The Universal Periodic Review: A Valuable New Procedure for the Right to Health?
Judith Bueno De Mesquita
Abstract
The right to health has been cast in increasingly broad terms in international human rights law, not only as a right to health care but also as a right to an ever more broad range of underlying and social determinants of health. Utilizing an analytical framework grounded in this broad view of the right to health, this article presents the findings of an empirical review of the right to health in the recommendations issued to states during the first two cycles of the Human Rights Council’s Universal Periodic Review. The Universal Periodic Review, a peer-review mechanism, has come to occupy a prominent position in global human rights oversight, not least because all United Nations member states are regularly scrutinized under the procedure. It has also been identified as a potentially valuable mechanism to enhance accountability around the Sustainable Development Goals. The article highlights that the right to health is prominent in the Universal Periodic Review’s recommendations, a conclusion that contrasts with existing perceptions that the right has been given limited attention by the procedure. However, the article argues that the quality of these recommendations is uneven. Increasing the engagement of key health stakeholders in the procedure will be important to enhance its potential for the right to health.
Introduction
Established in 2006, the Universal Periodic Review (UPR) is one of the most ambitious recent additions to the global human rights accountability architecture of the United Nations (UN).[1] A peer-review mechanism overseen by the UN’s Human Rights Council, the procedure involves a quinquennial review of the human rights record of every UN member state and culminates in recommendations issued to each state for improving its compliance with international human rights standards. Not only has the UPR come to assume a central role in global human rights oversight, but it has also been identified as having the potential to enhance state accountability around the Sustainable Development Goals (SDGs).[2]
Economic, social, and cultural (ESC) rights have become steadily more prominent in terms of the work of international human rights actors and mechanisms over the last 25 years. This is particularly true of the right to health, which has also increasingly been the focus of extensive scholarly, policy, and advocacy activity. By contrast, the right to health remains neglected by countries’ laws, policies, and institutions, a situation reinforcing the importance of global oversight. Pronouncing that the UPR would be underpinned by the principles of “universality, interdependence, indivisibility and interrelatedness of all human rights,” the Human Rights Council committed to balance its attention between ESC rights on the one hand and civil and political (CP) rights on the other.[3] Despite burgeoning academic and activist practice on the right to health, there has been limited attention to the UPR’s record on this human right, although there have been some largely critical reviews of the procedure’s record on ESC rights.[4]
This article is the first to provide an in-depth analysis of the UPR’s performance on the right to health. Drawing on a comprehensive empirical review of recommendations made to states during the UPR’s first and second cycles, I assess the mechanism’s performance in terms of the prominence of the right to health in UPR recommendations, as well as the quality of those recommendations. Highlighting that at least 22% of first-cycle and 25% of second-cycle recommendations addressed the right to health, I argue that the right to health is prominent in UPR recommendations. However, the quality of these recommendations is uneven: they do not consistently address the right to health situation on the ground, focusing on some right to health norms and obligations while neglecting others; moreover, they are often phrased in an unspecific way that provides insufficient guidance for implementation and subsequent reviews of progress. This calls into question whether the UPR is maximizing its potential to generate improvements, as well as whether it can meaningfully enhance SDG oversight for the right to health.
The article begins with an overview of the increasing prominence of the right to health before turning its attention to the UPR, analyzing the mechanism’s importance as a human rights review procedure and its potential to enhance SDG review. It also highlights existing critical research on the UPR’s ESC rights record, including health. It proceeds to focus on the research methods and findings with respect to the right to health in the UPR underpinning this article. The subsequent analysis investigates apparent disparities between these findings and previous analyses in terms of the prominence of the right to health. It asserts that previous studies reflect restrictive interpretations of the right to health as much as neglect of this human right in UPR recommendations. This discussion is framed with reference to the different theoretical approaches to interpreting human rights that contribute to, and help explain, these contrasting positions. Moving on, the article sets out a framework for assessing quality, based on usefulness to the state under review and measurability, which it uses as an analytical prism to assess right to health recommendations.[5] It also analyzes the reasons why recommendations often fall short on this front, pointing to the hitherto limited engagement of health stakeholders in the UPR process as a critical factor. Increasing these stakeholders’ engagement will be essential for catalyzing improvements, which are needed to support change on the ground and to better equip the UPR to support SDG review. At a practical level, this article’s findings, particularly on the prominence of the right to health in recommendations, should encourage key health stakeholders to enhance their engagement with the UPR, because one reason for their limited engagement to date is the perception that the UPR is not strongly relevant to health.[6]
The coming of age of the right to health in the UN system
Compared to the centuries-old codification of CP rights, health and other ESC rights have been recognized as legal and inalienable human rights for just over 60 years. The first international articulation of health as a fundamental human right came in the 1946 Constitution of the World Health Organization.[7] Since then, the right has been enshrined in core international human rights treaties, including the International Covenant on Economic, Social and Cultural Rights; key regional human rights treaties; and domestic constitutions, over two-thirds of which include provisions on health or health care.[8]
During the Cold War, UN oversight and implementation of health and other ESC rights was neglected compared to CP rights as a result of now-discredited, ideologically fueled assertions by Western states that ESC rights were aspirational goals and of secondary importance.[9] The end of the Cold War heralded a sea change in two ways: First, at a theoretical level, as expressed by states at the Word Conference on Human Rights, there was a new, at least ostensible, consensus that “all human rights are universal, indivisible and interdependent and interrelated. The international community must treat human rights globally in a fair and equal manner, on the same footing, and with the same emphasis.”[10] Second, at an institutional level, the international community created new mechanisms to bring international oversight of ESC rights in line with hitherto superior arrangements for CP rights, including the creation of the Committee on Economic, Social and Cultural Rights to oversee the International Covenant on Economic, Social and Cultural Rights, as well as the creation of the Special Rapporteur on the right to health.[11] Burgeoning jurisprudence on health, and rights-based guidelines, reports, and projects by civil society and international organizations, have, together with this formal UN machinery, enhanced clarity about the right to health, helped improved oversight, and supported the right to health’s operationalization in the work of public health organizations.[12]
These developments are lauded by some as a success story. John Harrington and Maria Stuttaford have declared that “the human right to health has moved to the center of political debate and social policy across the globe.”[13] Yet progress has remained partial. ESC rights remain legally precarious, generally maintaining a “second tier” status and a smaller body of jurisprudence in domestic and international human rights legal systems, and they face enduring challenges to their status as fundamental, justiciable human rights.[14] The ESC right that is the focus of this article—the right to health—is often neglected in policy making due to policy makers’ often limited awareness of it.[15] Equally problematic is the lack of a sophisticated understanding of public health and health systems among most human rights professionals. At a more profound level, the dominance of neoliberalism, which has been characterized by a rise of private providers in health care, poses both ideological and regulatory challenges for the right to health.[16] These circumstances make robust global review even more important—and the UPR, with its universal scope and influence, as well as its potential role in SDG review, is well located and equipped to play a role.
The UPR: Opportunities and challenges for human rights
The UPR is a peer-review mechanism operating under the auspices of the Human Rights Council. Its overriding objective is to “improve the human rights situation in all countries and address human rights violations wherever they occur.”[17] Established as part of a broader reform package to the UN’s Charter-based human rights procedures, the UPR has now undergone two full review cycles (2008–2012 and 2012–2016) and entered a third cycle in 2017. The procedure is intended to reinforce, not duplicate, the work of other international human rights mechanisms.[18]
The UPR has been described as “one of the most important innovations of the [Human Rights Council].”[19] The procedure offers some unique opportunities for the right to health. Three principal features—the first two being undoubtedly valuable and the third of more debatable merit—differentiate it from other international review mechanisms.
First, the UPR has a universal reach. In establishing the procedure, the General Assembly noted that the UPR would review the “fulfilment by each State of its human rights obligations and commitments in a manner which ensures universality of coverage and equal treatment with respect to all States.”[20] All UN member states were reviewed during the first two UPR cycles and almost all submitted their national reports for review on time. By contrast, international human rights treaties enjoy widespread, but not universal, ratification, and treaty bodies’ oversight extends only to states parties. Moreover, states’ periodic reports required under the treaties are often delayed or sometimes not submitted at all.[21] In other words, the UPR is valuable both in theory, because it applies to all states in a way that other human rights processes do not, and in practice, because all states take it seriously enough to subject themselves to review in a timely manner.
Second, the UPR’s review of each state extends to all rights, as it is based on comprehensive protections contained in the UN Charter, the Universal Declaration of Human Rights, international treaties ratified by the state in question, and voluntary commitments and pledges.[22] This inclusive approach again contrasts with reviews by other mechanisms, which focus on selected rights (for example, the Committee on Economic, Social and Cultural Rights), situations (for example, country Special Rapporteurs), or particular groups (for example, the Committee on the Rights of the Child). A further benefit of this approach is that it allows the procedure to consider rights on the ground in a joined-up way.
These two features mirror attributes of the SDGs, which also extend to all countries and encompass wide-ranging and mutually reinforcing issues. Indeed, the SDGs share profound connections with the human rights standards that are the subject of UPR scrutiny: over 90% of SDG targets can be linked to international human rights and labor standards, and, moreover, the SDGs are formally grounded in international human rights law.[23] Recognizing these synergies, the UPR has explicitly addressed the SDGs in some of its recommendations, with many more having implicit relevance. But more than this, it has also been suggested that the UPR can support the SDGs in other ways. For example, the Human Rights Council president has suggested that it could enhance accountability in the context of the formal international SDG review procedure overseen by the High-Level Political Forum on Sustainable Development by serving as a “comprehensive source of information,” and that countries could themselves use UPR outcomes when preparing their voluntary presentations for this forum.[24] This suggestion seems particularly salient in view of states’ neglect of human rights issues in their voluntary national reports submitted to date for review by the forum.[25]
A third defining feature is the state-to-state peer-review format of the procedure, which is intended to cultivate a spirit of cooperation.[26] This is markedly different from other UN human rights procedures, which are carried out by independent experts. Though the UPR is meant to be conducted in an objective, non-politicized manner, its composition inherently renders it more vulnerable to politicization than these other procedures.[27] Indeed, politics have been found to affect which states give recommendations to each other; the topic and framing of recommendations; and whether states accept recommendations: this interferes with the quality and credibility of the review.[28] However, the political dimension is also seen by some as an asset. A key tenet in international relations is that states tend to listen to one another. The influences of peer pressure and a desire to earn peer respect are two suggested forces driving engagement by states in the UPR.[29] States often take reporting more seriously under the UPR than by treaty bodies.[30] It has also been argued that UPR recommendations are more likely to give rise to follow-up, implementation, and change on the ground as a result of their being received from other states.[31]
The procedure’s review process, which is to be based on objective and reliable information and take into account the specificities of the state under review, draws on three main sources of information: (1) a national report submitted by the state under review; (2) a UN report compiled by the Office of the High Commissioner for Human Rights that provides a synthesis of information on the state under review, drawing on reviews by other UN human rights mechanisms and other official UN documents, including information submitted by UN agencies; and (3) a stakeholders’ report compiled by the Office of the High Commissioner for Human Rights that summarizes information provided predominantly by civil society organizations, national human rights institutions, and academics.[32] Following review, the state in question receives recommendations, which it can either “accept,” thus voluntarily committing to implement, or “note,” indicating no such commitment. Between cycles, states are expected to implement accepted recommendations. Implementation is formally assessed at the subsequent review of a state.
The UPR has been greeted by some as a success.[33] Others have given it a “cautious endorsement.”[34] However, it has not been free of criticism. In addition to concerns about politicization, other leading concerns center on the poor quality and uneven implementation of recommendations, as well as the limited engagement of valuable stakeholders. I return to these criticisms below in the context of the right to health.
However, it is important to flag upfront critiques of the UPR for neglecting ESC rights. Drawing on a comprehensive database of UPR recommendations maintained by the civil society organization UPR Info, the Center for Economic and Social Rights has reported that only 17% of recommendations made during the first cycle exclusively addressed ESC rights, compared to 37% on CP rights, leading it to conclude that ESC rights received much less attention than CP rights.[35] Similarly, the Special Rapporteur on extreme poverty and human rights has drawn on this database to raise concerns about “both the quantity and quality of ESC rights-related recommendations.”[36] The UPR Info database suggests that 2.4% of first-cycle and 3.6% of second-cycle recommendations included a focus on the right to health, ranking it 23rd out of 30 human rights issues addressed in the first cycle and 15th out of 30 in the second.[37]
By contrast, the United Nations Population Fund has found that 26.5% of first-cycle and 28.5% of second-cycle recommendations addressed sexual and reproductive health and rights and gender equality.[38] These recommendations span a range of rights, but the right to health is central to sexual and reproductive health, suggesting that it may be more prominent in recommendations than the UPR Info database suggests.
An empirical review of the right to health in the UPR: Methods and findings
Methods
Together with the World Health Organization and the Human Rights Centre Clinic at the University of Essex, I undertook empirical quantitative and qualitative research on all recommendations made to states during the UPR’s first two cycles, and in-depth case studies of recommendations received by eight countries. The research was, in the first instance, intended to support the World Health Organization in enhancing its engagement with the procedure in an informed way. The research was based on three questions: (1) How prominent was the right to health in the UPR’s recommendations? (2) What was the distribution of recommendations between different right to health issues? (3) What types of actions did recommendations require? This article is based on these findings, nine in-depth interviews with staff at UN agencies and civil society organizations, and a desk review of literature on the UPR.
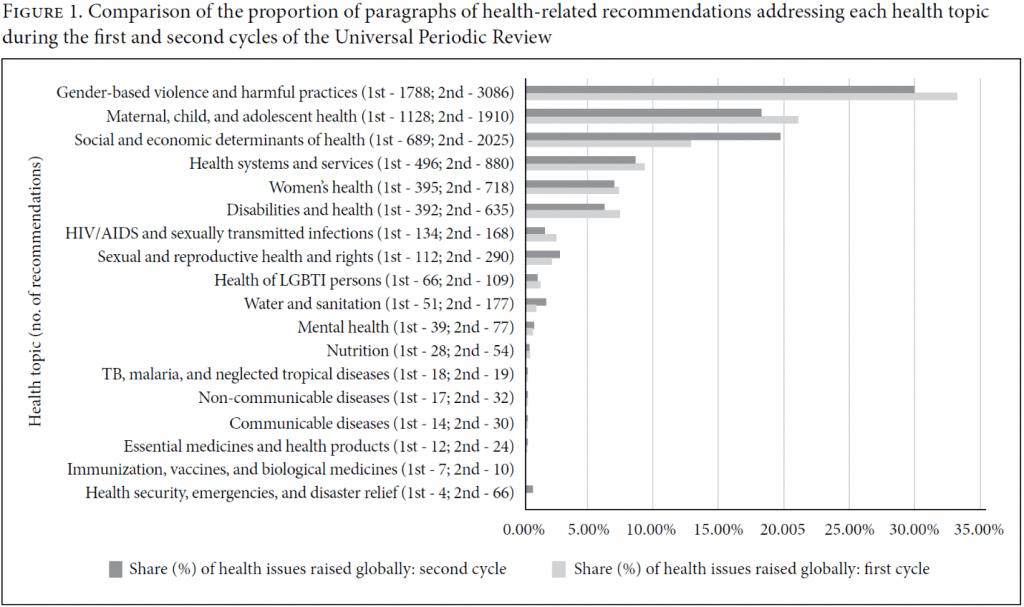
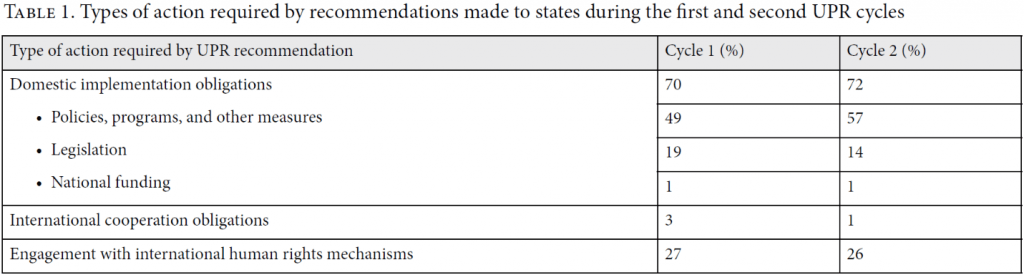
Before embarking on the empirical review, we carried out a detailed analysis of the parameters of the right to health under international human rights law, as set out in international human rights treaties, such as the International Covenant on Economic, Social and Cultural Rights, and general comments on the right to health adopted by treaty bodies.[39] Utilizing this framework, we coded recommendations as right to health recommendations if they specifically referred to the “right to health,” “health,” or other thematic issues that fall directly within the scope of the right to health, as interpreted by these actors (see Table 1). Some recommendations addressed issues that cut across a number of human rights, such as gender-based violence: thus, what we classify as a “right to health” recommendation may also embrace other human rights. We also coded right to health recommendations by theme, according to the specific issue they addressed (see Figure 1), and by action, in terms of the type of measure required (see Table 1). Since many right to health-related terms and formulations are used in UPR recommendations, we read and coded all recommendations manually rather than by using keyword searches.
The right to health is a broad right. Two further restrictions were applied to coding right to health recommendations. First, in recent years, the right to health has been interpreted by treaty bodies to include social determinants of health, which are the social and economic conditions in which people grow, live, work, and age, as well as economic and other inequalities.[40] Orielle Solar and Alec Irwin have identified different layers of determinants, notably intermediary determinants that directly affect health outcomes, such as material conditions, the health system, biological factors, behaviors, and psychosocial circumstances; and structural determinants that operate through these intermediary determinants to affect health, such as status considerations and inequalities.[41] Recommendations that referred to an intermediary determinant addressed by treaty bodies were automatically coded as right to health recommendations; by contrast, structural determinant recommendations were coded as such only if they also mentioned the right to health or a proxy or intermediary determinant term. This position is broadly reflective of the approach of treaty bodies.[42] Second, in order to align our research more closely with the operational priorities of the World Health Organization, for whom the empirical research was originally carried out, we excluded a small number of intermediary determinants of health, notably torture and adequate housing, unless reference was also explicitly made to health. This may result in our findings underestimating the number of UPR right to health recommendations.
Findings
In relation to question 1, during the first cycle, at least 22% (3,862/17,638) of recommendations were right to health recommendations. This increased to at least 25% (8,356/33,956) in the second cycle. The right to health was thus a prominent issue. Both the proportion and absolute numbers of right to health recommendations increased between the cycles.
In relation to question 2, gender-based violence (33% of first-cycle recommendations; 30% of second-cycle recommendations) and maternal, child, and adolescent health (21%; 19%) were the right to health issues most frequently raised, followed by social and economic determinants of health (13%; 20%) and health systems and services (9%; 9%). There were very few recommendations on issues such as HIV/AIDS (2%; 2%), water and sanitation (1%; 2%), mental health (1%; 1%), non-communicable (0%; 0%) and communicable diseases (0%; 0%), and essential medicines (0%; 0%) (see Figure 1). There was overall consistency between the cycles in terms of the distribution of recommendations among health issues, which may be partially explained by follow-up on first-cycle recommendations during the second-cycle review.[43] Both cycles produced an uneven distribution of right to health recommendations focused on selected population groups: women, children, and persons with disabilities received many more right to health recommendations than adolescents and LGBTI persons.
In relation to question 3, the recommendations tended to require three main types of action (see Table 1). Domestic implementation measures were the predominant focus, within which there was significant attention to legislation, policies, and programs or unspecific general measures to improve the right to health, with minimal attention to national funding. This was followed by engagement with international human rights mechanisms, and then by measures relating to international cooperation obligations, which received very limited attention. At times, recommendations were not specific: they provided general advice to implement the right to health or address specific issue such as child health or gender-based violence, but without concrete guidance on what should be done or when it should be achieved.
The quantity of right to health recommendations: What can interpretive doctrines of the right to health tell us about apparent disparities in findings between this and other studies?
In contrast to previous analyses suggesting a neglect of the right to health and other ESC rights in UPR recommendations, this article argues that the right to health is actually a prominent one. The proximate cause of these seemingly divergent positions is the different interpretations of the right to health used to frame our and UPR Info’s empirical reviews, the latter of which have been drawn on by the Center for Economic and Social Rights and Special Rapporteur Alston. Different interpretations of human rights legitimately arise because international treaty provisions are vague, with several interpretive doctrines allowing for more than one approach.[44]
Our interpretation is guided by the expansive normative scope of the right to health envisaged by international human rights treaties, one of the main sources of international law, and by the interpretations by treaty bodies, which are considered as authoritative and having significant legal weight.[45] The World Health Organization Constitution, which recognizes health as a human right, provides a broad definition of health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”[46] The International Covenant on Economic, Social and Cultural Rights’ article 12 on the right to health extends beyond health care to embrace other domains such as “environmental and industrial hygiene.”[47] The Convention on the Elimination of All Forms of Discrimination against Women recognizes that the right to health includes entitlements to adequate nutrition during pregnancy.[48] The Convention on the Rights of the Child includes nutritious foods, clean drinking water, environmental sanitation, and the abolition of harmful traditional practices and education on child health within its article on the right to health.[49] Finally, the Convention on the Rights of Persons with Disabilities requires states to prevent discriminatory denial of food and fluids on the basis of disability as part of its right to health article.[50] Over time, treaty bodies and others have updated interpretations of treaty protections on the right to health, taking into account changes in the world health situation and the widening of scope of the notion of health.[51] The treaty bodies have interpreted the right to health to require states to take action on issues such as safe and potable water and basic sanitation; adequate housing and safe and hygienic working conditions, an adequate supply of food, and proper nutrition; alcohol abuse, tobacco, drugs, and other harmful substances; gender-based violence; exclusion and social disparities in health; and corporal punishment.[52] These interpretations, and our findings, incorporate gender-based violence and corporal punishment—more traditionally viewed as CP rights issues of gender equality, security of the person, and the child’s right to protection from violence—as parts of the right to health. Such a teleological approach is derived from the widely held understanding that human rights are dynamic and evolutionary.[53] This approach is predominant within epistemic communities in global health and human rights.
By contrast, the category of right to health recommendations in the UPR Info database utilizes meaningfully narrower parameters. The database’s “Chart of Commonly Used Tags” explains that the following terms are tagged in the database’s right to health category: maternal mortality, reproductive health, sexual and reproductive rights, and achievements of MDGs in the area of health.[54] Recommendations containing the term “health” or health care terms (such as “medicines” and “hospitals”) are also included. Yet this excludes many social determinants. Indeed, many issues located at the intersection of the right to health and other rights are tagged in other categories—for example, nutrition is tagged as a right to food issue, while water/sanitation and HIV/AIDS are assigned their own categories. They are categorized as a right to health issue only if there is also a specific mention of health or another health-related keyword. Moreover, recommendations on right to health issues affecting particular groups are tagged according to the group rather than the right: for example, gender-based violence and abortion are tagged as women’s rights issues rather than as right to health issues. This results in a far smaller tally of right to health recommendations.
These different approaches arise in the context of broader theoretical debates around interpretations of international human rights law, including the right to health. John Tobin has identified intentional, formalist, historical, systematic, teleological, and sociological approaches that can be used to interpret the right to health and that are often combined in practice.[55] Rejecting the predominant teleological approach, Tobin adopts a formalist interpretation of the right to health, which gives particular weight to the text of treaties. This is motivated by his concern with “internal system coherence.”[56] He cautions against an approach that conceives of the right to health as “a repository for everything that impacts upon the health of an individual” and which “encroaches on the normative territory of other rights.”[57] Instead, he supports recognizing the connections between rights. The UPR Info database resembles this approach insofar as it categorizes recommendations according to a leading right or to a group with which a particular right has been predominantly connected in a treaty, rather than the teleological interpretation that results in ever more overlapping territory.
The debate on how overlaps between rights should be understood and how to interpret the concepts of indivisibility and inter-relatedness has yet to be settled.[58] However, given that issues such as gender-based violence, nutrition, and water and sanitation have been widely interpreted as falling within ambit of the right to health (as well as other rights), this article arguably provides an understanding of the extent of the UPR’s right to health recommendations that is more attuned to how this right has evolved. At the same time, because our study focused on the right to health, its findings do not allow for a comparison with other rights: thus, it cannot be said conclusively that the right to health is not neglected compared to other rights. Likewise, our findings cannot be extrapolated to the broader category of ESC rights, so it is quite possible that this category is indeed neglected. What our findings do show conclusively is that more recommendations include a right to health focus than previously thought.
The quality of right to health recommendations: Usefulness and measurability
The quality of the UPR’s recommendations is argued to be determinative of the procedure’s ability to fulfill its objectives.[59] The question of what constitutes a good-quality recommendation is a contested one. I argue that a quality-assessment framework such as the one proposed by Subhas Gujadhur and Marc Limon, based on twin principles of usefulness to the state under review and measurability, is particularly valuable because it is grounded in the UPR’s objectives, including improving the human rights situation on the ground.[60] Using this framework, the following paragraphs consider the quality of UPR right to health recommendations.
Turning first to the issue of usefulness, Gujadhur and Limon suggest that this is determined by the extent to which recommendations are based on an objective analysis of the main human rights challenges facing a country; are sensitive to the country’s situation and available resources; and have potential to effect change. As highlighted above, the normative distribution of right to health recommendations is highly skewed, as is their attention to the types of actions that they require. This provokes the question, is this balance reflective of the right to health situation on the ground, or is it also influenced by other considerations?
Remarkably, many leading right to health problems worldwide—including deficient water and sanitation, HIV/AIDS, communicable and non-communicable diseases, and mental health—were rarely addressed in recommendations. The disproportionate focus on a small range of right to health issues suggests that the right to health situation on the ground is funneled through a selection process that decides what information is presented for review and what topics elicit recommendations.
The UPR is meant to be based on information contained in review documents.[61] A logical assumption is that recommendations reflect the right to health issues that they raise. Indeed, these reports are already known to be important determinants of recommendations.[62] To test this assumption in relation to the right to health, the Human Rights Centre Clinic and World Health Organization carried out a sample analysis of review documents from eight countries and the corresponding right to health recommendations. The review documents for these countries also demonstrated skewed attention to right to health issues. Those issues that received high levels of attention, such as gender-based violence and maternal and child health, went on to receive a high, and sometimes disproportionately high, number of recommendations, while those issues that received limited attention received a much lower, and sometimes disproportionately low, number of recommendations.
The content of review documents is influenced by a range of factors, including, but not limited to, the human rights situation on the ground. A state’s own national report, which is understood to be the most influential input into the process, is meant to be objective and reliable and prepared through a multi-stakeholder process.[63] Yet in practice, national reports often dwell on progress while glossing over obstacles.[64] Many state reports are prepared by the government, sometimes principally by the ministry of foreign affairs, with little consultation within or outside government bodies. This does little to optimize an accurate representation of the right to health situation. Likewise, in terms of the UN report, a key relevant right to health stakeholder, the World Health Organization, has had limited engagement with the UPR process at the national level.[65] Causes may include the organization’s political member state structure and close working relationship with ministers of health; a lack of familiarity with human rights among its staff, who are more often public health and medical professionals; and a perception within the World Health Organization that the UPR is not effective in promoting health.[66] With regard to the stakeholders’ report, which condenses submissions across the range of human rights issues into a 10-page document, there is some suggestion that information on less prominent health and rights issues has not always made the final cut.[67] Below, I suggest that increasing health-stakeholder participation is an important way to improve the spread of issues covered in review documents and subsequently the responsiveness of UPR recommendations to the situation on the ground.
The Human Rights Council’s foundational UPR resolution commits to the operational principles of objectivity and non-politicization.[68] However, in practice, as highlighted above, politically uncontroversial issues are more widely raised than more sensitive ones.[69] In relation to the right to health, topics drawing recommendations from many states, such as gender-based violence, maternal health, child health, and social and economic determinants, are, in many instances, not considered sensitive. By contrast, the issue of abortion was rarely addressed. Many states have restrictive abortion laws that are defended by conservative forces in government and society to protect the fetus.[70] Yet such laws result in higher rates of unsafe abortions, maternal mortality, and other infringements of the sexual and reproductive rights of women.[71] UN treaty bodies and Special Procedures have increasingly called for progressive abortion law reform.[72] However, a keyword search of abortion and termination of pregnancy in UPR recommendations revealed that the issues were explicitly raised in just 28 recommendations (0.16% of right to health recommendations) during the first cycle, almost half of which were made to one state (Nicaragua). In the second cycle, 123 recommendations (0.36% of right to health recommendations) were made on the subject, to a bigger range of states. In both cycles, almost all of these recommendations were made by countries with progressive abortion laws, mostly from the Western European region.
Issue bias also appears to stem from the domestic and foreign policy priorities of recommending states. Gender-based violence and maternal and child health are often high on countries’ health agendas, even if they are not always successfully addressed. Conversely, mental health, which attracted limited attention in recommendations, is often a deeply marginalized right to health issue.[73] This is despite an estimated one in four people worldwide being affected by a mental health condition during their lifetime.[74] At the level of individual counties, Cuba, for example, gave many recommendations focused on access to health services, a well-known national and international cooperation priority of this country, while Norway’s recommendations frequently addressed issues of sexual violence, harmful practices, abortion, and LGBTI health issues, which have been high on the agenda in Norway’s domestic and foreign policies.[75]
The skewed distribution between the types of actions required by recommendations also raises questions about their usefulness in terms of their responsiveness to obstacles to the right to health. Most notable is the very limited number of recommendations on obligations to devote maximum available resources, particularly to the health sector, which is often deeply underfunded. Only 1% of first- and second-cycle recommendations focused on national funding. International cooperation, which includes resource and technical cooperation questions, was also rarely addressed (3% and 1% of first- and second-cycle recommendations, respectively), and almost all those recommendations suggested that states seek, rather than provide, cooperation, although both dimensions are obligations under treaties such as the International Covenant on Economic, Social and Cultural Rights. The reasons for this neglect require further research. However, two issues are perhaps relevant: first, the obligation to provide cooperation is not universally accepted by states, particularly high-income states; second, the review is meant to take into account broader resource constraints of states.[76] Obligations to provide international cooperation and national funding questions could be perceived as awkward to raise given the cooperative approach that animates the UPR.
Turning to a slightly different issue that is also relevant to quality, the UPR has been widely criticized for issuing recommendations that are non-specific, particularly concerning ESC rights.[77] A qualitative review of right to health recommendations reveals that this criticism holds true for these recommendations in two ways. First, it was not uncommon for recommendations to vaguely suggest that states should “take necessary measures” or “do more” to improve the right to health, particular health issues, or treaty implementation, without suggesting how to do so. Second, some recommendations clustered together multiple right to health or human rights issues. Both practices are questionable from the point of view of recommendations’ usefulness and measurability. Recommendations that are unspecific in terms of actions required, or that cluster issues together, provide minimal guidance as to what a state’s priority actions should be, thus affording overly wide discretion to the state. They are also difficult to measure for the same reason—the state can often report progress, including partial or full implementation, but it may not be clear whether these measures are moving the country as “effectively and expeditiously as possible“ toward the full realization of the right to health.[78] Gujadhur and Limon have recommended that the UPR use time-bound recommendations that incorporate indicators against which progress can be measured.[79] At the same time, it is important to recognize that not all recommendations were imprecise: those focused on international human rights mechanisms and domestic legislation were often quite specific, with recommendations focused on treaty ratification, the adoption of new laws, or the amendment of existing laws.
The skewed distribution of recommendations between right to health issues and obligations, as well as the vague phrasing of many recommendations, compromises their quality and limits their potential to improve the situation on the ground. These shortcomings also raise questions about the current suitability of the UPR to support SDG review. In particular, the UPR would need to align more closely to the wider range of right to health issues and obligations that are embraced by the SDGs, which include some issues that are already more prominently addressed (for example, maternal mortality, infant mortality, and access to health services), and some issues and obligations receiving more limited attention (for example, mental health, water and sanitation, HIV, tuberculosis, malaria, neglected and other communicable diseases, non-communicable diseases, tobacco control, the health workforce, health financing, and international cooperation).
The health stakeholder gap and unlocking the UPR’s potential for the right to health
Earlier in this article, I highlighted that the limited understanding of health systems and public health by the human rights community, and the limited understanding of and engagement in human rights by the public health community, pose enduring challenges to the right to health. The limited engagement in the UPR process of key health stakeholders from governments, international organizations, and civil society and the failure of the Human Rights Council to raise a range of relevant right to health norms and obligations in an objective and informed way in recommendations, as discussed in the previous section, are emblematic of this problem.
If the UPR is to make a positive contribution to the right to health on the ground, health stakeholders must be more actively engaged in the UPR process. In some quarters, there are positive existing practices for stakeholder engagement among states, international organizations, and civil society. For example, states are being encouraged to develop national mechanisms for reporting and follow-up, one purpose of which is to enhance engagement and communication between ministries in the UPR process.[80] The UN Secretary-General has requested UN that agencies deepen their participation in the UPR, including with a view to supporting links between the UPR and the implementation of the SDGs.[81] Indeed, the World Health Organization has begun to engage with the UPR at headquarter level, even if not yet routinely at the national level.[82] Some nongovernmental organizations working on health and human rights issues have turned their advocacy efforts away from the UPR, in part because the mechanism has failed to deliver recommendations on issues of concern.[83] In other areas, notably sexual and reproductive health, civil society engagement has been more extensive, whilst the UNFPA has also engaged extensively on these issues.[84]
The involvement of health stakeholders during the lead-up to a state’s review will not only provide expertise to improve the quality of information submitted but also optimize conditions for the implementation of recommendations. Although the implementation of recommendations is not the primary focus of this article, the patchy record of implementation of UPR recommendations is well documented, even if there is some suggestion that recommendations on the right to health have a better implementation record than some other rights.[85] The engagement of health stakeholders in submitting information provides a natural entry point to their engagement at a later date in supporting implementation.
Conclusion
The quantitative and qualitative research underpinning this article has provided an opportunity to reassess the performance of the UPR with respect to the right to health. Based on the empirical data, it is clear that if we understand the right to health in terms of its most widespread contemporary broad interpretation, the right is more prominently addressed by UPR recommendations than was previously understood to be the case.
While the quantity of recommendations appears to signal the value of the UPR for the right to health, this article concurs with previous more general analyses of UPR recommendations that have found the quality of recommendations to generally be poor: this is the case for the right to health too. The article has illustrated how the expert contribution of health stakeholders has been marginalized from the UPR process, notably from the review documents that are submitted for review and, at the same time, how recommendations appear to be influenced by domestic and international political agendas. The result is a spread of recommendations that does little to reflect the balance of obstacles impeding the right to health worldwide. Furthermore, recommendations often suffer from a lack of specificity. Health stakeholders’ greater engagement with the UPR could help provide the level of detail needed for more specific recommendations to be issued. Not only will this support a review that reflects the right to health situation on the ground, but it will also help promote positive change through appropriately tailored recommendations and provide a more comprehensive and balanced body of recommendations to support review of the right to health in the context of SDG review procedures.
Acknowledgments
I am grateful for the important contributions of Rebekah Thomas of the World Health Organization and the following former members of the Human Rights Centre Clinic at University of Essex with regard to data collection and analysis: Camille Gauter, Ingrid Legrand Gjerdset, Alexandra Havkwist, Robert Hoddy, Ajeng Larasati, Giulia Perrone, Tasneem Sadiq, and Raymond Smith. The findings will be published in World Health Organization and Human Rights Centre Clinic (eds), Advancing the right to health under the Universal Periodic Review (Geneva: World Health Organization, forthcoming).
Judith Bueno de Mesquita, MA, LLM, is Lecturer and Deputy Director of the Human Rights Centre Clinic in the School of Law and Human Rights Centre at the University of Essex, Colchester, UK.
Please address correspondence to the author. Email: jrbuen@essex.ac.uk.
Competing interests: None declared.
Copyright © 2019 Bueno de Mesquita. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1]. H. Charlesworth and E. Larking, “Introduction: The regulatory power of the Universal Periodic Review,” in H. Charlesworth and E. Larking (eds), Human rights and the Universal Periodic Review: Rituals and ritualism (Cambridge: Cambridge University Press, 2014), p. 1.
[2]. UN General Assembly, Res. 70/1, UN Doc. A/RES/70/1 (2015).
[3]. Human Rights Council, Res. 5/1, UN Doc. A/HRC/RES/5/1 (2007), para. 3(a).
[4]. For example, Center for Economic and Social Rights, The Universal Periodic Review: A skewed agenda? (New York: Center for Economic and Social Rights, 2015); P. Alston, Report of the Special Rapporteur on Extreme Poverty and Human Rights, UN Doc. A/HRC/32/31 (2016).
[5]. This framework was first proposed in S. Gujadhur and M. Limon, Towards the third cycle of the Universal Periodic Review (Versoix: Universal Rights Group, 2016), p. 18.
[6]. J. Bueno de Mesquita, D. Evans, and C. Fuchs, “The future of human rights accountability for global health through the Universal Periodic Review,” in B. Mason Meier and L. Gostin (eds), Human rights in global health: Rights-based governance for a globalizing world (Oxford: Oxford University Press, 2018), pp. 545–546.
[7]. Constitution of the World Health Organization (1946).
[8]. International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 12. See also, for example, Convention on the Elimination of All Forms of Discrimination against Women, G.A. Res. 34/180 (1979); Convention on the Rights of the Child, G.A. Res. 44/25 (1989); Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006); E. Kinney and B. Clark, “Provisions for health and health care in the constitutions of the countries of the world,” Cornell International Law Journal 37/2 (2004), pp. 285–355.
[9]. A. Kirkup and T. Evans, “The myth of Western opposition to economic, social and cultural rights? A reply to Wheelan and Donnelly,” Human Rights Quarterly 31/1 (2009), pp. 221–238.
[10]. World Conference on Human Rights, Vienna Declaration and Programme of Action, Vienna, June 14–25, 1993, UN Doc. A/CONF.157/24 (Part I) (1993), para. 5.
[11]. UN Commission on Human Rights, Res. 2002/31 (2002).
[12]. R. Thomas and V. Magar, “Mainstreaming human rights across the WHO,” in B. Mason Meier and L. Gostin (eds), Human rights in global health: Rights-based governance for a globalizing world (Oxford: Oxford University Press, 2018); P. Hunt, “Interpreting the international right to health in a human rights-based approach to health,” Health and Human Rights Journal 18/2 (2016), pp. 109–130; Global health and human rights database. Available at https://www.globalhealthrights.org/about-the-database.
[13]. J. Harrington and M. Stuttaford, “Introduction,” in J. Harrington and M. Stuttaford (eds), Global health and human rights: Legal and theoretical perspectives (New York: Routledge, 2010), p. 1. See also B. Mason Meier and L. Gostin, “Introduction,” in B. Mason Meier and L. Gostin (eds), Human rights in global health: Rights-based governance for a globalizing world (Oxford: Oxford University Press, 2018), p. 15.
[14]. Alston (see note 4), para. 9.
[15]. A. Chapman, Global health, human rights and the challenge of neoliberal policies (Cambridge: Cambridge University Press, 2016), ch. 1.
[16]. Ibid.
[17]. Human Rights Council, Universal Periodic Review. Available at https://www.ohchr.org/en/hrbodies/upr/pages/uprmain.aspx.
[18]. B. Mason Meier, M. de Milliano, A. Chakrabarti, et al., “Accountability for the human right to health through treaty monitoring: Human rights treaty bodies and the influence of concluding observations,” Global Public Health 13/11 (2018), pp. 1558–1576.
[19]. A. Allehone, “The role and future of the Human Rights Council,” in S. Sheeran and N. Rodley (eds), Routledge handbook of international human rights law (Abingdon: Routledge Press, 2013).
[20]. UN General Assembly, G.A. Res. 60/251, UN Doc. A/RES/60/251 (2006), para. 5(e).
[21]. OHCHR, Human Rights Council 35th session: Opening statement by Zeid Ra’ad Al Hussein, United Nations High Commissioner for Human Rights. Available at https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=21687&LangID=E.
[22]. Human Rights Council (2007, see note 3), para. 1.
[23]. S. Jensen, UN human rights mechanisms proving effective SDGs monitor (July 4, 2019). Available at https://www.openglobalrights.org/un-human-rights-mechanisms-proving-effective-sdgs-monitor; UN General Assembly (2015, see note 2), para. 18.
[24]. OHCHR, Inputs from the president of the HRC to the 2016 HLPF: The work of the HRC in relation to the 2030 Agenda for Sustainable Development (2016). Available at https://www.ohchr.org/Documents/Issues/MDGs/Post2015/Contribution2016HLPF.pdf.
[25]. K. Donald and M. Ramoroka, Five key takeaways from the 2018 High Level Political Forum (July 30, 2018). Available at http://www.cesr.org/es/node/49690.
[26]. Human Rights Council (2007, see note 3), para. 3(b).
[27]. Ibid., para. 3; V. Carrero, “The United Nations treaty bodies and Universal Periodic Review: Advancing human rights by preventing politicization?” Human Rights Quarterly 39/4 (2017), pp. 943–970.
[28]. Carrero (see note 27).
[29]. W. Kalin, “Rituals and ritualism at the Universal Periodic Review: A preliminary appraisal,” in H. Charlesworth and E. Larking (eds), Human rights and the Universal Periodic Review: Rituals and ritualism (Cambridge: Cambridge University Press, 2014), p. 38; Charlesworth and Larking (see note 1), p. 20.
[30]. M. Nowak, “It’s time for a world court of human rights,” in C. Bassiouni and W. Schabas (eds), New challenges for the UN human rights machinery (Antwerp: Intersentia, 2011), p. 23.
[31]. Gujadhur and Limon (see note 5), p. 18.
[32]. Human Rights Council (2007, see note 3), para. 15.
[33]. R. Chauville, “The Universal Periodic Review’s first cycle: Successes and failures,” in H. Charlesworth and E. Larking (eds), Human rights and the Universal Periodic Review: Rituals and ritualism (Cambridge: Cambridge University Press, 2014) , p. 87.
[34]. Charlesworth and Larking (see note 1), p. 7.
[35]. Center for Economic and Social Rights (see note 4).
[36]. Alston (see note 4), para. 50.
[37]. UPR Info, Statistics of recommendations. Available at https://www.upr-info.org/database/statistics/index.php?cycle=1.
[38]. United Nations Population Fund, Lessons from the second cycle of the Universal Periodic Review (New York: United Nations Population Fund, 2019).
[39]. For example, Committee on Economic, Social and Cultural Rights, General Comment No. 14, The Right to the Highest Attainable Standard of Health, UN Doc. E/C.12/2000/4 (2000); Committee on Economic, Social and Cultural Rights, General Comment No. 22, The Right to Sexual and Reproductive Health, UN Doc. E/C.12/GC/22 (2016).
[40]. Commission on the Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health (Geneva: World Health Organization, 2008).
[41]. O. Solar and A. Irwin, A conceptual framework for action on the social determinants of health, Social Determinants of Health Discussion Paper 2 (Policy and Practice) (Geneva: World Health Organization, 2010).
[42]. Committee on Economic, Social and Cultural Rights (2016, see note 39), paras. 7–8.
[43]. Human Rights Council, Res. 16/21, UN Doc. A/HR/Res/16/21 (2011), para. 7.
[44]. J. Tobin, The right to health in international law (Oxford: Oxford University Press, 2012), p. 75.
[45]. M. Craven, The International Covenant on Economic, Social and Cultural Rights: A perspective on its development (Oxford: Clarendon, 1995), p. 91; H. Steiner and P. Alston, International human rights in context: Law, politics, morals, 2nd ed. (Oxford: Oxford University Press, 2000), p. 265.
[46]. Constitution of the World Health Organization (1946), preamble.
[47]. International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), art. 12.
[48]. Convention on the Elimination of All Forms of Discrimination against Women, G.A. Res. 34/180 (1979), art. 12.
[49]. Convention on the Rights of the Child, G.A. Res. 44/25 (1989), art. 24.
[50]. Convention on the Rights of Persons with Disabilities, G.A. Res. 61/106 (2006), art. 25.
[51]. Committee on Economic, Social and Cultural Rights (2000, see note 39), para. 10.
[52]. Ibid; see also Committee on the Elimination of All Forms of Discrimination against Women, General Recommendation No. 24 on Women and Health (1999), para. 15; Committee on the Rights of the Child, General Comment No. 15 on the Right of the Child to the Enjoyment of the Highest Attainable Standard of Health, UN Doc. CRC/C/GC/15 (2013), para. 24.
[53]. S. Sheeran, “The relationship of international human rights law and general international law: a hermeneutic constraint, or pushing the boundaries?” in S. Sheeran and N. Rodley (eds), Routledge handbook of international human rights law (Abingdon: Routledge Press, 2013), p. 102.
[54]. UPR Info, UPR Info’s database (2016). Available at https://www.upr-info.org/database/files/Database_Issues_explanation.pdf.
[55]. Tobin (see note 44), p. 79.
[56]. Ibid., p. 105.
[57]. Ibid., pp. 108–109.
[58]. A. Chapman, “The social determinants of health, health equity and human rights,” Health and Human Rights 12/2 (2010), pp. 17–30.
[59]. Gujadhur and Limon (see note 5), p. 29.
[60]. Ibid., p. 30.
[61]. Human Rights Council (2007, see note 3).
[62]. Gujadhur and Limon (see note 5).
[63]. UN General Assembly (2006, see note 20); Human Rights Council (2007, see note 3), para. 15(a).
[64]. Gujadhur and Limon (see note 5), p. 39.
[65]. J. Bueno de Mesquita, R. Thomas, C. Gauter, et al., “Monitoring the sustainable development goals through human rights accountability reviews” World Health Bulletin 96/9 (2018), pp. 627–633.
[66]. B. Mason Meier and F. Kastler, “Development of human rights through WHO,” in B. Mason Meier and L. Gostin (eds), Human rights in global health: Rights-based governance for a globalizing world (Oxford: Oxford University Press, 2018), p. 111; Thomas and Magar (see note 12), p. 133; Bueno de Mesquita et al. (see note 6).
[67]. D. Lohman and J. Amon, “Evaluating a human rights-based advocacy approach to expanding access to pain medicines and palliative care: Global advocacy and case studies from India, Kenya, and Ukraine,” Health and Human Rights 17/2 (2015), pp. 149–165.
[68]. Human Rights Council (2007, see note 3).
[69]. Carrero (see note 27), p. 958.
[70]. Ibid.
[71]. S. Singh, D. Wulf, R. Hussain, et al., Abortion worldwide: A decade of uneven progress (New York: Guttmacher Institute, 2009).
[72]. J. Fine, K. Mayall, and L. Sepulveda, “The role of international human rights norms in the liberalization of abortion laws globally,” Health and Human Rights 19/1 (2017), pp. 69–79.
[73]. D. Puras, Report of the Special Rapporteur on the Right to Health, UN Doc. A/HRC/35/21 (2017).
[74]. World Health Organization, “Mental disorders affect one in four people” [press release], October 4, 2001. Available at https://www.who.int/whr/2001/media_centre/press_release/en.
[75]. See, for example, Ministry of Foreign Affairs, “Norway to increase support for women’s health and safe abortion,” [press release], October 12, 2017. Available at https://www.regjeringen.no/en/aktuelt/womens_health/id2574852.
[76]. J. Bueno de Mesquita, P. Hunt, and R. Khosla, “The human rights responsibility of international assistance and cooperation in health,” in M. Gibney and S. Skogly (eds), Universal human rights and extraterritorial obligations (Philadelphia: University of Pennsylvania Press, 2010).
[77]. Center for Economic and Social Rights (see note 4), p. 6.
[78]. Committee on Economic, Social and Cultural Rights, General Comment No. 3, The Nature of States Parties’ Obligations (1990), para. 9.
[79]. Gujadhur and Limon (see note 5), p. 31.
[80]. OHCHR, National mechanisms for reporting and follow-up (New York: United Nations, 2016).
[81]. Report of the Secretary-General on the Work of the Organization, UN Doc. A/72/1 (2016), para. 98.
[82]. F. Bustreo, V. Magar, R. Khosla, et al., “The future of human rights in WHO,” in B. Mason Meier and L. Gostin (eds), Human rights in global health: Rights-based governance for a globalizing world (Oxford: Oxford University Press, 2018).
[83]. Lohman and Amon (see note 67).
[84]. United Nations Population Fund (see note 38).
[85]. UPR Info, Beyond promises: The impact of the UPR on the ground (Geneva: UPR Info, 2014), p. 28.