An Assessment of Human Rights-Based Approaches to Health Knowledge, Attitudes, and Practices Among Centers for Disease Control and Prevention Locally Employed Staff
Volume 21/1, June 2019, pp 45 – 47
Izraelle McKinnon, Aun Lor, and Dabney P. Evans
Abstract
Despite the increasing use of human rights-based approaches to health, the Centers for Disease Control and Prevention (CDC) does not routinely train its staff in the use of such approaches as a part of public health practice. We conducted a training needs assessment among CDC locally employed staff working outside of the United States through eight key informant interviews and an online survey from June to December 2015. Key informants revealed an awareness that rights violations negatively affect access to health services and supported implementation of formal training among CDC staff. Most (82%) survey respondents felt that the CDC should do more to address health and human rights issues in its programs, policies, and research. However, 72% of respondents did not feel they had adequate knowledge to address human rights in their work. In particular, 86% of participants had no knowledge of the Siracusa Principles (criteria for human rights restrictions) and only 2% of participants had received any training on international human rights treaties related to the duties of public health professionals. Our findings inform and support the need to design a training on human rights-based approaches to health, focused on the knowledge and skill needs of CDC locally employed staff.
Introduction
The use of international human rights standards, bodies, and mechanisms to further the realization of human rights, known as human rights-based approaches (HRBAs), is one strategy for achieving the highest attainable standard of health for all.1 The civil, cultural, economic, political, and social rights described within human rights documents define the basic societal conditions necessary to achieve health, providing a framework for health policy and programming.2 Human rights documents, therefore, either explicitly or implicitly inform the duties of health professionals.3 For example, the Siracusa Principles are a set of legally agreed-upon guidelines to be followed in situations in which actors, such as health professionals acting on behalf of the state, must restrict human rights and civil liberties to protect the health of the community.4 At times, public health professionals have the authority to use rights-restricting measures to protect population health, particularly in disease control and prevention, and during health emergencies.5
Moreover, HRBAs identify the importance of not just the outcomes of public health practice, but necessary processes for public health practice.6 The World Health Organization (WHO) posits that human rights standards and principles—such as participation, accountability, equality and non-discrimination—can be integrated into all aspects of public health practice, including assessment and analysis, priority setting, program planning and design, implementation, and monitoring and evaluation.7 As a result, HRBAs develop individual and health systems by providing skills and resources to support ethical, sustainable, and improved outcomes. State actors, or duty bearers, in particular are better equipped to meet their obligations to respect, protect, and fulfill the right to health through understanding and utilizing HRBAs.8 Furthermore, human rights instruments, bodies, and mechanisms provide the political power and legal obligations to effect societal conditions by holding duty bearers accountable to their practices and outcomes.9
The need to address inequalities, discriminatory practices, and injustices that obstruct the fulfillment of human rights—including the right to health—provides the foundation for use of HRBAs. General Comment 14 provides an extensive interpretation of the right to health and the manner in which states must engage with that right; it discusses explicitly the nature of human rights as interdependent and interrelated—the violation or fulfillment of one right affecting the ability of individuals to achieve other rights.10 The potential to realize the right to health for all is dependent upon the realization of other social factors which are the underlying determinants of health, including food, housing, safe water and working conditions, and a healthy environment.11 Importantly, public health professionals—because of their role in the investigation of health needs, development of programs, and implementation of policy—play a unique role in impacting health-related human rights.12 An understanding of the relationship between health and human rights and the use of HRBAs among health professionals prevents discriminatory, coercive, or otherwise harmful practices in public health.13
HRBAs training for health professionals has been shown to improve identification of vulnerable groups, their health needs, and underlying conditions necessary for health, as well as attitudes toward stigmatized populations.14 Moreover, HRBAs training can increase awareness among staff of their ethical duties and the potential for their public health practice to impact the human rights of the populations they serve.15 For example, after recognizing a lack of awareness of patients’ rights and provider responsibilities, the Cambodian-German Social Health Protection Programme supported a policy framework to advance and promote patient rights along with operational guidelines, and codes of conduct and ethics.16 Implemented through workshops for ministry officials, providers, and communities, this framework led to increased awareness of patients’ rights, more respectful and professional treatment of patients, greater patient trust in providers, greater use of public clinics, and improved services in 90% of public health facilities. Other examples further demonstrate the potential power of increased awareness and knowledge of HRBAs among health care professionals to increase the availability, accessibility, acceptability, and quality of health services.17
In 1993, the World Conference on Human Rights included “Education in Human Rights” as a priority area in the Vienna Declaration and Programme of Action, calling for governments to take an active role in promoting human rights education, and addressing the health profession as a special group for participation in education.18 In 1998, the South African Truth and Reconciliation Commission recommended that training in knowledge, skills, and attitudes related to human rights must be a fundamental part of curricula for health professionals, as well as a part of their continuing education.19 WHO, as well as the United Nations Office of the High Commissioner for Human Rights, also promotes training in HRBAs among health professionals, and have released guidance on the use of HRBA to address specific health outcomes, including maternal morbidity and mortality, HIV/AIDS, and tobacco control.20 Public health professionals have advocated for training programs and curricula specific to different types of health professionals and health outcomes — and at times they have been developed and implemented.21 As of 2009, about one-third of schools of public health and medicine in the US provided some form of human rights education, with 22% offering required or elective courses.22 As of 2019, 38 courses appear in an online database of academic courses on health and human rights as interest in the area has grown since the introduction of such courses.23
Operationalizing health objectives that are consistent with human rights is just one means of using HRBAs to promote health equity and sustainable health outcomes.24 Training health professionals is a necessary step in the realization of this approach. Creating such a training first requires the identification of HRBA knowledge, attitude, and skill objectives and competencies.25 Potential knowledge competencies could include the identification of vulnerable groups or legislation pertaining to health; potential attitude competencies could include awareness of one’s own inherent prejudices or biases; and potential skill objectives could include the ability to recognize, report or respond to human rights violations.26 Previous research has shown that appropriate training on HRBAs methods for health include: 1) experiential learning techniques which promote critical thinking about locally relevant health and human rights issues (case studies, debates, site visits, etc.); 2) trainers who have a range of domestic and international experiences in approaching health using a human rights framework; and 3) objectives and teaching methods with practical application to the current and future work of trainees.27
As the United States’ lead public health agency, the Centers for Disease Control and Prevention (CDC) conducts and supports health promotion, prevention, and preparedness activities with the goal of improving population health.28 As a reflection of the CDC’s mission to preserve the health of US citizens, the agency engages in surveillance, population-based surveys, program monitoring and evaluation, laboratory science, and public health emergency response, among other activities.29 With more than 12,000 employees working in over 120 countries, the CDC is made up of multi-disciplinary teams of public health advisors and analysts, laboratory scientists, epidemiologists, health scientists, behavioral scientists, economists, statisticians, and medical and nurse officers.30 Given that disease and health conditions know no borders, the CDC employs locally employed (LE) staff in offices overseas.31 LE staff are experienced public health professionals, as well as citizens or residents of the countries in which they work, offering a valuable contribution to CDC’s global health activities.32
Despite this, the CDC does not currently have a regular training curriculum on the use of HRBAs to health. There is a longstanding history of health and human rights-related interest and activities at the CDC; the late Jonathan Mann, considered the father of the health and human rights movement spent his early career at the CDC. In 1997, the CDC’s National Center for HIV, STD, and TB Prevention (NCHSTP) created the first Health and Human Rights Workgroup (HHRW), though the group dissolved in 1998.33 A new HHRW was founded in 2001, initially in the Epidemiology Program Office, and later expanded CDC-wide, becoming an officially recognized science workgroup in 2003. HHRW includes more than 185 members representing every center, institute, and office (CIO) of the CDC. Through its work and collaborations, HHRW seeks to incorporate HRBAs into public health practice through seminars, workshops, and symposia. Despite these efforts, a formal training gap continues to exist among CDC staff.
Training needs assessments are an essential component of making an evidence-based determination of knowledge and skill gaps, desired educational components of a curriculum, and primarily, whether a formal training is appropriate for potential trainee populations.34 Such assessments are particularly important for adult-learners, as their work interests and skill needs should determine training objectives.35 The purpose of this project was to conduct a HRBAs training needs assessment among CDC LE staff. The objectives of the needs assessment were to determine the following: 1) the desire for training in HRBAs to health; 2) the need for training in HRBAs to health; 3) the necessary objectives to include in HRBAs training; and 4) the types of trainers and appropriate methods to include in HRBAs training. These data will inform the development of a HRBAs training for LE staff; the goal of the training would be increased capacity in using HRBAs as part of ongoing CDC health promotion and disease prevention efforts.
Methods
We conducted key informant interviews (KIIs) in June 2015 of staff members attending an annual CDC Center for Global Health regional training in Atlanta, Georgia; the target audience for the KIIs were supervisors of locally employed staff working in CDC country offices. We structured questions to assess HRBAs to health training needs among the key informants (KIs) as well as their staff. We also administered a web-based knowledge, attitudes, and practices (KAP) survey to CDC staff from June to December 2015.
Target population
Locally employed (LE) staff are employees of CDC working in country office in locations outside of the United States; they are typically citizens or residents of the countries in which they work. This includes locations in sub-Saharan Africa, Southeast Asia, Latin America, and the Caribbean.36 There are approximately 1,500 LE staff in more than 60 countries worldwide, many of whom liaise with key stakeholders such as the Ministry of Health in their country.37 They work closely with the populations they serve, often focusing on populations vulnerable to health concerns.
Tools
We conducted a literature review focused on HRBAs training, concepts, and methods. Informed by the literature review, we developed an original HRBAs to health KII guide; we also adapted existing survey instruments for use in quantitative data collection.38 We designed the study tools in collaboration with members of the CDC’s HHRW, and subject matter experts in public health, human rights, training/curriculum development, and adult education reviewed both instruments.
The semi-structured KII guide included ten open-ended questions. Domains for exploration included personal experiences in public health and HRBAs to health, as well as perceptions of LE staff experience with the same topics. Preferred training methods were a third domain of inquiry.
The 35-question KAP survey included three parts. The first part collected demographic and work experience information, including gender identity, age, country of origin, race/ethnicity, education, position, and years working at CDC. The second part included items on HRBAs knowledge, attitudes, and practices. The third part consisted of five questions on preferred training methods, including educational methods (lecture, case study, problem solving), types of trainers (local/international public health experts, local/international human rights experts, local/international HRBAs experts), and public health topics (emergency preparedness and response, influenza, malaria).
Data collection procedures
We conducted KIIs on June 9 and 10, 2015. We recruited LE staff in supervisory roles at an annual regional training. KIs gave verbal consent to be interviewed and recorded. We conducted interviews until saturation.39
We distributed the KAP survey to staff via the internal CDC Global Health Community listserv—a list of all CDC staff who work in global health. One week later, we disseminated the KAP survey via the CDC Today Announcements, a listserv to which all CDC staff are subscribed. The KAP survey was open from September 1, 2015 to December 31, 2015. On October 28, 2015, we sent reminders through the same listservs. The KAP survey took approximately 10–15 minutes to complete.
Data analysis
The KIIs were transcribed verbatim and coded in MAXQDA 11.40
We extracted KAP survey data from Survey Monkey into an Excel spreadsheet and imported the data into SAS 9.4 statistical software.41 Although data were collected for all CDC staff, we only analyzed data for LE staff. We conducted univariate analyses to measure frequencies and percentages. We collapsed knowledge variables from a 4-point scale (“trained,” “have read about,” “have heard about,” and “no knowledge”) to a 3-point scale with the categories of “trained,” “limited knowledge,” and “no knowledge.”
Ethical considerations
This project was reviewed in accordance with CDC human subjects review procedures and was determined to be a non-research activity. The Emory University Institutional Review Board also reviewed this project and found it to be exempt from human subject review. Nevertheless, ethical standards were maintained throughout the study process including informed consent and confidentiality.
Results
Key informant interviews
Eight staff members participated in the interviews, which lasted from 12 to 24 minutes. Three KIs were working in Asia and five in Africa. Seven worked in the Division of Global HIV/AIDS and TB, and one KI worked in the Global Immunization Division. There were no apparent differences between responses from those working in Africa or Asia; informants from both regions expressing similar attitudes toward training, training needs, and training method preferences. Five themes emerged inductively from the KIIs: 1) human rights violations impact access to health services, 2) there is a lack of knowledge of HRBAs, 3) there is a need for HRBAs training, 4) there is a preference for interactive training methods, and 5) a combination of facilitator types is most desirable.
All KIs were able to identify instances in their work where violations of human rights impacted health. Much of this surrounded discrimination experienced by vulnerable groups overseas, including sexual minorities, sex workers, injection drug users, criminals, and those living in remote areas. One KI elaborated upon the attitudes of people working in the health facilities for which he is responsible, paraphrasing such interactions in the following way:
“Hey, this guy is gay, he’s got HIV, so why should we treat him? He’s suffering for his sins, so leave him alone. And we don’t even have enough to take care of people who are considered normal citizens. Why should we waste our money on this?” And we have to tell them that’s not the point. The issue is that they are humans. They have the right to health, and they are the ones that are affected. So we need to treat them.
KIs were able to verbalize the ways in which a lack of human rights, specifically those related to discrimination, could lead to a lack of access to health services. However, when asked the extent of their knowledge in HRBAs, five of the eight informants answered with some version of “no idea” or “not much.” Two revealed a limited amount of knowledge, which they had gained through reading or partnering with human rights and advocacy groups. However, neither of these two felt they had “sufficient knowledge” to overcome service provision obstructions in the face of human rights violations, or to incorporate HRBAs into their health work. One KI articulated the knowledge level of most KIs:
More and more, given the work that we do on HIV/AIDS with our local partners, we become aware of the areas, of arenas, where human rights clearly has a role in it, you know. But me personally, I have to admit that I’ve not always known what to do with that.
All KIs expressed the feeling that their staff did not have knowledge in HRBAs. Informants also acknowledged that rights violations can interfere with the work of their staff in ways that neither informants nor their staff are equipped to address. One KI revealed, “They come back and talk to me, and there’s nothing I can do for them in some ways.”
Regardless of their knowledge levels, all KIs verbalized a desire for training in HRBAs. KIs expressed the need for general knowledge in human rights in order to know what to look for, and to know what their responsibilities may be. Informants felt they were unable to ensure human rights if they didn’t have this knowledge. Some wanted the ability to communicate using human rights frameworks. They wanted to understand not only the language of human rights, but how to speak about and promote human rights in a non-confrontational manner with people of varying perspectives, including political leaders. One KI pointed to the need to evaluate programs in order to know that they are reaching all groups, including vulnerable groups. Others expressed the desire to know which entities and organizations to reach out to or direct problems. One KI explained the potential benefits of training on HRBAs:
Well, I think it would, at the very least, awaken me to recognize where there may be insufficient human rights in a particular…in a sector where I am working at. It may awaken me to see where [there] are gaps and help me to develop the programs and the strategies to hopefully be able to bridge those gaps…and eventually some implementation of practice to respect people’s rights, to design systems in ways in which we do not victimize people because of their differences, because of their orientation, or whatever the case may be.
Whether for themselves as leaders and advisors, or for their staff as implementers, KIs expressed a strong interest in HRBAs training.
Consistent with adult learning theory, all KIs expressed the need for interactive training methods.42 They recommended case studies, problem solving, and role play—all of which allow for a hands-on learning experience. Informants wanted to share experiences and lessons as part of the interactive learning process.
Along with an interactive learning environment, KIs also wanted to leave with practical skills that they could apply to their work. As one informant expressed, “Adult learning is not the volume of information you pour in. It’s to make it more practical and what they can relate to and apply.”
Some KIs expressed interest in engagement with human rights actors themselves, as well as people who have experienced human rights abuses that have affected their health. Two informants also expressed the desire for the training to take place within their country. This would save resources for those coming from low-income areas, and allow facilitators “to actually see what we are dealing with; to see some of the challenges we are dealing with, some of the dynamics that we, I don’t know, whether they be power dynamics, whether they be dynamics that revolve around economics…some of the cultural realities.”
Overall, KIs saw the value in having varied types of facilitators. They felt that international experts were the most equipped to offer best practices occurring in other settings, as well as a broader perspective on the concepts related to HRBAs. Two informants did stress, however, that there should not be a US-focus. KIs felt that local experts have more knowledge of the context and experience in the overseas setting. Local experts were seen as more important if there was a language barrier in a training audience with low English language proficiency.
Knowledge, attitudes, and practices survey
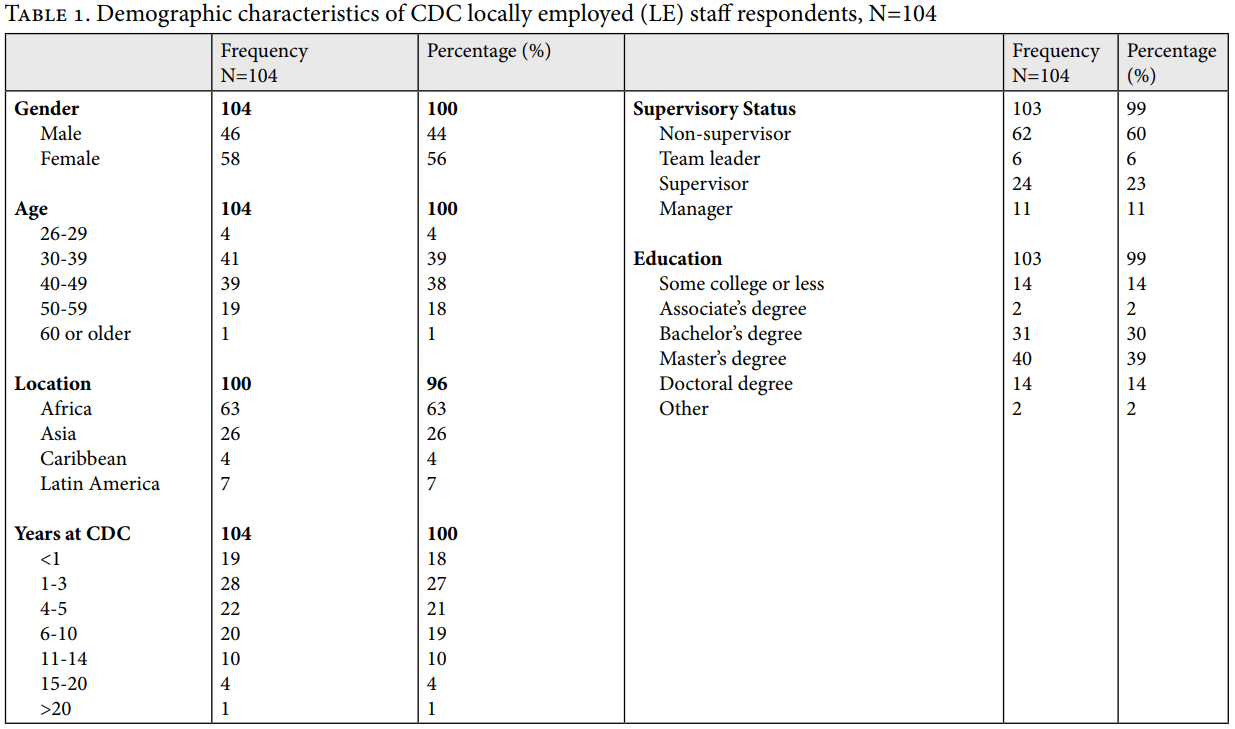
Of approximately 1,465 LE staff members, 104 took part in the KAP survey (7% response rate). Sixty-three percent (63%) of the respondents worked in Africa, 26% worked in Asia, and the remainder worked in Latin America and the Caribbean (LAC) (11%) (Table 1). A slight majority of respondents were female (56%) and ranged in age from 30 to 49 years old (77%). Most of the respondents were not in a supervisory role (60%). The majority of respondents had advanced degrees, such as a bachelor’s (30%), master’s (39%), or doctoral degree (14%). Two-thirds (66%) had worked at CDC country offices for five years or less.
Less than 6% of LE staff respondents were trained on any of the six HRBAs knowledge indicators included in the KAP survey. No LE staff had any training on the Siracusa Principles; 14% had limited knowledge, and 86% had no knowledge. In all other categories, most LE staff reported having “limited knowledge,” including the concept of progressive realization (64%) and the connection between international human rights treaties in relation to duties of public health professionals (65%). Most (80%) had limited knowledge of HRBAs for the protection of populations, and of the underlying determinants of health (82%). On using a HRBAs approach to health planning, implementation, and monitoring, 75% had limited knowledge (See Table 2).
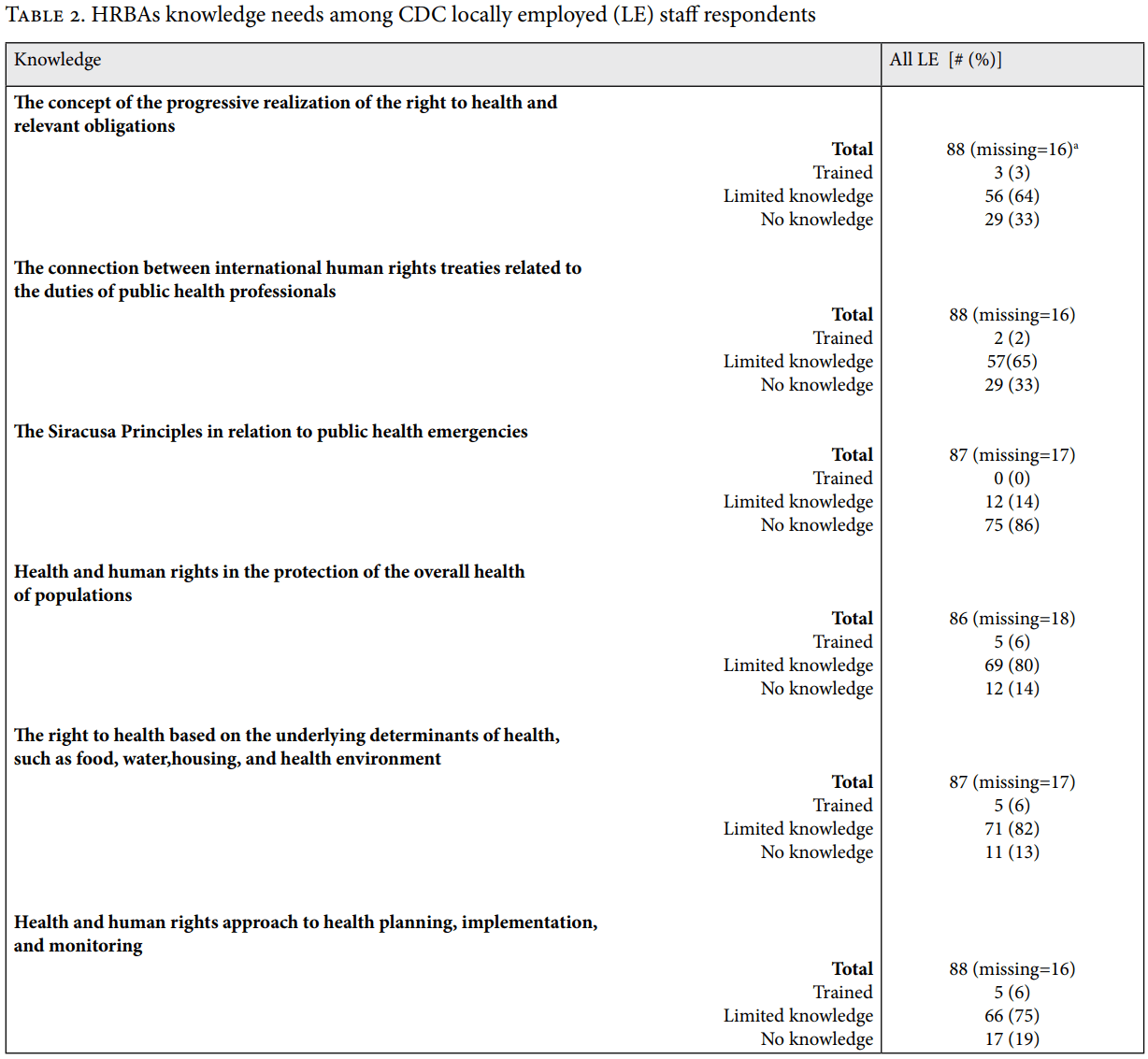
- ‘Missing’ refers to respondents who did not answer the question. All questions other than LE staff status were optional.
We determined interest in a HRBAs training through two attitude indicators. Overall, 86% of LE staff felt that public health could benefit from incorporating a HRBAs framework into programs, policies, and research. Additionally, 82% of LE staff felt that CDC should do more to address human rights issues in its programs, policies, and research.
We asked respondents to consider their current skills in HRBAs to health. Overwhelmingly, respondents felt that they were unable to develop programs using HRBAs (90%). On the other hand, most LE staff felt that they were able to identify human rights violations with 53% of LE staff claiming to have this skill. Among the other HRBAs skills presented, 75% of LE staff did not know how to communicate human rights violations and 82% of LE staff did not know how to use data to promote health using HRBAs.
Many (42%) respondents preferred a combination of training methods (lecture, case study, problem solving, workshop, webinar series). Overall, respondents preferred trainers who are experts in HRBAs to health as opposed to experts in public health or in human rights alone. Forty-nine percent (49%) of respondents preferred local HRBAs experts, while 55% preferred international HRBAss experts. Respondents also identified particular content areas of interest. Most frequently, they had an interest in HIV/AIDS as a topic within a HRBAs training more than any other topic (54%). There was also a preference for training in Emergency Preparedness, with 42% of respondents indicating interest in this topic.
Limitations
There are important limitations to this study. We created the KAP survey instrument based on HRBA literature and feedback from experts in public health, human rights, training/curriculum development, and adult education. We did not test the KAP survey for validity or reliability. Moreover, the KAP survey did not capture prioritization of human rights issues that respondents were particularly interested in. We wrote and conducted the KAP survey and KII in English, which may not have been the first language of the LE staff; however, all KII participants indicated their willingness to be interviewed in English.
We used convenience sampling for both the KII and the KAP survey. There are likely systematic biases affecting the results of both the interviews and the KAP survey as a result of these non-probability sampling methods. In particular, those who participated in this study may be inherently different from those who did not participate. Since our sample selection likely does not accurately reflect the target population, the assessment is not generalizable to all CDC LE staff. We had a low response rate for the KAP survey, affecting the internal and external validity of our results. Despite these limitations to the quantitative data, the rich content of the KII—where saturation was reached—supports much of the KAP survey findings. Lessons learned may be helpful for addressing training needs of health professionals, including at other federal agencies.
Seven of the eight KIs worked in the Division of Global HIV/AIDS and TB; over half of KAP survey respondents expressed interest in HIV/AIDS as a topic area of a HRBA to health training. While most CDC LE staff work on HIV/AIDS, our results may overemphasize an interest in this topic and miss the interests of staff working with other areas.
While time has passed since these data were collected in 2015, no significant changes have taken place in terms of CDC efforts to address HRBAs to health learning needs, indicating that the data likely still hold true.
Discussion
KIs felt that while human rights violations have affected processes and outcomes related to their work, neither they nor their staff had the capacity to address these violations. They responded definitively that their work and that of their staff would benefit from a HRBAs training. Even those KIs who did express having more exposure to HRBAs felt they needed a better understanding. Most KAP survey respondents reported a lack of HRBAs knowledge or skills and very few had received HRBAs-related training in their duties as public health professionals. The majority of respondents believed that public health and the CDC could benefit from incorporating HRBAs into programs, policies, and research. HRBAs training needs included being able to communicate human rights violations, promote human rights, and create programs which uphold human rights for all. Respondents identified several needed skills, including the ability to a) develop and evaluate programs for rights-related impacts and b) use data to promote human rights.
The widespread lack of knowledge of the Siracusa Principles is another important finding. The Siracusa Principles specify conditions that public health professionals should consider before enacting rights restricting measures, as well as conditions that must be maintained in disease control and public health emergencies.43 An understanding of these principles and other relevant human rights standards is instrumental to ensuring that restrictive public health intervention is justified, necessary, non-discriminatory, and the least restrictive possible to achieve the goal of curbing serious threats to the health of populations and individuals. KAP survey respondents noted Emergency Preparedness and Response as a preferred training topic area, reinforcing the need for training in the Siracusa Principles.
In terms of educational methods, KIs made abundantly clear the need for an interactive, cooperative learning environment. In this environment, trainees experience the use of hands-on activities such as case studies, problem solving, and role playing to build practical skills which staff members can apply to their work, and which fits their context and content area. They also encouraged the sharing of ideas and expertise among training participants. These preferences are consistent with Knowles’ theory of andragogy, including principles of: participation, use of learner experiences, practical activities, and immediate applicability.44 KAP survey respondents showed a preference for a combination of educational techniques.
Both KIs and KAP survey respondents preferred HRBAs to health experts versus experts in human rights or public health alone. KIs expressed an interest in local experts for their ability to provide context-specific knowledge and experience while international experts were believed to provide a broader perspective on ways to engage in HRBAs. To our knowledge, this is the first time that a needs assessment in this topic area has been conducted among this population. Other needs assessments in HRBAs training have focused on other populations and some in specific contexts or human rights areas.45 KIs vocalized the extent to which failures in human rights protections can affect their processes and outcomes, yet, as echoed by KAP survey respondents, there is a lack of capacity among CDC LE staff to address health related human rights concerns. Based on the strong appeals for a HRBAs training among both KIs and KAP survey respondents, as well as the evidence of limited knowledge in this area, we recommend the development and systematic implementation of a HRBAs training for CDC LE staff. This training has the potential to develop LE staff capacity for use of HRBAs as part of ongoing CDC health promotion and disease prevention efforts.
CDC leadership and academics can partner to develop HRBAs training for CDC employees based on the results of this needs assessment. The overall goals of such a training would include 1) filling HRBAs knowledge gaps by increasing knowledge of human rights standards, bodies, and mechanisms, and 2) filling HRBAs skill gaps by increasing competency in implementation of HRBAs in reporting, policy, and/or programmatic actions. Examples of knowledge competencies include identifying international human rights treaties and standards and examining how these are related to the duties of public health professionals, and interpreting the Siracusa Principles and applying their use in public health emergencies. Example skill competencies would include developing a program using a HRBA to health, conducting a human rights impact assessment for a proposed public health program, and evaluating a health program’s impacts on human rights. Trainings would use case studies and other interactive methods that allow for information exchange and discussion of local context-based issues and needs. Case studies would cover health topics such as HIV/AIDS and Emergency Preparedness and Response. Moreover, both local and international HRBAs to health experts will be involved in the development and implementation of trainings in order to provide a combination of broad perspective and best practices along with a context-specific focus. The primary function of this initial training would be to increase awareness of HRBAs among trainees; while increased awareness of HRBAs has been found to improve health practices and services, we acknowledge that information is necessary but not sufficient.46 This training provides a starting position to begin the use of HRBAs to health among CDC LE staff. Further training would likely be necessary to ensure the effective application of HRBAs for the protection and promotion of human rights.
In collaboration with the CDC’s Center for Global Health, we hope to pilot such a training at existing CDC regional trainings which occur quarterly across Asia, Africa, and the Americas. Regional trainings are primarily targeted towards LE staff working in various CDC country offices. Next steps to advance this effort include 1) a review of existing courses and curricula relevant to the LE audience; 2) the development of a HRBA to health syllabus and learning modules for CDC LE staff; 3) resource allocation to pilot and evaluate the HRBA training at CDC regional trainings; 4) adaptation to the curriculum based on evaluation feedback; and 5) systematic rollout and scale-up of the HRBA training if proven successful.
Conclusion
The objectives of the needs assessment were to determine the following: 1) the desire for training in HRBAs to health, 2) the need for training in HRBAs to health, 3) the necessary objectives to include in HRBAs training, and 4) the types of trainers and appropriate methods to include in HRBAs training. Based on the combined results of the KII and KAP survey, we determined that CDC LE staff desire HRBAs training in order to benefit their work as health professionals. There are also HRBAs knowledge and skill gaps which indicate the need for training. Therefore, we recommend the creation and implementation of HRBAs training for LE staff. Training topics should include HIV/AIDS, Emergency Preparedness and Response, and potentially others. The training of LE staff should utilize a combination of interactive, cooperative learning measures, and a combination of local and international HHR experts. Advancing these efforts contributes towards increased health workforce capacity for the use of HRBAs as part of ongoing CDC health promotion and disease prevention efforts.
Izraelle McKinnon, MPH, is a PhD student in Epidemiology at Emory University, Atlanta, GA, USA.
Aun Lor, MPH, MA, PhD, is Deputy Associate Director for Science in the Center for Global Health at the US Centers for Disease Control and Prevention, Atlanta, GA, USA.
Dabney P. Evans, PhD, MPH, is an Associate Professor in the Hubert Department of Global Health and Executive Director of the Institute of Human Rights at Emory University, Atlanta, GA, USA.
Please address correspondence to Dabney P. Evans. Email: devan01@emory.edu.
Competing interests: None declared.
Copyright © 2019 McKinnon, Lor, and Evans. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestHRBAricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited. AL was an employee of the US Federal Government when this work was conducted and prepared for publication; therefore, it is not protected by the Copyright Act.
Disclaimer: The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
- WHO, A human rights based approach to health. Available at https://www.who.int/hhr/news/hrba_to_health2.pdf.
- J. M. Mann, L. Gostin, S. Gruskin et al., “Health and human rights,” Health and Human Rights (1994), 6-23.
- J. Mann, “Health and human rights: If not now, when?,” Health and Human Rights (1997), 113-120.
- Siracusa principles on the limitation and derogation provisions in the international covenant on civil and political rights, E/CN.4/1985/4 (1985). Available at https://www.refworld.org/docid/4672bc122.html.
- WHO, International health regulations (2005). Available at https://www.who.int/ihr/publications/9789241580496/en/.
- E. Beracochea, C. Weinstein, and D. Evans, Rights-based approaches to public health, (Springer Publishing Company, 2010).
- WHO, A human rights based approach to health. Available at https://www.who.int/hhr/news/hrba_to_health2.pdf.
- General comment no. 14: The right to the highest attainable standard of health, E/C.12/2000/4 (2000). Available at https://www.refworld.org/docid/4538838d0.html.
- P. Braveman and S. Gruskin, “Poverty, equity, human rights and health,” Bulletin of the World Health Organization 81/7 (2003), 539-545.
- Fact sheet no. 31: The right to health 31 (2008). Available at https://www.refworld.org/docid/48625a742.html.
- General comment 14, the right to the highest attainable standard of health, E/C.12/2000/4 (2000). Available at https://www.refworld.org/docid/4538838d0.html.
- Braveman (2003, See note 9).
- J. M. Mann, L. Gostin, S. Gruskin et al., “Health and human rights,” Health and Human Rights (1994), 6-23.
- WHO, Human rights and health. Available at https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health.
- S. Glowa-Kollisch, J. Graves, N. Dickey et al., “Data-driven human rights: Using dual loyalty trainings to promote the care of vulnerable patients in jail,” Health Human Rights 17/1 (2015), E124-E35.
- T. Silberhorn, “Germany’s experience in supporting and implementing human rights-based approaches to health, plus challenges and successes in demonstrating impact on health outcomes,” Health and Human Rights 17/2 (2015), 21-29.
- M.-L. Escobar, L. Cubillos, and R. Iunes, “Looking for evidence of the impact of introducing a human rights-based approach in health: The saluderecho experience,” Health & Human Rights: An International Journal 17/2 (2015).
- Vienna declaration and programme of action, A/CONF. 157/23 (1993). Available at https://www.refworld.org/docid/3ae6b39ec.html.
- TRC,” South Africa Truth and Reconcilliation Commission Report: Volume 4, chapter 5. Institutional hearings: The health sector,” (1998), 109-164.
- Technical guidance on the application of a human rights‐based approach to the implementation of policies and programmes to reduce preventable maternal morbidity and mortality, (2012). Available at https://www2.ohchr.org/english/issues/women/docs/A.HRC.21.22_en.pdf.
- P. Chastonay, A. M. Klohn, V. Zesiger et al., “Developing a health and human rights training program for french speaking africa: Lessons learned, from needs assessment to a pilot program,” BMC International Health and Human Rights 9/1 (2009), 19.
- L. E. Cotter, J. Chevrier, W. N. El-Nachef et al., “Health and human rights education in us schools of medicine and public health: Current status and future challenges,” PloS One 4/3 (2009), e4916.
- USC, Health & human rights syllabi database. Available at http://apruglobalhealth.org/hhrsyllabi/.
- L. London, “What is a human-rights based approach to health and does it matter?,” Health and Human Rights (2008), 65-80.
- J. Brown, “Training needs assessment: A must for developing an effective training program,” Public Personnel Management 31/4 (2002), 569-578.
- L. London and L. Baldwin-Ragaven, “Human rights and health: Challenges for training nurses in south africa,” Curationis 31/1 (2008), 5-18.
- V. Iacopino, “Teaching human rights in graduate health education,” Health and Human Rights: the Educational Challenge. Boston: François-Xavier Bagnoud Center for Health and Human Rights (2002), 21-42.
- CDC, CDC at-a-glance. Available at https://www.cdc.gov/about/facts/cdcfastfacts/cdcfacts.html.
- P. Farmer, “Pathologies of power: Rethinking health and human rights,” American Journal of Public Health 89/10 (1999), 1486-1496.
- CDC, CDC at-a-glance. Available at https://www.cdc.gov/about/facts/cdcfastfacts/cdcfacts.html.
- DHHS, Department of health and human services secretary’s locally employed staff of the year award. Available at https://www.cdcfoundation.org/blog-entry/compassion-fund-global-health-workers.
- E. Mitchell, CDC foundation’s compassion fund for global health workers. Available at https://www.cdcfoundation.org/blog-entry/compassion-fund-global-health-workers.
- N. Nijim, “The birth of the health and human rights workgroup (HHRW),” HHRW Bulletin 1/1 (2007).
- J. Brown, “Training needs assessment: A must for developing an effective training program,” Public Personnel Management 31/4 (2002), 569-578.
- S. B. Merriam, “Andragogy and self‐directed learning: Pillars of adult learning theory,” New directions for adult and continuing education 2001/89 (2001), 3-14.
- E. Mitchell, CDC foundation’s compassion fund for global health workers. Available at https://www.cdcfoundation.org/blog-entry/compassion-fund-global-health-workers.
- NIH, “CDC views global health as key priority,” Fogarty International Center 13/4 (2014), ; ([internal communication]).
- P. Chastonay, A. M. Klohn, V. Zesiger et al., “Developing a health and human rights training program for french speaking africa: Lessons learned, from needs assessment to a pilot program,” BMC International Health and Human Rights 9/1 (2009), 19.
- M. Hennink, I. Hutter, and A. Bailey, Qualitative research methods, (Sage, 2010).
- VERBI Software. (2015). MAXQDA. (11) Berlin, Germany.
- SAS Institute Inc. (2011). SAS intitute inc. (9.4) Cary, NC.
- M. S. Knowles, The making of an adult educator: An autobiographical journey, (Jossey-Bass Inc Pub, 1989).
- Siracusa principles on the limitation and derogation provisions in the international covenant on civil and political rights, u.N. Doc. E/cn.4/1985/4, annex, (1985). Available at https://www.refworld.org/docid/4672bc122.html.
- M. S. Knowles, The making of an adult educator: An autobiographical journey, (Jossey-Bass Inc Pub, 1989).
- R. Asgary, “Graduate public health training in healthcare of refugee asylum seekers and clinical human rights: Evaluation of an innovative curriculum,” International Journal of Public Health 61/3 (2016), 279-287.
- T. Silberhorn, “Germany’s experience in supporting and implementing human rights-based approaches to health, plus challenges and successes in demonstrating impact on health outcomes,” Health and Human Rights 17/2 (2015), 21-29.