A Comparison of Health Achievements in Rwanda and Burundi
Hari S. Iyer, Adanna Chukwuma, Jean Claude Mugunga, Anatole Manzi, Melino Ndayizigiye, and Sudhir Anand
Abstract
Strong primary health care systems are essential for implementing universal health coverage and fulfilling health rights entitlements, but disagreement exists over how best to create them. Comparing countries with similar histories, lifestyle practices, and geography but divergent health outcomes can yield insights into possible mechanisms for improvement. Rwanda and Burundi are two such countries. Both faced protracted periods of violence in the 1990s, leading to significant societal upheaval. In subsequent years, Rwanda’s improvement in health has been far greater than Burundi’s. To understand how this divergence occurred, we studied trends in life expectancy following the periods of instability in both countries, as well as the health policies implemented after these conflicts. We used the World Bank’s World Development Indicators to assess trends in life expectancy in the two countries and then evaluated health policy reforms using Walt and Gilson’s framework. Following both countries’ implementation of health sector policies in 2005, we found a statistically significant increase in life expectancy in Rwanda after adjusting for GDP per capita (14.7 years, 95% CI: 11.4–18.0), relative to Burundi (4.6 years, 95% CI: 1.8–7.5). Strong public sector leadership, investments in health information systems, equity-driven policies, and the use of foreign aid to invest in local capacity helped Rwanda achieve greater health gains compared to Burundi.
Introduction
Countries in sub-Saharan Africa have faced significant challenges in improving population health.[1] To protect the right to the highest attainable standard of health for their citizens, several African states have become parties to the International Covenant on Economic, Social and Cultural Rights. This covenant commits state parties to take the steps necessary to promote child health, improve environmental and industrial hygiene, manage infectious disease outbreaks, and assure access to health services for all.[2] At the dawn of the twenty-first century, sub-Saharan Africa has made substantial progress in health, including a 52% reduction in under-five mortality from 1990 to 2015, a 49% reduction in maternal mortality from 1990 to 2013, and a 46% reduction in HIV infections from 2000 to 2013—partly through a renewed global commitment to poverty reduction and health promotion in response to the Millennium Development Goals.[3] However, much work remains to reduce the deprivations of the estimated 41% of people living on less than $1.25 a day and of the 23% of undernourished people in sub-Saharan Africa.[4]
One country in the region that has seen remarkable improvements in health in recent years is Rwanda—a small, hilly, landlocked nation in East Africa. In 1994, it experienced ethnically driven genocide that claimed the lives of roughly one million of its citizens. Following this tragedy, Rwanda sought to build a stronger nation through reconciliation and poverty reduction.[5] Guided by principles of equity and led by a powerful central government that has implemented evidence-based policies, Rwanda has shown substantial achievements that belie its size and standing in the region. It is currently one of the only countries in the region to meet the health-related Millennium Development Goals and has recorded steep declines in under-five and maternal mortality over the past 15 years.[6]
Burundi, Rwanda’s southern neighbor, despite similar geography, lifestyle practices, history, and resources, has struggled to keep pace. Burundi emerged from a decade-long civil war in the early 2000s that had ethnically driven causes, like Rwanda.[7] The parallels between the two countries have been mirrored more recently. In the summer of 2015, both countries began the process of changing their constitutions to allow the president to run for a third term. Rwanda’s legislature voted and approved the change, based on a popular petition and with very little opposition.[8] Burundi’s Parliament rejected the proposed constitutional changes, and the country has experienced protracted civil unrest and concerns about renewed ethnic violence.[9]
The goal of this paper is to explain the differences in health achievements between Rwanda and Burundi following their respective periods of genocide and civil war. We begin by presenting time-series data from the World Bank highlighting the differing trends in life expectancy before and after the period of conflict. We then contrast the specific health policy reforms that were implemented in the two countries. Finally, we suggest hypotheses for the observed differences and discuss the generalizability of our findings to other sub-Saharan African contexts.
Methods
Analytic overview
To assess the association between health policy reform and health outcomes, we undertook two investigations. First, we compared trends in life expectancy from 1960 to 2015 in Rwanda and Burundi, controlling for macroeconomic variables using data from the World Bank’s World Development Indicators in an interrupted time-series analysis (Statistical Appendix).[10] Second, we analyzed health policy reforms in Rwanda and Burundi from 2000 onward using Walt and Gilson’s health policy analysis framework.[11]
Health and development indicators
In 1990, the United Nations Development Programme released the Human Development Index (HDI), a composite index that could be standardized across countries to measure performance with respect to human development.[12] The HDI includes life expectancy, gross domestic product (GDP) per capita in constant purchasing power parity dollars, and education. For our analysis, we decided to focus on health and macroeconomic indicators. We omitted the education variable due to a lack of data from 1960 to 2015. To assess changes in health over time, we decided to compare life expectancy in both countries as a core component of the HDI. Since we have data for GDP per capita over the full historical period, we chose to control for it in our regression model (see Statistical Appendix).
Statistical analysis
We used controlled-interrupted time-series analysis to study trends in life expectancy following the implementation of health policy reforms adopted by both countries in 2005, specifically the First Health Sector Strategic Plan in Rwanda and the National Health Policy Plan in Burundi.[13] We chose the pre-conflict period to be 1960–1992 for both Rwanda and Burundi, corresponding to the start of the conflict in both countries. The post-implementation period was defined as 2005–2015 in both countries. Our outcome was national life expectancy for Rwanda and Burundi over the study period. We fitted segmented regression models using generalized least squares regression, with autoregressive and moving average terms to account for autocorrelation in the time series. Indicator variables for the pre- and post-implementation time periods were used to compare relative trends in life expectancy between Rwanda and Burundi during these periods. GDP per capita was measured in constant 2010 US dollars. Full details regarding the statistical model are provided in the Statistical Appendix. We conducted our analysis using R v. 3.1.0.
Health policy analysis
We compared Rwanda’s and Burundi’s health policy reforms using Walt and Gilson’s framework for health policy analysis.[14] This approach defines the process of health policy reform through various components: context, actors, content, and process. We used these features to frame our analysis and determine how the different aspects of health policy reform were conducted in Rwanda and Burundi. We focused on institutional and individual actors in government and nonprofit sectors that were involved in setting and implementing health policy. We then discussed the similarities and differences in the health policies that were implemented in each country and concluded with a discussion of what could be learned from their respective experiences. We used the World Health Organization’s health systems “building blocks” classifications to analyze health policy reforms.[15]
For the health policy analysis, we conducted a literature review on health policies implemented in Rwanda and Burundi after 2000, including a review of online research databases such as PubMed, and gray literature such as government press releases and local newspaper articles.
Results
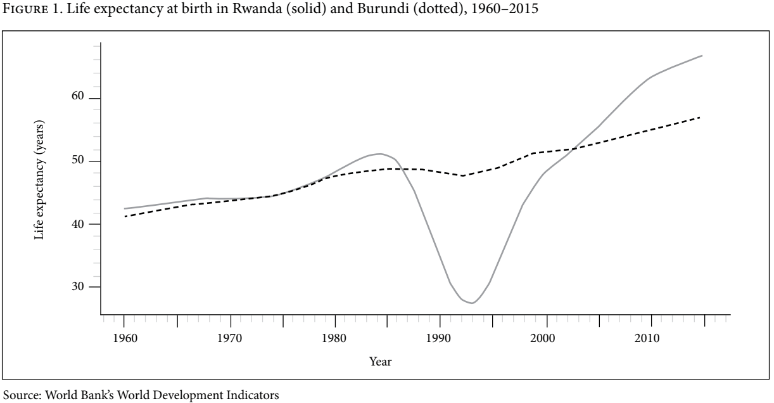
Source: World Bank’s World Development Indicators
Figure 1 shows that life expectancy was similar in the two countries prior to 1984. The period from 1984 to 1994 showed a steep decline in life expectancy in Rwanda and a small decline in Burundi. The steep decline preceding the genocide in 1994 was due to economic instability brought on by a drop in world coffee prices, at that time Rwanda’s main export, and the onset of armed conflict between the Rwandan Patriotic Front and the national government in 1990.[16] The slight decline in Burundi during this period was due to its civil war (1993–2005). Starting in 2002, the curves diverged sharply, with life expectancy in Rwanda accelerating at a much faster rate than that of Burundi.
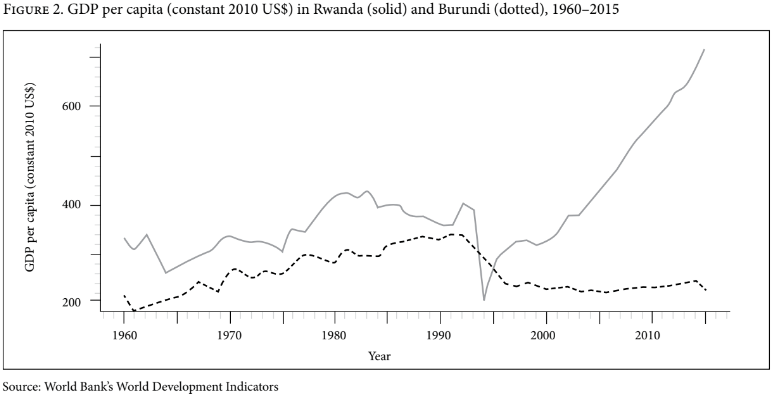
Source: World Bank’s World Development Indicators
Figure 2 shows that trends in economic growth were weakly positive for both countries from 1960 to 1981. Rwanda experienced economic shocks due to falls in the prices of coffee and agricultural exports in 1985, which persisted through the 1990s.[17] In 1994, Rwanda experienced a steep decline in GDP per capita as a result of the genocide but rebounded from 2000 onward. Burundi also experienced a decline in GDP per capita during the civil war that coincided with the Rwandan genocide, from which it has not recovered.
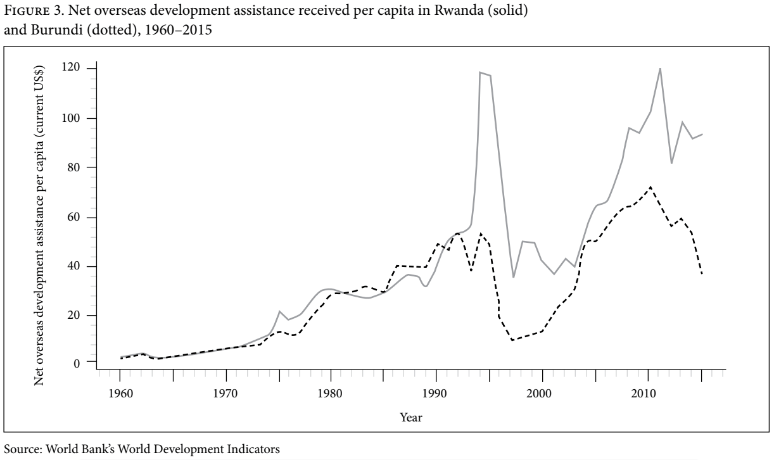
Overseas development assistance in Rwanda and Burundi accounts for a large proportion of overall government expenditure (between 30% and 40% in Rwanda and 60% in Burundi).[18] Foreign assistance in these two countries consists primarily of grants and loans from multilateral institutions. American and European donors are the major bilateral providers of such assistance. Reports in 2011 estimated that 25% (US$322 million) of overseas aid in Rwanda is spent on health, compared to 17% (US$102 million) in Burundi.[19]
Figure 3 shows similar levels of funding for both countries until 1992. Thereafter, overseas development assistance increased sharply for Rwanda but not for Burundi. Some authors argue that the rise in such assistance to Rwanda following the genocide could be attributed to guilt on the part of Western countries for their failure to intervene.[20] For the period from 2000 to 2010, Rwanda received increasing levels of overseas assistance. A decline in this assistance from 2010 to 2012 could be explained by the US government’s restriction of funds to Rwanda following reports of the country’s military intervention in the Congo.[21]
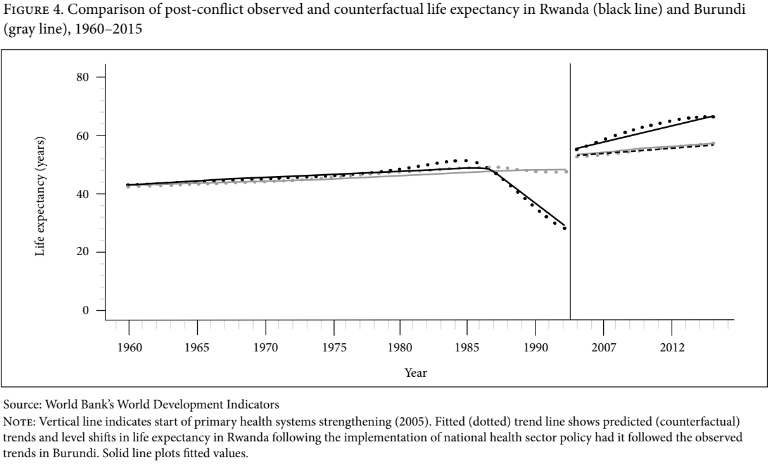
Figure 4 shows the level and trend in life expectancy in Rwanda compared to Burundi during the study period. During the postwar period, we found a significant annual increase in Rwanda’s life expectancy compared to Burundi’s upon adjustment for GDP per capita (β=0.69 years of life expectancy per annum, 95% CI: 0.19–3.56). This resulted in an estimated increase of 14.7 years (95% CI: 11.4–18.0) in life expectancy over the 11-year postwar period in Rwanda, compared to an estimated increase of 4.6 years (95% CI: 1.8–7.5) in Burundi over the same period.
Health policy analysis
Our observations above demonstrate that trends in health indicators and economic development were quite similar in Rwanda and Burundi prior to the outbreak of conflict, driven by similar contexts and government approaches to improve in these areas. Both countries saw declines in economic and health gains during the periods of political instability, but following the end of the conflicts, Rwanda experienced a much larger increase in life expectancy than Burundi. Much has been written on Rwanda’s progress in health and the observed successes of its health system with respect to maternal and child care and HIV control.[22] Far less has been written on Burundi, though analyses of some of its policies appear in the health and medical literature.[23] Below we compare the contexts, processes, and outcomes of health policy reform that occurred in Rwanda and Burundi after 2005.
Context
At the time of independence (1962) in both countries, colonization by Germany and Belgium had resulted in inequalities of opportunity between the majority Hutu and the minority Tutsi, favoring Tutsi as the enforcers of colonial rule. The Tutsi were the political elite and tended to hold positions of power within society. During the colonial period, foreign powers codified these class groupings into ethnic groupings, going as far as providing identity cards that delineated a person’s ethnicity. Following independence, the Hutu majority in Rwanda established a government that engaged in the oppression of minority Tutsi. In Burundi, Tutsi elite maintained their positions of power following independence, and used this power to intimidate and suppress Hutu opposition.[24]
The health systems in both countries were severely damaged following the genocide in Rwanda and the civil war in Burundi.[25] Infrastructure was destroyed, many health professionals lost their lives, and the war fueled the spread of HIV.[26] In such settings of endemic poverty and resource constraints, achieving adequate health coverage would prove to be a challenge following the wars in both countries.
Actors
Health policy reforms in Rwanda and Burundi were guided by different actors and were directed in different ways. In Rwanda, decisions were made by the national government. Health policy was communicated to Ministry of Health officials at the central and district levels through a series of health sector strategic plans, emphasizing the key areas of focus.[27] Nongovernmental organizations (NGOs) and multilateral donors were then consulted for technical and financial support.[28] Rwanda discouraged the independent implementation of health programs by NGOs, mandating that the work be done in collaboration with the government. In this way, Rwanda successfully negotiated with foreign implementing partners to guide funding directly to its government rather than to NGO partners, as in other countries. These arrangements allowed Rwanda’s government to maintain control over how projects were implemented and to steer policy.[29]
Burundi’s health policy was guided by both the Ministry of Health and NGOs. The presidential office also unilaterally decreed policy, including an abolition of user fees for delivery services for pregnant women and care for children under five.[30] Due to foreign funding structures, the Burundian government had separate bodies for health and for HIV/AIDS, leading to political conflict between the two branches.[31] The significant influence of foreign NGOs in health policy and implementation in Burundi may have reduced local capacity to direct policy.[32] Furthermore, a lack of coordination among programs possibly led to reduced gains in health-system performance due to conflicting priorities of the various actors. In conclusion, while the Rwandan government acted in a stewardship role, set policy, and directed international partners’ implementation activities in its facilities, the Burundian government struggled to set effective policy due to a lack of coordination between international actors and two branches of government.
Process and content
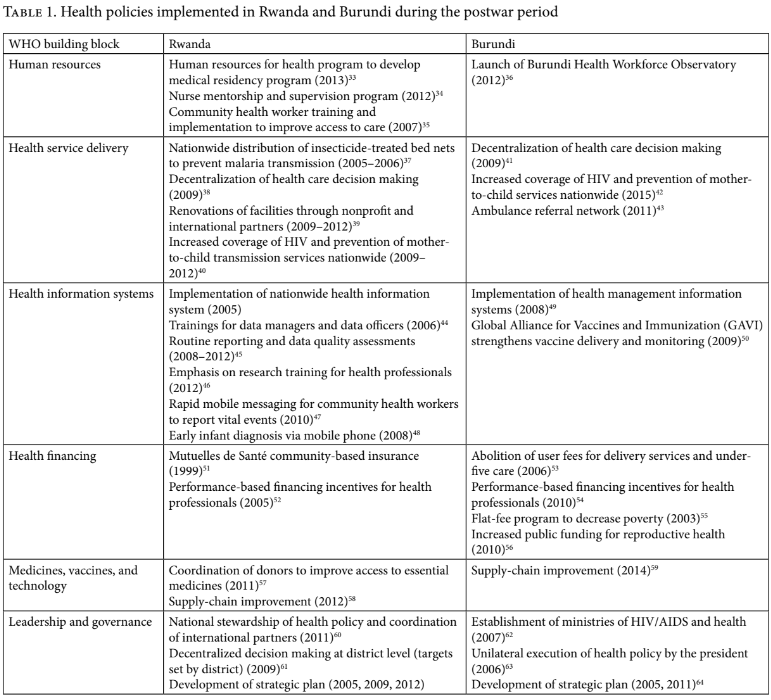
We categorized the major health policies adopted by each country using the World Health Organization’s “building blocks” (Table 1) and analyzed the “process” and “content” components of Walt and Gilson’s model.
Rwanda and Burundi adopted similar health policies to expand access to health care services. However, the manner in which these policies were implemented varied between the two countries.
Though both countries invested in health information systems, Rwanda’s political leadership in health drove its greater embrace of health information systems to monitor and study public health. Using a national health information system, Rwanda’s health ministry was able to use data to inform its priority setting and strengthen research skills among health workers.[65] To this end, it also integrated disease-specific systems for HIV, malaria, and tuberculosis so that policy makers could easily monitor multiple health statistics using the same system. Burundi’s health information system suffered from quality issues due to skills gaps.[66] Rwanda also experienced quality issues when rolling out its national community health database, finding poor concordance between electronic and paper records.[67] However, Rwanda was able to address these challenges by incorporating routine data quality assessments into its national data capture systems. Evaluations of health service delivery interventions were thus possible using those same data.[68]
Human resource density has been shown to be a significant predictor of countries’ ability to reduce under-five and maternal mortality and vaccine coverage.[69] During the postwar period, both Rwanda and Burundi struggled with a brain drain of medical personnel, which contributed to low health worker densities.[70] In response, Rwanda’s human resource interventions prioritized the capacity building of local health workers through formal academic training programs for physicians and mentorship for nurses at local clinics to improve the quality of under-five care.[71] In Burundi, health worker productivity was adversely affected by other health policy reforms. For example, increased demand for services followed the abolition of user fees for maternal and child health services, which led to increased demands on the health workforce and in turn reduced the effectiveness of the user-fee intervention.[72] Qualitative studies of community members’ perceptions of maternal services and neonatal care found that the poor quality of care in Burundi was related to health worker shortages and turnover.[73] Rwanda’s approach to working with partners to build heath workforce capacity led both to increased health worker density and improved quality of services, which contributed to greater efficiency in its health workforce compared to Burundi.
Both countries incorporated policies to increase access to care by removing financial barriers. In Rwanda, the government implemented a nationwide community-based health insurance scheme called Mutuelles de Santé, which enabled the poorest members of the population to access health care.[74] This program was later rebranded as “community-based health insurance.” Evaluations of the policy showed that insurance-holders experienced very few episodes of catastrophic health expenditure.[75] Recent evaluations have also found that children whose families have Mutuelles are significantly less likely to be stunted.[76] The same evaluation, conducted in 2010, estimated Mutuelles coverage to be 79% for children. Burundi attempted to address equity through the abolition of user fees for all under-five care and delivery-related expenses for all pregnant women.[77] This intervention led to increased utilization of services but also led to challenges for health providers in delivering the services because adequate financing mechanisms were not in place to recoup the costs.[78] Working with nonprofit partners, Burundi also implemented a policy to selectively target indigent members in a province covering roughly 330,000 people, through a card that would remove financial barriers to care. However, this intervention failed to remove the barrier for much of this population due to problems in correctly identifying its targeted beneficiaries.[79]
Discussion
Our analysis shows that following periods of violence, Rwanda’s and Burundi’s life expectancies diverged. Though both countries attempted to implement health policy reforms aimed at addressing health inequities, Rwanda was far more successful in improving population health. The key factors responsible for Rwanda’s relative success were stronger leadership, data-driven policy making, and greater political commitment to equitable health coverage.
Rwanda’s governing bodies are characterized by the integration of services and information, and strong leadership. Rwanda’s president has served for roughly 15 years. Effective health leadership was exercised in this period through an experienced public servant who served as executive secretary for Rwanda’s National AIDS Commission, then as permanent secretary for health, and finally minister of health. Rwanda’s stability in leadership over time allowed policies to be tested and scaled. Burundi, on the other hand, has had little stability in its executive office and has suffered from continued disruptions due to ongoing smaller conflicts with rebel groups.[80] Between 1993 and 2005, no fewer than seven people held the title of president, and two of them were assassinated while in office. This instability of government in Burundi led to a lack of coordination of health policy, whereas Rwanda’s relatively strong and stable institutions allowed it to make longer-term progress in health.
Another contributor to Rwanda’s success was its investment in health information systems and direction of health research. This allowed Rwanda to monitor disease burden and design and evaluate policies to address it.[81] Rwanda also successfully developed the research skills of its health workforce. Rwanda’s data-driven priorities for health research has made it attractive to foreign researchers and provided the country with the ability to develop lasting collaborations with them. On the other hand, Burundi has not succeeded in creating a government-led research infrastructure with strong national health information systems. The result has been that foreign groups have driven health research without creating local capacity.
Our analysis sought to estimate the effect of Rwanda’s health policy reforms by contrasting the observed increase in life expectancy in Rwanda with predicted life expectancy estimated from our model, assuming that changes post-reform had the same level and trend that we witnessed in Burundi. Our estimate will be unbiased if there is no co-intervention that occurred in 2005 that differentially affected life expectancy in one country but not the other, and did not result from health policy reform. Time-varying factors that affect both Rwanda and Burundi are controlled for by design. Because rapid gains in life expectancy arise mainly from the prevention of deaths in children, co-occurring social, economic, and political factors are unlikely to lead to rapid decreases in under-five mortality in the absence of health interventions for children. We thus believe that changes in life expectancy are best attributed to health system reforms focused on primary care.[82]
A limitation of our health policy analysis is that while we attempted to review all primary health care policies implemented in both countries during the study period, we could access only those materials that were available as research articles or as technical reports. However, by examining a wide range of policies in each country (using the health system building blocks approach), we have attempted to capture the mainstay of health policies explaining the divergence in life expectancy observed in Rwanda and Burundi.
Though Rwanda has made rapid gains due to strong leadership and evidence-based health policies, its government has come under criticism from the international community for its intolerance of opposition parties and limits to freedom of speech.[83] Despite these critiques, Rwanda has made remarkable progress in health and development following a period of acute instability, while Burundi’s progress has been less successful. Renewed violence in Burundi following political conflict over presidential term limits could lead to difficulties in sustaining health gains. In response to the outbreaks of violence in Burundi, Rwanda has accepted inflows of Burundian refugees, who have decided that Rwanda offers them better health and economic opportunities.
This case study provides a few lessons to other low-income countries seeking to implement universal health coverage. First, countries should have national policies in place for primary care delivery, although this alone is not sufficient for achieving better health outcomes. In addition, national governments should be encouraged to take the lead in setting strategy and building strong teams capable of implementing them at the national and subnational levels. Partnering with international nonprofits and academic institutions can provide opportunities for skill transfer and collaboration. Finally, investments in information systems are essential for evaluating and refining policies. Adopting these approaches could help governments of other low-income countries attain the right to health for their people.
Acknowledgments
The authors are indebted to colleagues at Inshuti Mu Buzima/Partners In Health Rwanda, the Rwandan Ministry of Health, and the Burundian Ministry of Health for their tireless work in implementing the programs discussed in this paper. This work stemmed from discussions in a course taught by Professors Sudhir Anand and Amartya Sen at the Harvard T. H. Chan School of Public Health. We appreciate the insights shared by the instructors and participants. Hari S. Iyer was supported in part by a National Institutes of Health research training grant (NIH, T32 CA 009001). The findings, interpretations, and conclusions expressed in this paper are those of the authors and, in the case of Adanna Chukwuma, do not necessarily represent the views of the World Bank, its executive directors, or the governments that they represent.
Hari S. Iyer, MPH, is a doctoral candidate in the Department of Epidemiology at the Harvard T. H. Chan School of Public Health, Boston, MA, USA.
Adanna Chukwuma, MBBS, MSc, ScD, is a Young Professional at the World Bank Group, Washington, DC, USA.
Jean Claude Mugunga, MD, MS, is associate director of monitoring, evaluation, and quality at Partners In Health, Boston, MA, USA.
Anatole Manzi, MPhil, MPH, is director of clinical practice and quality improvement at Partners In Health, Boston, MA, USA.
Melino Ndayizigiye, MD, MMSc, is clinical director at Partners In Health–Lesotho, Maseru, Lesotho.
Sudhir Anand, DPhil, is Centennial Professor at the London School of Economics, a professor of economics at the University of Oxford, UK, and an adjunct professor of Global Health at the Harvard T. H. Chan School of Public Health, Boston, MA, USA.
Please address correspondence to Hari S. Iyer. Email: hai161@mail.harvard.edu.
Competing interests: None declared.
Copyright © 2018 Iyer, Chukwuma, Mugunga, Manzi, Ndayizigiye, and Anand. This is an open access article distributed under the terms of the Creative Commons Attribution
Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
Statistical Appendix
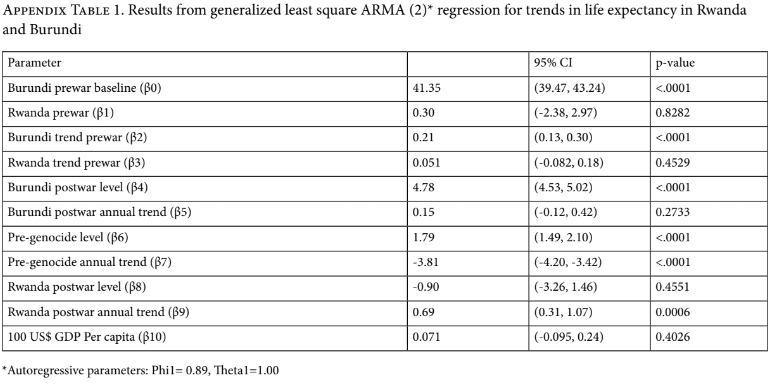
This appendix outlines the statistical model and parameter estimates used to produce Figure 4 in the main paper. We tested for autocorrelation using Durban-Watson statistics and visual inspections of autocorrelation function graphs, partial autocorrelation function graphs, and normal QQ plots of residuals as described by Wagner et al. [13].
We fitted a generalized least square regression of the form below, with an autoregressive lag term of 2 (Equation 1):
Equation 1
Where E[LEXP|C] is mean annual life expectancy conditional on covariates, RWANDA is a binary indicator variable coded as 1 for Rwanda and 0 for Burundi, TREND is an incremental time variable indicating number of years since 1959, and POSTWAR is a dummy variable indicating the postwar period compared to the pre-war period (starting in 2005). In inspecting the trends and levels of mean life expectancy in both countries, we found that Rwanda experienced unique, dramatic changes in life expectancy in the years immediately before and after the genocide. We decided to account for these changes in our linear regression model. RWPREGEN is a dummy variable indicating the pre-genocide period in Rwanda alone (defined as the period from 1987 to 1993), and GDPPC is the national estimate of GDP per capita for a given country in a given year and represented as constant 2010 US dollars. To make the beta coefficient more interpretable, we divided GDPPC by 100 so that a one-unit increase could be interpreted as a US$100 increase. Parameter estimates and 95% confidence intervals are provided in the table below.
- Heldring and J. Robinson, Colonialism and economic development in Africa (Cambridge: National Bureau of Economic Research Working Paper Series, 2012).
- International Covenant on Economic, Social and Cultural Rights, G.A. Res. 2200A (XXI) (1966), Art. 27.
- United Nations Department of Economic and Social Affairs, Millennium development goals report 2015 (Geneva: United Nations Department of Economic and Social Affairs, 2015).
- Ibid.
- International Monetary Fund, An approach to the poverty reduction action plan for Rwanda: The interim PSP (Washington, DC: International Monetary Fund, 2000).
- A. Binagwaho, P. Farmer, S. Nsanzimana, et al., “Rwanda 20 years on: Investing in life,” Lancet 384/9940 (2014), pp. 371–375; A. Binagwaho and K. Scott, “Improving the world’s health through the post-2015 development agenda: Perspectives from Rwanda,” International Journal of Health Policy and Management 4/4 (2015), pp. 203–205; United Nations Development Programme, Human development report 2013: The rise of the south; Human progress in a diverse world (Geneva: United Nations Development Programme, 2013).
- P. Uvin, “Ethnicity and power in Burundi and Rwanda: Different paths to mass violence,” Comparative Politics 31/3 (1999), pp. 253–271.
- L. Iaccino, “Rwanda: Ruling party RPF set to change constitution to allow President Kagame third term bid,” International Business Times c. (June 16, 2015).
- C. Jones and O. Donovan-Smith, “How the West lost Burundi,” Foreign Policy (August 28, 2015).
- World Bank, World Development Indicators (2015). Available at http://data.worldbank.org/data-catalog/world-development-indicators.
- G. Walt and L. Gilson, “Reforming the health sector in developing countries: The central role of policy analysis,” Health Policy and Planning 9/4 (1994), pp. 353–370.
- S. Anand and A. Sen, Human Development Index: Methodology and measurement, Human Development Report Office Occasional Paper 12 (New York: United Nations Development Programme, 1994).
- A. Wagner, S. Soumerai, F. Zhang, and D. Ross-Degnan, “Segmented regression analysis of interrupted time series studies in medication use research,” Journal of Clinical Pharmacy and Therapeutics 27/4 (2002), pp. 299–309; Government of Rwanda, Health Sector Policy (Kigali: Ministry of Health, 2005). Available at https://www.uhc2030.org/fileadmin/uploads/ihp/Documents/Country_Pages/Rwanda/HealthSectorPolicy.pdf; Ministre de la Sante Publique, Plan National de Developpement Sanitaire (Bujumbura: Republique du Burundi, 2005). Available at http://www.healthyfutures.eu/images/healthy/deliverables/D5.1/Burundi/burundi%20plan%20nationale%20de%20developpement%20sanitaire%202006%20-%202010.pdf.
- G. Walt and L. Gilson (see note 11).
- D. De Savigny and T. Adam, Systems thinking for health systems strengthening (Geneva: World Health Organization, 2009).
- M. Meredith, The fate of Africa: From the hopes of freedom to the heart of despair; A history of fifty years of independence, 1st ed. (New York: Public Affairs, 2005), pp. 494–495.
- P. Uvin, Development, aid and conflict: Reflections from the case of Rwanda (Helsinki: UNU World Institute for Development Economics Research, 1996).
- World Bank, Rwanda overview (2015). Available at http://www.worldbank.org/en/country/rwanda/overview; World Bank, Burundi: Country assistance strategy for the period FY13–16 (Washington, DC: World Bank, 2012).
- Development Initiatives, Investments to end poverty (United Kingdom: Development Initiatives, 2013), pp. 254–255, 278–279.
- P. Uvin (1996, see note 17).
- United Nations Security Council, Letter dated 12 November 2012 from the chair of the Security Council Committee established pursuant to resolution 1533 (2004) concerning the Democratic Republic of the Congo addressed to the president of the Security Council. S/2012/843. Available at http://www.securitycouncilreport.org/atf/cf/%7B65BFCF9B-6D27-4E9C-8CD3-CF6E4FF96FF9%7D/s_2012_843.pdf.
- A. Binagwaho et al. (2014, see note 6); Binagwaho and Scott (see note 6); P. Farmer, C. Nutt, C. Wagner, et al., “Reduced premature mortality in Rwanda: Lessons from success,” British Medical Journal 346/f65 (2013).
- J. Falisse, J. Ndayishimiye, V. Kamenyero, and M. Bossuyt, “Performance-based financing in the context of selective free health-care: An evaluation of its effects on the use of primary health-care services in Burundi using routine data,” Health Policy and Planning 30/10 (2015), pp. 1251–1260; C. Chaumont, C. Muhorane, I. Moreira-Burgos, et al., “Maternal and reproductive health financing in Burundi: Public-sector contribution levels and trends from 2010 to 2012,” BMC Health Services Research 15/446 (2015); P. Chi, P. Bulage, H. Urdal, and J. Sundby, “Barriers in the delivery of emergency obstetric and neonatal care in post-conflict Africa: Qualitative case studies of Burundi and Northern Uganda,” PloS One 10/9 (2015), p. e0139120.
- P. Uvin (1999, see note 7).
- A. Binagwaho et al. (2014, see note 6); W. Wakabi, “Ethnic war leaves Burundi’s health sector in ruins,” Lancet 369/9576 (2007), pp. 1847–1848.
- Ibid; P. Drobac, M. Basilico, L. Messac, et al., “Building an effective rural health delivery model in Haiti and Rwanda,” in P. Farmer, J. Kim, A. Kleinman, and M. Basilico (eds), Reimagining global health: An introduction (Berkeley, CA: University of California Press, 2013), pp. 167–179.
- Rwanda Ministry of Health, Health Sector Strategic Plan (Kigali: Ministry of Health, 2009). Available at http://www.healthyfutures.eu/images/healthy/deliverables/D5.1/Rwanda/rwanda%20health%20sector%20strategic%20plan%202009%20%202012%202009.pdf.
- A. Binagwaho and Scott (see note 6).
- Ibid.
- G. Nsengiyumva and L. Musango, “The simultaneous introduction of the district health system and performance-based funding: The Burundi experience,” Field Actions Science Reports Special Issue 8 (2012), p. 2351.
- S. Witter, J. Falisse, M. Bertone, et al., “State-building and human resources for health in fragile and conflict-affected states: Exploring the linkages,” Human Resources for Health 13/33 (2015), pp. 1–15.
- J. Cailhol, I. Craveiro, T. Madede, et al., “Analysis of human resources for health strategies and policies in 5 countries in sub-Saharan Africa, in response to GFATM and PEPFAR-funded HIV-activities,” Globalization and Health 9/52 (2013).
- A. Binagwaho, P. Kyamanywa, P. Farmer, et al., “The human resources for health program in Rwanda: New partnership,” New England Journal of Medicine 369/21 (2013), pp. 2054–2059.
- A. Manzi, H. Magge, B. Hedt-Gauthier, et al., “Clinical mentorship to improve pediatric quality of care at the health centers in rural Rwanda: A qualitative study of perceptions and acceptability of health care workers,” BMC Health Services Research 14/275 (2014).
- C. Mugeni, A. Levine, R. Munyaneza, et al., “Nationwide implementation of integrated community case management of childhood illness in Rwanda,” Global Health: Science and Practice 2/3 (2014), pp. 328–341; J. Condo, C. Mugeni, B. Naughton, et al., “Rwanda’s evolving community health worker system: A qualitative assessment of client and provider perspectives,” Human Resources for Health 12/71 (2014).
- Africa Health Workforce Observatory, Official launch of the Burundi health workforce observatory (January 26, 2012). Available at: http://www.hrh-observatory.afro.who.int/en/events/110-launch-hwo-burundi.html.
- C. Karema, M. Aregawi, A. Rukundo, et al., “Trends in malaria cases, hospital admissions and deaths following scale-up of anti-malarial interventions, 2000–2010, Rwanda,” Malaria Journal 11/236 (2012).
- Rwanda Ministry of Health (2009, see note 27).
- H. Iyer, E. Kamanzi, J. Mugunga, et al., “Improving district facility readiness: A 12-month evaluation of a data-driven health systems strengthening intervention in rural Rwanda,” Global Health Action 8 (2015), p. 28365.
- A. Binagwaho, P. Mugwaneza, A. Irakoze, et al., “Scaling up early infant diagnosis of HIV in Rwanda, 2008–2010,” Journal of Public Health Policy 34 (2013), pp. 2–16; S. Nsanzimana, S. Kanters, E. Remera, et al., “HIV care continuum in Rwanda: A cross-sectional analysis of the national programme,” Lancet HIV 2/5 (2015), pp. e208–e215.
- Nsengiyumva and Musango (see note 30).
- UNAIDS, Rapport d’activites sur la lutte contre la SIDA et rapport sur les progres enregistres vers un acces universel (Bujumbura: Conseil Nationale de Lutte Contre le Sida, 2015), pp. 17–19.
- K. Tayler-Smith, R. Zachariah, M. Manzi, et al., “An ambulance referral network improves access to emergency obstetric and neonatal care in a district of rural Burundi with high maternal mortality,” Tropical Medicine and International Health 18/8 (2013), pp. 993–1001.
- RTI International, Rwanda HMIS Assessment Report (Washington, DC: United States Agency for International Development, 2006).
- M. Nisingizwe, H. Iyer, M. Gashayija, et al., “Toward utilization of data for program management and evaluation: Quality assessment of five years of health management information system data in Rwanda,” Global Health Action 7 (2014) p. 25829; T. Mitsunaga, B. Hedt-Gauthier, E. Ngizwenayo, et al., “Utilizing community health worker data for program management and evaluation: Systems for data quality assessments and baseline results from Rwanda,” Social Science and Medicine 85 (2013) pp. 87–92.
- Binagwaho and Scott (see note 6); C. Cancedda, P. Farmer, P. Kyamanywa, et al., “Enhancing formal education and training programs in rural Rwanda: A partnership among the public sector, a nongovernmental organization, and academia,” Academic Medicine 89/8 (2014), pp. 1117–1124; Rwanda Ministry of Health, Guidelines for researchers intending to do health research in Rwanda (Kigali: Ministry of Health, 2012). Available at http://www.moh.gov.rw/fileadmin/templates/Docs/Researchers-Guidelines.pdf.
- F. Ngabo F, J. Nguimfack, F. Nwaigwe, et al., “Designing and implementing an innovative SMS-based alert system (RapidSMS-MCH) to monitor pregnancy and reduce maternal and child deaths in Rwanda,” Pan African Medical Journal 13/31 (2012).
- Binagwaho et al. (2013, see note 40).
- Nsengiyumva and Musango (see note 30).
- C. Carlson and A. Karibwami, GAVI health system strengthening support evaluation: Burundi case study (London: HSLP, 2009).
- S. Anand, C. Desmond, N. Marques, and H. Fuje, The cost of inaction: Case studies from Rwanda and Angola (Cambridge, MA: Francois-Xavier Bagnoud Center for Health and Human Rights, 2012), pp. 24–35; C. Lu, B. Chin, J. Lewandowski, et al., “Towards universal health coverage: An evaluation of Rwanda Mutuelles in its first eight years,” PloS One 7/6 (2012), p. e39282
- P. Basinga, P. Gertler, A. Binagwaho, et al., “Effect on maternal and child health services in Rwanda of payment to primary health-care providers for performance: An impact evaluation,” Lancet 377 (2011), pp. 1421–1428.
- Witter et al. (see note 31); B. Meessen, D. Hercot, M. Noirhomme, et al., “Removing user fees in the health sector: A review of policy processes in six sub-Saharan African countries,” Health Policy and Planning 26 (2011), pp. ii16–ii29.
- Falisse et al. (see note 23).
- S. Lambert-Evans, F. Ponsar, T. Reid, et al., “Financial access to health care in Karuzi, Burundi: A household-survey based performance evaluation,” International Journal for Equity in Health 8/36 (2009).
- Chaumont et al. (see note 23).
- Binagwaho and Scott (see note 6).
- Supply Chain Management System and Rwanda Ministry of Health, Rwanda NCSA and pharmaceutical supply chain strategic plan technical report (Arlington: Supply Chain Management System, 2013).
- M. Levenger, T. Busch, C. Bahati, and P. Namahoro, Burundi national supply chain assessment: Baseline capability and performance (Arlington, VA: Supply Chain Management System, 2014).
- G. Alleyne, “Lessons and leadership in health comment on ‘Improving the world’s health through the post-2015 development agenda: Perspectives from Rwanda’,” International Journal of Health Policy and Management 4/8 (2015), pp. 553–555.
- Rwanda Ministry of Health (2009, see note 27).
- Witter et al. (see note 31).
- Ibid.
- Burundi Ministry of Public Health and Fighting AIDS, National Health Development Plan 2011–2015 (Bujumbura: Ministry of Public Health and Fighting AIDS, 2011).
- Binagwaho and Scott (see note 6); Nisingizwe et al. (see note 45); Ngabo et al. (see note 47); D. Thomson, M. Semakula, L. Hirschhorn, et al., “Applied statistical training to strengthen analysis and health research capacity in Rwanda,” Health Research Policy and Systems 14/73 (2016).
- Carlson and Karibwami (see note 50).
- Mitsunaga et al. (see note 45).
- Mugeni et al. (see note 35).
- S. Anand and T. Bärnighausen, “Human resources and health outcomes: Cross-country econometric study,” Lancet 365 (2004), pp. 1603–1609; S. Anand and T. Bärnighausen, “Health workers and vaccination coverage in developing countries: An econometric analysis,” Lancet 369 (2007), pp. 1277–1285.
- N. Gupta, B. Maliqi, A. Franca, et al., “Human resources for maternal, newborn and child health: From measurement and planning to performance for improved health outcomes,” Human Resources for Health 9/16 (2011).
- Manzi et al. (see note 34); H. Magge, A. Manzi, F. Cyamatare, et al., “Mentoring and quality improvement strengthen integrated management of childhood illness implementation in rural Rwanda,” Archives of Disease in Childhood 100/6 (2015), pp. 565–570.
- M. Nimpagaritse and M. Bertone, “The sudden removal of user fees: The perspective of a frontline manager in Burundi,” Health Policy and Planning 26 (2011), pp. ii63–ii71.
- Chi et al. (see note 23); P. Chi, P. Bulage, H. Urdal, and J. Sundby, “A qualitative study exploring the determinants of maternal health service uptake in post-conflict Burundi and Northern Uganda,” BMC Pregnancy and Childbirth 15/18 (2015).
- Lu et al. (see note 51).
- Ibid; P. Saksena, A. Antunes, K. Xu, et al., “Mutual health insurance in Rwanda: Evidence on access to care and financial risk protection,” Health Policy 99/3 (2011), pp. 203–209.
- C. Lu, I. Mejia-Guevara, K. Hill, et al., “Community-based health financing and child stunting in rural Rwanda,” American Journal of Public Health 106/1 (2015), pp. 49–55.
- Meessen et al. (see note 53).
- ; Nimpagaritse and Bertone (see note 72).
- Lambert-Evans et al. (see note 55).
- “FNL Signs Peace Deal,” Africa Research Bulletin: Political, Social and Cultural Series 43/9 (2006), pp. 16775–16810.
- A. Binagwaho, C. Nutt, V. Mutabazi, et al., “Shared learning in an interconnected world: Innovations to advance global health equity,” Globalization and Health 9/37 (2013).
- S. Preston, P. Heuveline, and M. Guillot, Demography: Measuring and modeling population processes (Oxford: Blackwell Publishers, 2001).
- J. Tepperman, “Rebooting Rwanda,” Foreign Affairs (May/June 2014).