Witnessing Obstetric Violence during Fieldwork: Notes from Latin America
Volume 21/1, June 2019, pp 103 – 113
Arachu Castro
Abstract
Violence against women in labor occurs frequently in Latin America, based on observations from my extensive ethnographic fieldwork in various Latin American countries. In this article, focused on Mexico and the Dominican Republic, I contextualize obstetric violence within the larger context of social exclusion and discrimination against women. I establish associations between maternal deaths and health care systems characterized by a lack of continuum of care, a lack of accountability toward women, and the withholding of care. I argue that clinical staff learn to operate within the structural limitations of health care systems by not assuming the responsibility of the continuum of care that each woman needs, and that this discharge of accountability is at the heart of how health professionals can navigate, tolerate, and perpetuate the structure of the system and, in so doing, create the breeding ground for obstetric violence to occur. Finally, I explain that although reporting on the suffering of women will not, on its own, prevent obstetric violence, increasing its visibility through research can contribute to human rights-based advocacy on behalf of women in labor, to the monitoring of human rights standards, and to the creation of accountability measures within health systems to prevent obstetric violence.
Witnessing violence against women in labor
I have conducted fieldwork in public hospitals across Latin America since 1998. In every case, the administrators of public hospitals and health centers allowed me in as part of research projects conducted collaboratively between my United States-based university—Harvard University until 2012 and Tulane University since 2013—and ministries of public health, at times also involving international organizations. These studies, conducted in Mexico, Cuba, Colombia, Peru, Nicaragua, and the Dominican Republic, received ethical review approval. Their methodologies included open-ended interviews with women and health professionals, the observation of clinical encounters in public health facilities during pregnancy and childbirth, and epidemiological data analysis.[1] I served as research director for these studies and, as an academic trained both in medical anthropology and in public health, I had both the urge and the curiosity to observe women’s experiences in a clinical setting, without intermediaries. Having given birth twice before I started research related to childbirth allowed me, at least to a certain extent, to understand other women’s experiences from a vantage point of shared human experience. My preliminary concerns around seeing blood easily subsided, but my struggle as an observer of violence against women and of human rights violations became a real predicament.
The first time I observed a woman giving birth, I was researching the rise of cesarean sections in Mexico. The 20-year-old woman in labor had no obstetric complications, but she had to endure several threats from her female obstetrician, who kept yelling at her because she refused epidural anesthesia as a result of how painful it had been during her previous childbirth. Her plea to not be punctured was unsuccessful, and she gave birth to a healthy child a few minutes later. While the doctor took the newborn to a side table to conduct the Apgar test, the young woman kept asking if her child was a boy or a girl. Given that nobody was answering and that I was standing between the woman and the child, I told her she had a boy. Later that week, I observed my first birth by cesarean section:
July 14, 1998. In a large public maternity hospital in Mexico City, Antonia arrives in a wheelchair at the operating room. She is 23, mother of a young child, and is 37 weeks pregnant with twins, one of which is breeched. She is going to have a cesarean section, just like she had the first time she gave birth. Soon after the anesthetist places an epidural, most of her body starts to numb. A male surgeon arrives in the operating room and asks Antonia how many children she has. She responds one. The surgeon bluntly asks her if she’s going to “get tied” this time—¿y te vas a ligar ya? Antonia says no, and the surgeon looks at her in dismay and leaves. Twelve minutes later the cesarean section begins. Two residents are performing the surgery, and there are a total of nine people around Antonia, including myself. The male surgeon comes back. Six minutes later, two healthy girls are born. While the residents are stitching Antonia, the male surgeon asks her: “Aren’t you going to get tied?” Upon Antonia’s firm and negative response, he gets mad at her and leaves.[2]
I started to take these notes and to sketch a drawing of the operating room while seated on the floor against a wall, as I was concerned that I would not be able to withstand observing the surgery while standing up. Immediately after the procedure began, Antonia had asked if someone could hold her hand, but everyone around us seemed too busy to care about her request. I was compelled to get closer to her and hold her hand, and I did as soon as I realized I would be okay standing so close to the procedure without fainting. I was by her side while a medical doctor was yelling at her, trying to force her to agree to be permanently sterilized. I talked to her while memorizing the scene so that I could later record the episode in my notes.
Beyond some degree of empathy that I could transmit to these young women while they were giving birth, I knew that my presence during these critical moments in their lives was easily forgettable. In these and all the subsequent births that I observed, I did no harm, but did I do any good? As an anthropologist, I could at least see myself as a participant observer and not as a mere observer. I was interacting with the women in labor after all, but I was keeping quiet. At a minimum, I could write about it, and in doing so, I deliberately chose the word violence to define these obstetric events:
The increase of caesarean sections can thus be regarded as a process in which women are finally given less information and less choice and in which obstetricians appropriate the central role of childbirth at the expense of women. Finally, “violence” is a strong word, and labelling unnecessary caesarean sections as form of violence against women could be disturbing. But for many women, a caesarean section that could have been avoided is a violation of their bodily integrity, just like having routine episiotomy (or perineal cutting), epidural anesthesia without consent, non-indicated oxytocin induction or augmentation, multiple and painful vaginal examination, non-indicated amniotomy, or pubic shaving, needless exposure of sexual parts in common labour rooms, or even transcaesarean tubal ligations when women do not understand the permanent nature of the procedure. In order to give back to women the central role in childbirth, new guidelines aimed at restricting the use of caesarean sections and other birth technologies by improving the quality of care should be welcomed.[3]
Scenes of violence against women in labor are the norm, rather than the exception, in the various Latin American countries where I have conducted ethnographic fieldwork. Beginning in 2009, I started to conduct fieldwork in hospitals in the Dominican Republic, first to explore the management of HIV and syphilis during pregnancy and then, having identified a series of issues that could be behind the country’s high maternal mortality ratio, to focus on referrals of women with obstetric complications and on the causes of their deaths.[4] In that context, I was in the labor room where a woman was giving birth vaginally, assisted by two residents, when the nurse, seated in the bench next to mine, told the woman in labor, ¡No grites tanto! (Don’t scream that loud!). Not convinced that arguing with the nurse was the most effective way to bring that humiliation to an end, I decided to challenge her differently. If the nurse verbally attacked the woman in labor again, I would ask her why. “Excuse me, nurse, why did you tell her not to scream that loud? What is your purpose?” I struggled to navigate my appropriate role as a researcher in this context, wanting neither to compromise my access to the hospital nor to allow what I felt was abusive behavior to go unchallenged. I felt this approach would potentially allow me to continue my research without being involved in an argument.
A few minutes later, I was invited to observe a cesarean section in a tiny operating room, wearing a white coat like during many other observations, and with the consent of the young woman in labor. Two obstetricians and an anesthesiologist were diligently caring for the woman, shown in Figure 1. As in the past, and to prevent interfering with clinical care, I was standing against the wall, about three feet away from the woman in labor. A nurse kept passing between us. As the young woman’s abdomen was being cut, I purposely made eye contact with her and started a conversation. To my surprise, the nurse asked me, “What’s up, are you her relative or what?” I smiled, ironically, at the fact that showing some humanity could be considered out of place.
Building a case for obstetric violence
In 2010, I started to collect data from medical records, verbal autopsies, and hospital case discussions of all reported maternal deaths in the capital city of Santo Domingo to determine the social context in which the deaths occurred and to establish which types of delays (in seeking medical care, in reaching the health facility, or in obtaining care once in the health facility) and which health system factors contributed to the deaths. The study was aimed at informing the national program to reduce maternal mortality. In 2008–2012, hypertensive disorders of pregnancy (mainly preeclampsia and eclampsia) constituted the first cause of the 625 reported maternal deaths in the Dominican Republic, accounting for 36% of cases, followed by hemorrhage, other obstetric complications, sepsis, and abortion; 55% of deaths occurred in Santo Domingo and the surrounding province.[5] But without understanding the social and health system contexts in which these happened, I argue that limiting the analysis to the ultimate cause of death would not be sufficient to create an efficient program to reduce maternal mortality.
Although the study was originally going to last 12 months, halfway into the research and having studied the circumstances of 49 dead women, it became clear to me that, beyond the distribution of clinical causes, these women were dying according to set patterns. The patterns were systemic, produced mostly by the health care system. Health care systems vary in the way that they organize the functioning of teams, networks, and facilities; therefore, we can expect different health systems to achieve different epidemiological outcomes. With an average of one maternal death every four days in Santo Domingo and one death every other day in the country, these were not unpredictable or random, but expected events produced by the health system.[6]
The following three narratives present examples of maternal deaths that could have been prevented, according to the field epidemiologists who conducted the verbal autopsies of the three women and the maternal mortality review committees that discussed two of their deaths:
- In August 2010, a 29-year-old domestic worker in the late stage of pregnancy and her husband went to the local rural public hospital where she had been receiving prenatal care. While waiting to be seen, she developed seizures, was treated with magnesium sulfate to prevent additional seizures, and was told to go to a larger hospital to continue her treatment. The woman and her husband took a two-hour bus ride on a bumpy road through sugarcane plantations to get to the closest general hospital—a ride that takes just 45 minutes by car. Upon their arrival at 12:40 p.m., she was diagnosed with severe preeclampsia, was treated with magnesium sulfate and hydralazine (a hypotensive medication), had an emergency cesarean section, and gave life to a newborn. Because her seizures were not subsiding and the intensive care unit was not operational, hospital staff immediately drove her by ambulance to the national maternity hospital in Santo Domingo, the capital city, where she arrived unconscious at 3:40 p.m. She was admitted and transferred to the intensive care unit, where she was treated for eclampsia. Five days later, due to neurological trauma, she was taken by ambulance with a doctor to the intensive care unit at a general hospital in the city, where she died four days later after a second cardiac arrest. The reported cause of death was cerebral edema. Most of the information about the care that she received at the four hospitals, which was missing from her clinical history, was reconstructed through a verbal autopsy conducted with her husband and during a discussion of the maternal mortality review committee that evaluated her case. Committee members determined, while I was taking notes, that her death could have been avoided if the staff in the last two hospitals had followed the national clinical protocols; they stated that the first two facilities were underresourced and should not be held accountable.
- In January 2011, a 27-year-old hotel janitor who was the mother of an eight-year-old was admitted to a nonprofit general hospital in Santo Domingo with vaginal hemorrhage, a high temperature, and jaundice—which had resulted from an unsafe curettage performed at a clandestine clinic two days earlier. Upon diagnosis of multiorgan failure, a multidisciplinary clinical team recommended an emergency blood transfusion and a laparotomy, followed by dialysis. The staff contacted her family, urging them to bring blood before they could perform any procedures. The following evening, after the family was able to find a suitable donor and bring blood to the hospital, the surgery began. The doctors discovered a massive internal hemorrhage and a punctured uterus, which they removed along with the woman’s ovaries and fallopian tubes. One day later, after a multitude of severe symptoms, the woman died; her reported cause of death was septic abortion. A few days later, I accompanied the two epidemiologists who conducted the verbal autopsy at her family’s home. The woman’s parents and siblings explained that the hospital never informed them of the severity of the condition. Upon learning that she died as a result of “what cannot be spoken,” her father said that “silence killed her.” When epidemiologists from the health district tried to conduct the maternal mortality review meeting at the hospital, the staff declined and directed the epidemiologists to identify the clandestine clinic, which they never found.
- In February 2011, a 28-year-old woman in her 37th or 38th week of pregnancy and mother of four went to the emergency room of a public maternity hospital in Santo Domingo at 11:10 a.m. She was diagnosed with severe preeclampsia and was admitted to the prelabor room at 11:50 a.m. The staff contacted her family members by phone, urging them to bring blood. At 7 p.m., after the family brought the blood, the blood transfusion and cesarean section began under epidural anesthesia. The woman gave life to a newborn son and had her fallopian tubes and 200 cc of blood clots removed. She was transferred to the recovery room and was left alone until three hours later, when a second-year resident found her profusely bleeding and under respiratory distress. An attending doctor and a fourth-year resident evaluated the woman, diagnosed uterine atony, and conducted an emergency laparotomy, during which she lost 300 cc of blood and had her uterus removed. The woman went into cardiac arrest and died in the operating room at 1 a.m. The reported cause of death was preeclampsia. The maternal mortality review committee members determined, while I took notes, that her death could have been prevented if the woman had not been neglected in the recovery room.
All three women were diagnosed with severe obstetric complications at health facilities, where interruptions in care eventually led to their deaths. In the first case, the medical staff discharged a woman on the brink of death without fully attempting to manage the situation; in the second and third cases, the staff withheld the women’s care while waiting for replacement blood donors; additionally, the staff abandoned the third woman after surgery in the recovery room. There are undoubtedly limitations in access to blood in Dominican health facilities, where 80% of blood in 2011 came from replacement donors, mostly family members, and in access to safe abortion, which is strictly forbidden with no explicit legal exceptions.[7] Despite clinical errors that maternal mortality review committees could identify in each case, the fundamental contributing determinant of these deaths was the structural state of the health system—in particular, its limited capacity to provide people-centered care that is convenient, comprehensive, integrated, longitudinal throughout the life cycle, proactive, and in which health providers are responsible and accountable to their patients.[8]
When I told my collaborators at the Dominican Ministry of Public Health that I was ready to share my preliminary findings, they invited me to give a formal presentation in March 2011 to a group of public health decision makers and hospital directors. Wanting to move away from the concept that clinical errors occur in a vacuum, I summarized the causes of the 49 deaths according to five systemic categories, each of which was formed by a list of criteria—the causes of the causes of the maternal deaths. Four of the categories relate to health system issues—the organization of care inside the hospitals, the lack of a culture of patient safety, the lack of guidelines for referrals and counter-referrals of women from one facility to another, and infrastructure limitations—whereas the fifth highlights the structural conditions of poverty and social inequality among the population that usually seeks care in public health facilities. The disconnect between the needs of this population and a health care delivery system that is better designed to meet the needs of medical doctors than those of women who live with multiple deprivations creates additional friction in an already rough landscape.
Drawing from the concepts of diagnostic and classification criteria for diseases—according to which a set of criteria must be met to reach a particular diagnosis—I created a list of systemic symptoms associated with maternal morbidity and mortality. My collaborators accepted the findings and began circulating “The 30 Reasons” list to other decision makers and hospital administrators.
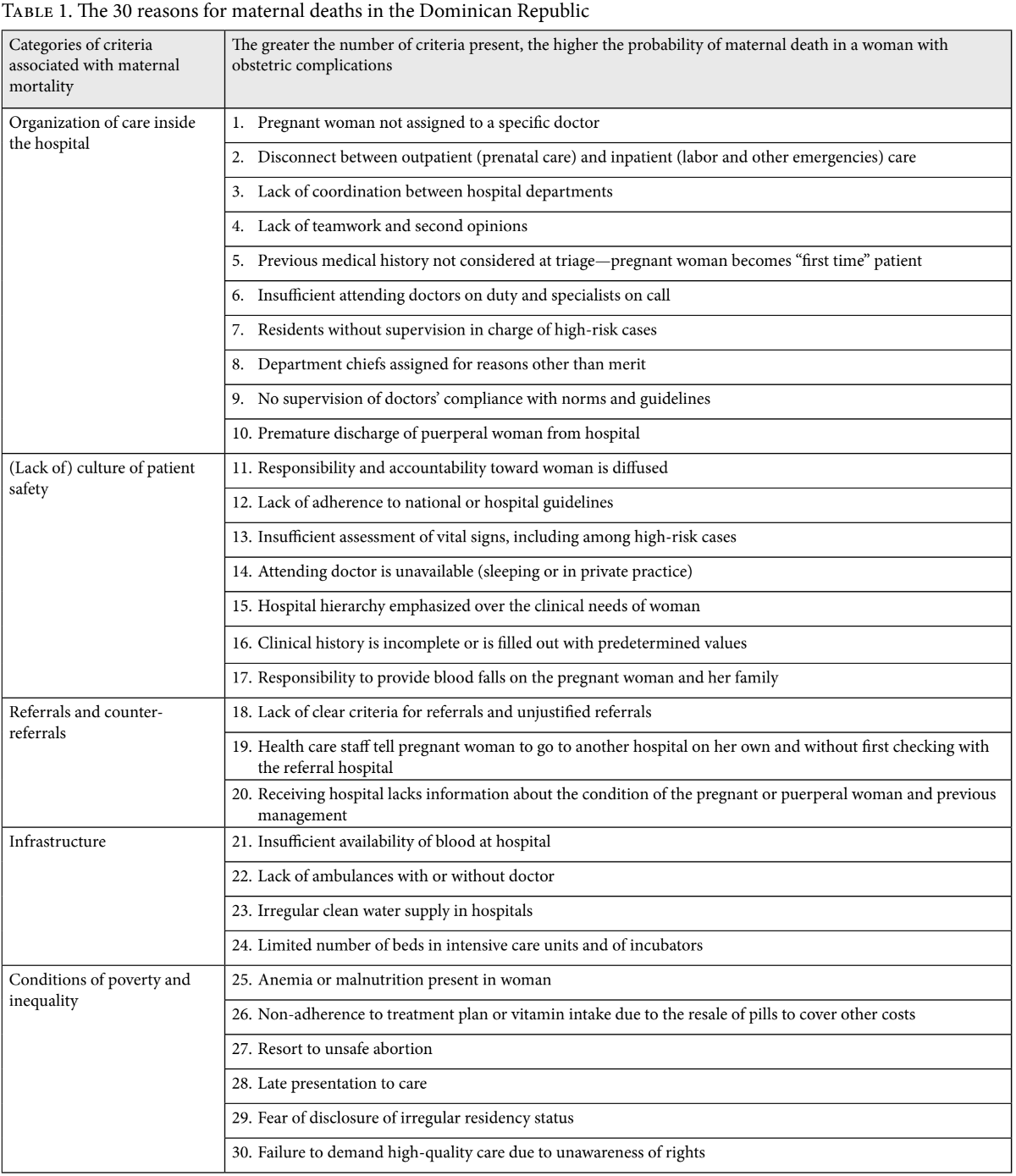
Without exception, each maternal death fulfilled several of the thirty criteria, bringing to the fore a health system characterized by a lack of continuum of care, a lack of accountability toward women on the part of health care providers, and the withholding of care and even outright neglect. Unfortunately, eight years later, the list is still applicable, and casualties remain high. The number of reported maternal deaths between 2011 and 2018 kept steady at an average of 186 per year; in 2017, the last year with complete data, the maternal mortality ratio was 124 maternal deaths per 100,000 live births—much higher than the Millennium Development Goal target of 47 deaths per 100,000 live births by 2015.[9] Without mechanisms to redress the systemic causes of maternal mortality, the right to health will remain an elusive aspiration for many pregnant women, particularly for those living with multiple deprivations. Although a maternal death is considered a rare event in epidemiological terms, it adds up to about 7,000 deaths in Latin America each year—20 every day—usually as a result of causes that are preventable with current knowledge bases; these deaths occur disproportionately among indigenous women, Afro-descendant women, and women who live in poverty.[10]
Violence against women in labor as an affront to human rights
Throughout the world, broad social exclusion and discrimination—the denial of rights, resources, and services available to dominant groups—against women, ethnic minorities, the poor, sexual minorities, and other populations whose rights are often trespassed have a significant negative impact on these populations’ mental and physical health that result from stress responses.[11] In segmented health systems in which users of public health facilities are overwhelmingly from the lowest wealth quintiles, the clinical encounters in the public system become the locus of reproduction of unbalanced social and gender power dynamics between patients and healers (doctors, nurses, and nurse assistants) and among health care workers of different hierarchical positions; unbalanced dynamics can also result from racist treatment. In these contexts, the resulting mistreatment—which often takes a form of triple exclusion and discrimination on account of being poor, dark-skinned, and female—is systematically embedded within clinical encounters, contributing to differential health outcomes, not only as a stressor, but as a result of poor quality of care or outright neglect.[12]
These forms of violence are dually intolerable: they are both an infringement of human rights and fuel for inequitable health outcomes between minority and dominant ethnicities. Given its magnitude, I decided to embrace the concept of obstetric violence, first defined in 2007 in Venezuela as “the appropriation of women’s bodies and reproductive processes by health personnel that is expressed through dehumanizing treatment, the abuse of medicalization, and the pathologization of natural processes, resulting in a loss of women’s autonomy and ability to decide freely about their bodies and sexuality, negatively affecting their quality of life.”[13] Such violence stems both from the actions of medical personnel and from structural issues within health care facilities and health systems.[14]
Most definitions of obstetric violence in Latin America emphasize the medicalization of the natural process of childbirth, as well as the unbalanced power dynamics between health personnel and women in labor that result from a combination of institutional and structural violence. In the 1990s, researchers working in Mexico started to focus on mistreatment of women during institutional childbirth—such as unnecessary cesareans or episiotomies and nonconsensual intrapartum sterilizations—as a form of violence or abuse that resembles other forms of violence against women, and to discuss the institutional and structural violence that reflect gender inequalities and power hierarchies within health facilities.[15]
I argue that in the Dominican Republic, physicians and nurses learn to operate within the structural limitations of the health care system by providing care for concrete evaluations and procedures, but without assuming the responsibility of the continuum of care that each woman needs. Even when their interventions may be clinically appropriate for each circumstance, the responsibility for the management of each woman is so diffused that nobody seems to be in charge. This discharge of accountability is at the heart of how health professionals can navigate, tolerate, and perpetuate the structure of the health care system and, in so doing, create the breeding ground for obstetric violence to occur. As the examples in this paper illustrate, it can be difficult to isolate the boundaries between the structural violence of a low-resourced health system failing to provide adequate care and acts of obstetric violence that women in labor experience at the hands of clinical staff. Here, we can see that obstetric violence is perpetuated by a system but enacted by individuals, and it is precisely these individuals who hold the power to transform the right to health guaranteed by treaties and laws from rhetorical to real.[16]
The 30 Reasons highlight the lack of enforcement of Dominican laws aimed at guaranteeing the right to health—through timely, quality, and dignified health care—for pregnant women and at preventing violence against women in any form. In 1997, the Congress of the Dominican Republic incorporated into law the Inter-American Convention on the Prevention, Punishment and Eradication of Violence against Women of 1944 and the Convention on the Elimination of All Forms of Discrimination against Women of 1979.[17] Furthermore, the country’s General Law of Health of 2001, in its article 14, establishes that the Ministry of Public Health should “ensure that patients receive timely care, of quality and provided with warmth, respectful of their cultural environment, their human rights and citizenship rights enshrined in constitutional regulations.” According to article 28 of this law, all people have the right to “respect for their personality, human dignity and privacy, and not to be discriminated against for reasons of ethnicity, age, religion, social condition, politics, sex, legal status, economic situation, or physical, intellectual, sensory, or any other limitations.” Additionally, article 30 defines priority groups as “people who are at and below the poverty line, within which … priority must be given to women, with special emphasis on pregnant women, children up to the age of 14, the elderly, and the disabled.”[18] Pregnancy and motherhood are further protected by article 30 of the Code for the Protection of the Rights of Children and Adolescents of 2003, according to which “the state will protect motherhood. To this end, it will guarantee [women’s] care through free services and programs of the highest quality, during pregnancy, delivery and the postnatal phase.”[19]
The Constitution of 2015 also prohibits violence against women and protects personal integrity. Article 42 states that “everyone has the right to respect for their physical, mental, and moral integrity and to live without violence,” that “no person may be subjected to penalties, torture or humiliating procedures that involve the loss or diminution of their health, or of their physical or mental integrity,” and that “the state will guarantee by law the adoption of necessary measures to prevent, punish, and eradicate violence against women”; in addition, article 61 states that “everyone has the right to comprehensive health.”[20] Finally, the 2030 National Development Strategy, which was signed into law in 2012, “guarantees the right of the population to access a model of comprehensive care, with quality and warmth, which privileges the promotion of health and the prevention of disease, through the consolidation of the National Health System.” It aims to provide “ongoing training to health personnel to improve and promote the early diagnosis, care and rehabilitation of victims of gender violence and against children and adolescents,” to design “a system for supervising and sanctioning non-compliance with protocols among the clinical and administrative personnel of the health system,” to develop “health system units for gender-based violence, domestic and/or sexual violence that report to competent authorities,” and to promote “a culture of eradication of domestic violence and against women, children and adolescents.”[21]
The Ministry of Public Health—through the National Health Quality Policy and the Technical Regulations for the Care of Women during Pregnancy, Childbirth and Postpartum, both issued in 2013—promotes humanized, dignified, and non-discriminatory care.[22] According to the latter, the principles of maternal care include “respect for human rights. No pregnant woman can be obliged to receive services or care without her prior consent, expressed in a conscious way and free of coercion of any kind. The care should be performed in a responsible, dignified and respectful manner, without discrimination of any kind and with full respect for her rights as a patient.” Finally, obstetric violence was referenced for the first time in the Dominican Republic through a 2016 health regulation issued by the Ministry of Public Health. This regulation—known as the Protocol of Attention for the Integral Management of Pregnancy, Childbirth and Postpartum in Adolescents under the Age of 15—states that during any vaginal birth, cesarean section, or abortion being experienced by an adolescent, it is essential to humanize care and to “ensure respect for their privacy and modesty, avoiding any manifestation of obstetric violence.”[23] Although I expect that future protocols will be updated to include women of any age, the Dominican Constitution and existing laws provide a human rights framework to protect women during pregnancy and childbirth, to guide the provision of respectful maternal health care, and to eliminate the practice of obstetric violence. The critical question becomes how to translate this aspirational framework into a health care system in which clinical staff no longer neglect their accountability toward women in labor but instead enable their attainment of the right to health.
Scholarship with commitment: Obstetric violence as the object of study
I reject being a pacific bystander while conducting fieldwork in public health facilities, one of the few institutional spaces where, in Latin America, indigenous and Afro-descendant women are more present than women from dominant ethnic groups—the latter being understood as powerful and not necessarily greater in number. I am compelled to engage dynamically with the issue of obstetric violence by bringing it to the center of my studies, in line with the “scholarship with commitment” perspective promoted by Pierre Bourdieu and other social scientists, as well as the “praxis” concept developed by the Latin American social medicine movement.[24] The triple exclusion of and discrimination against women who seek care in public health facilities (on account of their being female, dark-skinned, and poor), which causes the withholding of timely and quality care, a lack of accountability mechanisms toward them, and other forms of obstetric violence, run counter a human rights-based approach.[25]
Unlike other Latin American contexts in which women who have been dehumanized during childbirth refrain from seeking care in the future, Dominican women who have these three attributes that silently make them a target for obstetric violence continue to deliver in overcrowded public hospitals. In a recent study that I coauthored with Virginia Savage, in which we interviewed women who were being discharged from a public hospital right after childbirth, we found that most women who experienced obstetric violence talked about it uneventfully.[26] Philosophers such as Martha Nussbaum have described this form of resignation or endurance as “adaptive preference”—that is, “the preference to put up with abuse” in response to restricted options among the structurally deprived, which creates “overtly subservient tendencies”; or, as Amartya Sen has explained, “the underdog learns to bear the burden so well that he or she overlooks the burden itself.”[27] In our study, we found that only those women who feared for their lives or those of their newborns or who realized that they were being neglected developed a capacity to critically reflect on the coercive circumstances that could eventually cause them to die, to understand that their survival depended on hospital personnel, and to develop an autonomous rejection of obstetric violence.[28]
Explaining the suffering of women will not, on its own, prevent obstetric violence. However, the visualization of obstetric violence rendered by research offers two key benefits. First, it contributes to advocacy for the adoption of human rights-based approaches that protect women during pregnancy and childbirth when none exist. Second, it contributes to the monitoring and documentation of human rights standards “to deepen our understandings of the nature of violations, their causes and effects, and the development of more comprehensive human rights standards to guide remedy and redress measures” and to create accountability measures within health systems to prevent obstetric violence.[29] In Proyecto Mujer al Centro (Pregnant Women-Centered Care Project), we are studying the associations among obstetric violence, adverse maternal and child health outcomes, and inequity in the right to health—and, by doing so, we aim to dispel the myth that obstetric violence in a health care setting is uneventful.
Acknowledgments
I thank Marilyn Heymann for her diligent assistance with the coordination and analysis of my maternal mortality study in the Dominican Republic, Naiara Appaix-Castro for her critical review of this paper, Rachel Hall-Clifford for her suggestions, and Dr. José Mordán for his continuous support of my research on behalf of the Ministry of Public Health of the Dominican Republic and for our fruitful conversations on the issue of obstetric violence.
Note: All translations from Spanish to English were performed by the author.
Arachu Castro, PhD, MPH, is Samuel Z. Stone Chair of Public Health in Latin America in the Department of Global Community Health and Behavioral Sciences at the Tulane University School of Public Health and Tropical Medicine, New Orleans, USA, and President of the Society for Medical Anthropology.
Please address correspondence to the author. Email: acastro1@tulane.edu.
Competing interests: None declared.
Copyright © 2019 Castro. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
[1]. A. Castro, A. Heimburger, and A. Langer, Iatrogenic epidemic: How health care professionals contribute to the high proportion of Cesarean sections in Mexico (Cambridge, MA: David Rockefeller Center for Latin American Studies at Harvard University, 2003); A. Castro, “Contracepting at childbirth: The integration of reproductive health and population policies in Mexico,” in A. Castro and M. Singer (eds), Unhealthy health policy: A critical anthropological examination (Walnut Creek, CA: Altamira Press, 2004), pp. 133–144; A. Castro, Y. Khawja, and I. González-Núñez, “Sexuality, reproduction, and HIV in women: The impact of antiretroviral therapy in elective pregnancies in Cuba,” AIDS 21/S5 (2007), pp. 49–54; A. Castro and U. Sandesara, Integración de la atención prenatal con los procesos de detección y manejo clínico del VIH y de la sífilis en el Perú / Integration of prenatal care with the testing and treatment of HIV and syphilis in Peru (Lima: Socios En Salud, Ministry of Health of Peru, UNAIDS, and UNICEF, 2009); M. Connolly, C. Bautista, and A. Castro, “Utilización del formulario de la historia clínica perinatal y neonatal en República Dominicana,” Boletín del Centro Nacional de Investigaciones en Salud Materno Infantil 19/3 (2009), pp. 17–23; E. Pérez-Then, M. Miric, and A. Castro, Integración de la atención prenatal con los procesos de detección y manejo clínico del VIH y de la sífilis en la República Dominicana (Santo Domingo: Centro Nacional de Investigaciones de Salud Materno Infantil, Harvard Global Health Institute, Ministry of Public Health, Consejo Presidencial del Sida, UNICEF, 2011); A. Castro, J. R. Espinoza, M. E. Quintana, et al., Integración de la Atención Prenatal con los Procesos de Detección y Manejo Clínico del VIH y de la Sífilis en Nicaragua (Managua: UNICEF, 2010); A. Castro, “En estado de buena esperanza: Análisis de la experiencia reproductiva en mujeres con VIH en Cuba,” in J. A. Haro (ed), El planteamiento de una epidemiología sociocultural: Un diálogo en torno a su sentido, métodos y alcances (Buenos Aires: Lugar Editorial and El Colegio de Sonora, 2011), pp. 155–168; Ö. Tunçalp, C. Stanton, A. Castro, et al., “Measuring coverage in MNCH: Validating women’s self-report of emergency cesarean sections in Ghana and the Dominican Republic,” PLoS ONE 8/5 (2013), p. e60761; A. Ettenger, T. Bärnighausen, and A. Castro, “Health insurance for the poor decreases access to HIV testing in antenatal care: Evidence of an unintended effect of health insurance reform in Colombia,” Health Policy and Planning 29/3 (2013), pp. 352–358; A. Castro and V. Savage, “Obstetric violence as reproductive governance in the Dominican Republic,” Medical Anthropology 38/2 (2019), pp. 123–136.
[2]. Castro (2004, see note 1).
[3]. A. Castro, “Commentary: Increase in caesarean sections may reflect medical control not women’s choice,” British Medical Journal 319 (1999), pp. 1401–1402.
[4]. Pérez-Then et al. (see note 1).
[5]. Ministry of Public Health of the Dominican Republic, Perfil de la salud materna: ODM 5; República Dominicana (Santo Domingo: Ministry of Public Health, 2013).
[6]. Ibid.
[7]. Ministry of Public Health of the Dominican Republic, Política nacional de sangre (Santo Domingo: Ministry of Public Health, 2014); Guttmacher Institute, Fact Sheet: Abortion in Latin America and the Caribbean (New York: Guttmacher Institute, 2018).
[8]. World Health Organization, World health report: Primary health care now more than ever (Geneva: World Health Organization, 2008); M. P. Fort, D. E. Grembowski, J. C. Verdugo, et al., “Implementation and progress of an inclusive primary health care model in Guatemala: Coverage, quality, and utilization,” Pan American Journal of Public Health 30/3 (2011), pp. 217–224; R. Álvarez Sintes, Medicina general integral (Havana: Editorial Ciencias Médicas, 2008).
[9]. Ministry of Public Health of the Dominican Republic, General directorate of epidemiology weekly bulletins (Santo Domingo: Ministry of Public Health, 2011–2019).
[10]. United Nations Children’s Fund and Tulane University, Health equity report 2016: Analysis of reproductive, maternal, newborn, child, and adolescent health inequities in Latin America and the Caribbean to inform policy making (UNICEF: Panama City, 2016).
[11]. A. Castro, V. Savage, and H. Kaufman, “Assessing equitable care for indigenous and Afrodescendant women in Latin America,” Pan American Journal of Public Health 38/2 (2015), pp. 96–109.
[12]. A. Castro, “Health and inequality,” in H. Callan (ed), The international encyclopedia of anthropology (Hoboken, NJ: Wiley-Blackwell, 2018); Castro et al. (2015, see note 11).
[13]. Bolivarian Republic of Venezuela, Ley orgánica sobre el derecho de las mujeres a una vida libre de violencia (2007).
[14]. V. Savage and A. Castro, “Measuring mistreatment of women during childbirth: A review of terminology and methodological approaches,” Reproductive Health 14/138 (2017), pp. 1–27.
[15]. Castro (1999, see note 3); R. Castro, La vida en la adversidad: El significado de la salud y la reproducción en la pobreza (Cuernavaca: CRIM/UNAM, 2000); R. Castro and J. Erviti, “Violations of reproductive rights during hospital births in Mexico,” Health and Human Rights 7/1 (2003), pp. 90–110; G. Freyermuth, “Antecedentes de Acteal, muerte materna y control natal ¿Genocidio silencioso?,” in R. Hernández (ed), La otra palabra. Mujeres y violencia en Chiapas, antes y después de Acteal (Mexico City: Centro de Investigaciones y Estudios Superiores en Antropología Social, 1998), pp. 63–83; Red por la Salud de las Mujeres del Distrito Federal, Tribunal para la defensa de los derechos reproductivos: Dossier de casos (Mexico City: Red por la Salud de las Mujeres del DF, 1996); C. Rincón, “Violaciones a los derechos reproductivos por parte de las instituciones médicas en México,” in C. Bunch, C. Hinojosa, and N. Reilly (eds), Los derechos de las mujeres son derechos humanos: Crónica de una movilización mundial (Mexico City: Edamex, 2000), pp. 115–118.
[16]. G. Backman, P. Hunt, R. Khosla, et al., “Health systems and the right to health: An assessment of 194 countries,” Lancet 372/9655 (2008), pp. 2047–2085.
[17]. National Congress of the Dominican Republic, Ley No. 24-97 que introduce modificaciones al código penal y al código para la protección de niños, niñas y adolescentes (1997).
[18]. National Congress of the Dominican Republic, Ley 42-01: Ley general de salud (2001).
[19]. National Congress of the Dominican Republic, Ley 136-03: Código para la protección de los derechos de los niños, niñas y adolescentes (2003).
[20]. Government of the Dominican Republic, Constitución Política de la República Dominicana (2015).
[21]. National Congress of the Dominican Republic, Ley 1-12: Estrategia nacional de desarrollo 2030 (2012).
[22]. Ministry of Public Health of the Dominican Republic, Política nacional de calidad en salud (2013); Ministry of Public Health, Reglamento técnico de atención a la mujer durante el embarazo, el parto y el puerperio (Santo Domingo: Ministry of Public Health, 2013).
[23]. Ministry of Public Health of the Dominican Republic, Protocolo de atención para el manejo integral del embarazo, el parto y el puerperio en adolescentes menores de 15 años (Santo Domingo: Ministry of Public Health, 2016).
[24]. P. Bourdieu, “Pour un savoir engagé,” Le Monde Diplomatique (February 2002), p. 3; D. Galeano, L. Trotta, and H. Spinelli, “Juan César García and the Latin American social medicine movement: Notes on a life trajectory,” Salud Colectiva 7/3 (2011), pp. 285–315; E. Granda Ugalde, La salud y la vida, Volumen 1 (Quito: Pan American Health Organization, 2009); J. Breilh, “La epidemiología crítica: Una nueva forma de mirar la salud en el espacio urbano,” Salud Colectiva 6/1 (2010), pp. 83–101; P. Farmer, Pathologies of power: Health, human rights, and the new war on the poor (Berkeley: University of California Press, 2003).
[25]. S. Miller, M. Cordero, A. L. Coleman, et al., “Quality of care in institutionalized deliveries: The paradox of the Dominican Republic,” International Journal of Gynecology and Obstetrics 82/1 (2003), pp. 89–103; J. Ruminjo, C. Cordero, K. J. Beattie, and M. N. Wegner, “Quality of care in labor and delivery: A paradox in the Dominican Republic; Commentary,” International Journal of Gynecology and Obstetrics 82/1 (2003), pp. 115–119; G. La Forgia, R. Levine, A. Díaz, and M. Rathe, “Fend for yourself: Systemic failure in the Dominican health system,” Health Policy 67/2 (2004), pp. 173–186; J. Foster, R. Burgos, C. Tejada, et al., “A community-based participatory research approach to explore community perceptions of the quality of maternal–newborn health services in the Dominican Republic,” Midwifery 26/5 (2010), pp. 504–511; Castro and Savage (2019, see note 1).
[26]. Castro and Savage (2019, see note 1).
[27]. M. Nussbaum, “Adaptive preferences and women’s options,” Economics and Philosophy 17 (2001), pp. 67–88; R. Terlazzo, “Conceptualizing adaptive preferences respectfully: An indirectly substantive account,” Journal of Political Philosophy 24/2 (2016), pp. 206–226; A. Sen, Resources, values and development (Oxford: Basil Blackwell, 1984).
[28]. Castro and Savage (2019, see note 1).
[29]. R. Khosla, C. Zampas, J. P. Vogel, et al., “International human rights and the mistreatment of women during childbirth,” Health and Human Rights Journal 18/2 (2016), pp. 131–143.