The Cholera Epidemic in Zimbabwe, 2008–2009: A Review and Critique of the Evidence
C. Nicholas Cuneo, Richard Sollom, and Chris Beyrer
Abstract
The 2008–2009 Zimbabwe cholera epidemic resulted in 98,585 reported cases and caused more than 4,000 deaths. In this study, we used a mixed-methods approach that combined primary qualitative data from a 2008 Physicians for Human Rights-led investigation with a systematic review and content analysis of the scientific literature. Our initial investigation included semi-structured interviews of 92 key informants, which we supplemented with reviews of the social science and human rights literature, as well as international news reports. Our systematic review of the scientific literature retrieved 59 unique citations, of which 30 met criteria for inclusion in the content analysis: 14 of the 30 (46.7%) articles mentioned the political dimension of the epidemic, while 7 (23.3%) referenced Mugabe or his political party (ZANU-PF). Our investigation revealed that the 2008–2009 Zimbabwean cholera epidemic was exacerbated by a series of human rights abuses, including the politicization of water, health care, aid, and information. The failure of the scientific community to directly address the political determinants of the epidemic exposes challenges to maintaining scientific integrity in the setting of humanitarian responses to complex health and human rights crises. While the period of the cholera epidemic and the health care system collapse is now nearly a decade in the past, the findings of this work remain highly relevant for Zimbabwe and other countries, as complex health and rights interactions remain widespread, and governance concerns continue to limit improvements in human health.
Introduction
The 2008–2009 cholera epidemic in Zimbabwe resulted in 98,585 reported cases and 4,287 reported deaths, making it the largest and deadliest in the history of Zimbabwe.1 The initial outbreak was notable for its high cumulative case fatality rate (4.3%) that persisted over a protracted duration (10 months). It was then followed by a second wave of infections lasting through June 2011.2 The epidemic emerged within months of two violent rounds of presidential elections that pitted President Robert Mugabe of the Zimbabwe African National Union-Patriotic Front (ZANU-PF), in power since 1980, against the primary opposition leader, Morgan Tsvangirai, of the Movement for Democratic Change (MDC).
In December 2008, in response to the epidemic, Physicians for Human Rights dispatched an emergency delegation to Zimbabwe to investigate the country’s health infrastructure and to document possible ongoing human rights abuses.3 The organization’s investigation revealed multiple such abuses as well as the true scale and scope of the epidemic. These findings have been supported by other reports.4 Most critically, ZANU-PF’s loss of municipal elections in Zimbabwe in 2005 led party leaders to refuse to fund municipal budgets for cities where it had been defeated, including in Harare, the capital.5 These retaliatory cuts led to a cessation of water purification for the city and, eventually, the redirection of raw human sewage into the city’s main reservoir.6
In this paper, we contextualize the Zimbabwean epidemic within a broader conceptual framework that outlines the role of political institutions in mediating cholera outbreaks. Using data from Physicians for Human Rights’ 2008 investigation, as well as supplementary information from the social science and human rights literature and from international news reports, we describe the human rights abuses that contributed to the epidemic in relation to a larger pattern of human rights violations by ZANU-PF leaders under the Mugabe regime, including the politicization of water and sanitation. Then, through a systematic review and content analysis of peer-reviewed scientific literature, we explore the extent to which these abuses, including ZANU-PF’s role in perpetrating them, were discussed or not discussed in scientific discourse.
With regard to the scientific literature on the cholera epidemic, it is striking how few authors directly noted the political or human rights aspects of the crisis. This seeming reluctance of the scientific community to fully address the political determinants of the epidemic exposes challenges to preserving scientific integrity in the setting of humanitarian responses to complex health and human rights crises. The imperative to seek access to vulnerable populations in such settings limits many partners from discussing the political and human rights aspects of these crises, even when they are well documented by other sectors, including human rights organizations. In the case of Zimbabwe, both the Zimbabwe Association of Doctors for Human Rights and the Zimbabwe Health Students Network had reported on abuses in this period and were active participants in the research effort described here.
While Zimbabwe’s cholera epidemic and health care system collapse is now nearly a decade in the past, our findings remain highly relevant for Zimbabwe and other countries in the region and beyond, as complex health and rights interactions remain all too common, and governance concerns continue to limit improvements in human health.
Methods
We utilized a mixed-methods approach that combined qualitative research from a primary investigation by Physicians for Human Rights in 2008 with a review of the social science and human rights literature and of international news reports. We then performed a systematic review and content analysis of articles published on the epidemic in peer-reviewed scientific journals.
Qualitative assessment: Physicians for Human Rights’ investigation
Physicians for Human Rights sent a team of four investigators, including the second and third authors of this paper, to Zimbabwe for seven days in December 2008 to conduct an emergency health and human rights assessment. Investigators comprised two physicians with expertise in public health and epidemiology and two with primary expertise in human rights. The team conducted a series of key-informant interviews and several focus group discussions, speaking with a wide range of stakeholders in urban and rural areas of four provinces (Harare, Mashonaland Central, Mashonaland West, and Mashonaland East); they interviewed a total of 92 participants. Participants included health care workers in private and public hospitals and clinics, medical students from Zimbabwe’s two medical schools, representatives from local and international nongovernmental organizations, representatives from United Nations agencies, Zimbabwean government health officials, members of parliament, water and sanitation engineers, farmers, and schoolteachers.
The qualitative domains of the interview instrument were adapted from health and rights instruments used in similar circumstances by Physicians for Human Rights, the Center for Public Health and Human Rights at Johns Hopkins University, and the School of Public Health at the University of the Western Cape, South Africa. Survey instruments, research protocols, and consent processes were reviewed and approved for adoption in Zimbabwe by Physicians for Human Rights’ Ethics Review Board – Human Studies Research, which has been operating since 1996 in accordance with the US Code of Federal Regulations, Title 45, Part 46. Local authorities were not approached in the beginning out of concern for the safety of participants.
After explaining the purpose of the investigation and the intent to conduct advocacy based on the findings, Physicians for Human Rights’ investigators asked participants for their informed verbal consent. All participants were aged 18 or older. Verbal, rather than written, consent was obtained to safeguard participant confidentiality: consent was not formally recorded in association with any identifying information for participants to ensure their safety in the event that research materials were intercepted by authorities while in the country.
Every effort was made to ensure participants’ protection and confidentiality and to reduce potential adverse consequences, such as political reprisal. Measures included data encryption and de-identifying the participant’s name, profession, residence, hospitalization, history of arrest, and information pertaining to family members and co-workers. Interviews took place in private settings and were never conducted if interviewers judged that risk to the participant was too high or that the participant’s ability to assess risk was impaired. Interviewers were careful not to publicize their presence in Zimbabwe or the purpose of their visit.
We supplemented qualitative data from this investigation with a review of social science, international news, and human rights sources to be able to present a comprehensive overview of the specific political and social determinants of the epidemic within the country’s wider human rights context.
Systematic review and content analysis: Discussion of political determinants in peer-reviewed scientific literature
We conducted a systematic review of articles published in peer-reviewed scientific journals between August 2008 and May 2013. We performed this review through the PubMed and Web of Knowledge databases using the search term “cholera AND Zimbabwe.” This search yielded 59 unique citations, including commentary/editorial pieces, news updates, and original research articles.
All 59 articles underwent a full text review. We included English-language articles for which the 2008–2009 Zimbabwean cholera epidemic was a major subject of discussion (rather than a peripheral example) and for which mention of at least one causal factor for the epidemic was provided. These inclusion criteria yielded 30 articles: 5 commentary/editorial pieces, 12 news updates, and 13 original research articles. The articles came from 22 peer-reviewed journals.
We further evaluated these 30 articles using a basic content analysis for inclusion of subject matter addressing the political dimensions of the epidemic, including Mugabe, his ZANU-PF political party, and the 2008 Zimbabwean presidential elections. The analysis involved searching the body of the text (excluding references) for the four terms and their etymological variants: “Mugabe,” “ZANU,” “election,” and “politic.” Representative quotations involving assertions of causality in the epidemic were extracted and tabulated.
Findings
This section presents our findings regarding the political and social determinants of the epidemic based on our in-country investigation and our supplementary literature review. In doing so, it utilizes a framework that we developed to understand cholera epidemics as a product of compromises in infrastructure, human rights, and health care and their interactions with the environmental, human biological, and pathogenic factors of the disease (Figure 1).
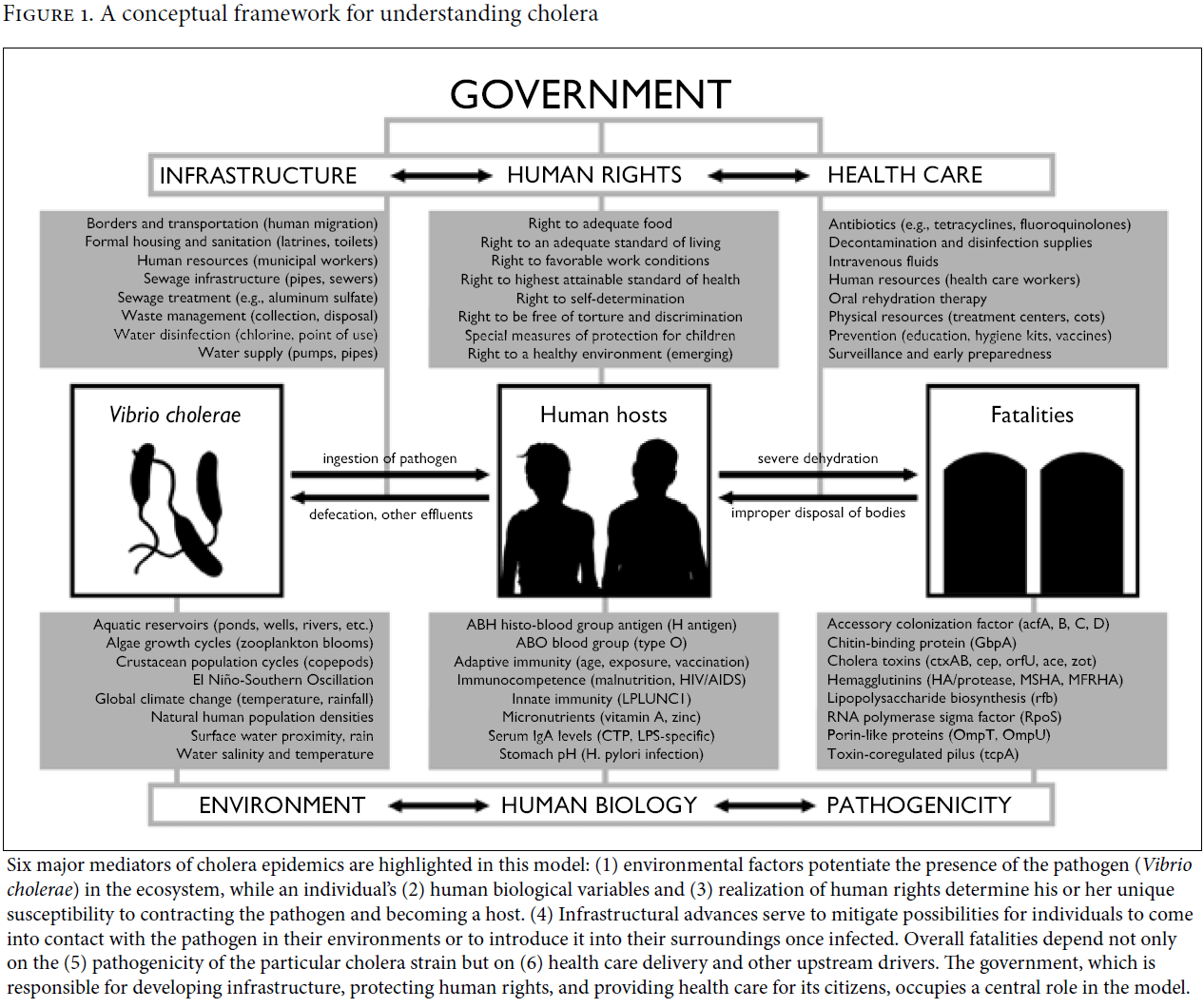
Six major mediators of cholera epidemics are highlighted in this model: (1) environmental factors potentiate the presence of the pathogen (Vibrio cholerae) in the ecosystem, while an individual’s (2) human biological variables and (3) realization of human rights determine his or her unique susceptibility to contracting the pathogen and becoming a host. (4) Infrastructural advances serve to mitigate possibilities for individuals to come into contact with the pathogen in their environments or to introduce it into their surroundings once infected. Overall fatalities depend not only on the (5) pathogenicity of the particular cholera strain but on (6) health care delivery and other upstream drivers. The government, which is responsible for developing infrastructure, protecting human rights, and providing health care for its citizens, occupies a central role in the model.
Infrastructure: The politicization of water and sanitation and the origins of the epidemic
Recent literature has highlighted the essential role of water and sanitation infrastructure in preventing and combating cholera.7 This relationship has been established since the earliest days of modern epidemiology, when John Snow identified the contaminated “Broad Street pump” as the source of the 1854 London outbreak. Maintaining proper infrastructure remains the most effective public health mechanism for combating the fecal-oral route of transmission on which the cholera pathogen, Vibrio cholerae, depends.8
A breakdown in the most basic elements of water and sanitation infrastructure underpinned the cholera epidemic in Zimbabwe. On May 9, 2005, just weeks after parliamentary elections in which the MDC opposition party had made a strong showing, ZANU-PF issued a national directive to overturn the 1976 Water Act and bring municipal water authorities across the country under the Zimbabwe National Water Authority. This directive came at a politically charged time, weeks before ZANU-PF’s execution of Operation Murambatsvina (“Drive Out Trash” in Shona language), which displaced more than 700,000 Zimbabweans—many of whom supported the opposition party. This government-sanctioned action was widely interpreted as a response to the MDC’s success in the election.9
The decision to usurp municipal authority over water, which had been under the control of the MDC in many areas of opposition support (including Harare), had major implications: (1) it immediately deprived MDC-controlled city councils of an important source of revenue, which they had been using to fund civic projects and maintain infrastructure; (2) it provided the cash-strapped ZANU-PF regime with a new stream of revenue (confirmed as a major motivation behind the move by one of our government informants); and (3) it allowed the ZANU-PF to assume control of another essential element for life—the government had a history of politicizing access to food amid famine through the national Grain Marketing Board (Table 1).10
In nationalizing water services, ZANU-PF claimed to be taking a step toward relieving Zimbabweans of “persistent water woes.”11 Instead, it raised water rates for residents while simultaneously neglecting infrastructure and diverting revenue to military and security forces.12 This approach predictably led to widespread service disruptions, resident discontent, and water-borne disease, particularly in and around Harare. In March 2006, there were 27 cholera-related deaths as civil groups in Harare warned of a “cholera time bomb” should the Zimbabwe National Water Authority not make essential repairs to the deteriorating water system. The water agency did not heed these calls: in August 2007, reports surfaced of it pumping raw sewage into Lake Chivero, the main source of water for Harare, a claim that was later confirmed by agency representatives who were quoted in regional media.13 Water supply became increasingly erratic while quality deteriorated. In March 2008, Mugabe suffered a definitive defeat by MDC opposition leader Morgan Tsvangirai, further inflaming the political situation in the country.
The 2008–2009 cholera epidemic began in late August in Chitungwiza, a high-density center outlying Harare that was also part of the Lake Chivero catchment area.14 Chitungwiza, a stronghold of MDC support, had been a target of ZANU-PF’s Operation Murambatsvina two years before, through which over 45% of the city’s million informally settled inhabitants had seen their homes and possessions seized or destroyed by ZANU-PF forces.15 The failure of ZANU-PF to maintain basic infrastructure, particularly in areas of opposition support, continued as the epidemic began to take root. On November 29, 2008, Harare residents reported a complete cut in water supply, as the Zimbabwe National Water Authority had ceased pumping water from its main treatment plant after running out of aluminum sulfate, one of four chemicals it had been using to treat the water. Multiple sources we spoke with, including two members of parliament, confirmed that ZANU-PF leaders continued to willfully neglect their responsibility in repairing infrastructure, even after the epidemic began.
Human rights: Decades of politically motivated abuses against a vulnerable population
Despite the country having signed and ratified both major international human rights covenants—the International Covenant on Civil and Political Rights and the International Covenant on Economic, Social and Cultural Rights—ZANU-PF, under Mugabe’s leadership, has engaged in human rights abuses since its earliest days in power.16 A review of the chronology of the actions, motivations, and consequences surrounding many of the regime’s human rights violations reveals a common theme: the targeted intimidation and punishment of opposition leaders and their supporters, along with the consolidation of power necessary to ensure the party’s continued reign in the country (Table 1).
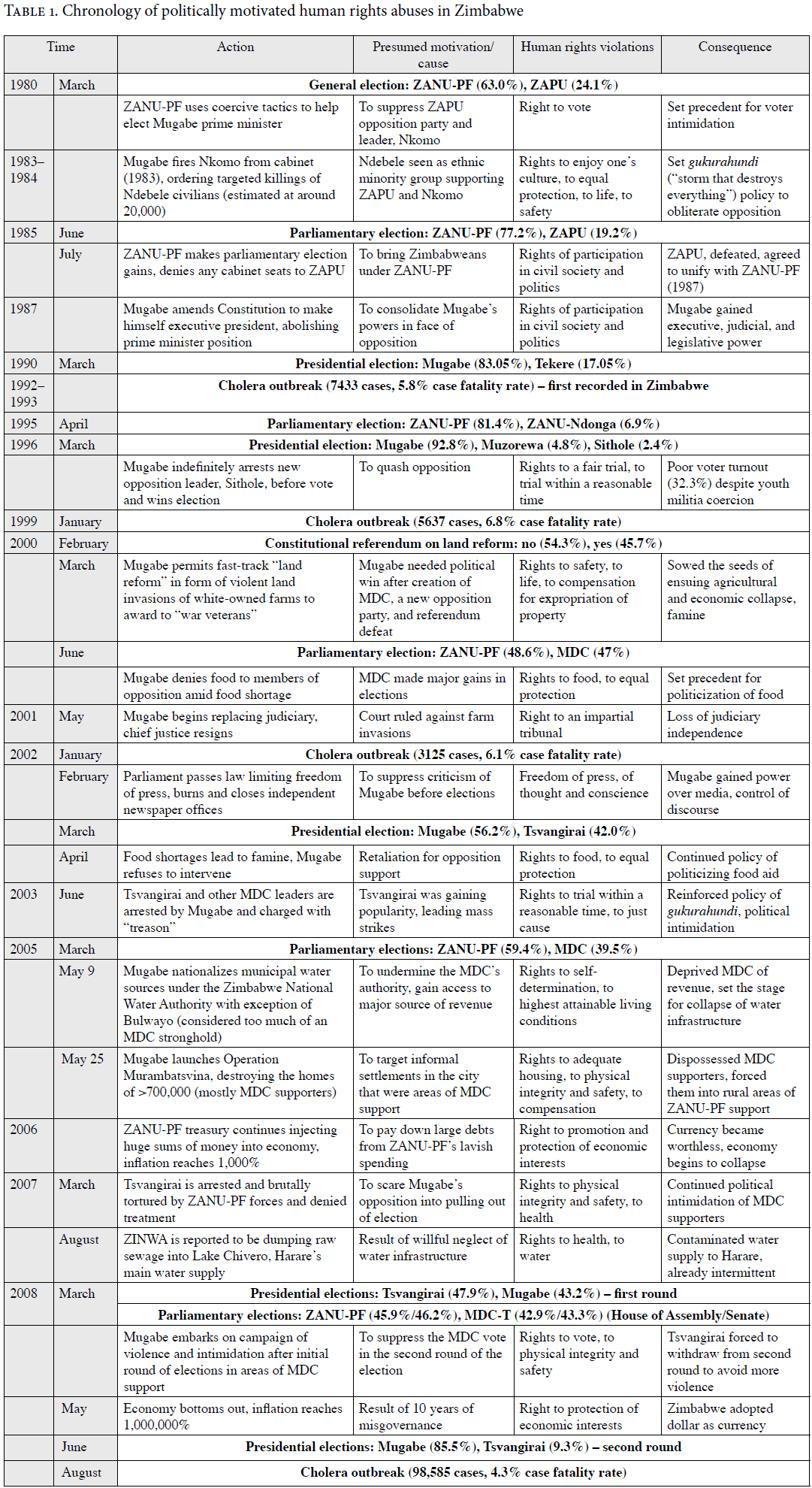
The 2008–2009 cholera epidemic was no exception to this theme. Emerging in a presidential election year, as did the previous cholera epidemic in 2002, the outbreak was the culmination of a series of politically motivated human rights violations that had intensified after the 2005 parliamentary elections. These violations had in fact become official policy under Operation Murambatsvina. Such policies were specifically directed at areas of MDC support, including Glenview, Chitungwiza, and Dzivarasekwa—districts that were among the most affected by the epidemic.17 While such a link may be dismissed as merely coincidental by those unaware of ZANU-PF’s human rights record, it is consistent with the Mugabe regime’s denial of food aid to areas of opposition during famines.18 An earlier example would be the killings of more than 20,000 civilians in Matabeleland (where Mugabe’s major opponent at the time, Joshua Nkomo, was drawing much of his support) in the 1980s through its policy of gukurahundi (“storm that destroys everything”).19
Health care: The economic collapse of a system and exacerbation of an epidemic
While the failures in water and sanitation infrastructure served to initially precipitate the epidemic and permit it to spread rapidly across the country, the failures of the health care system played a role in extending and exacerbating it. The Zimbabwean government’s public health response was characterized by early denial of the epidemic, suppression of health information, inadequate resourcing of health care centers, and abandonment of other health care priorities. As a result of these failures, the epidemic assumed a high initial case fatality rate, over five times the international standard of <1%.20
Cholera broke out in Zimbabwe following the 2008 elections and amid an economic crisis that led to the hyperinflation of the Zimbabwean dollar (inflation surpassed 2,000,000% in July 2008) and successive devaluations of the currency.21 The economic crisis was the result of ZANU-PF’s poor economic governance, fiscal indiscipline, and destruction of property rights following the implementation of the jambanja (“direct action”) policy in 2000.22 Jambanja called for the seizure of thousands of white-owned farms despite a constitutional referendum opposing such action and a constitutional court ruling against it.23 The violent land seizures undermined business confidence in Zimbabwe and gutted one of the country’s most productive sectors after the ousted farmers were replaced largely by those lacking the skills, resources, and access to credit to continue producing agricultural surpluses. Zimbabwe subsequently became the target of international sanctions that were targeted mainly at individuals and entities believed to be the most responsible for undermining democratic processes within the country.24
While jambanja sowed the initial seeds of Zimbabwe’s economic collapse, ZANU-PF’s economic policies sealed its fate. Through increased spending on military and security forces to appease party loyalists, ZANU-PF racked up huge deficits, which were financed by having the Reserve Bank of Zimbabwe print new money under the direction of the bank’s governor and the minister of finance. This money was then injected into the economy at unprecedented rates, fueling hyperinflation.25 Furthermore, ZANU-PF maintained a series of fiscal mandates, such as a fixed exchange rate and excessively high reserve requirements for banks, which made participating in Zimbabwe’s formal sector virtually impossible. Zimbabweans, who had enjoyed a relatively high standard of living in southern Africa, were impoverished by these policies, and several million (including many skilled workers such as health care professionals) were forced to leave the country in search of work and food security.
ZANU-PF’s primary focus on power—as opposed to governance—was highlighted during the cholera epidemic. When the outbreak began to surface amid Zimbabwe’s economic crash, ZANU-PF initially suppressed information about it.26 When it became difficult to hide the burgeoning disaster, ZANU-PF fabricated data and refused offers of assistance by local physicians.27 Georges Tadonki, head of the United Nations Office for the Coordination of Humanitarian Affairs in Zimbabwe at the time, was wrongfully terminated for blowing the whistle on the impending epidemic by United Nations country chief Agostinho Zacarias, who was later found to be colluding with ZANU-PF.28 The Zimbabwe Association of Doctors for Human Rights informed us that when the association offered help to the Harare City Council in treating cholera victims, the City Council responded, “We have the situation under control.” The MDC had lost its leadership of the council when Emmanuel Chiroto, who had been elected to serve as mayor in June 2008, was forced into hiding after his home was bombed and his wife presumably murdered by ZANU-PF supporters.29 Instead of making an early appeal for international aid, which would have injected essential foreign capital into the health system, Mugabe stalled for nearly four months, publicly declaring there to be “no cholera in Zimbabwe,” even after his own health minister, David Parirenyatwa, had finally issued such a call.
Our investigation unveiled the near-complete cessation of public sector health care delivery in the early days of the epidemic, a time when such intervention would have been especially critical for curbing the epidemic and associated fatalities. Between September and November 2008, most wards in the large public hospitals were shuttered. The acute collapse of the health system culminated in the dramatic November 17 closure of the Parirenyatwa Hospital and the Medical School, Zimbabwe’s premiere medical institutions, at the height of the epidemic due to a lack of water supply. Other hospitals became nonfunctional due to shortages in essential medicines and supplies and staff absenteeism as a result of the prohibitive costs of transportation.
Content analysis: Discussion of political determinants in peer-reviewed scientific literature
In our systematic search, we analyzed 30 articles from peer-reviewed scientific journals that addressed risk factors or described contextual factors related to the 2008–2009 cholera epidemic in Zimbabwe. The articles included 5 commentary/editorial pieces, 12 news reports and updates, and 13 original research papers (Table 2). Fewer than half (46.7%) explicitly mentioned politics as an influence, while only seven (23.3%) explicitly mentioned Mugabe’s or ZANU-PF’s involvement in water supply and sanitation disruptions, denial of the cholera epidemic, or refusal to respond to the crisis. Only two articles (6.7%) mentioned the antecedents of the 2005 and 2008 political elections. While many articles did cite the most direct causal factors responsible for the outbreak (that is, failures in basic infrastructure and health care delivery systems), few acknowledged the fundamental role of ZANU-PF, under the leadership of Mugabe, in generating these failures, despite widespread evidence in the general media, human rights reports, United Nations reports, and other fora.
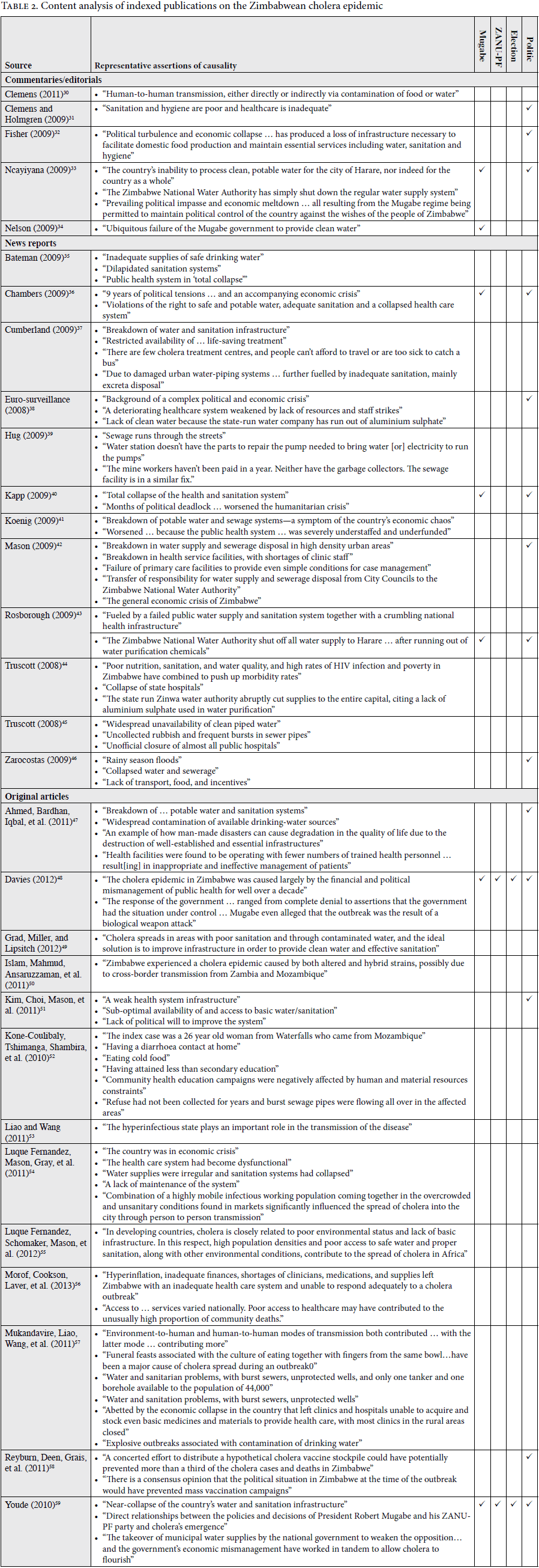
Several articles focused on individual-level risk factors. For example, the attribution of a “hyper-infectious state” to ongoing transmission was reported by one group; attending “funeral feasts associated with the culture of eating together with fingers from the same bowl” was reported by another; and “eating cold food” was noted by a third group.60 Others employed general and vague political terminology, such as describing the epidemic as “unfolding against a background of a complex political and economic crisis.”61
Seven of the thirteen original research papers presented mathematical, epidemiologic, and economic models based on data collected from the epidemic to either characterize pathogen transmission patterns from the epidemic or assess the suitability of a reactive mass vaccination campaign post hoc. Any discussion of the concomitant political situation beyond the superficial—for example, “exacerbated by a … lack of political will to improve the system”—was missing from the analyses, which contained no mention of Mugabe, ZANU-PF, or the elections.62
A few authors and journals stood out in their coverage of the explicit political and human rights dimensions of the outbreak. Jeremy Youde, in the International Journal, detailed the root causes of the outbreak and the political factors that exacerbated it.63 Notably, this Web of Science-indexed journal focuses on international relations, with little readership in the biomedical sciences. Interestingly, all three reports on the Zimbabwe outbreak published in the Lancet included an assessment of the political nature of the epidemic and the Mugabe regime’s complicity in it.64 In addition to the Lancet, the regional scientific literature, including two reports in the South African Medical Journal, was also notable for identifying the political factors behind the epidemic.65
Discussion
In this paper, we present a synthesis of original and supporting data documenting the major political forces behind the 2008–2009 Zimbabwean cholera epidemic, adding to the existing body of literature on the structural aspects of health care delivery as they relate to sociopolitical determinants, including human rights abuses.66 On the basis of Physicians for Human Rights’ investigation and our primary literature review, we found that the epidemic was a tragic case of a man-made disaster—an outcome of the politicization of water and aid by an authoritarian government with a long history of human rights abuses, acting in fear of opposition gains in recent elections.
We then critically assess the literature published on the epidemic in peer-reviewed scientific journals by using a systematic review and content analysis to explore the causal factors identified. Despite ample publicly available evidence linking direct actions by the Zimbabwean government under the control of Mugabe’s ZANU-PF party to the initiation, propagation, and exacerbation of the cholera epidemic, only a minority (23.3%) of authors referenced Mugabe or the ZANU-PF party, and fewer than half (46.7%) explicitly mentioned the role of politics in the health system collapse. In the rare cases when such factors were discussed, authors used passive and in some cases permissive language that at times obfuscated causality, negating the central role that ZANU-PF’s polices played in creating the crisis. Phraseology such as “a deteriorating health care system weakened by lack of resources and staff strikes” neglects the deliberate withholding of resources following the 2008 elections and may implicitly blame the striking health professionals.67 Medical and nursing staff, whose government salary did not even cover the cost of public transportation to go to work, did indeed protest the collapse of Zimbabwe’s health sector; they exercised their right to peaceful assembly to demand services, resources, food, water, and medicine for their patients. Several notable exceptions came from regional authors, who, not surprisingly, exhibited a more nuanced understanding of the relevant political dimensions of the epidemic. This distinction underscores the importance of regional medical literature concerning health crises with political dimensions. Of note, South Africa became involved in both mediating sanction-related discussions between Zimbabwe and the international community and in compelling a direct response after the epidemic began to cross Zimbabwe’s borders.
These findings demand inquiry. Why would scientists choose not to explicitly address the political dimensions of an epidemic? Possible explanations include a lack of political or human rights knowledge outside one’s disciplinary focus (which biases against addressing those issues), a belief that explicit political references in scientific literature would violate a perceived norm of neutrality, and (perhaps most commonly) deliberate avoidance of overt political analysis in order to protect one’s ability to conduct future research or maintain one’s personal safety.
The first example represents a narrow disciplinary focus on the part of scientists who fail to address issues outside the scope of their specific medical or public health expertise, even when such factors are directly relevant to the subject of inquiry. By neglecting to investigate or adequately address these elements when contextualizing their results, researchers oversimplify a complex system to a point at which the integrity of their observations may be compromised. Cholera—a preventable and curable infectious disease at the intersection of a wide range of social and biological mediators—is a prime example of a disease that necessitates multidisciplinary scientific inquiry, including an analysis of its political and social dimensions.
The second case of deliberate neutrality is similarly problematic. Here, cognizant investigators choose to withhold data based on an erroneous belief that revealing such evidence is tantamount to espousing an openly moral or ethical stance, thus violating a perceived doctrine of neutrality that guides scientific inquiry. Philosopher C. P. Snow, the authoritative voice of the “moral un-neutrality of science,” famously challenged this belief in a 1961 issue of Science.68 Nevertheless, a half century later, the belief remains pervasive, stemming from a persistent and flawed conflation of the terms “objectivity” and “neutrality.” Indeed, as Snow argued, there is nothing morally neutral about the pursuit of objectivity: “The desire to find the truth is itself a moral impulse, or at least contains a moral impulse … The way in which a scientist tries to find the truth imposes on him a constant moral discipline.”
The third example concerns the complicated phenomenon of the “silent witness.”69 We must not dismiss the threat to personal and professional security that academics and humanitarian workers face while practicing in politically charged environments around the world. The ability of humanitarian organizations such as the International Committee of the Red Cross and Médecins Sans Frontières to safely provide assistance in areas of conflict derives from their perceived political impartiality. One can readily infer the importance of such impartiality among humanitarian organizations in their reporting language. For example, they are often disinclined to name political entities responsible for health rights violations: “the health care system had become dysfunctional”; “water supplies were irregular and sanitation systems had collapsed”; and “a lack of maintenance of the system.”70 These tangible compromises in reporting are likely unavoidable, but they place weight on those groups less affected by such constraints to establish such causation explicitly and robustly on behalf of colleagues whose terms of engagement may make them less able to directly report on human rights and political determinants.
Conclusion
Researchers have shown the importance of understanding and addressing the political determinants of health in order to implement effective public health interventions that save lives. In this paper, we take a human rights-based approach to present findings from a primary investigation of a prolonged, high-mortality cholera epidemic in Zimbabwe, which we then utilize to frame a subsequent analysis of a systemic literature review. We found the peer-reviewed scientific literature to be lacking in appreciation of the basic human rights issues and political factors responsible for the outbreak and its subsequent pathogenicity. Using the example of the Zimbabwean epidemic, we argue that neglecting to address the political determinants of complicated epidemics can limit the integrity of scientific research. The man-made health system collapse in Zimbabwe serves as an important case study that elucidates the linkages between political violence and attendant rights abuses that ultimately led to thousands of preventable deaths from cholera.
Nicholas Cuneo, MD, is a Doris and Howard Hiatt Global Health Equity Resident in Internal Medicine and Pediatrics at Brigham and Women’s Hospital and Boston Children’s Hospital, Boston, MA, USA.
Richard Sollom, MA, MPH, is a senior fellow at the François-Xavier Bagnoud Center for Health and Human Rights at the Harvard T.H. Chan School of Public Health, Boston, MA, USA.
Chris Beyrer, MD, MPH, is Desmond M. Tutu Professor in Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Please address correspondence to C. Nicholas Cuneo. Email: cncuneo@bwh.harvard.edu.
Competing interests: None declared.
Copyright: © 2017 Cuneo, Sollom, and Beyrer. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- Z. Mukandavire, S. Liao, J. Wang, et al., “Estimating the reproductive numbers for the 2008–2009 cholera outbreaks in Zimbabwe,” Proceedings of the National Academy of Sciences of the United States of America 108/21 (2011), pp. 8767–8772.
- World Health Organization, Zimbabwe weekly epidemiological bulletin (Harare: WHO, 2011).
- R. Sollom, C. Beyrer, D. Sanders, and F. Donaghue, Health in ruins: A man-made disaster in Zimbabwe (Boston: Physicians for Human Rights, 2009).
- R. Gilpin, “Depoliticizing Zimbabwe’s economy: Solutions for two million percent,” United States Institute of Peace (2008). See also R. E. Howard-Hassmann, “Mugabe’s Zimbabwe, 2000–2009: Massive human rights violations and the failure to protect,” Human Rights Quarterly 32/4 (2010), pp. 898–920.
- J. Youde, “Don’t drink the water: Politics and cholera in Zimbabwe,” International Journal 65/3 (2010), pp. 687–704.
- “Zimbabwe: Untreated sewage makes its way into drinking water,” IRIN Humanitarian News and Analysis (August 23, 2007).
- J. M. Drazen and M. S. Klempne, “Disaster, water, cholera, vaccines, and hope,” New England Journal of Medicine 352/8 (2005), p. 827; N. H. Gaffga, R. V. Tauxe, and E. D. Mintz, “Cholera: A new homeland in Africa?” American Journal of Tropical Medicine and Hygiene 77/4 (2007), pp. 705–713N.
- A. Gulland, “Building hygiene infrastructure is key to ending Haitian cholera epidemic, agree agencies,” British Medical Journal 344 (2012), p. e395; D. A. Sack, R. B. Sack, and C. L. Chaignat, “Getting serious about cholera,” New England Journal of Medicine 355/7 (2006), pp. 649–651.
- See, for example, Howard-Hassman (see note 4); Youde (see note 5); S. Bracking, “Development denied: Autocratic militarism in post-election Zimbabwe,” Review of African Political Economy 32/104–5 (2005), pp. 341–357; M. Musemwa, “From ‘Sunshine City’ to a landscape of disaster,” Journal of Developing Societies 26/2 (2010), pp. 165–206.
- Human Rights Watch, Not eligible: The politicization of food in Zimbabwe (New York: Human Rights Watch, 2003).
- Musemwa (see note 9).
- Youde (see note 5).
- “Zimbabwe: Untreated sewage makes its way into drinking water” (see note 6). See also “South Africa-Zimbabwe: Cholera crosses the border too,” IRIN Humanitarian News and Analysis (November 19, 2008).
- M. A. Luque Fernandez, P. R. Mason, H. Gray, et al., “Descriptive spatial analysis of the cholera epidemic 2008–2009 in Harare, Zimbabwe: A secondary data analysis,” Transactions of the Royal Society of Tropical Medicine and Hygiene 105/1 (2011), pp. 38–45M.
- Bracking (see note 9).
- Howard-Hassmann (see note 4).
- Musemwa (see note 9). See also World Health Organization, Cholera country profile: Zimbabwe (Geneva: WHO, 2009).
- Human Rights Watch (see note 10).
- I. Phimister, “Zimbabwe is mine: Mugabe, murder, and Matabeleland,” Journal of South African and American Studies 10/4 (2009), pp. 471–478.
- C. Kapp, “Zimbabwe’s humanitarian crisis worsens,” Lancet 373/9662 (2009), p. 447.
- Gilpin (see note 4).
- Ibid.
- B. H. Kinsey, “Who went where … and why: Patterns and consequences of displacement in rural Zimbabwe after February 2000,” Journal of Southern African Studies 36/2 (2010), pp. 339–360.
- I. Phimister and B. Raftopoulos, “Mugabe, Mbeki and the politics of anti-imperialism,” Review of African Political Economy 31/101 (2004), pp. 385–400.
- S. H. Hanke, Zimbabwe: From hyperinflation to growth (Washington, DC: CATO Institute, 2008).
- Tadonki v. Secretary-General of the United Nations (United Nations Appeals Tribunal, Case No. 2013-449, Order No. 126, March 12, 2013).
- L. Makamure, “Cholera deaths masked in official figures,” Zimbabwe Independent (November 13, 2008).
- A. Rosen, “How the UN covered up a cholera epidemic in Zimbabwe: A country chief got too close to the Zanu-PF and fired an officer who was trying to stop a deadly disease,” Atlantic (April 3, 2013).
- P. Thornycroft, “Zimbabwe: Wife of Harare’s MDC mayor killed,” Telegraph (June 18, 2008).
- J. D. Clemens, “Vaccines in the time of cholera,” Proceedings of the National Academy of Sciences of the United States of America 108/21 (2011), pp. 8529–8530.
- J. Clemens and J. Holmgren, “Urgent need of cholera vaccines in public health-control programs,” Future Microbiology 4/4 (2009), pp. 381–385.
- D. Fisher, “Cholera in Zimbabwe,” Annals of the Academy of Medicine, Singapore 38/1 (2009), p. 82.
- D. J. Ncayiyana, “The Zimbabwe mayhem—how many people must die for the neighbours to act?” South African Medical Journal 99/1 (2009), p. 7.
- E. Nelson, “Beyond cholera—the Zimbabwe health crisis,” Lancet Infectious Diseases 9/10 (2009), pp. 587–588.
- C. Bateman, “Cholera—Getting the basics right,” South African Medical Journal 99/3 (2009), p. 138.
- K. Chambers, “Zimbabwe’s battle against cholera,” Lancet 373/9668 (2009), pp. 993–994.
- S. Cumberland, “An old enemy returns,” Bulletin of the World Health Organization 87 (2009), pp. 85–86.
- Eurosurveillance Editorial Team, “Concerted international response to control ongoing cholera epidemic in Zimbabwe,” Eurosurveillance 13/50 (2008), p. 13.
- A. Hug, “Inside Zimbabwe’s cholera epidemic,” Canadian Medical Association Journal 180/3 (2009), pp. 285–286.
- Kapp (see note 20).
- R. Koenig, “International groups battle Cholera in Zimbabwe,” Science 323/5916 (2009), pp. 860–861.
- P. R. Mason, “Zimbabwe experiences the worst epidemic of cholera in Africa,” Journal of Infection in Developing Countries 3/2 (2009), pp. 148–151.
- S. Rosborough, “World update: Cholera crisis in Zimbabwe,” Disaster Medicine and Public Health Preparedness 3/1 (2009), p. 11.
- R. Truscott, “Zimbabwe appeals for medical aid as it declares state of emergency over cholera epidemic,” British Medical Journal 337 (2008), p. a2942.
- R. Truscott, “Zimbabwe faces a ‘major health disaster,’ as hospitals close,” British Medical Journal 337 (2008), p. a2710.
- J. Zarocostas, “Aid organisations warn Zimbabwe’s cholera crisis is far from over,” British Medical Journal 338 (2009), p. b693.
- S. Ahmed, P. K. Bardhan, A. Iqbal A, et al., “The 2008 cholera epidemic in Zimbabwe: Experience of the icddr,b team in the field,” Journal of Health, Population, and Nutrition 29/5 (2011), pp. 541–546.
- S. E. Davies, “Duty in the time of epidemics: What China and Zimbabwe teach us,” Australian Journal of International Affairs 66/4 (2012), pp. 413–430.
- Y. H. Grad, J. C. Miller, and M. Lipsitch, “Cholera modeling: Challenges to quantitative analysis and predicting the impact of interventions,” Epidemiology 23/4 (2012), pp. 523–530.
- M. S. Islam, Z. H. Mahmud, M. Ansaruzzaman, et al., “Phenotypic, genotypic, and antibiotic sensitivity patterns of strains isolated from the cholera epidemic in Zimbabwe,” Journal of Clinical Microbiology 49/6 (2011), pp. 2325–2327.
- S. Y. Kim, Y. Choi, P. R. Mason, et al., “Potential impact of reactive vaccination in controlling cholera outbreaks: An exploratory analysis using a Zimbabwean experience,” Southern African Medical Journal 101/9 (2011), pp. 659–664.
- A. Kone-Coulibaly, M. Tshimanga, G. Shambira, et al., “Risk factors associated with cholera in Harare City, Zimbabwe, 2008,” East African Journal of Public Health 7/4 (2010), pp. 311–317.
- S. Liao and J. Wang, “Stability analysis and application of a mathematical cholera model,” Mathematical Biosciences and Engineering 8/3 (2011), pp. 733–752.
- Luque Fernandez et al. (2011, see note 14).
- M. A. Luque Fernandez, M. Schomaker, P. R. Mason, et al., “Elevation and cholera: An epidemiological spatial analysis of the cholera epidemic in Harare, Zimbabwe, 2008–2009,” BMC Public Health 12/442 (2012).
- D. Morof, S. T. Cookson, S. Laver, et al., “Community mortality from cholera: Urban and rural districts in Zimbabwe,” American Journal of Tropical Medicine and Hygiene 88/4 (2013), pp. 645–650.
- Mukandavire (see note 1).
- R. Reyburn, J. L. Deen, R. F. Grais, et al., “The case for reactive mass oral cholera vaccinations,” PLoS Neglected Tropical Diseases 5/1 (2011), p. e952.
- Youde (see note 5).
- Liao and Wang (see note 53); Mukandavire (see note 1); Kone-Coulibaly et al. (see note 52).
- Eurosurveillance Editorial Team (see note 38).
- Kim et al. (see note 51).
- Youde (see note 5).
- Kapp (see note 20); Nelson (see note 34); Chambers (see note 36).
- Ncayiyana (see note 33); Bateman (see note 35).
- See, for example, P. Farmer, Pathologies of power: Health, human rights, and the new war on the poor (Berkeley: University of California, Berkeley, 2005); S. Gruskin, “History, principles, and practice of health and human rights,” Lancet 370/9585 (2007), pp. 449–455; J. M. Mann, “Health and human rights,” British Medical Journal 312/7036 (1996), pp. 924–925; M. Marmot, “Social determinants of health inequalities,” Lancet 365/9464 (2005), pp. 1099–1104.
- Eurosurveillance Editorial Team (see note 38).
- W. Weaver, C. P. Snow, T. M. Hesburg, and W. O. Baker, “The moral un-neutrality of science,” Science 133/3448 (1961), pp. 255–262.
- See, for example, F. Terry, Condemned to repeat?: The paradox of humanitarian action (Ithaca, NY: Cornell University Press, 2002), p. 25; M. Anderson, “You save my life today, but for what tomorrow? Some moral dilemmas of humanitarian aid,” in J. Moore (ed), Hard choices: Moral dilemmas in humanitarian intervention (Lanham, MD: Rowman and Littlefield Publishers, 1998), pp. 137–156.
- Luque Fernandez et al. (2011, see note 14).