in human rights, intersects with each intercept.
Pre-detention factors include (1) experiences of trauma in one’s home country that precipitated the migration (such as domestic violence, gang violence, poverty, and war); (2) experiences during the migration journey (such as physical trauma, sexual trauma, and trafficking), which can be compounded by dehydration or malnutrition; and (3) community conditions such as poverty, racism, housing instability, and employee exploitation that confer independent health risks.[48] These experiences vary depending on an individual’s legal status—a structural and racialized determinant of health in itself, with a host of collateral consequences such as restricted employment prospects, housing instability, and stigma.[49]
After detention, immigrants may be released due to receiving an immigration benefit, being released on bond, or being deported. The end of detention, however, does not terminate an individual’s contact with negative aspects of the immigration system. Many formerly detained immigrants experience a readjustment period similar to re-entry following incarceration.[50] They also disproportionately return to impoverished communities of color in the United States or economically struggling communities in their home countries, further exacerbating existing health inequities. Whether released into a US community or deported, they may experience a disruption of medical care as they attempt to connect to health care professionals to address new or chronic medical issues. The consequences of deportation can be fatal, especially when individuals are removed to countries without adequate health systems or where they are at risk of persecution.[51]
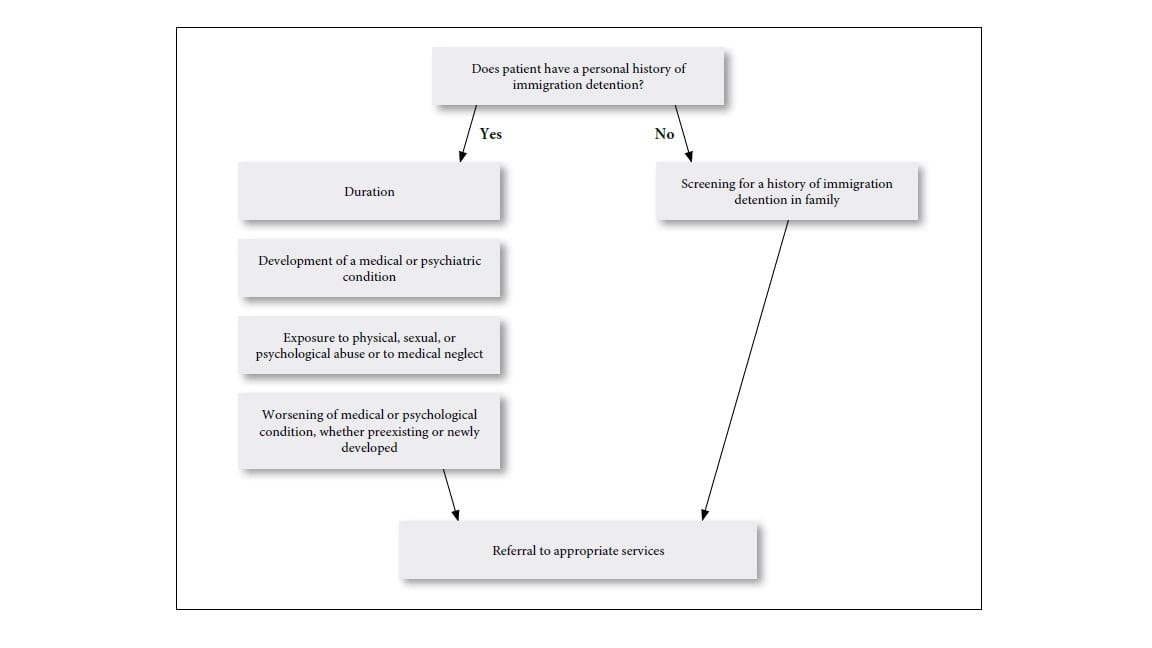
From a clinical perspective, heeding the Immigration Intercept Model might mean screening for a history of immigration detention as one of the factors that compounds health risks and leads to trauma accumulation among immigrant patients. Follow-up questions should center on the patient’s duration in immigration detention, whether they developed a medical or psychological condition while in detention, and whether a condition worsened while in detention (Figure 2). Clinicians can use communication strategies similar to those described above to obtain incarceration history. For example, health care professionals can implement a structural vulnerability “checklist” to engage all immigrant patients equally, or they can directly screen by asking questions that destigmatize and normalize detention experiences.[52] For example, they could say, “A lot of my immigrant patients and their family members have experienced detention in immigration detention centers in the past, and this can affect how healthy people and their families are. Has this ever happened to you or to a loved one?”[53] Given the psychological and financial toll that immigration detention can have on the entire family unit, screening for a family member in detention is relevant. At the same time, health care professionals should take care to ask these questions in a manner that reduces, rather than amplifies, fears, trauma, and stigma; similarly, they should avoid documenting their patients’ immigration status in medical records.[54] Health care professionals can then refer patients to legal or other health services as appropriate. Notably, clinicians should also consider detained immigrants’ resilience and agency as potential protective factors for health.
Figure 2. Components of health care screening for immigration detention (click on image for full size view)
 Call to action and future directions
Call to action and future directions
The immigration detention system has a significant negative impact on immigrant patient and community well-being. Health care professionals have a critical role to play in addressing the health impacts of detention—both by ensuring that issues related to detention are explicitly incorporated into immigrant health and human rights efforts and by developing new strategies to address the social-structural determinants of health in detention in order to better promote health.
A human rights-based approach emphasizes the meaningful participation of individuals and communities in decisions that directly affect them. Thus, health care professionals’ efforts must be centered on the experiences and perspectives of people who are directly affected by the detention system despite the challenges inherent in engaging with this vulnerable group. Detained individuals have limited rights and are at risk of retaliation for engaging in activism or advocacy efforts. Similarly, those released on bond face the continued burden of fighting their deportation case, while those who are deported—although no longer legally vulnerable in the United States—may face stigma and violence in their native countries.
The Immigration Intercept Model provides a framework for identifying points at which health care professionals can address health and detention. Many clinical and public health efforts already exist at these points—trauma-informed care models offer ways to elicit information about pre-migratory, migratory, and post-migratory trauma in a clinical encounter, and clinicians broach stressors and discrimination faced by immigrants while living in communities. But the impact of detention should be explicitly incorporated into these efforts to care for immigrant patients, with clinicians aware of, and comfortable addressing, the possibility of patients having experienced detention. Additional recommendations tailored to the detention context may be an area of future focus.
Finally, because this is an emerging area at the confluence of immigrant health, human rights, and public policy, it is critical to develop new partnerships and approaches. Legal and human rights groups are key stakeholders that provide individual support to those who are detained and that conduct monitoring of detention centers. Given the challenges of entry into detention centers, health care professionals should collaborate with legal experts who have developed relationships with detained individuals. Further, states such as California have taken steps to conduct evidence-based oversight of ICE detention, and these efforts should be widely expanded until alternatives to detention and more structured oversight are developed at the federal level.[55] These practices are crucial in the current political context, in which immigration laws are becoming increasingly punitive, indefinite detention is ever more commonplace, and human rights standards are not prioritized.
Acknowledgments
Caitlin Patler acknowledges support of the University of California–Mexico Program and the Russell Sage Foundation (award no. 93-16-15; any opinions expressed are those of the authors alone and should not be construed as representing the opinions of the Russell Sage Foundation). Maria-Elena De Trinidad Young acknowledges support from the National Institute on Minority Health and Health Disparities (grant no. R01MD012292-02). Altaf Saadi acknowledges support from the National Clinician Scholars Program at the University of California, Los Angeles.
Addendum
In this paper, we proposed a call to action to incorporate awareness of the health risks of immigration detention into trauma- and human rights-informed models of care. Harmful conditions and inadequate health care provision within detention facilities have taken on new urgency in the COVID-19 pandemic, representing significant risks to both detained people and the rest of US society by driving the national epidemic curve upward.
COVID-19, like other infectious disease outbreaks before it, enters detention settings where disease mitigation efforts are minimal or nonexistent: crowded and close quarters make social distancing enormously challenging, unsanitary conditions often include a lack of access to hygienic hand washing, and inadequate health services are all well documented by medical professionals and human rights organizations.[56] The introduction and spread of COVID-19 in detention facilities is facilitated by staff who come and go each day across two or three shifts. Once inside a facility, the virus cannot be contained and can then easily spread outside to surrounding communities. The reality of immigration detention centers makes them a ticking time bomb for the spread of COVID-19, which will result in preventable illness and death among detained immigrants, staff, and wider communities.
We have already seen the harm of COVID-19 in other carceral settings: in just a two-week span, the New York City jail system went from two confirmed cases to more than 500.[57] We can expect to see this trajectory replicated throughout the US immigration detention system.
In maintaining this civil detention system, the US immigration enforcement system is not only exposing thousands of detained people to heightened risk of serious illness and death but also doing the same for the staff who work in these settings—all the while wasting precious health care resources. Indeed, as hospital workers and paramedics face severe shortages of personal protective equipment to care for patients, ICE has requested thousands of N95 masks to continue apprehensions in the community.[58] The primary response in these circumstances must be release, especially given the complete lack of a public safety rationale for continuing to hold most people currently in immigration custody. ICE and other immigration enforcement agencies can contribute to nationwide mitigation measures by releasing detained people, with a special focus on those who possess risk factors for serious illness and death from COVID-19 infection. ICE officials report having released more than 160 people already as part of such efforts.[59] A perspective based on the social determinants of health helps us understand the social factors that contribute to the spread of viral diseases such as COVID-19. A human rights perspective compels us to respect the human dignity of each individual detained while upholding international standards and the values of equality, transparency, and humanity.
Altaf Saadi, MD, MS, is a neurologist at Massachusetts General Hospital and Instructor of Neurology at Harvard Medical School, Boston, USA.
Maria-Elena De Trinidad Young, PhD, MPH, is Assistant Professor at the Department of Public Health, School of Social Sciences, Humanities and Arts, University of California, Merced, USA.
Caitlin Patler, PhD, is Assistant Professor at the Department of Sociology, University of California, Davis, USA.
Jeremias Leonel Estrada is a community stakeholder in Ciudad Hidalgo, Mexico.
Homer Venters, MD, is Clinical Associate Professor at the College of Global Public Health, New York University, USA, and President of Community Oriented Correctional Health Services, New York, USA.
Please address correspondence to Altaf Saadi. Email: asaadi@mgh.harvard.edu.
Competing interests: None declared.
Copyright © 2020 Saadi, Young, Patler, Estrada, and Venters. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1] Kaiser Family Foundation, Population distribution by citizenship status (November 2018). Available at https://www.kff.org/other/state-indicator/distribution-by-citizenship-status/.
[2] Department of Homeland Security Office of Immigration Statistics, Annual Flow Report Refugees and Asylees: 2017 (March 2019), p. 11.
[3] H. Castañeda, S. M. Holmes, D. S. Madrigal, et al., “Immigration as a social determinant of health,” Annual Review of Public Health 36/1 (2015), pp. 375–392.
[4] K. M. Perreira and J. M. Pedroza, “Policies of exclusion: Implications for the health of immigrants and their children,” Annual Review of Public Health 40/1 (2019), pp. 147–166.
[5] Ibid.
[6] L. E. Gulbas, L. H. Zayas, H. Yoon, et al., “Deportation experiences and depression among U.S. citizen-children with undocumented Mexican parents,” Child Care Health Development 42/2 (2016), pp. 220–230; R. B. Toomey, A. J. Umaña-Taylor, D. R. Williams, et al., “Impact of Arizona’s SB 1070 immigration law on utilization of health care and public assistance among mexican-origin adolescent mothers and their mother figures,” American Journal of Public Health 104/Suppl 1 (2014), pp. S28–S34.
[7] R. Warren and D. Kerwin, “Mass deportations would impoverish US families and create immense social costs,” Journal on Migration and Human Security 5/1 (2017), pp. 1–8.
[8] Perreira and Pedroza (see note 4).
[9] Physicians for Human Rights and Bellevue/NYU Program for Survivors of Torture, From persecution to prison: The health consequences of detention for asylum seekers (Boston: Physicians for Human Rights ; Bellevue/NYU Program for Survivors of Torture, 2003); Human Rights Watch, American Civil Liberties Union, National Immigrant Justice Center, and Detention Watch Network (eds), Code red: The fatal consequences of dangerously substandard medical care in immigration detention (New York: Human Rights Watch, 2018).
[10] US Immigration and Customs Enforcement, Fiscal year 2018 ICE enforcement and removal operations report. Available at https://www.ice.gov/doclib/about/offices/ero/pdf/eroFY2018Report.pdf.
[11] I. Dias, “ICE is detaining more people than ever—and for longer,” Pacific Standard Magazine (August 1, 2019). Available at https://psmag.com/news/ice-is-detaining-more-people-than-ever-and-for-longer.
[12] M. H. Lopez, A. Gonzalez-Barrera, and J. M. Krogstad, “Hispanics and their views of immigration reform,” Pew Research Center’s Hispanic Trends Project (October 2014). Available at https://www.pewresearch.org/hispanic/2014/10/29/chapter-5-hispanics-and-their-views-of-immigration-reform.
[13] E. D. Vargas, M. Juárez, G. R. Sánchez, and M. Livaudais, “Latinos’ connections to immigrants: How knowing a deportee impacts Latino health,” Journal of Ethnic and Migration Studies 45/15 (2019), pp. 2971–2988.
[14] A. R. Chapman, “The social determinants of health, health equity, and human rights,” Health and Human Rights Journal 12/2 (2010), pp. 17–30.
[15] Ibid; E. Acer and J. Goodman, “Reaffirming rights: Human rights protections of migrants, asylum seekers, and refugees in immigration detention,” Georgetown Immigration Law Journal 24 (2010), pp. 507–531.
[16] P. Macías-Rojas, From deportation to prison: The politics of immigration enforcement in post-civil rights America (New York: New York University Press, 2016).
[17] Dias (see note 11); C. Patler and T. M. Golash‐Boza, “The fiscal and human costs of immigrant detention and deportation in the United States,” Sociology Compass 11/3 (2017), p. e12536.
[18] J. M. Krogstad, J. S. Passel, and D. Cohn, “5 facts about illegal immigration in the U.S.,” Pew Research Center (June 12, 2019). Available at https://www.pewresearch.org/fact-tank/2019/06/12/5-facts-about-illegal-immigration-in-the-u-s.
[19] Macías-Rojas (see note 16).
[20] I. V. Eagly and S. Shafer, “A national study of access to counsel in immigration court,” University of Pennsylvania Law Review 164/1 (2015), pp. 1–91.
[21] J. Longazel, J. Berman, and B. Fleury-Steiner, “The pains of immigrant imprisonment: Pains of immigrant imprisonment,” Sociology Compass 10/11 (2016), pp. 989–998.
[22] L. Luan, “Profiting from enforcement: The role of private prisons in U.S. immigration detention,” Migration Policy Institute (May 2, 2018). Available at https://www.migrationpolicy.org/article/profiting-enforcement-role-private-prisons-us-immigration-detention.
[23] P. Spiegel, N. Kass, and L. Rubenstein, “Can physicians work in US immigration detention facilities while upholding their Hippocratic oath?” JAMA (August 2019).
[24] Human Rights Watch et al. (see note 9).
[25] Ibid.
[26] Chapman (see note 14).
[27] R. Merton and C. Fialho, Sexual abuse, assault, and harassment in U.S. immigration detention (April 2017). Available at http://www.endisolation.org/wp-content/uploads/2017/05/CIVIC_SexualAssault_Complaint.pdf.
[28] Ibid.
[29] C. Patler, J. O. Sacha, and N. Branic, “The black box within a black box: Solitary confinement practices in a subset of U.S. immigrant detention facilities,” Journal of Population Research 35/4 (2018), pp. 435–465.
[30] A. J. Fischer, P. Gonzalez, and R. Diaz, There is no safety here: The dangers for people with mental illness and other disabilities in immigration detention at GEO Group’s Adelanto ICE Processing Center (Disability Rights California, 2019). Available at https://www.disabilityrightsca.org/system/files/file-attachments/DRC_REPORT_ADELANTO-IMMIG_DETENTION_MARCH2019.pdf; Office of Inspector General, Concerns about ICE detainee treatment and care at detention facilities (2017). Available at https://www.oig.dhs.gov/sites/default/files/assets/2017-12/OIG-18-32-Dec17.pdf.
[31] Physicians for Human Rights and Bellevue/NYU Program for Survivors of Torture (see note 9); H. D. Venters and A. S. Keller, “The immigration detention health plan: An acute care model for a chronic care population,” Journal of Health Care for the Poor and Underserved 20/4 (2009), pp. 951–957.
[32] J. Leung, “Notes from the field: Mumps in detention facilities that house detained migrants—United States, September 2018–August 2019,” Morbidity and Mortality Weekly Report 68 (2019); H. Venkat, “Notes from the field: Measles outbreak at a United States Immigration and Customs Enforcement facility―Arizona, May–June 2016,” Morbidity and Mortality Weekly Report 66 (2017); E. N. Nyangoma, C. S. Arriola, J. Hagan, et al., “Notes from the field: Hospitalizations for respiratory disease among unaccompanied children from Central America—Multiple States, June–July 2014,” Morbidity and Mortality Weekly Report 63 (2014).
[33] Fischer et al. (see note 30); T. K. Wong, S. Bonilla, and A. Colemana, Seeking asylum: Part 1 (La Jolla, CA: U.S. Immigration Policy Center at University of California San Diego, 2019). Available at http://usipc.ucsd.edu/publications/usipc-seeking-asylum-part-1-final.pdf.
[34] Wong et al. (see note 33).
[35] D. Gilman and L. A. Romero, “Immigration Detention, Inc.,” Journal on Migration and Human Security (May 2018); C. Patler, The economic impacts of long-term immigration detention in Southern California (September 2015). Available at https://escholarship.org/uc/item/23h0r12q.
[36] T. Jawetz and S. Shuchart, “Language access has life-or-death consequences for migrants,” Center for American Progress. Available at https://www.americanprogress.org/issues/immigration/reports/2019/02/20/466144/language-access-life-death-consequences-migrants.
[37] Transactional Records Access Clearinghouse Immigration, Legal noncitizens receive longest ICE detention (June 3, 2013). Available at https://trac.syr.edu/immigration/reports/321/#f1.
[38] C. Patler and N. Branic, “Patterns of family visitation during immigration detention,” RSF: The Russell Sage Foundation Journal of the Social Sciences 3/4 (2017), pp. 18–36.
[39] I. Hasselberg, Enduring uncertainty: Deportation, punishment and everyday life (New York: Berghahn Books, 2017); L. I. Pearlin and A. Bierman, “Current issues and future directions in research into the stress process,” in C. S. Aneshensel, J. C. Phelan, and A. Bierman (eds), Handbook of the sociology of mental health (Dordrecht: Springer Netherlands, 2013).
[40] T. Golash-Boza and P. Hondagneu-Sotelo, “Latino immigrant men and the deportation crisis: A gendered racial removal program,” Latino Studies 11 (2013).
[41] A. Armenta, Protect, serve, and deport: The rise of policing as immigration enforcement, 1st ed. (University of California Press, 2017).
[42] The Sentencing Project, Report to the United Nations on racial disparities in the U.S. criminal justice system (2018). Available at https://www.sentencingproject.org/publications/un-report-on-racial-disparities/.
[43] J. Morgan-Trostle, K. Zheng, and C. Lipscombe, The state of black immigrants, part II: Black immigrants in the mass criminaliztion system (Black Alliance for Just Immigration and NYU Law Immigrant Rights Clinic, 2018). Available at https://www.sccgov.org/sites/oir/Documents/sobi-deprt-blk-immig-crim-sys.pdf.
[44] Ibid.
[45] P. St. John and J. Rubin, “ICE held an American man in custody for 1,273 days. He’s not the only one who had to prove his citizenship,” Los Angeles Times (September 17, 2018). Available at https://www.latimes.com/local/lanow/la-me-citizens-ice-20180427-htmlstory.html; S. Sabo, S. Shaw, M. Ingram, et al., “Everyday violence, structural racism and mistreatment at the US-Mexico border,” Social Science and Medicine 109 (2014), pp. 66–74.
[46] S. P. Kulkarni, S. Baldwin, A. S. Lightstone et al., “Is incarceration a contributor to health disparities? Access to care of formerly incarcerated adults,” Journal of Community Health 35/3 (2010), pp. 268–274.
[47] M. R. Munetz and P. A. Griffin, “Use of the Sequential Intercept Model as an approach to decriminalization of people with serious mental illness,” Psychiatric Services 57/4 (2006), pp. 544–549.
[48] H. Castañeda, S. M. Holmes, D. S. Madrigal, et al., “Immigration as a social determinant of health,” Annual Review of Public Health 36/1 (2015), pp. 375–392; S. M. Holmes, “‘Is it worth risking your life?’ Ethnography, risk and death on the U.S.-Mexico border,” Social Science and Medicine 99 (2013), pp. 153–161; O. Martinez, The beast: Riding the rails and dodging narcos on the migrant trail (London: Verso, 2013).
[49] A. L. Asad and M. Clair, “Racialized legal status as a social determinant of health,” Social Science and Medicine 199 (2018), pp. 19–28.
[50] C. Patler, “Blurring the borders of stigma: Socioeconomic reintegration among noncitizens following imprisonment” (presentation at UC Davis Hemispheric Institute on the Americas, University of California, Davis, 2018).
[51] S. Romero and V. J. Blue, “A Mexican man’s fatal journey to reclaim his American life,” New York Times (October 14, 2018). Available at https://www.nytimes.com/2018/10/14/us/immigrant-death-crossing-border-smuggler.html.
[52] K. Sue K, “How to talk with patients about incarceration and health,” AMA Journal of Ethics 19/9 (2017), pp. 885–893.
[53] Ibid.
[54] G. Kim, U. S. Molina, and A. Saadi, “Should immigration status information be included in a patient’s health record?” AMA Journal of Ethics 21/1 (2019), pp. 8–16; M. G. Kuczewski, J. Mejias-Beck, and A. Blair, “Good sanctuary doctoring for undocumented patients,” AMA Journal of Ethics 1/21 (2019), pp. E78–E85.
[55] California Department of Justice, Immigration detention in California (2019). Available at https://oag.ca.gov/sites/all/files/agweb/pdfs/publications/immigration-detention-2019.pdf.
[56] J. Leung, “Notes from the field: Mumps in detention facilities that house detained migrants—United States, September 2018–August 2019,” Morbidity and Mortality Weekly Report 68 (2019); H. Venkat, “Notes from the field: Measles outbreak at a United States Immigration and Customs Enforcement facility―Arizona, May–June 2016,” Morbidity and Mortality Weekly Report 66 (2017); E. N. Nyangoma, C. S. Arriola, J. Hagan, et al., “Notes from the field: Hospitalizations for respiratory disease among unaccompanied children from Central America—Multiple States, June–July 2014,” Morbidity and Mortality Weekly Report 63 (2014).
[57] Board of Correction Daily Covid-19 Update (April 3, 2020). Available at https://www1.nyc.gov/assets/boc/downloads/pdf/News/covid-19/Public_Reports/Board%20of%20Correction%20Daily%20Public%20Report_4_3_2020_TO%20PUBLISH.pdf.
[58] M. M. Lopez and S. M. Holmes, “ICE agents are still performing raids—and using precious N95 masks to do so,” Guardian (March 31, 2020). Available at https://www.theguardian.com/commentisfree/2020/mar/31/ice-raids-coronavirus-n95-masks.
[59] H. Aleazis, “Hundreds of immigrant detainees considered vulnerable to the coronavirus may be released,” Buzzfeed News (April 7, 2020). Available at https://www.buzzfeednews.com/article/hamedaleaziz/immigrant-detainees-coronavirus-risk-early-release.