Two Row Wampum, Human Rights, and the Elimination of Tuberculosis from High-Incidence Indigenous Communities
Volume 21/1, June 2019, pp 253 – 265
Richard Long, Courtney Heffernan,* Melissa Cardinal-Grant, Amber Lynn, Lori Sparling, Dorilda Piche, Mara Nokohoo, and Diane Janvier
Abstract
The Two Row Wampum belt is a symbolic record of the first agreement between Europeans and American Indians on Turtle Island (North America). The agreement outlined a commitment to friendship and peace between people living perpetually in parallel, with each party recognizing the other as an equal partner. Subsequent treaty relationships between the Indigenous peoples of the Canadian prairies and settler society, along with the colonially imposed structures they spawned, are widely regarded as having broken the Covenant Chain, the foundation of which is Two Row Wampum. For example, the universal right to health, especially public health, as protected by provincial and territorial legislation in Canada, is under threat in Indigenous communities with a high incidence of tuberculosis. The rights of Indigenous peoples have been asserted, and reasserted, in the United Nations Declaration on the Rights of Indigenous Peoples, the Truth and Reconciliation Commission of Canada, the International Patients’ Charter for Tuberculosis Care, and Jordan’s Principle. Herein we describe the implementation of a strategic plan that reinforces human rights and dignity in the spirit of Two Row Wampum in contemporary tuberculosis elimination efforts.
Introduction
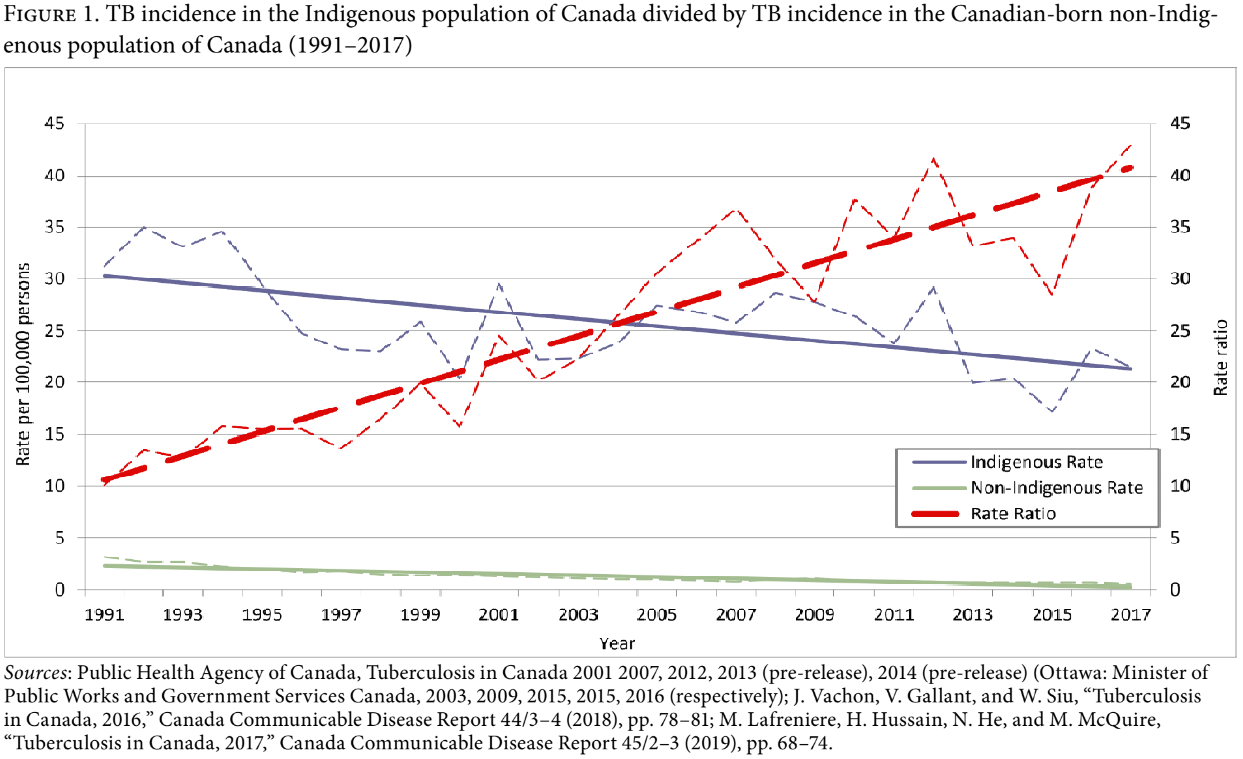
Tuberculosis (TB) is a communicable disease of poverty that exploits conditions of socioeconomic inequity.1 Every country experiences some inequitable distribution of wealth; national, population-specific measures of TB disease reflect this reality. Disparities in the experience of TB disease are perhaps most stark in high-income countries, where resources are available to effect successful TB prevention and care programs. This is borne out in the literature. TB in India, for example, is five times higher among the poorest quintile than the wealthiest.2 Meanwhile, in Canada, a high-income, low-incidence country, TB is concentrated in two underserved populations. While the overall rate of TB in Canada is low (4.9 per 100,000 individuals), among foreign-born persons and Indigenous peoples, which include First Nations, Métis and the Inuit (see below), it remains relatively high, at 14.7 and 21.5 per 100,000 individuals, respectively, compared to 0.5 per 100,000 in the Canadian-born non-Indigenous population.3 This translates into a 29-fold and 43-fold difference in rates, respectively. Most concerning is that for Indigenous peoples, the relative rate of disease has increased over time. This underscores national TB prevention failures (see Figure 1). If what we call “structural violence” is either that which increases the distance or impedes the decrease of the distance between the potential (the incidence of disease in Canadian-born non-Indigenous populations) and the actual (the incidence of disease in Indigenous populations), then with respect to TB and its causes, an act of violence is being experienced by Indigenous peoples in Canada.4
Central to structural violence is the colonization of Indigenous peoples. Writing in the Lancet, Malcolm King et al. grouped colonization, globalization, migration, loss of language and culture, and disconnection from the land as Indigenous-specific social inequities, which, along with classic socioeconomic and connectivity deficits, account for disparate health outcomes.5 Similarly, at the International Symposium on the Social Determinants of Indigenous Health in Adelaide, Australia, in 2007, Indigenous scholar Martin Mowbray opined, “This process [of colonization] continues to impact health and wellbeing and must be remedied if the health disadvantages of Indigenous peoples are to be overcome. One requirement for reversing colonization is self determination, to help restore to Indigenous Peoples control over their lives and destinies.”6 Inter alia, the history of colonization—which in Canada includes the devastating legacy of residential schools—targeted the culture of Indigenous peoples and changed the course of their health for many generations to come.7
Colonization is a process whereby a nation in a position of power imposes culture, values, lifestyle, and political structures on those with less power.8 It has been nearly invariably damaging to the people who experience it, despite motivations that may ostensibly be well intentioned.9 Relationships between original inhabitants and colonizers have historically manifested in a spectrum of power exchanges that depends on the context of a region. For example, in the plantation settings of the West Indies, such as Haiti, the French, having replaced the Spanish, imposed control of the region through oppression and slavery. Conversely, in regions where colonial settlers had less secure means to subsist, they depended on building relationships with local populations in order to survive.10 The latter example is evidenced by an agreement reached between the Haudenosaunee of North America and Dutch traders outlining a mutual, three-part commitment to friendship, and peace between peoples, living in parallel forever. Forever is understood to be “as long as the grass is green, as long as the water flows downhill, and as long as the sun rises in the East and sets in the West.” Symbolizing this agreement is a “Two Row Wampum belt.”
Wampum is a mnemonic device—essentially, a cultural archive. Wampum belts recorded important discussions and agreements between nations, especially pertaining to matters of war and peace. Subsequent to agreements, an Indigenous speaker would remind all parties of the expectations of that agreement by reading the Wampum. This occurs when the Wampum commemorating the pact is held up, and the terms of the understanding between the parties that were recorded on the Wampum “document” are reaffirmed.11 The two rows of the Wampum belt signify Indigenous and non-Indigenous peoples traveling side by side in harmony and health, with neither having jurisdiction over the other.12 Two Row Wampum embodies an unchanging relationship between the Haudenosaunee (Iroquois), other Native nations, and their European partners, beginning with the Dutch, then the English, and later Canadians. Despite promotion in the Royal Commission on Aboriginal Peoples, it is not patently obvious that this Two Row Wampum commitment to mutually beneficial relationships has ever been formally practiced.13
This paper describes a recent project designed to change the delivery of public health, specifically TB programming, in high-incidence First Nations and Métis communities on the Canadian prairies, through the lens of Two Row Wampum. This project illustrates how relations between Indigenous and non-Indigenous Canadians may be renewed on the basis of the principles of respect and reciprocity in the sphere of health. Strategically, this project has forged a new relationship (or revisits the concept of the Two Row Wampum relationship) between governmental stakeholders and communities. This relationship establishes communities as equal partners in decision making to dismantle, figuratively, the colonially rooted jurisdictional boundaries that separate communities and have heretofore confounded TB control. The principles of Two Row Wampum have application to other communities in Canada with high TB incidence. We posit that a return to Two Row Wampum is not literally decolonizing but shines a light on a path that respects dignity and human rights and has the potential to improve health outcomes in the face of preexistent and persistent colonizing practices by settlers against Indigenous Canadians.
Background
Complicating the delivery of health services in Canada are the multitude of responsible jurisdictions, which suffer from limited communication and standardization. Under most circumstances, provinces and territories have legislated authority for health, including TB programming, within their borders. Provincial public health legislation and regulations are “laws of general application” that extend into First Nation reserves. Making this possible is the obligation of First Nations and Inuit Health Branch of Health Canada to provide or make accessible TB services to on-reserve First Nations. Generally, the federal government has a fiduciary responsibility to provide resources and care to reserves and the peoples living therein.14 In more recent years, resources have been shifting to encourage the autonomy of First Nations to provide their own health services; the most established of these transferred organizations is the First Nations Health Authority of British Columbia.15 Finally, territories have the sole responsibility for TB prevention and control for their entire populations, though in recent years they have received considerable financial support from Health Canada.16 Within each province or territory, the provision of TB services is dependent on the priorities, organization, and resources of their governments. 17
Overlaying the contemporary jurisdictional challenges are invisible and historically fraught relationships between the first peoples of Canada and settler society. These relationships are now legacy. Historian J. R. Miller writes:
In the latter part of the 1870s, the government of Canada began to reformulate the basis of its policies towards First Nations. Principal in this realignment was the passage by parliament in the spring of 1876 of the Indian Act, a compendium of all legislation dealing with First Nations. The hard centre of the act was casting the relationship of government and Indians as that between trustee and ward. Under the Indian Act First Nations people were legally children, and their legal parent, the federal government, had the right and responsibility to make decisions on their behalf. The trustee-ward/adult-child relationship embodied in the Indian Act is the antithesis of the kin relationship—brother to brother, sister to sister, under their mutual parent, the Great White Queen Mother (the British monarch at the time, Queen Victoria)—agreed to during treaty negotiations.18
The Inuit were never asked to sign a treaty and were never represented under the Indian Act, in spite of a Supreme Court decision in 1939 stating that “Eskimos [Inuit] were Indians” and thus should be considered wards of the federal government.19 In 1982, an amendment to the Constitution Act of Canada recognized three major groups of Indigenous peoples: First Nations, who may be registered or unregistered with the federal government under the terms of the Indian Act; Métis, self-identified persons of mixed Indigenous and European ancestry; and Inuit, original inhabitants of the far north who are distinct from other Indigenous groups in heritage, language, and culture. Section 35 of the Canadian Constitution provides recognition and affirmation of Indigenous and treaty rights; it constitutionalized treaties and provided them with immunity against legislatures, as well as enhanced the ability of Inuit and First Nations to advance their rights prior to signing a treaty and protect their interests afterward.20
One such interest is comparable health outcomes. TB is a disease of poverty, and elevated rates of TB disease represent an especially evocative disparity between Indigenous and non-Indigenous Canadians, with some First Nations currently experiencing rates of disease rivaling those found in developing nations.21 In 1992, the Medical Services Branch (the forerunner of the First Nations and Inuit Health Branch of Health Canada) released a National Tuberculosis Elimination Strategy.22 In 2012, in the face of sustained high rates of TB in First Nations on-reserve, the strategy was renewed in Health Canada’s Strategy against Tuberculosis for First Nations On-Reserve.23 The renewal was divided into three themes: (1) preventing, diagnosing and managing TB, (2) targeting populations at greatest risk for TB, and (3) developing and maintaining partnerships.
Though the strategy was well intentioned, problems with the themes emerged in the months and years following its release. First, themes one and two were not likely to succeed if theme three failed. Second, on-reserve TB is often linked to off-reserve TB. And third, no steps were taken to see that theme three was implemented, mainly due to a lack of direction. As a way forward, if theme three is about the respectful and meaningful engagement of communities for the purposes of achieving TB elimination, the answer might lie in Two Row Wampum. This arrangement helps bring into the orbit of kin relationship strangers with whom association is desirable. It creates what may be characterized as “imagined communities,” or virtual collectivities fashioned for shared purposes.24 Moreover, Two Row Wampum helps create an intercultural ethical space that transforms the power dynamic underlying public health. Rather than seeing individuals and communities as passive recipients of government benevolence, it recognizes them as rights holders, with human rights imposing corresponding obligations on governmental duty bearers.25 An ethical space between the distinctive rows of the Wampum supports the application of rights-based documents to TB prevention and care. Most existing literature recognizes the importance of community engagement on this and other public health issues but provides little instruction as to how that engagement can be meaningful for all parties or how it respects the rights of Indigenous peoples.26
Our study explored (1) the development of this aforementioned ethical space, (2) the operationalizing of a human rights-based approach, and (3) a participatory mechanism for working across multiple colonially imposed jurisdictional boundaries. We received funding through a signature Canadian Institutes of Health Research initiative titled “Pathways to Health Equity for Aboriginal Peoples.” In the context of this work, we collaborated with four heterogeneous—with respect to geography, designation, and jurisdiction responsible for delivering health care services—communities. What they share in common are their status as predominantly First Nations and Métis populations and their high rates of TB. These major differences and similarities are important for generalizing any results from participation. All communities are connected with one another historically, linguistically (Dene speakers), economically, and culturally. As a result, their jurisdictional separation, both provincially and on-/off-reserve, constitute potential obstacles to TB control. There is no doubt that progress toward TB elimination is required in all communities to obtain sustained success in any one community. What follows is a reflection on the process of engaging the communities to turn inter-jurisdictional challenges associated with TB control into an opportunity for advocacy and community-led collaboration.
Community engagement
Partner communities are located in Northwestern Saskatchewan and Northeastern Alberta (see Figure 2). Each has a sustained high incidence of TB. The weight of ongoing contagion therein was demonstrated by former patients interviewed as part of an earlier study.27 Against this backdrop, we began a two-phase engagement process consisting of a team-building phase and an implementation science phase.28
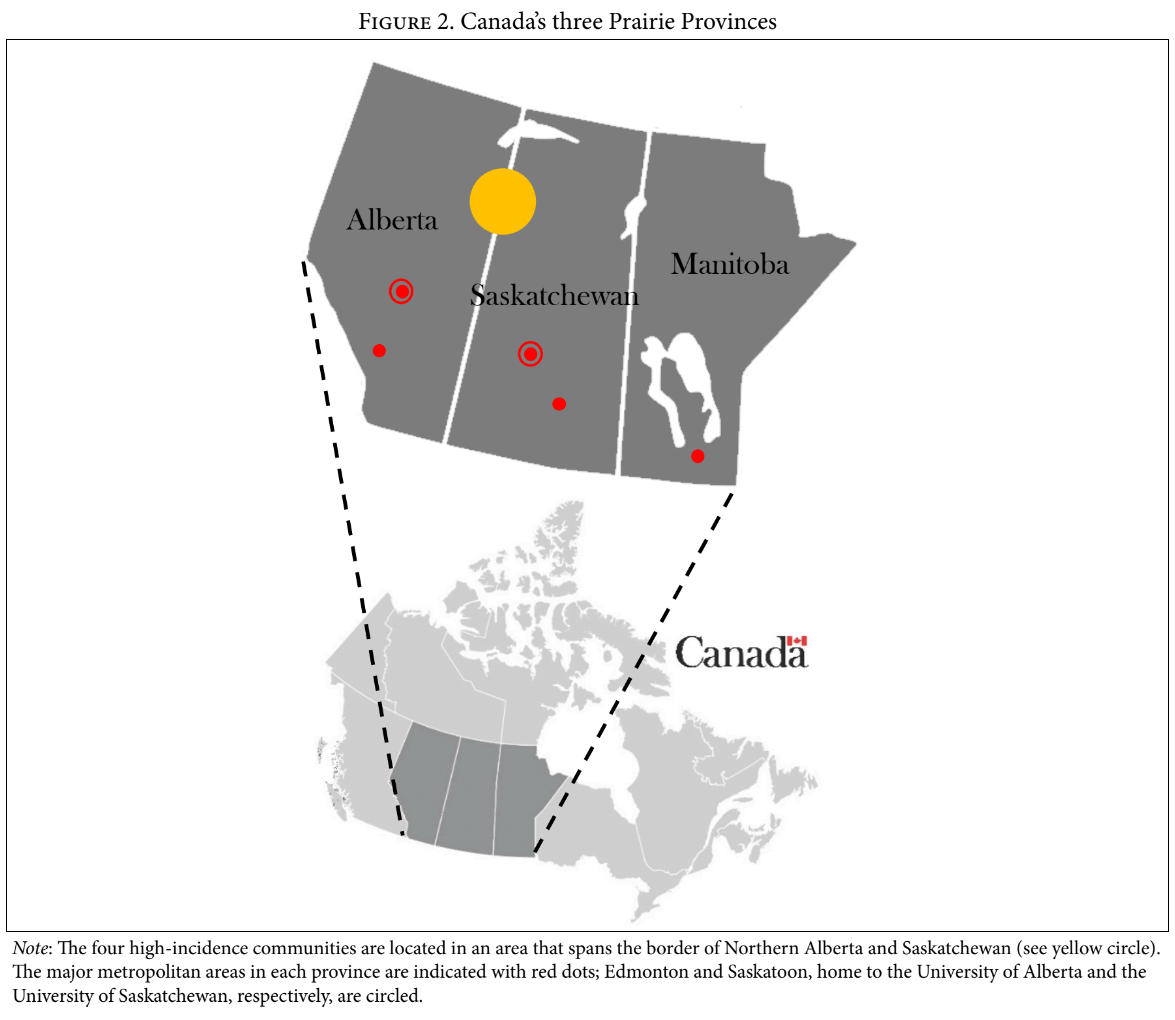
We built a broad coalition of community, government, First Nations and Métis organizations (tribal councils), and other stakeholders, with the scientific team at the University of Alberta and the University of Saskatchewan acting as brokers. By linking all four communities, this coalition builds on real patterns of human mobility and social relationships rather than a patchwork of externally imposed colonial jurisdictions. Among other people, membership includes the health directors from each of the two reserve communities, the community health education and outreach worker in a predominately Métis community, and the Aboriginal liaison worker in an inner city acting as community co-investigators. Teambuilding began with a face-to-face meeting to reach four goals: (1) determining how decisions would be made within the group, (2) initiating a shared “statement of values” from which all discussion and decision making would proceed, (3) identifying community supports and barriers that have ensured or limited the success of prior TB prevention and care efforts, and (4) discussing “tried and true” interventions for the elimination of TB.
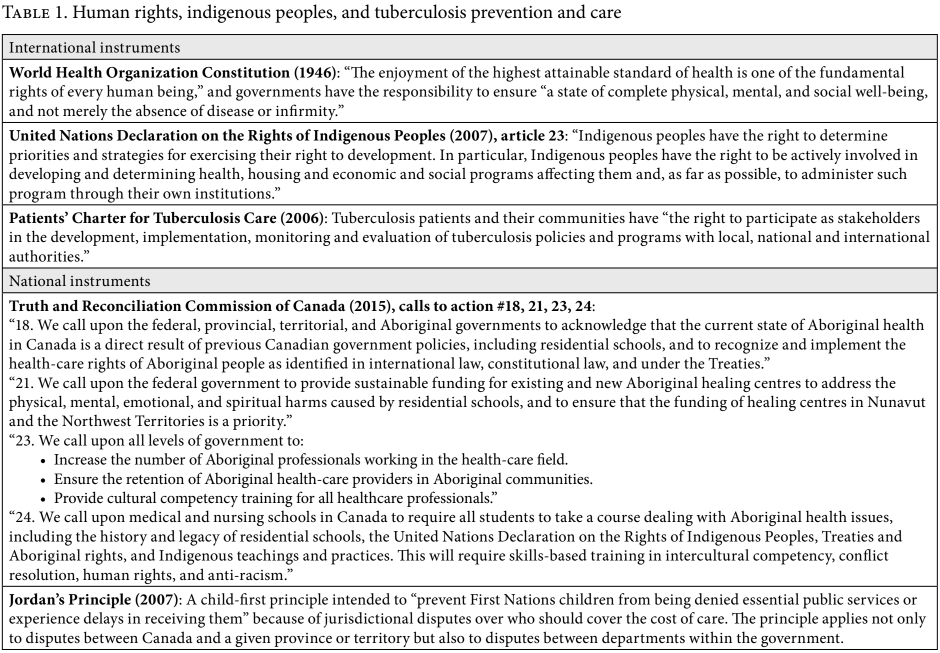
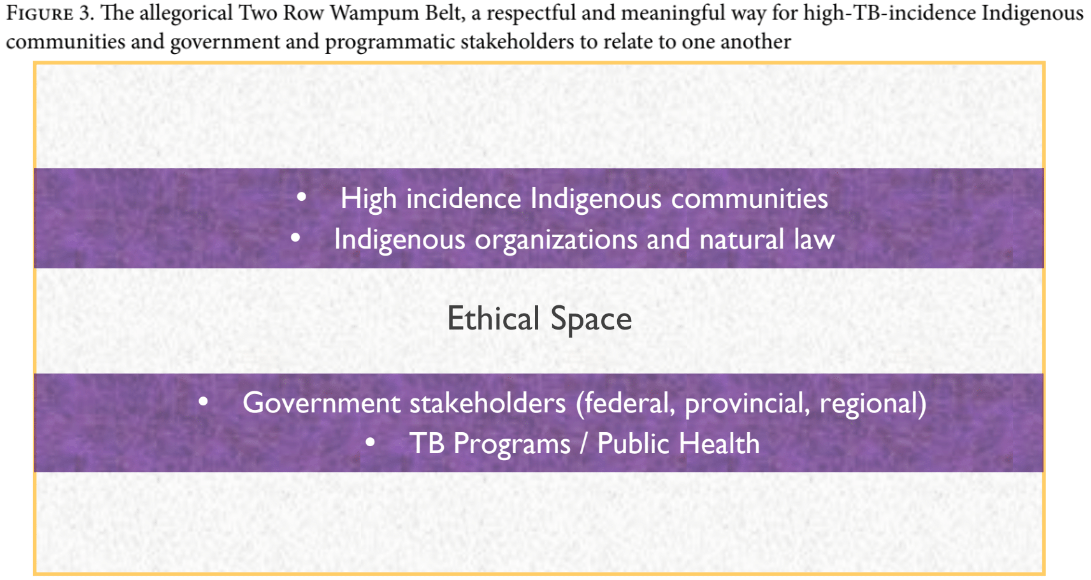
Apropos of the first two goals, we agreed to work together to develop TB programming efforts and interventions with, by, and for Indigenous peoples in their own communities. Decision making within and across communities is by consensus, given the respect accorded to diversity and local autonomy in Indigenous cultures. We routinely speak and share information openly, honestly, and with respect and dignity; no one member or population group presumes to know what harms or enhances the well-being of others. By unanimous decision, we agreed to respect the rights of Indigenous peoples and the corresponding obligations of governments and other key stakeholders as articulated in the Patients’ Charter for Tuberculosis Care, the United Nations Declaration on the Rights of Indigenous Peoples, the Truth and Reconciliation Commission of Canada, and Jordan’s Principle (see Table 1), and to use those rights to hold the deliberations and actions of the coalition to account.29 Present and future assemblage of the coalition occurs within an ethical space, divested of any undercurrent of epistemic racism, where First Nations and Métis collaborators feel safe and free to be themselves. The broad outlines of this space and the narrative defining the coalition is manifest in the concept of Two Row Wampum (see Figure 3).
Apropos of goals three and four, we identified a need to better resource the communities and create committees to represent local interests. Accordingly, out of partnership funds raised by the scientific team, half-time TB workers were recruited from the communities, and they arranged two committees, one on each side of the provincial border. These committees include community co-investigators, TB workers, Elders, former patients, traditional healers, and students. Their role is indefinite and supported in the future by the communities and governments as appropriate. The fourth goal initiated a conversation about possible interventions for phase two of our study, two of which we implemented after consensus agreement. These two local-level interventions were (1) region-specific surveillance and translation of those surveillance data back to the community and (2) an expanded program of outreach that has community wellness as its primary focus.
Surveillance
Up until this point, data has been collected from communities, aggregated, and then used to make decisions centrally at the TB program level. Such aggregate reports obfuscate troubling rates of disease at the community level. Indigenous peoples and communities cannot provide input about solutions they anticipate will be effective if governments and reporting mechanisms serve to maintain ignorance. Our partners want to access data, analyze trends, and advocate for regionally specific strategies against TB. The flow of these data is down. Input about solutions in response to these shared data may spur community-collected and -owned data. Examples include contact tracing successes and failures, barriers to effective case and contact management (for example, substance misuse), and community-preferred strategies to promote education and reduce stigma. In turn, we anticipate that these locally collected data will be shared with trusted TB stakeholders to ultimately improve TB services. The flow of these data is up.
Surveillance as an elimination strategy has been widely promoted in recently released policy documents and peer-reviewed publications, but the concept of bi-directionality—in other words, sharing data between and across communities and in accordance with an Indigenous ethics code (ownership, control, access and possession, or OCAP)—is unprecedented in Canada.30 In addition to allowing communities to respond to surveillance data, increasing their ownership of the epidemiologic narrative is a political act.31 As such, it has the potential to affect not just the delivery of highly specialized services but also the delivery of substantial financial investment in infrastructure and human resources dedicated to community authority and control of health care.
Outreach
Rather than focusing narrowly on the diagnosis and treatment of patients with TB who manage to access care on their own, outreach aims to aggressively find all cases of TB, prevent the disease in those populations at highest risk, and attend to populations and places of highest transmission. Further, since local conceptions of wellness tend to be holistic, in the sense that they seek a balance in the health of the mind, body, and spirit with the health of the community and the land, we designed outreach activities in line with this epistemology. A biosocial approach to TB management uniquely tailored to address at-risk populations should take into account cultural nuances and pervasive stigma. Locally delivered outreach is an ideal framework within which a comprehensive strategy for TB elimination can be implemented.32
This project and its emphasis on partnership relies on the principle of reciprocal learning to effect change. On the one hand, the education of non-Indigenous stakeholders on the fraught history of colonization and its connection to TB, rights-based documents, and OCAP is necessary. On the other hand, local committees are learning about their rights and the fundamentals of TB prevention and care. With these tools in hand, we expect that both groups will respect the expertise the other has to offer to achieve the common goal of TB elimination. For example, respect for different worldviews is a sustainable action through the provision and joint interpretation of bidirectional TB surveillance data. Together, team members undertook OCAP training to facilitate the process of data collection and sharing moving forward.
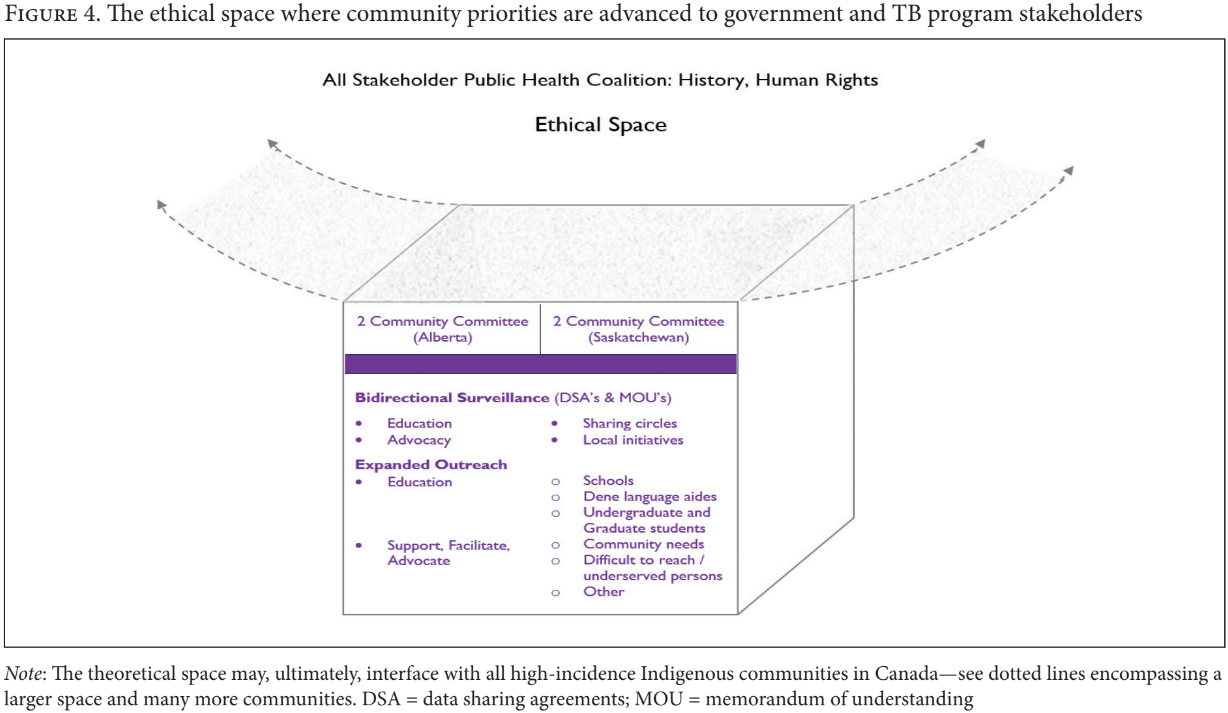
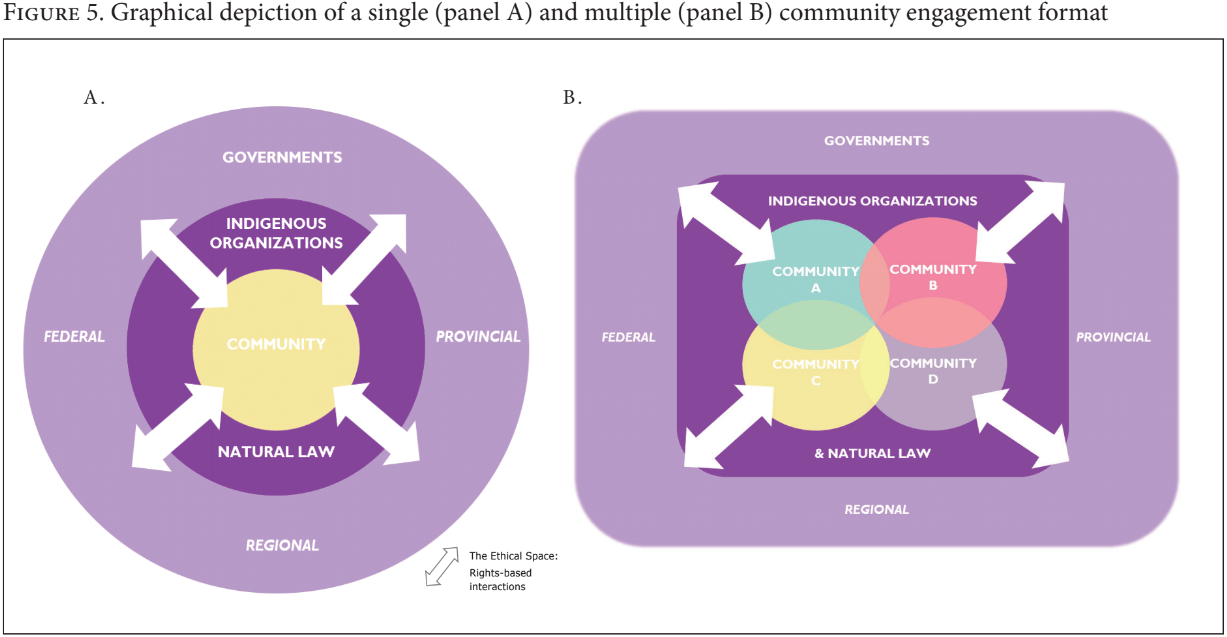
Sustaining the recovery of First Nations and Métis agency within the project and the concept of Two Row Wampum are processes that will eventually fall to programmatic and government stakeholders within the coalition. For example, transforming a system that reinforces social exclusion by marginalizing communities from their data into a system in which communities are fully and centrally involved in decision making will likely not occur within the timelines of a project.33 Therefore, it is overly ambitious to expect to effect substantial change by research teams alone. Moreover, for the concept of Two Row Wampum to be truly transformative, it would need to be scaled up or rippled out to other high-incidence communities or to all Indigenous communities (see Figures 4 and 5).
Discussion
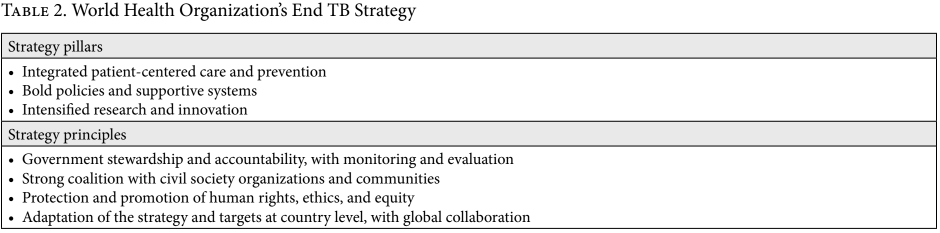
The World Health Organization’s End TB Strategy recognizes the “protection and promotion of human rights, ethics and equity” as one of four principles essential to ending the global TB epidemic, as do we (see Table 2).34 In 2016, the STOP TB Partnership, the International Human Rights Clinic at the University of Chicago Law School, and the Kenya Legal and Ethical Issues Network on HIV and AIDS developed the Nairobi Strategy: A Human Rights-Based Approach to Tuberculosis.35 Of the many components of this strategy, the one that overlaps most closely with our project is the component that aims “to formulate and clarify the conceptual, legal, and normative context of a human rights based approach to TB” in a key population group. It relates directly to the Indigenous-specific social inequities that constitute barriers to better TB outcomes, such as the colonially imposed structures that impede the realization of the right to health. Only indirectly does it relate to the usual catalogue of human rights-related barriers to TB services, such as access to care and the stigma and discrimination related to TB in the community. These strategies all have in common aspirational goals for TB programs, with little direction about how to operationalize rights in their local contexts. We have provided an example herein of how to achieve these goals and why they are critical to TB elimination.
We argue that colonially imposed structural barriers—top-down, paternalistic programming and complex, disconnected jurisdictional systems—serve neither the aspirations of Indigenous peoples for self-expression and self-determination nor the elimination of TB and its upstream determinants. Further, we argue that health, particularly population and public health, of both Indigenous and non-Indigenous peoples, as well as a nation-to-nation vision of relations, requires the creation of an intercultural ethical space where we can achieve parity of thought and power. The structure of this “space” is supported by rights-based approaches to TB programming and care promoted in the Patients’ Charter for Tuberculosis Care, the United Nations Declaration on the Rights of Indigenous Peoples, the calls to action in the Truth and Reconciliation Commission Report, and Jordan’s Principle. We view the space and coalition described herein, as well as the governing processes relating to decision making, as a scalable intervention. Community-specific, local-level interventions are responses to priorities made possible by the advocacy of the coalition and its structure.
In the early twentieth century, savant Albert Schweitzer wrote:
Colonial problems, as they exist today, cannot be solved by political measures alone. A new element must be introduced; white and coloured must meet in an atmosphere of the ethical spirit. Then only will mutual understanding be possible. To work for the creation of that spirit means helping to make the course of world politics rich in blessings for the future.36
More recently, Indigenous scholar and ethicist Willie Ermine saw an “ethical space” as being formed when two societies with disparate worldviews are poised to engage each other, each worldview having been molded by a distinct history, knowledge tradition, philosophy, and social and political reality.37 With respect to population and public health, we see the two (Indigenous and non-Indigenous) as reconciled in such an ethical space.38 This space requires that equality of nations—rather than the pervasive and often unseen non-Indigenous notions of a monoculture—be respected. The equality and the health of nations was intended in Two Row Wampum, but over time and with the process of colonization, its spirit has been quieted but not forgotten.39
These considerations led us to conclude that our research project was as much about the implementation of rights as the implementation of science. Though evidence may support the value of diversity in decision making, the plurality envisaged within Two Row Wampum’s ethical space is about the right to self-determination, as affirmed and reaffirmed in multiple rights pronouncements. In the words of Indigenous scholar Marlene Brant Castellano, “Fundamental to the exercise of self-determination is the right of peoples to construct knowledge in accordance with self-determined definitions of what is real and what is valuable.”40 One of the local-level interventions chosen by our communities, expanded outreach, reflects the importance of comprehensive kinship obligations. It has precedence in Canada.41 The other, surveillance as a strategy, has recognized utility elsewhere, but its bi-directionality is unprecedented in Canada. Bi-directional surveillance might more properly be construed as the implementation of an Indigenous right.42 Given their general application to TB prevention and care, these local-level interventions are also potentially scalable. Our project has called for dialogue and praxis (or the understanding gained through an ongoing cycle of reflection and action) between communities and programmatic and government stakeholders to directly address the question of power and to create a reciprocity in which both parties become “the changer and the changed.”43 As we approach the end of phase two and the need to undertake an evaluation, the scientific team is conscious of the contested power dynamics of the research relationship within a participatory evaluation process.44
We conclude that human rights movements, as they relate to public health and communicable disease in Indigenous communities, are complicated by colonially entrenched structural barriers and sociocultural divides that threaten their application.45 In Canada, this is so despite universal health care and a consistently high ranking in the United Nations Development Programme’s Human Development Index.46 Clearly, the politics of assimilation—relentlessly pursued in Canada through discriminatory practices, treaties, and the residential school system—has failed. Perhaps it is failing globally as the industrial mindset (only a few centuries old) proceeds apace at the expense of respect for the universe, the interconnectedness of all living things, and the virtue of being—Indigenous concepts developed by rich and diverse cultures over many millennia. Herein we affirm the existence of two objectivities, each claiming its own distinct and autonomous worldview. For the health of nations and the elimination of biosocial diseases, we propose the co-creation of an ethical space for dialogue, its placement within the concept of Two Row Wampum, and its linkage to human rights law. Human rights, now so clearly enunciated, are critical to ending structural violence and placing members of both nations on a better path.
Acknowledgments
The authors are very grateful to all of the members of the coalition for the many contributions to the success of this project and to the funding agencies (Canadian Institutes of Health Research, Saskatchewan Health Research Foundation, Alberta Innovates Health Solutions, and the First Nations and Inuit Health Branch, Alberta and Saskatchewan Region) for their generous support.
Funding
Canadian Institutes of Health Research (Grant numbers RN246253-337694 and RN298107-379492), Saskatchewan Health Research Foundation, and Alberta Innovates Health Solutions.
* Richard Long and Courtney Heffernan are joint first authors.
Richard Long is a professor in the Department of Medicine, Faculty of Medicine and Dentistry, and an adjunct professor in the School of Public Health at the University of Alberta, Canada.
Courtney Heffernan is a doctoral student in the Department of Medicine, Faculty of Medicine and Dentistry at the University of Alberta, Canada.
Melissa Cardinal-Grant is a research associate at the Tuberculosis Program Evaluation and Research Unit in the Department of Medicine at the University of Alberta, Canada.
Amber Lynn is a master’s student in the School of Public Health at the University of Alberta, Canada.
Lori Sparling is a health director in a First Nations community in the Province of Saskatchewan, Canada.
Dorilda Piche is a health educator in a Northern Saskatchewan village with a predominantly Métis population, Canada.
Mara Nokohoo is a former health director in a First Nations community in the Province of Alberta, Canada.
Diane Janvier is a health director in a First Nations community in the Province of Alberta, Canada.
Please address correspondence to Richard Long. Email: richard.long@ualberta.ca.
Competing interests: None declared.
Copyright © 2019 Long, Heffernan, Cardinal-Grant, et al. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- K. Lönnroth, E. Jaramillo, B. G. Williams, et al., “Drivers of tuberculosis epidemics: The role of risk factors and social determinants,” Social Science and Medicine 68 (2009), pp. 2240–2246.
- O. Oxlade and M. Murray, “Tuberculosis and poverty: Why are the poor at greater risk in India?” PLoS ONE 7/11 (2012), p.e47533.
- M. Lafreniere, H. Hussain, N. He, and M. McQuire, “Tuberculosis in Canada, 2017,” Canada Communicable Disease Report 45/2–3 (2019), pp. 68–74.
- J. Galtung, “Violence, peace and peace research,” Journal of Peace Research 6 (1969), pp. 168–191; S. Patel, C. Paulsen, C. Heffernan, et al., “Tuberculosis transmission in the Indigenous peoples of the Canadian Prairies,” PLoS One 12/11 (2017), p. e0188189; P. E. Farmer, B. Nizeye, S. Stulac, and S. Keshavjee, “Structural violence and clinical medicine,” PLoS Medicine 3/10 (2006), p. e449.
- M. King, A. Smith, and M. Gracey, “Indigenous health part 2: The underlying causes of the health gap,” Lancet 374 (2009), pp. 76–85.
- Commission on Social Determinants of Health, Social determinants and indigenous health: The international experience and its policy implications; Report on specially prepared documents, presentations and discussion at the international symposium on the social determinants of Indigenous health Adelaide, 29–30 April 2007 (Adelaide: Finders University, 2007).
- F. J. P. Hackett, S. Abonyi, and R. F. Dyck, “Anthropometric indices of First Nations children and youth on first entry to Manitoba/Saskatchewan residential schools—1919 to 1953,” International Journal of Circumpolar Health75/1 (2016); J. S. Milloy, A national crime: The Canadian government and the residential school system, 1879 to 1986 (Winnipeg: University of Manitoba Press, 1999).
- E. I. Daes, “Prologue: The experience of colonization around the world,” in M. A. Battiste (ed), Reclaiming indigenous voice and vision (Vancouver: UBC Press, 2000), pp. 3–8; J. S. Youngblood Henderson, “The context of the state of nature,” in M. A. Battiste (ed), Reclaiming Indigenous voice and vision (Vancouver: UBC Press, 2000), pp. 11–38.
- Youngblood Henderson (see note 8).
- A. M. Carlos and D. L. Frank, Commerce by a frozen sea: Native Americans and the European fur trade (Philadelphia: University of Pennsylvania Press, 2010).
- J. R. Miller, Compact, contract, covenant: Aboriginal treaty-making in Canada (Toronto: University of Toronto Press, 2009).
- J. Parmenter, “The meaning of kaswentha and the two row Wampum belt in Haudenosaunee (Iroquois) history: Can Indigenous oral tradition be reconciled with the documentary record?” Journal of Early American History 3 (2013), pp. 82–109; Chief I. Powless Jr., “Treaty making,” in G. P. Jemison and A. M. Schein (eds), Treaty of Canandaigua 1794–200: Years of treaty relations between the Iroquois confederacy and the United States (Santa Fe: Clear Light Publishers, 2003), pp. 15–34.
- Royal Commission on Aboriginal Peoples, Report of the royal commission on Aboriginal peoples (Ottawa: Canada Communication Group – Publishing, 1996). Available at http://www.bac-lac.gc.ca/eng/discover/aboriginal-heritage/royal-commission-aboriginal-peoples/Pages/final-report.aspx.
- Pan-Canadian Public Health Network, Guidance for tuberculosis prevention and control programs in Canada (Ottawa: Public Health Agency of Canada, 2012). Available at http://www.phn-rsp.ca/pubs/gtbpcp-oppctbc/pdf/Guidance-for-Tuberculosis-Prevention-eng.pdf.
- Tuberculosis Services, Community programming guide: First Nations Health Authority. Available at www.fnha.ca.
- Inuit Tapiriit Kanatami, Inuit tuberculosis elimination framework (Ottawa: Inuit Tapiriit Kanatami, 2018). Available at https://www.itk.ca/wp-content/uploads/2018/12/FINAL-ElectronicEN-Inuit-TB-Elimination-Framework.pdf.
- National Collaborating Centre for Aboriginal Health, The state of knowledge of Aboriginal health: A review of public health in Canada. Available at https://www.ccnsa-nccah.ca/docs/context/RPT-StateKnowledgeReview-EN.pdf.
- Miller (see note 11).
- Reference as to whether “Indians” includes in s. 91 (24) of the B.N.A. Act includes Eskimo in habitants of the Province of Quebec (1939), S.C.R. 104 (1939 CanLII 22 (SCC)).
- The Constitution Act, 1982, Schedule B to the Canada Act 1982 (UK) (1982), c 11.
- R. Long, V. Hoeppner, P. Orr, et al., “Marked disparity in the epidemiology of tuberculosis among Aboriginal peoples on the Canadian Prairies: The challenges and opportunities,” Canadian Respiratory Journal 20 (2013), pp. 223–230.
- Medical Services Branch Working Group on Tuberculosis, National tuberculosis elimination strategy (Ottawa: Medical Services Branch, 1992).
- Health Canada, Health Canada’s strategy against tuberculosis for First Nations on-reserve (Ottawa: Health Canada, 2012). Available at http://publications.gc.ca/collections/collection_2012/sc-hc/H34-245-2012-eng.pdf.
- Miller (see note 11).
- B. M. Meier, D. P. Evans, M. M. Kavanagh, et al., “Human rights in public health: Deepening engagement at a critical time,” Health and Human Rights Journal 20 (2018), pp. 85–91.
- D. Wilson, S. de la Ronde, S. Brascoupé, et al., “Health professionals working with First Nations, Inuit, and Metis consensus guidelines,” Journal of Obstetrics and Gynaecology Canada 35 (2013), pp. 550–558; A. Sisco, “Honoring the katswenta (two row Wampum): A Framework for consultation with Indigenous communities in Canada and Australia,” doctor of philosophy thesis, School of Education, Faculty of Social Sciences, University of Wollongong (2015). Available at https://ro.uow.edu.au/theses/4345; N. Romero-Sandoval, O. Flores-Carrera, M. A. Molina, et al., “DOTS strategy and community participation: An experience in the Ecuadorian Andes,” International Journal of Tuberculosis and Lung Disease 13 (2009), pp. 1569–1571; E. George, T. Mackean, F. Braun, and M. Fisher, “Social determinants of Indigenous health and Indigenous rights in policy: A scoping review and analysis of problem representation,” International Indigenous Policy Journal 10 (2019).
- J. Boffa, M. King, K. McMullin, and R. Long, “A process for the inclusion of Aboriginal people in health research: Lessons from the determinants of TB transmission project,” Social Science and Medicine 72 (2011), pp. 733–738; K. McMullin, S. Abonyi, M. Mayan, et al., “Evoking ‘Old Keyam’ as a response to the disproportionate experience of tuberculosis among Aboriginal peoples of the Canadian Prairies,” Journal of Aboriginal Health 9 (2012), pp. 30–40; S. Abonyi, M. Mayan, K. McMullin, et al., “‘Finally when I started falling down’: Indigenous tuberculosis patient experiences of health and illness on the Canadian Prairies,” International Journal of Indigenous Health 11/2 (2017), pp. 3–23; S. Komarnisky, P. Hackett, C. Heffernan, et al., “‘Years Ago’: Reconciliation and First Nations narratives of tuberculosis in the Canadian Prairie Provinces,” Critical Public Health 26/4 (2016), pp. 381–393; M. Mayan, T. Robinson, R. Gokiert, et al., “Respiratory isolation for tuberculosis: The experience of Indigenous peoples on the Canadian Prairies,” Public Health Action 7/4 (2017), pp. 275–281; M. Mayan, R. Gokiert, T. Robinson, et al., “Community setting as a determinant of health for Indigenous peoples living in the Prairie Provinces of Canada: High rates and advanced presentations of tuberculosis,” International Indigenous Policy Journal International Indigenous Policy Journal 10 (2019).
- S. Theobald, N. Brandes, M. Gyapong, et al., “Implementation research: New imperatives and opportunities in global health,” Lancet 392 (2018), pp. 2214–2228.
- K. Arunagiri, The patients’ charter for tuberculosis care: Patient rights and responsibilities (World Care Council, 2006); United Nations Declaration on the Rights of Indigenous Peoples, G.A. Res. 61/295 (2007); Truth and Reconciliation Commission of Canada, Honouring the truth, reconciling for the future: Summary of the final report of the truth and reconciliation commission of Canada (Ottawa: Truth and Reconciliation Commission of Canada, 2015); Government of Canada, Jordan’s Principle (Ottawa: House of Commons, 2007); World Health Organization, Constitution of the World Health Organization (New York: World Health Organization, 1946).
- G. Theron, H. E. Jenkins, F. Cobelens, et al., “Data for action: Collection and use of local data to end tuberculosis,” Lancet 386 (2015), pp. 2324–2333; K. Lönnroth, G. B. Migliori, I. Abubakar, et al., “Towards tuberculosis elimination: An action framework for low incidence countries,” European Respiratory Journal 45 (2015), pp. 928–952; Health Canada, Summary: Monitoring and performance framework for tuberculosis programs for First Nations on-reserve. Available at https://www.canada.ca/en/health-canada/services/publications/science-research-data/monitoring-performance-framework-tuberculosis-programs-first-nations-reserve-2015.html; B. Schnarch, “Ownership, control, access, and possession (OCAP) or self-determination applied to research: A critical analysis of contemporary First Nations research and some options for First Nations communities,” International Journal of Aboriginal Health 1 (2004), pp. 80–95.
- J. O’Neil, J. Reading, and A. Leader, “Changing the relations of surveillance: The development of a discourse of resistance in Aboriginal epidemiology,” Human Organization 57 (1998), pp. 230–237.
- K. F. Ortblad, J. A. Salomon, T. Bärnighausen, and R. Atun, “Stopping tuberculosis: A biosocial model for sustainable development,” Lancet 386 (2015), pp. 2354–2362.
- J Smylie, A. Lofters, M. Firestone, and P. O’Campo, “Population-based data and community empowerment,” in P. O’Campo and J. R. Dunn (eds), Rethinking social epidemiology: Towards a science of change (Dordrecht: Springer, 2012), pp. 67–92.
- World Health Organization, The end TB strategy (Geneva: World Health Organization, 2015).
- Stop TB Partnership, Kenya Legal and Ethical Issues Network on HIV and AIDS, and University of Chicago School of Law, The Nairobi strategy: A human rights-based approach to tuberculosis (Geneva: Stop TB Partnership, 2016).
- A. Schweitzer, Out of my life and thought (New York: The New American Library of World Literature, 1959).
- W. Ermine, “The Ethical space of engagement,” Indigenous Law Journal 6 (2007), pp. 193–203.
- P. McIntosh, “White privilege: Unpacking the invisible knapsack,” in S. Rothernburg (ed), Race, class and gender in the United States: An integrated study (New York: St Martin’s Press, 1998), pp. 165–168.
- Royal Commission on Aboriginal Peoples (see note 13).
- B. Castellano, “Ethics of aboriginal research,” Journal of Aboriginal Health 1 (2004), pp. 98–114.
- G. G. Alvarez, D. D. VanDyk, S. D. Aaron, et al., “TAIMA (Stop) TB: The impact of a multifaceted TB awareness and door-to-door campaign in residential areas of high risk for TB in Iqaluit, Nunavut,” PLoS ONE 9/7 (2014), p. e100975.
- J. Smylie, I. Anderson, M. Ratima, et al., “Indigenous health performance measurement systems in Canada, Australia, and New Zealand,” Lancet 367 (2006), pp. 2029–2031.
- N. Wallerstein, “Power between evaluator and community: Research relationships within New Mexico’s healthier communities,” Social Science and Medicine 49/1 (1999), pp. 39–53.
- , p. 49.
- B. Citro, E. Lyon, M. Mankad, et al., “Developing a human rights-based approach to tuberculosis,” Health and Human Rights Journal 18 (2016), pp. 1–8; C. Gianella, C. Ugarte-Gil, G. Caro, et al., “TB in vulnerable populations: The case of an Indigenous community in the Peruvian Amazon,” Health and Human Rights Journal 18 (2016), pp. 55–68.
- United Nations Development Programme, Human development indices and indicators: 2018 statistical update (New York: United Nations Development Programme, 2018).