The Rohingya in Cox’s Bazar: When the Stateless Seek Refuge
Abhishek Bhatia, Ayesha Mahmud, Arlan Fuller, Rebecca Shin, Azad Rahman, Tanvir Shatil, Mahmuda Sultana, K. A. M Morshed, Jennifer Leaning, and Satchit Balsari
Abstract
The Rohingya people of Myanmar have been subject to human rights violations through government-sponsored discrimination and violence. Since August 2017, an intensified assault by Myanmar authorities has resulted in a rapid increase of Rohingya pouring into Bangladesh, and the expansion of refugee settlements in the district of Cox’s Bazar has strained humanitarian and government relief efforts. Assessing Rohingya and host community needs is critical for prioritizing resource allocations and for documenting the rights violations suffered by Rohingya refugees. From March 15 to 18, 2018, we conducted a rapid needs assessment of recently arrived Rohingya and host community households. We collected data on demographics, mortality, education, livelihoods, access to food and water, vaccination, and health care. Among other things, our survey found high levels of mortality among young Rohingya men, alarmingly low levels of vaccination among children, poor literacy, and rising poverty. Denied formal refugee status, the Rohingya cannot access due protections and find themselves in a state of insecurity in which they are unsure of their future and unable to formally seek work or send their children to school. While the government of Bangladesh explores the options of repatriation, relocation, and third-country resettlement for these refugees, it is important to ensure that they are not denied a life of dignity.
Introduction
The Rohingya people of Myanmar are one of the most persecuted minorities of our time. Denied citizenship since 1982, they have been subject to government-sponsored discrimination, detention, violence, and torture, causing several waves of mass exodus to Bangladesh, the most recent in 2017.1 Since August 25, 2017, close to 700,000 Rohingya have entered Bangladesh, almost half of whom are now settled in holding camps on the narrow strip of land in Cox’s Bazar District.2
There is now irrefutable evidence of ethnic cleansing in Myanmar’s systematic expulsion of Rohingya across international borders and in the periodic fierce and indiscriminate killings, rapes, and burning of Rohingya homes and farms.3 In Myanmar, the Rohingya are denied legal identities, birth certificates, and even access to essential childhood vaccinations. Restrictions on movement have forcibly confined the Rohingya in Rakhine State, requiring that those seeking work outside their village receive prior authorization from the government.4 Poverty rates in Rakhine, where the Rohingya constituted one-third of the population before the latest mass flight, is nearly twice that of the national average (43.5% of Rakhine’s population live below the poverty line, compared to the 25.6% national average).4 For the Rohingya, this sweeping and selective denial of rights has resulted in abysmal health outcomes. While data from Rakhine State are scarce, key indicators of acute malnutrition, child mortality, and maternal mortality provide a glimpse of the suffering that is occurring due to negligent and hostile government policies.5 Since August 2017, there has been an escalation of campaigns to drive the Rohingya out of Myanmar, transforming a slow but steady stream of Rohingya crossing the border into a massive exodus of hundreds of thousands of people.
Though not a signatory to the 1951 Refugee Convention, Bangladesh has allowed the Rohingya to seek shelter within its borders. Since the first waves of forced migration to Bangladesh in 1977, the Rohingya have been settled in two refugee camps run by the United Nations High Commissioner for Refugees (UNHCR) in Nayapara and Kutupalong. In 1992, the government of Bangladesh stopped recognizing these Rohingya as refugees. After that point, the Rohingya first settled in “unregistered” camps adjacent to the UNHCR camps and finally self-settled in nearby host communities. There are ongoing bilateral attempts to “repatriate” large numbers of Rohingya refugees to Myanmar, but many Rohingya who were sent back have since returned.6 Since August 2017, Bangladesh, the fifth most densely populated country in the world, has accommodated over a million Rohingya refugees and is mobilizing to find resources to take care of these people who literally have nowhere else to go.
However, the refusal of Bangladeshi authorities to grant formal refugee status to this population fleeing from massacre and pillage has placed the Rohingya in a legal and humanitarian limbo. They cannot obtain the protections guaranteed by legal recognition. They can work only in the informal sector, face barriers to accessing education and health services, do not have recourse to the law, and are often arbitrarily detained.7 In response to the latest influx, the government of Bangladesh has provided Rohingya with access to UNHCR services but continues to categorize the Rohingya as illegal migrants. The government does not view their settlement in Cox’s Bazar as a tenable solution and continues to explore all options, including resettlement elsewhere in Bangladesh and onward migration to a third country.8 Competing with the local community for scant resources, the Rohingya are reportedly being blamed for growing tensions with host communities.9
It is in this context, and in the quickly evolving current scenario, that we conducted a rapid needs assessment in both the Rohingya and host communities in Cox’s Bazar to obtain systematic information on the most pressing needs among these two groups of people, with particular attention to the communities’ demographic profiles, education, livelihoods, finances, and aid. This study establishes the parameters for a series of planned participatory studies among the Rohingya aimed at better understanding their needs, their aspirations for their future, and their attitudes as rights-holders. Host community information will help establish a baseline to monitor the impact of this large influx of refugees on local services, wages, and well-being, and to help target interventions to meet needs in both communities.
Methods
We conducted a randomized survey of 802 households between March 15 and March 18, 2018, to assess the basic needs, adequacy of services, and priorities among both the Rohingya and local Bangladeshi host communities in Cox’s Bazar, Bangladesh.
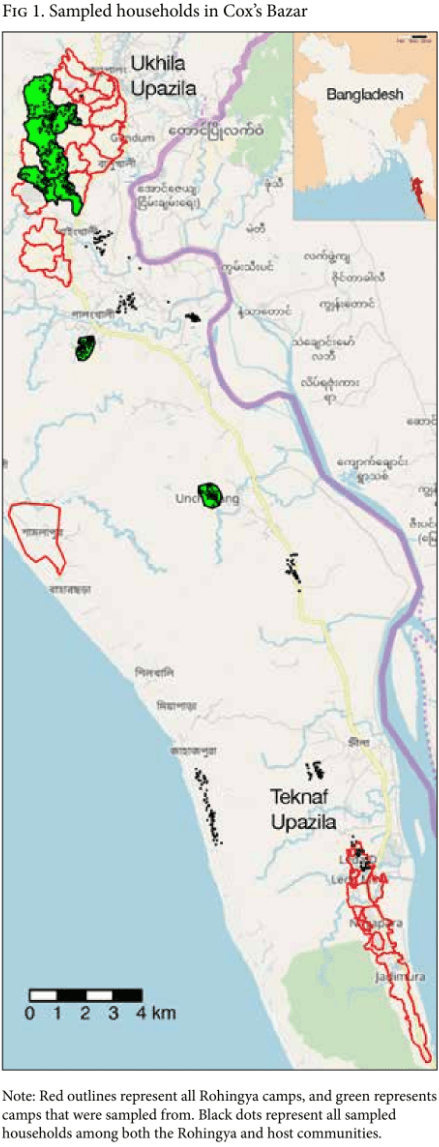
We conducted our study in the Rohingya makeshift camps located in the Ukhia and Teknaf subdistricts of Cox’s Bazar and among host community households located within a five-kilometer radius of these camps. We surveyed 402 Rohingya households and 400 host community households (see Figure 1). The sample size was powered to detect differences within each group at the 95% significance level; our sample size calculation assumed a conservative proportion estimate of 50%, with a 5% margin of error. We defined “household” as a person or group of persons who live together. Each survey was administered to one adult respondent (over 18 years of age) per household, after obtaining that person’s consent.
Sampling in the Rohingya communities
We used a two-stage random sampling strategy to select Rohingya households for our survey. Drawing from a complete list of Rohingya settlements in Cox’s Bazar provided by BRAC, we restricted the sampling universe of Rohingya camps to settlements that (1) were designated as either a “makeshift settlement” or a “spontaneous site;” (2) had a population greater than 50 as of February 25, 2018; and (3) had no occupants prior to August 2017.10 This initial selection resulted in nine camps in Ukhia (of which we randomly selected six) and two camps in Teknaf.
We identified Rohingya households within each camp using OpenStreetMap (OSM) layers for structures identified as “buildings.” We then randomly selected 50 households within each of the eight selected camps by using the OSM “buildings” layer. These structures were marked with red dots, and their GPS coordinates were provided to the enumerators on geospatial PDF maps. If a marked structure had multiple households, enumerators used a random number generator to select from all households residing in the selected structure. When the selected structure was not a residential building, enumerators selected the nearest household to the right of the structure; if there were multiple households nearby, they used a random number generator to sample from the total number of houses. When there were no adjacent residential structures, enumerators chose randomly from a pool of 15 additional preselected OSM buildings. This protocol was also followed when the selected structure had no occupants, if interviewees did not provide informed consent, or if the occupants did not match the sampling group (that is, if a sampled host community household was occupied by a Rohingya family or vice versa).
Sampling in the host communities
Ukhia and Teknaf subdistricts are divided into three unions each, making up of a total of 100 villages (unions are the rural administrative units under rural subdistricts).11 We selected two villages from each union. Due to the unavailability of geospatial village boundary data, OSM could not be used for sampling. Enumerators randomly selected an initial household and then selected every 10th household thereafter to reach a total of 33 households in each of the 12 villages. Two additional households were selected in the two largest villages, resulting in a final sample size of 400.
Survey instrument
Our survey collected demographic information—age, gender, and educational attainment—for each household member. It also collected household mortality information for the last 12 months. The survey included additional questions on access to food and water, vaccination status of children, health care services, occupation, and livelihoods. No personal identifiers were collected. Our survey-based research study was granted exemption by institutional review boards at BRAC and the Harvard T.H. Chan School of Public Health per the US Federal Code of Regulation 45 CFR 46.101(b)(2).
Survey administration
BRAC hired 27 enumerators, all of whom were trained by our research team. They had good contextual knowledge of the Rohingya crisis, having worked in these or adjacent communities in the months prior to the survey. Our survey was administered in the Rohingya dialect. Data were collected using the CommcareHQ application on a tablet computer and, upon survey completion, were encrypted at source on the tablet. Every evening, the enumerators reported to a local BRAC office to upload the data to the cloud.
Statistical analysis
We used descriptive statistics and data visualization in RStudio (version 1.1.414) and Stata SE 15 to summarize the characteristics and responses of the study population.12 Comparisons were drawn between the Rohingya and host community responses for key variables in relevant domains.
Results
Household demographics
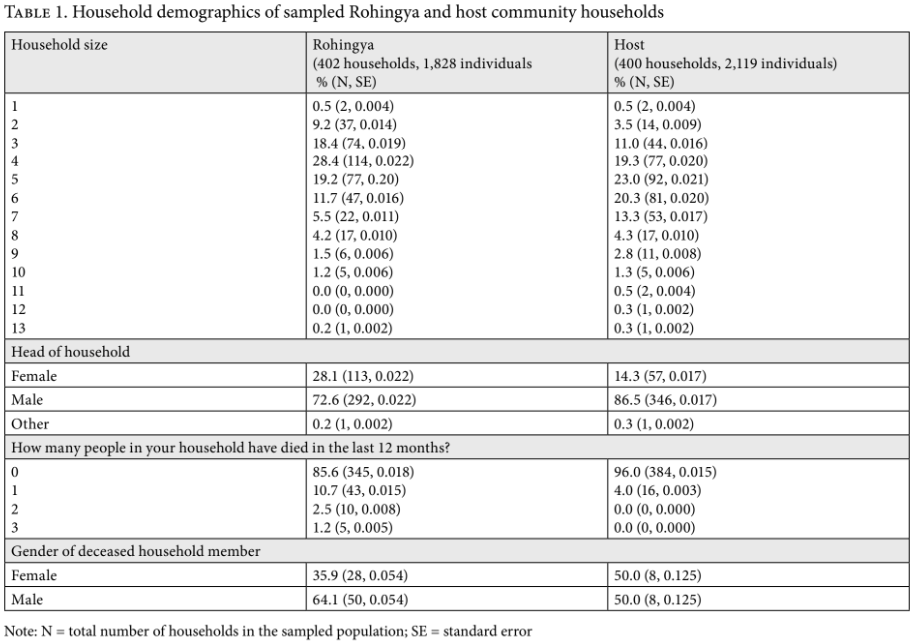
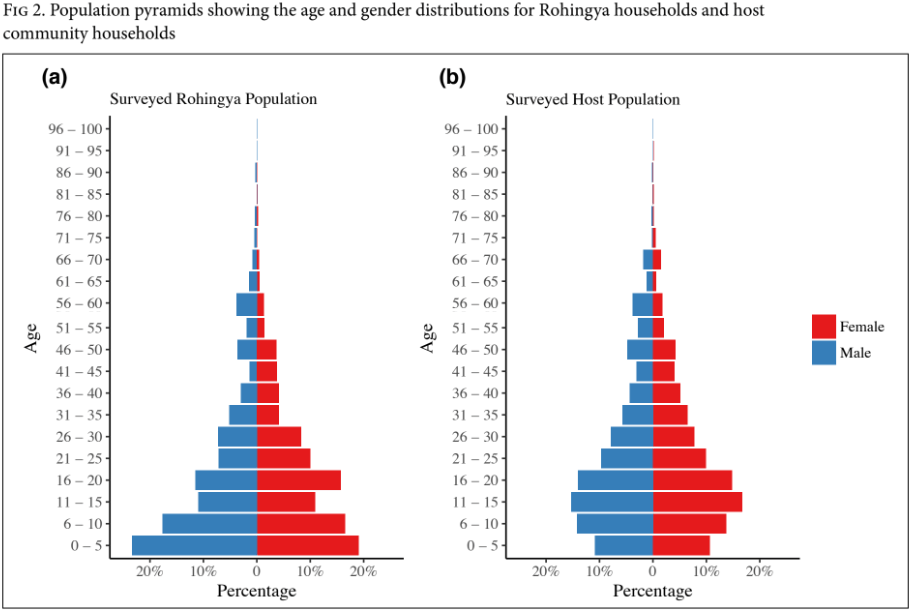
The surveyed sampled population consisted of 1,828 individuals in 402 Rohingya households that had arrived after August 2017, and 2,119 individuals across 400 host community households. Table 1 provides descriptive statistics on household demographics for the two populations. Both populations had similar household sizes (median = 4 in Rohingya households; median = 5 in host community households). Rohingya households were younger (see Figure 1), with mean and median ages of 20 and 16 years, respectively, while host community households had mean and median ages of 24 and 18, respectively.
Mortality
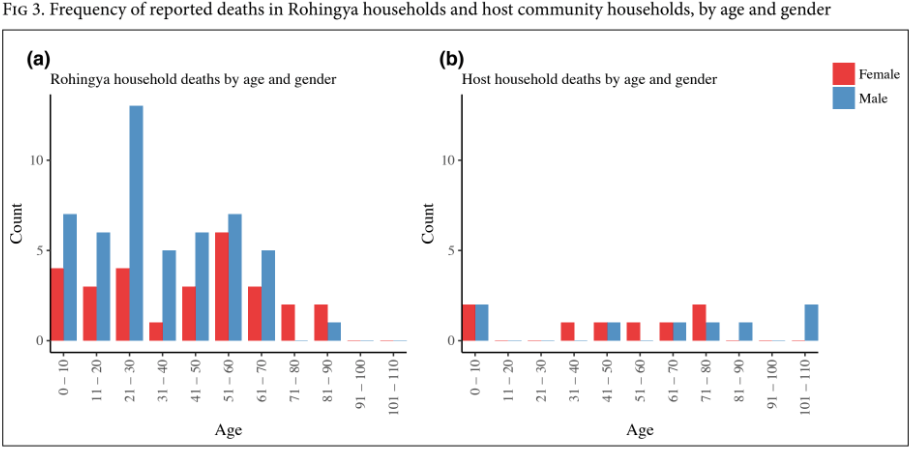
Rohingya households reported 78 deaths in the 12 months preceding the survey; host community households reported 16 deaths. Of surveyed Rohingya households, 10.7% reported one death in the household, 2.5% reported two deaths, and 1.2% reported three deaths; in the host communities, no household reported more than one death. Figure 3 shows the distribution of age at death, by gender, for Rohingya households and host community households. Reported deaths in the Rohingya household were predominantly male (64.1%) and young (mean age at death = 38.7 years; median = 35 years; standard deviation = 24.2). The host community households reported equal numbers of male and female deaths, with deaths occurring at older ages (mean age at death = 56.1 years; median = 65 years; standard deviation = 35.2).
Education
A vast majority of Rohingya household members over the age of 15 (76.0%) reported having had no education, and 52.6% of Rohingya children under the age of 15 were not attending school. Of those children who were attending school, 88.2% of them attended learning centers or schools run by nongovernmental organizations. Among host community members, 43% of those over the age of 15 had received no education, and 33.6% of children under 15 were not attending school. Among school-going children, 53.2% attended government schools, 24.2% attended Islamic schools (known as madrassas), and 18.8% attended private schools. Figure 4 illustrates the distribution of educational attainment among adults in both populations.
Household income and debt
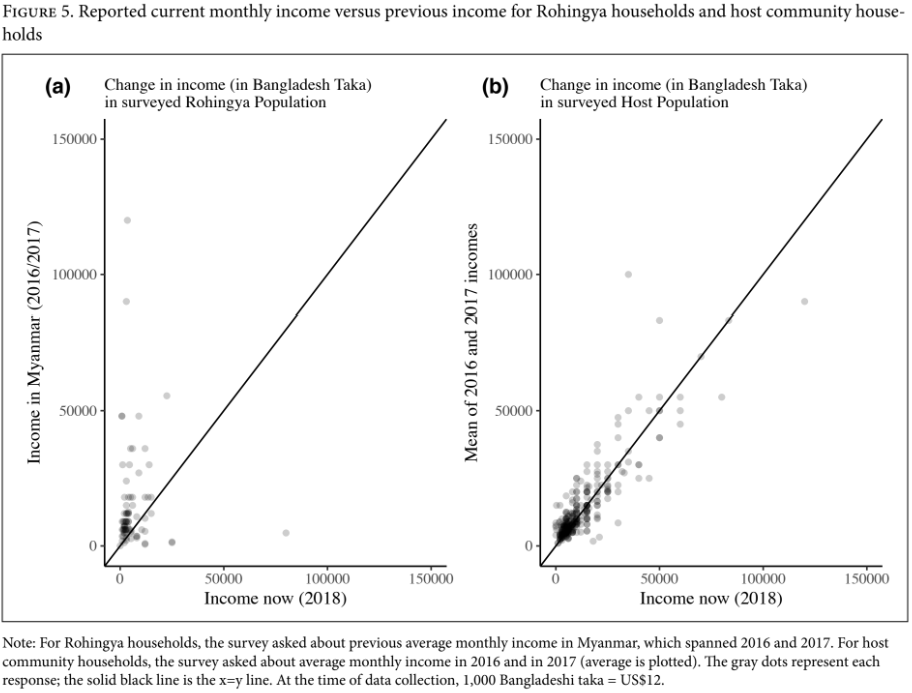
Most Rohingya households (93.5%) reported a decrease in income over the previous 12 months. Among interviewed Rohingya households, the mean monthly income earned in Bangladesh was significantly lower than that earned in Myanmar (95% confidence interval for difference in means: -8405.6 taka, -2931 taka; p-value < 0.0001). In host community households, 49.5% reported a decrease in household income in the prior 12 months; however, there was no significant difference in the mean monthly income earned in 2018 compared to that earned in the previous two years (95% confidence interval for difference in means: -3022.1 taka, 1343.7 taka; p-value = 0.45). Figure 5 shows the change in income levels among both Rohingya and host community households.
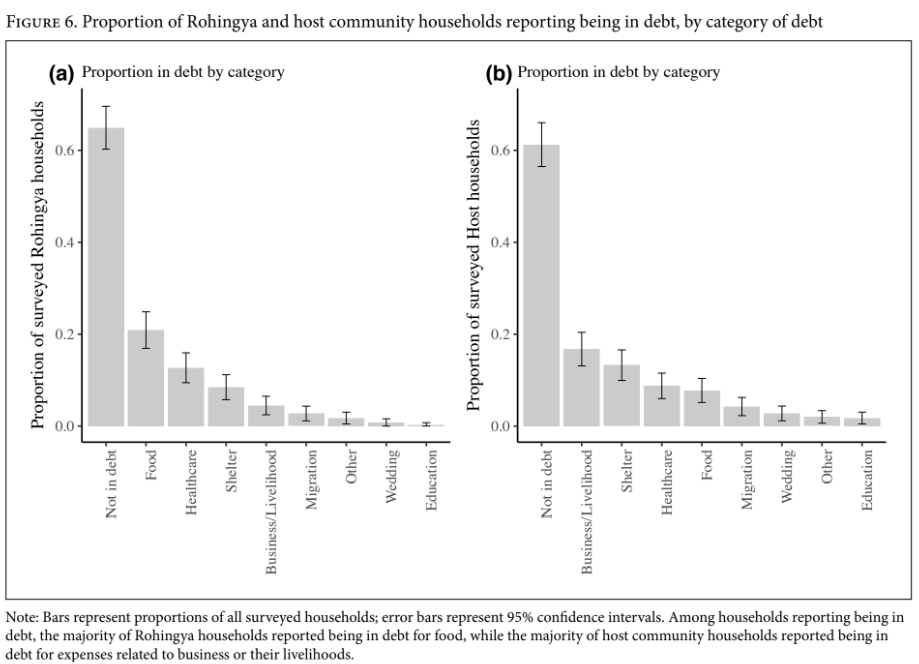
Borrowing is common. In the Rohingya households, 35.1% were in debt. Of these, 72.2% had debts of less than 10,000 takas. The top three reasons for borrowing money were food, health care, and shelter. Regarding lenders, 97.2% were family and friends. No households reported borrowing from BRAC.
In the host community households, 38.8% were in debt, among whom 65.4% owed more than 20,000 takas. They borrowed money mostly for work-related expenses, shelter, and health care. Among households in debt, 76.3% borrowed from family or friends, 19.2% from moneylenders, and smaller factions from banks, BRAC, and other micro-finance institutions (see Figure 6).
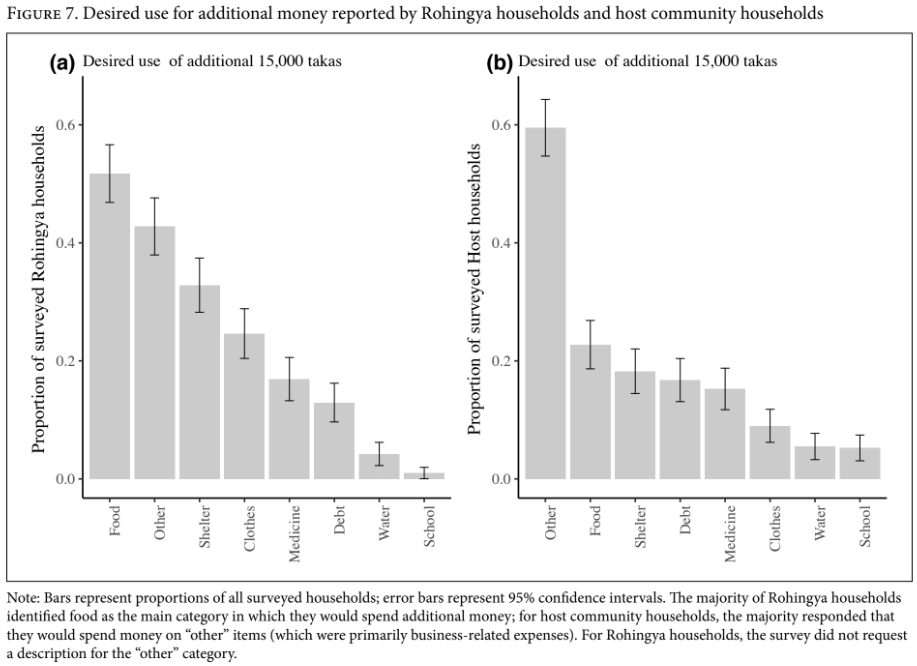
Our survey also asked respondents what they would do if they were to receive 15,000 takas in cash assistance (their answers were not limited to a single response). Among the Rohingya households, 51.7% said they would spend it on food, 32.8% on shelter, and 24.6% on clothing. A large proportion (42.8%) also reported that they would spend the money on “other” items not specifically listed. Meanwhile, in the host communities, 47.5% of households preferred to spend the money on work-related expenses, 22.8% on food, and 18.3% on shelter (see Figure 7).
Water
The majority of households in both the Rohingya community (88.6%) and host communities (79.3%) used tube wells to obtain water for drinking, cooking, and bathing. The remaining Rohingya households sourced drinking water from wells (4.9%), rivers (0.5%), and other unspecified sources (5.7%). Among those households that did not source water from tube wells, 69.3% of host community households did not purify their drinking water, compared to only 35.6% of Rohingya households. The remaining households used conventional methods of boiling, filtering iodine tablets, or UV machines to purify their water.
Food security
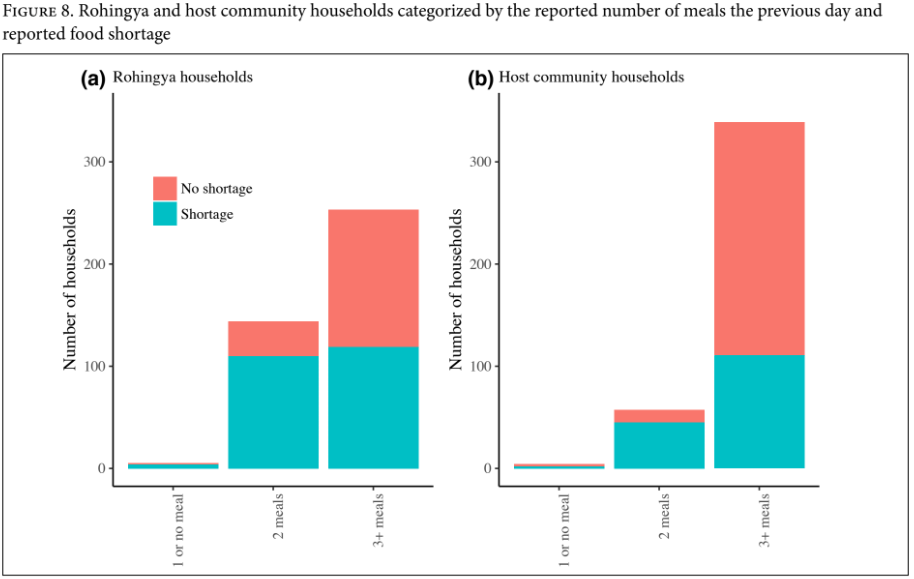
When asked how many meals they ate the previous day, 62.9% of Rohingya households reported having three meals, while 35.8% reported having two. In the host communities, 84.8% of households reported having three meals, while 14.2% reported having two. One percent or less of all surveyed households reported only one or no meals the previous day. However, self-reported rates of food shortage were high: 58% of all Rohingya households and 39.5% of host community households reported experiencing food shortages. Even among households that reported having at least three meals the previous day, 47% of Rohingya households and 32.7% of host community households reported a shortage (see Figure 8).
Vaccination
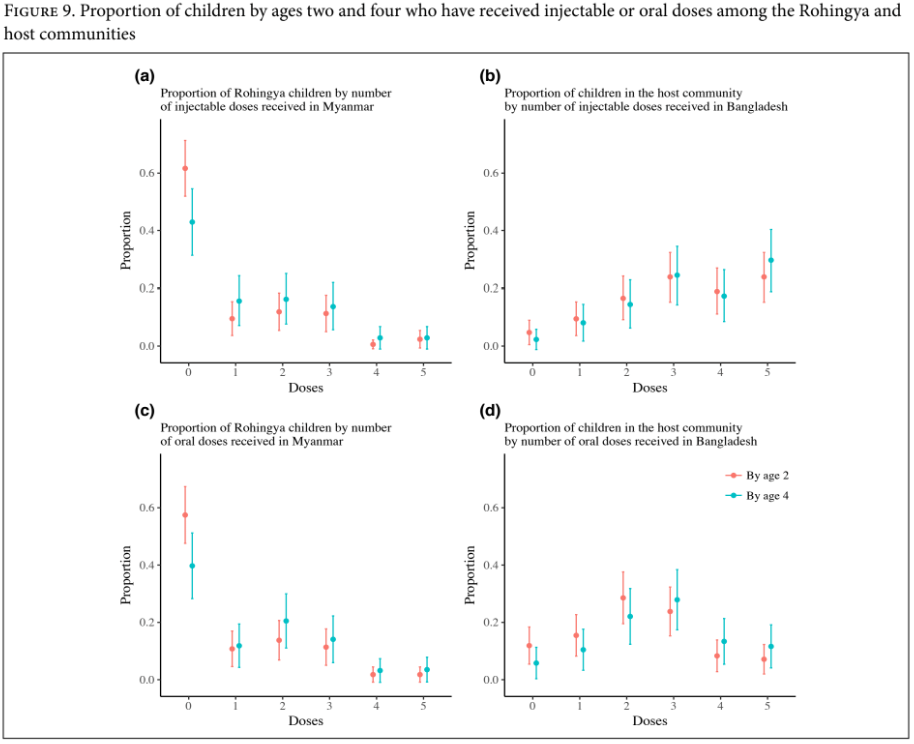
According to the recommended vaccination schedule for children, all children should receive nine doses of injectable vaccines and four doses of oral vaccines by the age of two.13 Among the Rohingya households, of the 167 children aged two and younger, 61.7% had received no doses of injectable vaccines in Myanmar, and only 2.4% had received five or more doses in Myanmar. Even when older children are included, 42.9% of children under the age of four had not received any doses of an injectable vaccine in Myanmar, and only 2.8% had received five or more doses. For oral vaccines, 57.5% of children aged two and younger had received no doses in Myanmar, and only 3.6% had received the recommended number of oral doses (see Figure 9).
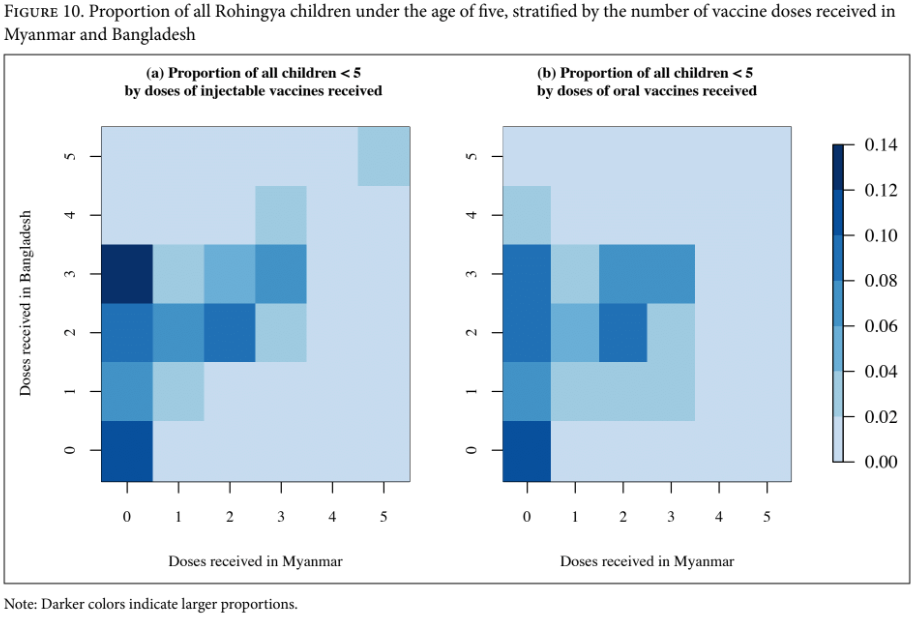
Several vaccination campaigns (for diphtheria, cholera, polio, and measles) have taken place in the Rohingya camps.14 Among the 314 Rohingya children under the age of five, 88.2% had received at least one dose of an injectable vaccine since arriving in Bangladesh, and 82.4% had received at least one dose of an oral vaccine. However, among children who had received no doses of injectable vaccines in Myanmar, 24.8% received no injectable doses in Bangladesh; of those who received no oral vaccines in Myanmar, 29.6% had also not received any doses in Bangladesh (see Figure 10).
Among the host communities, of the 84 children aged two and younger, only 4.8% had not received any doses of injectable vaccines, and 23.9% had received five or more doses. For oral vaccines, 11.9% had not received any doses, and 15.4% had received the recommended number of doses. By age five, 24.9% of children had received the recommended doses of oral vaccines.
Health care access
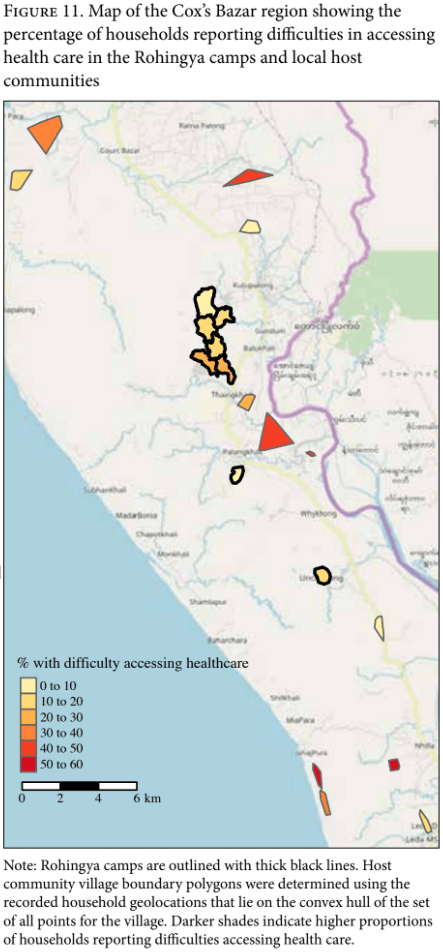
Of all surveyed Rohingya households, 14.2% reported experiencing challenges in accessing health care. There was some variation across Rohingya sites, with the least number of households (5.9%) reporting difficulties at CXB 108 Chakmarkul, and the highest number (24%) reporting difficulties at CXB 219 Camp 19. Among those facing challenges in accessing care, 61.4% said that the nearest facility was too far, 12.3% said they could not afford care, and 40.4% cited other reasons. In the host communities, 32.5% of all surveyed households reported issues in accessing health care, with a wide variation (0 to 57.6%) among locations. Among those who reported difficulties, 70.2% stated that the health care facility was too far, 35.9% claimed they could not afford care, and 9.9% cited other reasons. Figure 11 provides a snapshot of the Rohingya and host community households reporting difficulties in access to care.
Of the 18.9% Rohingya households that reported a pregnancy in the prior year, the majority of pregnant women (56.6%) received no antenatal care. Of those women who gave birth in the previous 12 months, 73.7% did so at home without a certified birth attendant. In the host communities, 11.3% of households reported a pregnancy during the last year, of whom 42.2% had at least one antenatal visit and 24.4% had two. Of those reporting a childbirth in the prior 12 months, 51.7% gave birth at home without a certified birth attendant.
Discussion
The results of this rapid needs assessment offer important insights into the most pressing challenges facing the Rohingya while also providing contextual information about the neighboring Bangladeshi communities hosting them. Our data underscore the gross violations and abandonment faced by the Rohingya in Myanmar.
High mortality
The Rome Statute of the International Criminal Court defines the crime of genocide as any of the following acts committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group . . . : killing members of the group; causing serious bodily or mental harm to members of the group; deliberately inflicting on the group conditions of life calculated to bring about its physical destruction in whole or in part; [among others].15
The demographic pyramid representing Rohingya refugees demonstrates the loss of working-age men. In conjunction with the high number of household deaths reported in our survey, this pyramid shape speaks to a war-affected population with violent deaths of males. Our findings corroborate findings of systematic massacres of young men and boys as reported by other human rights and advocacy organizations.16 Sampled Rohingya households reported nearly five times as many deaths as host community households, with a majority of them occurring among young men. In the Rohingya households, the median age for male deaths was lower than that for females, and the overall mean age at death in these households was lower than that in the host communities. This trend of high deaths among young Rohingya men is consistent with the targeted killings that have been observed as part of systematic ethnic cleansing and genocide elsewhere.17
Education
Literacy levels among Rohingya adults (those over 15 years) are very low, as is school enrollment. While we sampled only those who had arrived after August 2017, the numbers shed critical light on the need to prioritize access to formal schooling—an ongoing challenge among populations on the move.18 Currently, BRAC provides primary education through 200 learning centers for over 21,000 students, available to all, with the rollout of additional centers planned in the near future. Contrary to concerns about Rohingya migrants seeking education in madrassas, our survey found that refugee children were not attending these institutions. However, based on our earlier surveys among the long-settled Rohingya in the region, madrassa attendance may eventually rise, especially if there are no viable alternatives. School access is a persistent challenge for many of the earlier arrivals; denied refugee status, they cannot access UNHCR-led services. Even those in the UNHCR camps have access only up to the eighth grade, consistent with national laws that provide for compulsory education up to the eighth grade.
Bangladesh has ratified the Convention on the Rights of the Child. The country’s education system is one of the largest in the world, with 21.9 million children in kindergarten and primary school. Two percent of the gross domestic product (and 14.4% of the national budget) is spent on education. A stated outcome of the government’s Third Primary Education Development Program is to reduce “regional and other disparities” in terms of participation, completion, and learning outcomes. Despite these commitments, the need to expand access to schools and vocational training for both children and adults is evident in the host communities as well, where age-disaggregated data show that about one-third of Bangladesh’s population falls in the 10–24 age group, with large gaps in basic education and employability.19
Livelihoods and debt
Rohingya households have become significantly impoverished, as expected during migration, with 79.9% of surveyed households reporting no current income. Among the host communities, contrary to the fear that the presence of Rohingya was driving down wages, our survey found small increases in the number of households reporting an income, as well as in the total income for some households.
Bangladesh’s transition toward a country with a lower fertility rate and improved health services is reflected in its overall demographic profile, with a decreasing dependency ratio and a growing percentage of the population entering the labor market.20 The Rohingya population will add to the dependency ratio in the country unless the Rohingya are allowed to participate in the labor market. There is growing and convincing evidence globally that legally integrating refugees into the labor force promotes dignity and self-reliance, while positively contributing to the local economy.21 Our own studies of long-settled Rohingya migrants have shown that almost all eventually find some form of work, albeit in the informal sector, irregularly, and for low wages.
There is an urgent need to address and alleviate barriers to refugees’ ability to legally seek work, including while they await decisions about their fate. Particular attention must be paid to involving women in income-generating activities, given the high ratio of female-headed households among the Rohingya population and the cultural barriers (in both Rohingya and host communities) against allowing women to work.
Bangladesh’s existing restrictions preventing the Rohingya from being able to work and to borrow money only compound the economic burden inflicted on this community through the loss of property and possessions while fleeing Myanmar. These issues have led to the accrual of informal debt to family and friends. Rohingya debts are mostly below 10,000 takas and may reflect limited access to larger amounts through formal mechanisms of lending, including microfinance. The host communities, whose debts are often in excess of 20,000 takas, have better access to loans and use them primarily to support their means of livelihood.
Water
Our survey did not elicit any alarming deficits in access to water. Both groups procured water mainly from tube wells, which, if not contaminated at the source, provide water that does not require additional purification.
Food
We found high levels of food insecurity among the Rohingya, with more than one-third of these households reporting eating only two meals a day, and 32.7% of those that have three meals a day reporting a food shortage in their household. This food shortage among Rohingya refugees is also reflected in their prioritization of food over all else if provided additional cash assistance, as well as in their borrowing money to procure food, as reported in our survey. Currently, the Rohingya population that arrived in 2017 is reliant on humanitarian assistance for food, with the World Food Programme providing food vouchers that can be used to purchase from a pre-set list of food items, though these offerings lack dietary diversity.22 The provision of cash assistance instead of food vouchers could allow the Rohingya to decide where they would like to allocate their money (for example, toward their own livelihood generation) and allow them to access a more diverse offering of foods than the current pre-set list.23
Vaccination
A high number of Rohingya children had received no vaccines while in Myanmar, as had been suspected after the recent diphtheria outbreak in the Rohingya camps in Cox’s Bazar in December 2017.24 Despite the large number of vaccination campaigns in the camps, a majority of Rohingya children have yet to receive vaccinations according to the prescribed universal schedule. The failure to vaccinate Rohingya children in Myanmar provides additional evidence of the discriminatory and unconscionable practices of Myanmar’s government against the most vulnerable section of their society.
Health care access
Data on the observed (and wide) variation in health care access in the host communities will help the government and the aid sector plan services in the region, including the deployment of mobile clinics to reach areas where distances have been reported as prohibitive. Improving the utilization of antenatal care in both communities will require increased access and awareness.
Study limitations
While survey-based studies allow for rapid assessments in humanitarian emergencies, they suffer from inherent limitations associated with self-reported data, including recall and respondent biases.
In addition, our sampling approach in the Rohingya camps, which utilized OSM data, may be biased due to the limited availability of data on the presence of household structures from which to sample across locations. In the host communities, true randomization was hampered by the unavailability of a complete household census for these villages.
Our survey instrument was coded in Bengali on the tablets but administered in the Rohingya dialect; responses were recorded in Bengali. However, given that most questions were restricted to selecting from a list of possible responses, the translation of responses is not likely to have resulted in statistically significant errors.
The interpretation of our mortality data may be susceptible to systematic biases in our sampled Rohingya populations. For example, it is possible that only families where young, working-age men were killed left for Bangladesh, while others remained. These data may also be affected by recall bias favoring remembering male deaths or young adult deaths, as well as any inherent sex-preferences for males in the underlying population that may lead to a higher count of male deaths overall.25 Our questions about Rohingya mortality were limited and did not include information on the cause, time, or location of deaths of household members. Given the consistency of our findings with reports on systematic discriminatory killings, further inquiry into these data would be beneficial.
Our questions (and the elicited responses) about vaccination also need further inquiry. It is important to know which vaccines the children have gotten, which they have not, and which need to be prioritized.
The study did not explore issues around identity, security, and safety facing the Rohingya, including questions about gender-based violence. It did not include further details about the high death rates among young men. Additional studies have been planned to address this gap.
Our findings indicate that an overwhelming number of Rohingya felt safe in Bangladesh. Among those who felt unsafe, most feared repatriation. Among the small percentage of people in host communities who felt unsafe, the majority feared the presence of the Rohingya. These sentiments need additional in-depth and focused inquiries among both groups.
Conclusion
The Rohingya are denied refugee status in Bangladesh. As a consequence, they are further denied many of the protections ensured through international law. The absence of legal registration precludes any formal mechanism of repatriation or of resettlement to a third, more hospitable nation. Accordingly, while some individuals have attempted the unsafe onward journeys (sometimes with fatal consequences) to locations such as Thailand, Malaysia, Indonesia, and the Middle East, the vast majority of Rohingya have been forced to seek work illegally, on the fringes of the informal sector.
Hundreds of thousands of new arrivals in the camps find themselves confined, with significant restrictions on work and schooling. Though Bangladesh’s Constitution provides for the legal protection of non-citizens, it has not incorporated into domestic law article 25 of the Universal Declaration of Human Rights, which protects the right to an adequate standard of living.26 It is in this legal vacuum that many Rohingya, whether refugees or legal residents, remain suspended indefinitely with little prospect of improvement. Denied the chance in Myanmar to fulfill their human capabilities, the Rohingya must not be consigned to inanition, sequestered in camps in Bangladesh.
The gaps in services identified by our data require renewed efforts to fulfill these human security needs. The general consensus among analysts is that many Rohingya will likely remain in camps in Bangladesh for the foreseeable future.27 Most notably, however, other countries from the Association of Southeast Asian Nations seem to have abrogated responsibility for the Rohingya people.28 The government of Bangladesh should not be expected to take on this burden alone. The international community must provide the support needed to rehabilitate these refugees from campaigns of ethnic cleansing while insisting that the Rohingya be officially recognized as refugees. While the government of Bangladesh explores a range of placement options—including settling the Rohingya within Bangladesh, repatriating them to Myanmar, and supporting onward migration to a third country—it is of urgent importance that the Rohingya be furnished with tools of self-reliance. Solutions exploring relocation or onward migration will fall short unless they also include short-term measures aimed at allowing the Rohingya to find work and education while in Bangladesh. This population is burdened with high illiteracy rates and limited skill sets. While mounting evidence from around the world shows the prudence of formally integrating refugees into the labor force, doing so in Bangladesh will entail substantial upstream investment in imparting skills and education to migrant populations, with a particular focus on women.29 These strategic interventions are likely to work best and cost least if migrant populations are integrated into the host community, as geographic isolation would render them unable to participate in or contribute to the local economy.30 Such refugee integration efforts typically require expansion of services to the host community as well, in order to be equitable and to prevent further resentment among host communities.31
People seeking asylum must not be expelled or forced to return to situations where they are not safe. The principle of non-refoulement is a firmly established prohibition in international law.32 Although the government of Bangladesh has taken steps to ensure that any instances of repatriation are safe and voluntary, the proposed repatriation efforts cannot be presumed to be uncoerced as long as evidence demonstrates that the environment in Rakhine State remains insecure.33 Our data echo the international community’s alarm at Myanmar’s continued ethnic cleansing of the Rohingya from Rakhine State. Myanmar must be held accountable.
Abhishek Bhatia, MSc, is a visiting scholar and researcher at the François-Xavier Bagnoud Center for Health and Human Rights, Harvard University, Boston, MA, USA.
Ayesha Mahmud, PhD, is the Rockefeller Foundation Planetary Health Postdoctoral Fellow at the Center for Communicable Disease Dynamics, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
Arlan Fuller, JD, MA, is executive director of the François-Xavier Bagnoud Center for Health and Human Rights, Harvard University, Boston, MA, USA.
Rebecca Shin, MPA, MEd, is program coordinator of the François-Xavier Bagnoud Center for Health and Human Rights, Harvard University, Boston, MA, USA.
Azad Rahman, MBA, MPA, MPS, is program head of the Advocacy for Social Change program at BRAC, Dhaka, Bangladesh.
Tanvir Shatil, MSS, is a researcher in the Research and Evaluation Division at BRAC, Dhaka, Bangladesh.
Mahmuda Sultana, MSS, MSc, is a policy analyst in the Advocacy for Social Change program at BRAC, Dhaka, Bangladesh.
K.A.M Morshed, MPF, is director of the Advocacy for Social Change, Technology, and Partnership Strengthening Unit at BRAC, Dhaka, Bangladesh.
Jennifer Leaning, MD, SMH, is François-Xavier Bagnoud Professor of the Practice of Health and Human Rights in the Department of Global Health and Population at the Harvard T.H. Chan School of Public Health and director of the François-Xavier Bagnoud Center for Health and Human Rights, Harvard University, Boston, MA, USA.
Satchit Balsari, MD, MPH, is on the faculty of emergency medicine at Beth Israel Deaconess Medical Center and a fellow at the François-Xavier Bagnoud Center for Health and Human Rights, Harvard University, Boston, MA, USA.
Please address correspondence to Satchit Balsari. Email: balsari@hsph.harvard.edu.
Competing interests: None declared.
Copyright © 2018 Bhatia, Mahmud, Fuller, Shin, Rahman, Shatil, Sultana, Morshed, Leaning, and Balsari. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- S. S. Mahmood, E. Wroe, A. Fuller, and J. Leaning, “The Rohingya people of Myanmar: Health, human rights, and identity,” Lancet 389/10081 (2017), pp. 1841–1850.
- International Organization for Migration, Rohingya Refugee Crisis Response: External Update (February 2018). Available at https://www.iom.int/sites/default/files/situation_reports/file/Bangladesh_SR_20180202-08.pdf.
- Office of the United Nations High Commissioner for Human Rights, Darker and more dangerous: High Commissioner updates the Human Rights Council on human rights issues in 40 countries(September 11, 2017). Available at https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=22041.
- Department of Population, Myanmar Ministry of Immigration and Population, “The 2014 Myanmar population and housing census,” in The Union Report: Occupation and Industry; Census Report Volume 2-B (Myanmar, 2016); UNICEF, Rakhine State: A snapshot of child wellbeing (2012). Available at https://www.unicef.org/myanmar/Rakhine_State_Profile_30-07-15.pdf; Y. Lee, Report of the Special Rapporteur on situation of human rights in Myanmar, UN Doc. A/69/398 (2014).
- Mahmood (2017, see note 1).
- R. Paul and Y. Lee, “Bangladesh agrees with Myanmar to complete Rohingya return in two years,” Reuters (January 16, 2018). Available at https://www.reuters.com/article/us-myanmar-rohingya-bangladesh/bangladesh-agrees-with-myanmar-to-complete-rohingya-return-in-two-years-idUSKBN1F50I2.
- R. Zetter and H. Ruaudel, “Refugees’ right to work and access to labor markets: An assessment,” Global Knowledge Partnership on Migration and Development Working Paper and Study Series (2016).
- “Rohingya crisis: Bangladesh and Myanmar agree repatriation timeframe,” BBC News (January 16, 2018). Available at http://www.bbc.com/news/world-asia-42699602.
- European Commission, Shelter NFI joint need assessment: Host community HH survey (November 2017). Available at https://reliefweb.int/sites/reliefweb.int/files/resources/host_community_report_final_180124.pdf; J. Bennett, “Myanmar: Rohingya refugees face increasing hostility in southern Bangladesh,” ABC News (September 27, 2017). Available at http://www.abc.net.au/news/2017-09-28/rohingya-refugees-face-increasing-hostility-in-bangladesh/8995238; “Rohingya Muslims thought they had found a safe haven in Bangladesh: That could be about to change,” Independent (December 30, 2017). Available at http://www.independent.co.uk/news/world/asia/rohingya-muslims-myanmar-burma-bangladesh-refugees-local-clashes-workers-food-border-a8121231.html; M. Sattar, “Rohingya camps in Bangladesh and Thailand, worlds apart,” Al Jazeera (January 28, 2017). Available at https://www.aljazeera.com/blogs/asia/2017/01/rohingya-camps-bangladesh-thailand-worlds-170127113046730.html; Council on Foreign Relations, What forces are fueling Myanmar’s Rohingya crisis? Available at https://www.cfr.org/backgrounder/rohingya-crisis.
- Rohingya Displacement, Humanitarian data exchange. Available at https://data.humdata.org/event/rohingya-displacement.
- Bangladesh, Local Government (Union Parishads) Act (In Bangla) (2009). Available at http://bdlaws.minlaw.gov.bd/bangla_all_sections.php?id=1027.
- RStudio, Integrated Development for R (Boston, MA: RStudio, Inc., 2015); Stata Statistical Software: Release 15. College Station, TX: StataCorp LP.
- Incepta Vaccine Ltd, Immunization Schedule (April 2018). Available at http://inceptavaccine.com/immunization-schedule.php; Centers for Disease Control and Prevention, 2018 recommended immunizations for children from birth through 6 years old (December 2017).
- UNICEF, Bangladesh steps up vaccination for new Rohingya arrivals as measles cases rise (2017). Available at https://www.unicef.org/media/media_101470.html.
- UN General Assembly, Rome Statute of the International Criminal Court, UN Doc. A/CONF.183/9 (1998).
- Amnesty International, “We will destroy everything”: Military responsibility for crimes against humanity in Rakhine State, Myanmar (London: Amnesty International, 2018); Human Rights Watch, Burma: Military massacres dozens in Rohingya village (October 4, 2017). Available at https://www.hrw.org/news/2017/10/03/burma-military-massacres-dozens-rohingya-village; Human Rights Watch, Burma: Methodical massacre at Rohingya village (December 19, 2017). Available at https://www.hrw.org/news/2017/12/19/burma-methodical-massacre-rohingya-village; W. Lone, K. Oo, S. Lewis, and A. Slodkowski, “Massacre in Myanmar,” Reuters (February 8, 2018). Available at https://www.reuters.com/investigates/special-report/myanmar-rakhine-events.
- D. Guha-Sapir and O. D’Aoust, Demographic and health consequences of civil conflict (Washington, DC: World Bank, 2010); Medecins Sans Frontieres, Retrospective mortality, nutrition and measles vaccination coverage survey in Balukhali 2 & Tasnimarkhola camps: Cox’s Bazar, Bangladesh (November 2017). Available at https://www.msf.org/sites/msf.org/files/report-rohingyas-emergency-17-vf1.pdf.
- United Nations High Commissioner for Refugees, Left behind: Refugee education in crisis (Geneva: UNHCR, 2017).
- Asian Development Bank, “Skills development in Bangladesh,” Asian Development Bank Briefs, Report No. 67. Available at https://www.adb.org/sites/default/files/publication/203881/skills-dev-bangladesh.pdf; A. Ali, “Informal Labour Force,” in R. Titumir (eds), Accumulation and alienation: State of labour in Bangladesh 2013 (Bangladesh: Unnayan Onneshan, 2013).
- United Nations Population Division, World population prospects. Available at https://esa.un.org/unpd/wpp/Graphs/DemographicProfiles.
- United Nations High Commissioner for Refugees, “Solutions for refugees,” in The 10-point plan, pp. 184–206. Available at http://www.unhcr.org/50a4c17f9.pdf.
- “New Rohingya arrivals in Bangladesh at risk from poor diets,” ReliefWeb (January 5, 2018). Available at https://reliefweb.int/report/bangladesh/new-rohingya-arrivals-bangladesh-risk-poor-diets; WFP Office of Evaluation, The contribution of food assistance to durable solutions in protracted refugee situations: Its impact and role in Bangladesh; A mixed method impact evaluation (2012) Available at https://reliefweb.int/sites/reliefweb.int/files/resources/510fcefb9_0.pdf.
- ScienceDirect, Cash, food, or vouchers? Evidence from a randomized experiment in northern Ecuador. Available at https://www.sciencedirect.com/science/article/pii/S0304387813001715.
- ReliefWeb, Bangladesh: Diphtheria outbreak (December 2017). Available at https://reliefweb.int/disaster/ep-2017-000177-bgd.
- L. Bourque, J. Siegel, M. Kano, and M. Wood, “Morbidity and mortality associated with disaster,” in Handbook of disaster research (New York: Springer, 2007), pp. 97–112.
- Constitution of the People’s Republic of Bangladesh (1972), arts. 31, 32; Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948), art. 25.
- B. Otto, “Rohingya camps in Bangladesh start to look permanent,” Wall Street Journal (April 3, 2018). Available at https://www.wsj.com/articles/rohingya-camps-in-bangladesh-start-to-look-permanent-1522762656.
- E. Pearson, “The Rohingya test ASEAN’s human rights responsibilities,” Human Rights Watch (February 27, 2009). Available at https://www.hrw.org/news/2009/02/27/rohingya-test-aseans-human-rights-responsibilities.
- A. Betts, “Help refugees help themselves,” Foreign Affairs (2015). Available at https://www.foreignaffairs.com/articles/levant/2015-10-20/help-refugees-help-themselves; Antonio Guterres, “Think the aid system can cope? It can’t,” World Economic Forum (January 18, 2015). Available at https://www.weforum.org/agenda/2015/01/think-the-aid-system-can-cope-it-cant.
- World Bank, Uganda’s progressive approach to refugee management (2016). Available at http://www.worldbank.org/en/topic/fragilityconflictviolence/brief/ugandas-progressive-approach-refugee-management.
- World Bank, Forcibly displaced: Toward a development approach supporting refugees, the internally displaced, and their hosts (Washington, DC: World Bank, 2017); United Nations Development Programme, International Labour Organization, and World Food Programme, Jobs make the difference: Expanding economic opportunities for Syrian refugees and host communities (Dubai: Rasil, 2017); Bennett (2017, see note 9).
- United Nations High Commissioner for Refugees, Convention and Protocol Relating to the Status of Refugees (1951). Available at http://www.unhcr.org/protection/basic/3b66c2aa10/convention-protocol-relating-status-refugees.html.
- United Nations High Commissioner for Refugees, Bangladesh and UNHCR agree on voluntary returns framework for when refugees decide conditions are right (2018). Available at http://www.unhcr.org/news/press/2018/4/5ad061d54/bangladesh-unhcr-agree-voluntary-returns-framework-refugees-decide-conditions.html.